

Abstract
Recovery High Schools (RHSs) provide educational programming and therapeutic support services for young people in recovery from substance use disorders (SUDs). The objectives of this study were to examine whether students with SUDs who attended RHSs report less delinquency and substance use than students with SUDs who attended non-RHSs, and how students’ social problem solving styles might moderate those associations. Participants were students from a longitudinal quasi-experimental study of adolescents who enrolled in high schools after receiving treatment for SUDs. The propensity-score balanced sample included 260 adolescents (143 in RHSs, 117 in non-RHSs) enrolled in schools in Minnesota, Wisconsin, or Texas (M age = 16; 83% White; 44% female). Negative binomial regression models were used to compare delinquency and substance use outcomes for RHS and non-RHS students at 6-month and 12-month follow-ups. The results indicated that students attending RHSs after discharge from SUD treatment reported less frequent delinquent behavior while intoxicated, and fewer days of substance use relative to students attending non-RHSs. Negative problem solving styles moderated the effect of RHS attendance on substance use outcomes, with RHSs providing minimal beneficial effects for those students endorsing maladaptive problem solving styles. We conclude that RHSs offer a promising continuing care approach for adolescents in recovery from SUD problems, but may vary in their effectiveness for students with impulsive, careless, or avoidant problem solving styles.
Keywords: Adolescents, delinquency, problem solving, recovery schools, substance use
Adolescent substance use and delinquency are critical public health concerns in the United States. In 2018, among adolescents aged 12-17, approximately 9% reported using alcohol and 8% reported using illicit drugs in the past month (Substance Abuse and Mental Health Services Administration [SAMHSA] 2019); and an estimated 916,000 adolescents (nearly 4% of the population) met criteria for a substance use disorder (SUD; SAMHSA 2019). Delinquent behavior and criminal activity are also prevalent among U.S. adolescents. Recent national estimates indicate that among U.S. high school students in grades 9-12, 24% reported being in a physical fight, 6% had been threatened or injured with a weapon on school property, and 20% had been offered or sold drugs on school property in the past year; but many of the adolescents represented in these prevalence estimates may be victims rather than perpetrators of delinquent acts (Musu et al. 2019). In 2018, the U.S. juvenile arrest rate was 2,180 per 1,000,000, with the most prevalent offense types among adolescents being simple assault, larceny-theft, and drug abuse violations (Office of Juvenile Justice and Delinquency Prevention [OJJDP], 2019). Adolescent substance use and delinquency are associated with a range of negative consequences in adulthood, including violent and nonviolent criminality, substance use problems, mental and physical health problems, and academic failure (Copeland et al. 2015; Fergusson, Horwood, and Swain-Campbell 2002). Interventions that aim to prevent and mitigate substance use and delinquency are therefore essential for promoting healthy adolescent development.
Recovery High Schools
Recovery high schools (RHSs) offer an alternative high school option for youth in recovery from SUDs and may be a promising continuing care strategy for addressing adolescent substance use and delinquency. The RHS model was originally developed in the late 1970s, with approximately 42 such schools now currently operating in 15 U.S. states (Association of Recovery Schools [ARS] 2016). Most RHSs have small enrollments, averaging 30-40 students per school (ARS 2016; Finch et al. 2016; White and Finch 2006). All RHSs meet state requirements for awarding secondary school diplomas and thus provide standard educational curricula for high school students. In addition to this academic programming, RHSs also provide therapeutic programming to support the unique needs of youth in recovery for SUDs (Finch and Frieden 2014; Moberg et al. 2014). Although the types of therapeutic services offered vary across RHSs, common services provided might include daily group check-ins, peer support groups, individual or group counseling sessions, and community service requirements (Moberg and Finch 2008). Enrollment in RHSs is typically voluntary, with students enrolling after referral from a substance use treatment center, counselor, parent, or health professional. Most RHSs do not require students to have previously completed SUD treatment, but instead, require students to pledge their commitment to sobriety and recovery during enrollment.
Given increased recognition of addiction as a chronic, relapsing condition, continuing care supports such as RHSs can be crucial for supporting adolescents’ substance use recovery process (Passetti et al. 2016). The recovery capital framework (Granfield and Cloud 1999; Hennessy 2017) highlights how access to and accumulation of resources (i.e., capital) at multiple ecological levels affects the substance use recovery process. Drawing on this recovery capital framework, RHSs aim to support students’ social and communal capital by fostering social connectedness with sober peers and supportive school staff (Finch et al. 2014; Karakos 2014). Affiliation with deviant peers is one of the strongest risk factors for adolescent delinquency and substance use (Fergusson, Swain-Campbell, and Horwood 2002; Hawkins et al. 1992), likely due to the peer pressure and deviant behavior modelling that can occur within a peer group. Thus, criminological theories of social learning (Akers 1998) and integrative social control (Le Blanc 1997) suggest that RHSs may help students reduce both their substance use and delinquency by providing them with a close network of sober, supportive, and prosocial peers. However, a competing theoretical perspective is that bringing deviant adolescents together in groups (such as the RHS environment) may promote deviancy training that leads to iatrogenic effects and increased problem behavior (Dishion et al. 2001). Therefore, the direction and magnitude of the effect of RHS attendance on delinquent behavior likely varies across adolescents. One malleable risk/protective factor that may play an important role in this relationship is adolescents’ social problem solving style.
