

Key Points
Question
Does community health worker care reduce 30-day hospital readmissions in inpatient adults participating in accountable care organization plans?
Findings
In this randomized clinical trial including 550 adults, intervention patients were significantly less likely to experience 30-day hospital readmissions than control participants. In post hoc subgroup analysis, the effect remained significant for participants discharged to short-term rehabilitation but not for those discharged home.
Meaning
In this study, community health workercare improved postdischarge outcomes in clinically complex patients insured by accountable care organizations, particularly for those discharged to short-term rehabilitation.
This randomized clinical trial examines the effect of community health worker care on hospital readmissions within 30 days for adults enrolled in an accountable care organization.
Abstract
Importance
Value-based care within accountable care organizations (ACOs) has magnified the importance of reducing preventable hospital readmissions. Community health worker (CHW) interventions may address patients’ unmet psychosocial and clinical care needs but have been underused in inpatient and postdischarge care.
Objective
To determine if pairing hospitalized patients with ACO insurance with CHWs would reduce 30-day readmission rates.
Design, Setting, and Participants
This randomized clinical trial was conducted in 6 general medicine hospital units within 1 academic medical center in Boston, Massachusetts. Participants included adults hospitalized from April 1, 2017, through March 31, 2019, who had ACO insurance and were at risk for 30-day readmission based on a hospital readmission algorithm. The main inclusion criterion was frequency of prior nonelective hospitalizations (≥2 in the past 3 months or ≥3 in the 12 months prior to enrollment). Data were analyzed from February 1, 2018, through March 3, 2021.
Intervention
CHWs met with intervention participants prior to discharge and maintained contact for 30 days postdischarge to assist participants with clinical access and social resources via telephone calls, text messages, and field visits. CHWs additionally provided psychosocial support and health coaching, using motivational interviewing, goal-setting, and other behavioral strategies. The control group received usual care, which included routine care from primary care clinics and any outpatient referrals made by hospital case management or social work at the time of discharge.
Main Outcomes and Measures
The primary outcome was 30-day hospital readmissions. Secondary outcomes included 30-day missed primary care physician or specialty appointments.
Results
A total of 573 participants were enrolled, and 550 participants (mean [SD] age, 70.1 [15.7] years; 266 [48.4%] women) were included in analysis, with 277 participants randomized to the intervention group and 273 participants randomized to the control group. At baseline, participants had a mean (SD) of 3 (0.8) hospitalizations in the prior 12 months. There were 432 participants (78.5%) discharged home and 127 participants (23.1%) discharged to a short rehabilitation stay prior to returning home. Compared with participants in the control group, participants in the intervention group were less likely to be readmitted within 30 days (odds ratio [OR], 0.44; 95% CI, 0.28-0.90) and to miss clinic appointments within 30 days (OR, 0.56; 95% CI, 0.38-0.81). A post hoc subgroup analysis showed that compared with control participants, intervention participants discharged to rehabilitation had a reduction in readmissions (OR, 0.09; 95% CI, 0.03-0.31), but there was no significant reduction for those discharged home (OR, 0.68; 95% CI, 0.41-1.12).
Conclusions and Relevance
This randomized clinical trial found that pairing ACO-insured inpatient adults with CHWs reduced readmissions and missed outpatient visits 30 days postdischarge. The effect was significant for those discharged to short-term rehabilitation but not for those discharged home.
Trial Registration
ClinicalTrials.gov Identifier: NCT03085264
Introduction
Hospitalizations account for one-third of US health care costs.1,2 Readmissions in the first 30 days after hospital discharge are common, and approximately 27% of adult 30-day readmissions are estimated to be preventable.3 Increasing movement toward value-based care within accountable care organizations (ACOs) has magnified the importance of reducing preventable readmissions.4 Factors associated with hospital readmissions include medical complexity,5 clinical comorbidities,6,7 and social determinants of health.8,9,10 Many health care organizations have increasing interest in developing interventions within the ACO framework that address clinical care gaps and unmet social needs. Integration of community health workers (CHWs) is one of few interventions that have generated promising outcomes in terms of reducing hospitalizations and health care costs.11,12,13
CHWs are trained to have basic knowledge of clinical conditions and to provide health coaching using motivational interviewing and psychosocial support.14,15,16 CHWs also have expertise in social determinants of health and can assist patients with economic, health care access–associated, social, educational, and environmental resources to help close gaps in patient health care.17,18 Specifically, CHWs can augment patient engagement by strengthening patient connections to primary care and identifying relevant community-, state-, or federal-based patient resources to meet unmet patient needs (eg, food, housing, transportation).19,20
While most CHW studies have focused on specific disease-based cohorts,21,22,23,24,25,26 some randomized clinical trials have examined the effectiveness of using CHWs to improve postdischarge outcomes in adult inpatient and outpatient general medicine populations. In a study of 222 Medicaid inpatients randomized to a CHW intervention, Kangovi et al27 found that having at least one 30-day readmission did not differ between the intervention and control groups; however, there was a significant reduction in the number of intervention participants with 2 or more 30-day readmissions. In a randomized clinical trial of 1009 inpatients older than 60 years, Balaban et al28 found that CHW care reduced 30-day readmission rates in intervention participants compared with control participants. Another randomized clinical trial by Kangovi et al29 of 592 primary care outpatients tested a 6-month CHW intervention and demonstrated a reduced likelihood of readmission. Two other randomized clinical trials examining 6-month interventions with CHWs demonstrated no significant difference in hospitalizations.30,31
To determine the effect of CHW care delivery on 30-day readmissions within an ACO population, we conducted a randomized clinical trial to test a 30-day CHW intervention for patients admitted to the internal medicine service in an academic medical center in Boston, Massachusetts. The hypothesis was that CHW care delivery initiated in the hospital and extending for 30 days after discharge would reduce 30-day readmissions compared with usual care.
