

Abstract
Introduction:
Adherence is a multifactorial phenomenon. Usually geriatric patients will have multiple co morbidities because of which poly pharmacy results. This can adversely affect medication compliance. The purpose of our study is to identify various factors responsible for low medication compliance. Elderly people are usually affected with chronic illnesses like Hypertension, Diabates Mellitus, Dyslipidemia, Coronary artery diseases, Osteoarthritis, etc., All these diseases require long-term treatment. So, medication compliance is a very important factor which increases therapeutic outcome.
Materials and Methods:
The study subjects were assessed by using 15 item structured questionnaires as per indigenously modified Morisky Medication Adherence Scale (MMAS).
Results:
A total of 100 patients of geriatric age group were assessed for the level of compliance for long term medication. The compliance level was assessed by providing a 15-item structured questionnaire as per indigenously modified MMAS. The level of compliance was high in 82%, medium in 16% and low in 2% in the first visit. The level of compliance was again assessed during next review visit. The level of score during review visit was high in 74%, medium in 25% and low in 1%.
Conclusion:
The compliance to medication is adversely affected by complicated regimes, ignorance about the disease and complications, physical and economic problems. Geriatric patients especially have a tendency to stop taking drugs off their own when they consider their symptoms have been ameliorated. This can hinder the expected improvement in adherence in the review visit
Keywords: Care giver, chronic illness compliance, drug economics, elderly, medication adherence, physical logistics
Introduction
It is being said that “Aging is not an option, not for anyone, it is how gracefully we handle the process and how lucky we are as the process handles us”- Cindy Mcdonald. Increasing age leads to increased prescription drug usage. Women take more drugs than men mainly psychotropic and analgesic drugs.[1] With increasing drug usage in the elderly it is a challenge to provide safe and effective drug therapy. In old age the organs will become damaged and the drug therapy in the elderly is further impacted by changes in the geriatric pharmacodynamics and pharmacokinetics. Drug usage in the elderly is compounded by economic and physical logistic factors too. The investigators explored all aspects of drug usage in elderly with chronic illness. Common diseases that are seen in elderly people are Hyperension, Diabates Mellitus, Bronchial Asthma, Dyslipidemia, Coronary artery diseases, Osteo arthritis, Benign prostatic hypertrophy, etc., All these are chronic illnesses. Hence, they have to take medication for long duration. Over usage of non-steroidal anti inflammatory drugs and sedative hypnotics can produce various adverse effects. Other than chronic diseases old people will have loss of mental sharpness, falls and fractures, incontinence, giddiness, impairment of hearing and vision which are overlooked. Most of them will have more than one disease which will result in polypharmacy. This can lead to lot of drug-drug interactions and drug-disease interactions. Non-pharmacological measures like diet restriction, regular exercise, yoga and relaxation techniques are also equally important in elderly people.
Materials and Methods
This prospective study was done to assess the level of medication compliance in elderly patients with chronic illness. After approval and clearance from the Institutional Ethics Committee, 100 patients visiting the out-patient department of Geriatrics in Amrita Institute of medical Sciences and Research Center were randomly included into the study. Written informed consent was obtained from all subjects after explaining the study procedure in both English and vernacular language. Subjects fulfilling the inclusion criteria were included in the study that is, patients above the age of 60 who have been diagnosed to be suffering from chronic illnesses and have been advised medications for a minimum period of 6 months and who are available for regular follow-up visits Ethics committee approved on 22-01-2018.
Patients with the following conditions were excluded from the study.
Newly diagnosed patients with recently started drug treatment
Patients receiving intermittent short course therapy on requirement basis
Infectious diseases like Tuberculosis, Leprosy, Human immunodeficiencydisease and viral disease
Patients with malignancies or terminal illnesses.
The compliance to the prescribed medication was assessed by making the patients answer a fifteen item structured questionnaire as per indigenously modified MMAS (Morisky Medication Adherence Scale). Compliance score was calculated as – High: 12 or above, Medium: 8/8-12, Low: Less than 8.
