

Abstract
BACKGROUND:
To prevent the rapid spread of infectious COVID-19 in India, many steps have been taken. Adherence to the control measures depends on the knowledge, attitude, and practices (KAPs) toward COVID-19 disease in health-care professionals. The present study was conducted among health-care professionals in Jaipur. The objective was to evaluate the KAPs about COVID-19 among health-care professionals.
MATERIALS AND METHODS:
A total of 385 participants took part in the study. A self-designed questionnaire was filled by the participants online (Google Form). The knowledge of the participants was assessed using 12 questions. Attitude and practices of the participants were assessed by two questions for each.
RESULTS:
Among the study completers, 52.20% were male, 71.42% of the participants were aged above 30 years, and 59.22% were nurse. The knowledge score was approximately 90%. The majority of the participants had a strong conviction that India can overcome this infectious disease in the near future. Multiple regression analysis found that good knowledge score of COVID-19 was associated with lower negative attitudes and less risky practices (P < 0.001).
CONCLUSION:
Participants of the study were knowledgeable, held positive attitudes, and had adequate practices for COVID-19.
Keywords: Attitude, COVID-19, knowledge, practices
Introduction
COVID-19 is a respiratory disease that is caused by novel coronavirus. It was initially reported in Wuhan, China, in December 2019.[1] Coronavirus disease is highly infectious, and its main clinical symptoms are dry cough, fever, dyspnea, myalgia, and fatigue.[1] In China, nearly 18.6% of patients with COVID-19 developed acute respiratory distress syndrome, coagulation and bleeding dysfunction, septic shock, and metabolic acidosis (difficult to control).[2] Empirical data have reported 2.3% fatality rate of COVID-19 in China.[3] COVID-19 is highly infectious and till February, 2020, the infection had spread across the globe in 26 countries.[4] The World Health Organization (WHO) has declared COVID-19 a public health emergency on January 30, 2020. The WHO has invited all countries for cooperative efforts to prevent the rapid spread of COVID-19.[5,6,7]
Some extraordinary control measures have been taken to prevent the transmission of COVID-19 in public such as suspension of public transportation, isolation and care of infected patients, closure of public spaces, and prevention of public gathering. The Government of India had announced a national lockdown starting from March 24, 2020, for 21 days in order to prevent and control the spread of the COVID-19 pandemic in the country.[8] On April 14, 2020, the duration of lockdown was further extended till May 3, 2020, with conditional relaxation starting from April 20, 2020, in areas where the spread of infection had been limited.[8] The fight to control COVID-19 infection is still ongoing in India because there is neither any vaccine nor definitive treatment available. Prevention and control practices are vital to prevent the spread of COVID-19 infection.
Health-care personnel continuously serve public to control the COVID-19 spread. This is a pandemic situation in which health-care workers at frontline are at greater risk to viral exposure, stress, fatigue, occupational burnout, and long working hours. Poor knowledge and awareness among health-care personnel is responsible for delayed diagnosis that affects the quality of treatment and may contribute to greater spread of COVID-19 infection. Thus, it is essential to understand the health-care professional's awareness on COVID-19 to control its outbreak. The present study has been conducted to investigate the knowledge, attitude, and practice (KAP) toward COVID-19 disease for which no literature is available on the northern part of India.
Materials and Methods
Study design and participants
The cross-sectional study was conducted among health-care professionals in Jaipur. The survey was conducted between March 5, 2020, and April 5, 2020, during the period of lockdown in India. As a result, it was not feasible to collect the data of the survey physically during this period. Alternatively, the data of the survey were collected online using Google Forms. An invitation letter requesting participation in the survey was posted on the WhatsApp group/groups of the participants, which contained a brief background, procedure, confidentiality, voluntary nature of participation, and notes for filling the Google Forms. All the interested participants provided their E-mail id at the end of the invitation letter. A total of 392 participants agreed to participate. Informed consent was taken from the interested participants on the Google Forms. The study participants were instructed to respond to the “yes” or “no” question to confirm their willingness. After approval, the participants were directed to fill out the questionnaire (Google Forms). The study participants were instructed to fill out the questionnaire (Google Forms) through both WhatsApp and Gmail. The ethical committee approval (reference number IT/01/2020) was taken from the institute to conduct the study.