Social Problem Solving
Social problem solving (SPS) refers to problem solving as it pertains to everyday situations, including interpersonal and intrapersonal problems for which individuals attempt to identify effective solutions through self-directed cognitive-behavioral processes (D’Zurilla et al. 2004). The construct of SPS can be categorized into positive or constructive problem solving orientation (rational problem solving style) versus negative or maladaptive problem solving orientation (impulsive/careless or avoidant styles) (D’Zurilla et al. 2002; D’Zurilla et al. 2004; Nezu, 2004). SPS is theorized to correlate with adolescent problem behavior such that individuals with negative problem solving orientations are less likely to have prosocial responses to risky environmental cues and situations (e.g., declining peer offers to use substances or engage in delinquent behavior). Indeed, negative or maladaptive problem solving has been linked to a range of negative mental health and behavioral outcomes in adolescents, including substance use (Jaffee and D’Zurilla 2009), delinquency (Antonowicz and Ross 2005; Jaffee and D’Zurilla 2003), and depression and suicidality (Becker-Weidman et al. 2010; Reinecke et al. 2001).
Given these numerous sequelae, many preventive intervention programs attempt to bolster positive SPS skills among youth, with recent meta-analytic research suggesting SPS training may be effective in improving student behavior and decreasing aggression among school-aged youth (Espada et al. 2012; Merrill et al. 2017). Furthermore, SPS styles may moderate the effectiveness of behavioral interventions and treatments, whereby individuals with positive or constructive problem solving styles may be more responsive to treatment (e.g., Becker-Weidman et al. 2010; Piehler and Winters 2017). Taken together, these findings suggest that SPS styles may moderate the effectiveness of RHSs as a continuing care intervention for adolescents with histories of SUDs.
Study Objectives
To date, we are unaware of any prior studies that have examined whether RHS attendance is associated with reductions in delinquency, and whether those associations may vary according to students’ SPS styles. A small but growing body of descriptive and observational research suggests that RHSs may yield beneficial effects on students’ substance use, school attendance, and school completion (Finch et al. 2014; Finch et al. 2018; Lanham and Tirado 2011; Moberg and Finch 2008; Tanner-Smith et al. 2019; Weimer et al. 2019). In the only controlled evaluation study of RHSs to date—and the parent study from which we derive data for the current study—Finch and colleagues (2018) examined the effects of RHS attendance on student’s school grades, truancy, school absenteeism, alcohol use, marijuana use, and other illicit substance use and reported beneficial effects on substance use and absenteeism outcomes at 6-month follow-up. Using data from the same parent study, Weimer et al (2019) examined 12-month follow-up data and found significant beneficial effects of RHS attendance on substance use and high school graduation outcomes but found no evidence of effects on adolescents’ illegal behavior, arrests, or use of medical care. Finally, although prior research suggests that SPS styles are associated with delinquent and other problem behavior among youth (Antonowicz and Ross 2005; Jaffee and D’Zurilla 2003), to date we are unaware of any prior research examining whether SPS styles moderate the effectiveness of continuing care interventions such as RHSs.
To address these identified gaps in the literature, the objectives of this study, therefore, were to examine (1) whether students attending RHSs experience lower levels of delinquency and substance use compared to students attending non-RHSs; and (2) whether students’ problem solving styles moderate those associations. We addressed these research questions by conducting a secondary analysis of data from a longitudinal quasi-experimental effectiveness study that focused on students’ experiences after discharge from SUD treatment.
Method
Participants
This study analyzed data from a longitudinal quasi-experimental evaluation of RHS attendance on student outcomes (Finch et al. 2018). Adolescents with histories of SUDs were recruited from 10 SUD treatment facilities in catchment areas within Minnesota, Wisconsin, or Texas where RHSs were known to be in operation at the time of study recruitment. Adolescents and their families were recruited upon discharge from the SUD treatment program (baseline data collection period), and then followed longitudinally after discharge at 3-month, 6-month, and 12-month follow-ups. After discharge from the SUD treatment program, families were free to enroll adolescents in any type of formal schooling, which included RHSs (intervention condition) and other non-recovery oriented high schools (non-RHSs; comparison condition). This recruitment plan yielded a smaller number of RHS enrollees than expected after the first year of the study, so in the second year, intervention group participants were also recruited directly from 12 RHSs operating within the same catchment areas as the SUD treatment facilities. Students were eligible to participate if they had completed SUD treatment within the prior 12 months. A total of 294 adolescents (171 in RHSs, 123 in non-RHSs) were enrolled in the study during the entire recruitment period, 237 of whom completed 6-month follow-ups, and 210 of whom completed 12-month follow-ups. As described below, the final analytic sample for the current study included 260 adolescents (143 in RHSs, 117 in non-RHSs) that were well-balanced on baseline demographics.1
Procedure
Study data were collected during extensive youth assessments completed via in-person computer-assisted interviewing by a team of trained, master’s level data collectors (Finch et al. 2018). Participating students were assured that their responses to the assessments would be kept confidential. The Institutional Review Board at the University of Minnesota approved all data collection procedures. Student assent and parent consent were secured for all research participants; at each assessment point, all participants received gift cards to a large general merchandise store to incentivize study participation.
Intervention and Comparison Conditions
This study used a longitudinal, non-equivalent comparison group design to compare outcomes for students with histories of SUDs who attended RHSs vs. non-RHSs after being discharged from SUD treatment. We used a quasi-experimental research design because randomization to conditions was deemed infeasible after initial planning discussions with local stakeholders. The intervention group included students who had received formal SUD treatment and subsequently enrolled in an RHS for at least 28 days at any point during the intake through the study follow-up period. Students in the intervention group attended 1 of 12 RHSs, 7 in Minnesota, 3 in Texas, and 2 in Wisconsin. The structural nature of the schools included “Area Learning Center” or other public alternative school programs (in Minnesota and Wisconsin), charter schools in Minnesota and Texas, and an independent non-profit contracting with the local public school district (in Wisconsin). The size of the RHS student body ranged from 3 to 115, with a median of 12 and a mean of 32 enrolled students. All RHSs provided high school curricula that met state requirements, as well as abstinence-oriented therapeutic services.
