

Abstract
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) provides breastfeeding support and free formula to low-income participating infants in the U.S. Literature has consistently documented worse breastfeeding outcomes in WIC infants and children than in non-participants, although self-selection bias poses a challenge in examining the relationship between WIC participation and breastfeeding in low-income mother-child dyads. The WIC program adopted a comprehensive food package revision in 2009, the first one in four decades. Since that time, few national studies have examined the relationship between WIC participation and breastfeeding while controlling for the endogeneity of WIC participation with the propensity score method. This paper applied an instrumental variable (IV) approach on a large, nationally representative survey sample of children, the National Immunization Surveys (NIS), to examine the relationship between WIC participation and breastfeeding among children born between 2005 and 2014. We identified state Supplemental Nutrition Assistance Program (SNAP) enrollment rates and SNAP Policy Indices as valid IVs to address WIC participation endogeneity. Without the IVs, WIC participation had a significantly negative relationship with breastfeeding. After addressing endogeneity using the IVs, the relationship became insignificant in the whole sample and in the subpopulations across race/ethnicity and child gender. The neutrality of WIC participation on breastfeeding is important for policy makers to understand in seeking to improve breastfeeding among WIC participants.
Keywords: WIC, breastfeeding, instrumental variable
1. Introduction
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is a federal nutrition assistance program in the U.S. that provides supplemental food packages, nutrition education, and health care referrals for eligible low-income women (pregnant, breastfeeding, and non-breastfeeding postpartum), infants, and children up to age five (USDA, 2020a). The monthly number of participants reached approximately 6.87 million in fiscal year 2018 (USDA, 2019). Given the well-documented health benefits of breastfeeding, the WIC program is designed at least in part by the governing federal regulations to promote breastfeeding among participating mother-infant dyads (USDA, 2016). At the same time, WIC provides free formula for participating women who do not fully breastfeed their infants. These seemingly conflicting policies have complicated the relationship between WIC participation and breastfeeding.
Literature has consistently documented worse breastfeeding outcomes in WIC infants and children than in non-participants (Ryan & Zhou, 2006; Ziol-Guest & Hernandez, 2010; Jensen, 2012). For example, the proportion of infants and children ever breastfed in 2016 was 81.1% in the general population but was only 71.0% in WIC participants (USDA, 2018; CDC, 2020). The latest report from the National Academies of Sciences, Engineering and Medicine (NASEM) Committee to Review WIC Food Packages (“the NASEM WIC Committee”) disclosed these consistent outcomes in WIC-participating infants compared to all infants in 2008–2013 (NASEM, 2017). Even compared with WIC-eligible non-participants, with adjustment for changes in socio-demographics, WIC-participating infants and children still had lower breastfeeding rates, although the gap has been closing in more recent years (Zhang et al., 2019). Therefore, it is an intriguing question whether WIC participation is causing the poorer breastfeeding outcomes, potentially due to the availability and distribution of free formula to mothers who do not fully breastfeed.
1.1. Background: WIC policy changes pertinent to breastfeeding
WIC is a joint federal-state program to provide nutrition assistance to eligible women, infants, and children. Different from other nutrition assistance programs, such as the Supplemental Nutrition Assistance Program (SNAP), WIC is not an entitlement program, which means its funding depends on the Congress’ authorization each year (USDA, 2020a, 2020b). The U.S. Department of Agriculture/Food Nutrition Service (USDA/FNS) is the federal agency that provides WIC grants to 90 agencies, including states, U.S. territories, and Indian tribes, and ensures their compliance with WIC regulations.
In the last three decades, guidelines on breastfeeding have been consistently updated to improve outcomes. The Child Nutrition and WIC Reauthorization Act of 1989 required state WIC agencies to incorporate breastfeeding into their nutrition education efforts and to assign breastfeeding coordinators to provide training and support to participants (H.R. 24, 1989). In addition, the Healthy Meals for Healthy Americans Act of 1994 mandated spending requirements for state WIC agencies to promote breastfeeding to pregnant and post-partum WIC participants (H.R. 8, 1993). In 1997, the USDA launched the Loving Support Makes Breastfeeding Work campaign to promote breastfeeding among WIC mothers (National WIC Association, 2019). In 2004, WIC launched the Breastfeeding Peer Counselor Initiative, in which peer mothers with breastfeeding training and experience served as counselors for WIC mothers’ breastfeeding (National WIC Association, 2019).
A milestone WIC policy change came in the 2009 WIC food package revision, the first overhaul of WIC in the past four decades. The changes reduced the amount of infant formula to women who received the partially breastfeeding package and increased the amount of non-formula supplemental food for fully breastfeeding mothers (NASEM, 2017). The rationale was to incentivize new WIC mothers to enroll in the fully breastfeeding package, thereby increasing breastfeeding rates among participants. However, evidence for the change’s impact has been mixed, despite reports of increased breastfeeding rates among WIC participants (NASEM, 2017). While some populations were more likely to breastfeed, some state WIC programs saw no change in the overall breastfeeding rates attributable to the food package changes (Langellier et al., 2014; Wilde et al., 2011, 2012). Although more new mothers enrolled in the fully breastfeeding package, more mothers were also assigned to the full formula package, which does not require breastfeeding (Wilde et al., 2011). In the absence of a proper point of comparison, such as eligible non-participants’ breastfeeding behaviors over the same period, it is challenging to determine whether or not these mother-infant dyads would have done the same without participating in WIC.
1.2. Previous studies related to the relationship between WIC participation and breastfeeding among participants
A series of studies have demonstrated that the endogeneity of WIC participation can create misestimates of the program’s effect on infants’ and children’s birthweight, oral health, and nutrition intake (Kowaleski-Jones & Duncan, 2002; Lee et al., 2004; Yen, 2010). The “selection bias” of WIC participation can also make breastfeeding outcomes appear worse among participants, i.e., observable or unobservable characteristics can lead to women who are less likely to breastfeed enrolling in the WIC program. Table 1 lists the series of efforts in the field to address the effect of endogeneity of WIC participation on breastfeeding outcomes.
Table 1.
Studies Addressing Selection Bias of WIC Participation in Breastfeeding
| Public ation Year | First Author’s Last Name | Data | Study Period | Sample Size | Approach | Results |
|---|---|---|---|---|---|---|
| 2005 | Bitler | Pregnancy Risk Assessment Monitoring System (PRAMS) (19 states) | 1992–1999 | 60,731 | State-year fixed effect | + |
| 2010 | Jiang | Panel Study of Income Dynamics | 1997 | 3,276 | Propensity score | biased negative relations hip |
| 2013 | Martin-Anderson | Infant Feeding Practices Study II | 2005–2007 | 785 | WIC duration | − |
| 2015 | Metallinos-Katsaras | Massachusetts WIC Program | 2001–2009 | 122,506 | WIC duration | + |
| 2016 | Bullinger | Infant Feeding Practices Study II | 2005–2007 | 3,029 | IV (state-level grocery price index) | − |
| 2016 | Gregory | Infant Feeding Practices Study II | 2005–2007 | 743 | Propensity score | no negative |
| 2017 | Sonchak | South Carolina Birth Certificate Data | 2004–2013 | 16,457 | Maternal fixed effects | no negative |
| 2017 | Topolyan | Infant Feeding Practices Study II | 2005–2007 | 2,616 | WIC duration | − |
| 2019 | Li | National Health and Nutrition Examination Survey (NHANES) | 2005–2014 | 4,308 | Propensity score | − |
+/−: Positive/negative relationship between WIC participation and breastfeeding
Four analytic approaches have been exploited to address the potential selection bias: fixed effects (Bitler & Currie, 2005; Sonchak, 2017), propensity score (Jiang et al., 2010; Gregory et al., 2016; Li et al., 2019), exposure to WIC duration (Martin-Anderson, 2013; Metallinos-Katsaras et al., 2015; Topolyan & Xu, 2017), and IV (Bullinger & Gurley-Calvez, 2016). The sample sizes of these studies were limited to around 4,000, and the results consistently indicated a negative relationship between WIC participation and breastfeeding. Jiang et al. (2010) used the Panel Survey of Income Dynamics (PSID) data but suggested the negative relationship might be biased. The other studies had larger sample sizes, but most of them were limited to one or multiple states with a more positive effect of WIC participation on breastfeeding (Bitler & Currie, 2005; Metallinos-Katsaras et al., 2015; Sonchak, 2017). Therefore, sample size could potentially affect the effect estimation even while controlling the self-selection bias. The most significant limitation of these studies is the short or outdated study periods, which could not capture the long-term WIC program and policy changes in breastfeeding promotion. The only exceptions are Sonchak (2017) and Li et al. (2019), which covered the periods of 2004–2014 and 2005–2014, respectively.
Given the continuing interest of the WIC program in breastfeeding outcomes, it is worth the effort to examine the relationship between WIC participation and breastfeeding by explicitly addressing endogeneity in empirical estimation. In this study, we used the National Immunization Survey (NIS) from 2006–2016, the standard national data used by the CDC to create the national breastfeeding report card annually, to examine the relationship between WIC participation and breastfeeding. An IV approach was used to address the endogeneity issues. This is the first national study using an IV approach to examine the WIC participation effect on breastfeeding after the milestone 2009 WIC revisions.
2. Methodology
2.1. Data sources
Our primary data source is the National Immunization Surveys (NIS), a national, population-based survey sponsored and conducted by the National Center for Immunization and Respiratory Diseases (NCIRD) of the Centers for Disease Control and Prevention (CDC) (CDC, 2018). It is an annual, telephone-based survey interviewing parents or guardians in all 50 states, the District of Columbia, and some U.S. territories to monitor vaccination coverage among children 19–35 months and teens 13–17 years. The NIS provides nationally, state, and locally representative estimates of vaccination coverage among children and teenagers. We used the NIS-child data in this study, which contains information on socio-demographics and health insurance coverage for children 19–35 months of age as well as their mothers’ WIC participation status and the child’s breastfeeding information. This is the data used by the CDC to produce the annual National Breastfeeding Report Card, which includes the national- and state-level breastfeeding rates (CDC, 2020).
Aiming to be consistent with the National Breastfeeding Report Card, we included the data from 50 states and D.C. and combined two survey years’ data into one cohort by the year of the child’s birth, following the methods used in the CDC NIS data analysis guide (NIS, 2018). Data for this study were derived from the 2006–2016 NIS-child public use data, which does not provide the survey child’s birth month and year information but includes the child’s age group information (age groups: 19–23 months, 24–29 months, and 30–35 months). We used the child’s age group information to infer their birth cohort. For example, children aged 19–23 months in the 2015 NIS-child survey year represent children born from January 2014 to May 2014. Similarly, children aged 24 months or older in the 2016 NIS-child survey data could also have been born in 2014. Therefore, we combined these children from the 2015 and 2016 NIS-child survey data to create a 2014 NIS-child birth cohort. In this study, we created the birth cohorts from 2005 to 2014 by using the 2006–2016 NIS-child survey data. Since 4.14% of NIS households had more than one child surveyed in the sample, we removed these households so that each sampled household had only one sampled child.
2.2. Key variables
We used NIS-child to construct our key variables of interest. The primary outcome variable was the ever-breastfeeding status, which was derived from the answer to the question, “Was the child ever breastfed or fed breastmilk.” The measurement is consistent with the National Breastfeeding Report Card, which uses the same data source (CDC, 2020).
