

Abstract
BACKGROUND:
Coronavirus (COVID-19) a worldwide pandemic has significantly affected life of people around the globe. It has also caused various psychological issues among public such as uncertainty, fear, anxiety, and of course stress. Globalization has facilitated it and has added greater complexity to the containment of infection leading to urgent call for public health challenge. Consequently, a multilevel stress coping adjustment process is going on. Hence, it is imperative to explore how people are affected psychologically and how they are coping with it. People are adopting different strategies for coping up from this challenging situation. In this sense, the present study intended to: explore which coping strategies were of relevance for people for adjusting in COVID-19 crises and were sociodemographic factors influencing the coping strategies.
MATERIALS AND METHODS:
The research is descriptive study. For the present study, a sample of 475 participants was asked for coping strategies used by them using valid and reliable scales.
RESULTS:
Results revealed that positive attitude and trust in God were the most used adaptive coping strategies and sociodemographic variables were playing a significant role in adaptive coping strategies.
CONCLUSION:
Hence, understanding and identification of coping strategies and their relationship with demographic variables can help health professionals to direct interventions to control stressors related to the pandemics.
Keywords: Coping skills, COVID-19, pandemic, stress
Introduction
Outbreak of infectious disease is not a new phenomenon; they have emerged at various times in history. In recent years, globalization has acted as catalyst and has facilitated the spread of pathological agents, which ultimately results in worldwide pandemics. This is not only a threat on political, economical, and psychological aspects but has also added greater complexity to the containment of infection leading to urgent call for public health challenges.[1,2,3,4,5] Plagues, HIV, Ebola, Zika, H1N1, and now the novel Coronavirus (COVID-19) are recent examples of such worldwide pandemics.[6]
The year 2019 had a terrible ending for the whole world as in December (2019) the COVID-19 was identified for the first time in Wuhan city of China. Nobody was initially aware that it has a high contagion potential and that its incidence will increase exponentially. The World Health Organization recognized its widespread transmission as pandemics and declared it a public health emergency of international concern. COVID-19 has created state of crises for majority of people. Spread of doubtful or fake information related to virus transmission, the quarantine period, its geographical reach, number of patients being infected, the rate of mortality, doubts regarding job security and yes of course the dubious future has led anxiety, panic insecurity, aggression, frustration, and fear in the population. The situation has been aggravated due to lack of proper control measures and a lack of effective or well-defined therapeutic mechanisms.[4,7,8]
The uncertainties caused by COVID-19 have had consequences in a number of sectors, with direct implications for the population's daily life and mental health. These consequences would be faced by humanity for a decade to come. The nature of this contagion virus has led to mass fear and hysteria and many misconceptions, with a wide spread stigma and discrimination of those infected. Altogether these perceptions have created immense stress among the population but still they are trying to cope up from this situation. They are trying to find out coping strategies for adjusting in these traumatic crises. In order to cope from a situation a person tries to manage his external and internal demands that are perceived as taxing or exceeding adaptive resources.[9]
Coping acts as stabilizing factor that may help individual maintain psychological adaptation during stressful period.[10] Coping mechanisms can be divided into two categories. The first of these is adaptive coping strategies, which traditionally benefit or positively affect the lives of those who use them.[11] Examples of this approach include religious/spiritual coping such as prayer and reading scripture;[12] exercise;[13] meditation; listening to music; and socializing with friends and family.[14]
The other form of coping, maladaptive coping, refers to methods often leading to adverse consequences including some of the mental health challenges. Prior research divided maladaptive coping into two different categories, emotional, in which individuals respond to a situation confrontationally or with an excessive emotional response, and avoidance-based, where individuals actively delay response to a situation or completely evade a stressful situation through isolation or other maladaptive behaviors.[11,15,16] Maladaptive coping behaviors can include drinking,[17] smoking,[18] drug use, overeating,[14] and other unbeneficial behaviors. Historically, these coping strategies can lead to negative effects on one's life including greater depression, greater pain and flare-up activities, greater functional impairment and lower self-efficacy.[19]
Thus, coping mechanisms can focus on the meaning, the practical aspects, the emotional aspects and the avoidance aspects linked to a crisis. People differ greatly in their ability to deal with stressful life events successfully, and a few coping strategies are way more effective than others when faced with a selected life changing event.[20] The way which one copes with the crises situation has important implications for wellbeing. Effective coping leads an individual to attain better life satisfaction.
