

Abstract
Objective:
Addressing recruitment challenges faced by researchers when the intended participants are young individuals from minority communities is crucial to prevent increases in study costs, prolonged length of the study, and loss of generalizability that may occur due to the resulting higher attrition rates. This article focuses on understanding the differences in census-tract level income, education, and socioeconomic status of young Latina and African American female participants and non-participants during the first 26 months of recruitment (June 2006–August 2008) in a longitudinal biobehavioral study.
Design:
The Transitions Study examines the psychological and physiological determinants influencing the decrease in physical activity during puberty among Latina and African American girls aged 8 to 11 years within the greater Los Angeles area. Recruitment and retention through five main steps in the process were examined: telephone contact, telephone screening, consent, clinical screening, and baseline overnight visit.
Results:
As of August 2008, the recruitment pool consisted of 110 African Americans (17.8%) and 373 Latinas (60.4%); of these, only 40 Latinas and 11 African American girls completed the final step into the study. African Americans were less willing to provide their phone numbers, but more likely to be reached at initial phone contact than Latino families.
Conclusions:
Understanding the heterogeneity within minority populations, population characteristics, through careful and timely analyses, could be used to adjust recruitment and retention strategies in a study involving minority youth.
Keywords: Recruitment, African American, Latino, Female, Minority, Socioeconomic, Census, Transitions Study, Physical Activity, Obesity
Introduction
Recruitment of study participants is one of the most important and challenging processes in research. Underestimating the time, resources, and knowledge of the target population needed to successfully recruit and retain participants has many risks. Risks include longer study length, higher drop-out rates and study costs, loss of data and statistical power.1
There are many obstacles when facilitating the recruitment of minority populations. These obstacles include distrust of the research system, language barriers, community and individual perceptions and attitudes toward the diseases and health risks in question, time commitment, fear of blood collection process, and incongruity between the community’s and researcher’s goals.2–5 More research is needed in minority youth who are disproportionately affected by obesity and its related health outcomes.6 However, recruitment of minority youth requires additional considerations. African American parents are more reluctant to have their children participate in research studies, especially studies that involve clinical examinations.5 Villarruel and colleagues7 found that parental opinions and involvement had a strong influence on a child’s desire to participate among Latinos, suggesting that researchers should consider guardian involvement. Additionally, respecting cultural and personal values while offering support and trust throughout the recruitment process proved to be effective for the Latino population.7 Overall, the literature on the processes of recruitment of minority populations to studies is limited.8 There are few prevention trials, longitudinal studies, or clinical studies involving minority youth. There are fewer studies that look directly at the recruitment of African American and Latino children.9,10
The Transitions Study is an ongoing longitudinal study designed to examine the psychological and physiological determinants of the profound decrease in physical activity that occurs in Latinas and African American girls during puberty. The recruitment of African American and Latina children into this intense metabolic study has been a difficult process and the various strategies used to recruit and retain participants were not completely effective. Consequently, the girls recruited and retained may have different characteristics than those who did not enter the study or dropped out of the study. Both the challenge of recruitment and the disparities seen in the recruited numbers between the Latina and the African American groups after two years of recruitment efforts led to a closer examination of population characteristics. This article examines whether African American and Latina participants and non-participants differ on census-tract level socioeconomic status, income, or education. Understanding these differences may help researchers focus efforts to obtain representative study samples and improve retention strategies.
Methods
Study Procedures
This article documents the first 26 months of study recruitment for the Transitions Study (June 2006–August 2008). The study aimed to recruit 50 Latinas and 50 African American girls in Los Angeles County. Eligibility was limited to girls aged 8–11 years, of African American or Latina descent, and classified as Tanner stage 1 or 2, which are the two initial stages of the Tanner scale developed to assess the degree of physical pubertal development through evaluation of primary and secondary sex characteristics.11 The participants were defined as Latina or African American if they, their parents, and their grandparents self-identified with the specified cultural group. To reduce heterogeneity within the sample of Latinas, we only recruited Mexican American and Central American individuals, who constitute the largest percentage of the Hispanic community in Greater Los Angeles. Overweight girls (≥85th age-and-sex-specific Centers for Disease Control body mass index [BMI] percentile)12 were eligible if they met ethnicity, age and Tanner stage criteria. Girls who were not considered overweight (<85th percentile) were considered eligible if they had at least one parent who was overweight or had been diagnosed with diabetes. Girls were not eligible to participate if they had diabetes, a fasting plasma glucose ≥126 mg/dL, used any medications that alter body composition or insulin action/secretion, had a disease that alters body composition or insulin action/secretion, or had a previous diagnosis of any major illness since birth. To minimize travel burden for staff and participants during the 5-year study, only participants who lived within a 20-mile radius of the University of Southern California (USC) General Clinical Research Center (GCRC) were invited into the study.
