

Abstract
Background
Socioeconomic inequalities between and within countries lead to disparities in the use of health services. These disparities could lead to child mortality in children under 5 years by depriving them of healthcare. Therefore, initiatives to remove healthcare fees such as the Free Healthcare Initiative (FHCI) adopted in Sierra Leone can contribute to reducing these inequities in healthcare-seeking for children. This study aimed to assess the socioeconomic inequalities in healthcare-seeking for children under 5 years of age before and after the implementation of the FHCI.
Methods
Data were included on 1207, 2815, 1633, and 1476 children under 5 years of age with fever from the 2008, 2013, 2016, and 2019 nationwide surveys, respectively. Concentration curves were drawn for the period before (2008) and after (2013–2019) the implementation of the FHCI to assess socioeconomic inequalities in healthcare-seeking. Finally, Erreyger’s corrected concentration indices were calculated to understand the magnitude of these inequalities.
Results
Before the implementation of the FHCI, there were inequalities in healthcare-seeking for children under five (Erreyger’s corrected concentration index (CI) = 0.168, standard error (SE) = 0.049; p < 0.001) in favor of the wealthy households. These inequalities decreased after the implementation of the FHCI (CI = 0.061, SE = 0.033; p = 0.06 in 2013, CI = 0.039, SE = 0.04; p = 0.32 in 2016, and CI = − 0.0005, SE = 0.362; p = 0.98 in 2019). Furthermore, before the implementation of the FHCI, a significant pro-rich inequality in the districts of Kenema (CI = 0.117, SE = 0.168, p = 0.021), Kono (CI = 0.175, SE = 0.078, p = 0.028) and Western Area Urban (CI = 0.070, SE = 0.032, p = 0.031) has been observed. After the implementation of the FHCI in 2019, these disparities were reduced, 11 of the 14 districts had a CI around the value of equality, and only in 2 districts the pro-rich inequality were significant (Western Area Urban (CI = 0.035, SE = 0.016, p = 0.039) and Western Area Rural (CI = 0.066, SE = 0.030, p = 0.027)).
Conclusion
The results of this study demonstrated that socio-economic inequalities in healthcare-seeking for children have been considerably reduced after the FHCI in Sierra Leone. To further reduce these inequalities, policy actions can focus on the increase of availability of health services in the districts where the healthcare-seeking remained pro-rich.
Keywords: Socioeconomic inequalities, Healthcare utilization, Children under five, Sierra Leone
Background
Notable progress has been made in reducing child mortality over the past 3 decades but improving child survival remains an urgent concern, especially in sub-Saharan Africa (SSA). Global estimates show that under-5 mortality declined in by 59%, from 93 deaths per 1000 live births in 1990 to 38 in 2019 [1]. The highest rates are still seen in SSA where more than 50% of the estimated 5.2 million children under-5 died in 2019 [1].
In SSA, most under-5 deaths are preventable with effective low-cost interventions but prevailing inequalities between subpopulations within countries in this region [2] pose a major challenge in expanding access to such interventions particularly in disadvantaged groups and areas with poor access to health services [3]. The poorest subpopulations thus remain lagging compared to their richest counterparts [3, 4].
Disparities in access to healthcare between the least and most deprived groups within a country are well established [5, 6], and factors related to socioeconomic status have been shown to exert varied effects on the variability of under-5 mortality in SSA [7]. Therefore, interventions within-country level plays a vital role in eliminating health inequalities. Recent evidence demonstrates that countries that have attained high coverage of maternal, newborn and child health interventions will also show reduced socio-economic inequalities in these coverage levels [6, 8–10].
In Sierra Leone, access to healthcare has been problematic over the past 2 decades especially for the vulnerable populations due to health system constraints from civil wars (1991–2002) [11] and waves of disease epidemics (Cholera and Ebola) [12, 13]. This was evident via the high rate (30%) of children under-5 who did not have access to healthcare in 2013 [14] and a slow decline in under-5 mortality from 120 deaths per 1000 live births in 2015 to 102 in 2020 [15]. In response, the government implemented the Free Healthcare Initiative (FHCI) for children under-5, pregnant women and lactating mothers in 2010 to reduce the inequalities in terms of access to healthcare and high mortality rate [16].
Since its implementation, the utilization of health services, particularly antenatal and postnatal services increased [17–19]. Antenatal care visits and institutional delivery increased by 25% from 2008 to 2013 [19], and the proportion of healthcare-seeking for febrile illness in children under-5 also increased from 62% in 2013 to 71% in 2016 [18]. However, this increase in accessibility to healthcare was unevenly distributed between wealth levels, regions, and types of places of residence [19].
The theoretical framework in Fig. 1 below explains how the FHCI is expected to work to increase healthcare-seeking for febrile children and lead to the reduction of the mortality of children under five. If health services are available and accessible in terms of cost and distance, and the quality of these services improved and sustained by motivated, competent workers, then socioeconomic inequalities will decrease. Consequently, more caregivers will use the free under-five mortality will rate.
Fig. 1.
