

Background
Research investigating the role of emotion regulation (ER) in the development and treatment of psychopathology has increased in recent years. Evidence suggests that an increased focus on ER in treatment can improve existing interventions. Most ER research has neglected young people, therefore the present meta-analysis summarizes the evidence for existing psychosocial intervention and their effectiveness to improve ER in youth. A systematic review and meta-analysis was conducted according to the PRISMA guidelines. Twenty-one randomized-control-trials (RCTs) assessed changes in ER following a psychological intervention in youth exhibiting various psychopathological symptoms. We found moderate effect sizes for current interventions to decrease emotion dysregulation in youth (g = − 0.46) and small effect sizes to improve emotion regulation (g = 0.36). Significant differences between studies including intervention components, ER measures and populations studied resulted in large heterogeneity. This is the first meta-analysis that summarizes the effectiveness for existing interventions to improve ER in youth. The results suggest that interventions can enhance ER in youth, and that these improvements correlate with improvements in psychopathology. More RCTs including larger sample sizes, different age groups and psychopathologies are needed to increase our understanding of what works for who and when.
Electronic supplementary material
The online version of this article (10.1007/s00787-020-01498-4) contains supplementary material, which is available to authorized users.
Keywords: Emotion regulation, Psychopathology, Youth mental health, Meta-analysis, Psychological intervention
Introduction
Most common mental health disorders, including depression, substance abuse, eating disorders and anxiety have their onset during adolescence [1]. It has been argued that this peak in psychopathological symptoms results from developmental changes, which hamper emotion regulation (ER) [2]. ER has been broadly defined as “the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” [3]. These regulatory processes comprise physiological, experiential, behavioural, as well as psychological components [4]
The concept of ER has faced significant definitional challenges in the past decades, with hundreds of research papers referring to it each year in various direct and indirect ways, but the majority do not provide a clear definition. One of the most influential definitions has been presented by James Gross, who introduced the Process model of emotion regulation, according to which we are able to modify emotional experiences at different points throughout the ER process by implementing different ER strategies [4, 5]. Gross clustered the ER strategies into categories based on the point in time at which they are applied during the ER process: situation selection (e.g. “I am worried that I will do badly on the test today, so I might rather not go”), selection modification (e.g., “My mom dropped me off at school, although I wasn’t feeling well. I could turn around or perhaps, I can ask my friend Johnny for help before the test), attentional deployment to certain aspects of the situation (e.g., “I am so nervous, I can hear my heart racing. I will try distracting myself with some music”), cognitively changing the meaning of a situation (e.g.,” It would be bad if I failed this test today. Luckily there is another test in 4 weeks”), and finally modifying the response to the emotion eliciting event (e.g., “The test was a catastrophe”. I told my mom about it and cried. I was so sad. She gave me a hug and said: “We cannot change what happened, but we can prepare better for the next test”).
Past research has identified various ER strategies for each of the above stages. Frequently, researchers have attempted to divide them into maladaptive (e.g., catastrophizing, rumination, avoidance, suppression) or adaptive (e.g., problem-solving, acceptance, savouring, cognitive reappraisal) strategies depending on their assumed impact on psychopathological symptoms.
Emotion regulation and psychopathology
One of the most comprehensive systematic reviews by Aldao et al. [6] looked at the relationship between six different ER strategies and four different psychopathologies, including depression, anxiety, eating disorders and substance abuse. The authors found that the six strategies, avoidance, problem-solving, reappraisal, suppression, rumination and acceptance, were all associated with the different types of psychopathology. More specifically, they found that avoidance and suppression were positively associated with anxiety, depression and eating disorders, while rumination was positively associated with anxiety, depression, eating- and substance-abuse disorders. Problem-solving and reappraisal correlated negatively with psychopathological symptoms, while acceptance showed no significant association with depressive or anxiety symptoms. Further moderator analyses demonstrated that age (child vs. adult) significantly moderated the association between suppression, problem-solving, and depression, with adults showing significantly larger effect sizes than children. Age group was however not a significant moderator for the links between rumination and depression.
Aldao’s systematic review results were primarily based on data derived from adult studies, with only six of the 114 studies including data on children or adolescent samples. However, similar findings demonstrating the close association between emotion dysregulation and psychopathology have also been reported for studies focusing on young populations. Schäfer et al. [7] summarized the evidence for different ER strategies in youth exhibiting sub-clinical symptoms of anxiety and depression. Similarly, they found that depression and anxiety had the strongest positive association with avoidance and rumination; but the strongest negative association with acceptance. Their review focused on adolescents in the ages of 13–18 years with sub-clinical symptoms, therefore no conclusions could be made regarding younger groups or those displaying severe clinical symptoms. Evidence from studies looking at other youth mental disorders such as attention-deficit/hyperactivity disorder, conduct disorder, eating disorders and borderline-personality disorder have reported similar patterns [8–11].
Most research looking at ER in clinical populations has focused on emotion dysregulation and strategies to regulate negative emotions, such as sadness or anger; while ER as an ability or positive ER strategies (e.g. savouring or gratitude) have been widely neglected [12]. Hence in the present review the term emotion dysregulation will refer to having difficulties, while the term emotion regulation will refer to abilities or skills. Furthermore, it will include both, strategies to regulate positive as well as negative emotions. Additionally, Aldao et al. [13, 14] highlighted that effective ER does not come down to mere down regulation of negative emotions and upregulation of positive emotions, but whether the individual is able to flexibly apply strategies that match the respective situation. Hence the present systematic review will also include ER measures that assess flexible ER.
Despite the growing evidence highlighting the importance of ER in the development of youth psychopathology, it remains unclear whether ER difficulties are a risk factor or a consequence of psychopathology. Until now, only a few studies have shed light on the nature of this relationship. McLaughlin et al. [15] investigated emotion dysregulation patterns in adolescents exhibiting different psychopathological symptoms (i.e. depression, anxiety, aggression, eating pathology) before and after a seven month period. They found that emotion dysregulation (in their study a latent factor based on low emotional understanding, emotion expression and ruminative response to distress), predicted increased symptoms seven months later for all psychopathologies, but depression. Emotion dysregulation on the other hand was not predicted by earlier psychopathological symptoms. Due to the limited availability of longitudinal studies so far, another way to explore this relationship would be through intervention studies that include mediation analyses, based on which one could conclude whether changes in ER lead to changes in psychopathology.
Emotion regulation in interventions
Due to findings relating ER to a wide range of mental disorders, ER has been argued to represent a transdiagnostic core feature underlying these disorders [16]. Transdiagnostic frameworks propose that multiple mental disorders are caused and maintained by a similar subset of underlying processes, which finds further support in high comorbidity rates among the disorders and observations showing that different disorders respond to similar treatments. Following this, it has been suggested that psychological interventions can be improved by having an increased focus on ER [17], as it is the case in most third wave interventions including mindfulness-based cognitive therapy (MBCT), dialectical-behavioural therapy (DBT) or acceptance-based behavioural therapy (ACT). Evidence from the adult literature indicates that promising psychological interventions did improve ER, and that these improvements mediated decreases in psychopathological symptoms [18]. Sloan et al. [19] recently examined whether changes in ER related to symptom reduction in anxiety, depression, substance abuse, eating and borderline personality disorder. They found that the use of maladaptive ER strategies improved following treatment, regardless the type of intervention or disorder. However, their systematic review only included participants older than 13 years.
Objective
The present meta-analysis aims to summarize the effectiveness of psychological interventions to improve ER in youth. To our knowledge there is no meta-analysis that has looked at research involving youth samples. Moreover, it focuses on emotion dysregulation, related strategies as well as ER abilities and related strategies. Finally, mediation analyses of changes in ER and psychopathology in response to interventions will be summarized.
We aim to answers the following research questions:
Do existing psychological interventions effectively improve emotion (dys-) regulation in youth?
Are improvements in emotion (dys-) regulation associated with changes in psychopathological symptoms?
Methods
Literature search
We followed the PRISMA guidelines for the present systematic review [20]. The literature search of the electronic databases was conducted on the 4th of December, 2017 and updated on the 9th of April, 2018 using the following electronic databases: Ovid/Medline, Ovid PsychINFO and Web of Science (a detailed overview of the search strategy can be found in the supplementary materials). Identified publications were downloaded from the databases and saved to a reference manager on the dates specified above. If relevant literature reviews were identified during the abstract screening process (see below), we manually screened their reference lists for further important publications. Our literature search was restricted to peer-reviewed journal articles written in English. Peer-reviewed publications have been assumed to increase the inclusion of studies with higher research quality.