Methods
This randomized clinical trial was approved by the of Partners Human Research Committee (Trial Protocol in Supplement 1; eAppendix in Supplement 2). All enrolled patients provided written informed consent for study enrollment. This study is reported following the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline for randomized clinical trials.
Trial Design
The Community Care Transitions study was a randomized clinical trial was designed to improve health care outcomes for patients at high risk for readmission by pairing CHWs with inpatients for 30 days after discharge.32 CHW care delivery was implemented in partnership with clinical teams that were unaware of outcomes until trial completion. The CHWs addressed and integrated patient-identified needs (eg, food, housing, transportation) into the clinical care plans and used motivational interviewing and psychosocial support strategies to improve adherence to clinical care.
Setting and Participants
The study was conducted at Massachusetts General Hospital, a 999-bed teaching hospital in Boston, Massachusetts. Six internal medicine hospital units (or clinical wards) were used for trial recruitment. Each unit had similar percentages of 30-day readmissions with no differences in the diagnoses or ages of hospitalized patients.
Eligibility criteria were developed based on findings from 2 prior studies by Carter et al.33,34 Briefly, patients aged 18 years or older who were admitted to 1 of the study units were potentially eligible if they met the high-risk hospital criteria for 30-day readmission, with threshold of 16% or greater readmission risk. This was determined by a Massachusetts General Hospital–based 12-factor risk algorithm that included prior hospitalizations, fall risk, wound care needs, and frailty. After being identified by this algorithm, patients were evaluated by research staff for additional study inclusion criteria: prior history of 2 or more nonelective hospitalizations in the 3 months prior to enrollment or 3 or more nonelective hospitalizations in the 12 months prior to enrollment; participation in a hospital-based ACO benefit (Medicare, Medicaid, or private insurance); living within a 20-mile radius of the main hospital; having access to a working telephone; being fluent in English; having 1 or more unmet care-related needs identified during inpatient multidisciplinary rounds (eg, difficulties with medication management, appointment scheduling, access to transportation, or social support); and having a primary care physician (PCP). Patients were ineligible if they were experiencing homelessness, unable to provide consent owing to cognitive impairment, or had an invoked health care proxy or prisoner status (Figure 1). Patients with preexisting outpatient program support (ie, integrated care management services with telephonic nursing, social work, and clinical resource care coordination), home nursing, or other supportive programming (eg, physical therapy) were eligible for participation in the trial. Patients living in nursing homes or discharged to long-term care were excluded prior to randomization.
Figure 1. Participant Recruitment Flowchart.

CHW indicates community health worker.
Enrollment and Randomization
Patients were identified with a hospital-based database that generated a daily report of inpatients at high risk for readmission. Eligible patients were discussed at multidisciplinary rounds daily on each inpatient unit with CHW staff, case managers, unit nurses, bedside nurses, and physicians who reviewed the potential barriers to discharge. After confirming eligibility, research staff approached patients for enrollment. After providing consent and agreeing to enrollment, patients were randomized by study staff via block randomization using the team statistician’s preloaded Excel spreadsheet version 16.0 (Microsoft) block with 6 participants per block to either the intervention or the control group. To allow enough time for enrollment procedures, most participants had to be enrolled prior to finalization of their discharge plans; therefore, it was not feasible to preidentify which participants would be discharged to home or to a short-term rehabilitation facility.
Intervention Care
CHWs met with intervention participants and inpatient multidisciplinary teams prior to discharge to establish goals identified by patients and clinical teams. After discharge, CHWs delivered care using multiple communication strategies, including telephone calls, text messages, home visits, rehabilitation facility visits, and field visits (eg, accompanying patient for medical or social service encounters). CHWs provided health coaching, as well as assistance with obtaining any needed clinical access or social resources. CHWs were trained in CHW core competencies,19 consisting of motivational interviewing, goal-setting, behavior change, and psychosocial support.
Three CHWs delivered the study intervention, and all had experience working with or living in communities similar to those of participants. All CHWs received 1 month of protocol training led by the study CHW supervisor. CHW core competencies were emphasized during training and applied to case-based scenarios. CHWs documented all encounters in the electronic medical record (EMR) (eg, enrollment notes, progress notes for in-person visits and telephone calls); all patient and care team interactions were documented by CHWs in a REDCap database (Vanderbilt University). Each patient’s clinical team members were copied on all CHW EMR notes and contacted directly by CHWs during the intervention when needed. CHW staff also communicated directly with any practitioners of each patient’s outpatient primary care based–support, such as care management, nursing, or physical therapy, to streamline care delivery.
Usual Care
Usual care was defined as routine postdischarge care from the hospital discharge team. Any outpatient referrals made by hospital case management (eg, visiting nursing association, physical therapy, occupational therapy) or social work (eg, meal preparation, transportation, elder care services) at the time of discharge were also considered part of usual care.
Measures
Study participants completed an enrollment questionnaire adapted from a previous survey instrument.26 This survey instrument was derived from some standard established measures of patient experience for benchmarking as well as validated questions generated by prestudy qualitative interviews with patients and physicians. Questionnaire domains included health-related social needs (eg, food, housing, transportation), perceptions of their physical and mental health, confidence in their ability to care for themselves after discharge, satisfaction with inpatient care, perceived likelihood of readmission, understanding of the care plan, and ability to independently perform activities of daily living. Basic demographic characteristics, insurance status, primary diagnosis associated with admission, and major medical and psychiatric comorbidities were collected by EMR review. All participants were asked to complete a 30-day postdischarge questionnaire that included questions to assess perceived likelihood of 30-day readmission and confidence in caring for oneself outside the hospital.