The primary exposure variable was WIC participation, which was derived from the question, “Has the child ever received WIC benefits.” We used the answer to this question, instead of “currently receiving WIC,” as a proxy of WIC participation at infancy due to the following reasons: First, NIS sample children were aged 19–35 months, which means a low prevalence of children still being breastfed at the survey time, so the indicator of currently receiving WIC was not directly related to their breastfeeding statuses at the survey time (CDC, 2020). Second, more than 70% of children started their WIC participation at infancy (age 0) (Burstein et al., 2000; Castner et al., 2009). The 2017 participation rates among eligible infants and children at ages 1, 2, 3, and 4 were 79.3%, 57.5%, 43.8%, 40.0%, and 25.0%, respectively (USDA, 2020c). Multiple barriers exist for children to participate in WIC, e.g., misconceptions that only infants are eligible and dissatisfaction with the contents of the children’s food package (FRAC, 2019). The average value of the children’s package was $39.07, compared with the infant food package value of $123.06 in Fiscal Year 2014 (USDA/FNS, 2018). Given no strong economic incentives but significant barriers, older children are unlikely to be enrolled in the WIC program as new participants. Therefore, it is appropriate to use the “ever received WIC benefits” as a proxy to measure WIC participation as infants.
The child’s and mother’s socio-demographics were controlled, including the child’s age group in the survey year (19–23 months, 24–29 months, 30–35 months), birth cohort, gender, and race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and others), poverty-income ratio (PIR), i.e., the ratio between household income and the federal poverty level (FPL), maternal education group (less than high school, high school graduate or GED, some college education but no degree, college graduate or higher), maternal age group in the survey year (less than 30 years old, equal to or older than 30 years), mother’s marital status (married, non-married), number of people in the household, and interview language (English, Spanish, other).
To control the state-level policy variables, except for adding the state dummies for state fixed effects, we also added the state annual unemployment rate, Temporary Assistance for Needy Families (TANF) enrollment rate, which was defined as number of participants divided by state population, and Children’s Health Insurance Program (CHIP) enrollment rate, which was defined as number of participating infants and children divided by number of children 18 or under in the state. State unemployment rates, TANF enrollment rates, and CHIP enrollment rates were derived from multiple national data sources (Hoag et al., 2011; IPPSR, 2019; Medicaid, 2020; The Annie E. Casey Foundation, 2020; U.S. BLS, 2020). Controlling state dummies and state-level policy variables is a common practice in policy analyses (Sloan & Shadle, 2009; Abaluck & Gruber 2011; Aguiar et al., 2013; Grabowski et al., 2013).
2.3. Endogenous WIC participation and IV selection
Nonrandom selection into WIC participation causes an endogeneity problem in estimating effects and drawing causal inferences about WIC participation on health behaviors and outcomes (Jiang et al., 2010). Without dealing with the endogenous selection problem, the estimated effects of any study would possibly be biased and reflect the influences of the characteristics of the WIC participants that led them to enroll instead of the impact of the WIC program.
To our best knowledge, only one previous study has employed IVs to address the endogeneity of WIC participation in breastfeeding (Bullinger & Gurley-Calvez, 2016). However, they used the state-level grocery price index as the IV, which was unlikely to be the primary motivator for WIC participation. Moreover, the result indicated that WIC participation reduced exclusive breastfeeding by 50%, which was beyond a reasonable range. Therefore, it is worth using a new IV to revisit the relationship between WIC participation and breastfeeding.
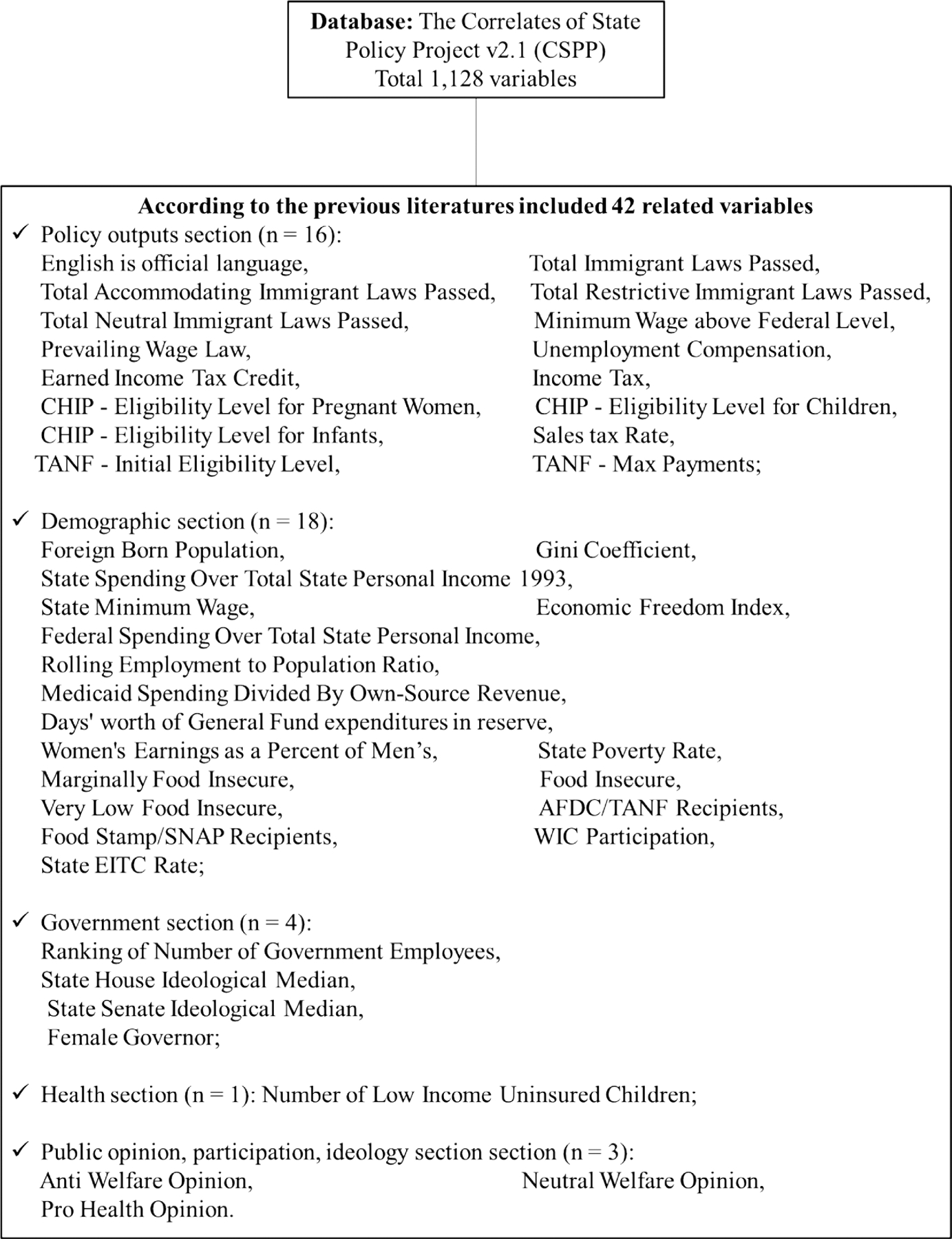
Empirically, we need to identify a set of legitimate IVs that are highly correlated with WIC participation but uncorrelated with the outcome: breastfeeding. Since WIC is implemented by state WIC agencies, state policies can influence the decision to participate in the WIC program (Bitler & Currie, 2005). Aiming to find a strong instrumental variable for WIC program participation, we explored a longitudinal state policy database, the Correlates of State Policy Project (CSPP), created by the Institute for Public Policy and Social Research (IPPSR) at Michigan State University (IPPSR, 2019). We screened 1,128 variables in CSPP and identified only one variable as a candidate: the annual state SNAP enrollment rate, which is defined as the number of SNAP participants in that year divided by the number of the state’s population in that year. The definition of the state SNAP enrollment rate was the same as in Ganong & Liebman (2018), and the IV screening process is summarized in Figure 1.
Fig. 1.
The IV Selection and Identification Process
2.4. SNAP enrollment rate as a possible IV for WIC participation
Heckman & Smith (2004) suggested that understanding the process of participating in a social program is required for identification of IVs. These participation processes can be divided into multiple stages, e.g., “eligibility, awareness, application, acceptance, and enrollment.” However, these heterogeneous processes make identifying a suitable IV challenging, since the ideal IV is supposed to affect all stages in the participation process while not affecting the outcome variable. For example, the WIC program’s outreach efforts may determine the awareness of the prospective participants but should not affect their breastfeeding intentions. Similarly, the WIC staff’s friendliness or professionalism may affect WIC-eligible women’s application process, but not their breastfeeding awareness. However, given the limited resources in the real world, these ideal IVs may not be able to be measured. Thus, we may have to make a tradeoff between being without an ideal IV or having any IV, which may not meet the strictest theoretical expectation but would survive the tests, i.e., a “second best” IV.
The state SNAP enrollment rate could be a valid candidate for such a “second best” IV. First, the SNAP participation process mirrors the WIC participation process. Both programs are nutrition assistance programs managed federally by the USDA and operated by state agencies (Hoynes & Schanzenbach, 2015). The SNAP enrollment rate could serve as a proxy outcome for many underlying factors related to the WIC participation process that are unobservable or challenging to measure, e.g., the staff’s general attitudes toward the applicant. Second, based on the socio-ecological framework proposed by Pinard et al. (2017), we conducted additional literature review to compare the factors affecting SNAP and WIC participation. As shown in Appendix Table 1, there was significant overlap between factors affecting either WIC or SNAP participation. For example, some state policies to improve enrollment are similar between SNAP and WIC programs (Swann, 2010; Ganong & Liebman, 2018). More specifically, state agencies can adopt policies to simplify reporting or determine the recertification lengths in both programs. Due to adjunctive eligibility, SNAP participants can be enrolled in WIC automatically (Swann, 2010). States can adopt different approaches, e.g., approval notice, phone call verification, and online verification, to check the adjunctive eligibility (Neuberger, 2017). Therefore, the SNAP participation process is a good proxy for the WIC participation process.
Like individual WIC participation, individual SNAP participation can be endogenous as well. However, the state SNAP enrollment rate depends more on exogenous economic conditions and state policies (Ganong & Liebman, 2018). Moreover, SNAP does not have any age limitation, while WIC is only applicable to pregnant or postpartum women, infants, and children under 5. In Fiscal Year 2017, approximately 42 million Americans participated in SNAP, but only approximately 7 million Americans participated in WIC (USDA, 2020d; USDA, 2020e). Therefore, the state-level SNAP enrollment rate could be a proxy for the state-level policies that may affect individual WIC participation, but it is unlikely to be endogenous to breastfeeding.
The SNAP enrollment rate may depend on other factors, e.g., the unemployment rate, and the effects of these factors on breastfeeding are unknown or inconclusive, having received limited research among WIC-eligible populations. Therefore, we enhanced the IVs by adding the SNAP Policy Index as an additional IV, which reflects the state-level welfare policies that can affect WIC participation. The SNAP Policy Index was constructed by the USDA/Economic Research Service (ERS) to reflect changes in eligibility, transaction costs, stigma, and outreach of the state-level SNAP policies since 1996 (USDA, 2020f).
Our approach provides new insights for future researchers to use in exploring IVs regards WIC participation. Given almost no valid IVs identified in the field to examine the important relationship between WIC participation and breastfeeding, the IVs identified in this paper serve as a compromised but ground-breaking choice until the day that ideal IVs can be identified in future research.
