

Summary
Umbilical cord hemangioma is an uncommon benign vascular neoplasm arising from the free segment of the umbilical cord, distinct from placental and fetal insertion, and is thought to originate from endothelial cells of the umbilical vessels. Cystic changes in the umbilical cord rarely occur as a consequence of the damage to the amnionic surface of the cord caused by the presence of the hemangioma. Until now, a total of 8 cases of umbilical cord hemangioma associated with cystic changes in the umbilical cord have been reported in the literature, however, among these cases, only one showed an associated cyst derived from inclusion of the amniotic epithelium, and the remaining seven cases consisted of hemangiomas with associated pseudocyst of the umbilical cord. We herein report a case of umbilical cord hemangioma with an associated amnionic epithelial inclusion cyst. Clinicopathological features and differential diagnostic considerations are also discussed.
Key words: Hemangioma, Plancenta, Umbilical cord, Cyst, Amnionic epithelium
Introduction
Hemangiomas are benign mesenchymal neoplasms composed of blood vessels and are the most common tumors during infancy and childhood. Most hemangiomas are superficial lesions that have a predilection for the skin and soft tissues, especially in the head and neck region, but they may affect almost any organ 1. On histological examination, hemangiomas are usually composed of a proliferation of capillary-sized vessels lined by a single layer of flattened endothelial cells. A characteristic histological finding in most hemangiomas is the presence of neoplastic vascular channels arranged around larger, dilated “feeder” vessels. Several cases of placental hemangioma have been reported in the literature, however the umbilical cord is an extremely rare site of occurrence 2. Umbilical cord hemangioma is regarded as a vascular proliferation placed on the free segment of the umbilical cord, distinct from placental and fetal insertion and is thought to originate from endothelial cells of the umbilical vessels 3. On gross examination, the tumor presents as a fusiform swelling in the cord surrounded by edema of the Wharton jelly. Umbilical cord cysts are usually classified as true cysts, which are epithelial-lined cysts derived from embryological remnants of the allantois or omphalomesenteric duct and pseudocysts, which arise from degeneration of Wharton’s jelly surrounding the cord vessels 4. Until now, a total of 8 cases of umbilical cord hemangioma associated with cystic changes in the umbilical cord have been reported in the literature, and only one case showed an associated cyst derived from inclusion of the amniotic epithelium 5-13. We herein report a singular case of umbilical cord hemangioma with an associated amnionic epithelial inclusion cyst. Clinicopathological features and differential diagnostic considerations are also discussed.
Materials and methods
The placenta and umbilical cord samples were submitted for histological examination in neutral-buffered 10% formalin. They were dehydrated according to the standard techniques, embedded in paraffin, cut to 5-mm, and stained with hematoxylin and eosin (H&E). Immunohistochemical analysis was performed with the labeled streptavidin–biotin peroxidase detection system using the Ventana automated immunostainer (Ventana Medical systems, Tucson, AZ). The following antibodies were tested: CD31 (dilution 1:50), CD34 (dilution 1:50), cytokeratins (AE1/AE3 clone; dilution 1:50); all from Dako, Glostrup, Denmark. Endothelial cells of the umbilical vessels and amnion epithelium of the umbilical cord were used as internal controls for pan-cytokeratin and CD31 antibody respectively.
Clinical summary
A 28-year old woman came into our observation at 34 weeks of gestational age for pelvic pain. US of the umbilical cord showed a solid hypoechoic mass measuring 7 x 5 cm consistent with an umbilical cord cyst. Cardiotocography and ECG showed no abnormalities. The patient came again to our observation after 2 weeks, at 36° week of pregnancy, for pelvic pain and reduced fetal movement. Cardiotocography showed a basic frequency of 120 bpm with unregular contractile activity. US of the umbilical cord showed an increase in size of the solid hypoechoic mass previously detected (10 x 9 cm). For these reasons, in agreement with the patient, a caesarean section was performed. The alive newborn was transferred to neonatal intensive care unit for low birth weight and respiratory distress, after 7 days the infant was resigned in good general condition.
Pathological findings
The placenta and its umbilical cord were submitted for pathologic examination. The placenta was discoid in shape, weighed 630 g and measured 17 x 15.5 x 5 cm. The chorionic blood vessels were normally distributed over the fetal surface. The umbilical cord showed three vessels, measured 40 cm in length and was inserted centrally. Twenty cm from the placental insertion, a large unilocular cystic mass of 10 cm in greatest diameter, filled with clear fluid was detected (Fig. 1). Cut sectioning through the wall of the cyst revealed a brown nodular mass of 6 cm in diameter originating from the umbilical cord. On histological examination, the mass consisted of a heterogeneous proliferation of multiple dilated thin-walled vascular channels, containing an admixture of capillary, cavernous and mixed vessel types. The neoplastic vessels were circumpherentially arranged around the umbilical artery and at higher magnification, an evident origin from endothelial cells of the umbilical vessel was noted. In fact, cross-sections of the umbilical artery, revealed endothelial lined channels transgressing the vessel wall and communicating with the surrounding vascular proliferation (Fig. 2). No apparent thrombus formation was seen. The neoplastic vessels were composed of a single layer of flat, non-atypical endothelial cells, showing no mitotic activity. Immunohistochemically, the vascular channels were positive for CD31 and CD34. The accompanying stroma showed marked myxo-edematous changes; no inflammatory infiltration was noted. The associated cyst was lined by a single layer of flattened to cuboidal cells, which showed positive immunostain for pan-cytokeratin antibody (clone AE1/AE3) (Fig. 1), consistent with an amnionic epithelial inclusion cyst. On the basis of the above-mentioned findings a diagnosis of umbilical cord hemangioma with associated amnionic epithelial inclusion cyst was rendered. Placenta examination showed chorangiosis, but no additional significant pathologic abnormalities were identified.