Statistical analysis
The demographic data collected was analysed by using descriptive statistics like mean, median and standard deviation. Significance of association of different parameters was evaluated by using Chi-square test and multinomial logistic regression.
Results
Figure 1 summarizes the chronic illnesses in the study subjects. 60% of patients had hypertension. Figure 2 shows the level of knowledge about the disease. 66% of patients were aware of their disease. Figure 3 compares the level of score for medication compliance in the first visit and review visit. Analysis showed that compliance among geriatric patients was high for 82% in the first visit and 74% in the review visit. Table 1 shows the number of medicines taken by each subject Table 2 gives an idea about the duration of treatment. The gender distributions in the study subjects is shown in Table 3. 44% geriatric patients were on medicinal therapy for 5-15 years and Table 4 gives an idea about the dependency of the patient on others to take medicine and to buy medicine.
Figure 1.
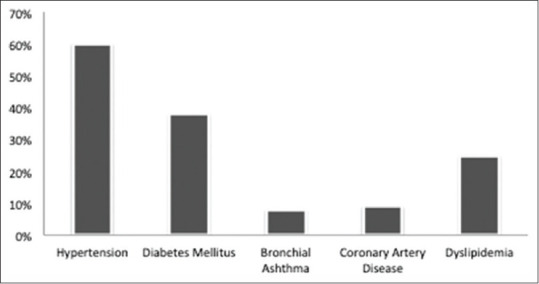
Distribution of study participants based on their co morbidities
Figure 2.
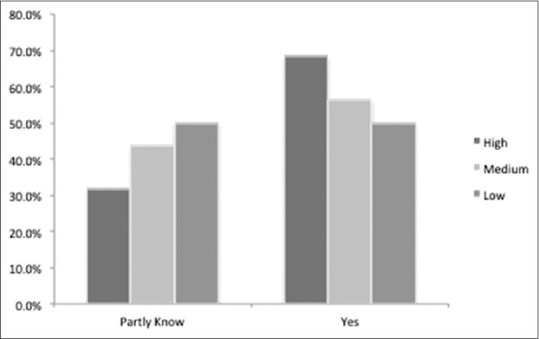
Distribution of study participants based on their knowledge about the disease
Figure 3.
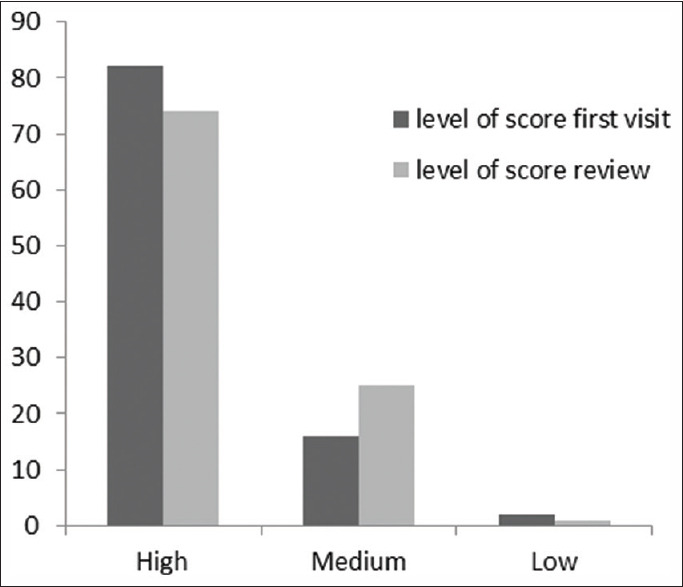
Distribution of study participants based on level of compliance
Table 1.
Distribution of study participants based on total number of medicines taken per day
| Number of medicines (n=100) | Percentage |
|---|---|
| <7 | 88.0 |
| >7 | 12.0 |
Table 2.
Distribution of study participants based on duration of therapy in years
| Duration of therapy (years) | Percentage |
|---|---|
| <5 | 25.0 |
| 5-15 | 44.0 |
| >15 | 31.0 |
Table 3.