Since other welfare programs, such as TANF and CHIP, are also operated at the state level and can be influenced by state-level policies, we tested these two programs’ state-level enrollment rates as potential IV candidates. Notably TANF and CHIP are administrated by the Department of Health and Human Services (DHHS) at the federal level (CMCS, 2020; U.S. DHHS, 2020), which is different from WIC’s federal agency. We compared these IV candidates with the SNAP enrollment rate and SNAP Policy Index as a robustness check of IV selection.
3. Empirical Application
Following the common practice to identify IVs (Wooldridge, 2010; Sovey & Green, 2011), we used the SNAP enrollment rate (SNAP), the squared form (SNAP2), and the SNAP Policy Index as the IV set. A two-stage estimation approach was used to assess the relationship between WIC participation and breastfeeding practices. First, a linear probability model was fit. The model is in the form of
| (1) |
where I indexes the child, and s is the state. IV indicates the instrumental variables. The variable S is a set of state-level variables, including the state dummies, state unemployment rate, TANF enrollment rate, and CHIP enrollment rate. Xis includes children’s characteristics, including child’s age group, birth cohort, gender, and race/ethnicity. Mis captures the mothers’ and household characteristics, including maternal age group and socioeconomic status, mother’s marital status, number of people in the household, and interview language. Equation (1) was the first-stage procedure to obtain the probability of participating in the WIC program for the mothers of income-eligible children.
Then, the predicted WIC participation from the first step was used in the second step regression model:
| (2) |
where BFis is an indicator of whether the child was ever breastfed. The main explanatory variable of interest is , the predicted probability of WIC participation.
Linear probability models (LPM) were employed given the following considerations:
First, as Angrist & Pischke (2008) suggested, using a linear probability model even though the response is binary is more appropriate in the context of limited dependent variable models with dummy endogenous regressors. Only the LPM guarantees that the first-stage regression produces fitted values that are uncorrelated with the residuals. Nonlinear models such as probit or logit may seem appropriate only when the first-stage conditional expected function (CEF) is actually nonlinear, which is difficult to test. In contrast, conventional two-stage least square (2SLS) estimates using LPM are consistent whether or not the first-stage CEF is linear. Even when the first-stage CEF is nonlinear, the marginal effects from nonlinear structural models are close to the conventional 2SLS using LPM. As Angrist (2001) stated, “If the dependent variable is binary, a nonlinear first-stage model such as probit or logit may seem appropriate for 2SLS estimation…. But the resulting second-stage estimates are inconsistent unless the model for the first-stage CEF is actually correct. On the other hand, conventional 2SLS estimates using a linear probability model are consistent whether or not the first-stage CEF is linear, so it is generally safer to use a linear first-stage” (Angrist, 2001).
Furthermore, as Wooldridge (2010) pointed out, it is forbidden to get a predicted value for an endogenous dummy using a nonlinear model such as a probit/logit model and to plug this into a second-stage probit/logit model. This type of regression is called “forbidden regression,” “a phrase that describes replacing a nonlinear function of an endogenous explanatory variable with the same nonlinear function of fitted values from a first-stage estimation.” One example similar to our approach is the Oregon health insurance experiment study that used LPMs with IV estimation (Finkelstein et al., 2012). As the authors noted, “We estimate linear models even though a number of our outcomes are binary. Because we are interested in the difference in conditional means for the treatments and controls, linear probability models pose no concerns in the absence of covariates or in fully saturated models” (Finkelstein et al., 2012). Therefore, 2SLS using LPM is appropriate for this study. To qualify for WIC benefits, the eligible family income must be equal to or less than 185% of the FPL. However, if people participate in Temporary Assistance for Needy Families (TANF), SNAP, or Medicaid, they are automatically eligible for WIC even if their incomes exceed 185% of the FPL (Carlson & Neuberger, 2017). Although the federal income eligibility level for Medicaid is 133% of the FPL, with Medicaid expansion states can elevate the income thresholds up to 300% of the FPL (Sommers & Rosenbaum, 2011; CMCS, 2019). Therefore, there is not a clear cut-off income threshold to determine WIC eligibility. We performed the primary analysis with 230% of the FPL as the income eligibility cutoff point, which is in line with other low-income mother and infant studies (Dague, 2014; Leung et al., 2014), but conducted a robustness check using 185%, 200%, and 215% of the FPL, as well.
The full analytical sample included a total of 92,335 children who were born in the years from 2005 to 2014 into households with income below or equal to 230% of the FPL. We first conducted the descriptive analyses, then fit 2SLS models with the IVs in the whole sample. We then stratified the samples by gender and race/ethnicity and ran the models separately, because the relationship between WIC participation and breastfeeding may vary in different gender and racial/ethnic groups (Hurley et al., 2008; Sparks, 2011; Langellier et al., 2012; Metallinos-Katsaras et al., 2015). We compared the ordinary least square (OLS) estimates with the 2SLS estimates models. To better demonstrate the magnitude of the effect size, we estimated percentage change of breastfeeding probability due to one percent change in WIC participation probability at the mean of breastfeeding and WIC participation distributions.
To examine the validity of the IVs, we conducted the under-identification test, weak instrument test, and over-identification test. First, we formally assessed the relevance of the instruments by conducting an under-identification test based on the Kleibergen-Paap rank LM statistic (Kleibergen & Paap, 2006; Baum et al., 2007). The null hypothesis was that the model was under-identified, i.e., the instruments were not significantly correlated with the endogenous variable. Second, we checked whether the instruments were weak instruments, meaning the instruments were only weakly correlated with the endogenous variable. Stock-Yogo weak identification tests were conducted to further assess the strength of correlation between the instruments and the endogenous variables (Stock & Yogo, 2005). Finally, we tested the exogeneity of the instruments, i.e., the instruments were uncorrelated with the error process. This was assessed through an over-identification test. The null hypothesis was that all instruments were uncorrelated with the error term, based on the Sargan test statistic (Baum et al., 2007). In the result tables, we used U, W, or O to indicate whether the IVs passed the under-identification test, weak instrument test, and over-identification test.
4. Results
4.1. Summary statistics
Table 2 provides summary statistics for WIC-eligible children whose household income was equal to or less than 230% of the FPL. The participants and eligible non-participants did not differ significantly in gender and age groups, but differed significantly in other socio-demographics. Compared with eligible non-participants, WIC participants had a higher percentage of non-Hispanic black, 19.0% vs. 8.8%, and Hispanic participants, 40.3% vs. 20.3%, but a lower percentage of non-Hispanic whites, 31.1% vs. 59.6% (P < 0.001). Moreover, the participants’ mothers had significantly lower education and were less likely to be married (P < 0.001).
Table 2.
Summary Statistics of WIC-Eligible Children in the National Immunization Survey (NIS) Born in 2005–2014 (Income ≤ 230% of the FPL)
| WIC-Eligible Children (N = 92,335) | WIC-Eligible Participating Children (N = 71,757) | WIC-Eligible Non-Participating Children (N = 20,578) | |||||
|---|---|---|---|---|---|---|---|
| Variables | Weighted Percentage (%) or Mean | S. E. (%) | Weighted Percentage (%) or Mean | S. E. (%) | Weighted Percentage (%) or Mean | S. E. (%) | P-value† |
| Gender of Child | 0.7 | ||||||
| Boys | 51.0 | 0.3 | 50.9 | 0.3 | 51.2 | 0.6 | |
| Girls | 49.0 | 0.3 | 49.1 | 0.3 | 48.8 | 0.6 | |
| Race/Ethnicity | < 0.001 | ||||||
| Non-Hispanic White | 35.9 | 0.2 | 31.1 | 0.3 | 59.6 | 0.6 | |
| Non-Hispanic Black | 17.3 | 0.2 | 19.0 | 0.2 | 8.8 | 0.4 | |
| Hispanic | 36.9 | 0.3 | 40.3 | 0.3 | 20.3 | 0.5 | |
| Other | 9.9 | 0.2 | 9.6 | 0.2 | 11.3 | 0.4 | |
| Age Group | 0.2 | ||||||
| 19–23m | 28.5 | 0.3 | 28.6 | 0.3 | 28.3 | 0.5 | |
| 24–29m | 37.1 | 0.3 | 37.2 | 0.3 | 36.4 | 0.6 | |
| 30–35m | 34.4 | 0.3 | 34.2 | 0.3 | 35.3 | 0.6 | |
| Maternal Education | < 0.001 | ||||||
| < High School | 28.0 | 0.3 | 31.1 | 0.3 | 13.0 | 0.5 | |
| High School/GED | 38.0 | 0.3 | 39.3 | 0.3 | 31.1 | 0.6 | |
| Non-college graduate | 23.4 | 0.2 | 22.7 | 0.2 | 27.1 | 0.5 | |
| College graduate | 10.6 | 0.1 | 6.9 | 0.1 | 28.8 | 0.5 | |
| Age of Mother | < 0.001 | ||||||
| < 30 years | 54.1 | 0.3 | 57.2 | 0.3 | 39.2 | 0.6 | |
| ≥ 30 years | 45.9 | 0.3 | 42.8 | 0.3 | 60.8 | 0.6 | |
| Maternal Marital Status | < 0.001 | ||||||
| Married | 48.9 | 0.3 | 43.8 | 0.3 | 74.2 | 0.6 | |
| Non-married | 51.1 | 0.3 | 56.2 | 0.3 | 25.8 | 0.6 | |
| Interview Language | < 0.001 | ||||||
| English | 76.0 | 0.3 | 73.4 | 0.3 | 89.1 | 0.5 | |
| Spanish | 21.1 | 0.3 | 23.8 | 0.3 | 7.5 | 0.4 | |
| Other | 2.9 | 0.1 | 2.8 | 0.1 | 3.4 | 0.3 | |
| Number of Household Members | 4.7 | 0.01‡ | 4.7 | 0.01‡ | 4.8 | 0.02‡ | < 0.001 |
P-value was calculated based on Pearson’s Chi-squared test and T-test between the WIC-Eligible participating children and eligible non-participants Child.
In this line, the number presents the standard error other than the percentage of standard error.
4.2. First-stage results
Table 3 reports the first-stage regression results of the IVs for the WIC-eligible children (income ≤ 230% of the FPL) and the stratified subgroups by gender or race/ethnicity (See the results of the full models in Appendix Tables 2A and 2B.). The coefficients of the three instruments, “SNAP enrollment rates (SNAP),” “Square of SNAP enrollment rates (SNAP2),” and “SNAP Policy Index,” along with other exogenous variables, e.g., socio-demographics and state-level policy variables, were used to generate a fitted value of the endogenous variable, WIC participation, using OLS.
Table 3.