Outcomes
The primary outcome was 30-day hospital readmission during the study period. Prespecified secondary outcomes were 30-day postdischarge missed outpatient physician appointments and emergency department (ED) visits. Outcomes were determined by the number of participants with 1 or more hospital admissions, ED visits (including ED observation stays but excluding ED visits resulting in hospitalization), or missed appointments during the 30 days after discharge from the index hospitalization. Automated email notifications of Partners Healthcare admissions and ED visits were generated by a hospital readmissions database and sent to study staff within 1 hour of occurrence. Hospital admissions were captured at Partners Healthcare–affiliated hospitals in Massachusetts (3 academic hospitals; 6 community hospitals) and New Hampshire (1 community hospital). Missed appointments were captured similarly by a hospital database and tabulated quarterly. Since the EMR was unable to capture encounters outside Partners Healthcare, participants were asked about clinical encounters during a 30-day postdischarge questionnaire. Owing to the nature of the intervention, patients and CHW staff were unable to be blinded to the study treatment arms. Study staff collecting EMR and patient-reported outcomes and performing data analysis were blinded. Clinical outcomes were adjudicated independently of the trial.
Power Calculation
For the power calculation, we assumed a readmission rate of 18% for usual care and a readmission rate of 13% with use of CHW care delivery, requiring a sample size of 1200 adults (600 intervention and 600 control) with more than 90% power to reject the null hypothesis that the readmission rate was greater than 13% using 1-sided binomial testing with 5% type I error. However, we were unable to enroll 1200 patients within the study funding timeline; therefore, recruitment was stopped prior to achieving the planned sample size.
Statistical Analysis
Demographic characteristics and baseline survey item responses were summarized between intervention and control groups. Bivariate analyses, using Pearson χ2 tests for categorical variables and t test for continuous variables, were performed to assess differences between binary clinical outcomes (30-day hospital readmission, missed appointments, ED visits) and study arms, as well as demographic characteristics and survey item responses. For every clinical outcome, a logistic regression model was applied to obtain unadjusted and adjusted odds ratios (ORs) to assess the intervention effect. Covariates adjusted for in the model included age, race/ethnicity, sex, number of hospitalizations, insurance, living alone status, and discharge disposition. Race/ethnicity was self-reported and collected as a potential confounder of readmissions, missed appointments, and ED visits. For 30-day patient experience outcomes, patient responses at admission and 30 days after discharge were compared, and a difference-in-differences analysis was performed. P values were 2-sided, and P < .05 was considered statistically significant. A separate univariate analysis was performed to identify types of CHW-patient contact along with categories of resources or care delivery administered. All analyses were performed using SAS statistical software version 9.4 (SAS Institute). Data were analyzed from February 1, 2018, through March 3, 2021.
Results
Patients were enrolled April 1, 2017, through March 31, 2019. A total of 1843 patients at high risk for readmission were screened, 1230 patients were deemed eligible, and 573 patients were randomized to the intervention (288 patients) or control (285 patients) groups (Figure 1). Six participants (1.0%), including 4 from the intervention group and 2 from the control group, withdrew from the study, and 17 participants (3.1%), including 7 from the intervention group and 10 from the control group, died prior to completing the study and were excluded. The remaining 550 participants were included in the final analyses, with 277 participants in the intervention group and 273 participants in the control group.
The mean age (SD) of participants was 70.1 (15.7) years, and 266 (48.4%) were women (Table 1). The most common insurance was Medicare (388 participants [70.5%]). All trial participants had a mean (SD) of 3 (0.8) hospitalizations in the 12 months prior to index hospitalization (Table 1). Overall, 67 participants (24.5%) in the control group and 60 participants (21.7%) in the intervention group were discharged to rehabilitation. The mean (SD) length of participant rehabilitation stay was 3.9 (1.1) days. Identified covariates were balanced in intervention and control groups.
Table 1. Patient Characteristics.
| Patient characteristics | No. (%) | |
|---|---|---|
| Control (n = 273) | Intervention (n = 277) | |
| Sex | ||
| Women | 119 (43.6) | 147 (53.1) |
| Men | 154 (56.4) | 130 (46.9) |
| Age, mean (SD), y | 69.7 (16.1) | 70.4 (15.3) |
| Race/ethnicity | ||
| Hispanic/Latino | 7 (2.6) | 9 (3.2) |
| White | 253 (92.7) | 241 (87.0) |
| Black | 10 (3.7) | 24 (8.7) |
| Asian | 3 (1.1) | 2 (0.7) |
| Othera | 0 (0.0) | 1 (0.4) |
| ≤High school education | 123 (45.1) | 140 (50.5) |
| Primary insurance | ||
| Medicare | 191 (70.0) | 197 (71.1) |
| Medicaid or MassHealth | 34 (12.5) | 30 (10.8) |
| Commercial or private | 48 (17.6) | 50 (18.1) |
| Preexisting services | ||
| Comprehensive case management | 113 (41.4) | 119 (43.0) |
| Clinical nursing or home services | 76 (27.8) | 70 (25.3) |
| Social determinants | ||
| Lives alone | 90 (33.0) | 94 (33.9) |
| Housing quality problems (eg, leaks, poor heat/cooling, insects) | 27 (10.0) | 21 (7.6) |
| Had trouble paying in the last 12 mo | ||
| Medical bills | 24 (8.8) | 29 (10.5) |
| Prescription drugs | 36 (13.2) | 40 (14.4) |
| Medical equipment or supplies | 10 (3.7) | 22 (7.9) |
| Health care services at home | 10 (3.7) | 10 (3.6) |
| Food | 39 (14.3) | 46 (16.6) |
| Clothing | 33 (12.1) | 38 (13.7) |
| Rent, mortgage, or housing costs | 27 (9.9) | 36 (13.0) |
| Inability performing ≥2 ADL independently | 121 (44.3) | 137 (49.5) |
| Healthcare utilization | ||
| No. of hospitalizations within 12 mo, mean (SD) | 3.0 (0.7) | 3.1 (0.9) |
| Primary reason hospitalization | ||
| Infectious disease | 78 (28.6) | 63 (22.7) |
| Gastroenterology condition | 47 (17.2) | 60 (21.7) |
| Cardiac | 58 (21.2) | 62 (22.4) |
| Respiratory condition | 24 (8.8) | 24 (8.7) |
| Fall or trauma | 21 (7.7) | 11 (4.0) |
| Other | 45 (16.5) | 57 (20.6) |
| Disposition at discharge | ||
| Home | 206 (75.5) | 217 (78.3) |
| Rehabilitation | 67 (24.5) | 60 (21.7) |
Abbreviation: ADL, activities of daily living.