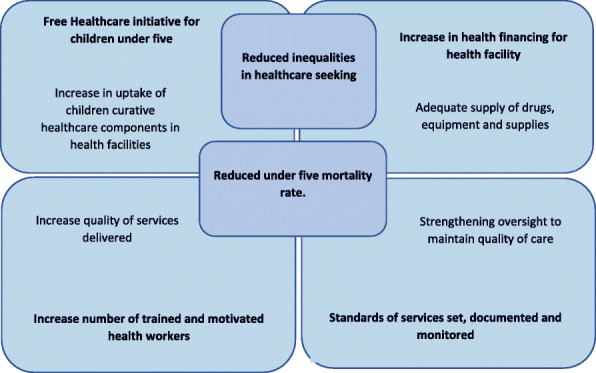
Theoretical framework of free healthcare initiative adapted from Manso et al. [20]
To date, no study has assessed the impact of the FHCI on the socioeconomic inequalities in access to curative healthcare for children under five in Sierra Leone. Using data collected from 4 cycles of the Sierra Leone Demographic Health Surveys (DHS 2008, 2013, 2016 and 2019), this study sort to assess the inequalities in access to healthcare for children under five in terms of quantity and magnitude before and after the implementation of the FHCI in Sierra Leone.
Such additional knowledge could be used for designing finer investigations to uncover and address the drivers of the inequalities persisting where the FHCI aimed at flattening them.
Methodology
Setting
Sierra Leone is a West African country located on the southwest coast, with a surface area of 71,740 km2 and an estimated population of 7,396,000 in 2016 [21]. The population is generally young, with about 63% of the total population aged less than 25 years, 17% representing children under 5 years [22]. Like other SSA countries, it has a tropical climate with two seasons and vegetation ranging from the savannah in the North to the rainforest in the South.
For these surveys, the country was divided into four administrative regions (the northern, eastern, southern, and western regions), and each region further subdivided into districts (total of 14 districts) in the country.
The health system in Sierra Leone is organized into three levels. The primary level, which is made up of peripheral health units (PHUs), of which 229 are community health centers (CHCs), 386 community health posts (CHPs), and 559 maternal and child health posts (MCHPs). The secondary level which consists of 21 district hospitals [23], and the tertiary level which includes regional and specialized hospitals. There are six teaching hospitals and several private clinics and hospitals spread across the 14 districts of the country. The distribution of the wealth index is not equal between the rural and urban areas. Approximately 61% of the population in the urban area are richest and in the rural area, 28% are poorest [24], while the inequality-adjusted human development index was low at 0.266 in 2017 [25].
Data source
This study used data from the 2008, 2013, and 2019 Sierra Leone Demographic and Health Surveys (DHS) and the 2016 Malaria Indicator Survey (MIS). These are national representative household surveys in which women aged 15–49 years were interviewed. Details of the complete description of the interview methods are available elsewhere [24, 26]. The current study focused on febrile children under 5 years of age whose caregivers sought healthcare in the 2 weeks preceding each of the surveys.
Variables
Outcome measure
The outcome variable is healthcare-seeking, which is the proportion of under-five children with fever in the 2 weeks preceding the surveys, whose caregivers sought care in public or private (coded 1) health centers or traditional/other (coded 0).
Socioeconomic variable
Household wealth index is used as the main socioeconomic variable in this study. The wealth index is a composite indicator of inequalities in household characteristics and was categorized (richest, richer, middle, poor, and poorest) based on the household’s ownership of consumer goods; dwelling characteristics; type of drinking water source; toilet facilities; and other characteristics that relate to a household’s socioeconomic status. The detailed construction and explanation of this variable has been previously described elsewhere [24, 26, 27].
Other variables
The independent variables were chosen based on similar studies [19, 28] and included sociodemographic variables and the determinants of healthcare-seeking for febrile children. The respondent’s age which was recorded as 15 to 59 years was re-categorized (15–24 years for younger mothers, 25–34 years for middle aged mothers, and ≥ 35 years for old mothers). Also, the mother’s level of education; attended school? Yes = 1 and No = 0, and the school level which was coded as primary = 0, junior secondary = 1, senior secondary = 2, vocational / commercial / nursing technical / teaching = 3 and higher = 4 was re-categorized (no formal education, primary education, and secondary education or higher). The total number of children born in the household recorded 0 to 9 and more was categorized as 1–2, 3–4, and ≥ 5 children. The sex of the head of the household (male = 1 and female = 0); the age of the head of the household (15–24, 25–34, and ≥ 35 years); the regions (east, north, south, and west); the districts of residence (Kailahum, Kenema, Kono, Bombali, Kambia, Koinadugu, Port Loko, Tonkolili, Bo, Bonthe, Moyamba, Pujehun, Western Area Rural, and Western Area Urban); the types of places of residence (coded rural = 0 or urban = 1) were also used. Child age recorded as 0 to 59 months was categorized (< 12, 12–35, and 36–59 months), and together with the sex of the child (male = 1 and female = 0), child’s household size (recorded 0 to 9 and more); and the type of facility where healthcare was sought (public, private, traditional, or other) were also selected as independent variables.
Sampling method
A two-stage cluster sampling method was used in all the 4 population-based surveys. The country was sub-divided into enumeration areas (EAs), and each EA included several households. In the first stage, EAs were selected with stratified probability proportional to sample size, and the place of residence (urban or rural) was used to stratify the EAs. In the second stage, households were selected using systematic random sampling from the EAs. The sampling frames were developed based on the 2004 census for the 2008 and 2013 surveys and on the 2015 census for the 2016 and 2019 surveys [22, 24, 26].