The comparison group included students who had received formal SUD treatment but did not enroll in an RHS for at least 28 days during the study period. This operational definition for the intervention and comparison groups was selected to correspond to a threshold of approximately one month of RHS attendance for the intervention group and designed to assess how RHS attendance, namely students’ participation in a set of unique educational programs and therapeutic supports, may affect students’ outcomes.2 The rationale for defining the two groups in this way was to permit examination of the effects of regular RHS attendance on students’ outcomes; however, this definition meant that the comparison condition included 9 participants who had elected to enroll in an RHS but then dropped out of the school before 28 days of enrollment. Those 9 comparison group participants were only enrolled in RHSs for an average of 1 day (SD = 0.33, Median = 1, Mode = 1). Sensitivity analyses excluding those participants yielded findings that were substantively similar to those reported here.
Because baseline differences between groups are one of the primary threats to internal validity in this type of quasi-experimental design (i.e., due to potential selection bias in choice of schools), we used propensity scores to address potential baseline non-equivalence between the two conditions (Tanner-Smith and Lipsey 2014). Propensity score methods attempt to remove the selection bias from causal effect estimates that may occur when the observed intervention effect is due to differences in observed characteristics of participants in the different conditions, rather than (or in addition to) the intervention itself (for more information on propensity score methods, see Imbens and Rubin 2015; Shadish and Steiner 2010). Propensity scores were conceptualized as the predicted probability of attending an RHS during the 12-month study follow-up period, estimated with multilevel logistic regression models that included baseline values of outcome variables as well as a wide range of covariates including adolescent demographics, SUD treatment histories, mental health histories, and family functioning (see Finch et al., 2018). The propensity score model was built following the recommendations of Imbens and Rubin (2015), using a stepwise procedure for selecting the covariates and higher-order terms included in the estimation model. We assessed and ensured balance conditional on the estimated propensity score using multilevel linear regression models and visual inspection of Q-Q plots. The linearized propensity score and the square of this propensity score were then used as covariate controls in the final outcome models to ensure balance between the intervention and comparison conditions.
The analytic sample was restricted to participants in the region of common support on the estimated propensity score (i.e., the range of the estimated propensity score for which intervention and comparison participants were both represented); 28 RHS participants and 6 non-RHS participants were outside the region of common support and were dropped from the analytic sample. The final analytic sample thus included 260 participants who were well-balanced on the baseline covariates included in the propensity score estimation model.
Measures
Substance use and delinquency outcomes.
Substance use was measured using the Timeline Followback method (Sobell and Sobell 1995), which asked students to self-report how many days they had used alcohol, marijuana, or another drug in the prior three months. We also examined two self-reported delinquency items measured using the Global Appraisal of Individual Needs-Q3 (GAIN-Q3; Titus et al. 2013): Daring the past 90 days, on how many days were you involved in any activities you thought might get you into trouble or be against the law, besides drug use? On how many of these days were you involved in these activities while you were high or drunk? All items were asked similarly at the baseline, 6-month, and 12-month assessments (range 0-90 days); however, the baseline assessments asked students about their behavior in the three months prior to SUD treatment enrollment whereas the 6-month and 12-month assessments asked about students’ behavior in the three months prior to the assessment period.
Social problem solving styles.
SPS styles were measured using a modified version of the Social Problem Solving Inventory-Revised Short Form (SPSI-R; D’Zurilla et al. 2002). The modified inventory included 25 binary (yes/no) items assessing SPS styles; 12 of those items reflected positive problem solving styles (e.g., If I can’t solve a problem first, I know if I keep trying, I will eventually be able to solve it; Before I try to solve a problem, I set a goal so that I know exactly what I want to happen) and 13 items reflected negative problem solving styles (e.g., I put off solving problems until it is too late to do anything about them; When I try to solve a problem and fail, I get very frustrated). We calculated a positive problem solving (PPS) style scale (α = .74) and negative problem solving (NPS) style scale (α = .79) by estimating the mean response pattern across the positive and negative items, respectively.
Covariate controls.
The original study collected data on a range of other student characteristics, including student demographics, SUD treatment histories, mental health histories, and family functioning. The following baseline measures were included in the propensity score estimation model: students’ self-reported age, race, gender; alcohol use and marijuana use, and mental health treatment service receipt (all collected using the Timeline Followback method); criminal justice system involvement and school problems (both collected using the GAIN-Q3); perceived psychological benefits of drug use and peer approval of substance use (both collected using the Personal Experiences Inventory), perceived availability of drugs, knowledge of RHS existence, interest in attending an RHS, interest in attending continuing care, frequency of self-help group attendance, prior year school attendance and grades, family income, parental history of substance use treatment, family history of mental health problems, problem solving (collected using the SPSI-R), frequency of religious activity participation, and frequency of helping with household chores. Additional measurement details and rationale for selection of control variables has been reported in prior articles (Botzet et al. 2014; Tanner-Smith and Lipsey 2014).
Analytic Strategies
Given that the outcome measures of student substance use and delinquency were overdispersed, non-negative count outcomes, we used negative binomial regression models to address the study objectives. Main effects negative binomial regression models were estimated separately for each outcome at the 6-month and 12-month follow-ups, respectively. Multiplicative interaction terms (i.e., expanded terms interacting RHS/non-RHS status with positive and negative SPS scales) were used to test for potential moderation effects. All negative binomial regression models were estimated in the Stata software (version 15.1; StataCorp 2017) using the NB1 model parameterization (Cameron and Trivedi 1986). The NB1 model that assumes constant dispersion was selected given that AIC fit statistics indicated the NB1 model was a consistently better fit than the NB2 model.
