

Abstract
Introduction
Abdominal pregnancy is one of the rare types of ectopic pregnancies that has a high rate of mortality. Its clinical presentation is similar to those of the other types of ectopic pregnancies.
Cases presentation
we report two cases of abdominal pregnancies whose the diagnosis was made by ultra-sonography and successfully treated by laparotomy in emergency obstetrical department of Ibn Rochd University Hospital of Casablanca.
Clinical discussion
the ultra-sonography based on precise criteria represents the fundamental paraclinical examination in the diagnosis of abdominal pregnancies. The treatment of early form is based on surgery; And despite the advent of laparoscopic surgery, laparotomy retains its indications including forms with hemorrhagic shock.
Conclusion
Due to the high risk of complications and maternal mortality, abdominal pregnancies should be surgically treated as soon as possible when the diagnosis is confirmed.
Keywords: Abdominal pregnancy, Ultra-sonographic, Diagnosis, Laparotomy
Highlights
-
•
Abdominal pregnancy is an exceptional type of ectopic pregnancies.
-
•
Their diagnosis is difficult to distinguish from other types of ectopic pregnancies.
-
•
Abdominal pregnancies should be surgically treated as soon as possible when the diagnosis is confirmed.
1. Introduction
Abdominal pregnancy corresponds to the direct implantation of the gestational sac in the abdominal peritoneum, it represents 1% of ectopic pregnancies [1]. Abdominal pregnancies are associated to a high-risk of maternal morbidity and mortality [2]. The treatment of early form is based on surgery; And despite the advent of laparoscopic surgery, laparotomy retains its indications including forms with hemorrhagic shock [3].We will present 2 cases of patients who have abdominal pregnancies in hemorrhagic forms and successfully treated by laparotomy in emergency obstetrical department in Ibn Rochd University Hospital of Casablanca. This work has been reported with respect to the SCARE 2020 criteria [4].
2. Cases report
2.1. Observation 1
A 36-years-old woman Gravida 2 Para 1, was referred to our unit with a history of 15-weeks of gestation and unmonitored pregnancy. No contraception was used in the past and no particular pharmacological or family history were founded in anamnesis. The patient was presented into emergency room with a pelvic pain and late periods, her urine pregnancy test was positive.
In admission, the patient had a pelvic pain and an instable hemodynamic status (shock), mild pallor, low blood pressure (systolic pressure 70mm Hg, diastolic pressure 40mm Hg) and high pulse rate 120 p/min. The patient benefited from a conditioning with 2 peripheral venous routes and infusion of crystalloid. Laboratory parameters were hemoglobin concentration 7.2 g/dl and hematocrit 28.2%.
Gynecological examination showed a long closed posterior cervix with bleeding and positive cervical excitation tenderness, and there was a complex mass in the right uterine during palpation. In addition, abdominal examination revealed a hypogastric tenderness and defense during deep abdominal palpation.
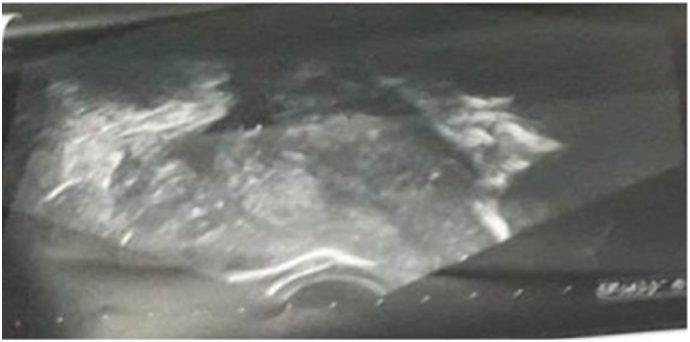
A transvaginal and Pelvic ultrasonography was made and showed an empty uterus with unusual size, pregnancy with no detectable myometrium around fetal membranes, amniotic cavity with fetus in retro uterine with movement and cardiac activity present (bi-parietal diameter 33 mm) associated with fluid in the pouch of Douglas as shown in Fig. 1, Fig. 2.
Fig. 1.

Abdominal pregnancy revealed during transvaginal ultrasound. Empty uterus increased in size; fetus in retro-uterine lying in pool of fluid with a bi-parietal diameter at 33 mm.
Fig. 2.

Abdominal pregnancy revealed during transvaginal ultrasound; fetus in retro-uterine with movement and cardiac activity present.
Diagnostic of abdominal pregnancy was made, the patient was transfused with two red blood cells, we proceeded to an urgent laparotomy under general anesthesia and in dorsal decubitus, where were found a fetus lying in a pool of blood in the abdominal cavity, a placenta attached to the posterior surface of the uterine fundus. However, her ovaries and both Fallopian tubes were found normal. The fetus and placenta were carefully evacuated and the peritoneal cavity copiously lavaged. A drain was inserted before closing the abdomen as shown in Fig. 3. Post-operative recovery was uneventful, healthy mother was discharged on 5th post-operative day and the regular follow-up of the patient was without anomaly.
Fig. 3.