Statistical methods
Statistical analyses were performed using Stata version 15.0. The characteristics of the children’s caregivers and those of the febrile children whose sought healthcare were described. For the analysis of wealth related inequalities in healthcare seeking, participants were grouped (according to their socioeconomic status) into wealth quintiles, as follows: Poorest (1st quintile), poorer (2nd quintile), middle (3rd quintile), richer (4th quintile), and richest (5th quintile). Analyses were performed separately for each survey to evaluate the proportion of caregivers seeking care for their febrile children. The descriptive analyses were weighted for probability sampling and adjusted for stratification and clustering. An alpha 0.05 was set for statistically significant difference between compared groups.
Measuring socioeconomic inequalities
The concentration curves and the concentration index were used to assess socioeconomic inequalities in the use of healthcare at the country level. At the district level, the concentration index was used to estimate the socioeconomic inequalities in the healthcare-seeking for children under five. The concentration curves were used to examine the trend in the pattern of the socioeconomic inequalities in healthcare-seeking, while the concentration index was used to assess the magnitude of the inequalities in healthcare-seeking. The use of the concentration curve and index in the quantification of the degree of the socioeconomic-related inequality in the health-state indicators is well documented [29–32].
Concentration curves
The concentration curves (Lorenz curve) were built using two keys’ variables: The wealth index and the healthcare-seeking for febrile children under five. The concentration curves represent a plot of the cumulative percentage of caregivers seeking care (y-axis) against the cumulative percentage of the households, ranked by the wealth index, beginning with the poorest, and ending with the richest (x-axis) [33].
The concentration curves were compared to the line of equality which is the 45-degree line running from the bottom left-hand corner to the upper right-hand corner, indicating the absence of inequalities in healthcare-seeking between the households ranked in the wealth quintiles. When the percentage of caregivers seeking care takes higher values among poorer households, the concentration curves lie above the line of equality. On the contrary, when it takes lower values among poorer households, the concentration curves lie below the line of equality. The farther the curves are above the line of equality, the more concentrated the health variable is among the poor [33].
Concentration index
The concentration index estimates the magnitude of wealth-related inequalities in healthcare-seeking. The formula of the concentration index is as follows:
where h represents healthcare-seeking, μ represents its mean, r is the fractional rank of an individual in the wealth index distribution, and cov is the covariance between care-seeking and the fractional rank of the wealth index [33]. The concentration index is calculated as twice the area between the curve and the line of equality. It’s also bounded between − 1 and 1.
In absence of wealth-related inequalities, the concentration index is zero. The concentration index takes a negative value when the curve lies above the line of equality, indicating a disproportionate concentration of healthcare-seeking among the poor. It takes a positive value when it lies below the line of equality, indicating a concentration of healthcare-seeking among the richer [33]. Given that the bounds of the C of a binary health indicator depend on the mean of this indicator which varied according to the periods studied, the Erreygers’ normalization option was selected in Stata. QGIS 3.12 software was used to map the concentration indices for healthcare-seeking for children under five at the health district level [34].
Results
In total, 1207 (21.5% of the total of children in 2008), 2815 (23.6% of the total of children in 2013), 1633 (26.3% of the total of children in 2016) and 1476 (15% of the total of children in 2019) children under five with a history of fever were included from the 2008, 2013, 2016 and 2019 surveys, respectively.
Characteristics of caregivers and children and healthcare-seeking for fever
Table 1 illustrates the healthcare-seeking for children under five by caregivers and children characteristics. Close to half (more than 45%) of the caregivers aged between 25 and 34 years sought care for fever in all four surveys. Similarly, about 50% of those who solicited care for fever came from large families (6–10 members) whilst over a third (more than 30%) had 3 or more children. Three in four (about 75%) caretakers belonged to households headed by middle-aged or older men. About two thirds (60%) were uneducated, came from rural areas and resided mainly in the Northern and Southern. Close to half (more than 45%) of the children were aged 12–35 months.
Table 1.