Several steps were required to recruit girls into the study: 1) telephone screening with interested individuals to complete a brief eligibility evaluation questionnaire, an appointment for consent was then made for eligible participants; 2) informed parental consent and child assent; 3) clinical screening by a physician to perform Tanner staging with a physical exam to confirm study eligibility; and 4) attending the first of 4 annual overnight clinical stays in which anthropometric, metabolic, and psychosocial evaluations are performed. Scheduled approximately two weeks after the clinical screening, the overnight stays at the USC GCRC included a complete medical history evaluation, a battery of psychosocial questionnaires, measurement of height, weight and body fat, and a metabolic evaluation including a frequently sampled intravenous glucose tolerance test (FSIVGTT). Due to the young age of the participants (mean=9.3 years, SD=1.4), a parent/guardian was required to stay overnight with their child in the hospital for the overnight stays. This study was approved by the USC Institutional Review Board.
Data Collection and Recruitment Overview
Recruitment strategies for the Transitions Study targeted Latinas and African American girls aged 8–11. Brochures, fliers, and comprehensive presentations provided simple descriptions of eligibility criteria, study procedures and study goals in both English and Spanish.
Trained recruiters, university research assistants, and students from diverse ethnic backgrounds were used. Recruiters visited a variety of locations and events in South and East Los Angeles and in the San Gabriel Valley. A bilingual recruiter was always present when recruiting Latino populations. Approval to visit schools was obtained from all participating school district research review boards.
To help minimize attrition rates, families were offered $25 gift cards for each overnight visit completed and $25 for each subsequent quarterly completed. Parents received an additional $20 if they drove their daughters to the overnight visit at the hospital, rather than have a Transitions team member provide transportation. Additionally, each participant was assigned to a specific Transitions Study team member who served as her main study contact and mentor throughout the study. Mentors kept in touch with both the girls and their families via email or phone. Mentoring events were held approximately twice a year for the participants, potential participants, and interested friends and family members, and included health education and tutoring, physical activity sessions, a health fair, visits to museums, and picnics.
This article tracks the recruitment process from initial contact to first overnight stay (baseline assessment) for all potential participants.
Obtaining Census Tract Data
Telephone numbers and addresses provided to the Transitions Study recruitment staff were coded to the census tract as a socioeconomic status (SES) indicator using the US Census Bureau’s online mapping engine, American FactFinder.13 Socioeconomic status corresponds to the median household income and distribution of educational attainment for all residents aged ≥25 years living in the census tract at the time of the 2000 census.14 The socioeconomic status indicator is coded from 1 (low) to 5 (high). The analysis also includes the separate factors that create SES, including the average years of educational attainment of adult residents of her census tract of residence and the median household income for her census tract. The analyses presented here are restricted to families who reside in Los Angeles County.
Statistical Analyses
The analyses assessed the socioeconomic and ethnic differences between the participants recruited and not recruited. Means and frequencies were used to present the descriptive statistics of the sample. Logistic regression was used to determine whether ethnic group membership predicted progression through each step in the recruitment process, as well as determining if different socioeconomic variables (income, education, and SES) were predictors of successful progression through each step in the recruitment process according to ethnicity. Significance was set at P<.05. Statistical analyses were completed using SAS 9.1(v3) statistical software package.
Results
Transitions Study personnel acquired names and contact information from 618 girls in Los Angeles County from recruitment efforts made from June 2006–August 2008. Fifty-one girls completed the baseline GCRC assessment.
Figure 1 presents the African American and Latina recruitment outcome through each step of the study. Those who were not contacted (16 African Americans and 90 Latinas) did not qualify based on preliminary screening of age, ethnicity, and sex provided on the recruitment forms, provided wrong/disconnected telephone numbers, were not able to be contacted after 7 attempts on different days, or contact was still pending. Of the 110 African Americans who showed initial interest in the study, 11 (10%) completed the baseline overnight stay. Among Latino families, of the initial 373 contacted, 40 (10.7%) completed the overnight stay. Those who did not progress through the entire process included those who lost interest; were ineligible at screening due to Tanner stage, weight or ethnicity; did not attend a consent, screening or overnight appointment; or lost contact with the study staff.