Measures
The study questionnaire comprised two parts of KAP and demographics. The demographic part included gender, age, marital status, occupation, and work experience. The KAP questionnaire was developed by the authors according to the community and clinical management guidelines of COVID-19 infection.[9] The study questionnaire included both close- and open-ended questions regarding COVID-19 infection. The questionnaire consisted of four sections, that is, knowledge section, attitude section, practice section, and one section for fear of COVID-19 infection.
Questionnaire scoring
The knowledge of the participants was checked using 12 questions: four questions regarding clinical presentations of the infection (A1–A4), three questions regarding the route of transmissions (A5–A7), and five regarding the control and prevention of COVID-19 infection (A8–A12) [Supplementary File 1]. All these questions were replied on a “true/false” option with an additional option of “I don't know.” Each correct answer was given 1 point and each incorrect/unknown answer was given 0 point. The total knowledge score varied from 0 to 12. Higher score indicates good knowledge of COVID-19 infection. The attitudes of the participants toward COVID-19 infection were checked using two questions (B1–B2) [Supplementary File 1]. The practices of the participants toward COVID-19 were assessed using two close-ended questions (C1–C2) [Supplementary File 1]. On fear of COVID-19 infection, the participants were instructed to score their fear on a 0–10 scale in which 0 signified “no fear” and 10 signified “high fear.” The score of fear was again categorized into “little fear/no fear” (scored 3 or less) and “moderate to high fear” (scored 4 and above). In the present survey, the value of Cronbach's alpha coefficient for KAP questionnaire was 0.72, indicating the validity of satisfactory internal consistency.[10]
Supplementary File 1.
Questionnaire of knowledge, attitudes, and practice toward coronavirus disease 2019
| Question | Options |
|---|---|
| Knowledge | |
| A1. Fever, dry cough, myalgia, and fatigue are the main clinical symptoms of COVID-19 | True, false, I don’t know |
| A2. Unlike the common cold, sneezing, stuffy nose, and runny nose are less common in patients of COVID-19 | True, false, I don’t know |
| A3. Currently, there is no effective treatment for COVID-2019, but symptomatic and supportive treatment can help most patients recover from the infection | True, false, I don’t know |
| A4. Only those patients who are elderly, are obese, and have chronic illnesses are more susceptible to COVID-19 and develop severe symptoms | True, false, I don’t know |
| A5. COVID-19 infection is transmitted by eating or contacting wild animals | True, false, I don’t know |
| A6. COVID-19 patients can’t infect other person if there is no fever | True, false, I don’t know |
| A7. Virus of COVID-19 spreads through respiratory droplets of infected patient | True, false, I don’t know |
| A8. Medical masks can prevent the spread of COVID-19 virus infection | True, false, I don’t know |
| A9.It is not necessary for young adults and children to adopt preventive measures for COVID-19 infection | True, false, I don’t know |
| A10. COVID-19 infection can be prevented if people avoid to visit crowded places and maintain distance from each other | True, false, I don’t know |
| A11. Effective ways to reduce the spread of coronavirus are isolation and treatment of the infected patients | True, false, I don’t know |
| A12. If any person have contact with a COVID-19 patient, he/she should be isolated and kept under observation for about 14 days | True, false, I don’t know |
| Attitude | |
| B1. Do you agree that coronavirus disease will finally be effectively controlled in the near future? | Agree, disagree, I don’t know |
| B2. Do you have confidence that India can win the battle against the infectious coronavirus disease? | Yes No |
| Practices | |
| C1. Have you visited any crowded area recently? | Yes No |
| C2. Have you worn mask recently when going outside and at the time of duty? | Yes No |
| Fear | |
| How would rate their fear of getting COVID-19 on a 1 (no fear) to 10 scale (much fear)? | 1 2 3 4 5 6 7 8 9 10 |
COVID-19=Coronavirus disease 2019
Statistical analysis
Data of the study were analyzed by Statistical Package for the Social Sciences version 21.0 (SPSS) ( Chicago, USA). Categorical data of the study were presented in the form of percentage and number. KAP scores of the participants according to the demographic variables were compared with independent variables using t-test, Chi-square test, and one-way analysis of variance, as appropriate. To identify the demographic factors related to the knowledge score, multiple linear regression analysis was performed. On applying multiple linear regression analysis, all the demographic factors were assumed independent and the score of knowledge was taken as the outcome. Binary logistic regression analysis was performed to identify the demographic factors related to practices and attitudes. Variables (factors) were chosen using backward step-wise method. The association between different factors and KAP was presented in the form of regression coefficient (β) and odds ratios (OR). The participants were also categorized as those with “good knowledge” and “poor knowledge” of COVID-19 using an appropriate percentage of knowledge score. Knowledge score of ≥80 represents “good knowledge” of participants on COVID-19. The level of statistical significance was set at P < 0.05.