First-stage Estimates of Two-stage Least Square IV Estimation of WIC Participation on Breastfeeding Practice in a WIC-eligible Population (Income ≤ 230% of the FPL) †
| Variables | SNAP enrollment rates (SNAP) | Square of SNAP enrollment rates (SNAP2) | SNAP policy index | R2 | U-Stat (P-value) | W-stat (10% Cutoff Point) | Identification test‡ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coeff. | S. E | P-value | Coeff. | S.E | P-value | Coeff. | S.E | P-value | |||||
| ALL | 1.563 | 0.382 | < 0.001 | −4.513 | 1.221 | < 0.001 | 0.006 | 0.005 | 0.266 | 0.161 | 13.08 (< 0.01) | 15.36 (9.08) | UW |
| Boy | 0.754 | 0.488 | 0.124 | −2.554 | 1.504 | 0.091 | 0.017 | 0.007 | 0.010 | 0.162 | 4.20 (0.24) | 10.40 (9.08) | |
| Girl | 2.410 | 0.543 | < 0.001 | −6.578 | 1.591 | < 0.001 | −0.006 | 0.007 | 0.411 | 0.164 | 15.71 (< 0.01) | 12.49 (9.08) | UW |
| Non-H White | 1.054 | 0.572 | 0.066 | −2.984 | 1.783 | 0.096 | −0.009 | 0.010 | 0.353 | 0.170 | 4.27 (0.23) | 2.24 (9.08) | |
| Non-H Black | 1.756 | 0.620 | 0.005 | −5.784 | 1.781 | 0.001 | −0.006 | 0.009 | 0.527 | 0.059 | 10.13 (0.02) | 4.05 (9.08) | U |
| Hispanic | 1.322 | 0.769 | 0.087 | −4.330 | 2.218 | 0.052 | 0.019 | 0.007 | 0.009 | 0.066 | 3.84 (0.28) | 13.99 (9.08) | |
| Other | 3.019 | 1.072 | 0.005 | −6.133 | 3.289 | 0.064 | 0.011 | 0.016 | 0.499 | 0.138 | 9.77 (0.02) | 7.81 (9.08) | U |
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test: W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size.
As shown in Table 3, the coefficient of SNAP was 1.563 (SE = 0.382) in the whole sample analysis, indicating that a 1 percentage point increase in the state SNAP enrollment rate was associated with about a 1.5 percentage point increase in WIC participation. In the sub-sample analyses, we observed similar magnitude. The coefficients of SNAP2 were negative, which suggested a concave, nonlinear relationship between SNAP enrollment rate and WIC participation. The coefficients ranged from −2.554 to −6.578 in different samples. The coefficients of the SNAP Policy Index varied from −0.009 to 0.019, which suggests the SNAP policy may have varied effects on WIC participation in different socio-demographic samples.
In the first-stage regression, we used the under-identification test and weak instrument test to determine the relevance condition of our instruments, i.e., whether the whole set of instruments were sufficiently correlated with the endogenous variable, WIC participation. As shown in Table 3, the null hypothesis in the under-identification test was rejected in the whole sample, girls, non-Hispanic blacks, and other racial/ethnic groups (P < 0.05).
We used the Stock-Yogo approach to assess the possibility of weak instruments (Stock & Yogo, 2005). The null hypothesis is that instruments are weak and lead to an asymptotic relative bias greater than a certain threshold, e.g., 10% maximal relative bias (relative to the bias of OLS). As reported in Table 3, the weak instrument hypothesis was rejected in the first-stage regression based on the bias test at a cutoff of 10% maximal IV relative bias level in the Stock-Yogo tabulation (Stock & Yogo, 2005) for the entire sample and for girls. This means that the relative bias of the IV estimates with respect to OLS will be no more than 10% of the bias of OLS, indicating a sufficiently strong IV in these samples. As a robustness check, we tested the TANF enrollment rate and CHIP enrollment rate as alternative IVs, but neither candidate passed under-identification tests or weak instrument tests (results not shown).
4.3. Second-stage results
Table 4 lists the regression results of OLS estimation and second-stage IV model estimates with the under-identification test, weak instrument test, and over-identification test. The results from under-identification tests and weak instrument tests at the second-stage regression were the same as those from the first-stage regression. Over-identification tests were conducted based on the 2SLS estimates, which helps assess the exogeneity of our instruments, i.e., that the instruments are not correlated with the outcome variable of interest. The null hypothesis of the over-identification test is that the instruments are exogenous. As Table 4 reports, we could not reject the null that our instruments are exogenous in the whole sample and all sub-sample stratified analyses, which suggests the validity of the IV. Additional results with different income cut-off points are presented in Appendix Tables 3A, 3B, and 3C.
Table 4.
Second-stage Estimates of Two-stage Least Square IV Estimation of WIC Participation on Ever Breastfeeding in a WIC-eligible Population (Income ≤ 230% of the FPL) †
| OLS | IV: SNAP+SNAP2+SNAP policy index | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Coeff. | S. E | P-value | Elasticity estimate (at the mean of breastfeeding probability)†† | Coeff. | S. E | P-value | Elasticity estimate (at the mean of breastfeeding probability)†† | O-stat | P-value | Identification test‡ | |
| ALL | −0.064 | 0.007 | < 0.001 | −0.011 | 0.085 | 0.298 | 0.775 | 0.014 | 3.951 | 0.139 | UWO |
| Boy | −0.072 | 0.009 | < 0.001 | −0.012 | 0.444 | 0.384 | 0.247 | 0.075 | 4.332 | 0.115 | O |
| Girl | −0.057 | 0.009 | < 0.001 | −0.010 | −0.147 | 0.367 | 0.689 | −0.025 | 0.930 | 0.628 | UWO |
| Non-H White | −0.084 | 0.008 | < 0.001 | −0.014 | −0.425 | 0.532 | 0.424 | −0.070 | 5.863 | 0.053 | O |
| Non-H Black | −0.071 | 0.018 | < 0.001 | −0.017 | 0.506 | 0.679 | 0.456 | 0.118 | 0.590 | 0.745 | UO |
| Hispanic | −0.026 | 0.012 | 0.040 | −0.004 | 0.614 | 0.290 | 0.034 | 0.093 | 1.956 | 0.376 | O |
| Other | −0.042 | 0.016 | 0.011 | −0.007 | −0.146 | 0.500 | 0.771 | −0.024 | 2.330 | 0.312 | UO |
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
Elasticity estimates were obtained from the marginal effect estimates and the breastfeeding and WIC participation means using the elasticity formula.
U means under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic and used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size; O means over-identification test > 0.05.
The coefficients of WIC participation from the OLS and 2SLS (Table 4) represent the effect of WIC participation on the probability of breastfeeding. On the population level, it is equivalent to the effect of the WIC participation rate on the prevalence of breastfeeding. As Table 4 shows, OLS estimates suggested that WIC participation was negatively associated with breastfeeding probability. For example, in the whole sample analysis, the estimate suggested that a one percent point increase in the WIC participation rate was associated with a 0.064 percent point decrease in the breastfeeding prevalence. If we compare the OLS estimates with the IV estimates, we can see that the IV estimates either became positive or their magnitudes increased. This is known as the attenuation bias in OLS estimates due to endogeneity (Wooldridge, 2010). The plausible explanation is that there are unobservable characteristics that are correlated with the endogenous variable, WIC participation, therefore the OLS estimates are biased (Wooldridge, 2010).
In addition, we estimated percentage change of breastfeeding probability due to a one percentage change in WIC participation probability at the mean of breastfeeding and WIC participation distributions (e.g., Jaffe, 1989). Such an effect estimate was reported as an elasticity estimate (at the mean of breastfeeding probability) in Table 4, which was obtained from the marginal effect estimates, the means of the breastfeeding, and the means of WIC participation. The magnitude of these elasticity estimates ranged from 0.014 (the whole sample) to 0.118 (non-Hispanic black), indicating that a 1% increase in WIC participation rate at the mean was associated with about 0.014% to 0.118% change in breastfeeding rates (the direction depends on the sign).
However, we should not overinterpret the magnitude of the estimates and should notice that OLS estimates of WIC participation effects were statistically significant, but the corresponding 2SLS estimates became statistically non-significant. This pattern is consistent in the whole sample and sub-sample analyses, in which OLS estimates suggested a statistically significant negative association between WIC participation and breastfeeding (e.g., boys: Coeff. = −0.072, P < 0.001), while IV estimates suggested that WIC participation was not significantly associated with breastfeeding probability in all groups, except in Hispanics (Coeff. = 0.614, P = 0.034).
In summary, the significantly negative relationship between WIC participation and breastfeeding can be caused by selection bias, and the results of this finding were robust across gender or racial/ethnic groups with extensive model checking.
4.4. Robustness checks
We conducted the robustness check using the sample of children whose family income was at or below 185%, 200%, and 215% of the FPL (Appendix Tables 3A, 3B, and 3C). As in the primary models, the OLS estimates were significantly negative in all groups, except in Hispanics (≤ 200% of the FPL) and in Hispanics and others (≤ 185% of the FPL), indicating that WIC participation was negatively associated with ever-breastfeeding in most gender and racial/ethnic groups without controlling for endogeneity. With the IV approach, no models generated any significantly negative coefficients of WIC participation across gender and racial/ethnic groups, regardless of the income-cutoff points. Our IVs performed reasonably well in some samples, e.g., the whole sample and girls, and the generalizability of our estimates are not specific to certain income thresholds.
5. Policy Implication
Encouraging breastfeeding is one of the most important missions for WIC. However, due to the availability of formula in the food package, the relationship of WIC participation and breastfeeding has been uncertain. The question is critical for policy makers and researchers to understand, but its answer remains inconclusive given the existence of endogeneity issues in WIC participation. The existing national studies have had the limitation of small sample size, and only one of them (Li et al., 2019) has included any data after the 2009 WIC revision, which was the most important WIC policy change in four decades (Jiang et al., 2010; Martin-Anderson et al., 2013; Bullinger et al., 2016; Gregory et al., 2016; Topolyan & Xu, 2017; Li et al., 2019).
To fill in this significant knowledge gap, this study included 92,335 children from the NIS data, the official data used for the National Breastfeeding Report. We applied the IV approach to examine the relationship between WIC participation and breastfeeding in the post-2009 WIC revision. The results not only confirmed the lower ever-breastfeeding prevalence among WIC participants compared with non-WIC participants, as in our previous study (Zhang et al., 2019), but also indicated that the worse breastfeeding outcomes can be related to the self-selection bias in WIC participation. Moreover, with alternative model specifications, the relationship between WIC participation and breastfeeding can turn from significantly negative to statistically no different from zero. One earlier study used different nationally representative data (NHANES) with an alternative method (propensity score) of controlling for the endogeneity of the WIC participation, but found similar results: WIC participation was not significantly negatively related to ever-breastfeeding after the 2009 WIC revision (Li et al., 2019). Therefore, this study adds more conclusive evidence to a long-term debate on the relationship between WIC participation and breastfeeding. Our results support the neutrality of the WIC program in ever-breastfeeding after controlling for self-selection bias, which is important for policy makers and researchers to know.
The self-selection bias identified in this study echoes the literature stating that economic incentives can influence mothers’ feeding choices and decisions, especially among low-income mothers (Phelps, 2011; Fornasaro-Donahue et al., 2014). However, weighing the benefits of formula or breastfeeding may be influenced by other WIC program factors as well (Jensen, 2012). For example, since WIC is federally funded but operated at the state level, there are variations in the food benefits provided. Varying food costs across states and non-formula food products included in the benefit packages at the state level can influence the participants’ redemption preference and behaviors (Zhang et al., 2017). All these state variations can influence WIC mothers’ perceptions and decisions about breastfeeding initiation and duration (Jensen, 2012). The process of controlling for self-selection in WIC participation needs to consider these state variations.
Our study suggests a new route to identify an IV for WIC participation. Although the IV method is a valid approach to address endogeneity, existing literature has rarely used any IVs to account for the endogeneity of WIC participation in studying the relationship with breastfeeding (Bullinger et al., 2016). The state SNAP enrollment rate and SNAP policy indices reflect the welfare policy and program operation in that state, which is likely to influence WIC participation, although the state SNAP characteristics do not have a direct impact on breastfeeding (Ganong & Liebman, 2018). By controlling multiple state-level policy variables, our results reflect the national average relationship between WIC participation and breastfeeding while controlling for state variation and endogeneity. The stratified analyses indicated that the IV model may fit some socio-demographic groups better than others. For example, the IV approach was more robust in girls and in non-Hispanic black children.