Healthcare-seeking for children under five by caregivers and children characteristics
| Characteristics of the population | 2008 | 2013 | 2016 | 2019 |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Caregivers | ||||
| Age of mother (years) | ||||
| 15–24 | 190 (28.4) | 604 (28.8) | 400 (34.2) | 339 (28.3) |
| 25–34 | 318 (50.2) | 971 (47.1) | 555 (46.3) | 533 (48.1) |
| ≥ 35 | 121 (21.4) | 499 (24.1) | 218 (19.5) | 249 (23.6) |
| Number of family members | ||||
| 1–5 | 183 (26.0) | 608 (31.0) | 374 (30.4) | 424 (37.6) |
| 6–10 | 356 (58.8) | 1114 (52.4) | 609 (52.5) | 546 (48.8) |
| > 10 | 90 (15.2) | 352 (16.6) | 190 (17.1) | 152 (13.6) |
| Total number of children born | ||||
| 1–2 | 251 (37.7) | 702 (33.2) | 369 (33.2) | 420 (36.8) |
| 3–4 | 195 (30.4) | 661 (32.5) | 358 (31.2) | 368 (31.4) |
| ≥ 5 | 183 (31.9) | 711 (34.3) | 446 (35.6) | 333 (31.8) |
| Mother’s education level | ||||
| None | 388 (64.9) | 1381 (65.8) | 688 (57.8) | 582 (51.7) |
| Primary | 108 (16.1) | 309 (14.9) | 188 (14.9) | 194 (18.0) |
| Secondary or higher | 133 (19.0) | 384 (19.3) | 297 (27.3) | 345 (30.3) |
| Gender of the household head | ||||
| Male | 491 (78.7) | 1530 (74.7) | 895 (76.1) | 884 (77.8) |
| Female | 138 (21.3) | 544 (25.3) | 278 (23.9) | 237 (22.2) |
| Age of the household head (years) | ||||
| 15–24 | 23 (3.3) | 73 (3.7) | 34 (2.8) | 45 (3.8) |
| 25–34 | 156 (22.5) | 514 (24.8) | 262 (20.5) | 255 (22.3) |
| ≥ 35 | 450 (74.2) | 1487 (71.5) | 877 (76.7) | 821 (73.9) |
| Place of residence | ||||
| Urban | 270 (35.1) | 669 (27.8) | 323 (34.1) | 345 (34.8) |
| Rural | 359 (64.9) | 1405 (72.2) | 850 (65.9) | 776 (65.2) |
| Region | ||||
| East | 188 (12.5) | 472 (26.0) | 254 (25.3) | 268 (26.0) |
| North | 184 (40.6) | 891 (39.4) | 447 (37.6) | 173 (12.6) |
| South | 170 (24.5) | 525 (23.1) | 388 (26.8) | 218 (18.9) |
| West | 157 (22.4) | 186 (11.5) | 84 (10.3) | 462 (42.5) |
| CHILDREN | ||||
| Gender of the child | ||||
| Male | 326 (50.8) | 1055 (50.7) | 595 (49.4) | 563 (50.0) |
| Female | 303 (49.2) | 1019 (49.3) | 578 (50.6) | 558 (50.0) |
| Age (months) | ||||
| < 12 | 88 (31.7) | 235 (22.7) | 266 (23.0) | 125 (20.9) |
| 12–35 | 129 (45.9) | 465 (46.8) | 558 (45.9) | 289 (47.3) |
| 36–59 | 66 (22.4) | 317 (30.5) | 349 (31.1) | 188 (32.8) |
Healthcare-seeking for children under five with fever increased from 51% in 2008 to 71.6, 70, and 74% in 2013, 2016, and 2019, respectively. Figure 2 shows the healthcare-seeking behavior for children under five by the wealth index. Healthcare-seeking was increased between 2008 and 2019 in each socioeconomic status, with the most increase observed among poorest population.
Fig. 2.
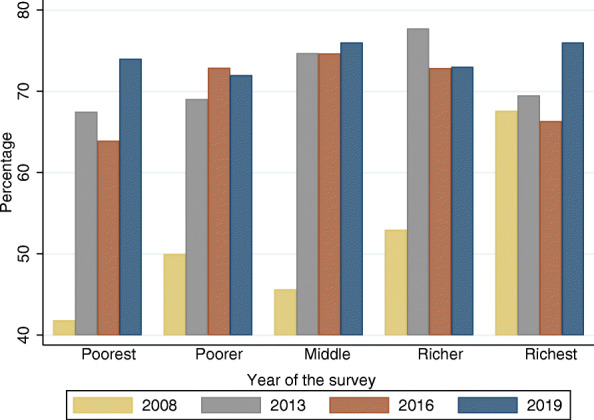
Distribution of healthcare-seeking for children under five by wealth index and by year
Socioeconomic inequalities in healthcare-seeking
Figure 3 shows the concentration curves of healthcare-seeking for children under five with fever before (2008) and after (2013, 2016, and 2019) the implementation of the FHCI. In 2008, before the initiation of the FHCI, socioeconomic-related inequalities in healthcare-seeking favored the rich households, meaning that healthcare-seeking was concentrated among the wealthy households. Following the implementation of the FHCI, the inequalities declined progressively up to the line of equality in 2019.
Fig. 3.
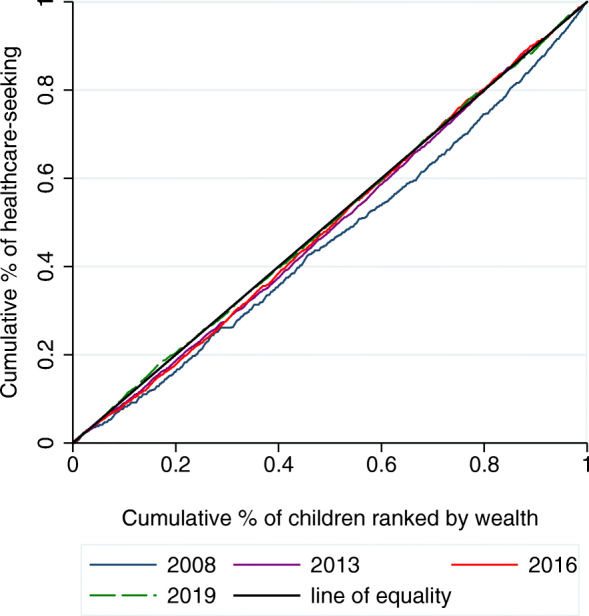
Concentration curves for healthcare-seeking for children under five, 2008–2019
The Fig. 4 shows the wealth-related inequalities in healthcare-seeing for febrile children under five in the four surveys at the district level. Healthcare-seeking was pro-rich in seven districts in 2008, while in 2019 there were three pro-rich districts.