There is also a propensity to be more efficient and productive in handling problems that may arise due to certain crises as well as demonstrating more creativity and open-mindedness. If effective coping strategy is applied in crises period probability of having elevated life satisfaction is quite high.
Hence, understanding and Identification of coping strategies can help health professionals to direct interventions to control stressors related to the disease, favoring the adaptive process to the therapeutic regimen. Since, coping strategies are influenced by various factors such as intensity of stress, nature of the stressful life event, personal characteristics such as age, gender, health status, religion, education, religion, marital status sociodemographic, socio-cultural, geographical, and environmental aspects. In this sense, the present study intended to explore which adaptive coping strategies were of relevance for people for adjusting in COVID-19 crises and to analyze them according to sociodemographic variables. Since, no study so far has explored how people are coping with this pandemic and whether they are using adaptive or maladaptive coping strategies. Hence, the present research is an attempt to fill this gap which would mileage the policy makers, researchers, and mental health practitioners to better plan in this pivot and make people aware about the link between adaptive coping strategies and better management of stress during the course of any crises.
Materials and Methods
The research is descriptive study and conducted during the month of April 2020. A sample of 475 participants was asked for coping strategies used by them using valid and reliable scales. The data were analyzed by SPSS Descriptive and inferential statistics.
Sample
The study was conducted during the month of April 2020. A Google form was created and circulated on different online platforms through snowball sampling technique. Online written consent was taken from all the participants before they answered the questions. Participation in the study was voluntary and anonymous. Participants have been briefed about the purpose of the study and were assured of confidentiality.
The sample comprised a total of 475 respondents out of which 236 were male and 239 were female. The age ranged from 15 to 80 years and the mean age was 27.518 (standard deviation = 7.77). To obtain a more naturalistic sample, we had neither inclusion nor exclusion criteria. The data were analyzed with the help of IBM SPSS Statistics, Version 21.0. Armonk, NY: IBM Corp. The demographic data of 475 (out of 490 participants) were summarized in Table 1 of results section. Further, t-test, and ANOVA were done to draw the inferences.
Table 1.
Demographic characteristics of sample
| Variable | Frequencies (%) |
|---|---|
| Gender | |
| Male | 236 (49.6) |
| Female | 239 (50.4) |
| Age (years) | |
| Below 18 | 15 (3.5) |
| 18-25 | 210 (44.2) |
| 26-35 | 195 (41.0) |
| 35-45 | 39 (8.1) |
| 45-60 | 14 (2.8) |
| Above 60 | 2 (0.4) |
| Religion | |
| Hindu | 86 (18.2) |
| Muslim | 362 (76.2) |
| Others | 27 (5.6) |
| Marital status | |
| Married | 154 (32.5) |
| Single | 321 (67.5) |
| Region | |
| Urban | 423 (89) |
| Rural | 52 (11) |
| Educational level | |
| Below graduation | 14 (3) |
| Graduation | 150 (31.6) |
| Postgraduation | 125 (26.4) |
| Higher education (Ph.D) | 84 (17.7) |
| Professionals (B.Tech, M.Tech, MBA, Law, Doctor, Counselor, Clinical Psychologists, M.Ed, B.Ed etc.)* | 101 (21.3) |
| Employment status | |
| Employed | 231 (49) |
| Unemployed | 244 (51) |
| Profession | |
| Academician | 63 (13.2) |
| Business | 23 (5) |
| Lawyer | 08 (2) |
| Clinical psychologists, counselor, health professional | 29 (6.2) |
| Student | 253 (53.2) |
| Homemaker | 18 (3.7) |
| Engineer | 18 (3.7) |
| Other corporate jobs | 48 (10) |
| Doctor | 15 (3) |
| Whether living with family or not | |
| Living with family | 384 (81) |
| Not living with family | 91 (19) |
| Country | |
| India | 409 (86) |
| Abroad | 66 (14) |
*Professional courses included a variety of training based courses which provide a well-defined career such as engineering, medical, law, management
Tools
The following measures have been used to collect the data for the present research.
Sociodemographic data sheet
It was a semi- structured pro forma especially designed for this study. It contained information about socio-demographic variables such as age, sex, religion, education, marital status, domicile, occupation, profession, country living in and whether the subject was living with family or not.