Inclusion and exclusion criteria
Inclusion criteria
Children and adolescents between the ages of 6–24 years. Research with younger children was excluded because it primarily involves observational methods. In line with recent definitions of “adolescence” we included the age of 24 [21].
Sample with depression, anxiety, eating disorder, substance abuse, attention-deficit hyperactivity disorder, borderline personality disorder symptom, as these have been shown to share common ER difficulties [6, 7, 19].
Intervention aims to improve ER and symptoms relating to any of the mental health disorders mentioned above.
Randomized and quasi-randomized control studies
Any control condition
Self-, parent, teacher or professional report through validated ER measure
Exclusion criteria
Adult population
Symptoms not relating to disorders mentioned above
No measure of emotion regulation included
Special populations (e.g. autism spectrum disorder, intellectual impairment, medical condition)
Medical or pharmacological intervention
No manual or description of intervention and the assumed active component
No control group present
Studies reporting outcomes of neural correlates only (e.g., fMRI)
Study selection
All identified articles were added to a systematic review software (Eppi-Reviewer). Duplicates were removed and abstracts and titles were screened based on the inclusion and exclusion criteria. The method section of each paper was screened for valid ER measures. All studies with a valid ER measure entered the full-text screening stage. A second researcher (D.M) randomly reviewed and rated 25% of the selected title and abstract papers. Where there was a disagreement (4%) regarding the inclusion of a study, the two researchers reviewed the article and discussed its eligibility until an agreement was achieved.
Data extraction
Information relating to study characteristics including: authors, year of publication, study design, intervention type, definition and measurement of ER, comparison group, study results (including sample size, age group, participation rate, attrition, relevant clinical and ER outcomes) and information to determine any study bias was extracted from each study. Correlations between changes in ER and clinical outcomes were collected if reported. Coding options for categorical variables are provided in the supplementary materials.
Outcome measures
Emotion regulation and dysregulation
Studies with any validated self-report measure to assess ER difficulties or skills, either as a single factor or in terms of the ER strategies, were included (see supplementary materials for an overview of included measures). We used Adrian et al. [22] review of emotion regulation assessment and similar reviews [6, 19] as guidance to decide on a measures’ eligibility. The authors of the present review acknowledge that some ER measures may have substantial overlap with measures assessing psychopathological symptoms, which are addressed in more detail in the discussion. The two meta-analyses included (a) studies that assessed emotion dysregulation (i.e., lack of access to strategies, difficulties accepting negative emotions) or any of the associated maladaptive ER strategies including: avoidance, suppression, catastrophizing, rumination and (b) ER ability (e.g., ER flexibility, emotional understanding) and any of the associated adaptive ER strategies including: acceptance, savouring, gratitude, cognitive reappraisal, problem solving and mindfulness (a complete list is provided in the supplements). We extracted all available data reported for subscales and overall mean scores. If possible we calculated overall mean scores, based on the subscales data provided. For the meta-analyses, all available effect sizes (subscale or full scale) were combined according to their categorization into emotion regulation or dysregulation (see supplements for coding scheme).
Psychopathology
Is treated as a secondary outcome measures in the present review as it was only used to answer our second research question, regarding the association between change in ER and change in psychopathology in response to treatment. Psychopathology symptoms were either based on self-report measures or clinician ratings (e.g., Beck Depression Inventory). If a study reported more than one scale for the same disorder category, we chose one measure based on its reliability and whether it had been used in one of the other studies in the present review. Reported mean scores were used to calculate standardised effect sizes, which were then entered in the meta-regression analysis.
Quality and risk of bias assessment
Two researchers (BM and DM) independently assessed the methodological quality of the included studies (interrater agreement = 98%) using the Effective Public Health Practice Project Quality Assessment tool (EPHPP). The EPHPP evaluates the quality of each study based on their rating, ranging from strong, moderate to weak, across the following six categories: selection bias, study design, the presence of confounding variables, blinding, data collection methods, and participant withdrawals and drop-outs. The EPHPP has been reported suitable for systematic reviews and evidence has shown good content and construct validity [23, 24].
Data analysis
A primary analysis was conducted to detect any influential studies in the data-set. This was done through the “metaninf” command in Stata, which indicates each study’s impact on the overall effect size if that study is omitted from the analysis. Furthermore, we assessed each studies level of heterogeneity through a Galbraith plot (“galbr” command in Stata) [25]. Studies with a great impact on the overall effect size and larger than expected level of heterogeneity, were regarded as influential studies. Subsequent meta-analyses were conducted with and without these studies, in order to identify their respective impact on the results. In line with current recommendations for meta-analysis models in psychology, we conducted two random effects models: one with emotion dysregulation as a primary outcome and one with ER abilities as the primary outcome [26]. To explore sources of heterogeneity we conducted a series of sub-group analyses. Subgroup analyses help identify whether there are differences in effect size or heterogeneity due to study-level factors (see “Meta-regression and subgroup-analyses” for more detail below). Furthermore, we conducted a meta-regression with effect size as the dependent variable and intervention type, age group, control group and quality rating as the predictor variables. A combination of these two approaches has been recommended [27]. In order to answer the second research question we conducted a second meta-regression, with effect sizes of psychopathological symptoms as the dependent variable, and effects sizes of improved ER as the predictor variable.
Effect sizes
Treatment effect was estimated using the weighted mean effect size Hedges’ g. Hedges’ g is interpreted like Cohen’s d, with effect sizes ranging from small (0.2), medium (0.5) to large (0.8) [28]. Hedges’g (see Formula 1) and the standard error were calculated based on standardized mean-differences, standard deviations and sample sizes. This data was entered into Stata and the “meta” command was used to conduct the random effects models.
| 1 |
Formula 1—Hedges’ g.
For studies with multiple treatment groups, the decision on how to include them, was made on a case-by-case basis with regards to the research question. In accordance with the Cochrane handbook the following options were considered [29]:
One of the treatment conditions was excluded if the treatment’s main target was not ER or any related concept and did therefore not add any additional insight to the research question.
Effect sizes of two treatment groups were pooled and compared to the control group, if the intervention groups were similar enough to be combined.
Each treatment group was entered as a single comparison group, by splitting the control group in half, if combining or excluding one condition would have resulted in loss of information. This approach was adopted where both interventions were assumed to improve ER, but differences between the conditions added valuable insights, e.g., whether one intervention could be more effective than the other.
Heterogeneity
Heterogeneity between the studies was assessed with the Q statistic, I2 and T2. The Q test follows the chi-square distribution and estimates the probability of sampling error being the only cause for variance. A significant Q test indicates that heterogeneity is present. However, it does not provide sufficient information about the source of heterogeneity. Therefore, I2 and T2 were also taken into account. T2 describes the between-study variance, while I2 describes what proportion of the observed variance in the effect estimates is due to systematic differences between the studies rather than sampling error. Smaller values of I2 suggest that the observed heterogeneity is mostly random, while larger values suggest study-level differences. The following levels of heterogeneity have been identified for I2: low: I2 = 25%, medium: I2 = 50%, and high: I2 = 75% [30]. We also calculated 95% prediction intervals (PI; see Formula 2) [31], which aim to predict the range of possible population parameters in future empirical studies (e.g., we expect that in future studies 95% of the true effects lie within this interval). Hence, PI’s are different from confidence intervals, which estimate the precision of the mean effect size in the general population.
| 2 |
Formula 2—prediction interval
Meta-regression and subgroup analyses
A meta-regression was performed to identify possible moderating effects of certain between study-level characteristics. The meta-regression was conducted with the “meta regress” command in Stata 16. Categorical variables are automatically dummy-coded by the software and the resulting estimates indicate how the effect size of each subgroup differs with respect to the chosen reference group. Furthermore, separate subgroup analyses with each relevant moderator were conducted to explore potential sources of heterogeneity and their impact on the overall effect size. With respect to the present research question the following subgroup analyses were conducted:
Type of intervention: distinguished between two types of interventions, those with a specific focus on ER (e.g., emotion focused CBT, emotion regulation training, or any of the third wave interventions) and non-specific interventions (e.g., standard CBT, motivational interviewing). An intervention was coded as ER specific, if they included specific ER modules or tasks; or if these were stated to take up most of the content or time, compared to other modules in the intervention programme. (See Table 5 in supplements for intervention descriptions).