Fig. 4.

Maps of the wealth-related inequalities in healthcare-seeking at the district level, 2008–2019
In 2008, a significant pro-rich inequality in the districts of Kenema (CI = 0.117, SE = 0.168, p = 0.021), Kono (CI = 0.175, SE = 0.078, p = 0.028) and Western Area Urban (CI = 0.070, SE = 0.032, p = 0.031) has been observed (Fig. 4a).
In 2013, healthcare-seeking for febrile children was significantly pro-rich in the districts of Kenema (CI = 0.073, SE = 0.018, p < 0.001), Bombali (CI = 0.037, SE = 0.016, p = 0.024), Koinadugu (CI = 0.068, SE = 0.023, p = 0.004), Port Loko (CI = 0.083, SE = 0.027, p = 0.003), and Bo (CI = 0.081, SE = 0.24, p < 0.001), (Fig. 4b).
In 2016, a significant pro-rich inequality was observed in the districts of Port Loko (CI = 0.171, SE = 0.062, p = 0.008), Bonthe (CI = 0.066, SE = 0.030, p = 0.030), Pujehun (CI = 0.053, SE = 0.017, p = 0.004), and in Western Area Rural (CI = 0.174, SE = 0.056, p = 0.003) (Fig. 4c).
In 2019, these disparities 11 of the 14 districts had a CI around the value of equality, and in 2 districts the pro-rich inequality were significant (Western urban Area (CI = 0.035, SE = 0.016, p = 0.039) and Western Area Rural (CI = 0.066, SE = 0.030, p = 0.027) (Fig. 4d).
Concentration index of healthcare-seeking for children under five with fever
To better appreciate the magnitude of the inequalities, the authors computed the concentration index as reported in Table 2.
Table 2.
The concentration index for healthcare-seeking for children under five by year
| Outcome | 2008 | 2013 | 2016 | 2019 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CI | SE | p-Value | CI | SE | p-Value | CI | SE | p-Value | CI | SE | p-Value | |
| Healthcare-seeking | 0.168 | 0.049 | < 0.001 | 0.061 | 0.033 | 0.061 | 0.039 | 0.040 | 0.32 | −0.0005 | 0.362 | 0.98 |
CI Erreygers’ corrected concentration index, SE standard error
The positive concentration index in 2008 suggests that healthcare was more accessible to rich households. A decrease in the magnitude of the inequalities was noted after the implementation of the FHCI (2013–2019), as indicated by a 2019 concentration index, close to zero (− 0.0005).
Discussion
This study aimed to assess socioeconomic inequalities in access to healthcare among under-five children in Sierra Leone with febrile illness before and after the implementation of the FHCI. This study showed evidence of wealth-related inequalities in healthcare-seeking for febrile children under five in favor of rich households before the implementation of the FHCI at the country level. However, these inequalities decreased following the implementation of the policy. It also highlights a difference of these inequalities in healthcare-seeking for children under-five between districts before and after the FHCI.
The study results are consistent with previous reports on wealth-related inequalities in favor of wealthy households [19, 28, 35]. The use of healthcare has a cost for societies [36, 37], and making access to health services possible for everyone by the policy makers remains a major challenge for developing countries. In 2008, healthcare costs were one of the major barriers to accessing healthcare [38], as evidenced by a positive concentration index of around 0.168, favoring the wealthy households. After the initiation of free healthcare for children under the age of five, a notable decrease in the inequalities in healthcare-seeking from 0.168 in 2008 to 0.04 in 2016, and − 0.0005 in 2019 was observed. This could be explained by a reduction in the barriers represented by the costs of care, thereby allowing access to healthcare for a fringe of children under five belonging to poor households. Moreover, this decrease could be explained by the reinforcement of resources in the health domain such as the increased density of health workers between 2008 and 2016. Indeed, the density of physicians increased from 0.016 to 0.025 per 1000 people, and that of midwives and nurses increased from 0.162 to 0.224 per 1000 people within the same period [39, 40]. This increase in the density of health staff could explain the fact that, in some districts, inequalities in healthcare-seeking showed a considerable reduction, which led to a reversal in healthcare-seeking in favor of vulnerable social strata.
In 2019 compared to 2008, the number of districts with an equal access to healthcare were high, this is consistent with reports on the sustainability and the equitable delivery of the FHCI in the country [16, 17, 41]. This suggest that efforts made to cover all the country with the health services are perceptible in the district level. With the difficulties experienced in the country by the health system, many non-governmental organizations are working to make available healthcare for vulnerable population by providing medical supplies and training health workers [42, 43]. These interventions conjugated with the FHCI have seen the reduction of the socioeconomic inequalities in healthcare-seeking for children under-five years of age by reducing the number of districts where healthcare-seeking were pro-rich.
It remains districts where healthcare-seeking is pro-rich in the context of free healthcare in 2019, namely Port Loko, Bonthe, Pujehun and Western Area Rural. Bonthe for example is made of mainland, and many isolated islands, and then are the most remote, hardest-to-reach areas of the country. It is part of district hardly experienced by Ebola outbreak and many health facilities were closed, reducing the accessibility to the healthcare [44, 45], maintaining the pro-rich inequalities in healthcare-seeking, as for Pujehun, it is one of the country’s poorest and least developed districts. This limited the access of population to the health services, because there is one hospital for a population of over 335,000 [46].
