

Key Points
Question
Of the thermal care interventions available in the delivery room, which is the most appropriate for reducing hypothermia and improving clinical outcomes in preterm neonates?
Findings
In this network meta-analysis of 34 trials involving 3688 newborns and 9 interventions, a combination of plastic bag or wrap with a plastic cap or with heated humidified respiratory gas was associated with reduced risk of mortality before discharge and major brain injury while stabilizing the core body temperature immediately after birth. Certainty of evidence for these interventions was moderate for temperature stabilization and low to moderate for other clinical outcomes.
Meaning
In this study, delivery room use of a plastic bag or wrap with a plastic cap or with heated humidified gas appeared to be the appropriate thermal care intervention for preterm neonates.
Abstract
Importance
Prevention of hypothermia in the delivery room is a cost-effective, high-impact intervention to reduce neonatal mortality, especially in preterm neonates. Several interventions for preventing hypothermia in the delivery room exist, of which the most beneficial is currently unknown.
Objective
To identify the delivery room thermal care intervention that can best reduce neonatal hypothermia and improve clinical outcomes for preterm neonates born at 36 weeks’ gestation or less.
Data Sources
MEDLINE, the Cochrane Central Register of Controlled Trials, Embase, and CINAHL databases were searched from inception to November 5, 2020.
Study Selection
Randomized and quasi-randomized clinical trials of thermal care interventions in the delivery room for preterm neonates were included. Peer-reviewed abstracts and studies published in non–English language were also included.
Data Extraction and Synthesis
Data from the included trials were extracted in duplicate using a structured proforma. A network meta-analysis with bayesian random-effects model was used for data synthesis.
Main Outcomes and Measures
Primary outcomes were core body temperature and incidence of moderate to severe hypothermia on admission or within the first 2 hours of life. Secondary outcomes were incidence of hyperthermia, major brain injury, and mortality before discharge. The 9 thermal interventions evaluated were (1) plastic bag or plastic wrap covering the torso and limbs with the head uncovered or covered with a cloth cap; (2) plastic cap covering the head; (3) skin-to-skin contact; (4) thermal mattress; (5) plastic bag or plastic wrap with a plastic cap; (6) plastic bag or plastic wrap along with use of a thermal mattress; (7) plastic bag or plastic wrap along with heated humidified gas for resuscitation or for initiating respiratory support in the delivery room; (8) plastic bag or plastic wrap along with an incubator for transporting from the delivery room; and (9) routine care, including drying and covering the body with warm blankets, with or without a cloth cap.
Results
Of the 6154 titles and abstracts screened, 34 studies that enrolled 3688 neonates were analyzed. Compared with routine care alone, plastic bag or wrap with a thermal mattress (mean difference [MD], 0.98 °C; 95% credible interval [CrI], 0.60-1.36 °C), plastic cap (MD, 0.83 °C; 95% CrI, 0.28-1.38 °C), plastic bag or wrap with heated humidified respiratory gas (MD, 0.76 °C; 95% CrI, 0.38-1.15 °C), plastic bag or wrap with a plastic cap (MD, 0.62 °C; 95% CrI, 0.37-0.88 °C), thermal mattress (MD, 0.62 °C; 95% CrI, 0.33-0.93 °C), and plastic bag or wrap (MD, 0.56 °C; 95% CrI, 0.44-0.69 °C) were associated with greater core body temperature. Certainty of evidence was moderate for 5 interventions and low for plastic bag or wrap with a thermal mattress. When compared with routine care alone, a plastic bag or wrap with heated humidified respiratory gas was associated with less risk of major brain injury (risk ratio, 0.23; 95% CrI, 0.03-0.67; moderate certainty of evidence) and a plastic bag or wrap with a plastic cap was associated with decreased risk of mortality (risk ratio, 0.19; 95% CrI, 0.02-0.66; low certainty of evidence).
Conclusions and Relevance
Results of this study indicate that most thermal care interventions in the delivery room for preterm neonates were associated with improved core body temperature (with moderate certainty of evidence). Specifically, use of a plastic bag or wrap with a plastic cap or with heated humidified gas was associated with lower risk of major brain injury and mortality (with low to moderate certainty of evidence).
This meta-analysis describes the outcomes associated with thermal care interventions that can be used immediately after the birth of neonates at 36 weeks’ gestation or less.
Introduction
Neonatal hypothermia is a serious problem in both low- or middle-income and high-income countries.1,2,3 The dose-response association between the severity of neonatal hypothermia and the risk of mortality is well established.3,4,5,6 Hence, prevention of neonatal hypothermia in the delivery room is touted as a cost-effective, high-impact intervention to reduce neonatal mortality. The 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations reiterated its previous advice to use additional thermal care interventions, such as maintaining delivery room temperature at 23 to 25 °C and using warm blankets, plastic wraps without drying, thermal mattresses, and caps for neonates born at less than 32 weeks’ gestation.7 However, authors of the 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations stressed the weakness of the previous guidance on the basis of very low certainty of evidence and indicated the need for an updated systematic review.7 Apart from assessing the benefits of the interventions, establishing the safety of these interventions is also essential, given that some studies have shown an increased risk of hyperthermia with their use.8,9,10
Previous systematic reviews have compared several thermal care interventions in pairwise meta-analyses.8,9,10,11 However, faced with a rapidly evolving evidence base and a choice of several competing interventions for which direct pairwise comparisons are not available, a systematic review based on network meta-analysis for data synthesis may be considered as an appropriate evaluation strategy.12 Hence, in the present study, we conducted a network meta-analysis to compare the outcomes and safety of different delivery room thermal care interventions. Our aim was to identify the delivery room intervention that can best reduce neonatal hypothermia and improve clinical outcomes for preterm neonates born at 36 weeks’ gestation or less.
Methods
The protocol was registered with PROSPERO.13 We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline with a network meta-analysis extension.14
Population, Interventions, and Outcomes
We included randomized clinical trials (RCTs) and quasi-RCTs that evaluated thermal care interventions in the delivery room for preterm neonates born at 36 weeks’ gestation or less. Studies published as peer-reviewed abstracts or in non-English language were also included. Studies that included the term infants or infants with birth weight greater than 2500 g were excluded.
The following 9 thermal care interventions were included: (1) plastic bag or plastic wrap covering the torso and limbs with the head uncovered or covered with a cloth cap; (2) plastic cap covering the head; (3) skin-to-skin contact; (4) thermal mattress; (5) plastic bag or plastic wrap covering the torso and limbs with the head covered with a plastic cap; (6) plastic bag or plastic wrap covering the torso and limbs along with use of a thermal mattress; (7) plastic bag or plastic wrap covering the torso and limbs along with heated humidified gas for resuscitation or for initiating invasive or noninvasive respiratory support in the delivery room; (8) plastic bag or plastic wrap covering the torso and limbs along with an incubator for transporting from the delivery room; and (9) routine care, including drying and covering the body with warm blankets, with or without a cloth cap.
The primary outcomes were core body temperature (using axillary or rectal measurement) and incidence of moderate to severe hypothermia (defined as body temperature <36 °C) at admission or within the first 2 hours of life. Although incidence of hypothermia was the a priori decided primary outcome, moderate to severe hypothermia was reported as the primary outcome in this systematic review. The secondary outcomes were incidence of hyperthermia (defined as body temperature >37.5 °C), major brain injury (grade 3 or 4 intraventricular hemorrhage15 or periventricular leukomalacia), and mortality before discharge.
Literature Search and Risk-of-Bias Assessment
We searched MEDLINE, the Cochrane Central Register of Controlled Trials, Embase, and CINAHL from their inception to November 5, 2020. Reference lists of included trials and published systematic reviews were also searched to identify additional studies. Two of us (T.B. and S.T.) screened the title and abstract of all studies using Rayyan-QCRI software (Rayyan),16 and independently assessed the full-text articles for potentially relevant trials. The search strategy is provided in eTable 1 in the Supplement.
Two of us (T.A. and V.V.R.) independently assessed the risk of bias (low, high, or unclear) in all included trials using the Cochrane risk-of-bias tool, version 1.0 (Cochrane).17 Discrepancies were resolved by consulting a third author (C.C.R.).
Data Extraction and Data Synthesis
Two of us (T.A. and V.V.R.) independently extracted data from the included trials and data in duplicate using a structured proforma. A network meta-analysis with bayesian random-effects model was used for data synthesis.18,19 Noninformative priors and generalized linear models with 4 chains, burn-in of 50 000 iterations, followed by 100 000 iterations and 10 000 adaptations, were used.19 Geometry of networks for all outcomes was evaluated using network plots. Model convergence was assessed with the Gelman-Rubin statistic trace and density plots.20 Fit of the model was analyzed with leverage plots, total residual deviance, and deviance information criterion. Node splitting was used to detect inconsistency.21 I2 statistic and Cochran Q test were used to evaluate heterogeneity in a pairwise meta-analysis for direct evidence. Publication bias was identified using a funnel plot when a meta-analysis included 10 or more trials.
Statistical Analysis
Statistical analysis was performed with R (R Foundation for Statistical Computing). Network estimates were expressed as risk ratio (RR) or mean difference (MD), with respective 95% credible interval (CrI), and were illustrated with league plots and forest plots. Ranking of interventions for all outcomes was done with surface under the cumulative ranking curve (SUCRA) plots.22 SUCRA values when expressed as a percentage can range from 0% to 100%. The higher the SUCRA value, the better the ranking of the intervention. SUCRA values are prone to misinterpretation; the value needs to be interpreted along with the certainty of evidence for any intervention. In addition, SUCRA can vary for an intervention for different outcomes. Although an intervention may be ranked higher for its improved outcomes, it could be ranked down for its adverse effect profile. These factors need to be considered by the clinician while interpreting SUCRA and before adopting any intervention to practice. Meta-regression with gestational age as a covariate was performed for the primary outcome. Certainty of evidence for all of the estimates was ascertained according to the GRADE Working Group recommendations for a network meta-analysis.23
We also conducted sensitivity analyses for the following: (1) neonates born at 30 weeks’ gestation or less; (2) plastic bag and plastic wrap as separate interventions; (3) drying vs no drying before application of plastic bag or wrap; and (4) incidence of any hypothermia defined as a core body temperature <36.5 °C at admission or within the first 2 hours of life.