Type of control group: compared studies with active versus passive control groups. Passive control groups included studies with a waitlist or assessment-only design, while active control groups included any type of intervention, including treatment as usual.
Type of emotion regulation strategy: compared studies based on different types of ER strategies. Subgroups could only be formed if sufficient data was available. (See supplements for specific ER strategies).
Type of disorder: compared effectiveness of studies relating to different types of disorders. Studies were categorized based on the authors’ description of the recruited sample and the diagnostic tools employed. Six main categories were included: (a) anxiety disorders, including generalized anxiety, phobias, PTSD, obsessive compulsive disorder; (b) depression, including major depressive disorder, bipolar disorder, suicidal thoughts; (c) ADHD; (d) borderline personality disorder; (e) substance abuse (f) eating disorders.
Age groups: differences in effectiveness for different age groups was explored by creating a new categorical variable for age with four levels. Studies with a participant mean age under 10 years, were categorised as “child” population. “Early adolescence” included samples with a mean age between 10 and 13 years. Studies with participants older than 13 years, but younger than 17 were categorised as “adolescence”. The fourth category “late adolescence” included all samples with a mean age larger than 17 years but younger than 25 years.
Quality of study: to investigate whether there was a difference in effect size depending on quality ratings. Studies were rated as being of low (3), moderate (2) or high (1) quality.
Publication bias
Publication bias was visually assessed with the help of a funnel plot. No publication bias was assumed if the points in the scatter plot form the shape of a funnel, while an asymmetrical shape suggests a publication bias. Furthermore, the Egger’s test was applied to test for small-study effects whereby precision seems to be related to the effect size estimate. Fail-safe N statistics were not performed due to unreliability [32]
Relationship between ER and psychopathological symptoms
To assess whether improvements in psychopathological symptoms were associated with changes in ER, a meta-regression was conducted, with effect sizes of psychopathological symptoms as the dependent variable, and effects sizes of improved ER as the predictor variable.
Results
Study selection
The search identified 1418 articles. After duplicates (n = 171) were removed 1250 papers were included for the abstract and title screening. 1049 articles were excluded based on the abstract and title screening. Of the remaining 201 papers, 122 papers had to be excluded due to missing ER measures. In total, 79 studies entered the full-text screening, of which 34 studies matched the selection criteria and provided sufficient data. Another 17 studies, matched the criteria, but the authors had to be contacted to provide additional information that could not be derived from the published article. During the data extraction phase 30 studies were excluded. Four of those were excluded because the authors were not accessible [33–36]. Finally, 21 independent studies were included in the meta-analysis, from which 33 treatment effects were extracted (19 emotion dysregulation, 14 emotion regulation; see Fig. 1 for study selection process).
Fig. 1.

Flow diagram
General study characteristics
The characteristics of the included studies are summarized in Table 1. For studies with multiple treatment conditions, where both treatment conditions were assumed to have an effect on ER, both groups were included in the analysis, by splitting the control group in half and pairing it with each treatment group. For the remaining studies (k = 3), the second treatment group was excluded. All of the included studies showed a large variety regarding the type of ER measure and intervention employed a detailed description of these is provided in the supplementary materials, see Table 5. CBT was the most commonly employed intervention (k = 16) and almost all interventions included some kind of CBT components. Eight studies stated to specifically address emotion dysregulation (i.e. emotion regulation training). Four interventions targeted specific ER strategies (i.e., rumination or mindfulness; see Table 1).
Table 1.
Study characteristics
| Study | Psychopathology | Design | N | Age | Conditions | ER measure | Quality rating |
|---|---|---|---|---|---|---|---|
| Slee et al. (2008)—The Netherlands | BPD | RCT | 82 | 24.2 | CBT − TAU | DERS | Strong |
| Schuppert et al. (2012)—The Netherlands | BPD | RCT | 109 | 15.98 | ERT − TAU | LPI subscale—emotion dysregulation | Strong |
| Suveg et al. (2017)—USA | AD | RCT | 92 | 8.93 | ECBT − CBT | ERC | Moderate |
| Dingle et al. (2017)—Australia | AD, MD | RCT | 51 | 18.68 | ERP − WL | DERS | Moderate |
| Hides et al. (2011)—Australia | MD, SUB | RCT | 88 | 19.2 | CBT + MI – TAU | CISS | Weak |
| Atkinson et al. (2016)—Australia | ED | RCT | 33 | 20.57 |
MF − WL Dissociationa |
FFMQ | Weak |
| Azrin et al. (2001)—USA | CD, SUB | RCT | 56 | 15.4 | CPS − FBT | SPSI-R | Moderate |
| Stasiak et al. (2014)—New Zealand | MD | RCT (pilot) | 34 | 15.2 | cCBT − TAU | ACS-PS | Moderate |
| Jacobs et al. (2016) | MD | RCT | 33 | 15.5 | RCBT − WL | RRS | Strong |
| Livheim et al. (2015)—Australia | MD | QRCT | 51 | 14.6 | ACT − TAU | AFQ | Strong |
| 1Livheim et al. (2015)—Sweden | MD | RCT | 32 | 14.5 | ACT − TAU | AFQ, MAAS | Weak |
| Kaufman et al. (2005)—USA | MD, CD | RCT | 93 | 15.1 | CBT − LS | IC-PS | Strong |
| Hennesdottir et al. (2017)—Iceland | ADHD | RCT (pilot) | 30 | 9.2 |
CBT − WL Parent traininga |
ERC | Strong |
| Meisner-Stedman et al. (2017) | AD | RCT | 29 | 24.56 | CTPTSD − WL | Rumination items | Strong |
| 1Essau et al. (2012)—Germany | AD | CRCT | 638 | 10.91 | CBT − WL | CSCY-PS | Moderate |
| Latimer et al. (2003)—USA | SUB | RCT (pilot) | 43 | 16.07 | CBT − DHPE | SPSI | Moderate |
| Winters et al. (2012) | SUB | QRCT | 192 | 16.13 |
MI-A − WL MI-Pa |
PSQ | Moderate |
| Smith et al. (2015) | MD | RCT | 109 | 13–16 | cCBT − WL | CRSQ | Strong |
| Fitzpatrick et al. (2005)—USA | MD | RCT | 94 | 19.02 | PS − Health Education | SPSI-R | Moderate |
| Multi-treatment trials entered with split groups | |||||||
| Hancock et al. (2016)—Australia | AD | RCT | 99 | 13.8 | ACT − WL | AFQ | Strong |
| AD | RCT | 94 | 13.8 | CBT − WL | AFQ | Strong | |
| Afshari et al. (2014)—Iran | AD | RCT | 77 | 10.57 | ERT− WL | CERQ, CEMS | Weak |
| AD | RCT | 55 | 10.57 | CBT− WL | CERQ, CEMS | Weak | |
BPD borderline personality disorder, AD anxiety disorder, MD major depression, SUB substance abuse, ED eating disorder, CD conduct disorder, ADHD attention deficit hyperactivity disorder, RCT randomized control trial, QRCT quasi-randomized control trial, CBT cognitive behavioural therapy, TAU treatment as usual, ERT emotion regulation training, ECBT emotion-focussed CBT, ERP emotion regulation program, WL waitlist, MI motivational interviewing, MF mindfulness, CPS cognitive problem solving, FBT family behavioural therapy, cCBT computerized CBT, RCBT rumination focussed CBT, ACT acceptance and commitment therapy, LS life skills, CT-PTSD cognitive therapy for PTSD, DGPE drugs harm psychoeducation curriculum, MIA motivation interviewing adolescence, MI-P motivation interviewing parents, PS problem solving, DERS difficulties with emotion regulation scale, LPI life problems inventory, ERC emotion regulation checklist, CISS coping inventory for stressful situations, FFMQ five factor mindfulness questionnaire, SPSI-R social problem solving inventory-revised, ACS-PS adolescent coping scale-problem solving, RRS ruminative response scale, AFQ avoidance and fusion questionnaire, MAAS mindful attention awareness scale, IC-PS issues checklist-problem solving, CSCY coping scale for children and youth, PSQ problem solving questionnaire, CRSQ child response style questionnaire, CERQ cognitive emotion regulation questionnaire, CEMS children’s emotion management scale
aCondition was part of multi-treatment trial and was excluded from meta-analysis 1outlier study removed from main analysis
Quality and publication bias
Quality ratings for each study are shown in Table 1. All studies were randomized control studies, however nine studies reported baseline differences between the groups, while two studies did not provide any information on potential baseline differences. One study did not provide any information about the control condition, six studies compared the intervention with a treatment as usual condition.