Adaptive coping strategies (AKU internal)
Adaptive coping strategies in response to COVID-19 pandemic conditions were measured with the AKU questionnaire (AKU is an acronym of the German translation of “Adaptive Coping with Disease”), which was designed to identify adaptive coping styles. developed by Büssing et al.[21] which was designed to identify adaptive coping styles, such as to create favorable conditions, search for information, medical support, religious support, social support, initiative spirit, and positive (re) interpretation of disease.
The 28-item instrument has the following six factorial structures:
Positive attitudes (6 items; α = 0.77) refers to internal cognitive and behavioral strategies (i.e., realization of shelved dreams and wishes; resolving cumbering situations of the past; take life in own hands; doing all that what pleases; positive thinking; and avoiding thinking at illness)
Reappraisal: Illness as chance (4 items; α = 0.71) addresses a reappraisal attitude referring to cognitive processes of life reflection (i.e., reflect on what is essential in life; illness has meaning; illness as a chance for development; and appreciation of life because of experience illness)
Conscious way of living (5 items; α = 0.75) addresses cognitive and behavioral strategies in terms of internal powers and virtues (i.e., healthy diet; physical fitness; living consciously; keep away harmful influences; and change life to get well)
Search for information and alternative help (4 items; α = 0.72) refers to external sources providing additional information or alternative help (i.e., thoroughly informed about disease; get thorough information how to become healthy again; find people which can help; and search for alternative ways of healing)
Trust in medial help (4 items; α = 0.83) addresses patients’ reliance on an external medical source of health control (i.e., trust in the therapeutic potentials of modern medicine, take prescribed medicaments, follow advises of medicals, and full confidence in doctors and therapists)
Trust in God's help (5 items; α = 0.88) in response to disease addresses nonorganized intrinsic religiosity as an external transcendent resource to cope (i.e., trust in a higher power which carries through; strong belief that God will help; faith is a strong hold, even in hard times; pray to become healthy again; live in accordance with religious convictions)
Escape from illness (3 items α = 0.72). The questionnaire holds 3 independent items (i.e., fear what illness will bring; would like to run away from illness; when I wake up, I do not know how to face the day). This scale addresses a passive (avoidance-escape) coping style.
Scoring
All items were scored on a five-point scale from disagreement to agreement (0 - does not apply at all; 1 - does not truly apply; 2 – do not know; 3 - applies quite a bit; and 4 - applies very much). The sum scores were referred to a 100% level (transformed scale score). Scores more than 50 indicated high agreement or utilization of coping strategy, while scores < 50 indicated low usage of respective strategy. The Cronbach's alpha of the entire scale was 0.86 for the current sample. Cronbach's alpha for the subscales was found to be 0.77 for positive attitude, 0.71 for reappraisal, 0.75 for conscious way of living, 0.72 for search for information, 0.83 for trust in medical help, 0.88 for trust in God's help, and 0.72 for escape from illness, respectively. The questionnaire was revalidated several times and has approved the 6 factorial structure of the 28-item instrument which had a good internal consistency (Cronbach's α = 0.867; difficulty index 0.67).[21]
Results
No missing value has been found in the data set as all the questions have been marked mandatory in Google form. There were no outliers in the data. Data were found to be normal as the skewness and kurtosis values were within the normal range for all the variables.
As all the data were self-reported therefore data were checked for common method variance. Harman Single factor test was run and it was found that 17.33% of the variance loaded on the single factor which is below the 50% standard.[22] Thus, it can be safely said that data of the present study do not suffer from common method variance.
Demographic characteristics of sample
As shown in Table 1, there was almost equal distribution of gender in the sample with 50% being males and 50% females. Most of the participants in the present study were Muslims (76%) and in the age range 18–35 (44%). They belong to heterogeneous educational and professional backgrounds such as academicians, doctors, lawyers, counselors, business professional, and students. Although majority of the participants belonged to India (86%), we also attempted to collect data from outside India such as USA, UK, UAE, Saudi Arabia, Germany, and Canada. Nonetheless, they constituted only 14% of the sample. Furthermore, bulk of participants were single (66%) and were living with their family (81%).
The Figure 1 shows the proportion of patients with a score greater than the median for each coping strategy. The median score for each coping strategy was as follows: positive attitude (19.16), trust in God (18.68), trust in medical help (12.83), conscious (12.31), reappraisal (11.72), search for information (11.37), and escape (5.67).