Results
A total of 392 questionnaires were distributed through Gmail and WhatsApp. Out of the 392 questionnaires, seven questionnaires were not included in the survey because of incomplete information. Finally, 385 participants were included in the survey. The average age of the participants was 39.5 ± 10.7 years, 62.5% of women were aged more than 30 years of age, and 40.7% of the participants were physician. The demographic data of the study participants are provided in Table 1.
Table 1.
Demographic variables of the study participants and coronavirus disease 2019 knowledge score according to demographic variables
| Variables | Number of participants (%) | Knowledge score (mean±SD) | t | P |
|---|---|---|---|---|
| Gender | ||||
| Male | 201 (52.20) | 10.2±1.8 | 3.01 | 0.002 |
| Female | 184 (47.79) | 10.8±2.1 | ||
| Age (years) | ||||
| ≤30 | 110 (28.57) | 10.4±1.9 | 4.74 | <0.001 |
| >30 | 275 (71.42) | 11.2±1.3 | ||
| Marital status | ||||
| Married | 278 (72.20) | 11.0±1.7 | 3.73 | <0.001 |
| Not married | 107 (27.79) | 10.3±1.5 | ||
| Occupation | ||||
| Physician | 157 (40.77) | 11.4±2.8 | 4.80 | <0.001 |
| Nurse | 228 (59.22) | 10.2±2.1 | ||
| Work experience (years) | ||||
| <5 | 98 (25.45) | 10.5±1.2 | 5.97 | 0.003 |
| 5-10 | 176 (45.71) | 11.0±1.8 | ||
| >10 | 111 (28.83) | 11.2±1.2 |
SD=Standard deviation
The correct answer rate of 12 questions of knowledge section on COVID-19 was 80.4 ± 9.86. The mean knowledge score of COVID-19 was 10.9 ± 1.8, indicating 90% (10.9/12 × 100) correct rate on the knowledge test. Scores of knowledge significantly varied across age, marital status, and occupation (P < 0.001) [Table 1]. Multiple linear regression analysis indicated that gender (β: −0.282, P < 0.001), age groups (β: −0.320, P < 0.001), marital status (β: −0.212, P < 0.001), occupation (β: −0.192, P < 0.001), and work experience <5 years versus 5–10 years (β: −1.421, P < 0.001) were statistically significantly related to the poor knowledge of COVID-19 [Table 2].
Table 2.