Meta-analysis: effectiveness of interventions to reduce emotion dysregulation
The first random effects model was based on the original 19 effect sizes from 17 independent studies, which indicated a medium treatment effect (g = 0.52), 95% CI [− 0.86, − 0.18], p < 0.001). Due to large heterogeneity I2 = 90.87% (Q = 129.64, df = 18, p < 0.001), we decided to run the “metainf” command and a Galbraith plot to identify highly influential studies [25, 37]. The results (see Plots 1 and 2 in supplementary materials) indicated that two studies, one by Slee et al. [38] and one of Livheim and colleague’s studies (based in Sweden [39]) had a significant impact on the overall effect size, while also contributing to a large amount of heterogeneity. We regarded these studies as highly influential studies and removed them from the main model, which effectively decreased the level of heterogeneity by I2 = 18.05% [37]. (Results of the full and the reduced meta-analysis model are presented in Table 2 and supplementary materials). Results of the reduced model are discussed in more detail below.
Table 2.
Random effect models and sub-group analyses with emotion dysregulation as outcome
| Reduced data set | m | k | n | Hedges g | 95% CI | p (z test) | Q | p (Q) | T2 | I2 (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Emotion dysregulation | 17 | 15 | 1744 | − 0.46 | − 0.67, − 0.26 | 0.00 | 54.06 | 0.00 | 0.12 | 72.82 |
| Emotion dysregulation by | ||||||||||
| Intervention | ||||||||||
| CBT intervention | 8 | 8 | 1058 | − 0.40 | − 0.64,− 0.15 | 14.84 | 0.02 | 0.06 | 59.37 | |
| ER intervention | 7 | 7 | 598 | − 0.51 | − 0.82,− 0.20 | 23.34 | 0.00 | 0.46 | 70.38 | |
| Control group | ||||||||||
| Active control | 8 | 8 | 532 | − 0.19 | − 0.41, − 0.03 | 10.44 | 0.11 | 0.03 | 39.45 | |
| Passive control | 9 | 7 | 1212 | − 0.66 | − 0.93, − 0.39 | 39.33 | 0.00 | 0.12 | 71.47 | |
| Quality rating | ||||||||||
| Strong | 9 | 8 | 612 | − 0.59 | − 0.85, − 0.33 | 16.35 | 0.02 | 0.08 | 57.22 | |
| Moderate | 5 | 5 | 973 | − 0.13 | − 0.26, − 0.01 | 5.95 | 0.31 | 0.00 | 0.0 | |
| Weak | 3 | 2 | 159 | − 0.81 | − 1.40, − 0.22 | 6.38 | 0.04 | 0.18 | 66.58 | |
| Full-data set | ||||||||||
| Emotion dysregulation | 19 | 16 | 1851 | − 0.52 | − 0.86, − 0.18 | 0.00 | 129.64 | 0.00 | 0.49 | 90.87 |
| Emotion dysregulation by | ||||||||||
| Intervention | ||||||||||
| CBT intervention | 8 | 8 | 1143 | − 0.71 | − 1.26,− 0.15 | 73.69 | 0.00 | 0.58 | 93.20 | |
| ER intervention | 9 | 8 | 623 | − 0.35 | − 0.80, 0.10 | 44.07 | 0.00 | 0.40 | 86.54 | |
| Control group | ||||||||||
| Active control | 8 | 8 | 639 | − 0.32 | − 0.99, − 0.35 | 90.31 | 0.00 | 0.98 | 94.03 | |
| Passive control | 9 | 7 | 1212 | − 0.66 | − 0.92, − 0.39 | 38.31 | 0.00 | 0.12 | 70.89 | |
| Quality rating | ||||||||||
| Strong | 9 | 8 | 691 | − 0.86 | − 1.35, − 0.36 | 61.08 | 0.00 | 0.50 | 89.23 | |
| Moderate | 6 | 6 | 973 | − 0.13 | − 0.26, − 0.01 | 5.74 | 0.33 | 0.00 | 0.0 | |
| Weak | 4 | 3 | 187 | − 0.81 | − 1.37, − 0.84 | 33.81 | 0.02 | 1.16 | 91.87 | |
The forest plot and confidence intervals (CI) show that eight studies significantly reduced emotion dysregulation (CIs are entirely on the negative side), while the remaining studies (k = 9) showed no significant treatment effect (Fig. 2). Overall, the results indicate a medium treatment effect (g = − 0.46), 95% CI [− 0.67, − 0.26], p < 0.001). The confidence interval (no value of 0 is present), and the z statistic (z = − 4.44, p < 0.001) suggest that the null hypothesis (H0: intervention had no impact on emotion dysregulation) can be rejected. The Q statistic (Q = 54.06, df = 16, p < 0.001) indicated that the effect sizes differed significantly across the studies. I2 of 72% suggests that most of the observed variance was due to differences on a study-level. T2 of 0.12 suggests a small amount of absolute dispersion. Calculation of the 95% PI [− 0.67, − 0.25] suggests that the true effect size of a similar future study would fall within this range in 95% of the time. Most of the PI lies in the negative range, thereby indicating that interventions would be effective in most settings [30, 31].
Fig. 2.

Forest plot: random-effects model (reduced) with emotion dysregulation as primary outcome
Meta-analysis: effectiveness of interventions to enhance emotion regulation
The original random effects model was based on 14 effect sizes from 13 independent studies with ER abilities as an outcome. The full model indicates a treatment effect of (g = 0.43, 95% CI [0.18, 0.69], p < 0.001).The metaninf and the Galbraith plot suggested two influential studies, Livheim et al. [40] and Essau et al. [41] (see supplementary material Plots 3 and 4). In comparison to Essau et al. (N = 638), the study by Livheim (N = 25) was significantly underpowered, hence we decided to remove this study from the following analysis. (Results of the full and the reduced model are both presented in Table 3). The forest plot of the reduced model indicated that three studies [41–43] showed a significant positive effect, while the remaining 10 studies had no significant effects (see Fig. 3). Overall, the results suggest a small treatment effect (g = 0.36, 95% CI [0.14, 0.58], p < 0.001). Based on the CI and the z statistic (z = 3.22, p < 0.001), the null hypothesis that the intervention has no impact on ER was rejected. The Q statistic (Q = 66.56, df = 12, p < 0.001) suggests that effect sizes differed significantly across the studies. I2 of 70.8% suggests that most of the observed variance was due to differences on a study level (e.g., sampling error). T2 of 0.10 suggests a small amount of between-study variance. The 95% PI = [0.14, 0.58] is in the positive range, suggesting that future studies will most likely find a positive effect size within this range [30, 31].
Table 3.
Random effect models and sub-group analyses with emotion regulation as outcome
| Reduced data set | m | k | n | Hedges g | 95% CI | p (z test) | Q | p (Q) | T2 | I2 (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Emotion regulation | 13 | 12 | 1513 | 0.36 | 0.14, 0.58 | 0.00 | 66.56 | 0.00 | 0.010 | 70.80 |
| Emotion regulation by | ||||||||||
| Intervention | ||||||||||
| CBT intervention | 8 | 8 | 969 | 0.45 | 0.15, 0.75 | 35.96 | 0.00 | 0.12 | 71.32 | |
| ER intervention | 4 | 4 | 269 | 0.22 | − 0.15, 0.58 | 58.86 | 0.06 | 0.08 | 58.86 | |
| Control group | ||||||||||
| Active control | 8 | 8 | 521 | 0.20 | − 0.01, 0.42 | 9.99 | 0.19 | 0.03 | 32.10 | |
| Passive control | 5 | 4 | 992 | 0.57 | 0.22, 0.93 | 25.71 | 0.00 | 0.12 | 77.35 | |
| Quality rating | ||||||||||
| Strong | 1 | 1 | 82 | 0.53 | 0.09, 0.96 | 0.00 | – | |||
| Moderate | 7 | 7 | 1148 | 0.29 | − 0.07, 0.65 | 63.03 | 0.00 | 0.19 | 84.30 | |
| Weak | 5 | 4 | 283 | 0.44 | 0.20, 0.68 | 1.82 | 0.77 | 0.00 | 0.00 | |
| Full-data set | ||||||||||
| Emotion regulation | 14 | 13 | 1538 | 0.43 | 0.18, 0.69 | 0.00 | 77.82 | 0.00 | 0.16 | 77.89 |
| Emotion regulation by | ||||||||||
| Intervention | ||||||||||
| CBT intervention | 7 | 7 | 969 | 0.58 | 0.30, 0.85 | 59.96 | 0.00 | 0.07 | 59.96 | |
| ER intervention | 5 | 5 | 321 | 0.57 | − 0.17, 1.32 | 23.53 | 0.00 | 0.63 | 90.13 | |
| Control group | ||||||||||
| Active control | 9 | 9 | 546 | 0.37 | 0.01, 0.73 | 26.64 | 0.00 | 0.22 | 75.35 | |
| Passive control | 5 | 4 | 992 | 0.57 | 0.22, 0.93 | 25.71 | 0.00 | 0.12 | 77.35 | |
| Quality rating | ||||||||||
| Strong | 1 | 1 | 82 | 0.53 | 0.09, 0.96 | 0.00 | – | |||
| Moderate | 7 | 7 | 1148 | 0.29 | − 0.07, 0.65 | 63.03 | 0.00 | 0.19 | 84.30 | |
| Weak | 5 | 4 | 308 | 0.63 | 0.16, 1.10 | 14.38 | 0.01 | 0.24 | 72.89 | |
Fig. 3.

