

Abstract
Introduction:
Maternal birthing positions refer to the various physical postures a pregnant mother may assume at the time of delivery. The World Health Organisation recommends that woman should be given an opportunity to make a choice on the type of position to use during labour. Alternative birth positions are associated with lower incidence rates of performing episiotomy, less perineal tears and less use of instrumental deliveries. Nurses' perspective on women's positions has rarely been explored in India. Present study aims at assessing the knowledge regarding alternative birth positions among nursing officers.
Materials and Methods:
This cross-sectional observational study was conducted on 52 nursing officers who were posted in the labour room. A pretested questionnaire was administered to them. Data analysis was done using SPSS software version 22.
Results:
Majority (82.7%) of nursing officers felt that there is a need of giving a choice to the woman regarding alternate birth position. 76.9% of them were aware of position other than lithotomy. Around 48.1% would recommend squatting position to a woman in labour. Ease and convenience in conducting the delivery was the foremost reason chosen in advocating a birth position. Whereas overcrowding in the labour room, ignorance about alternate positions and difficulty in converting to instrumental delivery were cited as reasons of not recommending these positions.
Conclusion:
Educating nursing officers about emerging evidence regarding birthing positions will enable them to give accurate information to women.
Keywords: Birthing position, knowledge, maternal choice, nursing officer, respectful maternity care
Introduction
Pregnancy and childbirth are the major events in the lives of women and their families. It also represents a time of intense vulnerability. The notion of safe motherhood is expanded beyond the prevention of morbidity and mortality. Respectful maternity care (RMC) is a universal right of the pregnant woman. RMC can be defined as an approach to care that emphasizes the fundamental rights of women, newborn and families, and that promotes equitable access to evidence-based care while recognizing the unique needs and preferences of both women and newborn.[1]
Maternal birthing positions refer to the various physical postures a pregnant mother may assume at the time of delivery. Other than the traditional lithotomy position, there are several alternate birthing positions that have been successfully used by midwives all over the world. Categorically, upright positions usually include: Sitting, kneeling, hands-and-knees/all-fours, squatting and standing; whereas horizontal positions usually include recumbent and/or semi-recumbent and/or lithotomy.[2] There are several documented advantages for being upright during labour and birth. These include the effect of gravity on the fetus within the uterus; reduced risk of aorto-caval compression; better alignment of the fetus; more efficient contractions and increased pelvic outlet when the woman is in squatting and kneeling positions.[3]
The World Health Organization recommends that woman should be given an opportunity to make a choice on the type of position to use during labour.[4] Women should be encouraged to adopt positions in which they are comfortable.[5] It contributes to a positive birth experience, which will aid further to a woman's sense of accomplishment, self-esteem, feelings of competence and wellbeing.[6] Alternative birth positions are associated with lower incidence rates of performing episiotomy, less perineal tears and less use of instrumental deliveries.[7,8]
In countries where midwives are the primary care givers for antenatal, childbirth and post natal services, their role is well defined and complimentary to the recent guidelines. Midwifery led care is based on the principles of dignity, privacy and compassion for women and respectful maternal care.[9]
In various studies it was observed that the advice given by midwives was the most important factor influencing the choice of birthing positions.[10,11] The decisions midwives make while supporting and caring for a woman are highly significant and influence a variety of childbirth outcomes.[12]
India is one of the few countries where midwives are not independent service providers. Training in midwifery is part of the curriculum for nursing, provided to registered nurses and registered midwife (RNRM) and auxiliary nurse- midwife (ANMs). The general nurse-midwife (GNM) provides nursing services in a range of public facilities from primary to tertiary care and also at private health facilities. Their duties range from nursing care to the sick and in emergency cases, dispensing of medicines, maintenance of data and stocks in the ward, communication with relatives etc. With so many tasks assigned to the GNM, providing midwifery services becomes challenging.
Nurses play a pivotal role in widening the range of women's choices. As the influence of the nurses is so crucial, it is important to find out what nurses think about this aspect of care. Nurses' views on women's positions have rarely been explored in India. Present study aims at assessing the knowledge regarding alternative birth positions among nursing officers.