To provide additional adjustment for any baseline differences between the RHS and non-RHS groups, all outcome models controlled for the estimates of the linearized propensity score and the squared propensity score. All models additionally controlled for the students’ gender, race, and baseline measures of the outcome. Finally, we used cluster robust standard errors to correct for the correlated errors associated with student nesting within schools. We assessed statistical significance at the α = .05 level and convey effect size magnitude with standardized mean difference effect sizes (d) and incidence rate ratios (IRR).3
There was a modest amount of missing data due to survey non-response on social problem solving styles (missing for 1% of cases) and illegal activity at baseline (2%), and due to attrition at 6-month follow-up (19%) and 12-month follow-up (30%). We therefore used multiple imputation (Schafer and Graham 2002) to handle missing data. We created 20 imputed datasets based on all variables of interest (i.e., substance use, delinquency, SPS, student demographics) and imputations were estimated separately for the RHS and non-RHS groups. Pooled estimates and inferential statistics were then calculated using Rubin’s rules (1987).
Results
The analytic sample included 260 students who attended RHSs (n = 143) vs. non-RHSs (n = 117) after receiving some form of SUD treatment. On average, students were 16.07 years old (SD = 1.03) at the time of SUD treatment receipt, with the most recent treatment delivered at inpatient/residential (52%), intensive outpatient (34%), or outpatient (14%) levels of care. Table 1 presents descriptive statistics for the analytic sample by condition and assessment period. The modal grade level of students was 11th grade (with an average age of 16), with 53% male in the RHS group and 60% male in the non-RHS group. The sample was predominantly White (87% in RHS group, 78% in the non-RHS group). SPS styles were similar across the two groups at baseline. Students in both groups reported frequent substance use and delinquency at baseline but reported reductions in these behaviors at 6- and 12-month follow-ups.
Table 1.
Descriptive statistics for student demographics, social problem solving styles, substance use, and delinquency by condition and assessment period
| Baseline | 6-Month | 12-Month | ||||
|---|---|---|---|---|---|---|
| M or % | SE | M | SE | M | SE | |
| Recovery High School Students (n = 143) | ||||||
| Age | 16.45 | (0.09) | ||||
| Gender (Boys) | 53.15% | |||||
| Race (Black) | 9.79% | |||||
| Race (White) | 86.71% | |||||
| Race (Other race) | ||||||
| Ethnicity (Hispanic) | 9.79% | |||||
| Positive problem solving style scale (PPS) | 0.73 | (0.02) | ||||
| Negative problem solving style scale (NPS) | 0.53 | (0.02) | ||||
| Days of substance use | 70.94 | (2.32) | 10.97 | (2.08) | 11.32 | (1.87) |
| Days of illegal activity | 8.99 | (1.50) | 5.98 | (1.23) | 6.38 | (1.49) |
| Days of intoxicated illegal activity | 3.25 | (0.88) | 2.45 | (0.89) | 2.82 | (0.98) |
| Non-Recovery High School Students (n = 117) | ||||||
| Age | 16.08 | (0.10) | ||||
| Gender (Boys) | 59.83% | |||||
| Race (Black) | 11.11% | |||||
| Race (White) | 77.78% | |||||
| Race (Other race) | ||||||
| Ethnicity (Hispanic) | 13.68% | |||||
| Positive problem solving style scale (PPS) | 0.68 | (0.02) | ||||
| Negative problem solving style scale (NPS) | 0.54 | (0.02) | ||||
| Days of substance use | 66.74 | (2.50) | 22.82 | (3.02) | 26.12 | (3.29) |
| Days of illegal activity | 12.48 | (1.94) | 9.52 | (2.00) | 6.82 | (1.59) |
| Days of intoxicated illegal activity | 7.56 | (1.58) | 4.51 | (1.36) | 4.02 | (1.17) |
Table 2 presents coefficients and confidence intervals from the negative binomial regression models estimated to assess the effects of RHS attendance on student outcomes. As shown in the top panel of Table 2, the results from the main effects models indicated that students who attended RHSs reported less substance use than non-RHS students at the 6-month (b = −0.58, 95% CI [−1.21, 0.04], IRR = .56, d = 0.19) and 12-month follow-ups (b = −0.50, 95% CI [−0.98, −0.02], IRR = .60, d = 0.21). Namely, students who attended RHSs reported rates of substance use at a rate approximately .60 times smaller than non-RHS students. At the 12-month follow-up, the predicted number of days using substances in the past 90 days was 13.86 for RHS students versus 25.67 for non-RHS students. The results from the main effects models also indicated that students with higher values on the positive SPS scale reported significantly lower levels of substance use at the 6-month follow-up (b = −1.06, 95% CI [−1.90, −0.23], IRR = .35), but there was no evidence of this association at the 12-month follow-up.
Table 2.