Forest plot: random-effects model (reduced) with emotion regulation as primary outcome
Heterogeneity and bias assessment
To explore possible causes of heterogeneity and investigate whether effect sizes varied for certain subgroups, a meta-regression and subgroup analyses were conducted (see Tables 2, 3, 4).
Table 4.
Meta- regression with effect size as dependent variable and potential moderators as predictors
| Predictor variables | Emotion dysregulation | Emotion regulation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | z | p | 95% CI | β | SE | z | p | 95% CI | |
| Intercept | − 0.48 | 0.19 | − 2.54 | 0.01 | − 0.86,− 0.11 | 1.24 | 0.56 | 2.19 | 0.02 | 0.13, 2.35 |
| Intervention | ||||||||||
| CBT intervention | ||||||||||
| ER intervention | − 0.27 | 0.21 | − 1.32 | 0.18 | − 0.69, 0.13 | 0.23 | 0.29 | 0.81 | 0.41 | − 0.33, 0.81 |
| Control group | ||||||||||
| Active control | ||||||||||
| Passive control | 0.24 | 0.21 | 1.18 | 0.23 | − 0.16, 0.66 | − 0.63 | 0.32 | − 1.92 | 0.05 | − 1.27, 0.01 |
| Quality rating | ||||||||||
| Strong | ||||||||||
| Moderate | 0.07 | 0.36 | 0.22 | 0.82 | − 0.63, 0.79 | − 0.42 | 0.35 | − 1.20 | 0.23 | − 1.11, 0.26 |
| Weak | − 0.72 | 0.52 | − 1.39 | 0.16 | − 1.75, 0.29 | − 0.34 | 0.34 | − 1.01 | 0.31 | − 1.01, 0.32 |
| Age group | ||||||||||
| Child | 0.55 | 0.46 | 1.20 | 0.23 | − 0.35, 1.45 | − 0.54 | 0.41 | − 1.32 | 0.18 | − 1.35, 0.26 |
| Early adolescence | 0.23 | 0.42 | 0.55 | 0.58 | − 0.60, 1.07 | 0.20 | 0.36 | 0.56 | 0.57 | − 0.51, 0.92 |
| Adolescence | ||||||||||
| Late adolescence | 0.13 | 0.41 | 0.32 | 0.75 | − 0.68, 0.95 | − 0.08 | 0.29 | − 0.29 | 0.77 | − 0.66, 0.49 |
Moderator meta-regression
Emotion dysregulation
The meta-regression model with effect size (k = 17) as the dependent variable and age group, intervention type, quality of study and control group as predictor variables, was non-significant (χ2 = 14.37, p = 0.07) thereby suggesting that none of the coefficients in the model, apart from the intercept, are significantly different from zero. Similarly, none of the moderators had a significant impact on the overall effect size. Furthermore, the I2 index (66%) suggest a moderate level of heterogeneity in the model and that only 31.5% of the between-study variance is explained by the moderators (R2 = 31.47). Based on the meta-regression results none of the included study-level factors seem to influence the overall effect-size. However, with respect to recent meta-regression recommendations, one should not conclude that a covariate is unrelated to the effect size if there are less than ten studies per covariate [44]. Consequently, we explore this further relationship further in the subgroup analyses.
Emotion regulation
The meta-regression model with effect size (k = 13) as the dependent variable was significant (χ2 = 20.58, p < 0.05) thereby suggesting that at least one of the coefficients in the model, apart from the intercept, is significantly different from zero. The results indicate that the control group variable had a significant impact on effect size (see Table 4). The I2 index (40%) suggest a moderate to small level of heterogeneity in the model and that 75% of the between-study variance is explained by the moderators in the model (R2 = 75.09). As stated above, due to the limited amount of studies per covariate in the model, the following subgroup-analyses were conducted to explore this relationship further.
Subgroup analysis: type of intervention
Emotion dysregulation
The results indicate that for individuals who received a specific ER intervention, emotion dysregulation decreased by g = − 0.51, and in non-specific interventions emotion dysregulation decreased by g = − 0.40. This suggests that interventions with a greater focus on ER could be more effective in reducing ER difficulties. However, the large amount of heterogeneity (I2 = 70% and 59%) makes direct comparisons between the subgroups difficult. This is also supported by the non-significant test of group differences (Qb (2) = 0.36, p = 0.84) (see Fig. 6 in supplements).
Emotion regulation
The results indicate that for individuals who received a specific ER intervention, emotion regulation improved by g = 0.22, and in non-specific interventions emotion regulation improved by g = 0.45. Heterogeneity is large for all subgroups (71% and 58%) and the test of group difference non-significant (Qb (2) = 1.29, p = 0.51). Furthermore, one of the subgroups only consisted of fours studies, which has been considered as too small to derive definite conclusions (see Fig. 7 in supplements).
Subgroup analysis: type of control group
Emotion dysregulation
The results indicate that for studies with an active control condition ED decreased by g = − 0.19, while for studies with passive control conditions ED decreased by g = − 0.66. The significant Q statistic (Q = 6.88, df = 1, p < 0.001), suggests that the true mean effect varies depending on the type of control condition. Heterogeneity within the active control subgroup was significantly lower (I2 = 39%) compared to the passive control subgroup (I2 = 71%). Thus differentiating between types of control groups partially explained the level of heterogeneity (see Fig. 8 in supplements).
Emotion regulation
Similarly, for ER effect sizes, studies with an active control condition improved ER by g = 0.20, while for studies with passive control conditions ER improved by g = 0.57. The significant Q statistic (Q = 3.09, df = 1, p < 0.001), suggests that the true mean effect varies depending on the type of control condition. Heterogeneity within the active control subgroup was significantly lower (I2 = 32%) compared to the passive control subgroup (I2 = 77%, see Fig. 9 in supplements)).
Subgroup analysis: type of disorder and ER strategy
Subgroup analyses for different types of disorders and different ER strategies were conducted, but due to insufficient numbers of studies (n ≤ 4) in the respective subgroups no meaningful interpretations were possible. (Results of these are provided in the supplementary materials, see Figs. 10 and 11.)
Subgroup analysis: age group
Emotion dysregulation
Subgroup analyses for different age groups indicate that that ED decreased by g = − 0.16 in children, g = − 0.62 in early adolescence, g = − 0.45 in adolescents and g = − 0.59 in late adolescents. Heterogeneity is large for all subgroups (50–89%) and the test of group difference non-significant (Qb (3) = 1.28, p = 0.73). Furthermore, apart from the age group “adolescence” all other subgroups only consisted of 2–3 studies, which has been considered as too small to derive definite conclusions (see Fig. 12 in supplementary materials).
Emotion regulation
Subgroups in this analysis did not exceed more than four studies per group, which is suggested to be too small in order to derive meaningful interpretations. (Results of these are provided in the supplementary materials, see Fig. 13.)
Subgroup analyses: quality rating
Emotion dysregulation
Studies (k = 7) with strong quality ratings decreased ED by g = − 0.59, which was higher than the overall effect-size g = − 0.46. Studies of moderate quality (k = 6) had smaller effect sizes g = − 0.13, while studies with the lowest quality ratings (k = 2) decreased ED by g = − 0.81.