Materials and Methods
This cross sectional observational study was conducted in the nursing officers who were posted in the labour room of selected Government hospitals of Nagpur, Maharashtra in the month of February and –March 2020. Ethical approval was obtained from the Institute Ethics Committee (IEC/Pharmac/18/2019). Verbal consent was obtained from all the participants, ensuring confidentiality and anonymity of collected information. A pretested questionnaire was administered by trained Obstetricians and it included questions pertaining to the knowledge of staff nurses on alternative birth positions. The questionnaire was submitted to five experts comprising of two professionals in the field of Nursing, two experts in Gynecology and one statistician for establishing content validity and was pretested over a group of ten nursing staff.
There is no literature available on knowledge regarding alternative birth positions among staff nurses in India. However, a few studies which were done outside India had a sample size ranging from 20 to 30 amongst midwives who met the inclusion criteria.[8] At the time of this study, about 70 staff nurses were working in the labour room of Government Institutes of Nagpur amongst which 52 were approached for the study on the basis of convenience sampling. The data collected was entered in a spread sheet and analysis was done using Statistical Package for Social Sciences (SPSS) software version 22.
Results
None of the nursing officers declined to participate and thus a 100% response rate was achieved.
Baseline characteristics
Table 1 shows the baseline characteristics, including demographic details of the study population. A total of 52 participants completely filled the questionnaire and were analyzed. The age of the nursing officers who participated in the study ranged from 22 to 57 years. The mean age of the study participants was 36.6 ± 8.8 years.
Table 1.
Demographic Profile of the study Participants
| Characteristics | Sample population n=52 (%) |
|---|---|
| Age Group (Years) | |
| <25 | 4 (7.69%) |
| 25-39 | 24 (46.15%) |
| 40-54 | 18 (34.61%) |
| ≥55 | 6 (11.53%) |
| Education Level | |
| GNM | 40 (76.92%) |
| BSc. | 11 (21.15%) |
| MSc. | 01 (1.92%) |
| Years of experience (Years) | |
| 1-2 | 1 (1.92%) |
| >2-5 | 10 (19.23%) |
| >5 | 41 (78.84%) |
| Labour room work experience (Years) | |
| <1 | 12 (23.07%) |
| 1-2 | 21 (40.38%) |
| 2-5 | 19 (36.53%) |
GNM - General nursing and midwifery; BSc - Bachelor of science; MSc - Masters in Science
For the majority (76.9%) of the participants, the highest level of educational qualification was General Nursing and Midwifery (GNM). The nursing staff had an average of 14.7 years of experience. Around 76.9% of the participants had more than 1 year of experience of working in the labour room.
Attitude for respectful maternity care
Almost all the participants (n = 51, 98.1%) believed that respectful maternity care is a universal human right. Around 51.9% of the study participants were aware of the WHO recommendations of adoption of birth position as every individual antenatal woman's choice. The majority (82.7%) felt that there is a need of giving a choice to the woman regarding alternate birth position [Table 2].
Table 2.
Awareness regarding the basic knowledge for maternity care
| Characteristics | Sample Population n (%) |
|---|---|
| Respectful maternity care is a universal human right? | |
| Yes | 51 (98.07%) |
| No | 01 (1.92%) |
| Are you aware of WHO recommendation of adoption of a birth position of the individual antenatal woman’s choice? | |
| Yes | 27 (51.92%) |
| No | 25 (48.07%) |
| Do you think, there is a need of giving choice to antenatal woman regarding alternate birth position? | |
| Yes | 43 (82.69%) |
| No | 09 (17.31%) |
| Not sure | 00 (0.0%) |
Knowledge and attitude towards birth positions
The majority of the nurses (92.3%) were aware of the lithotomy (lying on the back) position and 40 (76.9%) were aware of positions other than lithotomy, that a pregnant woman can assume for childbirth. Doctors were the most common source of information about alternate positions; the media (print and electronic) being the second. Twenty-six nurses responded that they had received enquiries from patients regarding alternate birth positions during their routine antenatal check-up. Almost all the participants (96.1%) were enthusiastic about gaining detailed information regarding alternate birthing positions [Table 3].
Table 3.