Effects of recovery high school attendance and social problem solving styles on student substance use and delinquency outcomes at 6-month and 12-month follow-up
| Days of substance use | Days of illegal activity | Days of intoxicated illegal activity | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6-Month | 12-Month | 6-Month | 12-Month | 6-Month | 12-Month | |||||||
| b | 95% CI | b | 95% CI | b | 95% CI | b | 95% CI | b | 95% CI | b | 95% CI | |
| Main Effects Models | ||||||||||||
| RHS student | −0.58† | [−1.21, 0.04] | −0.50* | [−0.98, −0.02] | −0.43† | [−0.91, 0.05] | −0.17 | [−0.62, 0.28] | −1.10* | [−1.89, −0.29] | −0.87* | [−1.57, −0.18] |
| PPS | −1.06* | [−1.90, −0.23] | 0.12 | [−0.90, 1.15] | −0.60 | [−1.59, 0.38] | 0.31 | [−0.82, 1.44] | 0.17 | [−1.54, 1.88] | −0.00 | [−1.68, 0.58] |
| NPS | −0.47 | [−1.41, 0.47] | −0.57 | [−1.46, 0.31] | 0.58 | [−0.27, 1.44] | 0.43 | [−0.39, 1.26] | 0.41 | [−1.02, 1.83] | −0.55 | [−1.68, 0.58] |
| Interaction Models | ||||||||||||
| RHS student | −1.93* | [−3.66, −0.20] | −1.15 | [−3.22, 0.91] | 1.01 | [−1.49, 3.51] | 0.23 | [−1.66, 2.11] | −0.45 | [−3.98, 3.07] | 0.02 | [−2.81, 2.86] |
| PPS | −1.02† | [−2.15, 0.10] | 0.18 | [−1.14, 1.50] | −0.13 | [−1.21, 0.95] | 0.51 | [−0.90, 1.91] | 0.42 | [−1.49, 2.32] | 0.31 | [−1.52, 2.15] |
| NPS | −1.39* | [−2.43, −0.35] | −1.14† | [−2.34, 0.05] | 0.89† | [−0.10, 1.87] | 0.48 | [−0.71, 1.67] | 0.36 | [−1.40, 2.11] | −0.51 | [−1.99, 0.98] |
| RHS x PPS | 0.17 | [−1.49, 1.83] | −0.01 | [−2.10, 2.07] | −1.39 | [−3.47, 0.69] | −0.46 | [−2.13, 1.22] | −0.93 | [−4.44, 2.58] | −1.08 | [−4.12, 1.96] |
| RHS x NPS | 2.22* | [0.70, 3.75] | 1.28 | [−0.32, 2.88] | −0.85 | [−2.81, 1.11] | −0.14 | [−2.04, 1.76] | 0.06 | [−2.47, 2.60] | −0.25 | [−2.51, 2.01] |
Notes: Results are pooled estimates across 20 multiply imputed datasets. b – unstandardized negative binomial regression coefficient; 95% confidence intervals estimated with cluster robust standard errors. NPS – negative problem solving style scale; PPS - positive problem solving style scale; RHS - recovery high school. All models controlled for gender, race, and baseline measures of the outcome.
p <.05.
As shown in the bottom panel of Table 2, the results from the interaction models indicated that negative SPS styles significantly moderated the effect of RHS attendance on students’ substance use at the 6-month follow-up (b RHS x NPS = 2.22, 95% CI [0.70, 3.75], IRR = 9.23). Namely, the beneficial effect of RHS attendance on students’ substance use was most pronounced for students who scored low on the negative problem solving scale. As shown in Figure 1, substance use rates at 6-month follow-up were indeed similar for RHS and non-RHS students who endorsed high levels of negative SPS. For instance, the standardized mean difference effect sizes (d) indexing differences in predicted mean values of substance use for RHS and non-RHS students were 0.51 for students scoring 0.20 on the negative problem solving scale (corresponding to the 15th percentile of the distribution), versus effect sizes of 0.31, 0.14, and 0.00 for students scoring values of 0.40, 0.60, and 0.80 on the negative problem solving scale. Thus, although RHS students, on average, reported lower levels of substance use at 12 months than non-RHS students, this beneficial effect did not hold true for those students endorsing negative SPS styles.
Figure 1.
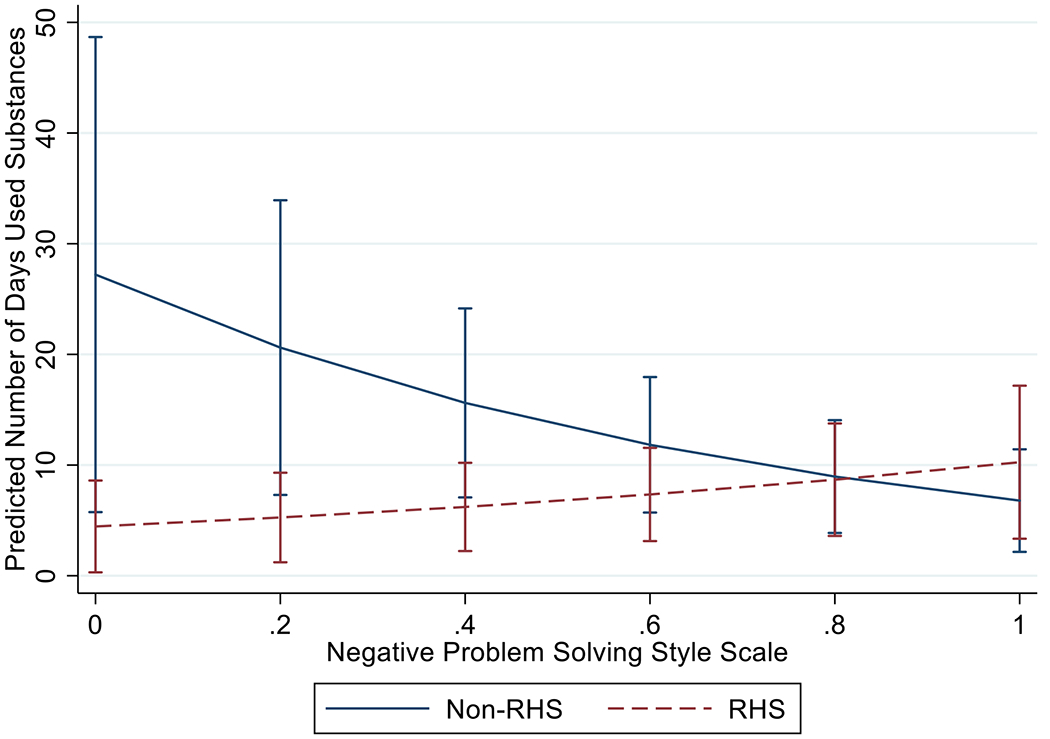
Predicted Days of Substance Use at 6-Month Follow-up, by RHS Condition and Negative Problem Solving Style Scale Score
Finally, the results shown in Table 2 provide no evidence that RHS students had significantly different rates of illegal activity at 12 months than non-RHS students. There was no evidence that SPS styles were associated with illegal activity frequency and no evidence that SPS styles moderated the (non)effects of RHS attendance on illegal activity. But, as shown in the right panel of Table 2, RHS students did report significantly lower levels of intoxicated illegal activity at both the 6-month (b = −1.10, 95% CI [−1.89, −0.29], IRR = .34, d = 0.37) and 12-month (b = −0.87, 95% CI [−1.57, −0.18], IRR = .42, d = 0.27) follow-ups. Again, however, there was no evidence that SPS styles were associated with students’ intoxicated illegal activity and no evidence that they moderated the effects of RHS attendance on intoxicated illegal activity.4
Discussion
The current study extended prior research on RHSs (Finch et al. 2018; Lanham and Tirado 2011; Moberg and Finch 2008; Tanner-Smith et al. 2019) by examining the long-term effects of RHS attendance on students’ substance use and delinquency outcomes. In an effort to better understand for whom and under what contexts RHSs may be beneficial, we examined SPS styles as a potential moderator of these outcomes. Although we found no evidence that RHS attendance was associated with reductions in illegal activity, RHS (vs. non-RHS) attendance was associated with lower levels of substance use and (consequently) intoxicated delinquent behavior at both the 6- and 12-month follow-ups. Further, some of these associations were moderated by SPS styles, such that RHS attendance may not yield beneficial reductions in substance use among those students who endorsed negative problem solving styles.
