

Summary
Guidelines for the management of hip fractures recommend timely identification, analgesia and optimisation, in order to facilitate prompt surgical repair. In achieving these aims, multidisciplinary care is essential. In this case series, we present five patients who received bedside pericapsular nerve group (PENG) blocks by emergency physicians in collaboration with the anaesthesia team for pain management following hip fracture. The PENG block is a novel motor‐ and opioid‐sparing technique, which offers long‐lasting analgesia and requires less volume than other blocks. In all of the cases in this series, the blocks were performed successfully in a short period of time, without complication. All patients reported a clinically important reduction in pain scores. Patients with hip fracture are often medically complex, and while early surgery is not always possible, pain management should be addressed from an early point in their hospital admission. Multidisciplinary input into peri‐operative pathways can enhance the provision of analgesia in the emergency department, by allowing anaesthetists and emergency physicians to work together for the benefit of these often‐frail patients.
Keywords: analgesia, hip fracture, nerve block, pain management
Introduction
The Association of Anaesthetists’ Guideline for the Management of Hip Fractures 2020 states that anaesthetists should develop formal institutional hip fracture care pathways regarding preparation for theatre and pain management [1]. For this purpose, multidisciplinary care must be provided from the emergency department setting through to rehabilitation. Currently, some patients face delays before their surgery as a consequence of medical comorbidity, operating theatre capacity or pending investigations. Guidelines recommend minimising these delays, as delayed management is associated with poor outcomes such as increased mortality, length of stay and decreased functionality [1, 2]. Nevertheless, high‐quality analgesia must be provided for patients who are awaiting fracture fixation.
Regional blocks are advocated as an important component of the analgesia approach for patients with hip fracture and have been shown to be both safe and effective, leading to decreased opioid consumption [1, 3]. The pericapsular nerve group (PENG) block is a recently described technique to block the innervation of the anterior hip capsule [4]. Because it does not block cutaneous nerves, it is most suitable for the management of pain arising from the fracture itself, rather than only postoperative analgesia.
Anticipating more significant delays to fracture fixation at the start of the COVID‐19 pandemic, we implemented the use of PENG blocks to provide analgesia for patients with hip fracture presenting to the emergency department of our institution, in collaboration with emergency physicians. This approach now forms a routine part of our hip fracture pathway. In this report, we share our experience of the first five cases where PENG blocks were provided in the emergency department during the pandemic. This service was commenced only after the emergency medicine physicians had received appropriate training, comprising theoretical lectures and supervised PENG block performance.
Report
Following written, informed consent, PENG block was performed on five patients with proximal femoral fracture. They were positioned supine, and aseptic technique was used.
Ultrasound guidance was used, as described by Girón et al. [4]. A curvilinear low‐frequency 6–2 MHz probe (Sparq, Philips, Amsterdam, The Netherlands) was placed over the anterior inferior iliac spine and aligned with the pubic ramus (Fig. 1a) allowing identification of the iliopubic eminence, femoral artery and illiopsoas muscle. A 10‐cm 22G spinal needle was advanced in plane in a lateral to medial direction to place the tip in the musculofascial plane between the psoas tendon anteriorly and the pubic ramus posteriorly (Fig. 1b). After negative aspiration, a total volume of 20 ml (9 ml lidocaine 2%, 10 ml bupivacaine 0.5% and 4 mg preservative‐free dexamethasone) was injected in 5‐ml increments while observing for an adequate fluid spread. All blocks were performed by experienced emergency physicians. Paracetamol was given to all patients as part of multimodal analgesic management.
Figure 1.
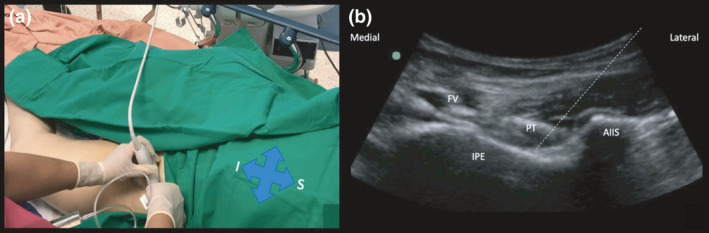
(a) Orientation of the ultrasound probe in the hip. S, superior; I, inferior. (b) Sonoanatomy. The dotted line depicts needle trajectory. FV; femoral vessels; IPE, iliopubic eminence; PT, psoas tendon; AIIS, anterior inferior iliac spine.