Figure 1.
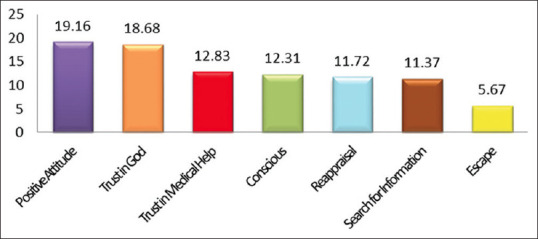
Distribution of coping strategies
With respect to various demographical variables, we found several significant differences which are depicted in Table 2. The utilization of the respective adaptive coping strategies did not significantly differ with respect to gender and country of living, while on age, religion, educational background, marital status, employment status and people living with their family, significant differences have been found.
Table 2.
Adaptive coping style used by people during COVID-19
| Positive attitude | Reappraisal | Conscious | Escape | Search for info | Trust in medical help | Trust in god help | |
|---|---|---|---|---|---|---|---|
| Age (mean±SD) | |||||||
| Below 18 | 18.5±2.6 | 11.5±2.5 | 10.2±3.7 | 6.1±3.3 | 10.6±3.1 | 12.5±2.7 | 19.4±1.3 |
| 18-25 | 18.6±3.6 | 11.4±3.0 | 12.8±4.1 | 6.4±3.1 | 11.1±3.1 | 12.4±3.2 | 17.1±3.8 |
| 26-35 | 18.9±3.8 | 11.4±3.2 | 11.4±4.5 | 5.3±3.3 | 11.1±3.2 | 12.3±3.2 | 17.0±4.5 |
| 35-45 | 18.9±3.4 | 10.9±2.7 | 12.1±3.9 | 4.3±3.4 | 10.0±3.1 | 11.5±4.7 | 16.2±4.4 |
| 45-60 | 20.4±3.1 | 11.1±2.6 | 10.3±4.8 | 4.8±3.4 | 11.3±2.7 | 14.1±2.1 | 17.7±3.2 |
| T (P) | 1.03 (0.39) | 0.324 (0.86) | 3.89 (0.004) | 5.50 (0.00) | 1.21 (0.30) | 1.71 (0.14) | 1.77 (0.13) |
| Religion (mean±SD) | |||||||
| Islam | 18.7±3.7 | 11.6±2.8 | 12.1±4.3 | 6.1±3.3 | 11.1±3.1 | 12.2±3.4 | 18.2±2.6 |
| Hindu | 19.4±3.3 | 11.4±2.8 | 12.5±3.9 | 4.7±3.1 | 10.8±3.1 | 12.9±2.6 | 14.3±4.7 |
| Others | 18.4±3.8 | 8.5±4.5 | 9.2±5.1 | 4.9±2.6 | 10.3±2.8 | 12.5±3.6 | 10.9±7.6 |
| T (P) | 1.43 (0.24) | 12.8 (0.001) | 6.1 (0.002) | 7.1 (0.001) | 1.0 (0.355) | 1.7 (0.176) | 84.8 (0.001) |
| Educational level (mean±SD) | |||||||
| Below graduation | 18.7±3.6 | 11.5±3.2 | 11.0±4.4 | 6.4±2.9 | 11.4±2.7 | 13.6±1.8 | 19.2±1.4 |
| Graduation | 18.9±3.5 | 11.5±3.1 | 12.6±4.4 | 6.6±3.3 | 10.8±3.3 | 12.1±3.7 | 17.2±4.2 |
| Postgraduate | 18.6±3.6 | 12.0±2.7 | 12.4±4.0 | 5.6±3.2 | 11.3±2.8 | 12.4±3.2 | 17.1±3.8 |
| Higher education (Ph.D scholars) | 19.1±3.9 | 10.8±3.1 | 11.2±4.5 | 4.9±3.3 | 10.8±2.7 | 12.2±3.1 | 16.1±4.9 |
| Prof Co | 18.7±3.5 | 10.9±3.1 | 11.5±4.2 | 5.2±3.1 | 10.9±3.5 | 12.6±2.8 | 17.2±3.7 |
| T (P) | 0.20 (0.94) | 2.4 (0.04) | 2.3 (0.05) | 4.9 (0.001) | 0.53 (0.71) | 0.88 (0.47) | 2.1 (0.07) |
| Marital status (mean±SD) | |||||||
| Single | 19.2±3.5 | 11.2±2.9 | 11.2±4.4 | 4.8±3.1 | 11.0±3.2 | 12.4±3.4 | 17.4±4.0 |
| Married | 18.6±3.6 | 11.4±3.1 | 12.4±4.2 | 6.2±3.2 | 11.0±3.1 | 12.3±3.2 | 16.9±4.2 |
| T (P) | 1.7 (0.08) | -0.66 (0.50) | -2.8 (0.004) | 4.2 (0.00) | 0.06 (0.94) | 0.19 (0.85) | 1.16 (0.24) |
| Living with family (mean±SD) | |||||||
| Living with family | 18.9±3.5 | 11.5±2.9 | 12.1±4.3 | 5.7±3.3 | 10.9±3.1 | 12.5±3.2 | 17.4±3.7 |
| Not living with family | 18.4±4.1 | 10.7±3.3 | 11.5±4.4 | 5.7±3.2 | 11.2±3.1 | 11.9±3.3 | 15.5±5.4 |
| T (P) | 1.0 (0.29) | 2.3 (0.020) | 1.2 (0.202) | 0.08 (0.935) | 0.66 (0.509) | 1.5 (0.13) | 4.1 (0.001) |
| Employment (mean±SD) | |||||||
| Full time | 18.9±3.8 | 11.1±3.2 | 11.5±4.5 | 5.0±3.4 | 10.8±3.3 | 12.3±3.6 | 16.6±4.7 |
| Unemployed | 18.7±3.5 | 11.6±2.8 | 12.4±4.1 | 6.4±3.1 | 11.2±2.9 | 12.4±2.9 | 17.5±3.4 |