Intraoperative finding of abdominal pregnancy.
2.2. Observation 2
The patient, a 26-year-old woman in her 9th week of gestation, primigravida, presented to the emergency room with abdominal pain and bleeding per vaginum accompanied by cold sweat and episodes of syncope.
In admission, patient has signs of shock with mild pallor and low blood pressure (systolic pressure 80mm Hg, diastolic pressure 50mmHg) and level pulse rate 110 p/min, her blood parameters were hemoglobin concentration 6 g/dl and hematocrit 26.4%,also her urine pregnancy test was positive.
The patient benefited from a conditioning with 2 peripheral venous routes and infusion of cristaloide. Physical examination showed a diffuse abdominal tenderness and long closed posterior cervix with bleeding in gynecological examination.
Ultra sonography revealed internal bleeding with empty uterus that has unusual size and gestational sac containing a vital embryo (Craniocodal Length 3 cm; 9 weeks of gestation and 5 days) with movement and cardiac activity that was present in the abdominal cavity as shown in Fig. 4, Fig. 5.
Fig. 4.
transvaginal ultrasound: Empty uterus with unusual size and haemoperitoneum.
Fig. 5.

Pelvic ultrasonography, pregnancy with no detectable myometrium around a gestational sac.
We proceeded to an urgent laparotomy under general anesthesia and in dorsal decubitus, on exploration the uterus is increased of the size with normal fallopian tubes and ovaries. A gestational sac of approximately 4 cm was identified in the pouch of Douglas, attached to the posterior surface of the uterine fundus and momentum, intact sac with embryo were dissected and removed as shown in Fig. 6. Patient was discharged on 5th post-operative day after the surgery and the regular follow-up of the patient was without anomaly.
Fig. 6.