We recorded block performance time, from probe‐skin contact to the end of injection, and onset time, defined as the time required to achieve a 50% decrease in rest pain. The numeric rating scale was used to assess both rest and dynamic pain scores. The time between the block and the first dose of opioid, motor block (as present or absent compared with baseline assessment) and complications were also recorded (Table 1).
Twenty minutes after block placement, all patients reported reduced rest and dynamic pain scores. The block performance time was no more than 4 min (plus approximately 2 min of bedside setup time). No opioid therapy was required by any of the patients. No motor block was clinically evident during the patients’ stays in the emergency department (Table 1). All patients subsequently went on to have surgical fracture fixation.
Table 1.
Summary of patient baseline characteristics, analgesia and procedural characteristics.
| Patient number | Age | Sex | Comorbidities |
Fracture type |
Numeric rating scale pain scores (out of 10); Rest / Dynamic |
Block Performance time; min | Block onset time; min | Muscle weakness | Time to first opioid; h | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 30 min | 6 h | 12 h | |||||||||
| 1 | 88 | M | Hypertension | Intertrochanteric | 7/10 | 0/0 | 0/5 | 3/5 | 3 | 20 | – | – |
| 2 | 79 | M | Hypertension diabetes mellitus | Subtrochanteric | 10/10 | 2/2 | 2/2 | 1/1 | 2 | 15 | – | – |
| 3 | 89 | M | None | Intertrochanteric | 10/10 | 0/0 | 0/1 | 0/2 | 4 | 20 | – | – |
| 4 | 80 | F | Asthma | Intertrochanteric | 7/10 | 0/2 | 1/3 | 1/4 | 1 | 20 | – | – |
| 5 | 73 | F |
Hypertension Diabetes mellitus |
Intertrochanteric | 9/10 | 1/2 | 0/0 | 1/2 | 4 | 15 | – | – |
−, absent; +, present; F, female; h, hours; M, male; min, minutes.
Discussion
Pericapsular nerve group blocks have demonstrated effectiveness in elderly patients with hip fractures [4], and are increasingly being used in the emergency department [5, 6]. The PENG block has some advantages when compared with other regional blocks, including a lack of motor block, long‐lasting analgesia and lower volume is required than for other blocks such as the fascia iliaca compartment block. The PENG block targets only the articular sensory branches from the anterior hip capsule, thereby avoiding quadriceps muscle weakness [6]. We consider that block specificity (when compared to femoral nerve or fascia iliaca compartment blocks) could be another advantage; it could be used as a diagnostic block for only articular hip pain. Finally, it could be safer than other blocks in the emergency setting because the needle tip must be resting on the bone (iliopubic eminence), not within soft tissues, a more definitive endpoint.
As this is a fragile patient population, we mixed lidocaine with levobupivacaine and dexamethasone to reduce the amount of levobupivacaine required, in order to minimise the risk of cardiac toxicity. Lidocaine is also useful to minimise onset time, and dexamethasone may prolong analgesia duration [7], thereby avoiding the need for catheter infusions.
Prior reports indicate that the PENG block has utility for several indications, including hip fracture and, with the use of alcohol and phenol, for neurolysis for chronic pain [4, 8, 9]. Although we found no other studies reporting the bedside use of PENG block by emergency physicians, a recent case series of three patients supports our findings that the PENG block can be useful in the emergency department [10].
Our case series highlights several learning points. Firstly, although many circumstances could delay definitive surgical treatment, pain management can be adequately addressed from the beginning. Secondly, multidisciplinary collaboration can produce a perioperative pathway to enhance the management of this frail patient group. Thirdly, single‐shot PENG blocks by emergency physicians resulted in opioid‐sparing pre‐operative analgesia (most studies only report opioid therapy in the postoperative phase); this approach could lead to better patient outcomes, for example, by minimising the risk of opioid‐associated delirium.