| T (P) | 0.79 (0.42) | 1.7 (0.07) | 2.2 (0.02) | 4.4 (0.001) | 1.3 (0.17) | 0.28 (0.77) | -2.5 (0.01) |
SD=Standard deviation
The age had a significant impact on conscious way of living (F = 3.89, P = 0.004), and escape (F = 5.51, P = 0.001). Results of post hoc analysis revealed that people in the age group of 18–25 years are more likely to use conscious way of living and escape coping strategies more than people falling in the age group of 26–35 and 36–45 years.
Furthermore, religion also determines one's way to cope with threatening situation. Results show that religion has a significant impact on Reappraisal (F = 12.82, P = 0.001), conscious way of living (F = 6.10, P = 0.002), escape (F = 7.15, P = 0.001), and trust in God help (F = 84.87, P = 0.001). Comparative to other religions, Muslims and Hindus use reappraisal and conscious way of living more as coping strategies. While on escape and trust in God help Muslims differ significantly with Hindus and other religious groups with Muslims practicing more escape and trust in God help as coping strategies.
As far as, educational background is concerned, significant differences have been found on Reappraisal (F = 2.46, P = 0.045, conscious way of living (F = 2.33, P = 0.05) and escape (F = 4.99, P = 0.001). Results show that post graduates use reappraisal and conscious way of living more followed by graduates while Ph.D scholars and professional courses students use them least. Moreover, people who are 12th pass or graduates, practice escape more than people from other educational background.
Marital status also plays a role of difference in coping styles. It was reported that marital status has a significant impact on conscious way of living (t = 2.89, P= 0.004) and escape (t = 4.22, P = 0.001). Results revealed that single people practice conscious way of living and escape more as a coping mechanism.
During this pandemic, family was also emerged an important determining factor as people living with their family are differing significantly with people living alone or not with their family on Reappraisal (t = 2.33, P = 0.020) and trust in God help (t = 4.08, P = 0.001). People who are living with their family use reappraisal and trust in God help more than people not living with their family.
Moreover, employment also has a significant impact on conscious way of living (t = 2.25, P = 0.025), escape (t = 4.43, P = 0.001) and trust in God help (t = −2.57, P = 0.01). It was investigated that unemployed people use conscious way of living, escape and trust in God help more than employed people.
Discussion
During the course of any pandemic, people face lots of physical and emotional stressors yet little is known about their coping strategies or the relationship between coping style and life satisfaction. Due to highly contagious nature of COVID-19, a public health emergency is being declared to prevent the contagion and limit the outbreak. Consequently, millions of lives have been affected. Thus, a multilevel stress coping adjustment process is going on. Hence, it is imperative to explore how people are affected psychologically and how they are coping with it.
