

Abstract
Objective: The effects of hemsball game skills development program on the motor proficiency level of children in the 12–16 age group with mild and moderate intellectual disabilities (ID) have been examined in this study.
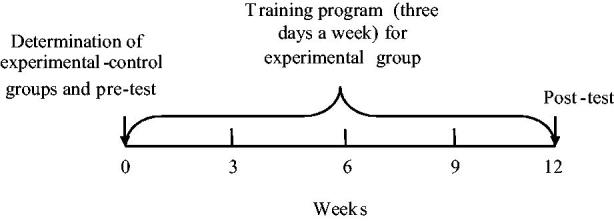
Method: A total of 50 (25 experimental group +25 control group) students, 23 of which had mild intellectual disabilities (ID) and 27 with moderate ID studying in special education classes in the schools in Afyonkarahisar province in Turkey participated in the study. While no training was given to the control group, the students in the experimental group were subjected to 60 min of applications involving a basic hemsball training program per day for 3 days per week throughout 12 weeks. Bruininks–Oseretsky Test of Motor Proficiency (BOT-2) sub-tests (balance, bilateral coordination, upper-limb coordination) were applied twice, once before starting the program (pre-test) and once after the program was completed (post-test). The obtained data were tested with paired-samples t-test and independent-samples t-test.
Result and Conclusion: As a result of the study, it was noted that the application of the hemsball game skill development program had incurred significant differences between the experimental and control group according to the post-test as well as the pre-test and post-test for the experimental group which were positive. However, it was determined that the application was more effective in students with moderate level ID than students with mild ID.
Keywords: Hemsball, intellectual disabilities (ID), motor proficiency, BOT-2
Introduction
Children with intellectual disabilities (ID) are characterized by impaired mental functioning and adaptive behavior (Schalock et al. 2010). It has been found that children with ID often manifest impaired motor function in terms of quantity and quality in performance and participation, such as motor skills acquisition, fine motor control, and strategic motor problems in the community, at school or at home (Hoover and Wade 1985; Elliott and Bunn 2004). The inadequate opportunities for people with intellectual disability to participate in training and games, along with weaknesses in motor development, such as weakness in visual and motor coordination, limitation in fine movements, challenges and constraints in learning new forms of activity have a negative impact on physical fitness and motor development (Clarke and Clarke 1978; Ronald 1991). However, as the level of intelligence decreases and kinetic and physical problems increase, children with mild intellectual disabilities have lower locomotors skills than children with borderline intellectual disabilities. Athletes with less severe intellectual disabilities achieve higher performance scores in the motor coordination test (Hartman et al. 2010; Guideti et al. 2010).
Salvador-Carulla et al. (2015) reported that training programs for ID in health sciences were inadequate and that focus on ID should be increased. The importance of vocational education as well as movement training is well known. Participating in physical activities and performing motor skills such as walking, running, jumping, hopping, bouncing, catching and throwing require physical and motor adequacy. These skills are often thought of as building blocks for the development of more complex motor and sport-specific skills and contribute positively to daily living activities (Watkinson et al. 2001; Wall 2004; Stodden et al. 2008). Movement training helps the physical, psychomotor, cognitive, emotional and social development of children and contributes to their strength and in becoming self-sufficient individuals. Chen et al. (2016) emphasized the psychological effect of walking as an exercise for persons with ID. It is commonly stated that those with intellectual disabilities who are inactive are less inclined to physical skills such as endurance, balance and strength than their peers in the general population. While balance, locomotors and manipulative skills that should develop with age are not at the necessary level in children with ID, commonly encountered mobility limitation manifest the prevalence of balance and walking problems (Hall and Thomas 2008; Cleaver et al. 2009). It has been shown that the balance performance of people with ID can be significantly improved with different activity programs (Wang and Ju 2002; Tsimaras and Fotiadou 2004; Fotiadou et al. 2009; Giagazoglou et al. 2012). However, it is known that educational games and movement training specific to different sports branches are important in the development of balance and coordination abilities. One of these sports branches is hemsball, which is quite new with movements required by the game (such as reaching, squatting, catching and throwing) and a basic training program that can be effective in developing individual motor skills.
Hemsball (Hand–Energy–Motion–Stability–Ball) was designed by Murat Altinay in the year 2011 in Turkey after which the necessary research and development work was carried out to give the game its final form. The Republic of Turkey Ministry of Youth and Sports, Sports for Everyone Federation also decided to provide its support to hemsball with its letter no. THISF/31 dated 20 January 2012. This new branch of sport was approved as “The Sports Branch Hemsball” by the Republic of Turkey Ministry of Youth and Sports General Directorate in their letter no. 20262901-020/4065 dated 11 July 2013.
Hemsball is a fun and entertaining new sport that can be played by people of all ages. It can be played easily in both outdoor and indoor areas. While playing hemsball it is important to have good hand-eye coordination, a high level of focus and concentration in order to be able to catch the ball and serve it. The name of the sport, as shown below, was derived from the first letters of the combination of the performance that is portrayed during the game.