Fig 1.
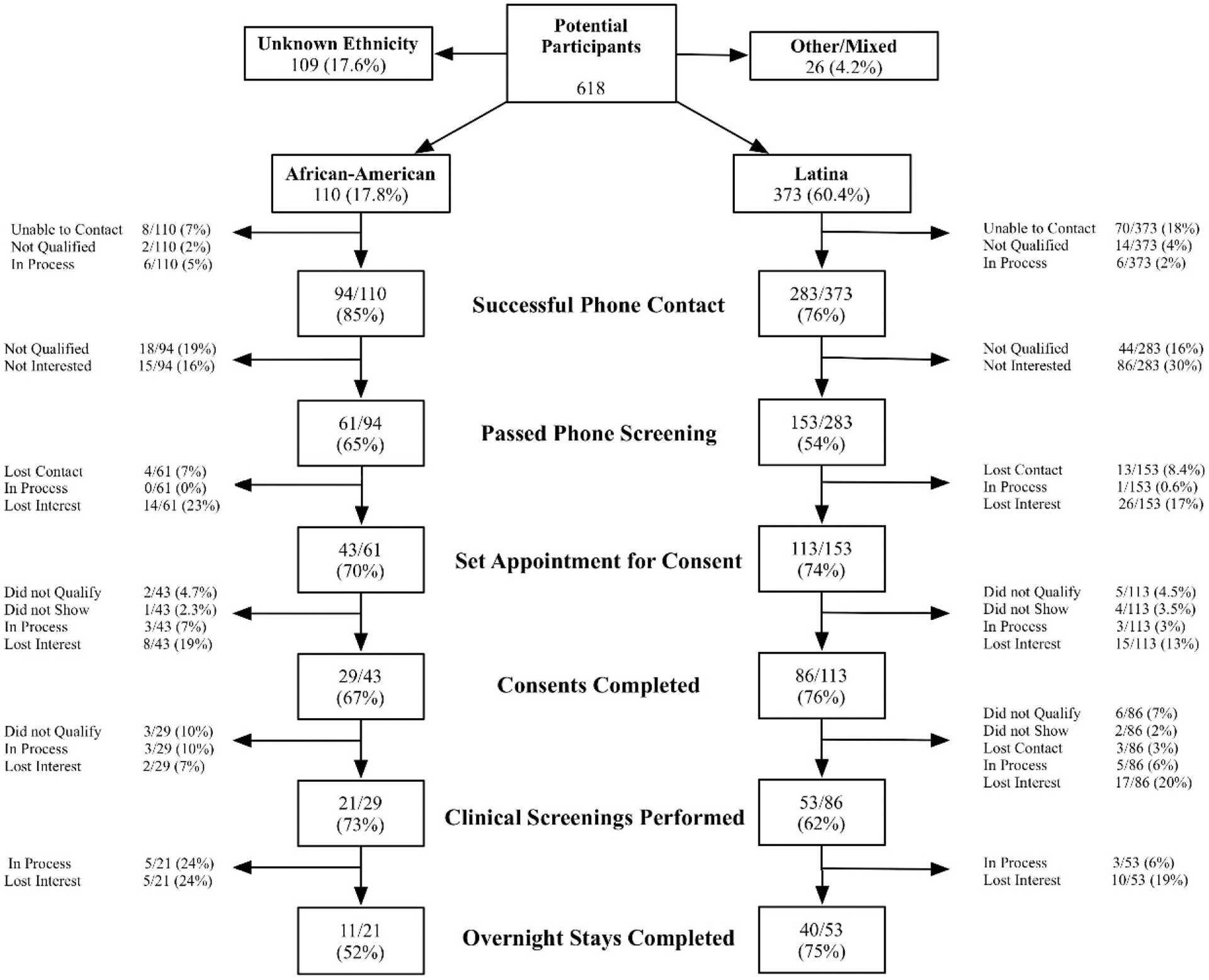
Participant recruitment and retention in the Transitions Study from June 2006–August 2008
Table 1 shows the demographic characteristics of all study subjects. The sample includes 618 subjects, 60.4% Latina, 17.8% African Americans. Girls with unknown ethnicity (17.6%) or other/mixed ethnicity (4.2%) were excluded from these analyses. Of the total, 334 girls (254 Latinas; 80 African Americans) provided a contact source used to obtain the census SES data. Girls were from 186 distinct census tracts. There was no significant difference in median household income between the African American and Latino subjects. African American participants lived in areas characterized by higher education and SES levels (P<.0001).