Emotion regulation
For ER only one study was rated as strong (g = 0.53), while the other studies were moderate (k = 7, g = 0.29) or weak (k = 4, g = 0.44). Due to the limited number of studies, we recommend that these results are treated with caution.
Publication bias
The contour-enhanced funnel plot (see Fig. 4) shows an asymmetric pattern. Visual inspection of the funnel plot indicates more studies on the left side. Furthermore, we see missing data points at the top and bottom of the funnel, for both the significant (light grey) and non-significant (dark grey) areas. In the case of a publication bias, we would expect to see missing studies in the non-significant areas. The present funnel plot seems to rather suggest a gap for studies including larger sample sizes. Most of the studies included in this review involved similar, small to medium-size samples (great density in the middle), which can result in spuriously increased effect sizes. Therefore, we conducted the Egger’s test, which was significant, thereby suggesting a bias, due to small-study effects (z = − 2.22, p < 0.05).It has been reported however that funnel-plot asymmetry can be caused by publication bias, as well as other factors such as poor methodological quality or between study heterogeneity [32]. Due to the large amount of heterogeneity in our analysis we performed the Egger’s test again, this time taking into account between-study heterogeneity, as a result of different types of interventions, ER measures and control groups. We found that heterogenity due to different intervention types, significantly influenced the results of the the Egger’s test, which was nonsignificant when intervention type was added to the model (z = − 1.31, p = 0.19).
Fig. 4.
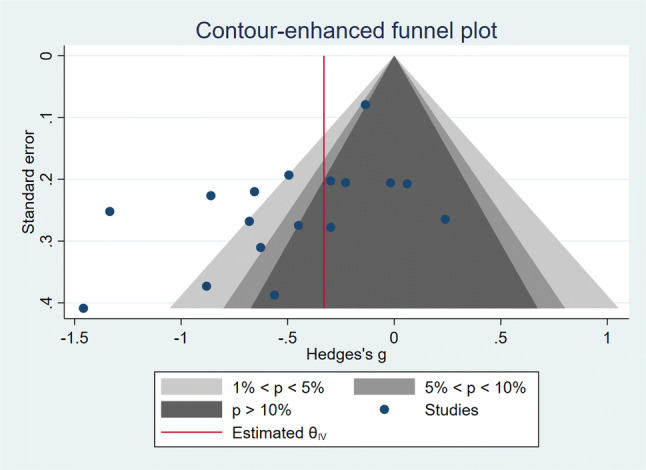
Funnel plot to detect publication bias
Sensitivity analyses
Effect of heterogeneity
Due to the large amount of heterogeneity in the presented models, we conducted further sensitivity analyses to test the robustness of our results. Hence, we fixed the value I2 to 10% to represent a small level of heterogeneity. The result suggest that with a smaller level of heterogeneity there is a smaller, but significant effect size of g = − 0.33 (z = − 6.64, p < 0.001) with a 95% CI of [− 0.46, − 0.23] for emotion dysregulation. The same analysis was performed for the emotion regulation model, indicating that lower heterogeneity would result in a larger effect size of g = 0.57 (z = 8.3, p < 0.001) with a 95% CI [0.47, 0.68]. These results suggest that heterogeneity has an impact on the overall effect size, but also that current interventions effectively improve emotion regulation processes whether heterogeneity is small or large.
Meta-regression: are changes in ER associated with changes in psychopathology?
Only two studies reported whether changes in ER were associated with changes in psychopathology. Slee et al. [43] investigated adolescents engaging in deliberate self-harm, and found that changes in ER difficulties partially mediated decreases in deliberate self-harm. The second study [45] found that changes in acceptance mediated decreases in anxiety and depression. Our meta-regression indicated a significant positive relationship between larger effect sizes of reduced ED and larger effect sizes of reduced psychopathology (see Fig. 5; β = 0.76, t = 2.93, p = 0.01). In other words, studies showing greater effectiveness in reducing ER difficulties were also more effective in reducing psychopathological symptoms (Figs. 6, 7, 8, 9).
Fig. 5.
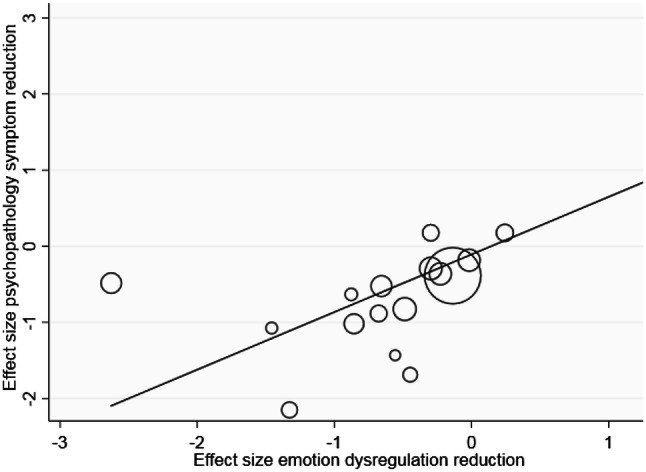
Meta-regression: showing significant positive relationship between reduced emotion regulation problems and reduced psychopathology
Fig. 6.

Subgroup analysis of type of intervention for emotion dysregulation
Fig. 7.

Subgroup analysis of type of intervention for emotion regulation
Fig. 8.

Subgroup analysis of type of control group for emotion dysregulation
Fig. 9.

Subgroup analysis of type of control group for emotion regulation
Discussion
The results of the meta-analyses suggested small to medium effect sizes for current interventions to improve ER in youth, regardless whether the full or reduced data set was employed. For emotion dysregulation effect sizes ranged between g = − 0.46 and g = − 0.52, and for emotion regulation effect sizes ranged between g = 0.36 and g = 0.43. Furthermore, our findings indicated that interventions, which effectively improved psychopathology also improved ER difficulties. These results are in line with the adult literature [19] showing that interventions which effectively improved ER difficulties also decreased psychopathology. Our results indicated that the type of control group had a significant impact on the effect size, whereby studies with a waitlist (passive) control group showed larger effect sizes in comparison to studies including an active control group. Unfortunately, the nature of the active control conditions was not always described in detail, therefore making any further conclusions difficult. The present meta-analysis adds to existing findings by synthesizing data from randomized control studies that involve children and adolescents as a target population, which has been neglected so far.
Clinical implications
Despite the limited evidence for the causal role of ER in the development and treatment of psychopathology in youth, the present findings encourage further development and evaluation of interventions that target ER specifically.
The average effect sizes suggest that interventions effectively change ER, irrespective of the type of the intervention program. However, the validation of existing interventions represents an important area for future work. As the present systematic review demonstrates there is a significant variety across intervention protocols in the way they target emotion regulation, and it is not clear yet which of the included components effectively enhance emotion regulation. Furthermore, there is still limited evidence with respect to different age groups and psychopathologies, which is of particular importance. First, research has shown that emotion regulation does not develop in a linear pattern, but that different developmental stages are characterised by certain advancements and deficits [46, 47]. For instance Cracco et al. [46] and Zimmermann et al. [47] have demonstrated that there is a significant shift in adolescents’ emotion regulation patterns (e.g., access to strategies, use of adaptive vs maladaptive strategies), which current interventions do not seem to take into consideration. Therefore, we argue that more efforts need to be made to increase our understanding of what works for who and when, so that relevant changes can be implemented in current clinical treatment plans. Secondly, young people frequently display a wide range of psychopathological symptoms and comorbidities [48, 49]. This can make interventions that have been designed for single-disorder symptoms, less suitable for this group. Thus the present review supports existing recommendations that ER interventions are effective in reducing a wider range of psychopathological symptoms by targeting underlying processes, which makes them highly suitable for young populations with high rates of comorbidities [17]. Furthermore, our results suggests the potential of transdiagnostic treatments being added as adjunctive modules in existing treatment protocols. This approach has already found support in adult studies where ER interventions in combination with CBT have resulted in better mental health and wellbeing outcomes than CBT alone [50].
Strengths and limitations
The results were based on a relatively small number of studies, which primarily involved small to medium sized samples. It can be assumed that the variety in populations, intervention settings (e.g., digital, inpatient and outpatient, schools) and use of ER measures lead to large between-study variation, which may have biased our findings. With respect to the latter it has been highlighted recently that meta-analyses with an increased psychometric focus could provide more insights regarding the impact of measurement error on outcome biases [51]. In the present meta-analysis, only 11 of the 19 studies reported information on reliability, which did not allow us to correct for measurement error. Hence, we highly encourage future meta-analysts to also consider bias due to measurement error. Moreover, there was a great variety between interventions, even though CBT formed the basis of most interventions. However, due to the limited amount of data available, it was impossible to provide further insights regarding the impact of these study artifacts on the overall effect size.