Hemsball has been mentioned in some studies in literature (Todorova et al. 2014; Tuglu 2016). It is evident that sufficient knowledge about the effect of hemsball on intellectual disabilities is not available. Therefore, the effects of hemsball game skills development program on the motor competence level of children in the 12–16 age group with mild and moderate ID have been examined in this study. Furthermore, whether or not the degree of disability makes a difference in motor development levels has also been examined.
Method
The population of the study was approved with the decision of the board of ethics of clinical research of Afyon Kocatepe University School of Medicine. The population consists of students in the 12–16 age bracket with ID attending special education classes in five schools affiliated with the Ministry of National Education in Afyonkarahisar province in Turkey. This study was limited because it includes only five schools in a province in Turkey and because the experimental group consisted of 25 people with intellectual disabilities in the 12–16 age group. On the other hand, the examination of the effect of the basic training program was limited to the students’ balance, bilateral coordination and upper-limb coordination which is another limitation of study.
The sample group consisted of a total of 50 students of which 23 had mild and 27 had moderate ID who were approved for participation in the study. After obtaining the necessary permission from the Directorate of National Education in Afyon Province for the study, informed consent forms were signed by the guardians of the students who had obtained medical reports confirming that there was no objection to their participation in sports. Subsequently, a meeting was held with the parents of 50 students with intellectual disabilities to inform them about the details of the study.
Important criteria in the selection of the students was to have a certain level of basic motor skills, have only the one disability and attend school in terms of the systematic of the application. The students were divided into two homogenous groups, one of which consisted of 25 students in the experimental group and 25 students in the control group taking the height, weight and type of disability of the students into consideration. Simple random method was used to separate the students.
While no training was given to the control group, the students in the experimental group were subjected to a total of 36 hemsball basic training programs comprised of 60 min of applications involving basic hemsball training programs per day for 3 days per week throughout 12 weeks. The pre- and post-tests were carried out completely objectively by the researchers. The flow diagram for the application process of the research is shown in Figure 1.
Figure 1.
The application process of the study
Materials used for the hemsball game were the hemsball ball, hoop, target board, foot pad and field strips. The objective of the game is to throw the hemsball into the hemsball hoop that is on the hemsball target board on the floor without hitting the hoop and make it go over to the opponent’s side and into the opponent’s area and to prevent the opponents from achieving the same goal. While sending the ball into the game and opponent’s area they may catch the ball in any way including on the plates where they are stepping. The ball is put into play with a draw in which the loser serves. The player, who serves, throws the ball at the hoop to send it to the rival side. The counting continues until a ball touches inside the hoop, goes out or a player makes a mistake. The player who wins a point gets to serve. The game zone for junior players is 3 × 1.23 cm. For adults, it is comprised of a 4 × 1.55 cm zone and for double players it is 4.15 × 2.10 cm of rectangular, flat, smooth and hard ground. The area should be set up so that there is a 2 m distance from any direction to the hemsball area. The hemsball junior-adult-doubles playing pitches and hemsball ball are shown in Figure 2.
Figure 2.

International hemsball pitches and ball
The sizes of the balls vary according to the age group and categories. A standard hemsball ball is a 55-mm diameter rubber filled ball weighing 95 g +2, and the characteristic feature of hemsball is that it is raised outwards with an embossed letter H on two equal sides. The official color for adults is orange. The circumference of the ball is 5.5 cm. The beginners ball size for juniors is 45–55 mm in diameter, sponge-filled, elastic-filled, rubber filled weighing 52 g +2 to a maximum of 95 g +2. The characteristic feature of hemsball is that it is raised outwards. No color difference is sought in other categories.
During pitching, the whole body turns in the direction of pitching. The eyes are focused on the target point. The hand gripping the ball to pitch moves forward while the foot on the same side is lifted off the ground. The shoulders are brought forward, as the ball leaves the hand, the arm continues to move in the direction of the ball (Figure 3). The following movements are considered important for the development of balance, bilateral and upper-limb coordination: pitching the hemsball in an upright position or crouching without going outside the foot plate (42 × 30 cm), throwing the ball while standing on one foot, reaching out over the foot plate while rallying to catch the ball from all directions, catching the ball thrown by the opponent while standing on one foot and throwing the ball into the hoop in the target from the other side without contacting the hoop.
Figure 3.

Hemsball game and a shooting technique
The hemsball basic training program applied to the experimental group was prepared to address an average condition without regard to the degree or severity of the disability and is presented below (Table 1).
Table 1.