Port Loko the most populous, and Western Area Rural districts were affected by the Ebola outbreak and considered as the “hotspot” of the outbreak. In additional, over 30% of the population are food insecure resulting to a slow progression of the level of social services and economic recovery since the end of the outbreak [47, 48]. The difficulties to cover needs of the districts in terms of health services led to the remaining pro-rich in the healthcare-seeking for children under five.
The lack of health resources made healthcare-seeking for children under five more accessible to rich households despite the free health care initiative in these districts.
One of the strengths of this paper is that the study used nationally representative data that allows the generalization of findings to the entire country. Moreover, the study presents, for the first-time, the wealth-related inequalities in healthcare-seeking for children under 5 years in Sierra Leone. However, this study, is subject to some limitations. Even if, the decrease in the socioeconomic inequalities coincided with the implementation of the FHCI, we cannot make causal interpretation due to the cross-sectional nature of the data. Some factors that may affect healthcare-seeking such as the quality of health services, the availability of supplies, and the differences in the sociocultural conception of illness and its etiology may have contributed to the socio-economic inequalities.
Conclusion
The current study pointed out that the inequalities in healthcare-seeking in Sierra Leone, were globally in favor of wealthy households before the FHCI. After the FHCI, these inequalities were reduced, though with some observable residual inequalities still in favor of wealthy households in two districts in 2019. Public health programs could be adjusted to better address drivers other than financial barriers so that inequalities in healthcare-seeking for children in Sierra Leone are reduced further.
Acknowledgements
The authors wish to thank the DHS Program for providing the Sierra Leone Demographic Health Surveys data for 2008 and 2013 and the Malaria Indicator Survey for 2016. Many thanks also go to Calypse Ngwasiri for his input in the final version of the manuscript.
Abbreviations
- CHC
Community healthcare
- CHP
Community health post
- CI
Concentration index
- DHS
Demographic and Health Surveys
- EAs
Enumeration areas
- FHCI
Free Healthcare Initiative
- ICF
International Coach Federation
- MCHP
Maternal and child health post
- PHC
Primary healthcare
- PHU
Peripheral health unit
- SDGs
Sustainable Development Goals
- SE
Standard error
- SSA
Sub-Sahara Africa
- WHO
World Health Organization
Authors’ contributions
K.S.F. and S.S. conceptualized the study; B.J.D. analyzed the data and wrote the first draft of the manuscript; K.S.F., S.S., OM, H.T., and C.V.M. contributed to the data interpretation and the intellectual content of the manuscript. All authors read and approved the final version of the manuscript.
Funding
The authors did not receive any funding for this work.
Availability of data and materials
The datasets analyzed during the current study are available from the Demographic and Health Surveys program repository and are accessible after written request: https://dhsprogram.com/data.
Declarations
Ethical approval and consent to participate in the survey
For the three surveys, the Sierra Leone National Ethics Committee, and the International Review Board of the International Coach Federation (ICF) approved the tools to be used and the participants’ written consent was obtained before data collection. Authorization was given by the DHS Program to access data on https://dhsprogram.com/data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Joel D. Bognini, Email: bogninijoel@gmail.com
Sekou Samadoulougou, Email: ouindpanga-sekou.samadoulougou.1@ulaval.ca.
Mady Ouedraogo, Email: omadess@yahoo.fr.
Tiga David Kangoye, Email: tigakd@yahoo.fr.
Carine Van Malderen, Email: cvmalderen@gmail.com.
Halidou Tinto, Email: halidoutinto@gmail.com.
Fati Kirakoya-Samadoulougou, Email: fati.kirakoya@ulb.ac.be.
References
- 1.The United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) Levels and Trends in Child Mortality: Report 2019. New York: UNICEF; 2020. [Google Scholar]
- 2.Tabutin D, Masquelier B. Mortality inequalities and trends in low-and middle-income countries, 1990-2015. Population. 2017;72(2):221–296. doi: 10.3917/popu.1702.0227. [DOI] [Google Scholar]
- 3.McKinnon B, Harper S, Kaufman JS, Bergevin Y. Socioeconomic inequality in neonatal mortality in countries of low and middle income: a multicountry analysis. Lancet Glob Health. 2014;2(3):e165–e173. doi: 10.1016/S2214-109X(14)70008-7. [DOI] [PubMed] [Google Scholar]
- 4.Chao F, You D, Pedersen J, Hug L, Alkema L. National and regional under-5 mortality rate by economic status for low-income and middle-income countries: a systematic assessment. Lancet Glob Health. 2018;6(5):e535–e547. doi: 10.1016/S2214-109X(18)30059-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Houweling TA, Kunst AE. Socio-economic inequalities in childhood mortality in low- and middle-income countries: a review of the international evidence. Br Med Bull. 2010;93(1):7–26. doi: 10.1093/bmb/ldp048. [DOI] [PubMed] [Google Scholar]