Factors associated with poor knowledge of coronavirus disease 2019 (multiple linear regression)
| Factors | Coefficient | Standard error | t | P |
|---|---|---|---|---|
| Gender (male vs. female) | −0.282 | 0.036 | 5.672 | <0.001 |
| Age group (≤30 vs. <30 years) | −0.320 | 0.056 | 4.221 | <0.001 |
| Marital status (not married vs. married) | −0.212 | 0.042 | 3.112 | <0.001 |
| Occupation (nurse vs. physician) | −0.192 | 0.045 | 3.568 | <0.001 |
| Work experience (<5 vs. 50-10 years) | −1.421 | 0.056 | 3.314 | <0.001 |
| Work experience (5-10 vs. >10 years) | −0.157 | 0.066 | 2.550 | 0.041 |
Majority of the participants (90.6%) agreed that COVID-19 infection will be controlled successfully. The response rates of the options “I don't know” and “disagree” were 7.2% and 1.4%, respectively. The attitude of the participants to control COVID-19 statistically significantly varied across gender (P < 0.05), age (P < 0.01), and work experience (P < 0.001). The participants reporting “I don't know” and “disagree” had less knowledge as compared to those reporting “agree” (P < 0.001) [Table 3]. Results of the multiple logistic regression showed that marital status and knowledge score of COVID-19 were statistically significantly related with disagreement in controlling the infection (P < 0.001). Occupation (P = 0.001), work experience (P = 0.001), and COVID-19 knowledge score (P < 0.001) were statistically significantly related with the response of “I don't know” [Table 4]. Majority of the participants had a strong belief that India can successfully win the fight against COVID-19. The knowledge score was statistically significantly less in the participants without as compared to those with the confidence of winning (P < 0.01) [Table 3].
Table 3.
Attitude of the study participants toward coronavirus disease 2019 according to demographic factors
| Factors | Attitudes, n (%) or mean±SD | ||||
|---|---|---|---|---|---|
| B1: Success in controlling | B2: Wining confidence | ||||
| Agree | Disagree | Don’t know | Yes | No | |
| Gender | |||||
| Male | 190 (94.52) | 3 (1.48) | 8 (3.98) | 137 (68.15) | 64 (31.84) |
| Female | 163 (88.58) | 5 (2.717) | 16 (8.69)* | 146 (79.34) | 38 (20.65) |
| Age (years) | |||||
| ≤30 | 76 (69.09) | 6 (5.45) | 28 (25.45) | 68 (61.81) | 42 (38.18) |
| >30 | 258 (93.81) | 5 (1.81) | 12 (4.36)** | 253 (92.0) | 22 (8.0) |
| Marital status | |||||
| Married | 218 (78.41) | 9 (3.23) | 51 (18.34) | 234 (84.17) | 44 (15.82) |
| Not married | 87 (81.30) | 4 (3.73) | 16 (14.95) | 89 (83.17) | 18 (16.82) |
| Occupation | |||||
| Physician | 122 (77.70) | 5 (3.18) | 30 (19.10) | 143 (91.08) | 14 (8.91) |
| Nurse | 181 (79.38) | 4 (1.75) | 43 (18.85) | 189 (82.89) | 39 (17.10)* |
| Work experience (years) | |||||
| <5 | 65 (66.32) | 7 (7.14) | 26 (26.53) | 58 (59.18) | 40 (40.81) |
| 5-10 | 157 (89.20) | 4 (2.27) | 15 (8.52) | 156 (88.63) | 20 (11.36) |
| >10 | 97 (87.38) | 3 (2.70) | 11 (9.90)*** | 91 (81.98) | 20 (18.01) |
| COVID-19 | |||||
| Knowledge score | 10.6±1.4 | 10.5±1.2 | 10.3±2.0*** | 10.7±1.4 | 10.1±2.4** |
*Statistically significant difference at P<0.05, **Statistically significant difference at P<0.01, ***Statistically significant difference at P<0.001. SD=Standard deviation, COVID-19=Coronavirus disease 2019
Table 4.