Hemsball basic training program
| Warm-up 10 min. | Mid-paced walk) 7 min Stretching 3 min | |
|---|---|---|
| Main period 45 min | Basic exercise examples | Exc.1: Roll the ball from one hand to the other through the palm of the hand. Exc.2: Throw the ball from one hand to the other with palms facing each other and held at a hand’s distance. Exc.3: Release the ball from the fingertips while pushing the arm upwards. Exc.4: Release the ball to the ground while standing, catch it with one or both hands. Exc.5: Catch the ball which has been released to the ground while standing with one or both hands while hunkering. Exc.6: Dribble the ball during every second step while walking. |
| Examples of individual wall exercises | Exc.1: Catch a ball that is thrown against a wall and bounces back while in a sitting position facing the wall with one or both hands (1-2-3 m). Exc.2: Hold the ball while standing up facing the wall and catching with the same or a different hand. Exc.3: Catch a ball that is thrown onto the ground and bounces back from the wall with one or both hands while standing and facing the wall. Exc.4: Catch a ball with one or both hands that is thrown into a hoop left in front of a wall and rebounds from the wall. | |
| Pairwise-double exercises examples | Exc.1: Two students with ID standing in alignment facing the wall catch a ball thrown onto the ground and rebounding from the wall with both hands. Exc.2: An ID student catches a ball that is thrown directly at the wall by the trainer and falls to the ground from the wall. Exc.3: The trainer standing behind the ID student facing the wall throws the ball on the ground and the ball rebounding from the wall is caught by the ID student. Exc.4: An ID student standing on a foot plate catches a ball that is thrown by the trainer at different speeds. Exc.5: Two ID students face each other on the foot plates in the game area and throw a ball at the target board with one hand and catch the ball with two hands. Exc.6: The trainer and student practice throwing on the game court on one foot and on two feet. | |
| Cool down 5 min | Low-paced walk 2 min Stretching 3 min | |
The motor proficiency levels of the students have been determined with the Bruininks-Oseretsky Motor Proficiency Test BOT-2 (Bruininks and Bruininks 2005). The validity and reliability study of BOT-2 in Turkey has been carried out by Mülazımoglu Balli (2006). BOT-2 was administered twice, once before the start of the basic training program (pre-test) and after the program was finished (post-test). BOT-2 is comprised of three sub-tests and 23 items, nine of which involve balance (standing on tiptoe and on the heel on a balance bar, walking forward on a line, standing on a line with one foot eyes open, standing on a line with feet at a forward angle and eyes closed, walking forward on a line on tiptoe and heel, standing with eyes closed on a line with one foot, standing on a balance bar with one foot and eyes open, standing on a balance bar heel to toe, standing on a balance bar on one foot with eyes closed), bilateral coordination, seven items involve (jumping simultaneously in place in the same and opposite directions and tapping contralateral feet and fingers simultaneously, touching the nose eyes closed with the index fingers, jumping jacks, simultaneous jumping in place on the same side, simultaneous jumping in place on opposite sides, twisting thumbs and index fingers – crossing them – simultaneous tapping of the foot and fingers on the same side, simultaneous tapping of the foot and fingers on the opposite sides) and upper-limb coordination while seven items involve (catching a thrown ball, dribbling, throwing the ball at a target, letting go and catching the ball with both hands, catching a thrown ball with both hands, letting go and catching the ball with one hand, catching a thrown ball with one hand, dribbling the ball with one hand, dribbling the ball by changing hands, pitching the ball at the target). The test takes about 30–45 min and the maximum achievable score is 100.
The data obtained in the study were analyzed with the SPSS 18.0 for Windows statistical package program. The test results of the data (Shapiro–Wilk test, Kolmogorov–Simirnov test) were commensurate with normal distribution. In this context, paired-samples t-test was used for intra-group comparisons (for pre-test/post-test) and independent-samples t-test was used for inter-group comparisons (for control and experimental groups). The repeated measures two way ANOVA was used to test the group–time interaction.
Results
The mean age of the participants was ± SD =13.85 ± 0.93, their mean height ± SD =1.51 ± 10.58 while their average weight was ± SD =46.48 ± 15.53. The results of the two-factor variance analysis for repeated measures of the effect of hemsball basic training skills on the motor proficiency level of children with ID are presented in Table 2. While no significant difference was found between the control and the experimental groups in terms of (BOT-2) (balance, bilateral coordination and upper-limb coordination) (p > 0.05) according to the pre-tests, significant differences were determined between the groups according to the post-tests (p < 0.05). However, while there was no significant difference between the pre-test and post-test in the control group (p > 0.05), there were significant differences between the pre-test and post-test of the experimental group (p < 0.05). Group-time interaction was not significant in two-way ANOVA (p > 0.05). An examination of the balance post-test averages indicated that the experimental group average (=20.72) was higher than the average of the control group (=27.16). Likewise, the post-test average for the experimental group (=18.84) for upper-limb coordination (=30.92) was much higher than in the control group (=10.76); (=16.12). When the change rates of the control and experimental groups in Table 2 are considered, an increase of 31.1, 71.1, and 91.8% have been obtained for the post-test in terms of balance, bilateral coordination and upper-limb coordination, respectively.
Table 2.