- 6.Barros AJD, Ronsmans C, Axelson H, Loaiza E, Bertoldi AD, França GVA, Bryce J, Boerma JT, Victora CG. Equity in maternal, newborn, and child health interventions in countdown to 2015: a retrospective review of survey data from 54 countries. Lancet. 2012;379(9822):1225–1233. doi: 10.1016/S0140-6736(12)60113-5. [DOI] [PubMed] [Google Scholar]
- 7.Van Malderen C, Amouzou A, Barros AJD, Masquelier B, Van Oyen H, Speybroeck N. Socioeconomic factors contributing to under-five mortality in sub-Saharan Africa: a decomposition analysis. BMC Public Health. 2019;19(1):760. doi: 10.1186/s12889-019-7111-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Victora CG, Barros AJD, Axelson H, Bhutta ZA, Chopra M, França GVA, Kerber K, Kirkwood BR, Newby H, Ronsmans C, Boerma JT. How changes in coverage affect equity in maternal and child health interventions in 35 countdown to 2015 countries: an analysis of national surveys. Lancet. 2012;380(9848):1149–1156. doi: 10.1016/S0140-6736(12)61427-5. [DOI] [PubMed] [Google Scholar]
- 9.Carrera C, Azrack A, Begkoyian G, Pfaffmann J, Ribaira E, O’Connell T, Doughty P, Aung KM, Prieto L, Rasanathan K, Sharkey A, Chopra M, Knippenberg R. UNICEF equity in child survival, health and nutrition analysis team a: the comparative cost-effectiveness of an equity-focused approach to child survival, health, and nutrition: a modelling approach. Lancet. 2012;380(9850):1341–1351. doi: 10.1016/S0140-6736(12)61378-6. [DOI] [PubMed] [Google Scholar]
- 10.Chopra M, Sharkey A, Dalmiya N, Anthony D, Binkin N. Strategies to improve health coverage and narrow the equity gap in child survival, health, and nutrition. Lancet. 2012;380(9850):1331–1340. doi: 10.1016/S0140-6736(12)61423-8. [DOI] [PubMed] [Google Scholar]
- 11.Mary K, James V. Evaluation of UNDP assistance to conflict-affected countries. 2006. [Google Scholar]
- 12.WHO . Cholera in Sierra Leone and Guinea. 2012. [Google Scholar]
- 13.Weyer J, Jansen van Vuren P, Ntshoe G, Ihekweazu C, Msimang V, Blumberg L, et al. Ebola virus disease outbreak in West Africa: one year down the line and the NICD response. NICD Commun Dis Surveill Bull. 2015;13:1–9. [Google Scholar]
- 14.Statistics Sierra Leone SSL. Sierra Leone demographic and health survey 2019. 2019. [Google Scholar]
- 15.Sierra Leone Under-5 mortality rate, 1960–2020 - knoema.com. Knoema. https://knoema.com//atlas/Sierra-Leone/topics/Health/Health-Status/Under-5-mortality-rate. Accessed 24 Mar 2021.
- 16.Witter S, Brikci N, Harris T, Williams R, Keen S, Mujica A, et al. The Sierra Leone Free Health Care Initiative (FHCI): process and effectiveness review. 2016. [Google Scholar]
- 17.Edoka I, Ensor T, McPake B, Amara R, Tseng F-M, Edem-Hotah J. Free health care for under-fives, expectant and recent mothers? Evaluating the impact of Sierra Leone’s free health care initiative. Health Econ Rev. 2016;6(1):19. doi: 10.1186/s13561-016-0096-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Druetz T, Fregonese F, Bado A, Millogo T, Kouanda S, Diabaté S, Haddad S. Abolishing fees at health centers in the context of community case Management of Malaria: what effects on treatment-seeking practices for febrile children in rural Burkina Faso? Plos One. 2015;10(10):e0141306. doi: 10.1371/journal.pone.0141306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jalloh MB, Bah AJ, James PB, Sevalie S, Hann K, Shmueli A. Impact of the free healthcare initiative on wealth-related inequity in the utilization of maternal & child health services in Sierra Leone. BMC Health Serv Res. 2019;19(1):352. doi: 10.1186/s12913-019-4181-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koroma MM, Kamara SS, Bangura EA, Kamara MA, Lokossou V, Keita N. The quality of free antenatal and delivery services in northern Sierra Leone. Health Res Policy Syst. 2017;15(S1):49. doi: 10.1186/s12961-017-0218-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.WHO | Sierra Leone statistics. WHO. http://www.who.int/countries/sle/en/. Accessed 20 Feb 2020.
- 22.Koroma D, Turay M, Moigua M. 2004 population and housing census: analytical report on population projection for Sierra Leone. 2006. https://www.statistics.sl/images/StatisticsSL/Documents/Census/2004/2004_population_and_housing_census_report_on_projection_for_sierra_leone.pdf. Accessed 23 Feb 2020.
- 23.Ministry of Health and Sanitation . Human Resources for Health Strategy 2017-2021. 2017. [Google Scholar]
- 24.Statistics Sierra Leone SSL, International ICF . Sierra Leone demographic and health survey 2013. 2014. [Google Scholar]
- 25.Classement des États du monde par indice de développement humain ajusté aux inégalités (IDHI). Atlasocio.com. https://atlasocio.com/classements/economie/developpement/classement-etats-par-indice-de-developpement-humain-ajuste-selon-les-inegalites-monde.php. Accessed 10 Aug 2020.