A few limitations of the study are worth noting. First, given the survey method, we could only target a specific age range (19m-35m) in this study, and we were unable to know exactly when mothers participated in the program, which could affect their breastfeeding decisions. Moreover, the public-use data does not have the exact birth year, so we could only use the age group to infer the birth cohorts. This approach works well to infer the ever-breastfeeding status but does not work for the other breastfeeding statuses. Therefore, we can only use the one breastfeeding outcome, although this is the most-used breastfeeding indicator in most breastfeeding reports and studies. Another limitation of the NIS data is that we could not fully measure the impact of the WIC program on individual breastfeeding status. For example, based on the participants’ self-reported breastfeeding status, WIC agencies certify the participants to receive specific packages (fully breastfeeding, partial breastfeeding, and formula feeding). Therefore, the choice of the package depends on the self-reported breastfeeding status, and the expectation of receiving certain packages (e.g., formula) may distort participants’ reporting on breastfeeding status (Jensen, 2012). However, the NIS does not provide specific package information. Except for package differences, WIC provides comprehensive breastfeeding support programs, which were also not reported in the NIS data (USDA, 2020g). To the best of our knowledge, no national data has that level of detailed information, so we can only acknowledge this as a limitation. Finally, we used the state SNAP policy variable as the candidate for the IV, which could itself depend on other exogeneous variables. But little research has been conducted to examine how these exogeneous variables may affect the breastfeeding outcomes of WIC-eligible participants. Even with these limitations, this study still generates important and conclusive results for WIC policy makers and researchers in the field.
6. Conclusion
This study used a large nationally representative data set and valid IVs to examine the relationship between WIC participation and breastfeeding among low-income children born in 2005–2014. The results have important policy implications: First, the study confirms the neutrality of the WIC program on participants’ breastfeeding outcomes at the national level across a long study period. It is important for policy makers and the WIC agencies to be able to respond to potential challenges to the formula availability policy, since at least the WIC program does not worsen breastfeeding outcomes, as our results indicated. Second, self-selection bias appears to be a strong factor for participation in WIC, which could be a potential target for intervention in the future. In addition to traditional health education, other innovative methods like behavioral economics can be employed to nudge the preset attitude towards WIC and therefore improve attitudes toward breastfeeding among these participants (Hansen, 2016). Last but not least, even when controlling the self-selection bias, breastfeeding disparities across gender and race/ethnicity still exist. Therefore, more research is needed to understand these disparities so effective policies can be adopted to reduce them.
Highlights.
New instrumental variable for WIC participation with vigorous testings
WIC participation not a significant predictor for low breastfeeding with IV
Large national data with long period to study WIC participation and breastfeeding
Acknowledgments
This work is supported by the National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD090387-01) and the US Department of Agriculture/Economic Research Service (#58-4000-8-0038-R; #58-4000-6-0061-R). The findings and conclusions in this presentation are those of the author and should not be construed to represent any official USDA or U.S. government determination or policy.
Appendix B: Ideal vs. Practical Strategy to Identify Instrumental Variable for WIC Participation
The ideal IV may only affect WIC participation but not affect the breastfeeding outcome. However, as pointed out in this paper, the ideal IV may not be realistic to measure. We tested the SNAP policy index only, which was promising conceptually, but the results indicated that none of the policy index passed the identification tests (see Appendix Table 4). Therefore, the state SNAP enrollment rate + SNAP policy index serve as a practical choice of IV identification. One limitation is that the SNAP enrollment rate may depend on other factors, such as unemployment rate, which may or may not affect the WIC-eligible population’s breastfeeding outcome. Without conclusive evidence in the literature, it is challenging to invalidate the SNAP enrollment rate as a possible IV.
Moreover, given the systematic thinking, any possible IV candidate may be dependent on some other variables. Without a clear boundary, researchers can fall into the “salami slicing dilemma” that identifies one variable after another variable that may be related to breastfeeding. Without knowing where to stop the salami slicing, we may conclude that all “exogenous” IVs may be endogenous eventually. This paper proposes the state SNAP enrollment rate not as an ideal IV for WIC participation, but a practical IV as a starting point of a long journey to identify better IVs for WIC participation. Given no valid IV in this field, our solution provides a breakthrough for researchers to think about alternative strategies to identify the IVs for WIC participation.
Appendix Table 1. Factors associated with WIC vs. SNAP participation across the levels of the social–ecological model.
| SNAP Factors (Pinard et al., 2017) | SNAP References (Pinard et al., 2017) (+/−) | WIC Factors | WIC (+/−) | WIC References | |
|---|---|---|---|---|---|
| Macrolevel Approaches | |||||
| Society level | Higher unemployment and poverty rates | + | Higher unemployment and poverty rates | + | Bitler et al, 2003; Carlson et al., 2017 |
| Strong economy | − | Strong economy | − | Carlson et al., 2017 | |
| Federal/state policy level | Broad-based categorical eligibility standards | + | N/A | ||
| Align SNAP policy with TANF and Medicaid | + | Adjunct eligibility for participants in SNAP, Medicaid, TANF | + | Carlson et al., 2017 | |
| Simplified enrollment and reporting | + | Difficult paperwork | − | NASEM, 2017 | |
| Shorter recertification periods | + | Shorter recertification period | + | Ver Ploeg et al., 2003 | |
| Lengthier application | − | Long waiting time | − | NASEM, 2017 | |
| Stricter verification and recertification | − | Unknown | |||
| Community/organizational level | Greater availability of state assistance offices | + | Local WIC agencies per 100 residents | +/− | Bitler et al., 2003 |
| Increased outreach | + | Program outreach | +/− | Ku, 1989;Lanese et al.,2018 | |
| High housing and utility costs | + | Unknown | |||
| Lack of transportation | − | NASEM, 2017 | |||
| Enhancing customer services for participants | + | Christie et al., 2006; NASEM, 2017 | |||
| Microlevel Approaches | |||||
| Household level | Single parent | + | Married | − | Jensen, 2012 |
| Increased number of children in a household | + | Increased number of children in a household | + | Kahler et al., 1992 | |
| Higher incomes and available assets | − | Income level increase | − | Gilbert et al., 2014 | |
| Individual level | Persons with disability | + | Unknown | ||
| Receiving other federal assistance benefits | + | Receiving other federal assistance benefits | +/− | Bitler et al., 2003; Gilbert et al., 2014 | |
| Lower levels of education | + | Lower levels of education | + | Smith, 2016 | |
| Job loss | + | Job loss | + | Smith, 2016 | |
| Age, in particular the elderly | − | Increasing maternal age | − | Gilbert et al., 2014 | |
| Race/ethnicity, in particular Hispanic | − | Race/ethnicity (Hispanic & Black) | + | Liu and Liu, 2016 | |
| Perceived stigma | − | Perceived stigma | − | Powell, 2015 | |
| Working full-time during nontraditional hours | − | Unknown | |||
| Working more than one job | − | Unknown | |||
| Lack of knowledge, motivation, or confidence in how to apply | − | Lack of knowledge | − | Gilbert et al., 2014; NASEM, 2017 | |
| Citizenship status (lack) | − | Citizenship status (lack) / Immigrants | − | Vargas and Pirog, 2016 | |
| Mothers reporting unplanned pregnancies | − | Liu and Liu, 2016 |
Note 1: SNAP indicates Supplemental Nutrition Assistance Program; TANF, Temporary Assistance for Needy Families; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Note 2: The direction of the relationship is described by +/− with +: related to an increase in SNAP or WIC participation and −: related to a decrease in SNAP or WIC participation.
Appendix Table 2A. First-stage Estimates of Two-stage Least Square IV Estimation (Full Model) of WIC Participation in a WIC-eligible Population (Income ≤ 230% of the FPL, model results of all sample and by gender group) †(Dependent Variable WIC participation)
| By Gender | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | All | Boy | Girl | ||||||
| Coeff. | S. E | P-value | Coeff. | S. E | P-value | Coeff. | S. E | P-value | |
| SNAP | 1.563 | 0.382 | < 0.001 | 0.754 | 0.488 | 0.124 | 2.410 | 0.543 | < 0.001 |
| SNAP2 | −4.513 | 1.221 | < 0.001 | −2.554 | 1.504 | 0.091 | −6.578 | 1.591 | < 0.001 |
| SNAP policy index | 0.006 | 0.005 | 0.266 | 0.017 | 0.007 | 0.010 | −0.006 | 0.007 | 0.411 |
| Number of Household Members | −0.005 | 0.001 | < 0.001 | −0.005 | 0.002 | 0.005 | −0.005 | 0.002 | 0.002 |
| Gender of Child | |||||||||
| Boys | Ref | Ref | Ref | - | - | - | - | - | - |
| Girls | < 0.001 | 0.003 | 0.979 | - | - | - | - | - | - |
| Race/Ethnicity | |||||||||
| Non-Hispanic White | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Non-Hispanic Black | 0.136 | 0.006 | < 0.001 | 0.133 | 0.007 | < 0.001 | 0.140 | 0.008 | < 0.001 |
| Non-Hispanic Black | 0.109 | 0.008 | < 0.001 | 0.106 | 0.009 | < 0.001 | 0.113 | 0.012 | < 0.001 |
| Other | 0.068 | 0.007 | < 0.001 | 0.063 | 0.011 | < 0.001 | 0.073 | 0.010 | < 0.001 |
| Maternal Education | |||||||||
| < High School | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| High School/GED | −0.023 | 0.004 | < 0.001 | −0.010 | 0.007 | 0.150 | −0.036 | 0.006 | < 0.001 |
| Non-college graduate | −0.064 | 0.005 | < 0.001 | −0.053 | 0.007 | < 0.001 | −0.075 | 0.007 | < 0.001 |
| College graduate | −0.268 | 0.010 | < 0.001 | −0.264 | 0.011 | < 0.001 | −0.271 | 0.014 | < 0.001 |
| Age Group | |||||||||
| 19–23m | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 24–29m | < 0.001 | 0.004 | 0.866 | 0.004 | 0.006 | 0.419 | −0.003 | 0.006 | 0.565 |
| 30–35m | −0.005 | 0.004 | 0.183 | −0.003 | 0.006 | 0.643 | −0.008 | 0.006 | 0.174 |
| Age of Mother | |||||||||
| ≥ 30 years | −0.061 | 0.005 | < 0.001 | −0.054 | 0.005 | < 0.001 | −0.068 | 0.007 | < 0.001 |
| < 30 years | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Marital Status of Mother | |||||||||
| Married | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Non-married | 0.102 | 0.005 | < 0.001 | 0.107 | 0.007 | < 0.001 | 0.097 | 0.007 | < 0.001 |
| Interview Language | |||||||||
| English | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Spanish | 0.072 | 0.008 | < 0.001 | 0.078 | 0.008 | < 0.001 | 0.065 | 0.013 | < 0.001 |
| Other language | 0.028 | 0.015 | 0.068 | 0.021 | 0.020 | 0.298 | 0.034 | 0.018 | 0.060 |
| Birth Year | −0.003 | 0.001 | 0.021 | −0.004 | 0.002 | 0.090 | −0.003 | 0.002 | 0.194 |
| Unemployment Rate | 0.002 | 0.001 | 0.123 | 0.003 | 0.002 | 0.236 | 0.002 | 0.001 | 0.267 |
| TANF Enrollment Rate | −0.878 | 0.621 | 0.159 | −1.404 | 0.933 | 0.134 | −0.323 | 0.744 | 0.664 |
| CHIP Enrollment Rate | −0.135 | 0.127 | 0.292 | 0.055 | 0.150 | 0.714 | −0.331 | 0.192 | 0.086 |
| _cons | 0.731 | 0.061 | < 0.001 | 0.664 | 0.069 | < 0.001 | 0.800 | 0.065 | < 0.001 |
| R2 | 0.161 | 0.162 | 0.164 | ||||||
| Identification test‡ | UW | UW | |||||||
Controlling state dummy (the results of State variables were not included in this table), sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size.