Findings of the effect of hemsball basic training on motor proficiency level
| Tests | Measurements | Control group | Experimental Group | p | Change |
|---|---|---|---|---|---|
| ±SD | ±SD | ||||
| Balance | Pre-test | 19.20 ± 11.49 | 17.20 ± 9.41 | 0.504 | – |
| Post-test | 20.72 ± 11.23 | 27.16 ± 6.70 | <0.05 | 31.1% | |
| p | 0.068 | <0.01 | |||
| Bilateral coordination | Pre-test | 9.56 ± 6.53 | 10.32 ± 6.18 | 0.675 | – |
| Post-test | 10.76 ± 7.26 | 18.84 ± 5.11 | <0.01 | 75.1% | |
| p | 0.092 | <0.01 | |||
| Upper-limb coordination | Pre-test | 15.52 ± 10.95 | 19.08 ± 8.98 | 0.215 | – |
| Post-test | 16.12 ± 10.43 | 30.92 ± 6.84 | <0.01 | 91.8% | |
| p | 0.551 | <0.01 |
The results of variance analysis for comparison of pre and post motor proficiency scores of the control and experimental groups in terms of intellectual disability level are given in Table 3. According to the balance post-test averages, there was no significant difference between the groups with mild ID (p > 0.05); however, there was a significant difference between the groups with moderate ID (p < 0.05). When the bilateral coordination and upper-limb coordination post-test results were examined, there was a significant difference between the experimental and control groups with both mild and moderate ID (p < 0.05). The balance scores of those with moderate levels of ID increased from 16.50 to 25.81 (56.4%). It was determined that the bilateral coordination of the group with a mild level of ID increased from 13.88 to 18.92 (36.3%) while the figures for the group with moderate ID increased from 9.00 to 18.72 (108.0%); for the upper-limb coordination, it was found that the values of the group with mild ID increased from 22.88 to 31.64 (38.3%) and the values of the group with a moderate level of ID increased from 12.31 to 30.00 (143.7%). These findings show that training for all motor proficiency tests is more effective in individuals with moderate intellectual disabilities.
Table 3.
Comparison of pre-test and post-test motor proficiency scores of the control and experimental groups according to the degree of intellectual disability
| Tests | Measurements | Degree of disability | Control group | Experimental group | p | Change |
|---|---|---|---|---|---|---|
| ±SD | ±SD | |||||
| Balance | Pre-test | Mild n = 23 | 24.88 ± 8.31 | 18.28 ± 10.52 | 0.127 | – |
| Moderate n = 27 | 16.00 ± 12.00 | 15.81 ± 8.07 | 0.965 | – | ||
| p | 0.062 | 0.527 | ||||
| Post-test | Mild n = 23 | 28.22 ± 4.38 | 28.21 ± 7.57 | 0.998 | – | |
| Moderate n = 27 | 16.50 ± 11.78 | 25.81 ± 5.43 | <0.05 | 56.4% | ||
| p | <0.05 | 0.386 | ||||
| Bilateral coordination | Pre-test | Mild n = 23 | 12.33 ± 5.47 | 11.35 ± 6.66 | 0.718 | – |
| Moderate n = 27 | 8.00 ± 6.72 | 9.00 ± 5.53 | 0.688 | – | ||
| p | 0.113 | 0.355 | ||||
| Post-test | Mild n = 23 | 13.88 ± 6.25 | 18.92 ± 5.29 | <0.05 | 36.3% | |
| Moderate n = 27 | 9.00 ± 7.37 | 18.72 ± 5.12 | <0.01 | 108.0% | ||
| p | 0.108 | 0.925 | ||||
| Upper-limb coordination | Pre-test | Mild n = 23 | 20.44 ± 11.78 | 18.85 ± 9.65 | 0.727 | – |
| Moderate n = 27 | 12.75 ± 9.76 | 19.36 ± 8.51 | 0.081 | – | ||
| p | 0.092 | 0.892 | ||||
| Post-test | Mild n = 23 | 22.88 ± 9.38 | 31.64 ± 5.48 | <0.05 | 38.3% | |
| Moderate n = 27 | 12.31 ± 9.17 | 30.00 ± 8.47 | <0.01 | 143.7% | ||
| p | <0.05 | 0.563 |
Discussion
The aim of this study was to examine the effect of the hemsball basic training program on the motor proficiency levels of 12–16-year-old children with mild to moderate intellectual disability levels as determined by the BOT-2. An experimental and control group comprised of 25 children in this age group were exposed to 60 min of hemsball basic training program 3 days per week for 12 weeks to total 36 h of basic hemsball training was to examine the effect of the hemsball basic training program. The idea that pitching from a high or low position while standing on the determined game area plate supported by one or both feet, catching the approaching ball without exiting a given area and throwing the ball into a hoop 135 cm from the area where the hemsball ball is could be influential in the development of balance and upper-limb coordination, hand-eye and bilateral coordination played a significant role in the execution of his study.