Results
A total of 6154 titles and abstracts were screened, of which 34 studies that enrolled 3688 neonates were included (eFigure 1 in the Supplement).24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57 Among the 34 studies were 4 three-armed RCTs.30,51,54,55 The mean gestational age of the neonates was 29 weeks, and their mean birth weight was 1200 g (eFigures 2 and 3 in the Supplement). The characteristics of the included trials are given in Table 1. The characteristics of some of the excluded studies are shown in eTable 2 in the Supplement along with the reasons for exclusion.58,59,60,61,62,63,64
Table 1. Characteristics of Included Studies.
| Source; country of origin | Intervention group (n) | Comparator group (n) | Drying (for PBWr) | Gestational age, mean (SD), wk | Birth weight, mean (SD), g | Method of temperature measurement used for analysis | Hypothermia definition, °C | Moderate to severe hypothermia definition, °C | Components of RCARE | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention group | Comparator group | Intervention group | Comparator group | ||||||||
| Ahmed et al,24 2013; Cairo | PBAG (25) | RCARE (25) | Wet | 29.56 (1) | 30.04 (1.75) | 1190 (200) | 1250 (40) | Rectal, admission | NR | <35 | Radiant warmer, cap, and transport incubator |
| Almeida,25 2013; US | TM (26) | RCARE (14) | NA | 32 (0.91) | 32 (1.3) | 1989 (626) | 1906 (526) | Axillary, admission | NR | NR | Radiant warmer, cap, and transport incubator |
| Bergman et al,26 2004; South Africa | SSC (20) | RCARE (14) | NA | 34.2 (1.9) | 35.3 (1.9) | 1813 (260) | 1866 (258) | NR | NR | Axillary <35.5 | Incubator, cap, booties, and heat shield if required |
| Bhavsar et al,27 2015; India | PBWrPCAP (49) | RCARE (47) | Dry | 32.6 (2.4) | 31.9 (2.8) | 1686 (446) | 1471 (446) | Axillary, admission | NR | Axillary <35 | Radiant warmer, transport incubator, and interhospital transport |
| Brennan,28 1996; US | TM (12) | RCARE (12) | NA | 27.8 | 27.3 | 1033 | 1027 | Axillary, admission | Axillary <36.5 | Axillary <36 | Radiant warmer, and as per NRP |
| Çağlar et al,29 2014; Turkey | PBAG (22) | PWRAP (37) | Wet | 29.27 (1.8) | 28.64 (2.05) | 1183 (520) | 1079 (336) | Axillary, 1 h | Axillary <36.5 | Axillary <36 | Radiant warmer, cap, and transport incubator |
| Cardona Torres et al,30 2012; Mexico | PWRAP-wet (30) and PWRAP-dry (30) | RCARE (30) | Wet and dry | 34.5 (2.6) and 35.2 (1.8) | 35.6 (1.68) | 1934 (456) and 2101 (319) | 2173 (275) | Axillary, 1 h | Axillary <36.5 | NR | Radiant warmer and transport incubator |
| Chantaroj and Techasatid,31 2011; Thailand | PBAG (19) | RCARE (19) | Wet | 28 (6) | 29 (2) | 1263 (274) | 1200 (258) | Rectal, admission | Rectal <36.5 | NR | Radiant warmer, yarn cap, and transport incubator |
| Chawla et al,32 2011; US | PBWrTM (53) | PBWr (49) | Wet | 28.7 (3) | 28.7 (2.4) | 1151 (407) | 1175 (413) | Axillary, admission | Axillary <36 | Axillary <35 | Radiant warmer, cap, and transport incubator |
| Doglioni et al,33 2014; Italy | PBWrPCAP (50) | PBWr (50) | Wet | 25.7 (1.7) | 25.8 (1.7) | 789 (214) | 770 (245) | NR | Axillary <36.5 | Axillary <36 | Radiant warmer and transport incubator |
| Farhadi et al,34 2012; Iran | PBAG (20) | RCARE (20) | Wet | 28.8 (2) | 29.2 (2.3) | 1278 (518) | 1190 (492) | Axillary, NR | NR | NR | Radiant warmer and cap |
| Gathwala et al,35 2010; India | PBAG (30) | RCARE (30) | Dry | 29.93 (1.08) | 29.46 (1.33) | 1120 (190) | 1110 (230) | Rectal, admission | NR | NR | Radiant warmer, cap, and transport incubator |
| Shafie et al,36 2017; Malaysia | PBWrPCAP (40) | PBWr (40) | Wet | 30.9 (2) | 31.3 (2) | 1410 (1170-1605) | 1642 (1260-1756) | Axillary, admission | Axillary <36.5 | Axillary <36 | Radiant warmer, cotton cap, and transport incubator |
| Hu et al,37 2018; China | PBAG (54) | RCARE (54) | Dry | 29.7 (2) | 30 (2) | 1185 (213) | 1225 (195) | Axillary, admission | Axillary <36.5 | Axillary <36 | Radiant warmer, cap, transport incubator, and interhospital transport |
| Knobel et al,38 2005; US | PBAG (41) | RCARE (47) | Wet | 26.5 (1.4) | 26.1 (1.4) | 918 (259) | 850 (253) | Rectal, admission | Rectal <36.5 | NR | Radiant warmer and warm blankets |
| Leadford et al,39 2013; Zambia | PBAG (49) | RCARE (55) | Dry | 34 (32-36) | 34 (31-36) | 2200 (560) | 2110 (520) | Axillary, 1 h | Axillary <36.5 | NR | Radiant warmer or SSC and blanket |
| Leslie et al,40 2007; India | PBWrTM (23) | PBWr (24) | Wet | 26 (23-28) | 26 (23-28) | 805 (560-1320) | 840 (530-1240) | Axillary, admission | Axillary <36.5 | NR | Radiant warmer and woolen cap |
| Mathew et al,41 2013; US | PBAG (21) | TM (20) | Wet | 26 (1.3) | 26 (1.2) | 768 (162) | 766 (186) | NR | NR | NR | Radiant warmer, cotton cap, and transport incubator |
| McCarthy et al,42 2013; Ireland | PBWrTM (37) | PBWr (35) | Wet | 28 (2) | 28 (2) | 1085 (360) | 1194 (386) | Rectal, admission | Axillary <36.5 | NR | Radiant warmer, cotton cap, and transport incubator |
| McGrory et al,43 2018; Australia | PBWrHHGAS (132) | PBWr (141) | Wet | 27 (1.8) | 27 (1.8) | 973 (288) | 930 (272) | Rectal, admission | Axillary <36.5 | Axillary <36 | Radiant warmer, cotton woolen cap, and transport incubator |
| Meyer and Bold,44 2007; New Zealand | INCUPBWr (30) | PBWr (32) | Wet | 26 (24.9-27) | 26 (25-27) | 870 (751-1031) | 902 (746-991) | Axillary, admission | Axillary <36.5 | Axillary <36 | Plastic wrap, radiant warmer, and radiant warmer or incubator for transport |
| Meyer et al,45 2015; New Zealand | PBWrHHGAS (100) | PBWr (100) | Wet | 29 (27-30) | 29 (26-30) | 1158 (890-1460) | 1190 (954-1396) | Axillary, admission | NR | Axillary <35.5 | Radiant warmer, cap, and radiant warmer or incubator for transport |
| Nimbalkar et al,46 2019; India | PBAG (74) | RCARE (77) | Wet | NR | NR | 1658 (358) | 1627 (425) | Axillary, 1 h | Axillary <36.5 | NR | Radiant warmer, cap, and transport in open trolley |
| Reilly et al,47 2015; US and Canada | PWRAP (404) | RCARE (397) | Wet | 25.6 | 26.0 | 800 (205) | 821 (199) | Axillary, admission | Axillary <36.5 | Axillary <34.5 | Radiant warmer, cap, and with or without transport incubator |
| Reilly et al,48 2019; US and Canada | PWRAP (14) | RCARE (14) | Wet | 22.8 | 22.7 | 565 | 552 | Axillary, admission | NR | NR | Radiant warmer, cap, and with or without transport incubator |
| Rohana et al,49 2011; Malaysia | PWRAP (50) | RCARE (60) | Wet | 29.7 (2.9) | 29.8 (2.7) | 1277 (462) | 1328 (459) | Axillary, admission | Axillary <36.5 | Axillary <36 | Radiant warmer, cotton cap, and transport incubator |
| Tecson-delos Santos et al,50 2012; The Philippines | PBWrPCAP (28) | RCARE (30) | Dry | NR | NR | NR | NR | Axillary, admission | NR | NR | Droplight and blankets |
| Shabeer et al,51 2018; India | PBAG (101) and TM (99) | RCARE (100) | Wet | 34.4 (1.9) and 34.9 (1.9) | 34.5 (2) | 1890 (242) and 1860 (184) | 1827 (208) | Axillary, admission | Axillary <36.5 | Axillary <35 | Radiant warmer, cotton cap, and transport incubator |
| Simon et al,52 2011; US | TM (17) | PBWr (19) | Wet | 26 (1.2) | 25.9 (1.3) | 812 (176) | 901 (248) | NR | Axillary <36.5 | NR | Radiant warmer, cotton or polyester cap, and transport incubator |
| Smith et al,53 2013; Australia | PWRAP (43) | RCARE (49) | Wet | NR | NR | 991 (299) | 982 (233) | Axillary, admission | NR | NR | Radiant warmer, cap, and transport in radiant warmer |
| Talakoub et al,54 2015; Iran | PBAG (32) and PBWrPCAP (32) | RCARE (32) | Wet | NR | NR | NR | NR | Axillary, admission | NR | NR | Radiant warmer, cotton cap, and transport incubator |
| Trevisanuto et al,55 2010; Italy | PBAG (32) and PCAP (32) | RCARE (32) | Wet | 25.8 (1.5) and 26.1 (1.4) | 26.3 (1) | 800 (223) and 834 (246) | 813 (225) | Axillary, admission | Axillary <36.4 | NR | Radiant warmer and transport incubator |
| Vohra et al,56 1999; Canada | PWRAP (27) | RCARE (32) | Wet | NR | NR | NR | NR | Rectal, admission | NR | NR | Radiant warmer and transport incubator |
| Vohra et al,57 2004; Canada | PWRAP (27) | RCARE (26) | Wet | 26 (1.5) | 26 (1.4) | 858 (199) | 825 (270) | Rectal, admission | NR | NR | Radiant warmer |
Abbreviations: INCUPBWr, plastic bag or wrap with incubator transport; NA, not applicable; NR, not reported; NRP, Neonatal Resuscitation Program; PBAG, plastic bag; PBWr, plastic bag or wrap; PWRAP, plastic wrap; PBWrHHGAS, plastic bag or wrap with heated humidified respiratory gases; PBWrPCAP, plastic bag or wrap with plastic cap; PBWrTM, plastic bag or wrap with thermal mattress; PCAP, plastic cap; RCARE, routine care; SSC, skin-to-skin contact; TM, thermal mattress.