Appendix Table 2B: First-stage Estimates of Two-stage Least Square IV Estimation (Full Model) of WIC Participation on Breastfeeding Practice in a WIC-eligible Population (Income ≤ 230% of the FPL, model results of by race group) †
| By race/ethnicity | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-H White | Non-H Black | Hispanic | Other | ||||||||||
| Variables | Coeff. | S. E | P-value | Coeff. | S. E | P-value | Coeff. | S. E | P-value | Coeff. | S. E | P-value | |
| SNAP | 1.054 | 0.572 | 0.066 | 1.756 | 0.620 | 0.005 | 1.322 | 0.769 | 0.087 | 3.019 | 1.072 | 0.005 | |
| SNAP2 | −2.984 | 1.783 | 0.096 | −5.784 | 1.781 | 0.001 | −4.330 | 2.218 | 0.052 | −6.133 | 3.289 | 0.064 | |
| SNAP policy index | −0.009 | 0.010 | 0.353 | −0.006 | 0.009 | 0.527 | 0.019 | 0.007 | 0.009 | 0.011 | 0.016 | 0.499 | |
| Number of Household Members | −0.008 | 0.002 | < 0.001 | −0.003 | 0.003 | 0.312 | < 0.001 | 0.003 | 0.775 | −0.002 | 0.003 | 0.489 | |
| Gender of Child | |||||||||||||
| Boys | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| Girls | −0.005 | 0.006 | 0.362 | −0.001 | 0.007 | 0.860 | 0.004 | 0.005 | 0.456 | 0.006 | 0.014 | 0.662 | |
| Maternal Education | |||||||||||||
| < High School | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| High School/GED | −0.030 | 0.012 | 0.009 | −0.011 | 0.009 | 0.244 | −0.020 | 0.006 | 0.001 | −0.026 | 0.014 | 0.054 | |
| Non-college | |||||||||||||
| Graduate | −0.077 | 0.011 | < 0.001 | −0.031 | 0.013 | 0.016 | −0.061 | 0.008 | < 0.001 | −0.063 | 0.015 | < 0.001 | |
| College graduate | −0.313 | 0.014 | < 0.001 | −0.145 | 0.020 | < 0.001 | −0.192 | 0.016 | < 0.001 | −0.261 | 0.022 | < 0.001 | |
| Age Group | |||||||||||||
| 19–23m | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| 24–29m | −0.003 | 0.008 | 0.714 | 0.009 | 0.010 | 0.382 | −0.001 | 0.006 | 0.828 | 0.003 | 0.014 | 0.825 | |
| 30–35m | −0.010 | 0.008 | 0.215 | −0.003 | 0.009 | 0.706 | −0.004 | 0.006 | 0.470 | −0.005 | 0.015 | 0.761 | |
| Age of Mother | |||||||||||||
| ≥ 30 years | −0.111 | 0.007 | < 0.001 | −0.027 | 0.006 | < 0.001 | −0.022 | 0.005 | < 0.001 | −0.087 | 0.015 | < 0.001 | |
| < 30 years | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| Marital Status of Mother | |||||||||||||
| Married | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| Non-married | 0.165 | 0.007 | < 0.001 | 0.067 | 0.009 | < 0.001 | 0.051 | 0.006 | < 0.001 | 0.123 | 0.016 | < 0.001 | |
| Interview Language | |||||||||||||
| English | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| Spanish | 0.123 | 0.045 | 0.007 | −0.015 | 0.071 | 0.828 | 0.062 | 0.007 | < 0.001 | −0.022 | 0.069 | 0.750 | |
| Other Language | 0.101 | 0.039 | 0.010 | 0.030 | 0.026 | 0.247 | −0.033 | 0.065 | 0.609 | 0.015 | 0.025 | 0.542 | |
| Birth Year | −0.001 | 0.003 | 0.912 | −0.002 | 0.003 | 0.577 | −0.005 | 0.003 | 0.095 | −0.012 | 0.004 | 0.002 | |
| Unemployment Rate | 0.010 | 0.002 | < 0.001 | −0.001 | 0.002 | 0.974 | < 0.001 | 0.002 | 0.990 | −0.006 | 0.005 | 0.231 | |
| TANF Enrollment Rate | 0.131 | 1.085 | 0.904 | −1.568 | 1.108 | 0.159 | −1.249 | 1.048 | 0.235 | −2.309 | 1.942 | 0.236 | |
| CHIP Enrollment Rate | −0.490 | 0.169 | 0.004 | −0.252 | 0.260 | 0.334 | −0.012 | 0.133 | 0.929 | 0.480 | 0.332 | 0.150 | |
| _cons | 0.964 | 0.092 | < 0.001 | 0.923 | 0.074 | < 0.001 | 0.681 | 0.089 | < 0.001 | 0.681 | 0.127 | < 0.001 | |
| R2 | 0.170 | 0.059 | 0.066 | 0.138 | |||||||||
| Identification test‡ | U | U | |||||||||||
Controlling state dummy (the results of State variables were not included in this table), sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size.
Appendix Table 3A. Robustness Check of the WIC Participation Status on Breastfeeding among NIS Children with Household Income ≤ 185% of the FPL†
| OLS | IV: SNAP+ SNAP2+SNAP policy index | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Coeff. of WIC participation | S. E | P-value | Coeff. of WIC participation | S. E | P-value | Identification test‡- |
| ALL | −0.063 | 0.008 | < 0.001 | −0.039 | 0.322 | 0.902 | O |
| Boy | −0.069 | 0.010 | < 0.001 | 0.347 | 0.402 | 0.388 | O |
| Girl | −0.059 | 0.011 | < 0.001 | −0.302 | 0.512 | 0.556 | UWO |
| Non-H White | −0.091 | 0.010 | < 0.001 | 0.680 | 1.089 | 0.533 | O |
| Non-H Black | −0.052 | 0.021 | 0.015 | 0.675 | 0.811 | 0.405 | UO |
| Hispanic | −0.024 | 0.014 | 0.087 | 0.543 | 0.283 | 0.055 | O |
| Other | −0.038 | 0.020 | 0.061 | −0.211 | 0.420 | 0.616 | UWO |
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size. O means over-identification test > 0.05.(O could not be tested in the first stage).
Appendix Table 3B. Robustness Check of the WIC Participation Status on Breastfeeding among NIS Children with Household Income ≤ 200% of the FPL†
| OLS | IV: SNAP+ SNAP2+SNAP policy index | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Coeff. of WIC participation | S. E | P-value | Coeff. of WIC participation | S. E | P-value | Identification test‡ |
| ALL | −0.064 | 0.007 | < 0.001 | −0.102 | 0.335 | 0.761 | UWO |
| Boy | −0.071 | 0.010 | < 0.001 | 0.262 | 0.373 | 0.482 | O |
| Girl | −0.059 | 0.009 | < 0.001 | −0.259 | 0.425 | 0.542 | UWO |
| Non-H White | −0.092 | 0.009 | < 0.001 | −0.361 | 0.724 | 0.618 | O |
| Non-H Black | −0.063 | 0.021 | 0.003 | 0.364 | 0.672 | 0.588 | UO |
| Hispanic | −0.021 | 0.012 | 0.077 | 0.547 | 0.309 | 0.077 | O |
| Other | −0.037 | 0.018 | 0.040 | −0.069 | 0.424 | 0.871 | UWO |
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test: W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size. O means over-identification test > 0.05. (O could not be tested in the first stage).
Appendix Table 3C. Robustness Check of the WIC Participation Status on Breastfeeding among NIS Children with Household Income ≤ 215% of the FPL†
| OLS | IV: SNAP+ SNAP2+SNAP policy index | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Coeff. of WIC participation | S.E | P-value | Coeff. of WIC participation | S.E | P-value | Identification test‡ |
| ALL | −0.064 | 0.007 | < 0.001 | 0.018 | 0.318 | 0.956 | UWO |
| Boy | −0.072 | 0.009 | < 0.001 | 0.374 | 0.386 | 0.332 | O |
| Girl | −0.057 | 0.009 | < 0.001 | −0.266 | 0.443 | 0.549 | UWO |
| Non-H White | −0.087 | 0.008 | < 0.001 | −0.403 | 0.925 | 0.663 | O |
| Non-H Black | −0.069 | 0.019 | <0.001 | 0.365 | 0.659 | 0.580 | UO |
| Hispanic | −0.025 | 0.012 | 0.030 | 0.590 | 0.287 | 0.040 | O |
| Other | −0.035 | 0.017 | 0.047 | −0.108 | 0.458 | 0.814 | UO |
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate. IV Variables including SNAP enrollment rates (SNAP, # of SNAP participants in that year/# of state population in that year), square of SNAP enrollment rates (SNAP2), and SNAP policy index.
U means the under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic were used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size. O means over-identification test > 0.05. (O could not be tested in the first stage).