Awareness and knowledge regarding various birthing positions among the study participants
| Characteristics | Sample Population n (%) |
|---|---|
| Which commonest birth position are you aware of? | |
| Lithotomy | 52 (100%) |
| Are you aware of alternate birth positions? | |
| Yes | 40 (76.92%) |
| No | 12 (23.07%) |
| What is the source of information about alternate birth positions? (Multiple options selected) | |
| Doctors | 33 |
| Media | 02 |
| Family members and friends | 20 |
| None | 07 |
| Did any antenatal women asked you regarding alternate birth positions? | |
| Yes | 26 (50%) |
| No | 26 (50%) |
| Will you like to get detailed knowledge about different birth positions? | |
| Yes | 50 (96.15%) |
| No | 02 (3.85) |
Knowledge regarding alternate birthing positions
The knowledge about different positions like standing, squatting, lateral, sitting and hand-knee was extremely poor among the respondents. Amongst the various alternate categories of birthing positions, the nurses knew squatting (n = 26, 50%), sitting (n = 19, 36.5%), lateral (n = 12, 23.1%), hand and knee (n = 12, 23.1%) and standing (n = 07, 13.4%). Thus, the most and the least common known alternate birthing positions was squatting and standing respectively. Given a choice other than lithotomy position, they (48.1%) would recommend squatting position to a woman in labour. Figure 1 shows knowledge about various alternate birthing positions other than lithotomy.
Figure 1.
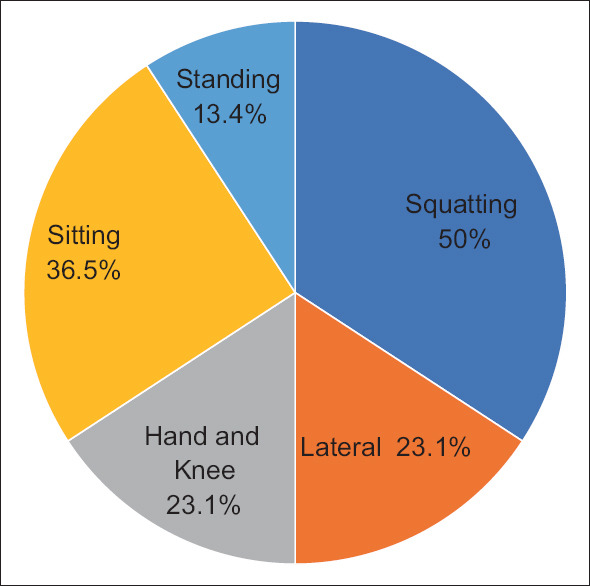
Knowledge about various alternate birthing positions other than lithotomy
There were various reasons cited by the participants for preferring or deferring a particular birth position. Ease and convenience in conducting the delivery was the foremost reason chosen in advocating a birth position. Whereas overcrowding in the labour room, ignorance about alternate positions and difficulty in converting to instrumental delivery were cited as reasons of not recommending these positions. Table 4 shows the reasons for selecting/refusing alternate birth positions among various respondents.
Table 4.
Reasons for selecting/refusing alternate birth positions among the study participants
| Reasons for selection* | Sample Population n (%) |
|---|---|
| Comfort and convenience | 33 (63.5%) |
| Ease of intervention | 05 (9.6%) |
| Less perineal injuries and vulval edema | 17 (32.7%) |
| Less use of instrumental deliveries | 05 (9.6%) |
| Reason for refusal | |
| Due to overcrowding and lack of space in labour room | 25 (48.1%) |
| Not aware of alternate birth positions | 24 (46.2%) |
| Difficult to do intervention if required | 12 (23.1%) |
Discussion
Childbirth is always a challenging process and has a profound effect on women's birth experience and satisfaction of the care provided. Nurses and midwives are in the forefront of health care providers during the time a woman spends in labour, having a major role on woman's physiological and psychological outcomes of the experience. Exploring nursing officer's knowledge and understanding of birthing positions is important as it gives us insights into current clinical practice and whether maternity care is supported by evidence.
In the present study, 98% of study participants believed that respectful maternity care is a universal human right and approximately 83% felt there is a need of giving choice to the women regarding alternate birth positions. Similar findings were reported by Kennedy et al.[13] where most care providers attempted to create a caring environment in which women's desires were met. In another study by Burrowes et al.[14] and Nieuwenhuijze et al.[15] health care providers were uniformly positive in acknowledging the importance of women's rights.
