

Abstract
Background:
Urolithiasis is the most common urological problem worldwide. It is a recurrent multifactorial problem that is caused by the interaction of several environmental and genetic factors. This study aimed to assess the prevalence of renal stones among local residents in Saudi Arabia in order to renew the statistics of renal stones occurrence in the current Saudi population.
Methods:
A cross-sectional study was conducted using an electronic questionnairethat was distributed randomly through phones and social media to reach the local residents in Saudi Arabia. We then reviewed the published papers in Saudi journals for patients with renal stones.
Results:
From a total of 580 responders to the electronic questionnaire, the prevalence of renal stones was 9.1% (n = 64). The median age at diagnosis was 29 years and the mean age at diagnosis was 36.91 years (SD = 18.66, Range of 20–99). Two peaks of age were observed, the first peak was at the (21–25) age group representing 34.4% of the kidney stones patients. The second peak was older than 47 years. The majority of those diagnosed with kidney stones had normal BMI (n = 29, 45.3%), and the family history of kidney stones among first degree relatives was found in 35.9% of the cases (n = 23).
Conclusion:
Kidney stones is a common health problem with the local incidence being underreported. In our sample, the prevalence was 9.1%. We also observed a relatively high percentage of positive family history among renal stone patients (34.9%) that could be attributed to the high rates of consanguinity. We encourage more local epidemiological studies to describe the patterns and the contributing factors of the development of kidney stones.
Keywords: Kidney stone, local residents, prevalence, Saudi Arabia
Introduction
Urolithiasis is a recurrent multifactorial disorder that is caused by the interaction of several environmental and genetic factors.[1,2] It is considered to be the most common urological disorder among adults. Over the last decades, the incidence has increased in all age groups, all genders, and all races.[1,3]
Several different risk factors can contribute to the development of urolithiasis such as age, gender, ethnic groups, local climate, dietary habits, physical activity, and occupation. Having a comorbid medical condition such as diabetes, hypertension, and obesity is another major factor.[4,5]
The incidence of this preventable disease ranges from 7%–13% in North America, 5%–-9% in Europe, and 1%–5% in Asia.[6]
In regard to the age at diagnosis, the peak age of presentation in Saudi Arabia is between 22 and 44 years of age.[7] Despite the increasing incidence and the underreported prevalence of kidney stones, it has a recurrent nature once it is developed. The chance of reoccurrence is as high as 50% within the next 5 years.[8]
There are different components of renal stones, however, stones composed of calcium such as calcium oxalate or calcium phosphate stones are considered to be the most common.[9]
Ongoing researches try to estimate the epidemiology of renal stones worldwide.[1,10] Locally speaking most of these researches are either directed toward pediatric population or the other several studies, which target adults in Saudi who are not considered new.[9,11,12,13,14] So, in this study, we aim to assess the prevalence of renal stones among local adult residents in Saudi Arabia in order to renew the statistics of renal stones occurrence in the current Saudi population.
Methods
A cross-sectional study to assess the prevalence of renal stones in Saudi Arabia. We distributed an electronic questionnaire randomly through phones and social media to reach the local public in the different Saudi regions then we reviewed the published papers in Saudi journals for patients with renal stones focusing mainly on adults.
Study participant
We included both genders, age above 18 years old, a local resident in Saudi Arabia who was previously or currently diagnosed with renal stone and we excluded anyone who does not fit those three criteria.
Data collection
The data collection process was accomplished by the main investigators. Using an electronic data collection sheet reviewed and approved by the ethical review board at king Abdulaziz university hospital, Jeddah, Saudi Arabia.
Statistical analysis
In the current study, statistical analysis using “IBM SPSS Statistics ver. 20.0” was applied to evaluate and test the hypothesis. Descriptive statistics was used to calculate means, std. deviation, median, and quartiles, simple frequency tables and percentages. Shapiro–Wilk test was used to test the normality of the study sample. Non-parametric “Mann–Whitney U” test was used between the group diagnosed with renal stones and who were not diagnosed with renal stones.
A Chi-square test was used to test the relation between the two variables.