Appendix Table 4. IV Test Results (IV Variables Including SNAP Policy Index Only) †
| First-stage | Second-stage | IV Test Results (U: Under-identification Test W: Weak Instrument Test O: Over-identification Test)‡ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | 1st Stage Regression Coeff. | SE | P-value | R2 | U-Stat | P-value | W-stat | 10% Cutoff Point | O-stat | P-value | |
| SNAP Policy Index | 0.010 | 0.006 | 0.101 | 0.161 | 1.89 | 0.17 | 15.20 | 16.38 | NA | NA | |
| Eligibility | 0.011 | 0.006 | 0.063 | 0.161 | 3.38 | 0.07 | 9.71 | 16.38 | NA | NA | |
| Transaction | 0.043 | 0.022 | 0.050 | 0.161 | 2.18 | 0.14 | 26.20 | 16.38 | NA | NA | |
| Stigma | 0.001 | 0.014 | 0.942 | 0.161 | 0.01 | 0.94 | 0.04 | 16.38 | NA | NA | |
| Outreach | −0.296 | 0.184 | 0.109 | 0.161 | 2.27 | 0.13 | 6.53 | 16.38 | NA | NA | |
| Combination 1 | 0.161 | 4.46 | 0.11 | 17.90 | 19.93 | 0.217 | 0.642 | O | |||
| Eligibility | 0.011 | 0.006 | 0.058 | ||||||||
| Transaction | 0.043 | 0.021 | 0.047 | ||||||||
| Combination 2 | 0.161 | 3.39 | 0.18 | 4.86 | 19.93 | 0.006 | 0.939 | O | |||
| Eligibility | 0.011 | 0.006 | 0.063 | ||||||||
| Stigma | 0.000 | 0.014 | 0.977 | ||||||||
| Combination 3 | 0.161 | 4.69 | 0.10 | 7.35 | 19.93 | 0.526 | 0.468 | O | |||
| Eligibility | 0.011 | 0.006 | 0.082 | ||||||||
| Outreach | −0.260 | 0.185 | 0.160 | ||||||||
| Combination 4 | 0.161 | 3.59 | 0.17 | 13.45 | 19.93 | 0.012 | 0.912 | O | |||
| Transaction | 0.044 | 0.021 | 0.039 | ||||||||
| Stigma | −0.004 | 0.011 | 0.694 | ||||||||
| Combination 5 | 0.161 | 2.74 | 0.25 | 15.56 | 19.93 | 1.105 | 0.293 | O | |||
| Transaction | 0.042 | 0.021 | 0.046 | ||||||||
| Outreach | −0.258 | 0.157 | 0.102 | ||||||||
| Combination 6 | 0.161 | 2.43 | 0.30 | 3.27 | 19.93 | <0.001 | 0.996 | O | |||
| Stigma | 0.001 | 0.014 | 0.967 | ||||||||
| Outreach | −0.296 | 0.181 | 0.104 | ||||||||
| Combination 7 | 0.161 | 5.51 | 0.14 | 12.25 | 9.08 | 0.277 | 0.871 | O | |||
| Eligibility | 0.012 | 0.006 | 0.055 | ||||||||
| Transaction | 0.044 | 0.021 | 0.037 | ||||||||
| Stigma | −0.005 | 0.011 | 0.640 | ||||||||
| Combination 8 | 0.161 | 4.88 | 0.18 | 13.14 | 9.08 | 1.169 | 0.557 | O | |||
| Eligibility | 0.011 | 0.006 | 0.075 | ||||||||
| Transaction | 0.042 | 0.021 | 0.043 | ||||||||
| Outreach | −0.222 | 0.159 | 0.165 | ||||||||
| Combination 9 | 0.161 | 3.87 | 0.28 | 10.64 | 9.08 | 1.161 | 0.560 | O | |||
| Transaction | 0.043 | 0.020 | 0.036 | ||||||||
| Stigma | −0.005 | 0.011 | 0.674 | ||||||||
| Outreach | −0.260 | 0.158 | 0.102 | ||||||||
Controlling state dummy, sex, race/ethnicity, education, child’s age, maternal age, maternal marital status, number of people in the household, interview language, birth year, TANF/Temporary Assistance for Needy Families enrollment rate (# of enrolled participants/# of state population), CHIP/Children’s Health Insurance Program enrollment rate (# of enrolled children/# of children 18 or under in the state), and state unemployment rate.
U means under-identification test P < 0.05. Stock–Yogo tabulations based on the Cragg–Donald statistic and used for the weak identification test; W means the F statistic of the weak identification test > 10% maximal IV relative bias or > 10% maximal IV size; O means over-identification test > 0.05.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of Interest: None.
Declaration of Competing Interests
The authors declare that they have no competing interests that could influence this paper.
Appendix A: Supplemental Materials
Supplemental data and codes associated with this article can be found at https://figshare.com/s/8ce12706789c847869c4.
References
- Abaluck J, Gruber J, 2011. Choice inconsistencies among the elderly: Evidence from plan choice in the Medicare Part D program. Am. Econ. Rev, 101(4), 1180–1210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aguiar M, Hurst E, Karabarbounis L, 2013. Time use during the great recession. Am. Econ. Rev, 103(5), 1664–96. [Google Scholar]
- Angrist J, 2001. Estimation of limited dependent variable models with dummy endogenous regressors: Simple strategies for empirical practice. J. Bus. Econ. Stat, 19(1), 2–28. [Google Scholar]
- Angrist JD, Pischke JS, 2008. Mostly harmless econometrics: An empiricist’s companion, Princeton University Press. [Google Scholar]
- Baum CF, Schaffer ME, Stillman S, 2007. Enhanced routines for instrumental variables/generalized method of moments estimation and testing. Stata. J, 7(4), 465–506. [Google Scholar]
- Bitler MP, Currie J, 2005. Does WIC work? The effects of WIC on pregnancy and birth outcomes. J. Policy. Anal. Manage, 24(1), 73–91. [DOI] [PubMed] [Google Scholar]
- Bullinger LR, Gurley-Calvez T, 2016. WIC participation and maternal behavior: Breastfeeding and work leave. Contemp. Econ. Policy, 34(1), 158–172. [Google Scholar]
- Burstein NR, et al. , 2000. WIC General Analysis Project: Profile of WIC Children. Abt Associates. https://fns-prod.azureedge.net/sites/default/files/profile.pdf (retrieved on 02.19.2020). [Google Scholar]
- Carlson S, Neuberger Z, 2017. WIC works: Addressing the nutrition and health needs of low-income families for 40 years. Center on Budget and Policy Priorities. https://www.cbpp.org/research/food-assistance/wic-works-addressing-the-nutrition-and-health-needs-of-low-income-families (retrieved on 02.08.2019). [Google Scholar]
- Castner L, Mabli J, Sykes J, 2009. Dynamics of WIC Program Participation by Infants and Children, 2001 to 2003. Final Report. Mathematica Policy Research, Inc. https://files.eric.ed.gov/fulltext/ED505595.pdf (retrieved on 02.19.2020). [Google Scholar]
- Centers for Disease Control and Prevention (CDC), 2018. About the National Immunization Surveys (NIS). https://www.cdc.gov/vaccines/imz-managers/nis/about.html (retrieved on 02.08.2019).
- Centers for Disease Control and Prevention (CDC), 2020. Breastfeeding Report Card. https://www.cdc.gov/breastfeeding/data/reportcard.htm (retrieved on 02.08.2020).
- Center for Medicaid and CHIP Services (CMCS), 2019. Medicaid Eligibility. https://www.medicaid.gov/medicaid/eligibility/index.html (retrieved on 02.08.2019).
- Dague L, 2014. The effect of Medicaid premiums on enrollment: A regression discontinuity approach. J. Health Econ, 37, 1–12. [DOI] [PubMed] [Google Scholar]
- Finkelstein A, et al. , 2012. The Oregon health insurance experiment: Evidence from the first year. Q. J. Econ, 127(3), 1057–1106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Food Research & Action Center (FRAC), 2019. Making WIC Work Better: Strategies to Reach More Women and Children and Strengthen Benefits Use. https://frac.org/wp-content/uploads/Making-WIC-Work-Better-Full-Report.pdf. (retrieved on 12.07.2020).
- Fornasaro-Donahue VM, Tovar A, Sebelia L, Greene GW, 2014. Increasing breastfeeding in WIC participants: Cost of formula as a motivator. J. Nutr. Educ. Behav, 46(6), 560–569. [DOI] [PubMed] [Google Scholar]
- Ganong P, Liebman JB, 2018. The decline, rebound, and further rise in SNAP enrollment: Disentangling business cycle fluctuations and policy changes. Am. Econ. J. Econ. Policy, 10(4), 153–76. [Google Scholar]
- Grabowski DC, Feng Z, Hirth R, Rahman M, Mor V, 2013. Effect of nursing home ownership on the quality of post-acute care: An instrumental variables approach. J. Health Econ, 32(1), 12–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gregory EF, Gross SM, Nguyen TQ, Butz AM, Johnson SB, 2016. WIC participation and breastfeeding at 3 months postpartum. Matern. Child. Health. J, 20(8), 1735–1744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- H.R. 24 – 101st Congress, 1989. Child Nutrition and WIC Reauthorization Act of 1989. https://www.govtrack.us/congress/bills/101/hr24 (retrieved on 02.08.2019).
- H.R. 8 – 103rd Congress, 1993. Healthy Meals for Healthy Americans Act of 1994. https://www.govtrack.us/congress/bills/103/hr8 (retrieved on 02.08.2019).
- Hansen K, 2016. Breastfeeding: A smart investment in people and in economies. Lancet, 387(10017), 416. [DOI] [PubMed] [Google Scholar]
- Heckman JJ, Smith JA, 2004. The determinants of participation in a social program: Evidence from a prototypical job training program. J. Labor Econ, 22(2), 243–298. [Google Scholar]
- Hoag S et al. , 2011. Children’s Health Insurance Program: An Evaluation (1997–2020): Interim Report to Congress. https://aspe.hhs.gov/system/files/pdf/76386/index.pdf (retrieved on 02.24.2020).
- Hoynes H, Schanzenbach DW, 2015. US food and nutrition programs. In Economics of Means-Tested Transfer Programs in the United States, Volume 1 (pp. 219–301). University of Chicago Press. [Google Scholar]
- Hurley KM, Black MM, Papas MA, & Quigg AM, 2008. Variation in breastfeeding behaviours, perceptions, and experiences by race/ethnicity among a low-income statewide sample of Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) participants in the United States. Matern. Child. Health. J, 4(2), 95–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute for Public Policy and Social Research (IPPSR), 2019. Correlates of State Policy. http://ippsr.msu.edu/public-policy/correlates-state-policy (retrieved on 02.08.2019).
- Jaffe AB, 1989. Real effects of academic research. Am. Econ. Rev, 79(5), 957–970. [Google Scholar]
- Jensen E, 2012. Participation in the Supplemental Nutrition Program for Women, Infants and Children (WIC) and breastfeeding: National, regional, and state level analyses. Matern. Child. Health. J, 16, 624–631. [DOI] [PubMed] [Google Scholar]
- Jiang M, Foster EM, Gibson-Davis CM, 2010. The effect of WIC on breastfeeding: A new look at an established relationship. Child. Youth. Serv. Rev, 32(2), 264–273. [Google Scholar]
- Kleibergen F, Paap R, 2006. Generalized reduced rank tests using the singular value decomposition. J. Econom, 133(1), 97–126. [Google Scholar]
- Kowaleski-Jones L, Duncan GJ, 2002. Effects of participation in the WIC program on birthweight: Evidence from the National Longitudinal Survey of Youth. Am. J. Public Health, 92(5), 799–804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langellier BA, Chaparro MP, & Whaley SE, 2012. Social and institutional factors that affect breastfeeding duration among WIC participants in Los Angeles County, California. Matern. Child. Health. J, 16(9), 1887–1895. [DOI] [PubMed] [Google Scholar]
- Langellier BA, Chaparro MP, Wang MC, Koleilat M, Whaley SE, 2014. The new food package and breastfeeding outcomes among women, infants, and children participants in Los Angeles County. Am. J. Public Health, 104(S1), S112–S118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee JY, Rozier RG, Norton EC, Kotch JB, Vann WF Jr, 2004. Effects of WIC participation on children’s use of oral health services. Am. J. Public Health, 94(5), 772–777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung CW, Epel ES, Ritchie LD, Crawford PB, Laraia BA, 2014. Food insecurity is inversely associated with diet quality of lower-income adults. J. Acad. Nutr. Diet, 114(12), 1943–1953.e2. [DOI] [PubMed] [Google Scholar]
- Li K, Wen M, Reynolds M, Zhang Q, 2019. WIC Participation and Breastfeeding after the 2009 WIC Revision: A Propensity Score Approach. Int. J. Environ. Res. Public Health, 16(15), e2645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin-Anderson S, 2013. Prenatal attitudes and parity predict selection into a US child health program: A short report. Soc. Sci. Med, 95, 128–132. [DOI] [PubMed] [Google Scholar]
- Medicaid, 2020. FY 2012–2014 Number of Children Ever Enrolled Report. https://www.medicaid.gov/chip/reports-and-evaluations/index.html (retrieved on 02.24.2020).