The exercise for students with mild and moderate intellectual disabilities in the 12–16 year age group participating as experimental and control groups was designed as a pre-test and post-test. The hemsball basic training program was adapted to the experimental group to support the development of balance, bilateral coordination and upper-limb coordination. The sample exercises started with getting used to the special embossed hemsball and finger-wrist exercises (such as throwing the ball from one hand to the other with the palms of the hands facing each other at a hand’s length and rolling the ball from the finger tips while pushing the arm upwards). The exercises included pitching the hemsball ball, which has extreme bouncing capacity, facing the wall and controlling the rebounding ball with one or both hands depending on the momentum of the ball. The exercises continued in different forms of free, on the wall, on the ground and with a partner by pitching the ball in the same direction with a partner and throwing it to each other and catching the ball from different angles and different speeds in an upright position or crouching. Fotiadou et al. (2009) carried out a study with an experimental and control group consisted of 18 adult individuals with intellectual disabilities with the application of a 12 week training program on top of routine exercises designed to develop the balance skills of the respondents while no changes were made in the usual sports program of the control group. The applied training program consisted of certain basic movements derived from rhythmic gymnastics, rhythm and dance elements and dynamic balance activities. Exercises were applied by using various musical instruments in accordance with the participant (walk in a different tempo, half turns, step change, passing the ball from one hand to the other and rotating it around the body while walking). In a study carried out by Giagazoglou et al. (2013), 18 school children from a private elementary school unit with moderate intellectual disability (ID) were selected randomly and separated into two equal groups comprised of seven boys and two girls. While the experimental group carried out trampoline exercises for 12 weeks the control group continued with their regular school program. The exercises chosen for each session were carried out by the experimental group on a trampoline. Different jump forms were created with various basic exercises using auxiliary equipment such as balls and balloons.
In a study carried out by Fotiadou et al. (2009) and Giagazoglou et al. (2013), they made modifications in their exercise content according to mentally retarded individuals and found improvement in balance skills. This aspect of the study is similar to our study. In our study, the individuals were taught basic hemsball pitching techniques and hemsball was adapted according to mental disability to enable the application of the basic movement forms (able to maintain balance on the footstand, throw the ball into the hoop of the target board and control the ball). The study was designed to address the average level of mentally retarded individuals included in the hemsball basic training program. However, the study differs from the studies of Fotiadou et al. (2009) and Giagazoglou et al. (2013) in that auxiliary materials other than hemsball game materials (hemsball, target board, hoop) were not included.
Champagne and Dugas (2010) carried out case study with two autistic children in which each hippotherapy session lasted ∼30 min and during this time the children were able to execute therapeutic activities with three different positions (facing forward, sitting sideways, facing backward) on a moving horse. Similarly to a study carried out by Champagne and Dugas (2010), they were asked to practice throwing and catching movements in different positions (sitting, squatting, standing on one leg and two legs) during the HemsBall basic training program.
Kao and Wang (2016) integrated the game concepts of throwing distance, shooting precision, rotation, and other skills in the course of the activities that include the basic movements of frisbee throwing and catching that the pre-test, post-test design used in the single group of the intellectually disabled.
As a result of the study, it was determined that the hemsball basic training program in the experimental group had a positive effect on balance, bilateral coordination and upper-limb coordination. Although there are some studies in literature regarding the hemsball game (Todorova et al., 2014; Tuglu 2016), it is noted that there are no studies on motor competence in intellectually disabilities. However, many studies have been conducted on the motor competencies of the disabled in different sports branches. In a study carried out by Rad et al. (2012), 20 randomly selected autistic children were subjected to 45 min of spark program (warm-up, basic motor performance exercises and cooling down) per day three times per week for 8 weeks. Ten subjects formed the control group and all the children were given the BOT-2 test before and after the study, and the static balance parameters in the exercise group were reported to be higher than in the control group. Arslan and Ince (2015) carried out a study (a 3-month program comprised of exercises including warming up, balance and jumping making up the main phase followed by cooling) to determine the effect on the rough motor skill levels of atypical autistic children, found that the balance I and balance II post-test results for BOT-2 were higher than the pre-test results. In a study carried out by Connolly and Michael (1986) it is emphasized that the BOT-2 sub-test results of children with ID without down syndrome are higher in running speed, balance, strength, visual motor control and all rough motor and fine motor skill scores than those of children with down's syndrome. Rad et al. (2012) and Arslan and Ince (2015) noticed an increase in balance values when exercise programs without play area limitations were examined. While the study showed differences in terms of exercise program content with our study, it proves that our study carried out in a restricted play area was also effective in terms of balance values.
In a study by Gunal (2007), it is emphasized that the Bruininks–Oseretsky Motor Competence Test (BOMYT) scores of autistic children are lower than the scores of normal children in the heel toe walking test results that evaluate the balance function in rough motor skills. In a study carried out by Yanardag (2007) with autistic children he emphasizes that exercises with autistic children improved the upper-limb coordination. Yanardag (2007) noted that the upper extremity coordination of autistic children was significantly improved by different forms of motion such as walking and light running on a treadmill, bouncing on a trampoline, riding a toy horse as well as ball-throwing exercises to a target at a distance of one meter. In our study, exercises that provide upper torso and arm movement during throwing and catching by focusing on the target were found to be similarly effective in upper extremity coordination.