Distribution of study participants based on factors associated with level of compliance to drugs in the first visit
| Variables | Category | Level of score | P | ||
|---|---|---|---|---|---|
| High | Medium | Low | |||
| Gender | Male | 26 | 6 | 0 | 0.558 |
| Female | 56 | 10 | 2 | ||
| Knowledge about the disease | Yes | 56 | 9 | 1 | 0.578 |
| Partly know | 26 | 7 | 1 | ||
| Who brings medicines | Self | 31 | 7 | 0 | 0.484 |
| Others | 51 | 9 | 2 | ||
| Who pay medicines | Self | 35 | 8 | 0 | 0.400 |
| others | 47 | 8 | 2 | ||
| Intake of medicines | Self | 67 | 14 | 1 | 0.423 |
| others | 15 | 2 | 1 | ||
| Forgotten | No | 71 | 5 | 0 | <0.001 |
| Yes | 11 | 11 | 2 | ||
| Purposely avoided | No | 76 | 12 | 1 | 0.024 |
| Yes | 6 | 4 | 1 | ||
| Taken medicine twice | No | 81 | 14 | 1 | <0.001 |
| Yes | 1 | 2 | 1 | ||
Table 4.
Distribution of study participants based on factors associated with level of compliance to drugs in the review visit
| Variables | Category | level of score review | P | ||
|---|---|---|---|---|---|
| High | Medium | Low | |||
| Gender | Male | 25 | 7 | 0 | 0.683 |
| Female | 49 | 18 | 1 | ||
| Knowledge about the disease | Yes | 48 | 18 | 0 | 0.304 |
| Partly know | 26 | 7 | 1 | ||
| Who brings medicines | Self | 33 | 5 | 0 | 0.067 |
| Others | 41 | 20 | 1 | ||
| Who pay medicines | Self | 36 | 7 | 0 | 0.134 |
| others | 38 | 18 | 1 | ||
| Intake of medicines | Self | 66 | 16 | 0 | 0.002 |
| others | 8 | 9 | 1 | ||
| Forgotten | No | 59 | 17 | 0 | 0.100 |
| Yes | 15 | 8 | 1 | ||
| Purposely avoided | No | 65 | 23 | 1 | 0.796 |
| Yes | 9 | 2 | 0 | ||
| Taken medicine twice | No | 72 | 24 | 0 | <0.001 |
| Yes | 2 | 1 | 1 | ||
Figure 3 compares the level of score for medication compliance in the first visit and review visit. Analysis showed that compliance among geriatric patients was high for 82% in the first visit and 74% in the review visit.
Discussion
This study investigated 100 geriatric patients having chronic illnesses for assessment of the level of compliance for long term medication. The investigators also explored various factors that can affect compliance. There was a preponderance of female in the study vide [Table 3] A similar study showed a preponderance of male which is done by R. Shruthi et al.[2]
Hypertension was the most common problem among the patients (60%). Other co-morbidities were Diabetes Mellitus, Coronary artery disease, Dyslipidemia, Bronchial asthma etc., vide
[Figure 1] The common co morbidities in Shruthi et al. study were Hypertension, Diabetes Mellitus, Coronary artery disease, Chronic obstructive pulmonary disease, etc.[2] A study was done on asthmatic patients which revealed reduced use of inhaled steroids and overdependence on short acting beta 2 agonists for relief of symptoms.[3]
About 66% of the subjects was aware of existing disease, antecedent complications and progress of the disease at the beginning and end of the study. There was no change in the knowledge at the observational study at the end as no intervention was set that educated the patient about the disease and prognosis. Knowledge about disease, complications and prognosis definitely helps in medication compliance [Figure 2]. In fact, session on awareness of the disease and incidental complications would motivate to adhere to medication and dietary restrictions. Medication review and knowledge about the purpose of treatment and consequences of omission will improve compliance.[4]
Regarding the number of medicines taken daily, on an average a geriatric person receives 4-5 medicines per day. An important method for simplifying medical regime is to prescribe single daily dose of drugs.[5] 88% of patients of our study was getting more than 7 medicines vide [Table 1].