Risk of Bias
Among the 34 included trials, 4 (12%) had high risk and 8 (24%) had unclear risk of selection bias.24,25,26,28,30,31,32,34,35,36,50,54 Masking of the interventions was not performed in most studies, except in 2 (6%) in which only the outcome assessors were masked.26,50 One trial (3%) had high risk of attrition bias,30 and 6 studies (18%) had high risk of other biases.26,27,30,40,43,50 The risk-of-bias assessment of individual trials is shown in eFigure 4 in the Supplement.
Primary Outcomes
Thirty-two studies (94%), which involved 3568 neonates, reported the primary outcome of core body (axillary or rectal) temperature at admission or within 2 hours of life.24,25,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,45,46,47,48,49,50,51,52,53,54,55,56,57 Eight interventions, including routine care, were evaluated in these 32 studies. Figure 1 shows the network plot, SUCRA plot, and forest plot with routine care as the common comparator. Figure 2 shows the league plot that depicts the network estimates for various comparisons. Forest plots for the direct evidence are provided in eFigure 5 in the Supplement. No inconsistency was found on node-splitting analysis (eFigure 6 in the Supplement). Certainty of evidence assessment for primary outcomes is listed in Table 2. The characteristics of the networks for all of the outcomes can be found in eTable 3 in the Supplement.
Figure 1. Network Plot, Surface Under the Cumulative Ranking Curve (SUCRA) Plot, and Forest Plot for Core Body Temperature at Admission or Within 2 Hours of Life.
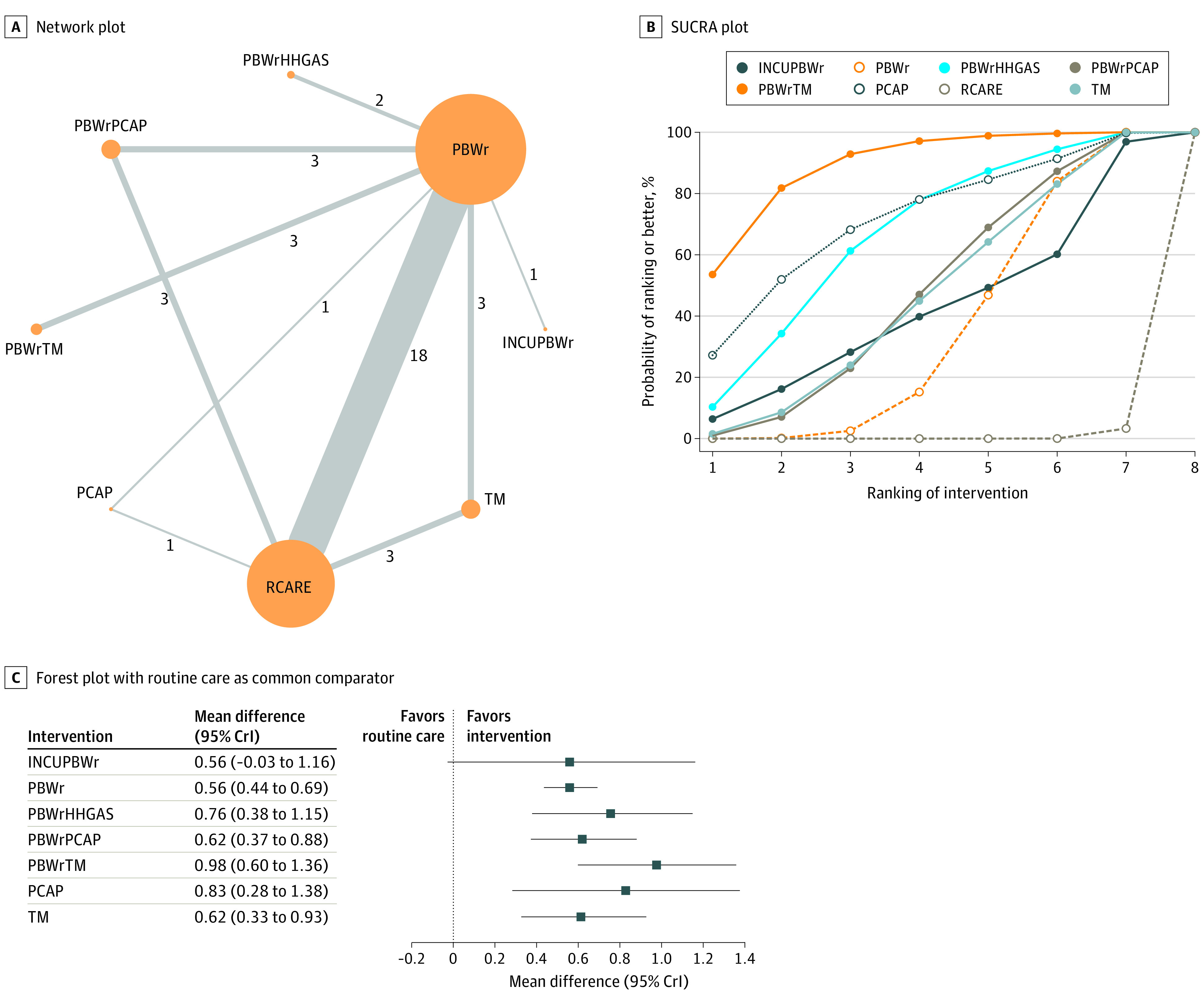
A, The size of nodes representing the interventions in network plots is proportional to the number of neonates receiving the intervention, and the width of the lines connecting the nodes is proportional to the number of trials evaluating the 2 interventions in a pairwise manner. The number of trials comparing any 2 interventions is indicated along the lines. B, SUCRA values for each intervention are as follows: plastic bag or wrap with thermal mattress (PBWrTM), 89.1%; plastic cap (PCAP), 71.6%; plastic bag or wrap with heated humidified respiratory gases (PBWrHHGAS), 66.5%; plastic bag or wrap with plastic cap (PBWrPCAP), 47.7%; thermal mattress (TM), 46.6%; plastic bag or wrap with incubator transport (INCUPBWr), 42.4%; plastic bag or wrap (PBWr), 35.5%; and routine care (RCARE), 4.7%. Higher rankings are associated with larger outcome values. C, Forest plot shows the mean difference (MD) in core temperature with 95% credible interval (CrI) of the different interventions with routine care as the common comparator.
Figure 2. League Plot of the Network Estimates for Core Body Temperature at Admission or Within 2 Hours of Life.
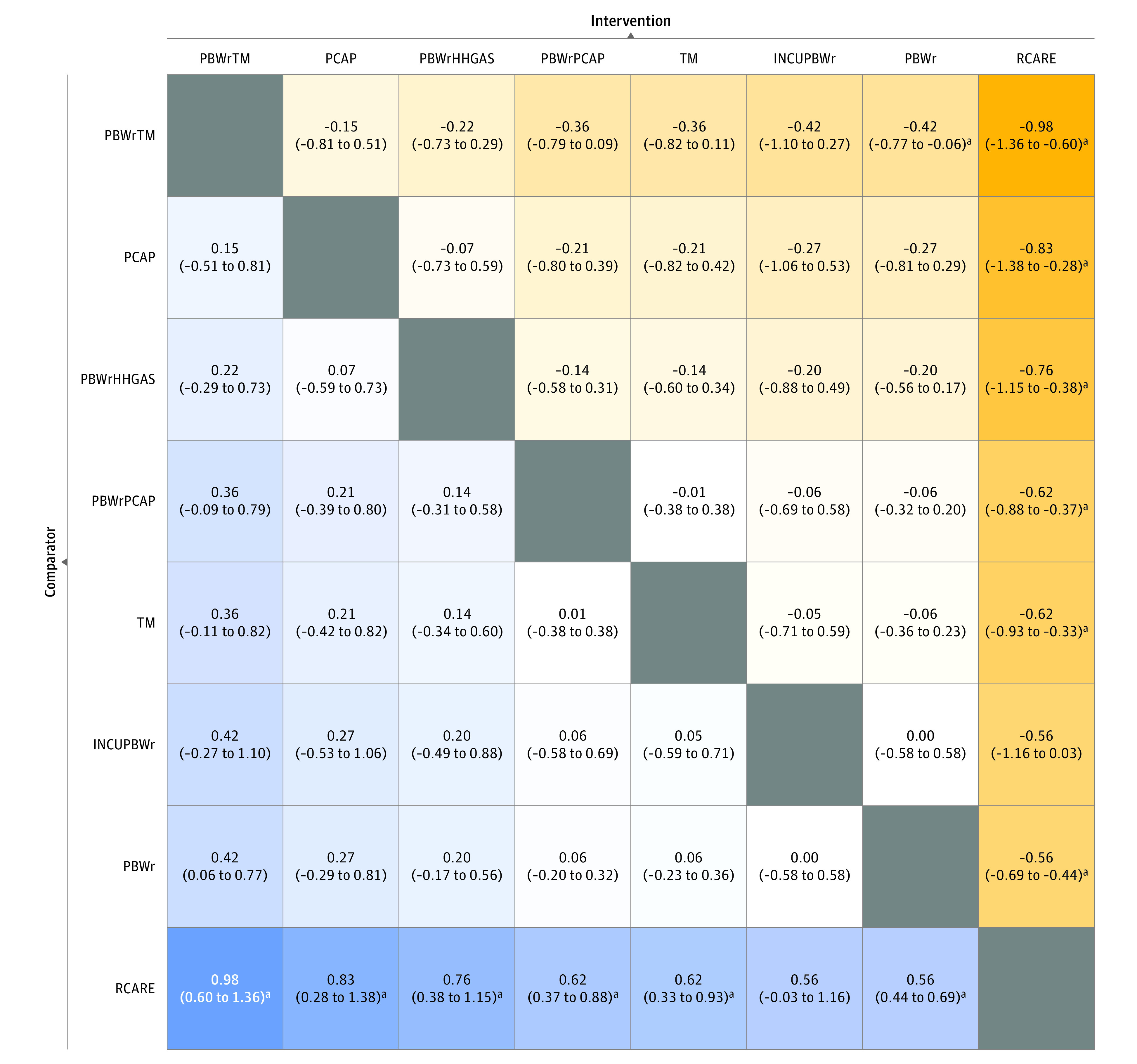
League plots compare the effect estimate for an intervention in the column with an intervention in a row. Network estimates are depicted as risk ratio (RR) with 95% credible interval (CrI). INCUPBWr indicates plastic bag or wrap with incubator transport; PBWr, plastic bag or wrap; PBWrHHGAS, plastic bag or wrap with heated humidified respiratory gases; PBWrPCAP, plastic bag or wrap with plastic cap; PBWrTM, plastic bag or wrap with thermal mattress; PCAP, plastic cap; RCARE, routine care; and TM, thermal mattress.
aRR is statistically significant.