Table 1.
Characteristics of all potential participants (N=618) for the Transitions Study, June 2006–August 2008†
| Potential Participants | |
|---|---|
| Total | 618 |
| Latina | 373 (60.4%) |
| African American | 110 (17.8%) |
| Unknown | 109 (17.6%) |
| Other race | 26 (4.2%) |
| Individuals with US Census 2000 tract data available* | |
| African American | Latina | P | |
|---|---|---|---|
| Total | 80 of 110 (73%) | 254 of 373 (68%) | |
| Census 2000: Average median household income ($) in geographic subarea | 30,742 (11,012) | 28,786 (9,866) | 0.13 |
| Census 2000: Completed years of education for those age 25+ within geographic subarea | 11.31 (2.2) | 10 (2.0) | <.0001 |
| Census 2000: Socioeconomic status (1: low, 5: high) of geographic subarea | 2.13 (1.05) | 1.65 (0.82) | <.0001 |
| Individuals in each socioeconomic status category | |||
| Low 1 | 27 (34%) | 133 (52%) | 0.001 |
| 2 | 26 (33%) | 88 (35%) | |
| 3 | 19 (24%) | 25 (9.8%) | |
| 4 | 6 (7.5%) | 6 (2.4%) | |
| High 5 | 2 (2.5%) | 2 (0.8%) |
Includes only individuals who were considered for further analyses (African Americans and Latinas only).
Data given in mean (standard deviation) or n (%).
Table 2 shows the results of the logistic regression, comparing African Americans’ and Latinas’ likelihood of progressing through study recruitment. The research team was more likely to complete the initial telephone contact with African Americans than with Latinas who provided contact information (OR=1.87, 95% CI: 1.05, 3.34). There were no other significant differences between the two populations regarding telephone screening, consent, clinical screening, and overnight phases.
Table 2.
Likelihood of successfully completing study steps among African American and Latina girls using logistic regression - detailed analysis of Figure 1
| Steps | African American n (%) |
Latina† n (%) |
p | |
|---|---|---|---|---|
| Contact | Contacted | 94 (85) | 283(76) | |
| Not contacted‡ | 16 (15) | 90 (24) | ||
| OR (95% CI) | 1.87 (1.05, 3.34)* | 1.00 | .04 | |
| Telephone screening | Passed screening | 61 (65) | 153 (54) | |
| Failed screening | 33 (35) | 130 (46) | ||
| OR (95% CI) | 1.57 (0.97, 2.56) | 1.00 | .07 | |
| Consent | Completed consent | 29 (48) | 86 (56) | |
| Did not consent§ | 32 (52) | 67 (44) | ||
| OR (95% CI) | .71 (.39, 1.28) | 1.00 | .25 | |
| Clinical screening‖ | Completed screening | 24 (92) | 59 (73) | |
| Did not screen | 2 (8) | 22 (27) | ||
| OR (95% CI) | 4.48 (.98, 20.53) | 1.00 | .05 | |
| Passed screening | 21 (88) | 53 (90) | ||
| Failed screening | 3 (12) | 6 (10) | ||
| OR (95% CI) | .79 (.18, 3.46) | 1.00 | .76 | |
| Overnight‖ | Completed overnight | 11(58) | 40 (80) | |
| Did not attend | 8 (42) | 10 (20) | ||
| OR (95% CI) | .34 (.11, 1.08) | 1.00 | .07 |
P<.05
Reference group
Includes individuals who were still trying to be contacted by recruiters.
Includes individuals who were not interested, disqualified, and could not be contacted between the time of telephone screening and when an appointment for consent was made, to actual time of intended consent.
Excludes individuals listed as “in process” at the time of data analysis.