In the present study, all our study participants were aware of lithotomy as common birth position, which was an expected finding. The supine position has been the advocated position for the past 200 years and has come to be the only position known to most nurses.[16] The supine position has become so common that neither health care providers nor labouring women now regard this as an intervention. Also, the presence of the delivery bed in labour rooms implicitly tells women that the supine position is ' normal'. These findings are in line with a study by Mselle et al. where midwives believed that the supine position was the best, most helpful, and best-known birthing position.[17] A preference for the supine position may be due to a lack of knowledge about alternate birth positions among nurses during their professional training.
Approximately 77% of study participants knew about alternate birth positions a woman can assume for childbirth. The most known birth position apart from lithotomy was squatting (26/52) followed by sitting (19/52). The least known birth position among nursing officer was standing (7/52). The observation is similar to a study done by Diorgu FC, et al.[18] where all the midwives were aware of at least one alternate birthing position, for example, squatting, kneeling or sitting. The squatting position is considered to be the most natural position for birth where women are in the habit of squatting to defecate and micturate. A number of advantages have been cited for the squatting position at birth. The position is related with lesser pain, increased pelvic dimensions and more efficient contractions and thus a shorter second stage of labour. This position also reduces the risk of aortocaval compression with an improvement of acid–base balance in newborns.[19,20]
In the present study, about 50% of nursing officers had received enquiries from antenatal women regarding alternate birth positions at the time of labour or delivery. A Study done by Diorgu et al. also suggests that mothers would be willing to adopt different birthing positions if given an opportunity.[18] On the contrary, a study conducted by Okonta documented that only 18.9% antenatal women were willing to try a different birthing position primarily if it was recommended by their health care provider.[16]
On enquiring further about various reasons for preference or refusal of a particular birth position, comfort and convenience were the most common reasons cited for selecting a particular birth position. Nevertheless, the comfort, convenience and the working conditions of nursing officer deserve attention. This fact is supported by a study done by CoppenR,[21] where many midwives had a strong preference for the semi-recumbent position because of their own comfort.[21] If this issue is not addressed, many women will be deprived of a choice in birthing positions in the future. Interestingly, Joeng AD, et al.[22] in his observations, documented that most midwives would go a long way to let a woman give birth in the position of her choice, even if it was inconvenient for them.[22]
Many nursing officers lack the necessary skills for conducting delivery in alternate birth positions. These results are in line with the study by Musie MR, et al.[7] where barriers to the utilization of alternative birth positions was due to lack of necessary skills and lack of facilities in the labour room.
There is global interest in improving the quality of maternal and newborn care. This includes a strong focus on respectful care as an essential component of high quality care. Labour companionship is a key component of providing respectful maternity care. It has been recommended as part of WHO recommendations on intrapartum care for positive childbirth experience. Labour companion provides practical support, encourages women to remain mobile during labour, provides emotional support and non-pharmacological pain relief such as massage and meditation. They also help women feel in control and build their confidence through praise, reassurance and continuous physical presence. Three meta-analysis proved that women who had continuous one to one support during labour were less likely to have a caesarean or instrumental delivery.[23,24,25]
In the present study, the main reason for not recommending other positions are overcrowding of labour rooms followed by lack of awareness. In Indian settings, one to one care of pregnant women during labour is difficult due to overcrowding. In an ideal situation, all antenatal women should be able to receive one to one care in labour. Due to overcrowding in the labour room, nursing staff tends to have multiple responsibilities for more than one labouring woman. They spend a large amount of time in managing and keeping records. Begin or end shifts in the middle of the women's labours is another issue faced in the labour room. This is evident from the study by Gagnon and Waghorn,[26] where only 6.1% of nurses time was spent in providing supportive care in labour room. Moreover, innovations are required to design alternate beds, chairs or other such equipment which can facilitate different birthing positions and those should be easily available in the labour room so that a woman could chose her position comfortably.