Table 2. Certainty of Evidence for Different Comparisons for the Primary Outcomesa.
| Comparison | Indirect evidence | Direct evidence | Network meta-analysis | |
|---|---|---|---|---|
| Certainty of evidence | Certainty of evidence | MD or RR (95% CrI) | Certainty of evidence | |
| Primary outcome: mean core body (axillary or rectal) temperature at admission or within first 2 h of life | ||||
| PBWrTM:PCAP | Lowb,c | NA | MD: 0.15 °C (−0.51 to 0.81 °C) | Low |
| PBWrTM:PBWrHHGAS | Lowb,c | NA | MD: 0.22 °C (−0.29 to 0.73 °C) | Low |
| PBWrTM:PBWrPCAP | Lowb,c | NA | MD: 0.36 °C (−0.09 to 0.79 °C) | Low |
| PBWrTM:TM | Lowb,c | NA | MD: 0.36 °C (−0.11 to 0.82 °C) | Low |
| PBWrTM:INCUPBWr | Lowb,c | NA | MD: 0.42 °C (−0.27 to 1.10 °C) | Low |
| PBWrTM:PBWr | NA | Lowb,c | MD: 0.42 °C (0.06 to 0.77 °C) | Low |
| PBWrTM:RCARE | Lowb,c | NA | MD: 0.98 °C (0.60 to 1.36 °C) | Low |
| PCAP:PBWrHHGAS | Lowd | NA | MD: 0.07 °C (−0.59 to 0.73 °C) | Low |
| PCAP:PBWrPCAP | Lowc,e | NA | MD: 0.21 °C (−0.39 to 0.80 °C) | Low |
| PCAP:TM | Lowf,g | NA | MD: 0.21 °C (−0.42 to 0.82 °C) | Low |
| PCAP:INCUPBWr | Lowd | NA | MD: 0.27 °C (−0.53 to 1.06 °C) | Low |
| PCAP:PBWr | Moderatec | Lowd | MD: 0.27 °C (−0.29 to 0.81 °C) | Moderate |
| PCAP:RCARE | Lowd | Moderatec | MD: 0.83 °C (0.28 to 1.38 °C) | Moderate |
| PBWrHHGAS:PBWrPCAP | Lowc,e | NA | MD: 0.14 °C (−0.31 to 0.58 °C) | Low |
| PBWrHHGAS:TM | Lowf,g | NA | MD: 0.14 °C (−0.34 to 0.60 °C) | Low |
| PBWrHHGAS:INCUPBWr | Lowd | NA | MD: 0.20 °C (−0.49 to 0.88 °C) | Low |
| PBWrHHGAS:PBWr | NA | Moderatef,h | MD: 0.20 °C (−0.17 to 0.56 °C) | Moderate |
| PBWrHHGAS:RCARE | Moderatef,h | NA | MD: 0.76 °C (0.38 to 1.15 °C) | Moderate |
| PBWrPCAP:TM | Lowc,e | NA | MD: 0.01 °C (−0.38 to 0.38 °C) | Low |
| PBWrPCAP:INCUPBWr | Lowc,e | NA | MD: 0.06 °C (−0.58 to 0.69 °C) | Low |
| PBWrPCAP:PBWr | Lowc,i,h | Lowc,e | MD: 0.06 °C (−0.20 to 0.32 °C) | Low |
| PBWrPCAP:RCARE | Lowc,i,h | Lowc,i,h | MD: 0.62 °C (0.37 to 0.88 °C) | Low |
| TM:INCUPBWr | Lowf,g | NA | MD: 0.05 °C (−0.59 to 0.71 °C) | Low |
| TM:PBWr | Moderatej,h | Lowf,g | MD: 0.06 °C (−0.23 to 0.36 °C) | Moderate |
| TM:RCARE | Lowf,g | Moderatej,h | MD: 0.62 °C (0.33 to 0.93 °C) | Moderate |
| INCUPBWr:PBWr | NA | Lowd | MD: 0.00 °C (−0.58 to 0.58 °C) | Low |
| INCUPBWr:RCARE | Lowd | NA | MD: 0.56 °C (−0.03 to 1.16 °C) | Low |
| PBWr:RCARE | Lowc,i,h | Moderatek,h,l | MD: 0.56 °C (0.44 to 0.69 °C) | Moderate |
| Primary outcome: incidence of moderate to severe hypothermia (core body [axillary or rectal] temperature <36 °C) at admission or within first 2 h of life | ||||
| SSC:PBWrHHGAS | Lowc,m | NA | RR: 32.44 (0.01-51.67) | Low |
| SSC:PBWrTM | Lowc,m | NA | RR: 34.67 (0.00-39.26) | Low |
| SSC:PBWrPCAP | Very lowg,n,o | NA | RR: 3.16 (0.00-9.51) | Very low |
| SSC:TM | Lowc,m | NA | RR: 136.23 (0.01-153.95) | Low |
| SSC:PBWr | Lowc,m | NA | RR: 3.24 (0.01-9.85) | Low |
| SSC:INCUPBWr | Lowc,m | NA | RR: 8.95 (0.00-10.38) | Low |
| SSC:RCARE | NA | Lowc,m | RR: 0.29 (0.00-1.20) | Low |
| PBWrHHGAS:PBWrTM | Lown,p | NA | RR: 5.23 (0.02-12.02) | Low |
| PBWrHHGAS:PBWrPCAP | Very lowg,n,o | NA | RR: 0.67 (0.02-2.81) | Very low |
| PBWrHHGAS:TM | Lown,p | NA | RR: 74.08 (0.04-87.00) | Low |
| PBWrHHGAS:PBWr | NA | Lown,p | RR: 0.54 (0.05-2.01) | Low |
| PBWrHHGAS:INCUPBWr | Lown,p | NA | RR: 1.10 (0.00-3.35) | Low |
| PBWrHHGAS:RCARE | Lown,p | NA | RR: 0.12 (0.00-0.47) | Low |
| PBWrTM:PBWrPCAP | Very lowg,n,o | NA | RR: 3.40 (0.02-8.65) | Very low |
| PBWrTM:TM | Lown,q | NA | RR: 192.45 (0.05-228.44) | Low |
| PBWrTM:PBWr | NA | Lown,q | RR: 1.78 (0.05-7.20) | Low |
| PBWrTM:INCUPBWr | Lown,q | NA | RR: 6.24 (0.01-9.33) | Low |
| PBWrTM:RCARE | Lown,q | NA | RR: 0.43 (0.01-1.46) | Low |
| PBWrPCAP:TM | Lowr | NA | RR: 102.96 (0.22-277.98) | Low |
| PBWrPCAP:PBWr | Lowr | Very lowg,n,o | RR: 1.65 (0.27-5.91) | Low |
| PBWrPCAP:INCUPBWr | Very lowg,n,o | NA | RR: 3.57 (0.02-11.03) | Very low |
| PBWrPCAP:RCARE | Very lowg,n,o | Lowr | RR: 0.33 (0.04-1.05) | Low |
| TM:PBWr | Lowc,m | Lows | RR: 0.91 (0.01-4.60) | Low |
| TM:INCUPBWr | Lowc,m | NA | RR: 5.17 (0.00-5.45) | Low |
| TM:RCARE | Lows | Lowc,m | RR: 0.12 (0.00-0.62) | Low |
| PBWr:INCUPBWr | NA | Lows | RR: 1.39 (0.02-5.92) | Low |
| PBWr:RCARE | Lows | Moderatec | RR: 0.23 (0.04-0.55) | Moderate |
| INCUPBWr:RCARE | Lows | NA | RR: 2.27 (0.02-9.31) | Low |
Abbreviations: CrI, credible interval; INCUPBWr, plastic bag or wrap with incubator transport; MD, mean difference; NA, not available; PBWr, plastic bag or wrap; PBWrHHGAS, plastic bag or wrap with heated humidified respiratory gases; PBWrPCAP, plastic bag or wrap with plastic cap; PBWrTM, plastic bag or wrap with thermal mattress; PCAP, plastic cap; RCARE, routine care; RR, risk ratio; SSC, skin-to-skin contact; TM, thermal mattress.
The primary outcome was not downgraded for lack of blinding in any comparison because it was an objective outcome and blinding was difficult for these interventions.
Downgraded by 1 level for serious risk of bias because of 1 study32 in which 45% weight was quasi-randomized.
Downgraded by 1 level for serious imprecision because an optimal information size criterion was not met.
Downgraded by 2 levels for very serious imprecision because of small sample size and the CrI included no difference.
Downgraded by 1 level for serious risk of bias because of possible selection bias in 2 studies.33,54
Downgraded by 1 level for serious imprecision because the CrI included no difference.
Downgraded by 1 level for serious inconsistency because of heterogeneity.
Not downgraded for inconsistency because the heterogeneity was associated with differences between small and large beneficial outcomes.
Downgraded by 1 level for serious risk of bias because of possible selection bias in 2 studies.50,54
Downgraded by 1 level for serious risk of bias because of possible selection bias in 2 studies.25,28
Downgraded by 1 level for publication bias.
Not downgraded for risk of bias because the studies with possible risk of bias24,30,31,34,35,54 contributed only 27% weight, and 73% weight of effect estimate was from good-quality studies.
Downgraded by 1 level for serious risk of bias because of possible selection bias in the included study.26
Downgraded by 1 level for serious imprecision because the CrI reached no difference.
Downgraded by 1 level for serious risk of bias because of possible selection bias in 1 study.36
Not downgraded for heterogeneity because the heterogeneity was associated with the differences between small and large beneficial outcomes.
Downgraded by 1 level for serious risk of bias because of possible selection bias in the included study.32
Downgraded by 2 levels for very serious imprecision because of data from 1 study27 with a small sample size and risk benefit could not be decided.
Downgraded by 2 levels for very serious imprecision because of data from 1 study44 with a small sample size and risk benefit could not be decided.