Furthermore, due to missing evidence from longitudinal mediation analyses, the present study could only partly address the second research question whether changes in ER precede changes in psychopathology. Only two studies [43, 45] reported whether changes in ER were associated with changes in psychopathology. Both studies found that changes in ER mediated decreases in psychopathology. Similarly, our meta-regression showed a significant positive relationship between effect sizes of improved ER difficulties and effect sizes of improved psychopathology. Moreover, most studies only assessed changes in anxiety or depression even though a wider range of symptoms was reported at baseline. Due to the current lack of research reporting on ER outcomes in relation to different psychopathology outcomes, we were not able to conduct more specific mediation analyses. Similar issues have been raised in previous systematic reviews [52]. We recommend that future research includes measures of ER so that underlying mechanisms of change can be identified.
The quality of the included studies ranged from weak to strong. Even though we focused primarily on RCTs, there was a significant lack of high quality studies. The limited evidence may have made it difficult to detect differences in effect sizes relating to study quality. Moreover, it has frequently been pointed out that the level of quality found in primary research has a significant impact on the quality of any systematic review, due to the fact that systematic reviews rely on data from existing studies. Following this we can only emphasize that future research needs to focus on the delivery of more high quality studies that provide high-quality research outcomes. In line with this, we acknowledge that while we had hoped to identify more high-quality studies by excluding non-peer-reviewed articles, the exclusion of such unpublished data may have resulted in biased outcomes. Although our publication bias assessment did not clearly indicate the presence of a publication bias, this may have been due to the high level of heterogeneity. However, we would like to highlight that there was significant lack of large-sample size studies that included a comprehensive psychopathology assessment and targeted youth populations.
Future suggestions
Further RCTs including larger sample sizes, different age groups and mental disorders are needed. While evidence suggests that research has widely neglected populations under the age of 25, future research should specifically address youth populations between the ages of 10 and 12 years. They form an interesting age group as research has emphasized a significant drop in ER skills at this age [47]. Furthermore, studies involving youth mostly investigate anxiety or depressive symptoms, while only a few have looked at ER in relation to other mental disorders. Similarly, interventions with a specific focus on ER often target specific disorders. Considering the suggested transdiagnostic nature of ER, future studies should involve participants from a broader psychopathological spectrum.
To increase our understanding of ER interventions and associated change mechanisms, future research needs to assess and actually report ER processes. A large number of studies was excluded, due to missing ER assessment. This can not only improve future interventions, but would also reduce the exploratory nature of current interventions. In line with this we suggest that future research should focus on the impact of measurement error in their studies. As mentioned above, studies included a wide range of ER measures, which have been based on different theories and models around ER. Thus, a psychometric meta-analysis of current ER measures, would be highly beneficial to the field.
Finally, we found that the investigation of positive ER strategies and ER abilities is still widely neglected. Although, past research has highlighted that adaptive ER strategies, as opposed to maladaptive strategies, were more strongly related to psychopathology in youth [53]. The opposite has been reported in adult studies [54]. We identified only one study that assessed a positive ER strategy [55]. This could be related to the fact that positive psychology is still a rather young field in comparison to the traditional CBT approaches or that the use of ER strategies has been less frequently studied in youth populations. Nevertheless, in line with previous research [12, 53] and our findings, we argue for a greater focus on the positive dimension of ER especially in researching and working with young populations.
Conclusion
This is the first meta-analysis that summarizes the evidence of psychological intervention to enhance ER in youth. The findings indicate that current interventions improve ER and that changes in ER co-occur with changes in psychopathological symptoms. The findings add to the existing literature, which has widely neglected youth populations thus far. Important implications for future clinical work and research have been made.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgements
The authors would to like to thank all authors who shared their data and missing information with us when we reached out to them. It was only due to their cooperation that we could conduct the present meta-analysis. Furthermore, we would like to thank Professor Peter Fonagy for his input during the conceptualization of the study and his support in reaching out to the authors. A big thank you goes to Darragh McCashin (DM) for his contribution to the screening and quality check of the selected studies. Funding for this study was provided by the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie Grant agreement No. 722561. The European Union’s Horizon 2020 research and innovation programme had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Compliance with ethical standards
Conflict of interest
All authors declare that they have no conflicts of interest.
References
- 1.Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustun TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. 2007;20(4):359–364. doi: 10.1097/YCO.0b013e32816ebc8c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dahl RE. Adolescent brain development: a period of vulnerabilities and opportunities. Ann N Y Acad Sci. 2004;1021(1):1–22. doi: 10.1196/annals.1308.001. [DOI] [PubMed] [Google Scholar]
- 3.Thompson RA. Emotion regulation: a theme in search of definition. Monogr Soc Res Child Dev. 1994;59(2/3):25–52. [PubMed] [Google Scholar]
- 4.Werner KH, Gross JJ. Emotion regulation and psychopathology: a conceptual framework. In: Kring AM, Sloan DM, editors. Emotion regulation and psychopathology: a transdiagnostic approach to etiology and treatment. New York: Guilford Press; 2009. pp. 13–37. [Google Scholar]
- 5.Gross J. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2(3):271–299. [Google Scholar]
- 6.Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. 2010;30(2):217–237. doi: 10.1016/j.cpr.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 7.Schäfer JÖ, Naumann E, Holmes EA, Tuschen-Caffier B, Samson AC. Emotion regulation strategies in depressive and anxiety symptoms in youth: a meta-analytic review. J Youth Adolesc. 2017;46(2):261–276. doi: 10.1007/s10964-016-0585-0. [DOI] [PubMed] [Google Scholar]
- 8.Lougheed JP, Hollenstein T. A limited repertoire of emotion regulation strategies is associated with internalizing problems in adolescence. Soc Dev. 2012;21(4):704–721. [Google Scholar]
- 9.Herts KL, McLaughlin KA, Hatzenbuehler ML. Emotion dysregulation as a mechanism linking stress exposure to adolescent aggressive behavior. J Abnorm Child Psychol. 2012;40(7):1111–1122. doi: 10.1007/s10802-012-9629-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Czaja J, Rief W, Hilbert A. Emotion regulation and binge eating in children. Int J Eat Disord. 2009;42(4):356–362. doi: 10.1002/eat.20630. [DOI] [PubMed] [Google Scholar]
- 11.Schuppert HM, et al. Emotion regulation training for adolescents with borderline personality disorder traits: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. 2012;51(12):1314–1323.e2. doi: 10.1016/j.jaac.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 12.Gilbert KE. The neglected role of positive emotion in adolescent psychopathology. Clin Psychol Rev. 2012;32(6):467–481. doi: 10.1016/j.cpr.2012.05.005. [DOI] [PubMed] [Google Scholar]
- 13.Aldao A, Sheppes G, Gross JJ. Emotion regulation flexibility. Cognit Ther Res. 2015;39(3):263–278. [Google Scholar]
