

Abstract
Cystic lymphangiomas (CLs) are benign congenital lymphatic malformations that are thought to represent developmental abnormalities rather than true neoplasms. The head and neck region is the most common site of occurrence, although CLs can be present elsewhere in the body including the axilla, mediastinum, groin, and retroperitoneum. More than 80% of CLs present before the age of two. Occurrence in adults is rare with only a few cases reported in the literature. We describe five cases of cervical CLs in adults and discuss imaging modalities used for diagnostics, clinicopathologic features, and therapeutic options.
Keywords: Cystic lymphangioma, Adults, Imaging studies, Histopathology
Introduction
Cervical cystic lymphangiomas (CLs) are malformations of lymphatic channels that usually develop when the lymphatic system fails to communicate with the normal jugular vein [1]. Most are found in the head and neck region, and 80% present before the age of two [2]. The etiology of lymphangioma development in adults is unclear, but some authors suggest their formation is caused by delayed proliferation of cell rests [3]. Most are asymptomatic. Branchial cleft cysts, dermoid cysts, and neoplasms of lymph nodes are chief considerations on the differential diagnosis of CL in an adult [2, 4]. Imaging modalities, especially ultrasonography (US) and contrast-enhanced computed tomography (CECT), play a crucial role in the characterization of cystic components, determining lesional extent, and guiding treatment decisions. A definitive diagnosis is confirmed by histopathology, and complete surgical resection is the treatment of choice.
Case 1
A 22-year-old woman visited the Ear, Nose, and Throat (ENT) department for a left neck swelling of four months duration. She reported mild pain and discomfort with neck movements. On physical examination, the swelling was soft, fluctuant, and non-tender with normal overlying skin.
US revealed a well-defined, thin-walled, anechoic, cystic mass measuring 20.0 × 46 × 36 mm in size and 18.0 cc in volume. It was located in the left supraclavicular region, posterior to the sternocleidomastoid (SCM) muscle. The common carotid artery and internal jugular vein (IJV) coursed posterior to the lesion. Internal septations of varying thickness were identified with no peripheral or septal vascularity on color flow Doppler imaging. The surrounding soft tissues were normal (Fig. 1). Venolymphatic malformation was suggested as a possible diagnosis.
Fig. 1.

a US grey scale and b color flow Doppler demonstrate a large, well-encapsulated, anechoic, cystic mass with multiple internal septations
Fine needle aspiration cytology (FNAC) of the swelling yielded 5 ml of milky fluid which considerably reduced the size of the lesion post-aspiration. Cytologic examination of May-Grunwald-Giemsa (MGG) stained smears showed moderate cellularity of mature lymphocytes against a proteinaceous background. These findings supported the radiologic impression of CL (Fig. 2a). Surgical excision of the lesion was performed and histopathologic examination confirmed the diagnosis (Fig. 2b). No recurrence was observed with six months of follow-up.
Fig. 2.

a MGG stained smear of the fluid aspirate shows mature lymphocytes against a proteinaceous background. b Characteristic histologic findings of dilated lymphatic spaces and moderate to dense lymphoid infiltrate in the surrounding fibrocollagenous stroma (H&E × 400)
Case 2
A 21-year-old female patient consulted an ENT physician for a swelling in the right supraclavicular region which had slowly increased in size over the preceding six months. She complained of mild pain and difficulty in swallowing. There was no history of neck trauma or respiratory tract infection. Her routine laboratory investigations were normal except for mild anemia.
US revealed a well-encapsulated, anechoic, cystic area that measured 17 × 13 mm. It was located in the right neck, posterior to the sternocleidomastoid muscle. Fine internal septations were observed and a diagnosis of CL favored. No cervical lymphadenopathy was present.
FNAC of the swelling revealed numerous small lymphocytes admixed with a few red blood cells (RBCs), and a presumptive diagnosis of benign cystic lesion was rendered.
The patient underwent preoperative contrast-enhanced computed tomography (CECT) of the neck to assess the extension of the cervical lesion. It revealed a voluminous, well-circumscribed, thin-walled, non-enhancing, hypodense mass lesion of fluid attenuation in the right neck, posterior to the SCM muscle. It extended cranially to the level of the upper margin of the C4 vertebra and inferiorly to the level of the thoracic inlet (upper margin of D1 vertebra). The lesion caused a mild compression of the adjacent paraspinal muscles in the retroclavicular region (Fig. 3).
Fig. 3.