Compared with routine care alone, plastic bag or wrap with a thermal mattress (MD, 0.98 °C; 95% CrI, 0.60-1.36 °C), plastic cap (MD, 0.83 °C; 95% CrI, 0.28-1.38 °C), plastic bag or wrap with heated humidified respiratory gas (MD, 0.76 °C; 95% CrI, 0.38-1.15 °C), plastic bag or wrap with a plastic cap (MD, 0.62 °C; 95% CrI, 0.37-0.88 °C), thermal mattress (MD, 0.62 °C; 95% CrI, 0.33-0.93 °C), and plastic bag or wrap alone (MD, 0.56 °C; 95% CrI, 0.44-0.69 °C) were associated with greater core body temperature. Certainty of evidence was moderate for 5 interventions and was low for plastic bag or wrap with a thermal mattress. Plastic bag or wrap with a thermal mattress was ranked as the most beneficial intervention (SUCRA value, 89.1%).
In a sensitivity analysis of plastic bag and plastic wrap as separate interventions, both plastic bag and plastic wrap were found to be equally good at maintaining core body temperature (MD, 0.06 °C; 95% CrI, −0.19 to 0.30 °C). Certainty of evidence was moderate (eFigures 7 and 8 in the Supplement). Inconsistency was detected in the network for the plastic bag vs routine care comparison (eFigure 9 in the Supplement). Certainty of evidence assessment for sensitivity analyses and secondary outcomes is listed in eTable 4 in the Supplement.
In a sensitivity analysis of studies in which the mean gestational age of the newborns was 30 weeks or less, the results were similar to those of the primary analysis. However, incubator transport was also associated with greater core body temperature compared with routine care (MD, 0.68 °C; 95% CrI, 0.16-1.22 °C) (eFigures 10-12 in the Supplement).
Core body temperature was evaluated at 3 gestational ages: 24, 30, and 34 weeks. Although all of the interventions were associated with significantly greater core body temperatures for neonates at 24 weeks of gestation, some interventions (ie, plastic cap, incubator transport, and plastic bag or wrap with heated humidified gas) had imprecise estimates for those at 30 and 34 weeks of gestation (eFigure 13 in the Supplement).
In a sensitivity analysis of drying vs no drying before application of plastic bag or wrap, the core body temperature was comparable between drying vs no drying for both plastic bag or wrap alone (MD, −0.09 °C; 95% CrI, −0.38 to 0.19 °C; moderate certainty of evidence) and plastic bag or wrap with plastic cap (MD, −0.37 °C; 95% CrI, −0.90 to 0.15 °C; very low certainty of evidence) (eFigures 14 and 15 in the Supplement).
Eight interventions, including routine care, were evaluated for the other primary outcome of incidence of moderate to severe hypothermia at admission or within 2 hours of life. Figure 3 shows the network, SUCRA, and forest plots for these interventions. Plastic bag or wrap alone (RR, 0.23; 95% CrI, 0.04-0.55), thermal mattress (RR, 0.12; 95% CrI, 0.00-0.62), and plastic bag or wrap with heated humidified gas (RR, 0.12; 95% CrI, 0.00-0.47) were associated with reduced risk of moderate to severe hypothermia compared with routine care. These findings are depicted in a league plot in eFigure 16 in the Supplement. Certainty of evidence was moderate for plastic bag or wrap alone and was low for thermal mattress and plastic bag or wrap with heated humidified gas. Thermal mattress (SUCRA value, 76.9%) and plastic bag or wrap with heated humidified gas (SUCRA value, 74.9%) were ranked as the 2 best interventions. However, certainty of evidence was low for both. Direct estimates are depicted in eFigure 17 in the Supplement, and no inconsistency was found in the network (eFigure 18 in the Supplement).
Figure 3. Network Plot, Surface Under the Cumulative Ranking Curve (SUCRA) Plot, and Forest Plot for Moderate to Severe Hypothermia at Admission or Within 2 Hours of Life.
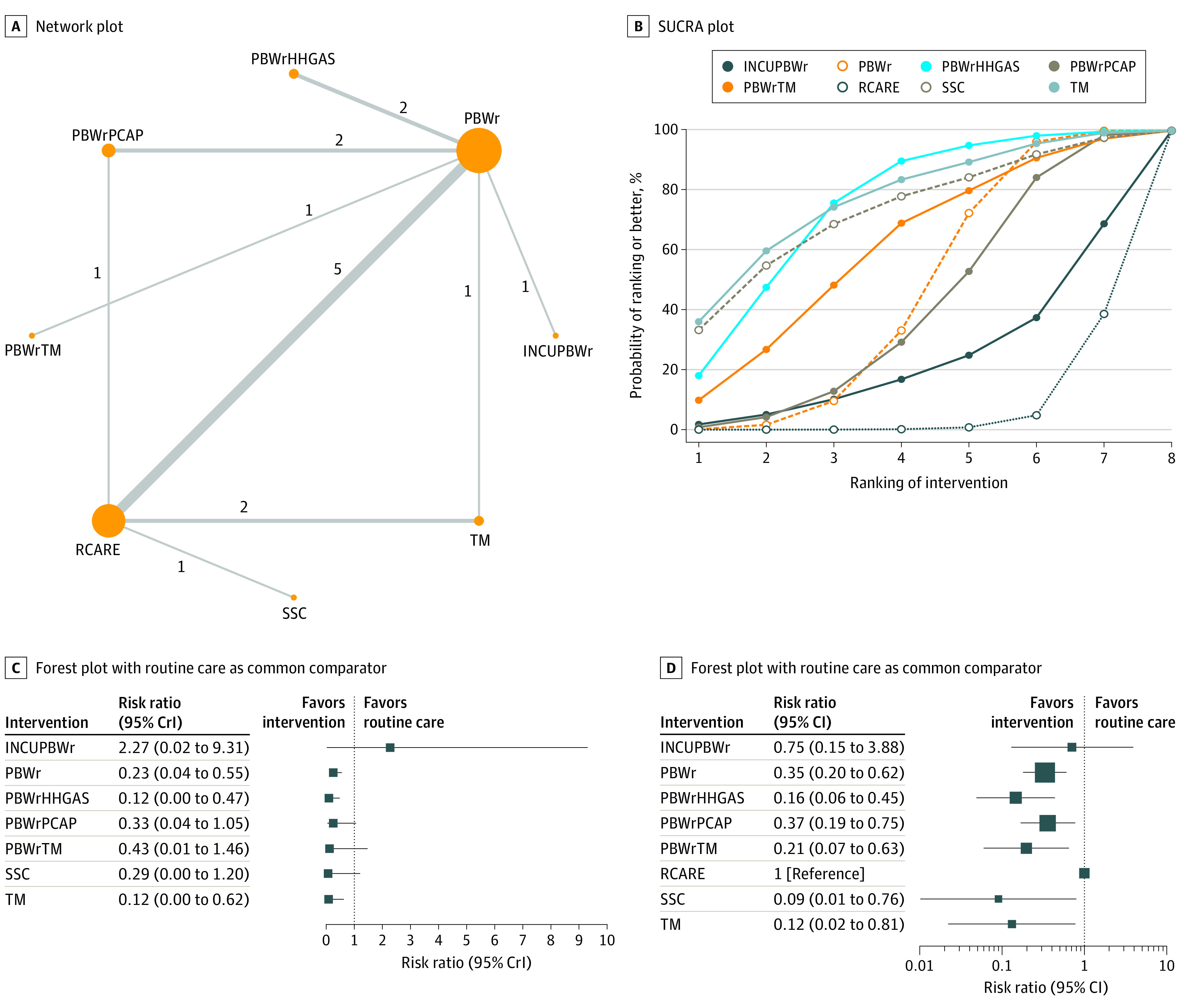
A, The size of nodes representing the interventions in network plots is proportional to the number of neonates receiving the intervention, and the width of the lines connecting the nodes is proportional to the number of trials evaluating the 2 interventions in a pairwise manner. The number of trials comparing any 2 interventions is indicated along the lines. B, SUCRA values are arranged from highest to lowest, as follows: thermal mattress (TM), 76.9%; plastic bag or wrap with heated humidified respiratory gases (PBWrHHGAS), 74.9%; skin-to-skin contact (SSC), 72.7%; plastic bag or wrap with thermal mattress (PBWrTM), 60.3%; plastic bag or wrap (PBWr), 44.8%; plastic bag or wrap with plastic cap (PBWrPCAP), 40.4%; plastic bag or wrap with incubator transport (INCUPBWr), 23.6%; and routine care (RCARE), 6.4%. Higher rankings are associated with better outcome values. C, Forest plot used the bayesian approach. D, Forest plot used the frequentist approach. CrI indicates credible interval; RR, risk ratio.
The CrIs of network estimates were wider for many comparisons when assessed against the direct evidence from pairwise comparisons. Hence, a sensitivity analysis was performed using the frequentist method of the random-effects model. The results were similar, and the estimates were more precise for plastic bag or wrap with a plastic cap (RR, 0.37; 95% CI, 0.19-0.75), plastic bag or wrap with a thermal mattress (RR, 0.21; 95% CI, 0.07-0.63), and skin-to-skin contact (RR, 0.09; 95% CI, 0.01-0.76) (Figure 3D).
In a sensitivity analysis of incidence of any hypothermia, interventions such as skin-to-skin contact, plastic bag or wrap with heated humidified gas, plastic bag or wrap with a thermal mattress, plastic bag or wrap with a plastic cap, thermal mattress, and plastic bag or wrap were associated with lower risk of any hypothermia compared with routine care alone (eFigures 19-22 in the Supplement).
Secondary Outcomes
Plastic bag or wrap with a plastic cap was associated with decreased risk of mortality before discharge when compared with plastic bag or wrap alone (RR, 0.26; 95% CrI, 0.02-0.86) and routine care (RR, 0.19; 95% CrI, 0.02-0.66; low certainty of evidence) (eFigures 23-26 in the Supplement).
Only direct evidence from pairwise meta-analysis revealed an increased risk of hyperthermia for plastic bag or wrap alone vs routine care (RR, 3.39; 95% CrI, 1.84-6.25) as well as for plastic bag or wrap with a thermal mattress vs plastic bag or wrap alone (RR, 2.25; 95% CrI, 1.13-4.50) (eFigures 27-30 in the Supplement).
Plastic bag or wrap with heated humidified gas was associated with decreased risk of major brain injury compared with routine care (RR, 0.23; 95% CrI, 0.03-0.67) and showed a pattern toward less risk for major brain injury compared with plastic bag or wrap alone (RR, 0.38; 95% CrI, 0.08-1.08; moderate certainty of evidence) (eFigures 31-33 in the Supplement). All of the results are summarized in eTable 5 in the Supplement.