In the present study, we examined which adaptive coping strategies is most used by people during this outbreak of COVID-19. Various interesting trends have been emerged. We identified the diverse, unique, and most commonly used ways of coping. Positive attitude and trust in God help, was found to be the most frequently used coping strategies followed by trust in medicine, conscious way of living and reappraisal [Figure 1]. However, search for information and Escape were among the least used coping strategies. Results shed light that people are holding on to positive attitude for overcoming the crises. In this sense, they used positive reappraisal to create new meanings for the stress, facing it with a positive attitude, leading to personal growth. Thus, they attribute new meanings to the disease to see it from a different perspective, that is, a positive perspective.[23] They are relying on trusting God and indulging in praying and reading the Holy Scriptures. They believe that it will strengthen their faith, hope and ultimately God will transform their lives.[24] Escaping from this crisis is least preferred coping strategy may be because they are aware that running away from this situation is of no use. They know that lack of interest in dealing with disease-related stressors, may negatively contribute for improving the clinical picture, as it may seem like a way of fantasizing possible solutions for the problems, without actually taking concrete actions to modify the reality.[20]
Moreover, one of the significant findings of the current research is that use of coping strategies do get influenced or determined by people's demographic background. It was explored that people of different age groups have different ways to deal with stress. As found in the present study that people in the age group of 18–25 years are more likely to use conscious way of living and escape coping strategies more than people falling in the age group of 26–35 and 36–45 years. Our findings revealed that these young adults use cognitive and behavioral strategies in terms of internal powers and virtues i.e., healthy diet; physical fitness; living consciously; keep away harmful influences; change life to get well. Literature also shows that this cohort of young adults are more aware because of the increasing scientific and public attention they have received, provide a reference point for understanding the dos and do don'ts of this pandemic. While 45–60 cohort use positive attitude, reappraisal, and trust in God's help. It may be due to that their life experiences have taught them how to cope during the phase of uncertainty. They may have experience similar situation in past also which gave them strength to maintain positive attitude that past has also passed so this will too.
It was found that people who are employed or have job scored higher mean compared to nonworking counterparts suggesting that job provides a sort of security, support and meaning to face uncertainty.[25] Since, any epidemic does not come alone it also brings with economic and financial loss. Because one of the consequences of COVID-19 is the declaration of lockdown by the government which has seized people's opportunities to go out and earn, hence, kept the future of many at stake. On the other hand, work also gives an engagement and sense of satisfaction. Thus, those who have a secure job would naturally likely to differ from those who are unemployed.
Further, living with the family during the phase of crisis led to higher mean scores in coping strategies. Results highlighted that people who are living with their family use reappraisal and trust in God help, more than people not living with their family. Our findings were in line with previous researches on pandemics where it has been demonstrated that support factor from helps in overcoming the family situation.[26]
Besides, it was observed that religiosity also acts as a buffer against stress and can cause differences in the preference of a particular coping mechanism. In line our study highlighted that comparative to other religions, Muslims used reappraisal, conscious way of living, escape, and trust in God help while, Hindus used reappraisal and conscious way of living more as coping strategies compared to other religious groups. Previous studies have also shown religion and spirituality among people living in pandemics are being used as strategies to deal with the adversities arising from the pandemic.[27,28]
In addition, one's educational background also found to determine their coping strategies. As found in this study that simple (B.A. B.Sc) graduates are differing from people of professional (Training based courses) background (B.Tech, BBA, BSW, etc.) and higher education (Ph.D). Post graduates use reappraisal and conscious way of living more followed by graduates while Ph.D scholars and professional courses students use them least. This finding is again conforming that 18–25 years of age group of people are more conscious about their way of living. Moreover, people who are 12th pass or graduates, practice escape more than people from other educational background.
Somehow these findings indicate that coping strategies not only influence physical and mental wellbeing but also certain coping styles may be more adaptive than others. Although trust in medical help is rather a passive strategy, but during this emergency situation, they are playing a significant role to save the lives of people. Nevertheless, it can be said that we have no choice than follow the advice from the experts and rely on prescribed preventive measures to save from this contagious virus. Further, evidence for this no choice position comes from reliance on “More Powerful,” i.e., trust in God help. It is interesting to find that this epidemic left us helpless and we had no choice but to rely and put our trust in external help.