Includes American Indian/Alaska Native, Asian, Native Hawaiian or other Pacific Islander, unknown or not reported, and other.
Overall, compared with the control group, fewer participants in the intervention group were readmitted in the 30 days after hospital discharge (67 participants [24.5%] vs 35 participants [12.6%]; OR, 0.44; 95% CI, 0.28-0.90; P < .001) (Figure 2A). In a post hoc subgroup analysis of this cohort (eTable 2 in Supplement 2), we found that intervention participants discharged to rehabilitation demonstrated a reduction of 32.3 percentage points in readmissions compared with control participants (3 participants [5.0%] vs 25 participants [37.3%]; OR, 0.09; 95% CI, 0.03-0.31; P < .001) (Figure 2B), but the difference observed in intervention vs control participants discharged home was not statistically significant (32 participants [14.7%] vs 42 participants [20.4%]; OR, 0.68; 95% CI, 0.41-1.12; P = .13) (Figure 2C). A total of 4 readmissions occurred outside the hospital system and were identified by the patient questionnaire.
Figure 2. Postdischarge Outcomes at 30 Days for Participants Paired With Community Health Workers vs Usual Care .
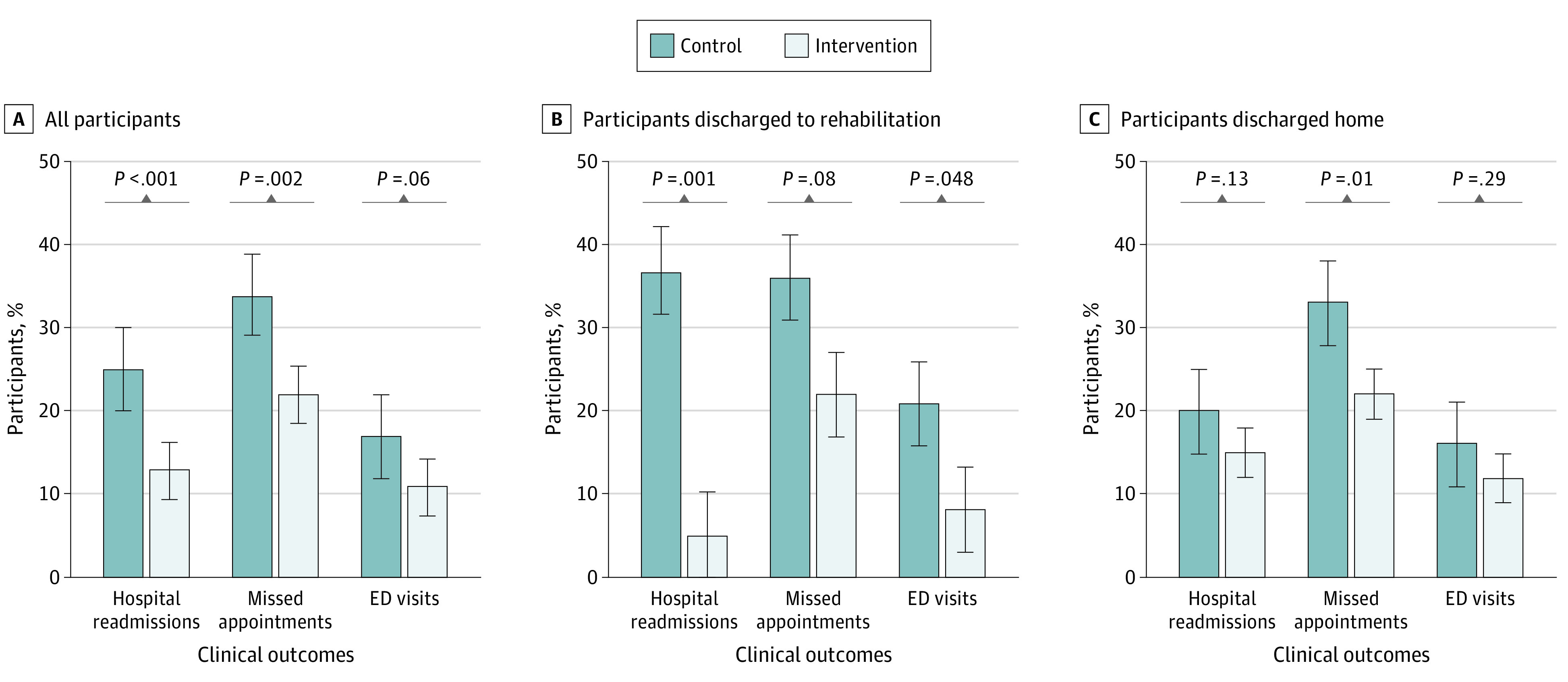
Adjusted for age, race/ethnicity, sex, number of hospitalizations, insurance, and living alone; discharge disposition was also applied for panel A only. ED indicates emergency department; error bars, 95% CI.