Discussion
This systematic review and network meta-analysis included 34 trials of 9 thermal care interventions in 3688 preterm neonates to prevent hypothermia immediately after birth in the delivery room. Most of the interventions showed better performance compared with routine care alone in stabilizing the core body temperature and reducing the risk of moderate to severe hypothermia. However, there were distinct differences between the interventions for the secondary outcomes of hyperthermia, mortality, and major brain injury.
A systematic review and meta-analysis by McCall et al8 showed that plastic bag or wrap was associated with improved core body temperature at admission or within 2 hours of life with moderate certainty of evidence. The data for other interventions were small, and the evidence was not graded.8 In the present study, we found moderate certainty of evidence that 5 interventions (plastic bag or wrap, thermal mattress, plastic bag or wrap with heated humidified gas, and thermal mattress and plastic cap) were associated with greater core body temperature. This finding could be attributed to an increase in statistical power by the addition of evidence from the indirect fraction as well as the inclusion of 9 additional studies in this network meta-analysis.24,25,36,37,43,44,45,46,48,51
Because the various thermal care interventions have different mechanisms of action for preventing heat loss, using a combination of interventions might be beneficial for the most vulnerable neonates. SUCRA ranked plastic bag or wrap with a thermal mattress as the best intervention for improving core body temperature at admission or within 2 hours of life. However, direct evidence indicated that plastic bag or wrap with a thermal mattress might be associated with higher risk of hyperthermia. Although these findings were not reflected in the final network estimates, these estimates were derived from a sparse network in which bayesian analysis with a random-effects approach is known to present imprecise results when compared with the direct evidence.65 Hence, plastic bag or wrap with a thermal mattress might not be recommended as the first choice until more adequately powered studies on hyperthermia are available.
The mean differences in the core temperature between the different thermal adjuncts and routine care varied from 0.56 °C to 0.98 °C. Although these differences were statistically significant, it is important to ponder whether they translated into clinical benefits. Observational studies and quality improvement projects have indicated that better temperature profiles at admission to the neonatal intensive care unit are associated with decreased mortality and morbidity, but meta-analyses of RCTs have failed to show the clinical benefits of these thermal care interventions.4,7,8 On the contrary, in this network meta-analysis, we found important clinical benefits for plastic bag or wrap with heated humidified gas, which decreased the risk of major brain injury (with moderate certainty of evidence), and for plastic bag or wrap with a plastic cap, which decreased the risk of mortality (with low certainty of evidence). In addition, plastic bag or wrap and plastic bag or wrap with a thermal mattress showed a pattern toward lower mortality (with low certainty of evidence) compared with routine care.
We conducted a meta-regression for core body temperature with gestational age as a covariate. Although the meta-regression showed that the benefit of thermal care adjuncts was greater at lower gestational ages, some of the interventions were still beneficial at 34 weeks of gestation. The results of individual trials that were conducted in more mature newborns were also in agreement with this finding.26,30,51 We suggest further research in this group of neonates, especially in resource-limited settings in which radiant warmers and transport incubators might not be available and low-cost interventions such as plastic bag or wrap and plastic cap may play an important role in reducing hypothermia and neonatal mortality. Furthermore, presterilized plastic bag or wrap and plastic cap might be the most feasible interventions during delayed cord clamping, which is now considered the standard of care in term and preterm neonates.66 None of the included studies had examined thermal care interventions during delayed cord clamping, which potentially represents a period of rapid heat loss in preterm newborns.
Plastic bags and wraps work by the same principle of reducing evaporative and convective heat loss and seem to be technically similar; however, they may differ in thickness of the plastic material, ease of application, extent of body coverage, and risk of displacement, among other factors. A systematic review on plastic bag or wrap suggested possible differences between plastic bags and wraps and recommended further studies to evaluate the advantages of plastic bags vs wraps.10 However, we found that plastic bags and wraps were equally beneficial. The 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations suggested applying a plastic bag or wrap to the newborn immediately after birth without prior drying.7 This advice is based on the understanding that extremely preterm neonates have high transepidermal water loss; keeping the newborn wet inside the plastic bag or wrap creates a high-humidity microenvironment and reduces evaporative heat loss. However, this recommendation does not have a high level of evidence. We found that drying vs no drying before applying a plastic bag or wrap may not make a difference in maintaining core body temperature, with moderate certainty of evidence.
To define hypothermia, the included studies used a cutoff temperature of less than 36.5 °C or less than 36 °C for rectal or axillary temperature. Although we considered both rectal and axillary temperature as core body temperature, as followed in the systematic review and meta-analysis by McCall et al,8 a difference of 0.5 °C or higher between rectal and axillary temperature has been reported in neonates.67,68 Hence, to avoid this variability and the risk of inconsistency secondary to intransivity, we analyzed the incidence of moderate to severe hypothermia (temperature <36 °C) as a primary outcome rather than any hypothermia. Plastic bag or wrap was associated with decreased risk of moderate to severe hypothermia at admission or within 2 hours of life (with moderate certainty of evidence) compared with routine care. Two other recent systematic reviews on plastic bag or wrap also found substantial reduction in hypothermia with use of this intervention.9,10 The frequentist analysis showed that most thermal care interventions were successful in reducing the risk of moderate to severe hypothermia.
Limitations
This study has several limitations. First, the variation among demographic and other characteristics, such as gestational age, diverse delivery room care practices, and the underlying sickness profile of the neonates, in the included trials might have introduced intransitivity in this network meta-analysis. Second, wide differences were observed in the way temperature was measured (axillary vs rectal) in the included trials. Third, we did not analyze some a priori decided secondary outcomes because limited data were available. Fourth, many of the included RCTs were single-center trials with small sample size and low event rates, making the effect estimates prone to selective reporting and publication bias. Fifth, we were unable to access unpublished data from the included studies and relied instead on the systematic review by McCall et al.8
Conclusions
Most of the thermal care interventions used in the delivery room were associated with better core body temperature (with moderate certainty of evidence) and decreased risk of moderate to severe hypothermia (with moderate certainty of evidence for plastic bag or wrap, but low to very low certainty of evidence for other interventions) at admission or within the first 2 hours of life compared with routine care alone. Use of a plastic bag or wrap with heated humidified gas was associated with reduced risk of major brain injury (with moderate certainty of evidence) and a plastic bag or wrap with a plastic cap was associated with lower risk of mortality (with low certainty of evidence). Future RCTs that are adequately powered to assess important clinical outcomes are warranted.
eFigure 1. PRISMA flow
eFigure 2. Mean gestational age of the enrolled neonates
eFigure 3. Mean birth weight of the enrolled neonates
eFigure 4. Risk of bias summary and graph of the included trials
eFigure 5. Direct evidence from the pair wise comparisons for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 6. Split between direct and indirect evidence for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 7. Sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 8. League plot depicting the network estimate [MD (95% CrI)] for sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 9. Split between direct and indirect evidence for sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 10. Sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 11. League plot depicting the network estimate for sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 12. Split between direct and indirect evidence for sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 13. Meta-regression with gestational age as covariate
eFigure 14. Sensitivity analysis by evaluating drying versus no drying before wrapping in a plastic bag/wrap for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 15. League plot depicting the network estimate for sensitivity analysis - drying vs no drying before wrapping in a plastic bag/wrap for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 16. League plot depicting the network estimate [RR (95% CrI)] for primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 17. Direct evidence from the pair wise comparisons for the primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 18. Split between direct and indirect evidence for the primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 19. Sensitivity analysis by evaluating any hypothermia (defined as core body temperature less than 36.5 °C at admission or within 1-2 hours of life). A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 20. League plot depicting the network estimate [RR (95% CrI)] for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 21. Split between direct and indirect evidence for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 22. Direct evidence from the pair wise comparisons for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 23. Mortality before discharge. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 24. League plot depicting the network estimate [RR (95% CrI)] for mortality before discharge
eFigure 25. Split between direct and indirect evidence for mortality before discharge
eFigure 26. Direct evidence from the pair wise comparisons for mortality before discharge
eFigure 27. Hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 28. League plot depicting the network estimate [RR (95% CrI)] for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life