Using logistic regression, the effects of income, education, and SES on the outcome at each step of the study are presented in Table 3. Latino families with greater than or equal to the median income of the study population (OR=.34, 95%CI: .17–.65), greater than 9.7 years of education (OR=.33, 95%CI: .17–.65), and higher SES (OR=0.31, 95%CI: .16–.61) were statistically significantly less likely to be contacted. Latino families of higher income level were 52% less likely to consent and 90% less likely to pass the screening than Latino families in lower income census tracts (OR=.48, 95% CI: .23–.97; OR=.10, 95% CI: .01–.92, respectively). The effects of the socioeconomic measures were not significantly associated with progression through the study for African Americans.
Table 3.
Logistic regression showing the effect of different measures of socioeconomic variables (based on census tract of residence and US Census Bureau data for the year 2000) on the outcome at each step of the Transition Study among African Americans and Latinas
| STEPS | African American | Latina | ||
|---|---|---|---|---|
| Contact | OR (95%CI) | OR (95%CI) | ||
| Contacted/not contacted, n | 73/7 | 204/50 | ||
| Income ‡ | <$27,431 | 1.00 | 1.00 | |
| ≥$27,431 | 2.14 (.45–10.30) | .34 (.17–.65)* | ||
| Education§ | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | .47 (.05–4.19) | .33 (.17–.65)* | ||
| SES ‖ | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | .77 (.14–4.25) | .31 (.16–.61)* | ||
| Telephone screening | Passed screen/did not pass screen, n | 56/17 | 134/70 | |
| Income | <$27,431 | 1.00 | 1.00 | |
| ≥$27,431 | 1.6 (.53–4.80) | 1.02 (.57–1.8) | ||
| Education | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | 1.25 (.37–4.18) | .94 (.53–1.67) | ||
| SES | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | 2.81 (.92–8.58) | .88 (.49–1.57) | ||
| Consent | Consented/did not consent, n | 27/29 | 83/51 | |
| Income | <$27,431 | 1.00 | 1.00 | |
| ≥$27,431 | .66(.22–1.97) | .48 (.23–.97)* | ||
| Education | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | 1.98 (.57–6.91) | 1.33 (.66–2.69) | ||
| SES | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | 1.29 (.40–4.13) | .76 (38–1.55) | ||
| Clinical screening † | Completed screening/did not complete screening, n | 23/2 | 57/21 | |
| Income | <$27,431 | 1.00 | 1.00 | |
| $27,431 | 1.56 (.09–28.15) | 1.26 (.44–3.6) | ||
| Education | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | .63 (.23–1.73) | .63 (.23–1.73) | ||
| SES | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | - | 1.18(.42–3.30) | ||
| Passed screen/did not Pass screen, n | 20/3 | 51/6 | ||
| Income | <$27,431 | 1.00 | 1.00 | |
| ≥$27,431 | - | .10 (.01–.92)* | ||
| Education | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | 2.00 (.14–27.99) | 1.78 (30–10.59) | ||
| SES | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | 1.17 (.09–15.46) | .70 (.13–3.8) | ||
| Overnight † | Completed overnight/did not complete overnig, n | 11/7 | 39/10 | |
| Income | <$27,431 | 1.00 | 1.00 | |
| ≥$27,431 | .20 (.02–2.27) | 1.17 (.26–5.27) | ||
| Education | <9.7 | 1.00 | 1.00 | |
| ≥9.7 | 1.8 (.19–16.98) | 2.46 (.55–10.91) | ||
| SES | Low (1) | 1.00 | 1.00 | |
| Higher than category 1 | 2.00 (.27–14.78) | 3.43 (.64–18.26) | ||
P<.05
Numbers exclude those who are still “in process” of transferring to the following step, those with no available address information and tract data, or who live outside the Los Angeles County perimeter.
Income (average median household income, in US dollars, in geographic subarea) analyzed using the study population median ($27,431).
Education (average completed years for those aged 25+ in geographic subarea) categorized based on the study population median (9.7 years).
Social economic status (1=Lowest, 2, 3, 4, Highest=5) analyzed as the lowest SES category (1) versus the higher SES categories (2,3,4,5).
Discussion
From June 2006 to August 2008, the Transitions Study staff was able to recruit and retain 51 Latinas and African American girls (8%) of the 618 individuals who initially showed interest in participating.