Many anaesthesia departments do not have the capacity to provide regional analgesia outside the operating room. Delivering the benefits of regional techniques to patients with hip fracture necessitates early implementation in the emergency department. Collaboration with emergency physicians is therefore a promising strategy to improve the patient experience, improve pain management, and improve outcomes.
Although we report only five cases in this series, our emergency department has now performed PENG blocks for more than 300 patients with hip fracture, obtaining satisfactory results. This experience suggests that this block has promising efficacy and usefulness as motor and opioid‐sparing adjunct for the management of hip pain in the emergency department, without interfering with the anaesthetic management. Furthermore, it allows for more comfortable positioning in the operating room for spinal anaesthesia.
This case series indicates how anaesthetists and emergency physicians can work together to benefit patients; expanding the use of regional anaesthesia techniques beyond the operative setting. However, there remains a lack of literature about the use of the PENG block by emergency physicians, and prospective randomised studies are needed to understand the expanding role of PENG block in hip fracture management.
Acknowledgements
Published with the written consent of all patients. No external funding or competing interests declared.
Contributor Information
A. Rocha‐Romero, Email: rocharomeroandres@gmail.com, @AndresR00916584.
P. W. H. Peng, @DrPhilipPeng.
References
- 1. Griffiths R, Babu S, Dixon P, et al. Guideline for the management of hip fractures 2020: Guideline by the Association of Anaesthetists. Anaesthesia 2021; 76: 225–37. [DOI] [PubMed] [Google Scholar]
- 2. Mukherjee K, Brooks SE, Barraco RD, et al. Elderly adults with isolated hip fractures‐orthogeriatric care versus standard care: a practice management guideline from the Eastern Association for the Surgery of Trauma. Journal of Trauma and Acute Care Surgery 2020; 88: 266–78. [DOI] [PubMed] [Google Scholar]
- 3. Hamilton GM, Lalu MM, Ramlogan R, et al. A population‐based comparative effectiveness study of peripheral nerve blocks for hip fracture surgery. Anesthesiology 2019; 131: 1025–35. [DOI] [PubMed] [Google Scholar]
- 4. Girón‐Arango L, Peng PWH, Chin KJ, Brull R, Perlas A. Pericapsular nerve group (PENG) block for hip fracture. Regional Anaesthesia and Pain Medicine 2018; 43: 859–63. [DOI] [PubMed] [Google Scholar]
- 5. Riddell M, Ospina M, Holroyd‐Leduc JM. Use of femoral nerve blocks to manage hip fracture pain among older adults in the emergency department: a systematic review. Canadian Journal of Emergency Medicine 2016; 18: 245–52. [DOI] [PubMed] [Google Scholar]
- 6. Ridderikhof ML, De Kruif E, Stevens MF, et al. Ultrasound guided supra‐inguinal fascia iliaca compartment blocks in hip fracture patients: an alternative technique. American Journal of Emergency Medicine 2020; 38: 231–6. [DOI] [PubMed] [Google Scholar]
- 7. Heesen M, Klimek M, Imberger G, Hoeks SE, Rossaint R, Straube S. Co‐administration of dexamethasone with peripheral nerve block: intravenous vs perineural application: systematic review, meta‐analysis, meta‐regression and trial‐sequential analysis. British Journal of Anaesthesia 2018; 120: 212–27. [DOI] [PubMed] [Google Scholar]
- 8. Kwun‐Tung Ng T, Chan W‐S, Peng PWH, Sham P, Sasaki S, Tsui H‐F. Chemical hip denervation for inoperable hip fracture. Anesthesia and Analgesia 2019; 130: 498–504. [DOI] [PubMed] [Google Scholar]
- 9. Rocha‐Romero A, Carvajal Valdy G, Lemus AJ. Ultrasound‐guided pericapsular nerve group (PENG) hip joint phenol neurolysis for palliative pain. Canadian Journal of Anesthesia 2019; 66: 1270–1. [DOI] [PubMed] [Google Scholar]
- 10. Luftig J, Dreyfuss A, Mantuani D, Howell K, White A, Nagdev A. A new frontier in pelvic fracture pain control in the ED: successful use of the pericapsular nerve group (PENG) block. American Journal of Emergency Medicine 2020; 38: E5–9. [DOI] [PubMed] [Google Scholar]