A noteworthy finding from this study is that RHS (vs. non-RHS) attendance was not associated with improvements in substance use for those students endorsing more maladaptive SPS styles. This finding supports evidence from prior research that adolescent problem solving styles can moderate the effects of interventions on adolescents’ behavioral and mental health outcomes (e.g., Piehler and Winters 2017). In the context of the present study, students endorsing maladaptive problem solving styles may be less able to generate multiple solutions to a problem or to consider long-term consequences—perhaps in interpersonal interactions in which they encounter substance or delinquency behavior in their peer group settings. As such, RHSs may want to consider incorporating programmatic elements that target SPS styles, such as focusing attention on generalizing problem solving strategies, specific skills training including building strategies for handling peer pressure, and activities to increase emotion regulation (Merrill et al. 2017). Such programmatic initiatives might help ensure that RHSs are more widely effective for participating students, including those who enter with maladaptive SPS styles. Although it is possible that some of the participating RHSs in the current study provided SPS skill training via the standard therapeutic programming offered, we did not systematically collect those data. Thus, an important direction for future research may be to examine whether RHSs that directly provide SPS training report improved SPS amongst participating students, and whether those improvements might mediate the effects of RHS attendance on other behavioral outcomes such as substance use and delinquency.
The results from the current study provide no evidence that SPS styles were associated with the frequency of students’ illegal activity or intoxicated illegal activity, and no evidence that SPS styles moderated the effects of RHS attendance on these delinquency outcomes. A potential explanation for these findings may be associated with the heterogeneity in services and treatments provided in different RHSs, and lack of fidelity monitoring of these services. Although RHSs share a common goal, schools typically offer a range of therapeutic services based on the needs and demands of their student body (Moberg and Finch 2008). While tailoring intervention components can help ensure students are receiving needed services, schools may inadvertently fail to offer therapeutic activities shown to be particularly effective in addressing substance use and delinquency such as cognitive-behavioral and motivational enhancement approaches (Jaffee and D’Zurilla 2009; Espada et al. 2012). Further, because RHSs and other continuing care models for youth recovering from SUDs are foremost designed to promote sobriety, the skills training and therapeutic programming available at RHSs may not meet the behavioral needs of students who engage in delinquent activities, regardless of recovery status. Program implementation data (e.g., fidelity to RHS logic model) were not available in the current study, so an important direction for additional research will be to examine the role of program implementation characteristics on RHS effects.
Another plausible explanation for the null findings of RHS attendance on delinquency outcomes could be related to the influence of peer groups outside the recovery environment of the RHS. Delinquency during adolescence is almost always a peer activity (Elliott, Huizinga, Ageton 1982) and some RHS students may continue interacting with deviant peer groups formed prior to SUD treatment enrollment. Although the RHS model provides a space for sobriety and abstinence within the school day, the current study did not account for students’ potential engagement with delinquent or substance-using peers, family members, or others outside of school. These social factors might outweigh individual characteristics (e.g., SPS styles), particularly during adolescence, a developmental period characterized by increased susceptibility for impulsivity and deviancy training among peers (Utrzan and Piehler 2016). Drawing upon the social augmentation hypothesis (Dishion et al. 2008), adolescents in recovery may no longer benefit from their prior (pre-SUD treatment) peer groups and may disengage with such peers over the course of their recovery; but there has been no systematic research that dynamically tracks these adolescents’ social networks over time. Further research is needed to examine changes in peer group affiliations among adolescents in recovery, which could provide important insights into differential effectiveness of RHSs on these long-term student outcomes.