Results
This is a cross-sectional study aimed to explore the prevalence of kidney stones in Saudi Arabia. We had a total of 580 responders to an electronic questionnaire distributed randomly to the general public. Figure 1, represents the distribution of the questionnaire among the local cities of Saudi Arabia. The mean age of the responders in our sample was 27.5 ± 10.8 years, there was unequal number of females to male responders, n = 329, 56.7%, and n = 251, 43.3%, respectively. Table 1 illustrates the epidemiological features of those diagnosed with kidney stones, incidence of renal stone in this sample was 9.1% (n = 64) and 2.6% of them are still having renal stone disease (n = 15). Females = 33 (51.6%) and males = 31 (48.4%). There was no significant relation between gender and renal stone incidence. (P = 0.377).
Figure 1.
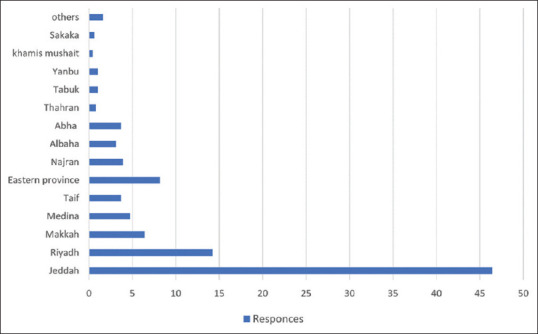
Distribution of the questionnaire responses among the cities of Saudi Arabia
Table 1.
The epidemiological features of those with Urolithiasis disease
| Urolithiasis disease | |
|---|---|
| Mean Age in years±SD | 36.91±18.66 |
| Gender | |
| Male (% within the gender) | 31 (12.4%) |
| Female (% within the gender) | 33 (10.0%) |
| BMI kg/m2 | |
| Underweight (< 18.5) | 7 (10.9%) |
| Normal weight (18.5-24.9) | 29 (45.3%) |
| Overweight (25-29.9) | 16 (25%) |
| Obese class 1 (30-34.9) | 7 (10.9%) |
| Obese class 2 (≥ 35) | 5 (7.8%) |
| Marital status | |
| Single | 27 (42.2%) |
| Married-divorced | 32 (50%) |
| Widowed | 5 (7.8%) |
| Employment | |
| Yes | 30 (46.9%) |
| No | 13 (20.3%) |
| Student | 21 (32.8%) |
Regarding the age at diagnosis, there were two peaks of age. The first peak was at the (21–25) age group representing 34.4% of the kidney stones patients. The second peak was older than 47 years. The median age at diagnosis was 29 years and the mean age at diagnoses 36.91 years (SD = 18.66, Range of 20–99). Chi-square test for the age groups and renal stones showed significant relation P < 0.0005. The median period of the disease = 4 years. The majority of those diagnosed with kidney stones had a normal BMI (n = 29, 45.3%). Family history of kidney stones among first degree relatives was found in 35.9% of the cases (n = 23) while 21.9% (n = 14) are not sure whether they have a positive family history or not. Regarding the socioeconomics of nephrolithiasis patients, the majority had university education (n = 51, 79.7%) and are employed (n = 30, 46.9%) or still a student (n = 21, 32.8%). Table 2 illustrates the clinical presentation of renal stone disease with flank pain being the most common presentation (n = 39, 60.9%). There was no significant relationship as illustrated by Chi-square test for the relationship between each clinical symptom at presentation and gender, age, marital status, or BMI classification within patients with renal stones.
Table 2.
The clinical presentation of renal stone disease
| Clinical presentation of the renal stone disease | No | Yes | ||
|---|---|---|---|---|
| Count | Table n % | Count | Table n | |
| Flank pain | 25 | 39.1% | 39 | 60.9% |
| Lower abdominal pain | 43 | 67.2% | 21 | 32.8% |
| Hematuria | 47 | 73.4% | 17 | 26.6% |
| Dysuria | 43 | 67.2% | 21 | 32.8% |
| Decreased amounts of urine, compared to the patient’s regular amount | 48 | 75.0% | 16 | 25.0% |
| Urinary Urgency | 43 | 67.2% | 21 | 32.8% |
| Fever/Chills | 56 | 87.5% | 8 | 12.5% |
| Nausea/Vomiting | 46 | 71.9% | 18 | 28.1% |
| No symptoms | 59 | 92.2% | 5 | 7.8% |
Discussion
Adults urolithiasis is still the most common uological problem.[1] Globally reported that the prevalence and the incidence of nephrolithiasis have increased dramatically for both genders with a huge cost implication related to providing medical care for such patients and accountable job absences.[2]
Few former studies have tried to estimate how prevalent nephrolithiasis locally in the country. Ahmad et al. looked into the epidemiology of urolithiasis among patients who have had visited a local clinic in Riyadh, reporting that 19.1% of the patients had calculi in the urinary tract and nephrolithiasis frequency was 14% from their 1029 patients who have had urinary calculi.[3] However, in this study, we observed that among 580 responses we received from the community, the prevalence of kidney stones was 9.1% (n = 64), which is lower than the former study. This could be since their population included sick patients who have had visited the clinic with or without urological complain while we tried to estimate the prevalence of kidney stones among the local community.
