

Abstract
Introduction
Fibrolipomatous hamartoma (FLH) is a benign tumorous condition of adipose tissue. It is a slow growing, rare tumour involving peripheral nerves with uncertain aetiology. The clinical presentation varies as per presenting severity. The gold standard to diagnose this rare entity is MRI and its management is still controversial. In this report, we have described one such rare presentation of FLH involving Median Nerve in an adolescent male who successfully witnessed resolution of symptoms following our surgical intervention for the same.
Case presentation
A 17-year-old male presented to our hospital with a history of swelling in his left hand since past 1 year. The detailed clinical evaluation revealed an irregular fusiform swelling extending from the ulnar aspect of wrist proximally to the thenar eminence along with involvement of the base of 2nd, 3rd and 4th fingers of left hand with consistency varying from soft to firm, tinel’s sign positive and a terminal restriction of palmar and dorsiflexion movements. Notably, motor weakness and sensory loss were not elicited. The definitive diagnosis was established by MRI of the left hand. With due consent, the patient was undertaken for surgical intervention whereby his carpal tunnel was decompressed and biopsy of the lesion was sent for further histopathological evaluation as per the protocol. The absolute resolution in symptoms was reported by the patient following our intervention.
Conclusion
A meticulous clinical and radiological correlation is required to diagnose such rare clinical entity for improvising the functional quality of life. There is no definitive treatment for lipomatosis of nerve. However, a conservative approach is commonly advocated with successful results from decompression as in our patient.
Keywords: Fibrolipomatous hamartoma, Median nerve, Carpal tunnel syndrome, Tinel sign
Introduction
The benign adipose tissue tumour of peripheral nerves is extremely rare. Among all the peripheral nerves, median nerve benign adipose tissue tumour constitutes 60–80% of cases [1]. Fibrolipomatous hamartoma (FLH) of median nerve is a slow growing benign tumour with an uncertain aetiology [2]. FLH of median nerve overlaps with the clinical presentation of carpal tunnel syndrome [3]. It is associated with macrodactyly and muscular lipo-macrodystrophy along the course of the nerve [4]. The treatment of FLH is based on the individualised clinical presentation and the functional needs of these patient. This manuscript outlines a case report of FLH of median nerve and its management in order to understand the natural course of disease with its due management.
Case Report
A 17 year old male presented at our hospital with a history of swelling in his left hand since past 1 year. Initially, it was a peanut sized swelling which progressed with gradual course of time to fill the entire palm extending from the distal forearm of wrist to the thenar eminence including the base of 2nd, 3rd and 4th fingers of left hand. He experienced on and off episodes of tingling sensation and paraesthesias over his 2nd, 3rd and 4th fingers. Notably, there was no history of trauma to his hand. Physical examination revealed an irregular fusiform swelling extending from the ulnar aspect of wrist proximally to the thenar eminence along with involvement of the base of 2nd, 3rd and 4th fingers of left hand (as shown in Fig. 1). On palpation, the swelling had a variable consistency ranging from soft over the ulnar aspect and firm over the 3rd and 4th metacarpal respectively. Slip sign was positive over ulnar aspect of the swelling. There was no elicitation of motor weakness or loss of sensations. Tinel’s sign was positive whereby patient witnessed the tingling sensation in his hand along with pain and burning sensation in his arm. The movements of left wrist revealed a terminal restriction of palmar and dorsiflexion movements. No other cutaneous or soft tissue lesions were additionally noted.
Fig. 1.
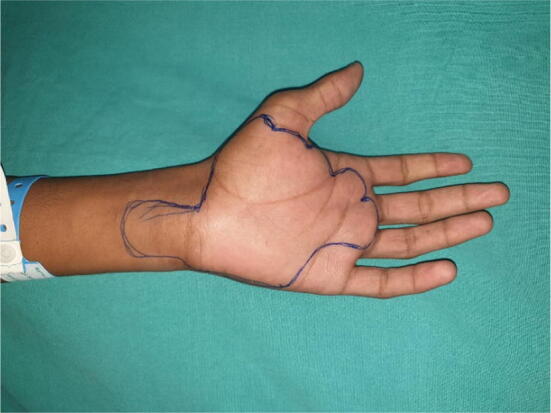
Clinical image of left hand (marked area) showing the extent of the lesion
Magnetic resonance imaging of the left hand revealed a gross thickening of median nerve with lipomatous tissue interdigitating between the prominent fascicles with a coaxial cable like appearance from distal forearm to distal end of the metacarpal region. The internal multiple serpiginous low T1 and T2 signal intensity structures represent thickened nerve fascicles surrounded by distributed fat of high signal intensity on T1/T2 W images with suppression on FLAIR sequence. The thickened nerve causing compression and displacement of flexor tendons and convexity of carpal tunnel retinacular sheath without any significant osseous lesions of forearm, carpals and hand (as shown in Fig. 2a–c).