Fewer intervention than control participants had missed appointments (61 participants [22.0%] vs 92 participants [33.7%]; OR, 0.56; 95% CI, 0.38-0.81; P = .002), but the difference in ED visits was not statistically significant (31 participants [11.2%] vs 46 participants [16.8%]; OR, 0.62; 95% CI, 0.38-1.02; P = .06) (Figure 2A). Similar effects were observed in the subgroup analysis among intervention vs control participants discharged to rehabilitation (missed appointments: 13 participants [21.7%] vs 24 participants [35.8%]; OR, 0.5; 95% CI, 0.22-1.09; P = .08; ED visits: 5 participants [8.3%] vs 14 participants [20.9%]; OR = 0.34; 95% CI, 0.12-1.02; P = .05) (Figure 2B) or to home (missed appointments: 48 participants [22.1%] vs 68 participants [33.0%]; OR, = 0.58; 95% CI, 0.37-0.89; P = .01; ED visits: 26 participants [12.0%] vs 32 participants [15.5%]; OR, 0.74; 95% CI, 0.42-1.29; P = .30) (Figure 2C). In multivariate analyses of all participants controlling for demographic and clinical covariates (ie, age, race/ethnicity, sex, number of hospitalizations, insurance, living alone status, and discharge to home vs rehabilitation), the adjusted ORs for clinical outcomes in intervention vs control participants were similar to the unadjusted ORs (30-day hospital readmissions: adjusted OR, 0.45; 95% CI, 0.29-0.72; missed appointments: adjusted OR, 0.56; 95% CI, 0.38-0.82; ED visits: adjusted OR, 0.62; 95% CI, 0.38-1.02) (eTable 1 in the Supplement). A similar analysis was performed for participants discharged home and to short-stay rehabilitation (eTable 3 and eTable 4 in the Supplement).
More than 80% of all participants indicated they were very or somewhat confident in caring for themselves at the time of enrollment, including 234 participants (84.5%) in the intervention group and 240 participants (87.9%) in the control group, and this did not change in their poststudy questionnaire (Table 2). Intervention participants demonstrated a decrease in their perceived likelihood of 30-day readmission in the poststudy questionnaire compared with the enrollment questionnaire (24 participants [12.5%] vs 53 participants [19.1%]; P = .04); this difference was not statistically different from the control group.
Table 2. Patient-Reported Experience Outcomes at 30 Days.
| Outcome | No. | No. (%) | Difference, percentage points | P value | Difference in differences, % | P value | ||
|---|---|---|---|---|---|---|---|---|
| Admission | Poststudy | |||||||
| Confident in caring for self (very/somewhat) | ||||||||
| Intervention | 192 | 234 (84.5) | 159 (82.8) | 1.7 | .43 | 1.0 | .84 | |
| Control | 196 | 240 (87.9) | 167 (85.2) | 2.7 | .32 | |||
| Likelihood of 30-d readmission (very/somewhat) | ||||||||
| Intervention | 192 | 53 (19.1) | 24 (12.5) | 6.6 | .04 | 2.9 | .38 | |
| Control | 196 | 56 (20.5) | 33 (16.8) | 3.7 | .26 | |||
Intervention participants had a mean (SD) of 3.2 (2.4) contacts with CHWs after hospital discharge during the 30-day study period. Of 277 intervention participants, 247 (88.9%) communicated with CHW staff during at least 1 phone call. In addition, 198 participants (71.4%) in the intervention group received at least 1 home, rehabilitation, or field visit during the study interval (Table 3). CHWs completed different types of interactions focused on medical, social, or basic needs and coaching or education. CHWs most commonly provided participants with counseling to reinforce adherence to their clinical care plans (239 participants [86.3%]) and with psychosocial support (229 participants [82.7%]). Other CHW-patient activities ranged widely across supportive clinical and social domains (Table 3), including making and confirming clinical appointments (128 participants [46.2%]), assistance with securing basic needs like food or housing (108 participants [39.1%]), helping with access to medications (97 participants [35.0%]), creating plans for reliable transportation (91 participants [32.9%]), initiating elder care services (80 participants [28.9%]), engaging case management support (76 participants [27.4%]), and assisting with completing insurance forms or obtaining benefits (75 participants [27.0%]).
Table 3. Types of CHW-Patient Contacts and Activities for Intervention Participants.
| Activity | No. (%) |
|---|---|
| Contacts | |
| Phone visit with patient or caregiver | 247 (89.2) |
| Direct patient contact | 198 (71.4) |
| Home visit | 139 (50.1) |
| Rehabilitation facility visit | 31 (11.1) |
| Field visit (clinical or social support appointment) | 28 (10.1) |
| Activities | |
| Medical needs | |
| Reinforcement of general adherence to care plans and medication | 239 (86.3) |
| Making or confirming clinical appointments | 128 (46.2) |
| Direct interaction with clinical care team member | 111 (40.1) |
| Arranging for access to medications (delivery or transportation) | 97 (35.0) |
| Engaging case management support | 76 (27.4) |
| Completion of forms associated with unmet insurance needs | 75 (27.0) |
| Social or basic needs | |
| Securing basic needs (eg, housing, food, electricity) | 108 (39.1) |
| Creating a reliable transportation plan | 91 (32.9) |
| Referral to a social service agency or program | 85 (30.7) |
| Referral to elder services | 80 (28.9) |
| Coaching or teaching | |
| Providing psychosocial support | 229 (82.7) |
| Organization and reconciliation (eg, calendar events, mail, bills) | 87 (31.4) |
| Nutrition and general health | 39 (14.1) |
Abbreviation: CHW, community health worker.
Discussion
In this randomized clinical trial at 1 academic medical center, a CHW intervention reduced 30-day hospital readmissions in adult general medicine inpatients by nearly 50%. However, subgroup analyses revealed that most of the effect occurred for participants initially discharged to short-term rehabilitation. Intervention participants also were less likely to miss clinic appointments, but no significant reductions in ED visits were noted. These results indicate that CHW interventions may help reduce hospital readmissions and improve preventive care among some clinically complex patients within an ACO.