- 26.Statistics Sierra Leone SSL, Macro ICF. Sierra Leone demographic and health survey 2008. 2009. [Google Scholar]
- 27.Shea OR, Sarah S. Making the demographic and health surveys wealth index comparable: DHS methodologicla reports 9. 2014. [Google Scholar]
- 28.Najnin N, Bennett CM, Luby SP. Inequalities in Care-seeking for Febrile Illness of under-five children in urban Dhaka, Bangladesh. J Health Popul Nutr. 2011;29(5):523–531. doi: 10.3329/jhpn.v29i5.8907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kakwani NC. Measurement of poverty and negative-income tax. Aust Econ Pap. 1977;16(29):237–248. doi: 10.1111/j.1467-8454.1977.tb00603.x. [DOI] [Google Scholar]
- 30.Doorslaer E, O’Donnell O. Measurement and explanation of inequality in health and health Care in low-Income Settings. 2008. [Google Scholar]
- 31.Kakwani N, Wagstaff A, van Doorslaer E. Socioeconomic inequalities in health: measurement, computation, and statistical inference. J Econom. 1997;77(1):87–103. doi: 10.1016/S0304-4076(96)01807-6. [DOI] [Google Scholar]
- 32.Schilirò D, Kakwani NC. Income Inequality and Poverty. Methods of Estimation and Policy Application. Oxford University Press, 1980. Riv Internazionale Sci Sociali. 1982;XC:251–2.
- 33.O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M. Analyzing Health Equity Using Household Survey Data : A Guide to Techniques and Their Implementation. Washington, DC: World Bank. © World Bank; 2008. [Google Scholar]
- 34.QGIS. https://www.qgis.org/fr/site/forusers/download.html. Accessed 13 Aug 2020.
- 35.Novignon J, Ofori B, Tabiri KG, Pulok MH. Socioeconomic inequalities in maternal health care utilization in Ghana. Int J Equity Health. 2019;18(1):141. doi: 10.1186/s12939-019-1043-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Witter S, Brikci N, Harris T, Williams R, Keen S, Mujica A, Jones A, Murray-Zmijewski A, Bale B, Leigh B, Renner A. The free healthcare initiative in Sierra Leone: evaluating a health system reform, 2010-2015. Int J Health Plann Manag. 2018;33(2):434–448. doi: 10.1002/hpm.2484. [DOI] [PubMed] [Google Scholar]
- 37.Bilan 2017 de la gratuité des soins au profit de la femme et des enfants de moins de cinq au Burkina Faso. Regional Office for Africa. https://afro.who.int/fr/news/bilan-2017-de-la-gratuite-des-soins-au-profit-de-la-femme-et-des-enfants-de-moins-de-cinq-au. Accessed 23 Dec 2018.
- 38.Rebuild Consortium. Country situation analysis: Sierra Leone. 2011. p. 56. https://www.gov.uk/research-for-development-outputs/country-situation-analysis-sierra-leone#citation.
- 39.The World Bank. Physicians (per 1,000 people) - | Data. https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=SL. Accessed 3 Jun 2020.
- 40.The World Bank. Nurses and midwives (per 1,000 people) - Sierra Leone | Data. https://data.worldbank.org/indicator/SH.MED.NUMW.P3?locations=SL. Accessed 3 Jun 2020.
- 41.Vallières F, Cassidy EL, McAuliffe E, Gilmore B, Bangura AS, Musa J. Can Sierra Leone maintain the equitable delivery of their free health care initiative? Case for more contextualised interventions: results of a cross-sectional survey. BMC Health Serv Res. 2016;16:258. doi: 10.1186/s12913-016-1496-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Casagrande. Our work in Sierra Leone. Doctors with Africa CUAMM. 2015. https://doctorswithafrica.org/en/where-we-work/in-africa/our-work-in-sierra-leone/. Accessed 1 May 2021.
- 43.Shin YA, Yeo J, Jung K. The Effectiveness of International Non-Governmental Organizations’ Response Operations during Public Health Emergency: Lessons Learned from the 2014 Ebola Outbreak in Sierra Leone. Int J Environ Res Public Health. 2018(4):15. 10.3390/ijerph15040650. [DOI] [PMC free article] [PubMed]
- 44.Gamanga AH, Owiti P, Bhat P, Harries AD, Kargbo-Labour I, Koroma M. The Ebola outbreak: effects on HIV reporting, testing and care in Bonthe district, rural Sierra Leone. Public Health Action. 2017;7(Suppl 1):S10–S15. doi: 10.5588/pha.16.0087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.OCHA Sierra Leone. SIERRA LEONE –BONTHE DISTRICT PROFILE 2015. https://reliefweb.int/sites/reliefweb.int/files/resources/district_profile-bonthe-_29_dec_2015.pdf.
- 46.UNOCHA Sierra Leone. SIERRA LEONE –PUJEHUN DISTRICT PROFILE 2015. https://reliefweb.int/sites/reliefweb.int/files/resources/district_profile_-_pujehun-_29_dec_2015_.pdf.
- 47.UNOCHA Sierra Leone. SIERRA LEONE –WESTERN RURAL DISTRICT PROFILE 2015. https://reliefweb.int/sites/reliefweb.int/files/resources/final_district_profile_template_western_rural_10_dec_2015am%20(1).pdf.
- 48.UNOCHA Sierra Leone. SIERRA LEONE –PORT LOKO DISTRICT PROFILE 2015. https://reliefweb.int/sites/reliefweb.int/files/resources/district_profile_port_loko_29_dec2015.pdf.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study are available from the Demographic and Health Surveys program repository and are accessible after written request: https://dhsprogram.com/data.