Fig. 2.

MRI of the left hand. a Coronal section and b sagittal section showing lipomatous tissue (shown in red arrow) around median nerve and c axial section showing T1/T2 W images with suppression on FLAIR sequence showing thickened nerve fascicles surrounded by distributed fat (shown in red arrow)
Under general anaesthesia, the patient underwent surgical decompression of carpal tunnel. After extensive dissection over palm, the grossly thickened median nerve was identified as two giant fascicles adherent with fibrolipomatous structures around (as shown in Fig. 3a, b). The biopsy of fibrolipomatous structures were taken from the lesion. An utmost care was taken by not injuring the giant median nerve bundles. Patient reported absolute relief in pain after the surgical decompression of carpal tunnel without any neurological deficit.
Fig. 3.

a, b Intraoperative images showing the dissected giant median nerve at carpal tunnel and double fascicles of median nerve respectively
Histopathological examination of the lesion revealed a uniform pattern consisting of lobules of mature adipocytes separated by the fibrocollagenous septae. In addition, there has been expansion of epi- and perineurium due to adipose tissue (fat) deposition coupled with perineurial fibrosis. Notably, this aforementioned further warrant IHC markers assessment such as Claudin and EMA for perineurium and S100P for Schwann cells and nerve fibres respectively (as shown in Fig. 4a–c).
Fig. 4.

a–c HPE (×40) of the lesion showing lobules of mature adipocytes interspersed by fibrocollagenous stromal elements with epi- and perineural tissue in between
Discussion
Fibrolipomatous hamartoma (FLH) of a nerve has been reported as lipofibroma, lipomatosis, fibrofatty overgrowth, fatty infiltration of the nerve and neurolipoma [5]. In 1964, Morley described the clinical entity of an intraneural lipoma [6]. In 1978, classification of benign adipose tumours of peripheral nerve was given by Terzis et al. into (a) well‑encapsulated intraneural lipomas, (b) diffusely infiltrating fibrofatty tumours (lipofibromatous hamartomas) and (c) macrodystrophia lipomatosa [7]. In 1994, Guthikonda et al. proposed a new system of classification for neural lipomatous tumours into (a) soft lipoma, (b) intraneural lipoma, (c) lipofibromatous hamartoma and (d) macrodystrophia lipomatosa [8].
In 2013, World Health Organization (WHO) designated fibrolipomatous hamartoma (FLH) as lipomatosis of the nerve [9]. The prevalence of fibrolipomatous hamartoma (FLH) or lipomatosis involving the peripheral nerves were reported in the median [10], radial [11], ulnar [12], brachial plexus [13], suprascapular [14], posterior tibial [15], fibular [16] and sciatic nerves [17].
Being rare tumour, fibrolipomatous hamartoma presents with a benign tumorous growth of combination of fibrous and lipomatous tissue within the nerve sheath. FLH lesion has predilection in males without macrodactyly and towards female sex with macrodactyly [18]. Due to their slow‑growing nature, fibrolipomatous lesions of nerve usually present as asymptomatic or minimally symptomatic swelling with or without mild to severe symptoms based on nerve affection [19]. In our case, FLH/lipomatosis affected an adolescent male who presented with the features of carpal tunnel compression whereas the detail evaluation confirmed the involvement of unilateral median nerve without macrodactyly. The review of fibrolipomatous hamartoma of median nerve from 2012 to 2019 were tabulated in Table 1.
Table 1.