A subgroup analysis of participants who were discharged directly home compared with those discharged to short-term rehabilitation before going home demonstrated that the CHW intervention effect on 30-day readmissions was large for participants who went to rehabilitation. Prior studies have shown that deconditioned patients with complex comorbidities who are discharged to rehabilitation facilities have elevated rates of readmission, ranging from 28% to 75%.35,36 The findings of our study suggest that CHWs had a significant effect on preventing readmissions during or after short rehabilitation stays. Potential reasons for this effect may be that CHWs addressed unmet medical and social needs that occurred during the transition from rehabilitation to home and that CHWs improved communication among the patient, rehabilitation staff, and primary physician prior to return to home. While inpatients discharged to rehabilitation prior to transitioning home have been identified as high-risk for 30-day readmission, little research has been done to determine effective interventions to reduce readmissions. Results from our post hoc analyses demonstrated that CHWs are a promising intervention for this population, but future studies are needed to confirm these findings.
Most CHW-focused trials have not demonstrated significant reductions in hospital readmissions. However, a 2020 pooled analysis of 3 CHW randomized clinical trials37 found a combined significance in reduced hospital readmissions. The Community Care Transitions intervention used in this study differed from prior studies in that all participants were affiliated with a hospital ACO insurance benefit and had a PCP, a working phone number, and a residential address within a specific radius. Preexisting participant connections to primary care and the ACO network were essential for effective communication between CHWs and clinical teams and for assisting participants with access to postdischarge care. This was key to CHWs connecting participants with resources and programs when they needed them. As in most prior published trials, CHWs in our study received unique training focused on reaching patients after discharge and identifying resources for patient health-related social needs. Each of these elements likely contributed to improved clinical outcomes.
The results of this randomized clinical trial also emphasized that even in an ACO where there are more resources than in prior published CHW-intervention focused trials, readmission rates for control participants were relatively high. Although an equal proportion of intervention and control participants were enrolled in comprehensive case management or nursing programs as a part of usual care in an ACO, adding CHW care significantly reduced readmission rates. This difference highlights CHW capacity to address gaps in care related to unmet psychosocial needs (eg, securing meal delivery, transportation, access to medications, elder care services, accompaniment to clinic visits). CHWs can add value to the ACO model in a large health care organization by better connecting patients to community resources and programs as well as primary and subspecialty clinical homes.
Overall, there was a reduction of more than 30 percentage points in missed appointments among intervention participants 30 days after discharge compared with control participants. This effect was sustained in the subgroup analysis for participants discharged to rehabilitation and home. This difference has been demonstrated in prior care transitions studies38,39 and underlines the efficacy of CHWs in improving postdischarge follow-up. Baseline and postintervention period surveys demonstrated a reduction in perceived likelihood of hospital readmission for intervention participants, although this reduction was not statistically significantly different from the control group. This suggests that CHWs may promote increased competence, knowledge, and engagement influencing perceptions about readmission.40,41
The most frequent CHW activities were psychosocial support and reinforcement of adherence to care plans. These activities were similar to those described in studies by Kangovi et al21 and Wells et al,23 but most studies to date have not established a standard of care for CHW interventions, making direct comparisons between studies challenging. This represents an area of opportunity to more completely categorize and describe CHW outreach as part of an evidence base.42,43,44,45
Limitations
This study has limitations. Despite use of validated self-reported measures of health care utilization in our 30-day postdischarge survey, we may not have identified all encounters occurring outside our hospital system. However, the fact that all participants were within the ACO network helped ensure that enrolled participants received most, if not all, of their care within designated ACO coverage. Also, healthy user bias, with patients who were the most ill being unable to enroll, may have resulted in underrepresentation of patients with even higher rates of medical complexity. While we considered individuals discharged to rehabilitation to be a legitimate group to study, study participants were enrolled and randomized while hospitalized, and it was not possible to determine who was going to rehabilitation vs home until the time of discharge. Therefore, we were unable to stratify on this characteristic at the time of randomization. Approximately 32% of 1280 patients identified as eligible for the study were unable to be enrolled owing to being busy with clinical care or discharged prior to meeting with study staff. In the future, this could be addressed by having CHWs contact patients via phone after discharge. We were unable to enroll non–English-speaking participants because of limited funding for bilingual study materials and staff. The study was conducted at a single urban hospital and enrolled ACO-insured inpatients with a working telephone and who lived within a 20-mile hospital radius. Therefore, study findings may not be generalizable to patients who have non-ACO health insurance, are uninsured, do not speak English, do not have a working telephone, or live in rural settings.
Conclusions
This randomized clinical trial found that integration of CHWs into clinical care improved preventive care and reduced 30-day readmissions for patients discharged to rehabilitation. Reducing preventable readmissions is a central priority for the Centers for Medicare & Medicaid Services and principal health care stakeholders. As US health care organizations continue to adopt ACO models with the goal of achieving higher quality care at lower costs, policies supporting insurance-based reimbursement for CHW care and investment in comprehensive training and integration of CHWs as valued members of patient care teams will continue to be critical.46 Future research is needed to identify which patients benefit most from certain CHW intervention activities.