By examining the demographics of at-risk and high-risk underserved communities, researchers could effectively increase awareness of the potential benefits that research could contribute to communities. Doing so may encourage study participation from individuals of the target populations. The African Americans in the Transitions Study came from higher income locations than the Latino families, opposite to what is seen in the Los Angeles County population, according to Los Angeles County population data retrieved from the US Census American Factfinder.13 There is a concern that African American families living in low-income areas are less likely to participate in research than those living in areas with higher income. Shavers and colleagues found that African Americans with at least a high school education were more willing to participate in medical research than African Americans who did not finish high school.15 It is possible that families with higher levels of education and income are more familiar with research, and may be more inclined to overcome the distrust in the research system. While there are certainly financial implications, it is the perception of the Transitions research team that further involvement with community advisors in low-income communities may help encourage study participation of individuals. These advisors who understand and communicate well with their communities would help participation rates by eliminating trust-associated barriers.2,16
In contrast with recruitment efforts in the African American community, it proved more difficult to recruit Latinas from areas with higher socioeconomic characteristics than it was to recruit Latinas from areas with lower socioeconomic characteristics. Bilingual recruiters were successful in collecting contact information from Latino families with different backgrounds. However, contacting and obtaining consent from Latinos in more affluent areas proved more difficult than with African Americans. Since higher income status may also indicate better access to health care, the annual free complete physical examinations offered by the Transitions Study for their daughters may not have presented a particularly attractive incentive for this group. Religious and cultural factors may also discourage parents from having their daughter participate in a study concerning physical maturation involving intense physical examinations.
Loss of interest in between study steps may be indicative of the need to tailor recruitment strategies based on the characteristics of the study population as the study progresses. The results suggest that it may be more effective to implement certain strategies to target individuals of particular characteristics who are more likely to lose interest at specific times during the study.
Single parent homes are examples of how demographic differences within these populations may affect study recruitment and retention rates during the course of the study. Of the families who completed the overnight stay, 45% of African Americans were from single-parent homes, as opposed to 6% of Latino families. Single-parent status might differentially influence recruitment and retention of participants; they may not be as willing to participate in certain steps of the study due to the different burdens they may experience as single parents. Despite the intense nature of the Transitions Study, single-parent African American households were still willing to continue participating in the study. Further qualitative research to understand the motivation to participate in demanding research protocols by diverse populations of different circumstances is warranted. This will allow for development and adaptation of recruitment and retention strategies specifically tailored for different types of families and communities.
Several challenges faced by the Transitions Study team may be attributed to the study’s research questions and design. This is an intense metabolic study that includes discussion of sensitive topics such as body weight and involves an annual overnight hospital visit. These requirements may not appeal to families who might be hesitant about allowing their young daughters to get their blood drawn and have physical examinations. Having to stay at a clinic overnight and getting blood drawn resulted in many girls dropping out of the study, usually a decision supported by parents. Ethnic groups from varying socioeconomic backgrounds might respond to these sensitive issues in different manners. Although recruitment and retention efforts were built on formative research in metabolically intense studies among minority youth,17–19 the literature is limited. These findings show that formative research prior to recruitment efforts should be undertaken for each sensitive study anew.
This study has some limitations. First, the homogeneity of the sample may prevent generalizing the findings to other children who belong to different sex, age, or ethnic groups. Second, socioeconomic data was obtained from only 73% of the African American and 68% of Latina participants originally interested in the study. Therefore, the analyses of SES may not be representative of the entire interested population. Third, the disproportionate numbers of Latinas as opposed to African Americans might affect group comparison. Fourth, changes in the data collection process may have improved the team’s ability to reassess recruitment strategies, such as collecting more in-depth data through recruitment sheets. Formal qualitative evaluation conducted during the recruitment process rather than the informal ongoing fact-finding conducted by the research team, could have provided more systematic guidance to improve recruitment and retention. This would allow better assessment and understanding of the reasons leading to failure of progression to the next study step among study individuals. Furthermore, increased efforts to make sure forms were completed at the time of recruitment would have been beneficial, so that useful data would not have to be disregarded during analyses due to incompleteness of the data provided.
In summary, these findings suggest that just-in-time analyses of population characteristics (ongoing immediate analyses of group characteristics so that disparities in recruited groups can be identified as recruitment progresses) could be used as a tactic to adjust strategies. Close supervision of the study progress is necessary to identify new challenges that may interfere with progression at the various study steps. Consideration of the heterogeneity of minority groups during the recruitment process is also crucial to develop and apply these new strategies in a timely fashion. These strategies would further help with retention rates to create generalizable results used to address the broad health disparities experienced among minority populations.
Acknowledgments
This work was supported by the National Institutes of Cancer (NCI), NCI Centers for Transdisciplinary Research on Energetics and Cancer (TREC, U54 CA 116848).