eFigure 29. Split between direct and indirect evidence for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 °C] at admission or within 2 hours of life
eFigure 30. Direct evidence from the pair wise comparisons for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life
eFigure 31. Major brain injury (MBI) defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 32. League plot depicting the network estimate [RR (95% CrI)] for MBI [defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia]
eFigure 33. Direct evidence from the pair wise comparisons for MBI [defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia]
eFigure 34. Funnel plots and trim plots for pairwise comparisons - 'PBWr' versus 'routine
care' for outcomes - mean core body temperature, mortality before discharge, hyperthermia
eTable 1. Literature search strategy for two electronic databases
eTable 2. Some of the studies that were excluded for valid reasons
eTable 3. Network characteristics for all the outcomes and sensitivity analysis
eTable 4. Certainty of evidence for different comparisons for the sensitivity analyses and secondary outcomes
eTable 5. Summary of results of the network meta-analysis
eReferences
References
- 1.Lunze K, Bloom DE, Jamison DT, Hamer DH. The global burden of neonatal hypothermia: systematic review of a major challenge for newborn survival. BMC Med. 2013;11:24. doi: 10.1186/1741-7015-11-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vermont Oxford Network . Despite decreases, nearly 4 in 10 infants are cold when admitted to the NICU. Accessed December 5, 2020. https://public.vtoxford.org/nicu-by-the-numbers/despite-decreases-nearly-4-in-10-infants-are-cold-when-admitted-to-the-nicu/
- 3.Laptook AR, Bell EF, Shankaran S, et al. ; Generic and Moderate Preterm Subcommittees of the NICHD Neonatal Research Network . Admission temperature and associated mortality and morbidity among moderately and extremely preterm infants. J Pediatr. 2018;192:53-59.e2. doi: 10.1016/j.jpeds.2017.09.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Laptook AR, Salhab W, Bhaskar B; Neonatal Research Network . Admission temperature of low birth weight infants: predictors and associated morbidities. Pediatrics. 2007;119(3):e643-e649. doi: 10.1542/peds.2006-0943 [DOI] [PubMed] [Google Scholar]
- 5.de Siqueira Caldas JP, Ferri WAG, Marba STM, et al. Admission hypothermia, neonatal morbidity, and mortality: evaluation of a multicenter cohort of very low birth weight preterm infants according to relative performance of the center. Eur J Pediatr. 2019;178(7):1023-1032. doi: 10.1007/s00431-019-03386-9 [DOI] [PubMed] [Google Scholar]
- 6.Wilson E, Maier RF, Norman M, et al. ; Effective Perinatal Intensive Care in Europe (EPICE) Research Group . Admission hypothermia in very preterm infants and neonatal mortality and morbidity. J Pediatr. 2016;175:61-67.e4. doi: 10.1016/j.jpeds.2016.04.016 [DOI] [PubMed] [Google Scholar]
- 7.Wyckoff MH, Wyllie J, Aziz K, et al. ; Neonatal Life Support Collaborators . Neonatal life support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation. 2020;156:A156-A187. doi: 10.1016/j.resuscitation.2020.09.015 [DOI] [PubMed] [Google Scholar]
- 8.McCall EM, Alderdice F, Halliday HL, Vohra S, Johnston L. Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2018;2(2):CD004210. doi: 10.1002/14651858.CD004210.pub5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Oatley HK, Blencowe H, Lawn JE. The effect of coverings, including plastic bags and wraps, on mortality and morbidity in preterm and full-term neonates. J Perinatol. 2016;36(suppl 1):S83-S89. doi: 10.1038/jp.2016.35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Li S, Guo P, Zou Q, He F, Xu F, Tan L. Efficacy and safety of plastic wrap for prevention of hypothermia after birth and during NICU in preterm infants: a systematic review and meta-analysis. PLoS One. 2016;11(6):e0156960. doi: 10.1371/journal.pone.0156960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Meyer MP, Owen LS, Te Pas AB. Use of heated humidified gases for early stabilization of preterm infants: a meta-analysis. Front Pediatr. 2018;6:319. doi: 10.3389/fped.2018.00319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dias S, Caldwell DM. Network meta-analysis explained. Arch Dis Child Fetal Neonatal Ed. 2019;104(1):F8-F12. doi: 10.1136/archdischild-2018-315224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Abiramalatha T, Ramaswamy V, Thanigainathan S, Bandyopadhyay T, Roehr CC, Pullattayil AK. Delivery room interventions to reduce hypothermia soon after birth in preterm and low birth weight infants: a systematic review and network meta-analysis. Accessed April 10, 2021. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020216008. [DOI] [PMC free article] [PubMed]
- 14.Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-784. doi: 10.7326/M14-2385 [DOI] [PubMed] [Google Scholar]
- 15.Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92(4):529-534. doi: 10.1016/S0022-3476(78)80282-0 [DOI] [PubMed] [Google Scholar]
- 16.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi: 10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Higgins JPT, Thomas J, Chandler J, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.0. Cochrane; 2021. Accessed December 5, 2020. http://www.training.cochrane.org/handbook
- 18.Shim SR, Kim SJ, Lee J, Rücker G. Network meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019013. doi: 10.4178/epih.e2019013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Béliveau A, Boyne DJ, Slater J, Brenner D, Arora P. BUGSnet: an R package to facilitate the conduct and reporting of Bayesian network meta-analyses. BMC Med Res Methodol. 2019;19(1):196. doi: 10.1186/s12874-019-0829-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Brooks S, Gelman A. General methods for monitoring convergence of iterative simulations. J Comput Graph Stat. 1998;7(4):434-455. [Google Scholar]
- 21.Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med. 2010;29(7-8):932-944. doi: 10.1002/sim.3767 [DOI] [PubMed] [Google Scholar]
- 22.Mbuagbaw L, Rochwerg B, Jaeschke R, et al. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst Rev. 2017;6(1):79. doi: 10.1186/s13643-017-0473-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Puhan MA, Schünemann HJ, Murad MH, et al. ; GRADE Working Group . A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi: 10.1136/bmj.g5630 [DOI] [PubMed] [Google Scholar]
- 24.Ahmed BT, Hussein M, Monir H. Effect of plastic bag (vinyl bags) on prevention of hypothermia in preterm infants. Med J Cairo Univ. 2013;81(2):169-173. [Google Scholar]
- 25.Almeida PG. Transwarmer Mattress Project (TeMP) at Delivery: A Prospective Randomized Control Trial of the Transwarmer Mattress to Reduce Admission Hypothermia of Low Birth Weight Infants. Dissertation. University of Hawaii; 2013. [Google Scholar]
- 26.Bergman NJ, Linley LL, Fawcus SR. Randomized controlled trial of skin-to-skin contact from birth versus conventional incubator for physiological stabilization in 1200- to 2199-gram newborns. Acta Paediatr. 2004;93(6):779-785. doi: 10.1111/j.1651-2227.2004.tb03018.x [DOI] [PubMed] [Google Scholar]
- 27.Bhavsar SR, Kabra NS, Avasthi BS, et al. Efficacy and safety of polyethylene wrap in preventing hypothermia in preterm and low birth weight neonates during transport: a randomised controlled trial. Perinatology. 2015;16(1):23–30. [Google Scholar]
- 28.Brennan AB. Effect of Sodium Acetate Transport Mattresses on Admission Temperatures of Infants ≤ 1500 Grams. Dissertation. University of Florida; 1996. [Google Scholar]
- 29.Çağlar S, Gözen D, Ince Z. Heat loss prevention (HELP) after birth in preterm infants using vinyl isolation bag or polyethylene wrap. J Obstet Gynecol Neonatal Nurs. 2014;43(2):216-223. doi: 10.1111/1552-6909.12291 [DOI] [PubMed] [Google Scholar]
- 30.Cardona Torres LM, Amador Licona N, Garcia Campos ML, Guizar-Mendoza JM. Polyethylene wrap for thermoregulation in the preterm infant: a randomized trial. Indian Pediatr. 2012;49(2):129-132. doi: 10.1007/s13312-012-0020-x [DOI] [PubMed] [Google Scholar]
- 31.Chantaroj S, Techasatid W. Effect of polyethylene bag to prevent heat loss in preterm infants at birth: a randomized controlled trial. J Med Assoc Thai. 2011;94(suppl 7):S32-S37. [PubMed] [Google Scholar]
- 32.Chawla S, Amaram A, Gopal SP, Natarajan G. Safety and efficacy of trans-warmer mattress for preterm neonates: results of a randomized controlled trial. J Perinatol. 2011;31(12):780-784. doi: 10.1038/jp.2011.33 [DOI] [PubMed] [Google Scholar]
- 33.Doglioni N, Cavallin F, Mardegan V, et al. Total body polyethylene wraps for preventing hypothermia in preterm infants: a randomized trial. J Pediatr. 2014;165(2):261-266.e1. doi: 10.1016/j.jpeds.2014.04.010 [DOI] [PubMed] [Google Scholar]
- 34.Farhadi R, Naderi M, Rahmani Z, Ghafari V, Khalilian A.. Effect of “ZIPKIF” plastic bag on prevention of hypothermia in preterm infants: a randomised controlled trial. J Mazandaran Univ Med Sciences. 2012;22(93):19-26. [Google Scholar]
- 35.Gathwala G, Singh GK, Agrawal N. Safety and efficacy of vinyl bags in prevention of hypothermia of preterm neonates at birth. Indian J Public Health. 2010;54(1):24-26. doi: 10.4103/0019-557X.70543 [DOI] [PubMed] [Google Scholar]
- 36.Shafie H, Syed Zakaria SZ, Adli A, Shareena I, Rohana J. Polyethylene versus cotton cap as an adjunct to body wrap in preterm infants. Pediatr Int. 2017;59(7):776-780. doi: 10.1111/ped.13285 [DOI] [PubMed] [Google Scholar]
- 37.Hu XJ, Wang L, Zheng RY, et al. Using polyethylene plastic bag to prevent moderate hypothermia during transport in very low birth weight infants: a randomized trial. J Perinatol. 2018;38(4):332-336. doi: 10.1038/s41372-017-0028-0 [DOI] [PubMed] [Google Scholar]
- 38.Knobel RB, Wimmer JE Jr, Holbert D. Heat loss prevention for preterm infants in the delivery room. J Perinatol. 2005;25(5):304-308. doi: 10.1038/sj.jp.7211289 [DOI] [PubMed] [Google Scholar]
- 39.Leadford AE, Warren JB, Manasyan A, et al. Plastic bags for prevention of hypothermia in preterm and low birth weight infants. Pediatrics. 2013;132(1):e128-e134. doi: 10.1542/peds.2012-2030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Leslie A, Wardle SP, Budge H, Marlow N, Brocklehurst P. Randomised controlled trial of gel warming mattresses to prevent hypothermia during resuscitation at birth of premature infants. Paper presented at: Neonatal Society 2007 Autumn Meeting; November 22, 2007; London. [Google Scholar]
- 41.Mathew B, Lakshminrusimha S, Sengupta S, Carrion V. Randomized controlled trial of vinyl bags versus thermal mattress to prevent hypothermia in extremely low-gestational-age infants. Am J Perinatol. 2013;30(4):317-322. [DOI] [PubMed] [Google Scholar]
- 42.McCarthy LK, Molloy EJ, Twomey AR, Murphy JF, O’Donnell CP. A randomized trial of exothermic mattresses for preterm newborns in polyethylene bags. Pediatrics. 2013;132(1):e135-e141. doi: 10.1542/peds.2013-0279 [DOI] [PubMed] [Google Scholar]
- 43.McGrory L, Owen LS, Thio M, et al. A randomized trial of conditioned or unconditioned gases for stabilizing preterm infants at birth. J Pediatr. 2018;193:47-53. doi: 10.1016/j.jpeds.2017.09.006 [DOI] [PubMed] [Google Scholar]