Trial Protocol
eAppendix. Summary of IRB Protocol Changes
eTable 1. Adjusted and Unadjusted Analysis for Clinical Outcomes of All Intervention and Control Participants
eTable 2. Discharge Disposition Subgroup Analysis With Clinical Outcomes for Intervention and Control Participants Discharged to Rehabilitation vs Home
eTable 3. Adjusted and Unadjusted Analysis for Clinical Outcomes of 127 Participants Discharged to Short-Stay Rehabilitation Prior to Home
eTable 4. Adjusted and Unadjusted Analysis for Clinical Outcomes of 423 Participants Discharged Home
Data Sharing Statement
References
- 1.Centers for Medicare & Medicaid Services . National Health Expenditure Data. Accessed December 18, 2017. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData
- 2.Freeman WJ, Weiss AJ, Heslin KC. Overview of U.S. hospital stays in 2016: variation by geographic region: statistical brief #246. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality; 2018. [PubMed] [Google Scholar]
- 3.Auerbach AD, Kripalani S, Vasilevskis EE, et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176(4):484-493. doi: 10.1001/jamainternmed.2015.7863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McWilliams JM, Hatfield LA, Landon BE, Hamed P, Chernew ME. Medicare spending after 3 years of the Medicare shared savings program. N Engl J Med. 2018;379(12):1139-1149. doi: 10.1056/NEJMsa1803388 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hannan EL, Racz MJ, Walford G, et al. Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 2003;290(6):773-780. doi: 10.1001/jama.290.6.773 [DOI] [PubMed] [Google Scholar]
- 6.Aujesky D, Mor MK, Geng M, Stone RA, Fine MJ, Ibrahim SA. Predictors of early hospital readmission after acute pulmonary embolism. Arch Intern Med. 2009;169(3):287-293. doi: 10.1001/archinternmed.2008.546 [DOI] [PubMed] [Google Scholar]
- 7.Harjai KJ, Thompson HW, Turgut T, Shah M. Simple clinical variables are markers of the propensity for readmission in patients hospitalized with heart failure. Am J Cardiol. 2001;87(2):234-237, A9. doi: 10.1016/S0002-9149(00)01328-X [DOI] [PubMed] [Google Scholar]
- 8.Calvillo-King L, Arnold D, Eubank KJ, et al. Impact of social factors on risk of readmission or mortality in pneumonia and heart failure: systematic review. J Gen Intern Med. 2013;28(2):269-282. doi: 10.1007/s11606-012-2235-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5):778-785. doi: 10.1377/hlthaff.2013.0816 [DOI] [PubMed] [Google Scholar]
- 10.Goldfield NI, McCullough EC, Hughes JS, et al. Identifying potentially preventable readmissions. Health Care Financ Rev. 2008;30(1):75-91. [PMC free article] [PubMed] [Google Scholar]
- 11.Jack HE, Arabadjis SD, Sun L, Sullivan EE, Phillips RS. Impact of community health workers on use of healthcare services in the United States: a systematic review. J Gen Intern Med. 2017;32(3):325-344. doi: 10.1007/s11606-016-3922-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.We analyzed 25 population health interventions—and these 2 give the best ‘bang for your buck.’ Advisory Board. March 22, 2018. Accessed July 19, 2018. https://www.advisory.com/blog/2018/03/population-health-interventions
- 13.Kangovi S, Mitra N, Grande D, Long JA, Asch DA. Evidence-based community health worker program addresses unmet social needs and generates positive return on investment. Health Aff (Millwood). 2020;39(2):207-213. doi: 10.1377/hlthaff.2019.00981 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.American Public Health Association . Support for community health worker leadership in determining workforce standards for training and credentialing. Accessed July 19, 2018. https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2015/01/28/14/15/support-for-community-health-worker-leadership
- 15.Lohr AM, Ingram M, Nuñez AV, Reinschmidt KM, Carvajal SC. Community-clinical linkages with community health workers in the United States: a scoping review. Health Promot Pract. 2018;19(3):349-360. doi: 10.1177/1524839918754868 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Malcarney M-B, Pittman P, Quigley L, Horton K, Seiler N. The changing roles of community health workers. Health Serv Res. 2017;52(suppl 1):360-382. doi: 10.1111/1475-6773.12657 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.The Rural Health Information Hub, Health Resources and Services Administration . Community Health Workers Toolkit. Accessed July 20, 2018. https://www.ruralhealthinfo.org/toolkits/community-health-workers
- 18.Balcazar H, Rosenthal EL, Brownstein JN, Rush CH, Matos S, Hernandez L. Community health workers can be a public health force for change in the United States: three actions for a new paradigm. Am J Public Health. 2011;101(12):2199-2203. doi: 10.2105/AJPH.2011.300386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Commonwealth of Massachusetts . Core Competencies for Community Health Workers. Revised May 2014. Accessed July 19, 2018. https://www.mass.gov/service-details/core-competencies-for-community-health-workers
- 20.Reinschmidt KM, Ingram M, Morales S, et al. Documenting community health worker roles in primary care: contributions to evidence-based integration into health care teams, 2015. J Ambul Care Manage. 2017;40(4):305-315. doi: 10.1097/JAC.0000000000000178 [DOI] [PubMed] [Google Scholar]
- 21.Brownstein JN, Chowdhury FM, Norris SL, et al. Effectiveness of community health workers in the care of people with hypertension. Am J Prev Med. 2007;32(5):435-447. doi: 10.1016/j.amepre.2007.01.011 [DOI] [PubMed] [Google Scholar]
- 22.Rothschild SK, Martin MA, Swider SM, et al. Mexican American trial of community health workers: a randomized controlled trial of a community health worker intervention for Mexican Americans with type 2 diabetes mellitus. Am J Public Health. 2014;104(8):1540-1548. doi: 10.2105/AJPH.2013.301439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wells KJ, Luque JS, Miladinovic B, et al. Do community health worker interventions improve rates of screening mammography in the United States: a systematic review. Cancer Epidemiol Biomarkers Prev. 2011;20(8):1580-1598. doi: 10.1158/1055-9965.EPI-11-0276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Percac-Lima S, Grant RW, Green AR, et al. A culturally tailored navigator program for colorectal cancer screening in a community health center: a randomized, controlled trial. J Gen Intern Med. 2009;24(2):211-217. doi: 10.1007/s11606-008-0864-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Krieger JW, Takaro TK, Song L, Weaver M. The Seattle-King County Healthy Homes Project: a randomized, controlled trial of a community health worker intervention to decrease exposure to indoor asthma triggers. Am J Public Health. 2005;95(4):652-659. doi: 10.2105/AJPH.2004.042994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Venditti EM, Zgibor JC, Vander Bilt J, et al. Mobility and Vitality Lifestyle Program (MOVE UP): a community health worker intervention for older adults with obesity to improve weight, health, and physical function. Innov Aging. 2018;2(2):igy012. doi: 10.1093/geroni/igy012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kangovi S, Mitra N, Grande D, et al. Patient-centered community health worker intervention to improve posthospital outcomes: a randomized clinical trial. JAMA Intern Med. 2014;174(4):535-543. doi: 10.1001/jamainternmed.2013.14327 [DOI] [PubMed] [Google Scholar]