CECT of the neck shows a voluminous, well-defined, thin-walled, non-enhancing mass lesion of fluid attenuation posterior to right sternocleidomastoid. It extends cranially to the C4 vertebra and caudally to the level of the thoracic inlet
The mass was treated with complete surgical resection. Histopathologic examination confirmed a diagnosis of a CL (Fig. 4). The patient was kept on regular follow-up for 1 year and was recurrence-free.
Fig. 4.
Ectatic lymphatic vessels lined by attenuated endothelium. Some contain lymphoid aggregates (H&E × 100)
Case 3
A 23-year-old male presented to the surgery department of our institute for a swelling of the right neck of three months duration. No history of trauma or infection was elicited.
US revealed a well-circumscribed, cystic mass posterior to the right submandibular region and anterior to the SCM muscle. Features included fine internal echoes and layering debris. The differential diagnosis included lymphangioma and branchial cleft cyst. A FNAC suggested a benign cystic lesion.
CECT imaging of the neck revealed evidence of a smooth, marginated, hypodense lesion in the right infrahyoid region that abutted the right thyroid cartilage. Anterosuperiorly, it extended to the right submandibular gland, inferiorly to the SCM muscle, and posteriorly to the carotid space without compression of the carotid vessels. The possibility of a branchial cleft cyst was considered.
Complete surgical excision of the lesion was performed. Histopathologic examination revealed multiple dilated lymphatic channels lined by attenuated endothelium with intervening stroma. The stroma contained moderate to dense lymphoid aggregates. A diagnosis of CL was given (Fig. 5a, b). The patient was lost to follow-up.
Fig. 5.

a Lymphatic channels of varying caliber (H&E × 100). b High power view shows a lymphoid aggregates in the lymph space and in the septa (H&E × 400)
Case 4
A 35-year-old female was referred to the surgery department for neck pain and a sudden enlargement of a pre-existent right-sided neck swelling. The patient was three months post-partum. She first noticed the swelling six months ago but reported a rapid increase in size over the last 15 days.
CECT neck revealed a well-defined, elongated, hypodense lesion of fluid density with enhancing thin internal septations and lobulated margins. It involved the right side of the neck near the internal jugular vein (IJV) and posteromedial to the SCM muscle. It extended from angle of mandible up to the proximal half of the muscle (Fig. 6a, b). Neck vessels were normal in caliber with contrast enhancement. No cervical lymphadenopathy was seen. A radiographic differential diagnosis favored branchial cyst or lymphangioma.
Fig. 6.

a and b CECT of the neck demonstrates an elongated, well-circumscribed, hypodense lesion with enhancing thin internal septations involving the right side of the neck. It is in close proximity to IJV and posteromedial to the sternocleidomastoid muscle
Complete surgical extirpation was performed. The histopathologic findings were consistent with CL (Fig. 7).
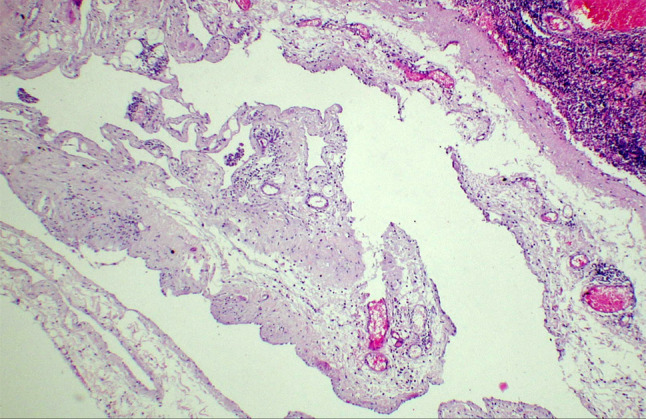
Fig. 7.