The quality of care received by the labouring women is an important measure of any health care system. It is dependent on the philosophy of childbearing held by those providing care. Primary care physicians should advocate use of alternate birthing position keeping their cultural beliefs in mind to uplift the status of maternity care and to promote safe birth practices. They serve as first contact and promote effective communication with patients; hence they can provide and educate the antenatal women as soon as pregnancy is confirmed or at their first visit. Moreover, lack of awareness regarding birthing positions is one of the major factors that hinder utilisation of alternative birth positions during labour. The present study highlighted the satisfactory knowledge of alternate birth positions among nursing officer. It is recommended that nursing officer teaching programme should incorporate theory into practice on provision of alternative birth positions. Educating nursing officers about emerging evidence regarding birthing positions will enable them to give accurate information to women.
Study limitations
The study was done in an urban public health care setting in one geographical area. There is a need to expand the study in more broad settings to include urban private sector and rural areas. This will give a better picture of the role of nurses and midwives and their influence in providing more birthing choices for women. There is a paucity of studies focusing on the use of alternative birth positions in India. This topic needs to be further explored in a larger sample. Further research is required to explore how altering a labour room environment in terms of adding more space and equipment change the attitude of nursing officers towards alternative birth positions. Further research must explore and develop new ways of monitoring the mother and fetus in an alternative birth positions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Shakibazadeh E, Namadian M, Bohren MA, Vogel JP, Rashidian A, Nogueira Pileggi V, et al. Respectful care during childbirth in health facilities globally: A qualitative evidence synthesis. BJOG. 2018;125:932–42. doi: 10.1111/1471-0528.15015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Soong B, Barnes M. Maternal position at midwife – Attended birth and perineal trauma: Is there an association? Birth. 2005;32:164–9. doi: 10.1111/j.0730-7659.2005.00365.x. [DOI] [PubMed] [Google Scholar]
- 3.De Jonge A, Teunisssen D, Lagro-Janssen A. Supine position compared to other positions during the second-stage of labor: A meta-analytic review. J Psychosom Obstet Gynaecol. 2004;25:35–45. doi: 10.1080/01674820410001737423. [DOI] [PubMed] [Google Scholar]
- 4.Zileni BD, Glover P, Jones M, Teoh K, Zileni CW, Muller A. Malawi women's knowledge and use of labour and birthing positions: A cross-sectional descriptive survey. Women Birth. 2017;30:e1–8. doi: 10.1016/j.wombi.2016.06.003. [DOI] [PubMed] [Google Scholar]
- 5.Berta M, Lindgren H, Christensson K, Mekonnen S, Adefris M. Effect of maternal birth positions on duration of second stage of labor: Systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19:466. doi: 10.1186/s12884-019-2620-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Diorgu F, Steen M, Keeling J, Mason-Whitehead E. Exploring Nigerian obstetricians' perspectiveson maternal birthing positions and perineal trauma. Evid Based Midwifery. 2016;14:64–70. [Google Scholar]
- 7.Musie MR, Peu MD, Bhana-Pema V. Factors hindering midwives' utilisation of alternative birth positions during labour in a selected public hospital. Afr J Prm Health Care Fam Med. 2019;11:2071. doi: 10.4102/phcfm.v11i1.2071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dabral A, Pawar P, Bharti R, Kumari A, Batra A, Arora R. Upright kneeling position during second stage of labor: A pilot study. Int J Reprod Contracept Obstet Gynecol. 2018;7:401–7. [Google Scholar]