Factors significantly associated with attitudes toward coronavirus disease 2019 infection (multiple binary logistic regression)
| Factors | OR (95%CI) | P |
|---|---|---|
| B1: Disagree with final success (vs. agree) | ||
| Gender (male vs. female) | 1.99 (1.02-3.69) | 0.049 |
| Marital status (married vs. not married) | 1.40 (0.67-0.78) | <0.001 |
| Knowledge score of COVID-19 | 0.81 (0.67-0.78) | <0.001 |
| B1: Don’t know about final success (vs. agree) | ||
| Age group (≤30 vs. >30) | 1.67 (1.03-2.65) | 0.012 |
| Occupation (physician vs. nurse) | 1.30 (1.14-1.60) | 0.001 |
| Work experience | ||
| <5 vs. 50-10 years | 1.52 (1.10-2.37) | 0.037 |
| 5-10 vs. >10 years | 1.30 (1.14-1.60) | 0.001 |
| Knowledge score of COVID-19 | 0.82 (0.63-0.72) | <0.001 |
| B2: No confidence of winning COVID-19 | ||
| Occupation (physician vs. nurse) | 1.73 (1.12-2.57) | 0.012 |
| Age group (≤30 vs. >30) | 1.52 (1.02-2.17) | 0.048 |
| Knowledge score of COVID-19 | 0.74 (0.60-0.72) | <0.001 |
SD=Standard deviation, CI=Confidence interval, OR=Odds ratio, COVID-19=Coronavirus disease 2019
The majority of the respondents had not visited crowded areas and wore masks while going out [Table 5]. Results of the multiple regression analyses indicated that occupation (P = 0.01) and COVID-19 knowledge score (P = 0.001) were associated with the practice of visiting crowded areas, while gender (P = 0.01) and knowledge score (P = 0.001) were statistically significantly related to the practice of not wearing mask outside [Table 6]. Majority of the participants reported “moderate-to-high” fear of COVID-19 infection. The difference in the variables related to the level of COVID-19 knowledge (poor and good knowledge) is shown in Figure 1.
Table 5.
Practices of the study participants toward coronavirus disease 2019 according to demographic factors
| Factors | Practices, n (%) or mean±SD | |||
|---|---|---|---|---|
| C1: Going to crowded areas | C2: Mask wearing | |||
| Yes | No | Yes | No | |
| Gender | ||||
| Male | 10 (4.97) | 191 (95.01) | 192 (95.51) | 9 (4.47) |
| Female | 2 (1.08) | 182 (98.91)* | 182 (98.91) | 2 (1.08)* |
| Age (years) | ||||
| ≤30 | 5 (4.54) | 105 (95.45) | 106 (96.36) | 4 (3.77) |
| <30 | 5 (1.81) | 270 (98.18) | 272 (98.90) | 3 (1.09) |
| Marital status | ||||
| Married | 6 (2.15) | 272 (97.84) | 277 (99.64) | 1 (0.35) |
| Not married | 8 (7.47) | 99 (92.52)** | 97 (90.65) | 10 (9.34)*** |
| Occupation | ||||
| Physician | 1 (0.63) | 156 (99.36) | 155 (98.72) | 2 (1.27) |
| Nurse | 8 (3.50) | 220 (96.49)* | 216 (94.73) | 12 (5.26)** |
| Work experience (years) | ||||
| <5 | 5 (5.10) | 93 (94.89) | 92 (93.87) | 6 (6.12) |
| 5-10 | 3 (1.70) | 173 (98.29) | 175 (99.43) | 1 (0.56) |
| >10 | 2 (1.83) | 109 (98.19) | 110 (99.09) | 1 (0.90) |
| COVID-19 | ||||
| Knowledge score | 10.2 (2.3) | 10.6 (1.4) | 10.7 (1.3) | 9.2 (2.3)*** |
*Statistically significant difference at P<0.05, **Statistically significant difference at P<0.01, ***Statistically significant difference at P<0.001. SD=Standard deviation, COVID-19=Coronavirus disease 2019
Table 6.