Intraoperative finding of abdominal pregnancy; gestational sac with embryo attached to the posterior surface of the uterine fundus and momentum.
3. Discussion
Abdominal pregnancy represents 1% of extrauterine pregnancies with an incidence of 1/10.000–1/30.000 of all pregnancies [1], the level of maternal mortality is estimated to 7.7 times than other ectopic tubal pregnancies and to 90 times higher than intrauterine pregnancies [2].
Multiple locations of ectopic abdominal pregnancies were reported, the most common ones were recto-uterine and vesico-uterine pouches (24.3%), uterine and tubal serosa (23.9%). The risk factors for abdominal pregnancy are not specific are the same as those for all ectopic pregnancy [6].
The first classification of abdominal pregnancies based on the physiopathological mechanism divided them into 2 groups. First abdominal pregnancy that refers to pregnancy where implantation of the fertilized ovum occurs directly in the abdominal cavity. In such cases, the Fallopian tubes and ovaries are intact. In contrast, secondary abdominal pregnancy accounts for most cases of advanced extra uterine pregnancy. It occurs following an extra uterine tubal pregnancy that ruptures or aborts and is reimplanted within the abdomen. [7]
This classification does not have any practical interest in opposition to the classification based on the pregnancy term. Therefore, we call early abdominal pregnancy when the term is less than 20 weeks of amenorrhea and advanced abdominal pregnancy when that limit exceeds 20 weeks [8].
Abdominal pregnancy can be asymptomatic hence the interest of ultrasonography which allows the diagnosis of abdominal pregnancy less than 12 weeks, thus make it possible to adapt the management and avoid the evolution towards the sometimes severe hemorrhagic forms [9,10].
A pre-operative ultra-sonographic diagnosis of abdominal pregnancy has been described in a more advanced gestation (12 weeks) [11], but in our case, the ultrasonographic diagnosis was performed in 9-weeks pregnant.
The ultrasonographic criteria observed in our cases were: (1) Empty uterus increased in size and absence of intrauterine gestational sac; (2) absence of adnexal abnormalities; (3) a gestational cavity surrounded by loops of bowel and separated by peritoneum; (4) a wide mobility, particularly evident with a gentle pressure of the transvaginal.
Medical treatments is offered mainly for abdominal pregnancies where the location or surgical treatment is potentially associated with an increased risk of hemorrhage. These sites are essentially represented by the hepatic and splenic location [8,12],
Patients should be closely monitored due to the possibility of a surgery in case of a hemorrhagic complication. The In situ or systemic methotrexate injection or in situ potassium chloride injection are the most widely used protocols [6,13].
The most of the patients who received the first medical treatment requires the combination of adjuvant therapy [5]. Other authors have reported deceiving results concerning methotrexate use in abdominal pregnancies [12].
Surgery is the treatment of choice for the management of abdominal pregnancy. Laparotomy was chosen to be better than laparoscopic surgery because of the risk of perioperative hemorrhage, which can be uncontrollable from the implantation site [2].
The laparoscopic surgery is chosen instead of laparotomy if the abdominal pregnancy is diagnosed at an early age (< 12 weeks) or if the implantation site allows a non-hemorrhagic surgical excision [13]. In addition, the advantage of laparoscopy that is associated with a significant reduction in blood loss and the length of hospital stays.
4. Conclusion
Abdominal pregnancy is a rare type of ectopic pregnancies that can be potentially serious due to the hemorrhagic complications. The early diagnosis offers a better prognosis. However, clinical polymorphism makes early diagnosis difficult.
Our report showed the interest of ultrasound in the diagnosis of abdominal pregnancy, which guided the urgent management by laparotomy of two cases of abdominal pregnancy with hemorrhagic forms.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Consent
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
Ethical approval
I declare on my honor that the ethical approval has been exempted by my establishment.
Funding
None.
Author contribution
El Miski Fatiha: Corresponding author writing the paper and operating surgeon
El Ouafidi Ibtissam: writing the paper and operating surgeon
El Azzouzi El Hassan: writing the paper and operating surgeon
Elquasseh Rajaa: writing the paper
Lamrissi Amine: study concept
Fichtali Karima: study concept
Bouhya Said: correction of the paper
Guarantor
El Miski Fatiha.
Research registration number
None.
Declaration of competing interest
The authors report no declarations of interest.
References
- 1.Krishna D., Damyanti S. Advanced abdominal pregnancy: a diagnostic and management dilemma. J. Gynecol. Surg. 2007;23:69e72. [Google Scholar]
- 2.Atrash H.K., Friede A., Hogue C.J. Abdominal pregnancy in the United States: frequency and maternal mortality. Obstet. Gynecol. 1987;69:333–337. [PubMed] [Google Scholar]
- 3.Cristalli B., Guichaoua H., Heid M., Izard V., Levardon M. Grossesse ectopique abdominale Limites du traitement cœlioscopique. J. Gynecol. Obstet. Biol. Reprod. 1992;21:751–753. [PubMed] [Google Scholar]
- 4.Agha RA, Franchi T, Sohrabi C, Mathew G, for the SCARE Group. The SCARE 2020 guideline: updating consensus surgical CAse REport (SCARE) guidelines, Int. J. Surg. 2020;84:226–230. [DOI] [PubMed]
- 5.Agha R.A., Borrelli M.R., Farwana R., Koshy K., Fowler A., Orgill D.P. For th SCARE group, the SCARE 2018 statement: updating consensus surgical case REport (SCARE) guidelines. Int. J. Surg. 2018;60:132–136. doi: 10.1016/j.ijsu.2018.10.028. [DOI] [PubMed] [Google Scholar]
- 6.Aaron P., David H., Everett F.M. Early abdominal ectopic pregnancies: a systematic review of the literature. Gynecol. Obstet. Investig. 2012;74:249–260. doi: 10.1159/000342997. [DOI] [PubMed] [Google Scholar]
- 7.Yildizhan R., Kolusari A., Adali F. Primary abdominal ectopic pregnancy: a case report. Cases J. 2009;2:8485. doi: 10.4076/1757-1626-2-8485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Beacham W.D., Hernquist W.C., Beacham W.D., Webster H.D. Abdominal pregnancy; discussion, classification, and case presentation. Obstet. Gynecol. 1954;4(Oct. (4)):435–439. [PubMed] [Google Scholar]
- 9.Ginath S., Malinger G., Golan A., Shahmurov M., Glezerman M. Successful laparoscopic treatment of a ruptured primary abdominal pregnancy. Fertil. Steril. 2000;74:601–602. doi: 10.1016/s0015-0282(00)00686-5. [DOI] [PubMed] [Google Scholar]
- 10.Makinen J. Histologically verified primary peritoneal pregnancy with implantation in the sigmoid mesenterium. Eur. J. Obstet. Gynecol. Reprod. Biol. 1986;22:171–174. doi: 10.1016/0028-2243(86)90063-8. [DOI] [PubMed] [Google Scholar]
- 11.Zaki Z.M.S. An unusual presentation of ectopic pregnancy. Ultrasound Obstet. Gynecol. 1998;11:456–458. doi: 10.1046/j.1469-0705.1998.11060456.x. [DOI] [PubMed] [Google Scholar]
- 12.Allibone G.W., Fagan C.J., Porter S.C. The sonographic features of intra-abdominal pregnancy. J. Clin. Ultrasound. 1981;9:383–387. doi: 10.1002/jcu.1870090706. [DOI] [PubMed] [Google Scholar]
- 13.Okorie C.O. Retroperitoneal ectopic pregnancy: is there any place for non-surgical treatment with methotrexate? J. Obstet. Gynaecol. Res. 2010;36:1133–1136. doi: 10.1111/j.1447-0756.2010.01270.x. [DOI] [PubMed] [Google Scholar]