References
- 1.Brown BA, Long HL, Gould H, Weitz T, Milliken N. A conceptual model for the recruitment of diverse women into research studies. J Womens Health Gend Based Med. 2000;9(6):625–632. [DOI] [PubMed] [Google Scholar]
- 2.Yancey AK, Ortega AN, Kumanyika SK. Effective recruitment and retention of minority research participants. Annu Rev Public Health. 2006;27:1–28. [DOI] [PubMed] [Google Scholar]
- 3.Staffileno BA, Coke LA. Recruiting and retaining young, sedentary, hypertension-prone African American women in a physical activity intervention study. J Cardiovasc Nurs. 2006;21(3):208–216. [DOI] [PubMed] [Google Scholar]
- 4.Keyzer JF, Melnikow J, Kuppermann M, et al. Recruitment strategies for minority participation: challenges and cost lessons from the POWER interview. Ethn Dis. 2005;15(3): 395–406. [PubMed] [Google Scholar]
- 5.Story M, Sherwood NE, Obarzanek E, et al. Recruitment of African American pre-adolescent girls into an obesity prevention trial: the GEMS pilot studies. Ethn Dis. 2003;13(1 Suppl 1):S78–87. [PubMed] [Google Scholar]
- 6.Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA. 2010;303(3):242–249. [DOI] [PubMed] [Google Scholar]
- 7.Villarruel AM, Jemmott LS, Jemmott JB, Eakin BL. Recruitment and retention of Latino adolescents to a research study: lessons learned from a randomized clinical trial. J Spec Pediatr Nurs. 2006;11(4):244–250. [DOI] [PubMed] [Google Scholar]
- 8.Eakin EG, Bull SS, Riley K, Reeves MM, Gutierrez S, McLaughlin P. Recruitment and retention of Latinos in a primary care-based physical activity and diet trial: The Resources for Health study. Health Educ Res. 2007; 22(3):361–371. [DOI] [PubMed] [Google Scholar]
- 9.Sexton K, Adgate JL, Church TR, et al. Recruitment, retention, and compliance results from a probability study of children’s environmental health in economically disadvantaged neighborhoods. Environ Health Perspect. 2003;111(5):731–736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Byrd-Williams C, Kelly LA, Davis JN, Spruijt-Metz D, Goran MI. Influence of gender, BMI and Hispanic ethnicity on physical activity in children. Int J Pediatr Obes. 2007;2(3): 159–166. [DOI] [PubMed] [Google Scholar]
- 11.Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child. 1976;51(3):170–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000. CDC Growth Charts for the United States: methods and development. Vital Health Stat 11, 2002;(246):1–190. [PubMed] [Google Scholar]
- 13.U.S. Census Bureau, American FactFinder: Advanced Geography Search, Census 2000. 2000. Available at: http://factfinder.census.gov/home/saff/main.html?_lang=en. Last accessed on December 15, 2010. [Google Scholar]
- 14.Liu L, Cozen W, Bernstein L, Ross RK, Deapen D. Changing relationship between socioeconomic status and prostate cancer incidence. Journal of the National Cancer Institute. 2001;93(9):705–709. [DOI] [PubMed] [Google Scholar]
- 15.Shavers VL, Lynch CF, Burmeister LF. Racial differences in factors that influence the willingness to participate in medical research studies. Ann Epidemiol. 2002;12(4):248–256. [DOI] [PubMed] [Google Scholar]
- 16.Dancy BL, Wilbur J, Talashek M, Bonner G, Barnes-Boyd C. Community-based research: barriers to recruitment of African Americans. Nurs Outlook. 2004;52(5):234–240. [DOI] [PubMed] [Google Scholar]
- 17.Baranowski T, Cooper DM, Harrell J, et al. Presence of diabetes risk factors in a large U.S. eighth-grade cohort. Diabetes Care. 2006; 29(2):212–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Davis JN, Tung A, Chak SS, et al. Aerobic and strength training reduces adiposity in overweight Latina adolescents. Med. Sci. Sports Exerc 2009;41(7):1494–1503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Spruijt-Metz D, Li C, Cohen E, Birch L, Goran M. Longitudinal influence of mother’s child-feeding practices on adiposity in children. J. Pediatr 2006;148(3):314–320. [DOI] [PubMed] [Google Scholar]