It is asserted that in addition to rhythmic gymnastics (Fotiadou et al. 2009), different activity programs such as hippotherapy sessions during which a child assumes three different positions for ∼30 min of therapeutic activities on horseback (Champagne and Dugas 2010) have a positive impact on the development of balance, motor performance and coordination of the intellectually disabled.
Hall and Thomas (2008) have reported that physical capacities such as endurance, balance, and strength are generally lower in non-athletic or inactive individuals with ID compared to their peers in the general population. The widespread mobility limitation of people with ID suggests that balance and gait problems are also common (Cleaver et al. 2009). It is observed that people with ID have difficulty in motor performance activities which require the coordination of two movements such as ball throwing and catching, jumping and throwing a ball and that they experience difficulties in developing application skills (Jankowicz-Szymanska et al. 2012). Bruininks and Chavat (1990) manifest that individuals with ID show the most loss in coordination, balance, speed and manipulative skills. On the other hand, studies have shown that the balance of individuals with ID is lower than that of individuals who do not have ID (Suomi and Koceja 1994; Gomes and Barela 2007; Dellavia et al. 2009). Kao and Wang (2016) implemented a frisbee course for 6 weeks which involved the basic movements of throwing and catching a frisbee for 40 min for 4 days of the week. They have shown that students with intellectual disabilities can improve upper-limb muscle strength, stamina, coordination and skills with a frisbee course. The fact that our study included similar forms of throwing and catching movements as Kao and Wang (2016) at a closer distance to the partner have made a significant difference in terms of both bilateral and upper extremity coordination development. It has also been observed that although they have not been measured, manual grip ability has also improved in order to catch the hemsball ball which has a diameter ranging from 45 to 55 mm.
In a study carried by Magnusson et al. (2012) with six autistic children aged 9–15 years subjected to an exercise program consisting of 60 min of exercise (warming up, high intensity interval exercise, aerobic exercises, plyometrics, resistance exercises, cooling exercises and stretching) per day for 2 days per week and provided that the program was completed in 8 or 12 weeks, the recorded balance post-test mean values of the children after the exercise program were higher than the pre-test values. A study carried out by Giagazoglou et al. (2013) manifested that a 12-week trampoline exercise program is effective in improving the balance and motor skills performance of people with intellectual disabilities. Damaged body sensitivity and poor spatial orientation in individuals with ID reduce the level of static and dynamic balance and manifests strange movements and increases the risk of falling. Applications carried out with open and closed eyes on variable surfaces have been shown to improve the static balance of people with down's syndrome (Jankowicz-Szymanska et al. 2012). Exercise programs have been reported to affect not only balance and walking capacities, but also reduce the number of falls (Gillespie et al. 2009). Boswell (1993) notes that dancing has a positive influence on the balance development of those with intellectual disabilities. While Giagazoglou et al. (2013) and Jankowicz-Szymanska et al. (2012) reported that exercises performed with foot movements on different surfaces with eyes open and closed have been effective in balance development, our study indicated that catching a ball while standing on one or two feet without leaving a determined area was effective in improving balance.
Some researchers suggest that physical exercises have a positive effect on the balance levels of individuals with mild ID (Marchewka 2002; Wang and Ju 2002; Dehghani and ve Günay 2015). In another study, it was stated that children who had mild ID showed a good improvement in maintaining balance (Franciosi et al. 2010). A study of children with mild ID in terms of their balance scores shows that they are better than those with moderate levels of ID, emphasizing the need for a more elaborate physical activity program that may affect the development of physical fitness (Golubovic et al. 2012). This study revealed that the hemsball basic training program is more effective in individuals with moderate ID than in individuals with mild ID in terms of all motor proficiency tests (balance, bilateral coordination, upper-limb coordination). This result emphasizes the importance of studying the effectiveness of the hemsball basic training program. The need to prepare a safe area and take precautionary measures, which is required for many games, is practically nonexistent for hemsball. The hemsball game set can easily be set up and played by students with mild intellectual disabilities without the accompaniment of a guide and considering the problems encountered in terms of a suitable activity area, the fact that hemsball does not require a special area (it can be played outdoors as well as indoors) is a major advantage especially for schools with limited means.
Conclusion
The motor proficiency and strength measurements of people with ID can be significantly improved with various activities. Dynamic balance and coordination ability are very important for motor skill performance in the developmental stage. Therefore, the balance and coordination capacities of persons with ID can be improved by basic training programs that constitute the appropriate sports branch, taking into account the appropriate level of exercise and disability. This study has clearly demonstrated the effectiveness of the basic training program of hemsball as a sport, especially for those with moderate levels of ID. In this framework, it is considered that the hemsball sport should be introduced more comprehensively and that the determination of its impact on the general population as well as different handicapped groups will be an important source of data for relevant persons, administrators and institutions as well as to literature.