Review of fibrolipomatous hamartoma of median nerve from 2012 to 2019
| Author and year of the study | No of FLH cases | Clinical presentation | Imagining modality | Management |
|---|---|---|---|---|
| Jennifer FH et al. (2012) [20] | 1 |
Diffuse swelling around right elbow with tingling of right thumb since 4 years; No macrodactyly |
USG and MRI of elbow | Microsurgical dissection of neural elements |
| Okubo et al. (2012) [21] | 3 |
Diffuse swelling of wrist and hand without any macrodactyly; No motor involvement |
MRI of wrist and hand | Carpal tunnel release and biopsy |
| Woosun Choi et al. (2012) [22] | 2 | Soft lump over palm without neurological involvement and macrodactyly | MRI of wrist and hand | Debulking surgery |
| Bansal A et al. (2015) [3] | 1 | Paraesthesia of right hand with macrodactyly | MRI of hand | Fasciotomy and biopsy |
| Ranjan Agarwal et al. (2016) [23] | 1 |
Swelling and pain of right index finger with symptoms of carpal tunnel syndrome; No macrodactyly and no motor involvement |
FNAC of the swelling | Decompression surgery with biopsy |
| Kini JR et al. (2018) [4] | 5 | Swelling and pain over forearm, wrist and hand with macrodactyly in three cases and without macrodactyly in two cases | MRI of wrists and hands | Surgical carpal tunnel decompression with debulking and biopsy |
| Muhammad A et al. (2018) [24] | 1 | Swelling over the wrist and reduced mobility of the middle finger with macrodactyly | MRI of wrist | Wide margin excision of the right middle finger with nerve grafting |
| MAM Saeed et al. (2019) [25] | 1 | Painless swelling over left palm with macrodactyly of ipsilateral middle finger | MRI of wrist and hand | Surgical decompression of carpal tunnel |
| Current study | 1 | Swelling of left palm with paraesthesia and without macrodactyly | MRI of wrist and hand | Carpal tunnel release and biopsy |
The etiopathogenesis of the lipomatosis of nerve lesion remains controversial. Guthikonda et al. proposed that the chronic microtrauma to the median nerve from the carpal ligament or pressure from an abnormally developing flexor retinaculum can initiate a reactive process which culminates in the development of fibrolipomatous hamartoma [8]. Various studies suggested that an unidentified trophic factor which may cause FLH may also be responsible for the associated conditions like macrodactyly [19–26].
MRI remains the gold standard for diagnosing this lipomatosis of nerve [1, 4, 6, 29, 30]. In our case, MRI of left hand suggested gross thickening of median nerve with lipomatous tissue interdigitating between the prominent fascicles with a coaxial cable like or spaghetti‑like appearance from the distal forearm to the distal end of the metacarpal region. MRI guides in deciding for planning up a surgical intervention and biopsy. Capelastegui et al. concluded that MRI has a positive predictive value of 94% in diagnosing lipomatous lesion of median nerve [27]. Histologically, the lesion revealed a uniform pattern consisting of lobules of mature adipocytes separated by the fibrocollagenous septae with perineural elements in between which were suggestive of fibrolipomatous hamartoma.
The management of FLH lesion/lipomatosis of nerve remains challenging and controversial. Various literature suggests surgical intervention ranging from carpal tunnel decompression to radical excision of the mass lesion. Talal et al. stated that the carpal tunnel decompression provided complete resolution of symptoms and relief [28]. Paletta et al. reported poor results with radical mass excision with fascicular cable graft repair [29]. Various studies stated that the minimal surgical technique of decompression and debulking of the fibrofatty sheath yields more positive results [2, 18, 20, 30]. Our patient had complete resolution of symptoms following biopsy of the lesion and decompression of carpal tunnel respectively.
Being a rare benign tumour of nerve sheath, MRI is the gold standard in diagnosing fibrolipomatous hamartoma of median nerve. A meticulous clinical and radiological correlation is required to diagnose such rare clinical entity to improvise the functional quality of life. There is no definitive treatment for lipomatosis of nerve. However, a conservative approach is commonly advocated with successful results from decompression as in our patient.