Various factors affect the incidence of forming kidney stones including gender, age, dietary factors as well as family history. Earlier studies concluded that males are more susceptible to renal calculi than females.[3,4,5,6] A study done by Amir et al. showed a significant gender disparity in stone formation with male predominance approaching up to 79% of cases.[5] However, in our study female has predominated (n = 33, 51.6%), with male to female ratio of 31:33. This could be due to the unequal number of males and females in the study population. Moreover, we find no significant relationship between gender and renal stone incidence (P = 0.377). Age, however, had a significant relation with kidney stones (P < 0.0005) with bimodal age distribution.
The first peak was at the (21–25) age group representing the greatest majority of nephrolithiasis patients to be among young individuals (n = 22, 34.4%). The second peak was older than 47 years (n = 14, 21.9%). Similar to local hospital statistics in Saudi Arabia,[11,15,16,17,18,19] for the peak age of presentation to be between 22 and 44 years. This observation of young age at presentation to predominate warrants more insight into factors that possibly affect stone formation among young Saudi residents.
Another observation is that 35.9% of the cases (n = 23) had a positive family history of kidney stones among first degree relatives (parents, siblings) and 21.9% (n = 14) could have a positive family history as well. Patients with urolithiasis commonly report positive family history and substantially increase the risk of renal calculi in their siblings, and have higher recurrence incidence than in those without a family history of stones. Therefore, a family history of stones is considered as one of the 8 items in the stone recurrence predictive score.[20] The high percentage of positive family history among the resident in our study who are diagnosed with RSD could be attributed to the genetic bases of the disease.
Hypercalciuria, hypocitraturia, primary hyperoxaluria, and cystinuria are all an inherited form of renal stones that have different forms of a genetic defect. Another explanation could be due to the high rate of positive consanguinity in Saudi Arabia. A local study by Jameel et al. have tried to shed light on such phenomena as the high rate of consanguinity in our country has helped to understand the genetic bases of different pediatric renal diseases.[21]
Limitations
Some of the questions in the survey have not been answered by the participants in which could have added more correlation to our study such as body mass index. Furthermore, since the study was held in the western region and most notably, Jeddah, it has been difficult to reach people from other regions, which could have emphasized the geographical distribution and lifestyle differences.
Future plan
If we were to design the study template again, we would have applied several changes. Most importantly, to apply the study on a wider scale with a larger number of participants, from various age groups and different regions across the country. Furthermore, we would highlight other aspects such as dietary habits in the form of the frequency of hydration, calcium intake, and bowel habits. Also, we would address different types of stones and follow-up management in the long term.