Histology shows a multi-cystic lesion lined by flattened endothelium along with dense lymphoid infiltrate in the wall (H&E × 100)
Case 5
A 36-year-old woman presented to the ENT department with a right-sided neck swelling of four months duration. The patient was asymptomatic and seeking medical advice for cosmetic reasons.
US revealed a well-defined, anechoic lesion with multiple thin septations on the right side of the neck. No evidence of internal echoes, vascularity, or calcifications was seen.
FNAC yielded 8 ml of yellow-colored fluid with cytologic findings consistent with lymphangioma. Histopathology confirmed the diagnosis. The patient was followed for six months and was recurrence-free.
Discussion
First described by Redenbacher in 1828, lymphangiomas comprise approximately 4% of all vascular tumors and about 26% of benign vascular tumors in children [5, 6]. CLs chiefly present at birth or during the first two years of life. They are classified into four types: (1) cavernous lymphangioma, (2) cystic hygroma/cystic lymphangioma, (3) lymphangioma circumscriptum, and (4) acquired progressive lymphangioma/benign lymphangioendothelioma [7, 8]. The majority represent developmental abnormalities rather than true neoplasms. There is no sex predilection and the lesions tend to affect the neck, axilla, and groin [9, 10].
Our case series describes the rare occurrence of CL in five adults, four females and one male, presenting in the third and fourth decades of life. CLs in adulthood are exceedingly rare lesions of uncertain histogenesis. The majority are asymptomatic and the patient usually seeks medical advice for cosmetic reasons or fear of underlying neoplastic pathology. Obstructive symptoms are rare. Entities that enter the differential diagnosis include thyroglossal duct cyst, bronchogenic cyst, cystic dermoid, and malignant lymph node [1].
In our series, the most common clinical presentation was a soft, fluctuant neck mass causing mild pain, restricted movement, and dysphagia. One case presented with a sudden increase in the size of pre-existent swelling.
Different imaging modalities used preoperatively to evaluate cystic neck masses include ultrasonography, CECT, and MRI depending on availability, cost-effectiveness, and patient convenience [11]. In our study, US with color flow Doppler was the first-line investigation. Venolymphatic malformation was suggested in four cases with a branchial cleft cyst as the most common second differential. CECT and MRI may be used to assess the intrathoracic extension which is seen in 10% of cervical CLs [12]. In our study, none of the cases revealed intrathoracic extension.
Although there is no consensus in the literature regarding the role of FNAC in the diagnosis of CL, FNAC supported the radiographic diagnosis of CL in two of our cases. In the other cases, it helped exclude malignancy, thus guiding the surgical approach. Aspiration of these lesions yielded 5 to 8 ml yellow turbid fluid. The cytologic findings revealed predominantly mature lymphocytes against the proteinaceous background, characteristic of lymphangioma.
The definitive diagnosis of CL is histopathologic after surgical resection. Microscopically, CLs are characterized by ectatic and dilated lymphatic spaces lined by an attenuated endothelium. Some of lumina contain lymph fluid. The spaces are surrounded by fibrocollagenous septa harboring varying degrees of lymphoid aggregates. All the cases of our study demonstrated these typical histologic features.
The best treatment for cervical CLs is complete surgical resection [12–16]. Partial removal is associated with high rates of recurrence, as high as 88% [13, 15]. Other treatment methods include sclerotherapy, radiotherapy, laser therapy, electrocoagulation, and cryotherapy. OK-432 is considered to be the sclerosing agent of choice for CL [17]. Usually, these therapies are used either alone or in combination with surgery in the treatment of large, complex lesions.