- Metallinos-Katsaras E, Brown L, Colchamiro R, 2015. Maternal WIC participation improves breastfeeding rates: A statewide analysis of WIC participants. Matern. Child Health J, 19(1), 136–143. [DOI] [PubMed] [Google Scholar]
- National Academies of Sciences, Engineering, and Medicine (NASEM), 2017. Review of WIC food packages: Proposed framework for revisions: Final Report. The National Academies Press, Washington, DC. doi: 10.17226/23655. [DOI] [PubMed] [Google Scholar]
- National Immunization Survey, 2018. Analysis: Breastfeeding Rates. https://www.cdc.gov/breastfeeding/data/nis_data/analysis.html (retrieved on 02.08.2019).
- National WIC Association, 2019. WIC Program Overview and History. https://www.nwica.org/overview-and-history (retrieved on 02.08.2019).
- Neuberger Z, 2017. Modernizing and streamlining WIC eligibility determination and enrollment processes. Center on Budget and Policy. https://www.cbpp.org/research/modernizing-and-streamlining-wic-eligibility-determination-and-enrollment-processes (retrieved on 02.24.2020). [Google Scholar]
- Phelps CE, 2011. Economic issues of breastfeeding. Breastfeed. Med, 6(5), 307–311. [DOI] [PubMed] [Google Scholar]
- Pinard CA, Bertmann FMW, Byker Shanks C, Schober DJ, Smith TM, Carpenter LC, & Yaroch AL, 2017. What factors influence SNAP participation? Literature reflecting enrollment in food assistance programs from a social and behavioral science perspective. J. Hunger. Environ. Nutr, 12(2), 151–168. [Google Scholar]
- Ryan AS, Zhou W, 2006. Lower breastfeeding rates persist among the Special Supplemental Nutrition Program for Women, Infants, and Children participants, 1978–2003. Pediatr., 117(4),1136–1146. [DOI] [PubMed] [Google Scholar]
- Sloan FA, Shadle JH, 2009. Is there empirical evidence for “defensive medicine”? A reassessment. J. Health Econ, 28(2), 481–491. [DOI] [PubMed] [Google Scholar]
- Sommers BD, Rosenbaum S, 2011. Issues in health reform: how changes in eligibility may move millions back and forth between Medicaid and insurance exchanges. Health Aff., 30(2), 228–236. [DOI] [PubMed] [Google Scholar]
- Sonchak L, 2017. The impact of WIC on breastfeeding initiation and gestational weight gain: Case study of South Carolina Medicaid mothers. Child. Youth Serv. Rev, 79, 115–125. [Google Scholar]
- Sovey AJ, Green DP, 2011. Instrumental variables estimation in political science: A readers’ guide. Am. J. Pol. Sci, 55(1), 188–200. [Google Scholar]
- Sparks PJ, 2011. Racial/ethnic differences in breastfeeding duration among WIC-eligible families. Women’s Health Issues, 21(5), 374–382. [DOI] [PubMed] [Google Scholar]
- Stock JH, Yogo M, 2005. Testing for weak instruments in linear IV regression. In: Andrews DWK (Ed.), Identification and Inference for Econometric Models. Cambridge University Press, New York, pp. 80–108. [Google Scholar]
- Swann CA, 2010. WIC eligibility and participation: The roles of changing policies, economic conditions, and demographics. B. E. J. Econ. Anal. Pol, 10(1), 21. [Google Scholar]
- The Annie E. Casey Foundation, 2020. Kids Count Data Center. https://datacenter.kidscount.org/ (retrieved on 02.24.2020).
- Topolyan I, Xu X, 2017. Differential effects of mother’s and child’s postnatal WIC participation on breastfeeding. Appl. Econ, 49(23), 2216–2225. [Google Scholar]
- U.S. Bureau of Labor Statistic, 2020. Local Area Unemployment Statistics. https://www.bls.gov/lau/ (retrieved on 02.24.20).
- U.S. Department of Agriculture (USDA), 2016. Special Supplemental Nutrition Program for Women, Infants and Children (WIC): Breastfeeding Policy and Guidance. https://www.fns.usda.gov/sites/default/files/wic/WIC-Breastfeeding-Policy-and-Guidance.pdf (retrieved on 02.08.19).
- U.S. Department of Agriculture (USDA), 2018. Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Participant and Program Characteristics 2016. https://fns-prod.azureedge.net/sites/default/files/ops/WICPC2016-Summary.pdf (retrieved on 02.08.2019).
- U.S. Department of Agriculture (USDA)/Food Nutrition Service (FNS), 2018. Fiscal Year 2014 WIC Food Package Costs: Final Report. https://fns-prod.azureedge.net/sites/default/files/resource-files/WICFoodPackageCost2014.pdf. (retrieved on 12.07.2020).
- U.S. Department of Agriculture (USDA), 2019. WIC Frequently Asked Questions (FAQs). https://www.fns.usda.gov/wic/frequently-asked-questions-about-wic (retrieved on 03.08.2020).
- U.S. Department of Agriculture (USDA), 2020a. Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). https://www.fns.usda.gov/wic (retrieved on 02.17.2020).
- U.S. Department of Agriculture (USDA), 2020b. Supplemental Nutrition Assistance Program (SNAP). https://www.fns.usda.gov/snap/supplemental-nutrition-assistance-program (retrieved on 02.17.2020).
- U.S. Department of Agriculture (USDA), 2020c. WIC 2017 Eligibility and Coverage Rates. https://www.fns.usda.gov/wic-2017-eligibility-and-coverage-rates#5 (retrieved on 12.07.2020).
- U.S. Department of Agriculture (USDA), 2020d. SNAP Data Tables. https://fns-prod.azureedge.net/sites/default/files/resource-files/SNAPsummary-1.pdf (retrieved on 02.17.2020).
- U.S. Department of Agriculture (USDA), 2020e. WIC Data Tables. https://fns-prod.azureedge.net/sites/default/files/resource-files/wisummary-1.pdf (retrieved on 02.17.2020).
- U.S. Department of Agriculture (USDA), 2020f. SNAP Policy Database: Interactive Tool. SNAP Policy Index. https://www.ers.usda.gov/data-products/snap-policy-data-sets/snap-policy-index-interactive-tool/. (retrieved on 12.07.2020). [Google Scholar]
- U.S. Department of Agriculture (USDA), 2020g. WIC Breastfeeding Support. https://wicbreastfeeding.fns.usda.gov/ (retrieved on 02.19.2020).
- U.S. Department of Health and Human Services, 2020. Temporary Assistance for Needy Families (TANF). https://www.acf.hhs.gov/ofa/programs/tanf (retrieved on 02.17.2020).
- Wilde P, Wolf A, Fernandez M, Collins A, Robare JF, 2011. Evaluation of the birth month breastfeeding changes to the WIC food packages. US Department of Agriculture, Food and Nutrition Service, Office of Research and Analysis. Alexandria, Virginia, US. https://www.fns.usda.gov/wic/evaluation-birth-month-breastfeeding-changes-wic-food-packages (retrieved on 02.08.2019). [Google Scholar]
- Wilde P, Wolf A, Fernandes M, Collins A, 2012. Food-package assignments and breastfeeding initiation before and after a change in the Special Supplemental Nutrition Program for Women, Infants, and Children. Am. J. Clin. Nutr, 96(3), 560–566. [DOI] [PubMed] [Google Scholar]
- Wooldridge JM, 2010. Econometric analysis of cross section and panel data, MIT Press. [Google Scholar]
- Yen ST, 2010. The effects of SNAP and WIC programs on nutrient intakes of children. Food Policy, 35(6), 576–583. [Google Scholar]
- Zhang Q, Tang C, McLaughlin P, Diggs L, 2017. Individual and Store Characteristics Associated with Brand Choices in Select Food Category Redemptions among WIC Participants in Virginia. Int. J. Environ. Res. Public Health, 14(4), 364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Q, Lamichhane R, Wright M, McLaughlin PW, Stacy B, 2019. Trends in breastfeeding disparities in US infants by WIC eligibility and participation. J. Nutr. Educ. Behav, 51(2), 182–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziol-Guest KM, Hernandez DC, 2010. First-and second-trimester WIC participation is associated with lower rates of breastfeeding and early introduction of cow’s milk during infancy. J. Am. Diet. Assoc, 110(5), 702–709. [DOI] [PubMed] [Google Scholar]
References
- Bitler MP, Currie J, Scholz JK, 2003. WIC eligibility and participation. J. Hum. Resour, 38, 1139–1179. [Google Scholar]
- Carlson S, Neuberger Z, Rosenbaum D, 2017. WIC participation and costs are stable: Have returned to pre-recession levels. Center on Budget and Policy Priorities. https://www.cbpp.org/sites/default/files/atoms/files/8-3-15fa.pdf. (Retrieved on 12.07.2020) [Google Scholar]
- Christie C, Watkins JA, Martin A, Jackson H, Perkin JE, Fraser J, 2006. Assessment of client satisfaction in six urban WIC clinics. Florida Public. Health. Rev, 3, 35–42. [Google Scholar]
- Gilbert D, Nanda J Paige D, 2014. Securing the safety net: Concurrent participation in income eligible assistance programs. Matern. Child. Health. J, 18(3), 604–612. [DOI] [PubMed] [Google Scholar]
- Jensen E, 2012. Participation in the Supplemental Nutrition Program for Women, Infants and Children (WIC) and breastfeeding: National, regional, and state level analyses. Matern. Child. Health. J, 16(3), 624–631. [DOI] [PubMed] [Google Scholar]
- Kahler LR, O’Shea RM, Duffy LC, Buck GM, 1992. Factors associated with rates of participation in WIC by eligible pregnant women. Public. Health. Rep, 107(1), 60–65. [PMC free article] [PubMed] [Google Scholar]
- Ku L, 1989. Factors influencing early prenatal enrollment in the WIC program. Public. Health. Rep, 104(3), 301–306. [PMC free article] [PubMed] [Google Scholar]
- Lanese BG, Fischbein R, Furda C, 2018. Public program enrollment following US state Medicaid expansion and outreach. Am. J. Public Health, 108(10), 1349–1351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu CH, Liu H, 2016. Concerns and structural barriers associated with WIC-participation among WIC eligible women. Public Health Nur, 33(5), 395–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NASEM Committee to Review WIC Food Packages; Food and Nutrition Board; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine, 2017. Review of WIC Food Packages: Improving Balance and Choice: Final Report. http://www.nap.edu/23655. (Retrieved on 12.07.2020) [PubMed]
- Powell L, Amsbary J, Xin H, 2015. Stigma as a communication barrier for participation in the federal government’s Women, Infants, and Children program. Qual. Res. Rep. Comm, 16(1), 75–85. [Google Scholar]
- Pinard CA, Bertmann FMW, Byker Shanks C, Schober DJ, Smith TM, Carpenter LC, and Yaroch AL, 2017. What factors influence SNAP participation? Literature reflecting enrollment in food assistance programs from a social and behavioral science perspective. J. Hunger. Environ. Nutr, 12(2), 151–168. [Google Scholar]
- Smith K, 2016. Fewer than half of WIC-eligible families receive WIC benefits. Carsey Research. https://scholars.unh.edu/cgi/viewcontent.cgi?article=1277&context=carsey. (Retrieved on 12.07.2020) [Google Scholar]
- Vargas ED, Pirog MA, 2016. Mixed-status families and WIC uptake: The effects of risk of deportation on program use. Soc. Sci. Q, 97(3), 555–572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ver Ploeg M, Betson DM, National Research Council, 2003. Income and adjunctive eligibility of infants and children. In Estimating Eligibility and Participation for the WIC Program: Final Report. National Academies Press (US). https://www.nap.edu/read/10804/chapter/7. (Retrieved on 12.07.2020) [PubMed] [Google Scholar]