The findings from the current study should be interpreted in light of several limitations. First, given that the analytic sample was comprised primarily of White, middle-class adolescents who had previously enrolled in SUD treatment, the results of the study should not be generalized broadly to all adolescents in recovery without replication in representative samples of students in RHSs. Second, given that participating students were not randomized to conditions, we cannot draw firm conclusions about the causal effects of RHS attendance on students’ substance use and delinquency outcomes. Although we used a controlled quasi-experimental design with propensity scores to control for potential selection bias on a range of observed characteristics, this approach does not account for any potential confounding associated with other unobserved characteristics. Future research will be needed to attempt to replicate these findings using other rigorous randomized, quasi-randomized, or controlled quasi-experimental designs. Third, given the relatively small sample size of the study, we were unable to conduct systematic examination of heterogeneity in student outcomes associated with features of the RHSs themselves (e.g., location, staff, founder, services provided) or the SUD treatment received prior to enrollment in the RHS. Future research examining such variability in effects associated with treatment and school characteristics will be critical in identifying some of the essential components of RHSs that maximize effectiveness in promoting positive outcomes among participating students, drawing on logic models explicating the theory of change underlying RHSs (e.g., Finch and Frieden 2014; Hennessy et al. 2018; Simington 2020).
Other limitations of the current study relate to the constructs and measures examined. For instance, the current study measured delinquency using a single self-reported item (number of days in which a student engaged in an illegal activity), a measure that may not fully capture the complexity and nuance of delinquent activity (Thornberry and Krohn 2000). Additional research on this topic may be warranted to explore the effects of RHS attendance on other measures of adolescent delinquency. Furthermore, this study only investigated one malleable risk/protective factor—social problem solving—as a potential moderator of the effects of RHS attendance on students’ substance use and delinquent behavior. Future research on this topic should examine other theoretically informed moderators, such as supportive family relationships, perceptions of stigma related to addiction, and bonding to recovery role models (Hennessy et al. 2019). Despite the limitations of the current study, our findings yield several important conclusions for the field of prevention and treatment of substance use and other comorbid problems among adolescents.
Conclusions
Given their apparent effectiveness at decreasing substance use and increasing high school completion, although with no evidence of effects on delinquency outcomes, RHSs should continue to be pursued as an option for maintaining sobriety for adolescents in recovery from SUDs. However, RHSs are unlikely to be universally effective in promoting recovery among all students, so it is essential to consider for whom, or under what circumstances, RHSs may be more or less beneficial. Individual characteristics such as SPS styles may be one important factor to consider, given that these modifiable characteristics can be addressed in programming efforts aimed at promoting healthy decision making in social contexts. Optimizing the benefits associated with RHSs thus will likely require the use of individualized needs assessments to identify the unique needs of students, combined with evidence-based programming that addresses these therapeutic needs.
Supplementary Material
Acknowledgements
Thanks to our many colleagues participating in this research including Andria Botzet, Christine Dittel, Barbara Dwyer, Tamara Fahnhorst, Emily Hennessy, Barbara Hill, Holly Karakos, Stephanie Lindsley, Mark Lipsey, Patrick McIlvaine, Katarzyna Steinka-Fry, Luis Torres, and Ken Winters.
Funding
This work was supported by the National Institute on Drug Abuse [R01DA029785]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of a an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
See Appendix A and Tanner-Smith et al. (2018) for descriptive statistics comparing students in the analytic sample across condition and recruitment site.
Of note, many students in the intervention condition attended an RHS for the entire duration of the 12-month follow-up period, with the mean number of calendar days enrolled in an RHS being 355 days (SD = 346.15, Median = 240).
Where IRR = exp(b) and indicates the expected change in the rate of behavior associated with a one-unit change in the predictor variable.
We also conducted post-hoc analyses to explore whether levels of RHS school attendance were correlated with substance use and delinquency outcomes, and the potential moderating effect of social problem solving styles. The main effects analyses were similar in pattern to that shown in Table 2; namely, each additional day of attending an RHS was associated with significantly lower levels of substance use at 6-months (b = −0.002, 95% CI [−0.003, −0.001], and 12-months (b = −0.001, 95% CI [−0.002, −0.0001], and intoxicated illegal activity at 12-months (b = −0.002, 95% CI [−0.003, −0.0002]. However, there was no evidence that the association between days of RHS attendance and those outcomes were moderated by students’ social problem solving styles.
Conflict of Interest
ETS, LMN, and CML declare that they have no conflicts of interest. AJF declares that he is a non-voting unpaid board member for the Association of Recovery Schools, but he will receive no financial benefit from the findings published in this article. DPM declares that he is an unpaid board member for a private nonprofit recovery high school, but he will receive no financial benefit from the findings published in this article.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the University of Minnesota Institutional Review Board and with the Helsinki Declaration of 1975, as revised in 2000.
Informed Consent
Informed assent and parental consent were obtained from all participants included in the study.