Conclusion
Cervical CLs are uncommon in adults but should be considered in the evaluation of cystic neck masses. FNAC can be useful as a preoperative diagnostic tool in combination with adequate imaging studies. Complete surgical resection constitutes the mainstay of treatment with regular follow-up.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they no conflict of interest.
Ethical Approval
This study is ethically approved by the institutional ethical committee because of its retrospective nature and all the procedures being performed were part of the routine care.
References
- 1.Gow L, Gulati R, Khan A, Mihaimeed F. Adult-onset cystic hygroma: a case report and review of management. Grand Rounds. 2011;11:5–11. doi: 10.1102/1470-5206.2011.0002. [DOI] [Google Scholar]
- 2.Kraus J, Plzak J, Bruschini R, et al. Cystic lymphangioma of the neck in adults: a report of three cases. Wiener Klin Wochenschr. 2008;120:242–5. doi: 10.1007/s00508-008-0950-4. [DOI] [PubMed] [Google Scholar]
- 3.Suk S, Sheridan M, Saenger JS. Adult lymphangioma: a case report. Ear Nose Throat J. 1997;76:881–83. doi: 10.1177/014556139707601210. [DOI] [PubMed] [Google Scholar]
- 4.Schefter RP, Olsen KD, Gaffey TA. Cervical lymphangioma in the adult. Otolaryngol Head Neck Surg. 1985;93:65–9. doi: 10.1177/019459988509300113. [DOI] [PubMed] [Google Scholar]
- 5.Coffin CM, Dehner LP. Vascular tumors in children and adolescents: a clinicopathologic study of 228 tumors in 222 patients. Pathol Annu. 1993;28:97. [PubMed] [Google Scholar]
- 6.Redenbacher EAH. De Ranula Sublingual, Speciali, Cum Casa Congenital. Monachii: Lindhauer; 1828. [Google Scholar]
- 7.Peachy RDG, Lim CC, Whimster IW. Lymphangioma of the skin. Br J Dermatol. 1970;83:519. doi: 10.1111/j.1365-2133.1970.tb15735.x. [DOI] [PubMed] [Google Scholar]
- 8.Watanawe M, Kishiyama K, Ohkawara A. Acquired progressive lymphangioma. J Am Dermatol. 1993;8:663–67. doi: 10.1016/S0190-9622(83)70076-9. [DOI] [PubMed] [Google Scholar]
- 9.Chervenak FA, Isaacson G, Blakemore KJ, et al. Fetal cystic hygroma: cause and natural history. N Engl Med. 1983;309:822. doi: 10.1056/NEJM198310063091403. [DOI] [PubMed] [Google Scholar]
- 10.Alqahtani A, Nguyen LT, Flageole H, et al. 25 years experience with lymphangiomas in children. J Pediatr Surg. 1999;34:1164. doi: 10.1016/S0022-3468(99)90590-0. [DOI] [PubMed] [Google Scholar]
- 11.Romeo V, Maurea S, Guarino S, Sirignano C, Mainenti PP, Picardi M, Salvatore M. A case of lower- neck cystic lymphangioma: correlative US, CT, and MR imaging findings. Quant Imaging Med Surg. 2013;3:224–27. doi: 10.3978/j.issn.2223-4292.2013.08.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Morley SE, Ramesar KC, Macleod DA. Cystic hygroma in an adult: a case report. J of the R Coll Surg Edinb. 1999;44:57–8. [PubMed] [Google Scholar]
- 13.Curran AJ, Malik N, McShane D, et al. Surgical management of lymphangiomas in adults. J Laryngol Otol. 1996;110:586–89. doi: 10.1017/S0022215100134334. [DOI] [PubMed] [Google Scholar]
- 14.Karkos PD, Spencer MG, Lee M, et al. Cervical cystic hygroma/lymphangioma: an acquired idiopathic late presentation. J Laryngol Otol. 2005;119:561–63. doi: 10.1258/0022215054352144. [DOI] [PubMed] [Google Scholar]
- 15.Riechelmann H, Muehlfay G, Keck T, et al. Total, subtotal, and partial surgical removal of cervicofacial lymphangiomas. Arch Otolaryngol Head Neck Surg. 1999;125:643–48. doi: 10.1001/archotol.125.6.643. [DOI] [PubMed] [Google Scholar]
- 16.Kennedy TL, Whitaker M, Pellitteri P, Wood WE. Cystic hygroma/ lymphangioma; a rational approach to management. Laryngoscope. 2001;111:1929–37. doi: 10.1097/00005537-200111000-00011. [DOI] [PubMed] [Google Scholar]
- 17.Ogita S, Tsuto T, Tokiwa T, Takahashi T. Treatment of cystic hygroma in children with special reference to OK-432 therapy. Z Kinderchir. 1987;42:279–81. doi: 10.1055/s-2008-1075602. [DOI] [PubMed] [Google Scholar]