Limitation
Our work had certain limitation. First, we relied on data from a cross-sectional study. The adaptive coping strategies may change during the course of disease, and people have to adapt their strategies to changing situations. This has to be address in future longitudinal studies. Second, participants completed the self-report scales and questionnaires, which may be affected by their current state and their willingness to cooperate.
Thus, the present research is a pioneer to explore the role of demographic variables in the practice and choice of a particular coping style among Indian population. These findings may help mental health professionals to create a therapeutic module for enhancing coping strategies to cope with adversities and the pandemic situation like COVID-19.
Conclusion
Thus, the present study is found one of its types during this COVID pandemic and will add significantly in the research gap. From the present research, it can be inferred that our subjects used a variety of coping strategies during this pandemic phase. Notably, most reported high utilization was positive attitude and trust in GOD, but a concerning proportion also reported high utilization of Trust in medical help and conscious way of coping. These findings highlight an important need to better understand how people during crises cope with the situation and to determine whether interventions can enhance more adaptive coping behaviors.
Future research should focus on developing interventions to facilitate the use of certain coping strategies while also determining the impact of these interventions on patients’ life satisfaction.
Ethical Standards and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to express our thanks to all the participants who participated in the present study and the anonymous reviewers for their invaluable help during the revision process.
References
- 1.Morens DM, Fauci AS. Emerging infectious diseases: Threats to human health and global stability. PLoS Pathog. 2013;9:e1003467. doi: 10.1371/journal.ppat.1003467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Semenza JC, Lindgren E, Balkanyi L, Espinosa L, Almqvist MS, Penttinen P, et al. Determinants and drivers of infectious disease threat events in Europe. Emerg Infect Dis. 2016;22:581–9. doi: 10.3201/eid2204.151073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bloom DE, Cadarette D. Infectious disease threats in the twenty-first century: Strengthening the global response. Front Immunol. 2019;10:549. doi: 10.3389/fimmu.2019.00549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Malta M, Rimoin AW, Strathdee SA. The coronavirus 2019-nCoV epidemic: Is hindsight 20/20? EClinicalMedicine. 2020;20:100289. doi: 10.1016/j.eclinm.2020.100289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ferguson NM, Laydon D, Nedjati-Gilani G, Imai N, Ainslie K, Baguelin M, et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. Imperial College London. 2020 10, 77482. doi: https://doi.org/10.25561/77482. [Google Scholar]
- 6.Tucci V, Moukaddam N, Meadows J, Shah S, Galwankar SC, Kapur GB. The forgotten plague: Psychiatric manifestations of ebola, zika, and emerging infectious diseases. J Glob Infect Dis. 2017;9:151–6. doi: 10.4103/jgid.jgid_66_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Statpearls. Publishing; 2020. Features, Evaluation and Treatment Coronavirus (COVID-19) [PubMed] [Google Scholar]
- 8.Peeri NC, Shrestha N, Rahman MH, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int J Epidemiol. 2020 doi: 10.1093/ije/dyaa033. pii: Dyaa033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Al-Dubai SA, Al-Naggar RA, Alshagga MA, Rampal KG. Stress and coping strategies of students in a medical faculty in Malaysia. Malays J Med Sci. 2011;18:57–64. [PMC free article] [PubMed] [Google Scholar]