- 28.Balaban RB, Galbraith AA, Burns ME, Vialle-Valentin CE, Larochelle MR, Ross-Degnan D. A patient navigator intervention to reduce hospital readmissions among high-risk safety-net patients: a randomized controlled trial. J Gen Intern Med. 2015;30(7):907-915. doi: 10.1007/s11606-015-3185-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kangovi S, Mitra N, Norton L, et al. Effect of community health worker support on clinical outcomes of low-income patients across primary care facilities: a randomized clinical trial. JAMA Intern Med. 2018;178(12):1635-1643. doi: 10.1001/jamainternmed.2018.4630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kangovi S, Mitra N, Grande D, Huo H, Smith RA, Long JA. Community health worker support for disadvantaged patients with multiple chronic diseases: a randomized clinical trial. Am J Public Health. 2017;107(10):1660-1667. doi: 10.2105/AJPH.2017.303985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Finkelstein A, Zhou A, Taubman S, Doyle J. Health care hotspotting—a randomized controlled trial. N Engl J Med. 2020;382(2):152-162. doi: 10.1056/NEJMsa1906848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Carter J, Walton A, Donelan K, Thorndike A. Implementing community health worker-patient pairings at the time of hospital discharge: a randomized control trial. Contemp Clin Trials. 2018;74:32-37. doi: 10.1016/j.cct.2018.09.013 [DOI] [PubMed] [Google Scholar]
- 33.Carter J, Ward C, Wexler D, Donelan K. The association between patient experience factors and likelihood of 30-day readmission: a prospective cohort study. BMJ Qual Saf. 2018;27(9):683-690. doi: 10.1136/bmjqs-2017-007184 [DOI] [PubMed] [Google Scholar]
- 34.Carter J, Ward C, Thorndike A, Donelan K, Wexler DJ. Social Factors and Patient Perceptions Associated With Preventable Hospital Readmissions. J Patient Exp. 2020;7(1):19-26. doi: 10.1177/2374373518825143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fisher SR, Graham JE, Krishnan S, Ottenbacher KJ. Predictors of 30-day readmission following inpatient rehabilitation for patients at high risk for hospital readmission. Phys Ther. 2016;96(1):62-70. doi: 10.2522/ptj.20150034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ottenbacher KJ, Karmarkar A, Graham JE, et al. Thirty-day hospital readmission following discharge from postacute rehabilitation in fee-for-service Medicare patients. JAMA. 2014;311(6):604-614. doi: 10.1001/jama.2014.8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Vasan A, Morgan JW, Mitra N, et al. Effects of a standardized community health worker intervention on hospitalization among disadvantaged patients with multiple chronic conditions: a pooled analysis of three clinical trials. Health Serv Res. 2020;55(suppl 2):894-901. doi: 10.1111/1475-6773.13321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nuti LA, Lawley M, Turkcan A, et al. No-shows to primary care appointments: subsequent acute care utilization among diabetic patients. BMC Health Serv Res. 2012;12(1):304. doi: 10.1186/1472-6963-12-304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ellis DA, McQueenie R, McConnachie A, Wilson P, Williamson AE. Demographic and practice factors predicting repeated non-attendance in primary care: a national retrospective cohort analysis. Lancet Public Health. 2017;2(12):e551-e559. doi: 10.1016/S2468-2667(17)30217-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gimpel N, Marcee A, Kennedy K, Walton J, Lee S, DeHaven MJ. Patient perceptions of a community-based care coordination system. Health Promot Pract. 2010;11(2):173-181. doi: 10.1177/1524839908320360 [DOI] [PubMed] [Google Scholar]
- 41.Brooks BA, Davis S, Frank-Lightfoot L, Kulbok PA, Poree S, Sgarlata L. Building a Community Health Worker Program: The Key to Better Care, Better Outcomes, & Lower Costs. CommunityHealth Works; 2018. [Google Scholar]
- 42.Covert H, Sherman M, Miner K, Lichtveld M. Core competencies and a workforce framework for community health workers: a model for advancing the profession. Am J Public Health. 2019;109(2):320-327. doi: 10.2105/AJPH.2018.304737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Rosenthal EL, Rush CH, Allen C. Understanding scope and competencies: a contemporary look at the United States community health worker field: progress report of the Community Health Worker (CHW) Core Consensus Project. Accessed October 5, 2020. https://sph.uth.edu/dotAsset/28044e61-fb10-41a2-bf3b-07efa4fe56ae.pdf
- 44.Ingram M, Reinschmidt KM, Schachter KA, et al. Establishing a professional profile of community health workers: results from a national study of roles, activities and training. J Community Health. 2012;37(2):529-537. doi: 10.1007/s10900-011-9475-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Arvey SR, Fernandez ME. Identifying the core elements of effective community health worker programs: a research agenda. Am J Public Health. 2012;102(9):1633-1637. doi: 10.2105/AJPH.2012.300649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lapidos A, Lapedis J, Heisler M. Realizing the value of community health workers—new opportunities for sustainable financing. N Engl J Med. 2019;380(21):1990-1992. doi: 10.1056/NEJMp1815382 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eAppendix. Summary of IRB Protocol Changes
eTable 1. Adjusted and Unadjusted Analysis for Clinical Outcomes of All Intervention and Control Participants
eTable 2. Discharge Disposition Subgroup Analysis With Clinical Outcomes for Intervention and Control Participants Discharged to Rehabilitation vs Home
eTable 3. Adjusted and Unadjusted Analysis for Clinical Outcomes of 127 Participants Discharged to Short-Stay Rehabilitation Prior to Home
eTable 4. Adjusted and Unadjusted Analysis for Clinical Outcomes of 423 Participants Discharged Home
Data Sharing Statement