References
- Arslan, E. and Ince, G. 2015. The effects of 12 weeks exercise program on the level of gross motor skill of the children with atypical autism. International Journal of Sports, Exercise and Training Science, 1, 51–62. doi: 10.18826/ijsets.66769. [DOI] [Google Scholar]
- Boswell, B. 1993. Effects of movement sequences and creative dance on balance of children with mental retardation. Perceptual and motor skills, 77, 1290. doi: 10.2466/pms.1993.77.3f.1290. [DOI] [PubMed] [Google Scholar]
- Bruininks, R. H. and Bruininks, B. 2005. Bruininks-Oseretsky test of motor proficiency (2nd ed.). Minneapolis, MN: NCS Pearson. [Google Scholar]
- Bruininks, R. H. and Chavat, M. 1990. Research on the motor proficiency of persons with mental retardation, psychomotor therapy and adapted physical activity. (Ed: Coppenolle H. V. and Simons J.). In Better Movement Proceeding of the 2 International Symposium, Belgium: 43–69. [Google Scholar]
- Champagne, D. and Dugas, C. 2010. Improving gross motor function and postural control with hippotherapy in children with down syndrome: Case reports. Physiotherapy Theory and Practice, 26, 564–571. doi: 10.3109/09593981003623659. [DOI] [PubMed] [Google Scholar]
- Chen, C. C., et al. 2016. Examining the Davidson’s Model via an exercise variable in individuals with intellectual disabilities. International Journal of Developmental Disabilities, 62, 70–75. doi: 10.1179/2047387714Y.0000000055. [DOI] [Google Scholar]
- Clarke, H. H. and Clarke, D. H. 1978. Developmental and adapted physical education. 2nd ed. Englewood Cliffs, NJ: Prentice Hall Inc. doi: 10.3109/09593981003623659. [DOI] [Google Scholar]
- Cleaver, S., et al. 2009. Physical mobility limitations in adults with intellectual disabilities: A systematic review. Journal of Intellectual Disability Research, 53, 93–105. doi: 10.1111/j.1365-2788.2008.01137.x. [DOI] [PubMed] [Google Scholar]
- Connolly, B. and Michael B. 1986. Performance retarded children, with and without down syndrome, on the Bruininks Oseretsky Test of motor proficiency. Physical Therapy, 66, 344–348. doi: 10.1093/ptj/66.3.344. [DOI] [PubMed] [Google Scholar]
- Dehghani, M. and ve Günay, M. 2015. The effect of balance training on static and dynamic balance in children with intellectual disability. Journal of Applied Environmental and Biological Sciences, 5, 127–131. [Google Scholar]
- Dellavia, C., et al. 2009. Postural stability of athletes in special olympics. Perceptual and Motor Skills, 108, 608–622. doi: 10.2466/PMS.108.2.608-622. [DOI] [PubMed] [Google Scholar]
- Elliott, D. and Bunn, L. 2004. Motor disorders in children with intellectual disabilities. In Dewey D. and Tupper D. E. (Eds.), Developmental motor disorders: A neuropsychological perspective. New York: Guilford Publications, 137–151. [Google Scholar]
- Fotiadou, E. G., et al. 2009. The effect of a rhythmic gymnastics program on the dynamic balance ability of individuals with intellectual disability. Journal of Strength and Conditioning Research, 23, 2102–2106. doi: 10.1519/JSC.0b013e3181b8d3b5. [DOI] [PubMed] [Google Scholar]
- Franciosi, E., et al. 2010. Selected factors correlated to athletic performance in adults with mental retardation. Journal of Strength and Conditioning Research, 24, 1059–1064. doi: 10.1519/JSC.0b013e3181ca503c. [DOI] [PubMed] [Google Scholar]
- Giagazoglou, P., et al. 2013. Effects of a trampoline exercise intervention on motor performance and balance ability of children with intellectual disabilities. Article in Research in Developmental Disabilities, 34, 2701–2707. doi: 10.1016/j.ridd.2013.05.034. [DOI] [PubMed] [Google Scholar]
- Giagazoglou, P., et al. 2012. Effect of a hippotherapy intervention program on static balance and strength in adolescents with intellectual disabilities. Research in Developmental Disabilities, 33, 2265–2270. doi: 10.1016/j.ridd.2012.07.004. [DOI] [PubMed] [Google Scholar]
- Gillespie, L. D., et al. 2009. Interventions for preventing falls in older people living in the community. Cochrane Database System Review CD007146. doi: 10.1002/14651858.CD007146. [DOI] [PubMed]
- Golubovic, S., et al. 2012. Effects of exercise on physical fitness in children with intellectual disability, Research in Developmental Disabilities, 33, 608–614. doi: 10.1016/j.ridd.2011.11.003. [DOI] [PubMed] [Google Scholar]
- Gomes, M. M. and Barela, J. A. 2007. Postural control in down syndrome: The use of somatosensory and visual information to attenuate body sway. Motor Control, 11, 224–234. doi: 10.1123/mcj.11.3.224. [DOI] [PubMed] [Google Scholar]
- Guideti, L., et al. 2010. Could sport specialization influence fitness and health of adults with mental retardation? Research in Developmental Disabilities, 5, 1070–1075. doi: 10.1016/j.ridd.2010.04.002. [DOI] [PubMed] [Google Scholar]