Acknowledgements
We thank Dr. Dushyant Chaudhary, Dr. Arunabh Arora, Dr. Sushmita H and Dr. Rashmi Jain who helped in data collection and proof reading the manuscript.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standard statement
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed consent
For this type of study informed consent is not required.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Marom EM, Helms CA. Fibrolipomatous hamartoma: Pathognomonic on MR imaging. Skeletal Radiology. 1999;28:260–264. doi: 10.1007/s002560050512. [DOI] [PubMed] [Google Scholar]
- 2.Razzaghi A, Anastakis DJ. Lipofibromatous hamartoma: Review of early diagnosis and treatment. Canadian Journal of Surgery. 2005;48(5):394–399. [PMC free article] [PubMed] [Google Scholar]
- 3.Bansal A, Verma A, Mourya C. Fibrolipomatous hamartoma of median nerve: A rare cause of carpal tunnel syndrome and macrodactyly. Journal of Orthopaedics and Allied Sciences. 2015;3:63–64. doi: 10.4103/2319-2585.158517. [DOI] [Google Scholar]
- 4.Kini JR, Kini H, Rau A, Kamath J, Kini A. Lipofibromatous hamartoma of the median nerve in association with or without macrodactyly. Turkish Journal of Pathology. 2018;34(1):87–91. doi: 10.5146/tjpath.2014.01282. [DOI] [PubMed] [Google Scholar]
- 5.Teles AR, Finger G, Schuster MN, Gobbato PL. Peripheral nerve lipoma: Case report of an intraneural lipoma of the median nerve and literature review. Asian Journal of Neurosurgery. 2016;11:458. doi: 10.4103/1793-5482.181118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Morley GH. Intraneural lipoma of the median nerve in the carpal tunnel. Report of a case. The Journal of Bone and Joint Surgery. British Volume. 1964;46:734–735. doi: 10.1302/0301-620X.46B4.734. [DOI] [PubMed] [Google Scholar]
- 7.Terzis JK, Daniel RK, Williams HB, Spencer PS. Benign fatty tumors of the peripheral nerves. Annals of Plastic Surgery. 1978;1:193–216. doi: 10.1097/00000637-197803000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Guthikonda M, Rengachary SS, Balko MG, van Loveren H. Lipofibromatous hamartoma of the median nerve: Case report with magnetic resonance imaging correlation. Neurosurgery. 1994;35:127–132. doi: 10.1227/00006123-199407000-00019. [DOI] [PubMed] [Google Scholar]
- 9.Fletcher CD. The evolving classification of soft tissue tumours—An update based on the new 2013 WHO classification. Histopathology. 2014;64:2–11. doi: 10.1111/his.12267. [DOI] [PubMed] [Google Scholar]
- 10.Bagatur, A.E., Yalcinkaya, M. (2009). Unilateral carpal tunnel syndrome caused by an occult palmar lipoma. Orthopedics, 32(10). [DOI] [PubMed]
- 11.Ganapathy K, Winston T, Seshadri V. Posterior interosseous nerve palsy due to intermuscular lipoma. Surgical Neurology. 2006;65:495–496. doi: 10.1016/j.surneu.2005.06.035. [DOI] [PubMed] [Google Scholar]
- 12.Balakrishnan A, Chang YJ, Elliott DA, Balakrishnan C. Intraneural lipoma of the ulnar nerve at the elbow: A case report and literature review. Canadian Journal of Plastic Surgery. 2012;20:e42–e43. doi: 10.1177/229255031202000305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sergeant G, Gheysens O, Seynaeve P, Van Cauwelaert J, Ceuppens H. Neurovascular compression by a subpectoral lipoma. A case report of a rare cause of thoracic outlet syndrome. Acta Chirurgica Belgica. 2003;103:528–531. doi: 10.1080/00015458.2003.11679484. [DOI] [PubMed] [Google Scholar]
- 14.Hazrati Y, Miller S, Moore S, Hausman M, Flatow E. Suprascapular nerve entrapment secondary to a lipoma. Clinical Orthopaedics and Related Research. 2003;411:124–128. doi: 10.1097/01.blo.0000063791.32430.59. [DOI] [PubMed] [Google Scholar]
- 15.Chen WS. Lipoma responsible for tarsal tunnel syndrome. Apropos of 2 cases. Revue de chirurgie orthopedique et reparatrice de l'appareil moteur. 1992;78:251–254. [PubMed] [Google Scholar]