Conclusion
Urolithiasis is a common health problem with the local incidence being underreported. In our sample, the prevalence was 9.1%. We also observed a relatively high percentage of positive family history among renal stone patients (34.9%) that could be attributed to high rates of consanguinity. We encourage more local epidemiological studies to describe the patterns and the contributing factors of the development of kidney stones.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Romero V, Akpinar H, Assimos DG. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev Urol. 2010;12:e86–96. [PMC free article] [PubMed] [Google Scholar]
- 2.Seitz C, Fajkovic H. Epidemiological gender-specific aspects in urolithiasis. World J Urol. 2013;31:1087–92. doi: 10.1007/s00345-013-1140-1. [DOI] [PubMed] [Google Scholar]
- 3.Ahmad F, Nada MO, Farid AB, Haleem MA, Razack SMA. Epidemiology of urolithiasis with emphasis on ultrasound detection: A retrospective analysis of 5371 cases in Saudi Arabia. Saudi J Kidney Dis Transpl. 2015;26:386–91. doi: 10.4103/1319-2442.152557. [DOI] [PubMed] [Google Scholar]
- 4.Alkhunaizi AM. Urinary stones in Eastern Saudi Arabia. Urol Ann. 2016;8:6–9. doi: 10.4103/0974-7796.164841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Amir A, Matlaga BR, Ziemba JB, Sheikh S. Kidney stone composition in the Kingdom of Saudi Arabia. Clin Nephrol. 2018;89:345–8. doi: 10.5414/CN109313. [DOI] [PubMed] [Google Scholar]
- 6.Liu Y, Chen Y, Liao B, Luo D, Wang K, Li H, et al. Epidemiology of urolithiasis in Asia. Asian J Urol. 2018;5:205–14. doi: 10.1016/j.ajur.2018.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jarrar BM, AL-Enazi MM, Al-Messar S. Chemical composition of urinary calculi from Al-jouf province of Saudi Arabia. JRMS. 2007;14:15–9. [Google Scholar]
- 8.Bihl G, Meyers A. Recurrent renal stone disease-advances in pathogenesis and clinical management. Lancet. 2001;358:651–6. doi: 10.1016/S0140-6736(01)05782-8. [DOI] [PubMed] [Google Scholar]
- 9.Ragab AR, Al-Mazroua MK. Pattern of pediatric toxicity in Saudi Arabia-Eastern province (incidence, demographics and predisposing factors)? Pediat Therapeut. 2015;5:1. DOI: 10.4172/2161-0665.1000220. [Google Scholar]
- 10.Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol. 2000;13:S45–50. [PubMed] [Google Scholar]
- 11.Abomelha MS, Al-Khader AA, Arnold J. Urolithiasis in Saudi Arabia. Urology. 1990;35:31–4. doi: 10.1016/0090-4295(90)80008-b. [DOI] [PubMed] [Google Scholar]
- 12.Khan AS, Rai ME, Gandapur, Pervaiz A, Shah AH, Hussain AA, et al. Epidemiological risk factors and composition of urinary stones in Riyadh Saudi Arabia. J Ayub Med Coll Abbottabad. 2004;16:56–8. [PubMed] [Google Scholar]
- 13.Alsuwaida AO, Farag YMK, Al Sayyari AA, Mousa D, Alhejaili F, Al-Harbi A, et al. Epidemiology of chronic kidney disease in the kingdom of Saudi Arabia-A pilot study. Saudi J Kidney Dis Transpl. 2010;21:1066–72. [PubMed] [Google Scholar]
- 14.Kari JA. Pediatric renal disease in the kingdom of Saudi Arabia. World J Pediatr. 2012;8:217–21. doi: 10.1007/s12519-012-0360-6. [DOI] [PubMed] [Google Scholar]
- 15.Kassimi MA, Abdel-Halim RE, Hardy MJ. The problem of urinary tract stones in the Western Region of Saudi Arabia. Saudi Med J. 1986;7:394–401. [Google Scholar]
- 16.Cutajar CL. The role of Schistosomiasis in urolithiasis. Br J Urol. 1983;55:349–52. doi: 10.1111/j.1464-410x.1983.tb03319.x. [DOI] [PubMed] [Google Scholar]
- 17.Taha S, Mitry NF, Hiondi G. The pattern of urinary calculi in the Eastern Province of Saudi Arabia. Arab J Med. 1985;4:4–8. [Google Scholar]
- 18.Ekman P, Husain I, Sharma ND, Al-Faqih SR. Transurethral ureteroscopy-Safety guide wire as an aid to a more aggressive approach. Br J Urol. 1987;60:23–27. doi: 10.1111/j.1464-410x.1987.tb09126.x. [DOI] [PubMed] [Google Scholar]
- 19.Abdel-Halim RE. Some observations on the operative management of renal stones. In: Ryall R, Brockis JG, Marshall V, Finlayson B, editors. Urinary Stone. Melbourne, Edinburgh, London, New York: Churchill Livingstone; 1984. pp. 125–30. [Google Scholar]
- 20.Koyuncu H, Yencilek F, Eryildirim B, Sarica K. Family history in stone disease: How important is it for the onset of the disease and the incidence of recurrence? Urol Res. 2010;38:105–9. doi: 10.1007/s00240-009-0249-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kari JA, Bockenhauer D, Stanescu H, Gari M, Kleta R, Singh AK. Consanguinity in Saudi Arabia: A unique opportunity for pediatric kidney research. Am J Kidney Dis. 2014;63:304–10. doi: 10.1053/j.ajkd.2013.08.033. [DOI] [PubMed] [Google Scholar]