- Gunal, A. 2007. Sensory, motor and cognitive functions' effects on daily living activities and quality of life in autistic children. PhD. Hacettepe University. [Google Scholar]
- Hall, J. M. and Thomas, M. J. 2008. Promoting physical activity and exercise in older adults with developmental disabilities. Topics in Geriatric Rehabilitation, 24, 64–73. doi: 10.1097/01.TGR.0000311407.09178.55. [DOI] [Google Scholar]
- Hartman, E., et al. 2010. On the relationship between motor performance and executive functioning in children with intellectual disabilities. Journal of Intellectual Disability Research, 54, 468–477. doi: 10.1111/j.1365-2788.2010.01284.x. [DOI] [PubMed] [Google Scholar]
- Hoover, J. H. and Wade, M. G. 1985. Motor learning theory and mentally retarded individuals: A historical review. Adapted Physical Activity Quarterly, 2, 228–252. doi: 10.1123/apaq.2.3.228. [DOI] [Google Scholar]
- Jankowicz-Szymanska, A., et al. 2012. The effect of physical training on static balance in young people with ıntellectual disability, Research in Developmental Disabilities, 33, 675–681. doi: 10.1016/j.ridd.2011.11.015. [DOI] [PubMed] [Google Scholar]
- Kao M. S. and Wang C. H. 2016. Impact of frisbee game course on the upper limb motor function of students with intellectual disabilities, International Journal of Developmental Disabilities, 64(2), 96–104. doi: 10.1080/20473869.2016.1267302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magnusson, J. E., et al. 2012. Beneficial effects of clinical exercise rehabilitation for children and adolescents with autism spectrum disorder (ASD). Journal of Exercise Physiology Online, 15, 71–79. [Google Scholar]
- Marchewka, A. 2002. The influence of the improving physical exercises for the body balance of mentally handicapped persons, in the moderate degree of retardation. Medycyna Sportowa, 18, 111–115. [Google Scholar]
- Mülazımoglu Balli, Ö. 2006. The Study of Validity and Reliability of Bruininks-Oseretsky Motor Proficiency Test and the Effects of Gymnastics Education Program on Motor Development of Five-Six–Years–Old Children. PhD Thesis, Ankara University, Ankara.
- Rad, L.S., et al. 2012. The effect of selected physical exercises on gross motor skills of autistic children. International Journal of Sport Studies, 2, 44–55. [Google Scholar]
- Ronald, C. A. 1991. Games, sport and exercises for the physically disabled, ISBN.0-8121-1180-X, 308.
- Salvador-Carulla, L., et al. 2015. Training on intellectual disability in health sciences: The European perspective. International Journal of Developmental Disabilities, 61, 20–31, doi: 10.1179/2047387713Y.0000000027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schalock, R. L., et al. 2010. Intellectual disability: Definition, classification, and systems of supports. 11th ed. Washington, DC: American Association of Intellectual and Developmental Disabilities. [DOI] [PubMed] [Google Scholar]
- Stodden, D. F., et al. 2008. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest, 60, 290–305. doi: 10.1080/00336297.2008.10483582. [DOI] [Google Scholar]
- Suomi, R. and Koceja, D. M. 1994. Postural sway patterns of normal men and women and men with mental retardation during a two-legged stance test. Archives of Physical Medicine and Rehabilitation, 75, 205–209. doi: 10.2466/PMS.75.5.456-456. [DOI] [PubMed] [Google Scholar]
- Todorova, R., et al. 2014. Hemsball game and its influence on handicapped children’s psychopsysical condition and the familys’ Opinion. International Journal of Science Culture and Sport, 1, 665–693. doi: 10.14486/IJSCS138. [DOI] [Google Scholar]
- Tuglu, B. 2016. The development process of hemsball according to the views of hemsball coaches. International Journal of Educational Search Review, 1(2), 34–41. [Google Scholar]
- Tsimaras, V. K. and Fotiadou, E. G. 2004. Effect of training on the muscle strength and dynamic balance ability of adults with down syndrome. Journal of Strength and Conditioning Research, 18, 343–347. doi: 10.1519/R-12832.1. [DOI] [PubMed] [Google Scholar]
- Wall, A. E. T. 2004. The developmental skill-learning gap hypothesis: Implications for children with movement difficulties. Adapted Physical Activity Quarterly, 21, 197–218. doi: 10.1123/apaq.21.3.197. [DOI] [Google Scholar]
- Wang, W. Y. and Ju, Y. H. 2002. Promoting balance and jumping skills in children with down syndrome. Perceptual and Motor Skills, 94, 443–448. doi: 10.2466/pms.2002.94.2.443. [DOI] [PubMed] [Google Scholar]
- Watkinson, E. J., et al. 2001. Engagement in playground activities as a criterion for diagnosing developmental coordination disorder. Adapted Physical Activity Quarterly, 18, 18–34. doi: 10.1123/apaq.18.1.18. [DOI] [Google Scholar]
- Yanardag, M. 2007. Effects of the different exercise training on motor performance and stereotypical behaviors of children with autism. PhD. Hacettepe University. [Google Scholar]