- 10.Thompson RJ, Mata J, Jaeggi SM, Buschkuehl M, Jonides J, Gotlib IH. Maladaptive coping, adaptive coping, and depressive symptoms: Variations across age and depressive state. Behav Res Ther. 2010;48:459–66. doi: 10.1016/j.brat.2010.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Folayan MO, Cáceres CF, Sam-Agudu NA, Odetoyinbo M, Stockman JK, Harrison A. Psychological stressors and coping strategies used by adolescents living with and not living with HIV infection in Nigeria. AIDS Behav. 2017 Sep;21(9):2736–2745. doi: 10.1007/s10461-016-1534-3. doi: 10.1007/s10461-016-1534-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stoltzfus KM, Farkas KJ. Alcohol use, daily hassles, and religious coping among students at a religiously affiliated college. Subst Use Misuse. 2012;47:1134–42. doi: 10.3109/10826084.2011.644843. [DOI] [PubMed] [Google Scholar]
- 13.Cairney J, Kwan MY, Veldhuizen S, Faulkner GE. Who uses exercise as a coping strategy for stress? Results from a national survey of Canadians. J Phys Act Health. 2014;11:908–16. doi: 10.1123/jpah.2012-0107. [DOI] [PubMed] [Google Scholar]
- 14.Feld LD, Shusterman A. Into the pressure cooker: Student stress in college preparatory high schools. J Adol. 2015;41:31–42. doi: 10.1016/j.adolescence.2015.02.003. [DOI] [PubMed] [Google Scholar]
- 15.McGee R, Williams S, Nada-Raja S, Olsson CA. Tobacco smoking in adolescence predicts maladaptive coping styles in adulthood. Nicotine Tob Res. 2013;15:1971–7. doi: 10.1093/ntr/ntt081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McHugh RK, Reynolds EK, Leyro TM, Otto MW. An examination of the association of distress intolerance and emotion regulation with avoidance. Cog Therapy Res. 2013;37:363–7. doi: 10.1007/s10608-012-9463-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Woolman EO, Becker MM, Klanecky AK. PTSD symptoms mediate academic stress and drinking to cope in college students. J Drug Educ. 2015;45:96–112. doi: 10.1177/0047237915607282. [DOI] [PubMed] [Google Scholar]
- 18.Berg CJ, Ling PM, Hayes RB, Berg E, Nollen N, Nehl E, et al. Smoking frequency among current college student smokers: Distinguishing characteristics and factors related to readiness to quit smoking. Health Educ Res. 2012;27:141–50. doi: 10.1093/her/cyr106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Perez-Tejada J, Garmendia L, Labaka A, Vegas O, Gómez-Lazaro E, Arregi A. Active and passive coping strategies: comparing psychological distress, cortisol, and proinflammatory cytokine levels in breast cancer survivors. Clin J Oncol Nurs. 2019;23:583–90. doi: 10.1188/19.CJON.583-590. [DOI] [PubMed] [Google Scholar]
- 20.Folkman S. Stress, coping, and hope. Psychooncology. 2010;19:901–8. doi: 10.1002/pon.1836. [DOI] [PubMed] [Google Scholar]
- 21.Büssing A, Ostermann T, Matthiessen PF. Wer kontrolliert die Gesundheit.-Adaptive Krankheitsverarbeitungsstile bei Patienten mit chronischen Erkrankungen? Deutsche Zeitschrift Onkologie. 2008;40:150–6. [Google Scholar]
- 22.Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. 7th ed. Harlow, Essex: Pearson Education Limited; 2014. [Google Scholar]
- 23.Zang C, Guida J, Sun Y, Liu H. Collectivism culture, HIV stigma and social network support in Anhui, China: A path analytic model. AIDS Patient Care STDS. 2014;28:452–8. doi: 10.1089/apc.2014.0015. [DOI] [PubMed] [Google Scholar]
- 24.Rabelo I, Lee V, Fallah MP, Massaquoi M, Evlampidou I, Crestani R, Decroo T, Van den Bergh R, Severy N. Psychological distress among Ebola survivors discharged from an Ebola treatment unit in Monrovia, Liberia – A qualitative study. Front Public Health. 2017;4:142. doi: 10.3389/fpubh.2016.00142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Freitas JG, Galvão MT, Araújo MF, Lima CE. I.C.V. Coping experiences in the work environment of men living with HIV/ AIDS. Rev Esc Enferm USP. 2012;46(3):720–726. doi: 10.1590/s0080-62342012000300026. [DOI] [PubMed] [Google Scholar]
- 26.Roger KS, Mignone J, Kirkland S. Social aspects of HIV/AIDS and aging: A thematic review. Can J Aging. 2013;32:298–306. doi: 10.1017/S0714980813000330. [DOI] [PubMed] [Google Scholar]
- 27.Rafferty KA, Billig AK, Mosack KE. Spirituality, religion, and health: The role of communication, appraisals, and coping for individuals living with chronic illness. J Relig Health. 2015;54:1870–85. doi: 10.1007/s10943-014-9965-5. [DOI] [PubMed] [Google Scholar]
- 28.Lee M, Nezu AM, Nezu CM. Positive and negative religious coping, depressive symptoms, and quality of life in people with HIV. J Behav Med. 2014;37:921–30. doi: 10.1007/s10865-014-9552-y. [DOI] [PubMed] [Google Scholar]