- 16.Vasudevan JM, Freedman MK, Beredjiklian PK, Deluca PF, Nazarian LN. Common peroneal entrapment neuropathy secondary to a popliteal lipoma: Ultrasound superior to magnetic resonance imaging for diagnosis. PMR. 2011;3:274–279. doi: 10.1016/j.pmrj.2010.09.014. [DOI] [PubMed] [Google Scholar]
- 17.Resende LA, Silva MD, Kimaid PA, Schiavão V, Zanini MA, Faleiros AT. Compression of the peripheral branches of the sciatic nerve by lipoma. Electromyography and Clinical Neurophysiology. 1997;37:251–255. [PubMed] [Google Scholar]
- 18.Clavijo-Alvarez JA, Price M, Stofman GM. Preserved neurologic function following intraneural fascicular dissection and nerve graft for digital and median nerve lipofibromatous hamartoma. Plastic and Reconstructive Surgery. 2010;125(3):120e–e122. doi: 10.1097/PRS.0b013e3181cb66b7. [DOI] [PubMed] [Google Scholar]
- 19.Gennaro S, Merciadri P, Secci F. Intraneural lipoma of the median nerve mimicking carpal tunnel syndrome. Acta Neurochirurgica (Wien) 2012;154:1299–1301. doi: 10.1007/s00701-012-1303-7. [DOI] [PubMed] [Google Scholar]
- 20.Jennifer FH, Teh BM, Abeysuriya DT, Luo DY. Fibrolipomatous hamartoma of the median nerve in the elbow: A case report. Ochsner Journal. 2012;12(2):152–154. [PMC free article] [PubMed] [Google Scholar]
- 21.Okubo T, Saito T, Mitomi H, et al. Intraneural lipomatous tumor of the median nerve: Three case reports with a review of literature. International Journal of Surgery Case Reports. 2012;3(9):407–411. doi: 10.1016/j.ijscr.2012.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi W, Jung JY, Song IN, Lee JS, Lee TJ, Jung YY. Fibrolipomatous hamartoma of digital branch of the median nerve without macrodystrophy: Two case reports with magnetic resonance imaging findings. Journal of the Korean Society of Radiology. 2012;67(6):483–487. doi: 10.3348/jksr.2012.67.6.483. [DOI] [Google Scholar]
- 23.Agrawal R, Garg C, Agarwal A, Kumar P. Lipofibromatous hamartoma of the digital branches of the median nerve presenting as carpal tunnel syndrome: A rare case report with review of the literature. Indian Journal of Pathology and Microbiology. 2016;59:96–98. doi: 10.4103/0377-4929.191752. [DOI] [PubMed] [Google Scholar]
- 24.Muhammad A, Waheed AA, Khan N, Sayani R, Ahmed A. Fibrolipomatous hamartoma of the median nerve with macrodystrophia lipomatosa. Cureus. 2018;10(3):e2293. doi: 10.7759/cureus.2293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Saeed MAM, Dawood AA, Mahmood HM. Lipofibromatous hamartoma of the median nerve with macrodactyly of middle finger. Journal of Clinical Orthopaedics and Trauma. 2019;10:1077–1081. doi: 10.1016/j.jcot.2019.05.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nardella D, Sohawon S, Carlier A. Lipofibromatous hamartoma of the median nerve. Three case reports. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2009;62(9):e314–7. doi: 10.1016/j.bjps.2007.11.061. [DOI] [PubMed] [Google Scholar]
- 27.Capelastegui A, Astigarraga E, Fernandez-Canton G, Saralegui I, Larena JA, Merino A. Masses and pseudomasses of the hand and wrist: MR findings in 134 cases. Skeletal Radiology. 1999;28:498–507. doi: 10.1007/s002560050553. [DOI] [PubMed] [Google Scholar]
- 28.Al-Jabri T, Garg S, Mani GV. Lipofibromatous hamartoma of the median nerve. Journal of Orthopaedic Surgery and Research. 2010;5:71. doi: 10.1186/1749-799X-5-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Paletta FX, Senay LC., Jr Lipofibromatous hamartoma of median nerve and ulnar nerve: Surgical treatment. Plastic and Reconstructive Surgery. 1981;68:915–921. doi: 10.1097/00006534-198112000-00012. [DOI] [PubMed] [Google Scholar]
- 30.Naveen R. Fibrolipomatous hamartoma of median nerve: An MRI diagnosis. Orthopedics and Rheumatology Open Access Journal. 2016;3(3):555614. [Google Scholar]