Fig. 1.
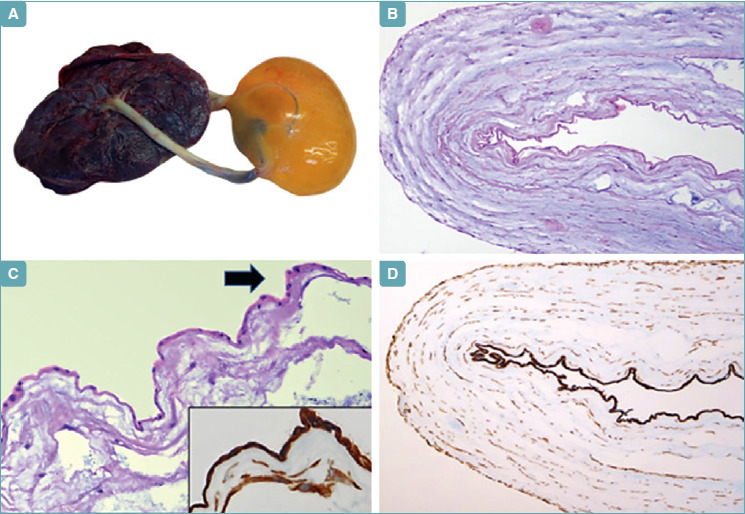
A) Macroscopic appearance the placenta and umbilical cord. A large cystic mass of 10 cm in greatest diameter can be appreciated in the umbilical cord close to the placental insertion. B) On histological examination, the cystic mass consisted of a single layer of eosinophilic cells. Myxoid degeneration of the cystic wall can also be appreciated. C) Higher magnification of the cyst reveals a single layer of amnionic epithelial cells with flattened or cuboidal morphology (arrow). The epithelial origin of the cyst is confirmed by positive immunostain for pan-cytokeratin antibody (clone AE1/AE3) (inset; D).
Fig. 2.
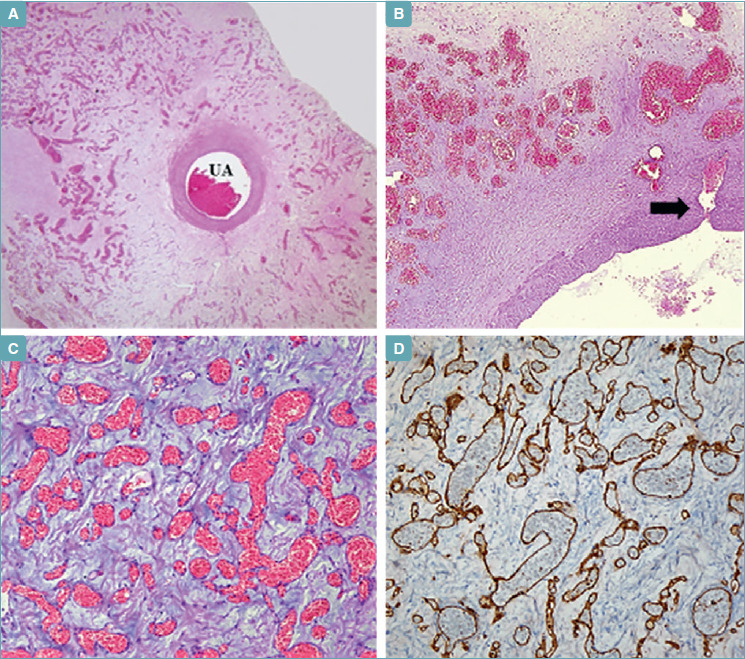
A) Photomicrograph of the hemagioma showing multiple round or elongated, vascular channel surrounding the umbilical artery (UA) (Stain: Haematoxylin and Eosin). B) The neoplastic vessels seem to originate and radiate from the umbilical artery (arrow). C) The neoplastic vascular channels are embedded in a dense myxoid stroma and show diffuse immunohistochemical staining for CD31 antibody (D).