- 9.Moridi M, Pazandeh F, Hajian S, Potrata B. Midwives' perspectives of respectful maternity care during childbirth: A qualitative study. PLoS One. 2020;15:e0229941. doi: 10.1371/journal.pone.0229941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.de Jonge A, Teunissen DA, van Diem MT, Scheepers PL, Lagro-Janssen AL. Women's positions during the second stage of labour: Views of primary care midwives. J Adv Nurs. 2008;63:347–56. doi: 10.1111/j.1365-2648.2008.04703.x. [DOI] [PubMed] [Google Scholar]
- 11.De Jonge A, Lagro-Janssen AL. Birthing positions. Aqualitative study into the views of women about various birthingpositions. J Psychosom Obstet Gynaecol. 2004;25:47–55. doi: 10.1080/01674820410001737432. [DOI] [PubMed] [Google Scholar]
- 12.Healy M, Nyman V, Spence D, Otten RHJ, Verhoeven CJ. How do midwives facilitate womento give birth during physiological second stage of labour? A systematic review. PLoS One. 2020;15:e0226502. doi: 10.1371/journal.pone.0226502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kennedy HP, Shannon MT, Chuahorm U, Kravetz MK. The landscape of caring for women: A narrative study of midwifery practice. J Midwifery Womens Health. 2004;49:14–23. doi: 10.1016/j.jmwh.2003.09.015. [DOI] [PubMed] [Google Scholar]
- 14.Burrowes S, Holcombe SJ, Jara D, Carter D, Smith K. Midwives' and patients' perspectives on disrespect and abuse during labor and delivery care in ethiopia: A qualitative study. BMC Pregnancy Childbirth. 2017;17:263. doi: 10.1186/s12884-017-1442-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nieuwenhuijze MJ, Low LK, Korstjens I, Lagro-Janssen T. The role of maternity care providers in promoting shared decision making regarding birthing positions during the second stage of labor. J Midwifery Womens Health. 2014;59:277–85. doi: 10.1111/jmwh.12187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Okonta P. Birthing positions: awareness and preferences of pregnant women in a developing country. Int J Gynecol Obstet. 2012;16:1–3. [Google Scholar]
- 17.Mselle LT, Eustace L. Why do women assume a supine position when giving birth? The perceptions and experiences of postnatal mothers and nurse-midwives in Tanzania. BMC Pregnancy Childbirth. 2020;20:36. doi: 10.1186/s12884-020-2726-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Diorgu FC, Steen MP, Keeling JJ, Mason-Whitehead E. Mothers and midwives perceptions of birthing position and perineal trauma: An exploratory study. Women Birth. 2016;29:518–23. doi: 10.1016/j.wombi.2016.05.002. [DOI] [PubMed] [Google Scholar]
- 19.Moraloglu O, Kansu-Celik H, Tasci Y, Karakaya BK, Yilmaz Y, Cakir E, et al. The influence of different maternal pushing positions on birth outcomes at the second stage of labor in nulliparous women. J Matern Fetal Neonatal Med. 2017;30:245–9. doi: 10.3109/14767058.2016.1169525. [DOI] [PubMed] [Google Scholar]
- 20.Gupta JK, Brayshaw EM, Lilford RJ. An experiment of squatting birth. Eur J Obstet Gynecol Reprod Biol. 1989;30:217–20. doi: 10.1016/0028-2243(89)90004-x. [DOI] [PubMed] [Google Scholar]
- 21.Coppen R. Birthing Positions: Do Midwives Know Best? London: MA Healthcare Limited; 2005c. Midwives' views on birthing positions; pp. 79–106. [Google Scholar]
- 22.De Jonge A, Teunissen DA, van Diem MT, Scheepers PL, Lagro-Janssen AL. Women's positions during the second stage of labour: Views of primary care midwives. J Adv Nurs. 2008;63:347–56. doi: 10.1111/j.1365-2648.2008.04703.x. [DOI] [PubMed] [Google Scholar]
- 23.Bohren MA, Hofmeyr GJ, Sakala C, Fukuzawa RK, Cuthbert A. Continuous support for women during childbirth? Cochrane Database Syst Rev. 2017;7:CD003766. doi: 10.1002/14651858.CD003766.pub6. doi: 10.1002/14651858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Scott KD, Klaus PH, Klaus MH. The obstetrical and postpartum benefits of continuous support during childbirth. J Womens Health Gend Based Med. 1999;8:1257–64. doi: 10.1089/jwh.1.1999.8.1257. [DOI] [PubMed] [Google Scholar]
- 25.Zhang J, Bernasko JW, Lebovich E, Fahs M, Hatch MC. Continuous labor support from labor attendant for primiparous women: A metaanalysis. Obstet Gynecol. 1996;88:739–44. doi: 10.1016/0029-7844(96)00232-3. [DOI] [PubMed] [Google Scholar]
- 26.Gagnon AJ, Waghorn K. Supportive care by maternity nurses: A work sampling study in an intrapartum unit. Birth. 1996;23:1–6. doi: 10.1111/j.1523-536x.1996.tb00453.x. [DOI] [PubMed] [Google Scholar]