- 44.Meyer MP, Bold GT. Admission temperatures following radiant warmer or incubator transport for preterm infants <28 weeks: a randomised study. Arch Dis Child Fetal Neonatal Ed. 2007;92(4):F295-F297. doi: 10.1136/adc.2006.107128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Meyer MP, Hou D, Ishrar NN, Dito I, te Pas AB. Initial respiratory support with cold, dry gas versus heated humidified gas and admission temperature of preterm infants. J Pediatr. 2015;166(2):245-250.e1. doi: 10.1016/j.jpeds.2014.09.049 [DOI] [PubMed] [Google Scholar]
- 46.Nimbalkar SM, Khanna AK, Patel DV, Nimbalkar AS, Phatak AG. Efficacy of polyethylene skin wrapping in preventing hypothermia in preterm neonates (<34 weeks): a parallel group non-blinded randomized control trial. J Trop Pediatr. 2019;65(2):122-129. doi: 10.1093/tropej/fmy025 [DOI] [PubMed] [Google Scholar]
- 47.Reilly MC, Vohra S, Rac VE, et al. ; Vermont Oxford Network Heat Loss Prevention (HeLP) Trial Study Group . Randomized trial of occlusive wrap for heat loss prevention in preterm infants. J Pediatr. 2015;166(2):262-268.e2. doi: 10.1016/j.jpeds.2014.09.068 [DOI] [PubMed] [Google Scholar]
- 48.Reilly MC, Vohra S, Rac VE, et al. Parallel exploratory RCT of polyethylene wrap for heat loss prevention in infants born at less than 24 weeks’ gestation. Neonatology. 2019;116(1):37-41. doi: 10.1159/000497253 [DOI] [PubMed] [Google Scholar]
- 49.Rohana J, Khairina W, Boo NY, Shareena I. Reducing hypothermia in preterm infants with polyethylene wrap. Pediatr Int. 2011;53(4):468-474. doi: 10.1111/j.1442-200X.2010.03295.x [DOI] [PubMed] [Google Scholar]
- 50.Tecson-delos Santos CM. Uy ME, Uy H, Sto Nino OV. Polyethylene plastic wrap and cap for thermoregulation of preterm infants 28 to 36 weeks old admitted to the neonatal intensive care unit: a randomised controlled trial. J Paediatr Child Health. 2012;48(suppl 1):154. doi: 10.1111/j.1440-1754.2012.02412.x [DOI] [Google Scholar]
- 51.Shabeer MP, Abiramalatha T, Devakirubai D, Rebekah G, Thomas N. Standard care with plastic bag or portable thermal nest to prevent hypothermia at birth: a three-armed randomized controlled trial. J Perinatol. 2018;38(10):1324-1330. doi: 10.1038/s41372-018-0169-9 [DOI] [PubMed] [Google Scholar]
- 52.Simon P, Dannaway D, Bright B, et al. Thermal defense of extremely low gestational age newborns during resuscitation: exothermic mattresses vs polyethylene wrap. J Perinatol. 2011;31(1):33-37. doi: 10.1038/jp.2010.56 [DOI] [PubMed] [Google Scholar]
- 53.Smith J, Usher K, Alcock G, Buettner P. Application of plastic wrap to improve temperatures in infants born less than 30 weeks gestation: a randomized controlled trial. Neonatal Netw. 2013;32(4):235-245. doi: 10.1891/0730-0832.32.4.235 [DOI] [PubMed] [Google Scholar]
- 54.Talakoub S, Shahbazifard Z, Armanian AM, Ghazavi Z. Effect of two polyethylene covers in prevention of hypothermia among premature neonates. Iran J Nurs Midwifery Res. 2015;20(3):322-326. [PMC free article] [PubMed] [Google Scholar]
- 55.Trevisanuto D, Doglioni N, Cavallin F, Parotto M, Micaglio M, Zanardo V. Heat loss prevention in very preterm infants in delivery rooms: a prospective, randomized, controlled trial of polyethylene caps. J Pediatr. 2010;156(6):914-917.e1. doi: 10.1016/j.jpeds.2009.12.021 [DOI] [PubMed] [Google Scholar]
- 56.Vohra S, Frent G, Campbell V, Abbott M, Whyte R. Effect of polyethylene occlusive skin wrapping on heat loss in very low birth weight infants at delivery: a randomized trial. J Pediatr. 1999;134(5):547-551. doi: 10.1016/S0022-3476(99)70238-6 [DOI] [PubMed] [Google Scholar]
- 57.Vohra S, Roberts RS, Zhang B, Janes M, Schmidt B. Heat loss prevention (HeLP) in the delivery room: a randomized controlled trial of polyethylene occlusive skin wrapping in very preterm infants. J Pediatr. 2004;145(6):750-753. doi: 10.1016/j.jpeds.2004.07.036 [DOI] [PubMed] [Google Scholar]
- 58.Agrawal N, Das K, Patwal P, Pandita N, Gupta A. Wrapping newborn infants in cloth and newspaper after delivery led to higher temperatures on arrival at the neonatal intensive care unit. Acta Paediatr. 2018;107(8):1335-1338. doi: 10.1111/apa.14211 [DOI] [PubMed] [Google Scholar]
- 59.Castro MM, Repeto M, Cancela MJ, Latof M, Hernandez C, Bustos R. Clinical experience in the use of polyethylene bags to reduce hypothermia in newborns less than 1000g . Archivos de Pediatria del Uruguay 2007;78(2):110–114. [Google Scholar]
- 60.Duman N, Utkutan S, Kumral A, Köroğlu TF, Ozkan H. Polyethylene skin wrapping accelerates recovery from hypothermia in very low-birthweight infants. Pediatr Int. 2006;48(1):29-32. doi: 10.1111/j.1442-200X.2006.02155.x [DOI] [PubMed] [Google Scholar]
- 61.Jia YS, Lin ZL, Lv H, Li YM, Green R, Lin J. Effect of delivery room temperature on the admission temperature of premature infants: a randomized controlled trial. J Perinatol. 2013;33(4):264-267. doi: 10.1038/jp.2012.100 [DOI] [PubMed] [Google Scholar]
- 62.Linnér A, Klemming S, Sundberg B, et al. Immediate skin-to-skin contact is feasible for very preterm infants but thermal control remains a challenge. Acta Paediatr. 2020;109(4):697-704. doi: 10.1111/apa.15062 [DOI] [PubMed] [Google Scholar]
- 63.Meyer MP, Payton MJ, Salmon A, Hutchinson C, de Klerk A. A clinical comparison of radiant warmer and incubator care for preterm infants from birth to 1800 grams. Pediatrics. 2001;108(2):395-401. doi: 10.1542/peds.108.2.395 [DOI] [PubMed] [Google Scholar]
- 64.Roberts JR. Use of a Stockinette Cap on Premature Infants After Delivery. Dissertation. Texas Women’s University; 1981. [Google Scholar]
- 65.Brignardello-Petersen R, Murad MH, Walter SD, et al. ; GRADE Working Group . GRADE approach to rate the certainty from a network meta-analysis: avoiding spurious judgments of imprecision in sparse networks. J Clin Epidemiol. 2019;105:60-67. doi: 10.1016/j.jclinepi.2018.08.022 [DOI] [PubMed] [Google Scholar]
- 66.Rabe H, Gyte GM, Díaz-Rossello JL, Duley L. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev. 2019;9(9):CD003248. doi: 10.1002/14651858.CD003248.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Hissink Muller PC, van Berkel LH, de Beaufort AJ. Axillary and rectal temperature measurements poorly agree in newborn infants. Neonatology. 2008;94(1):31-34. doi: 10.1159/000112840 [DOI] [PubMed] [Google Scholar]
- 68.Charafeddine L, Tamim H, Hassouna H, Akel R, Nabulsi M. Axillary and rectal thermometry in the newborn: do they agree? BMC Res Notes. 2014;7:584. doi: 10.1186/1756-0500-7-584 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. PRISMA flow
eFigure 2. Mean gestational age of the enrolled neonates
eFigure 3. Mean birth weight of the enrolled neonates
eFigure 4. Risk of bias summary and graph of the included trials
eFigure 5. Direct evidence from the pair wise comparisons for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 6. Split between direct and indirect evidence for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 7. Sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 8. League plot depicting the network estimate [MD (95% CrI)] for sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 9. Split between direct and indirect evidence for sensitivity analysis by evaluating plastic bag and plastic wrap as separate interventions for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 10. Sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 11. League plot depicting the network estimate for sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 12. Split between direct and indirect evidence for sensitivity analysis by evaluating studies in which the mean gestational age of the included neonates was</ = 30 weeks for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 13. Meta-regression with gestational age as covariate
eFigure 14. Sensitivity analysis by evaluating drying versus no drying before wrapping in a plastic bag/wrap for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 15. League plot depicting the network estimate for sensitivity analysis - drying vs no drying before wrapping in a plastic bag/wrap for the primary outcome: mean core body temperature (axillary or rectal) at admission or within first 2 hours of life
eFigure 16. League plot depicting the network estimate [RR (95% CrI)] for primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 17. Direct evidence from the pair wise comparisons for the primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 18. Split between direct and indirect evidence for the primary outcome moderate or severe hypothermia [defined as core body temperature (axillary or rectal) less than 36 degree Celsius] at admission or within 2 hours of life
eFigure 19. Sensitivity analysis by evaluating any hypothermia (defined as core body temperature less than 36.5 °C at admission or within 1-2 hours of life). A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 20. League plot depicting the network estimate [RR (95% CrI)] for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 21. Split between direct and indirect evidence for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 22. Direct evidence from the pair wise comparisons for sensitivity analysis - any hypothermia (defined as core body temperature less than 36.5 degree Celsius at admission or within 1-2 hours of life)
eFigure 23. Mortality before discharge. A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 24. League plot depicting the network estimate [RR (95% CrI)] for mortality before discharge
eFigure 25. Split between direct and indirect evidence for mortality before discharge
eFigure 26. Direct evidence from the pair wise comparisons for mortality before discharge
eFigure 27. Hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 28. League plot depicting the network estimate [RR (95% CrI)] for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life
eFigure 29. Split between direct and indirect evidence for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 °C] at admission or within 2 hours of life
eFigure 30. Direct evidence from the pair wise comparisons for hyperthermia [defined as core body temperature (axillary or rectal) more than 37.5 degree Celsius] at admission or within 2 hours of life
eFigure 31. Major brain injury (MBI) defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia A. Network plot; B. SUCRA plot; C. Forest plot depicting the network estimates [MD (95% CrI)] of the various interventions with “Routine Care” as the common comparator
eFigure 32. League plot depicting the network estimate [RR (95% CrI)] for MBI [defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia]
eFigure 33. Direct evidence from the pair wise comparisons for MBI [defined as grade III-IV intraventricular hemorrhage or periventricular leukomalacia]
eFigure 34. Funnel plots and trim plots for pairwise comparisons - 'PBWr' versus 'routine
care' for outcomes - mean core body temperature, mortality before discharge, hyperthermia
eTable 1. Literature search strategy for two electronic databases
eTable 2. Some of the studies that were excluded for valid reasons
eTable 3. Network characteristics for all the outcomes and sensitivity analysis
eTable 4. Certainty of evidence for different comparisons for the sensitivity analyses and secondary outcomes
eTable 5. Summary of results of the network meta-analysis
eReferences