In this study 44% geriatric patients were on medicinal therapy for 5-15 years as they are having multiple pathologies that require therapy for long periods/life time vide [Table 2]. The long term therapy would lead to variability in motivation and thus medication adherence would also falter in the long run. Average duration of therapy is 12.05 years. In another study it was noted that medication compliance in people with chronic diseases can be improved by open communication with the patient and inter professional cooperation.[6]
Analysis showed that adherence among geriatric patients was high for 82% in the first visit and 74% in the review visit vide [Figure 3]. There was no significant difference in the adherence over study period. This can be explained by patient's tendency to stop medicine once they are symptom free. R Shruthi et al. study also showed moderate to good compliance in 80%.[2]
Geriatric patients are not buying the medicines themselves (62%) as they have problem with their mobility and therefore depend on care givers like son, daughter or others to get medicine vide [Table 3].
It was noted that only 43% of geriatric patients were financially independent to afford. and 57% required financial help from others for their medication vide [Table 3] One study shows that the relationship between income and medication non adherence is complex and financial pressure alone is not responsible for impaired compliance.[7]
It is heartening to note that 18% geriatric patients required external help for the administration of drugs. P value is 0.002 the review visit which is significant vide [Table 3]. When daily activities of living among geriatric patients are not compromised, the responsibility of drug administration rests with the patients themselves. When considering the factors affecting compliance, it is not only the patient factors but also factors impacting care givers that would be relevant. Care givers require knowledge about the disease and the importance of giving right medication at right the time.[8]
It is significant to note that only 24% of geriatric patients has forgotten medicine at some time or the other. The elderly age group has dementia and other memory problems. But it shows that they are strongly self-driven for taking medication for their chronic illness. Here P value is very significant in the first visit which is 0.000 (<001) vide [Table 3]. Another study also emphasized forgetfulness or unintentional missing of drugs as important factors for reduced compliance.[9]
It is also surprising to note that 11% has purposefully avoided taking certain medication by his/her own decision. This could be because of experiencing adverse drug reaction or financial constraints to prolong the drug availability. Here P value is significant in the first visit which is 0.024 vide Table 3.
The issue of taking same medication twice could be due to inherent short-term memory loss, drug automatism, over enthusiasm in medication or bullying by the care giver. 4% of patients has taken the medicine twice. P value is very significant (<001) in the first visit and review visit [Tables 3 and 4]. In another study it was observed that medication compliance does not depend on demographic variables like age, income, and educational status.[10]
This study reiterates the importance of adherence to medication. Medication nonadherence increases during pandemics like Covod-19 which can be due to fear of immunosuppressive effects of drugs and nonavailability of drugs.[11] This requires that the various factors impacting compliance should be reduced. The number of drugs received should be optimal and individualized to meet the clinical objectives. The financial constraint is a detriment to medication compliance. The dependency on care givers for medication is a grave issue that needs to be tackled by highlighting the need of drugs and timely administration. Prolonged duration of therapy hinders medication compliance, but the geriatric patients are mostly having chronic illnesses that necessitates therapy over long periods. General practitioner should consider patient's opinion also while planning treatment and technical improvements like mobile communication can be used to improve adherence.[12] The regime may be simplified and reduced to once daily dosing that allows for effective compliance. Pharmacies can help to improve adherence through medication therapy management.[13]
Conclusion
Geriatric patient with chronic illness is receiving at least five drugs on an average. The compliance to medication is adversely affected by complicated regimes, ignorance about the disease and complications, purposeful omission of drugs, loss of memory, physical, economic and logistic problems. Geriatric patients especially have a tendency to stop taking drugs off their own when they consider their symptoms have been ameliorated. The study has shown that adherence to medication can be improved by simple regimens, health education of the patient about disease and drugs, uneventful drug interactions, easy availability and cheaper medication.