Factors significantly associated with practices toward coronavirus disease 2019 infection (multiple binary logistic regression)
| Factors | OR (95% CI) | P |
|---|---|---|
| C1: Going to a crowded place | ||
| Gender (male vs. female) | 1.36 (1.04-1.75) | 0.018 |
| Marital status (married vs. not married) | 1.16 (1.13-1.10) | 0.006 |
| Occupation (physician vs. nurse) | 1.70 (1.84-2.00) | 0.001 |
| Knowledge score of COVID-19 | 0.80 (0.58-0.69) | 0.001 |
| C2: Not using a mask | ||
| Gender (male vs. female) | 1.88 (1.23-2.43) | 0.001 |
| Marital status (married vs. not married) | 1.73 (1.64-1.58) | 0.003 |
| Occupation (physician vs. nurse) | 1.23 (1.02-1.21) | 0.004 |
| Knowledge score of COVID-19 | 0.76 (0.37-0.38) | 0.001 |
CI=Confidence interval, OR=Odds ratio, COVID-19=Coronavirus disease 2019
Figure 1.
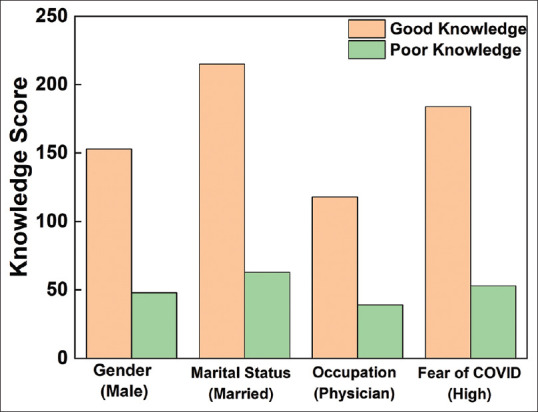
Comparison of study factors in relation to COVID-19 knowledge score. Knowledge score ≥ 80% used for good knowledge
Discussion
Knowledge about COVID-19 is essential to control and manage the spread of the infection. The overall knowledgeable rate among health-care professionals in the present study was 90%, which is quite high. Nour Mo et al.[11] evaluated the KAPs of health-care providers on MERS-CoV infection and also reported a better knowledge score (89.2%). A high knowledge score among health-care professionals could be attributed to proficiency in medical field. Moreover, knowledge score of physicians was greater as compared to nurses. The multiple linear regression analysis found that male gender, occupation, and work experience were the major factors linked with poor knowledge. Clements[12] also reported that COVID-19 knowledge score was significantly associated with gender and occupation.
Majority of the participants (90.6%) held a positive attitude and a strong conviction that COVID-19 infection can be effectively contained and controlled in India. The optimistic attitude of the respondents was significantly associated with knowledge score as shown by multiple regression analysis. The results were comparable with those of the study conducted by Shi et al.[13] who reported a significant relationship between knowledge score and the optimistic attitude of medical staff. In addition, Baseer et al.[14] carried out an awareness study on COVID-19 infection among dental health professionals and found that knowledge score and attitude score were directly correlated.
The practices of health-care workers were watchful as majority of the participants (73%) avoided visiting crowded areas and wore good-quality masks. Similar practices in studies have been reported in literature.[15,16,17] Multiple binary logistic regression was carried out between demographic factors (marital status, gender, and occupation) and practices toward COVID-19 infection. On analysis, it was observed that occupation and marital status have a significant influence on practice skills. A significant association was found between dangerous practices and gender (male) as young male participants often visit crowded places without wearing mask. Similar relationship has been observed in previously published studies.[18,19]
Limitations
The major limitation of the present study is the inadequate and unstandardized assessment of practices and attitudes toward COVID-19 disease. Adequate assessment of attitude and practices requires in-depth interview and group discussion that was not possible through Google Forms. Therefore, in this study, both attitude and practices were measured using only two simple questions.
Conclusion
It has been observed that the participants who have good knowledge score of COVID-19 follow correct practices and have a positive attitude. Demographic factors such as gender, occupation, and experience significantly affect the KAPs of the participants. Few participants have a negative attitude and follow inadequate practices. Thus, health-care systems should implement some advance health programs to educate the health-care workers. Further studies with larger sample size are required to explore the KAP toward COVID-19 among health-care professionals for better understanding.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to acknowledge all the participants, faculty, and staff members for providing their valuable time and support for the study.