- 14.Bonanno GA, Burton CL. Regulatory flexibility: an individual differences perspective on coping and emotion regulation. Perspect Psychol Sci. 2013;8(6):591–612. doi: 10.1177/1745691613504116. [DOI] [PubMed] [Google Scholar]
- 15.McLaughlin KA, Hatzenbuehler ML, Mennin DS, Nolen-Hoeksema S. Emotion dysregulation and adolescent psychopathology: a prospective study. Behav Res Ther. 2011;49(9):544–554. doi: 10.1016/j.brat.2011.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fernandez KC, Jazaieri H, Gross JJ. Emotion regulation: a transdiagnostic perspective on a new RDoC domain. Cognit Ther Res. 2016;40(3):426–440. doi: 10.1007/s10608-016-9772-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Berking M, Wupperman P, Reichardt A, Pejic T, Dippel A, Znoj H. Emotion-regulation skills as a treatment target in psychotherapy. Behav Res Ther. 2008;46(11):1230–1237. doi: 10.1016/j.brat.2008.08.005. [DOI] [PubMed] [Google Scholar]
- 18.Gratz KL, Weiss NH, Tull MT. Examining emotion regulation as an outcome, mechanism, or target of psychological treatments. Curr Opin Psychol. 2015;3:85–90. doi: 10.1016/j.copsyc.2015.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sloan E, Hall K, Moulding R, Bryce S, Mildred H, Staiger PK. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: a systematic review. Clin Psychol Rev. 2017;57(September):141–163. doi: 10.1016/j.cpr.2017.09.002. [DOI] [PubMed] [Google Scholar]
- 20.Moher D, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sawyer SM, Azzopardi PS. The age of adolescence. Lancet Child Adolesc Health. 2018;2(18):223–228. doi: 10.1016/S2352-4642(18)30022-1. [DOI] [PubMed] [Google Scholar]
- 22.Adrian M, Zeman J, Veits G. Methodological implications of the affect revolution: a 35-year review of emotion regulation assessment in children. J Exp Child Psychol. 2011;110(2):171–197. doi: 10.1016/j.jecp.2011.03.009. [DOI] [PubMed] [Google Scholar]
- 23.Deeks JJ, et al. Evaluating non-randomised intervention studies. Health Technol Assess (Rockv) 2003;7:27. doi: 10.3310/hta7270. [DOI] [PubMed] [Google Scholar]
- 24.Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176–184. doi: 10.1111/j.1524-475X.2004.04006.x. [DOI] [PubMed] [Google Scholar]
- 25.Bax L, Ikeda N, Fukui N, Yaju Y, Tsuruta H, Moons KGM. More than numbers: the power of graphs in meta-analysis. Am J Epidemiol. 2009;169(2):249–255. doi: 10.1093/aje/kwn340. [DOI] [PubMed] [Google Scholar]
- 26.Schmidt FL, Oh IS, Hayes TL. Fixed- versus random-effects models in meta-analysis: model properties and an empirical comparison of differences in results. Br J Math Stat Psychol. 2009;62(1):97–128. doi: 10.1348/000711007X255327. [DOI] [PubMed] [Google Scholar]
- 27.Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. 2. Chichester: Wiley; 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hedges LV, Olkin I. Statistical methods for meta-analysis. Orlando: Academic Press; 1985. Random effects models for effectt sizes; pp. 205–222. [Google Scholar]
- 29.Higgins J, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0. Cochrane Collab. 2011;2011:20. [Google Scholar]
- 30.Borenstein M, Higgins JPT, Hedges LV, Rothstein HR. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res Synth Methods. 2017;8(1):5–18. doi: 10.1002/jrsm.1230. [DOI] [PubMed] [Google Scholar]
- 31.Riley RD, Higgins JPT, Deeks JJ. Interpretation of random effects meta-analyses. BMJ. 2011;342:20. doi: 10.1136/bmj.d549. [DOI] [PubMed] [Google Scholar]
- 32.Sterne JAC, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343(7818):1–8. doi: 10.1136/bmj.d4002. [DOI] [PubMed] [Google Scholar]
- 33.Latimer WW, Winters KC, D’Zurilla T, Nichols M. Integrated family and cognitive-behavioral therapy for adolescent substance abusers: a stage I efficacy study. Drug Alcohol Depend. 2003;71(3):303–317. doi: 10.1016/s0376-8716(03)00171-6. [DOI] [PubMed] [Google Scholar]
- 34.Goldstein TR, Axelson DA, Birmaher B, Brent DA. Dialectical behavior therapy for adolescents with bipolar disorder: a 1-year open trial. J Am Acad Child Adolesc Psychiatry. 2007;46(7):820–830. doi: 10.1097/chi.0b013e31805c1613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fishbein D, et al. Behavioral and psychophysiological effects of a yoga intervention on high-risk adolescents: a randomized control trial. J Child Fam Stud. 2016;25(2):518–529. [Google Scholar]
- 36.Smith P, et al. Computerised CBT for depressed adolescents: randomised controlled trial. Behav Res Ther. 2015;73:104–110. doi: 10.1016/j.brat.2015.07.009. [DOI] [PubMed] [Google Scholar]
- 37.Harrer M, Cuijpers P, Furukawa TA, Ebert DD (2019) Doing meta-analysis in R: a hand-on guide
- 38.Slee N, Arensman E, Garnefski N, Spinhoven P. Cognitive-behavioral therapy for deliberate self-harm. Cris J Cris Interv Suicide Prev. 2007;28(4):175–182. doi: 10.1027/0227-5910.28.4.175. [DOI] [PubMed] [Google Scholar]
- 39.Livheim F, et al. The effectiveness of acceptance and commitment therapy for adolescent mental health: Swedish and australian pilot outcomes. J Child Fam Stud. 2015;24(4):1016–1030. [Google Scholar]
- 40.Livheim F, et al. The effectiveness of acceptance and commitment therapy for adolescent mental health: Swedish and Australian Pilot Outcomes. J Child Fam Stud. 2015;24(4):1016–1030. [Google Scholar]
- 41.Essau CA, Conradt J, Sasagawa S, Ollendick TH. Prevention of anxiety symptoms in children: results from a universal school-based trial. Behav Ther. 2012;43(2):450–464. doi: 10.1016/j.beth.2011.08.003. [DOI] [PubMed] [Google Scholar]
- 42.Afshari A, Neshat-Doost HT, Maracy MR, Ahmady MK, Amiri S. The effective comparison between emotion-focused cognitive behavioral group therapy and cognitive behavioral group therapy in children with separation anxiety disorder. J Res Med Sci. 2014;19(3):221–227. [PMC free article] [PubMed] [Google Scholar]
- 43.Slee N, Spinhoven P, Garnefski N, Arensman E. Emotion regulation as mediator of treatment outcome in therapy for deliberate self-harm. Clin Psychol Psychother. 2008;15(4):205–216. doi: 10.1002/cpp.577. [DOI] [PubMed] [Google Scholar]
- 44.Borenstein M. Introduction to meta-analysis. Chichester: Wiley; 2009. [Google Scholar]
- 45.Swain J, Hancock K, Hainsworth C, Bowman J. Mechanisms of change: exploratory outcomes from a randomised controlled trial of acceptance and commitment therapy for anxious adolescents. J Context Behav Sci. 2015;4(1):56–67. [Google Scholar]
- 46.Cracco E, Goossens L, Braet C. Emotion regulation across childhood and adolescence: evidence for a maladaptive shift in adolescence. Eur Child Adolesc Psychiatry. 2017;26(8):909–921. doi: 10.1007/s00787-017-0952-8. [DOI] [PubMed] [Google Scholar]
- 47.Zimmermann P, Iwanski A. Emotion regulation from early adolescence to emerging adulthood and middle adulthood. Int J Behav Dev. 2014;38(2):182–194. [Google Scholar]
- 48.Aldao A, Gee DG, De Los Reyes A, Seager I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: current and future directions. Dev Psychopathol. 2016;28(4):927–946. doi: 10.1017/S0954579416000638. [DOI] [PubMed] [Google Scholar]
- 49.Merikangas KR, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the national comorbidity survey replication-adolescent supplement (NCS-A) J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–989. doi: 10.1016/j.jaac.2010.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Berking M, Ebert D, Cuijpers P, Hofmann SG. Emotion regulation skills training enhances the efficacy of inpatient cognitive behavioral therapy for major depressive disorder: a randomized controlled trial. Psychother Psychosom. 2013;82(4):234–245. doi: 10.1159/000348448. [DOI] [PubMed] [Google Scholar]
- 51.Schmidt FL, Hunter JE (2017) Study artifacts and their impact on study outcomes. In: Methods of meta-analysis: correcting error and bias in research findings, pp 38–84
- 52.Riosa PB, McArthur BA, Preyde M. Effectiveness of psychosocial intervention for children and adolescents with comorbid problems: a systematic review. Child Adolesc Ment Health. 2011;16(4):177–185. doi: 10.1111/j.1475-3588.2011.00609.x. [DOI] [PubMed] [Google Scholar]
- 53.Braet C, et al. Emotion regulation in children with emotional problems. Cognit Ther Res. 2014;38(5):493–504. [Google Scholar]
- 54.Aldao A, Nolen-Hoeksema S. When are adaptive strategies most predictive of psychopathology? J Abnorm Psychol. 2012;121(1):276–281. doi: 10.1037/a0023598. [DOI] [PubMed] [Google Scholar]
- 55.Kwok SY, Gu M, Kit KK. Positive psychology intervention to alleviate child depression and increase life satisfaction: a randomized clinical trial. Res Soc Work Pract. 2016;26(4):350–361. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.