Discussion
The association between umbilical cord hemangioma and cystic degeneration of umbilical cord is a rare evenience with only 8 cases reported in the literature so far. In all reported cases except one, the cystic mass of the umbilical cord revealed to be a pseudocyst covered by amnion with no epithelial or endothelial lining 5-12. These lesions were located near the placental side or at the end of the umbilical cord and ranged in size from 8 to 25 cm. Regarding their origin, it has been suggested that pseudocystic changes of the umbilical cord might result from liquefaction of the mucopolysaccharide-rich membrane surrounding the cord vessels 12. S.M. Jacques et al. in 2013 reported a unique case of hemangioma of the umbilical cord associated with a true cyst covered and lined by a layer of amnionic epithelium. The author suggested that the cyst formation was a consequence of the damage to the amnionic surface of the cord caused by the presence of the hemangioma 13. Amnionic epithelial inclusion cysts are very uncommon lesions that arise from inclusions or infoldings of the amnionic surface 13. These are simple cysts lined by a single layer of amnionic epithelium and usually contain clear fluid. The present case showed overlapping macroscopic and histological features with the above-mentioned case. In fact, in proximity of the brown, nodular lesion that we diagnosed as hemangioma, a 10 cm cystic lesion, lined by a single layer of flattened to cuboidal cells identical to that seen on the outer surface of the cord was observed. On the basis of the clinical and histological findings, a diagnosis of hemangioma of the umbilical cord with amnionic epithelial inclusion cyst was made. To the best of our knowledge this is the second case in the literature which reports the unusual association between umbilical cord hemangioma and amnionic epithelial inclusion cyst. Differently from the case reported by Jacques et al. where these lesion lead to intrauterine fetal demise, in our case the child was born alive showing low birth weight and respiratory distress due to obstruction of blood flow from the umbilical cord. In conclusion we provide a detailed clinical morphological and immunohistochemical characterization of two extremely uncommon condition that presented simultaneously in the same patient: umbilical cord hemangioma and amnionic epithelial inclusion cyst. Further studies on larger cohorts are needed in order to establish their clinical significance as well as their etiopathogenetic correlation.
Figures and tables
Footnotes
CONFLICT OF INTEREST STATEMENT
None declared.
References
- 1.George A, Mani V, Noufal A. Update on the classification of hemangioma. J Oral Maxillofac Pathol 2014;18:117-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ghidini A, Romero R, Eisen RN, et al. Umbilical cord hemangioma. Prenatal identification and review of the literature. J Ultrasound Med 1990;9:297-300. [DOI] [PubMed] [Google Scholar]
- 3.Heifetz SA, Rueda-Pedraza ME. Hemangiomas of the umbilical cord. Pediatr Pathol 1983;1:385-98. [DOI] [PubMed] [Google Scholar]
- 4.Nguyen M, Addicott B, Chu J, et al. Congenital cyst of the umbilical cord. Fetal Pediatr Pathol 2016;5:1-4. [DOI] [PubMed] [Google Scholar]
- 5.Yavner DL, Redline RW. Angiomyxoma of the umbilical cord with massive cystic degeneration of Wharton’s jelly. Arch Pathol Lab Med 1989;113:935-7. [PubMed] [Google Scholar]
- 6.Jauniaux E, Moscoso G, Chitty L, et al. An angiomyxoma involving the whole length of the umbilical cord. Prenatal diagnosis by ultrasonography. J Ultrasound Med 1990;9:419-22. [DOI] [PubMed] [Google Scholar]
- 7.Wilson RD, Magee JF, Sorensen PH, et al. In utero decompression of umbilical cord angiomyxoma followed by vaginal delivery. Am J Obstet Gynecol 1994;171:1383-5. [DOI] [PubMed] [Google Scholar]
- 8.Søndergaard G. Hemangioma of the umbilical cord. Acta Obstet Gynecol Scand 1994;73:434-6. [DOI] [PubMed] [Google Scholar]
- 9.Tennstedt C, Chaoui R, Bollmann R, et al. Angiomyxoma of the umbilical cord in one twin with cystic degeneration of Wharton’s jelly. A case report. Pathol Res Pract 1998;194:55-8. [DOI] [PubMed] [Google Scholar]
- 10.Iyoob SD, Tsai A, Ruchelli ED, et al. Large umbilical cord hemangioma: sonographic features with surgical pathologic correlation. J Ultrasound Med 2006;25:1495-8. [DOI] [PubMed] [Google Scholar]
- 11.Daniel-Spiegel E, Weiner E, Gimburg G, et al. The association of umbilical cord hemangioma with fetal vascular birthmarks. Prenat Diagn 2005;25:300-3. [DOI] [PubMed] [Google Scholar]
- 12.Matsuda S, Sato Y, Marutsuka K, et al. Hemangioma of the umbilical cord with pseudocyst. Fetal Pediatr Pathol 2011;30:16-21. [DOI] [PubMed] [Google Scholar]
- 13.Jacques SM, Qureshi F. Hemangioma of the umbilical cord with amnionic epithelial inclusion cyst. Fetal Pediatr Pathol 2013; 32:235-9. [DOI] [PubMed] [Google Scholar]