Non-adherence to treatment is seen with many elderly patients. The few reasons could be poor cognition, financial burden due to polypharmacy, multiple timings of medications and fear of adverse drug effects. Primary care physicians should find time to communicate to the patient and bystander and make them understand the importance of taking drugs in proper dose and correct time. Non-adherence will lead to economic wastage and lack of improvement in patient's condition.
Medication adherence is an important aspect of patient care especially with elders. As this age group suffer from multiple co morbidities they tend to have multiple drugs. Avoidance of polypharmacy may not be possible always. The primary care physician can try to reduce the number of medications. Encourage to use a pill box so that the medications are not skipped. Proper availability of drugs is to be ensured.
The primary care physician should consider various co morbidities. The medication list should be checked, before prescribing a new medication.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mark Ruscin BJ, Linnebur SA. Overview of drug therapy in older adults. MSD-Manual Profession version. 2018 [Google Scholar]
- 2.Shruthi R, Jyothi R, Pundarikaksha HP, Nagesh GN, Tushar TJ. A study of medication compliance in geriatric patients with chronic illnesses at a tertiary care hospital. J Clin Diagn Res. 2016;10:FC40–3. doi: 10.7860/JCDR/2016/21908.9088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Amin S, Soliman M, Mclvor A, Cave A, Cabrera C. Understanding patient perspectives on medication adherence in asthma: A targeted review of qualitative studies. 2020;14:541–51. doi: 10.2147/PPA.S234651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Smaje A, Weston-Clark M, Raj R, Orlu M, Davis D, Rawle M. Factors associated with medication adherence in older patients: A systematic review. Aging Med (Milton) 2018;1:254–66. doi: 10.1002/agm2.12045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brauner DJ. Adherence to medication in patients with dementia: Problems and solutions. Geriatr Ageing. 2009;12:259–63. [Google Scholar]
- 6.Kivarnsrm K, Airaksinen M, Liira H. Barriers and facilitators to medication adherence: A qualitative study with general practitioners[6] BMJ Open. 2018;8:e015332. doi: 10.1136/bmjopen-2016-015332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee S, Jiang L, Dowdy D, Hong YA, Ory MG. Attitudes, beliefs and cost related medication non adherence among adults aged 65 or older with chronic diseases. Prev Chronic Dis. 2018;5:E148. doi: 10.5888/pcd15.180190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.El-Saifi N, Moyle W, Jones C. Family care giver's perspectives on medication adherence challenges in older people with dementia: A qualitative study. Aging Ment Health. 2019;23:1333–9. doi: 10.1080/13607863.2018.1496226. [DOI] [PubMed] [Google Scholar]
- 9.Holt EW, Rung AL, Leon KA, Firestein C, Krousel-Wood MA. Medication adherence in older adults: A qualitative study. Educational Gerontology. 2014;40:198–211. doi: 10.1080/03601277.2013.802186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jahanpour F, Rafiei Z, Ravanipour M, Motamed N. Assessment of medication adherence in elderly patients with cardiovascular diseases based on demographic factors in Bushehr city in the year 2013. Jundishapur Journal of chronic disease care. 2015;4:e2839. [Google Scholar]
- 11.Khabbazi A, Kavandi H, Paribanaem R, Khabbazi R, Malek Mahdavi A. Adherence to medication in patients with rheumatic diseases during COVID-19 pandemic? Ann Rheum Dis. 2020 doi: 10.1136/annrheumdis-2020-218756. doi: 10.1136/annrheumdis-2020-218756. [DOI] [PubMed] [Google Scholar]
- 12.Malik M, Kumari S, Manalai P. Treatment nonadherance: An epidemic hidden in plain sight. Psychiatric Times. 2020;37:25–6. [Google Scholar]
- 13.Khairullah A, Platt B, Chater RW. Medication non adherence in older adults: Patient engagement solutions and pharmacist impact. 2018-11-06. [Google Scholar]