References
- 1.Surveillances V. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) China, 2020. China CDC Weekly. 2020;2:113–22. [PMC free article] [PubMed] [Google Scholar]
- 2.Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet. 2020;395:507–13. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Munster VJ, Koopmans M, van Doremalen N, van Riel D, de Wit E. A novel coronavirus emerging in China-Key questions for impact assessment. N Engl J Med. 2020;382:692–4. doi: 10.1056/NEJMp2000929. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. 2020. [Last accessed on 2020 Mar 06]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports .
- 5.World Health Organization. 2019-nCoV Outbreak is an Emergency of International Concern. 2020. [Last accessed on 2020 Mar 06]. Available from: http://www.euro.who.int/en/health-topics/emergencies/pages/news/new s/2020/01/2019-ncov-outbreak-is-an-emergency-of-international-concern .
- 6.Kazemi-Karyani A, Safari-Faramani R, Amini S, Ramezani-Doroh V, Berenjian F, Dizaj MY, et al. World one-hundred days after COVID-19 outbreak: Incidence, case fatality rate, and trend. J Educ Health Promot. 2020;9:199. doi: 10.4103/jehp.jehp_483_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shanbehzadeh M, Kazemi-Arpanahi H, Mazhab-Jafari K, Haghiri H. Coronavirus disease 2019 (COVID-19) surveillance system: Development of COVID-19 minimum data set and interoperable reporting framework. J Educ Health Promot. 2020;9:203. doi: 10.4103/jehp.jehp_456_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aggarwal V. Effective ways to make coronavirus lockdown: Productive and positive. Purakala with ISSN 0971-2143 is an UGC CARE J. 2020;31:1798–807. [Google Scholar]
- 9.Revised Guidelines on Clinical Management of COVID - 19. Government of India Ministry of Health & Family Welfare Directorate General of Health Services (EMR Division) [Last accessed on 2020 Apr 09]. Available from: https://www.mohfw.gov.in/pdf/Revised National Clinical ManagementGuidelineforCOVID 1931032020.pdf .
- 10.Taber KS. The use of Cronbach's alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48:1273–96. [Google Scholar]
- 11.Nour MO, Babilghith AO, Natto HA, Al-Amin FO, Alawneh SM. Knowledge, attitude and practices of healthcare providers towards MERS-CoV infection at Makkah hospitals, KSA. Int Res J Med MedSci. 2015;3:103–2. [Google Scholar]
- 12.Clements JM. Knowledge and behaviors toward COVID-19 among US residents during the early days of the pandemic: Cross-sectional online questionnaire. JMIR Public Health Surveill. 2020;6:e19161. doi: 10.2196/19161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Shi Y, Wang J, Yang Y, Wang Z, Wang G, Hashimoto K, et al. Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID-19. Brain Behav Immun Health. 2020;29:100064. doi: 10.1016/j.bbih.2020.100064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Baseer MA, Ansari SH, Al-Shamrani SS, Alakras AR, Mahrous R, Alenazi AM. Awareness of droplet and airborne isolation precautions among dental health professionals during the outbreak of coronavirus infection in Riyadh city, Saudi Arabia. J Clin Exp Dent. 2016;8:379–87. doi: 10.4317/jced.52811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Khan MU, Shah S, Ahmad A, Fatokun O. Knowledge and attitude of healthcare workers about middle east respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health. 2014;14:1–7. doi: 10.1186/1471-2458-14-1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Giao H, Thi N, Han N, Van KT, Ngan VK, Van TV, et al. Knowledge and attitude toward COVID-19 among healthcare workers at Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13:1–6. [Google Scholar]
- 17.Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health and Surveillance. 2020;6(2):e19160. doi: 10.2196/19160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cobey KD, Laan F, Stulp G, Buunk AP, Pollet TV. Sex differences in risk taking behavior among Dutch cyclists. Evol Psychol. 2013;11:350–64. [PubMed] [Google Scholar]
- 19.Pawlowski B, Atwal R, Dunbar RI. Sex differences in everyday risk-taking behavior in humans. Evol Psychol. 2008;6:39–42. [Google Scholar]