Contributor Information
Emily E. Tanner-Smith, University of Oregon, Eugene, OR
Lindsey M. Nichols, University of Oregon, Eugene, OR
Christopher M. Loan, University of Oregon, Eugene, OR
Andrew J. Finch, Vanderbilt University
D. Paul Moberg, University of Wisconsin-Madison, Madison, WI
References
- Akers RL (1998). Social learning and social structure: A general theory of crime and deviance. Boston, MA: Northeastern University Press. [Google Scholar]
- Antonowicz DH, & Ross RR (2005). Social problem-solving deficits in offenders. In McMurran M & McGuire J (Eds.), Social problem-solving and offending: Evidence, evaluation and evolution (pp. 91–102). Hoboken, NJ: Wiley. [Google Scholar]
- Association of Recovery Schools (ARS). (2016). The State of Recovery High Schools, 2016 Biennial Report. Denton, TX. Retrieved from www.recoveryschools.org. [Google Scholar]
- Becker-Weidman EG, Jacobs RH, Reinecke MA, Silva SG, & March JS (2010). Social problem-solving among adolescents treated for depression. Behaviour Research and Therapy, 48(1), 11–18. 10.1016/i.brat.2009.08.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Botzet AM, McIlvaine PW, Winters KC, Fahnhorst T, & Dittel C (2014). Data collection strategies and measurement tools for assessing academic and therapeutic outcomes in recovery schools. Peabody journal of Education, 89(2), 197–213. 10.1080/0161956X.2014.895648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cameron AC, & Trivedi PK (1986). Econometric models based on count data. Comparisons and applications of some estimators and tests. Journal of Applied Econometrics, 1(1), 29–53. 10.1002/jae.3950010104 [DOI] [Google Scholar]
- Copeland WE, Wolke D, Shanahan L, & Costello EJ (2015). Adult functional outcomes of common childhood psychiatric problems: A prospective, longitudinal study. JAMA Psychiatry, 72(9), 892–899. doi: 10.1001/jamapsychiatry.2015.0730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- D’Zurilla TJ, Nezu AM, & Maydeu-Olivares A (2002). The Social Problem-Solving Inventory-Revised: Technical manual. North Tonowanda: Multi-Health Systems. [Google Scholar]
- D’Zurilla TJ, Nezu AM, & Maydeu-Olivares A (2004). Social problem solving: Theory and assessment. In Chang EC, D’Zurilla TJ, & Sanna LJ (Eds.), Social problem solving: Theory, research, and training (pp. 11–27). Washington, DC: American Psychological Association. [Google Scholar]
- Dishion TJ, Piehler TF, & Myers MW (2008). Dynamics and ecology of adolescent peer influence. In Prinstein MJ & Dodge KA (Eds.), Understanding peer influence in children and adolescents (pp. 72–93). New York, NY: Guilford Press. [Google Scholar]
- Dishion TJ, Poulin F, & Burraston B (2001). Peer group dynamics associated with iatrogenic effect in group interventions with high-risk young adolescents. New Directions For Child And Adolescent Development, 91, 79–92. [DOI] [PubMed] [Google Scholar]
- Elliott DS, Huizinga D, Ageton SS (1982). Explaining delinquency and drug use. Boulder, CO: Behavioral Research Inst. [Google Scholar]
- Espada JP, Griffin KW, Pereira JR, Orgilés M, & García-Fernández JM (2012). Component analysis of a school-based substance use prevention program in Spain: Contributions of problem solving and social skills training content. Prevention Science, 13(1), 86–95. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, & Swain-Campbell N (2002). Cannabis use and psychosocial adjustment in adolescence and young adulthood. Addiction, 97(9), 1123–1135. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Swain-Campbell NR, & Horwood LJ (2002). Deviant peer affiliations, crime and substance use: A fixed effects regression analysis. Journal of Abnormal Child Psychology, 30(4), 419–430. [DOI] [PubMed] [Google Scholar]
- Finch AJ, & Frieden G (2014). The ecological and developmental role of recovery high schools. Peabody Journal of Education, 89(2), 271–287. 10.1080/0161956X.2014.897106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finch AJ, Moberg DP, & Krupp AL (2014). Continuing care in high schools: A descriptive study of recovery high school programs. Journal of Child & Adolescent Substance Abuse, 23(2), 116–129. 10.1080/1067828X.2012.751269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finch AJ, Tanner-Smith E, Hennessy E, & Moberg DP (2018). Recovery high schools: Effect of schools supporting recovery from substance use disorders. The American Journal of Drug and Alcohol Abuse, 44(2), 175–184. 10.1080/00952990.2017.1354378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finch A, Karakos H, & Hennessy EA (2016). Exploring the policy context around recovery high schools: A case study of schools in Minnesota and Massachusetts. In Reid T (Ed.), Substance Abuse: Influences, Treatment Options and Health Effects (pp. 109–138). Hauppauge, NY: Nova Science Publishers. [Google Scholar]
- Granfield R, & Cloud W (1999). Coming clean: Overcoming addiction without treatment. New York, NY: NYU Press. [Google Scholar]
- Hawkins JD, Catalano RE, & Miller JY (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin, 112(1), 64–105. [DOI] [PubMed] [Google Scholar]
- Hennessy EA (2017). Recovery capital: A systematic review of the literature. Addiction Research & Theory, 25(5), 349–360. [Google Scholar]
- Hennessy EA, Tanner-Smith EE, Finch AJ, Sathe N, & Kugley S (2018). Recovery schools for improving behavioral and academic outcomes among students in recovery from substance use disorders: A systematic review. Campbell Systematic Reviews, 14(1), 1–86. doi: 10.4073/csr.2018.9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hennessy EA, Cristello JV, & Kelly JF (2019). RCAM: A proposed model of recovery capital for adolescents. Addiction Research & Theory, 27(5), 429–436. [Google Scholar]
- Imbens GW, & Rubin DB (2015). Causal inference in statistics, social, and biomedical sciences: An introduction. Cambridge, United Kingdom: Cambridge University Press. [Google Scholar]
- Jaffee WB, & D’Zurilla TJ (2003). Adolescent problem solving, parent problem solving, and externalizing behavior in adolescents. Behavior Therapy, 34(3), 295–311. 10.1016/S0005-7894(03)80002-3 [DOI] [Google Scholar]
- Jaffee WB, & D’Zurilla TJ (2009). Personality, problem solving, and adolescent substance use. Behavior Therapy, 40(1), 93–101. [DOI] [PubMed] [Google Scholar]
- Karakos HL (2014). Positive peer support or negative peer influence? The role of peers among adolescents in recovery high schools. Peabody Journal of Education, 89(2), 214–228. 10.1080/0161956X.2014.897094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanham CC, & Tirado JA (2011). Lessons in sobriety: An exploratory study of graduate outcomes at a recovery high school. Journal of Groups in Addiction & Recovery, 6(3), 245–263. 10.1080/1556035X.2011.597197 [DOI] [Google Scholar]
- Le Blanc M (1997). Socialization or propensity: Does integrative control theory apply to adjudicated boys? Studies on Crime and Crime Prevention, 6, 200–223. [Google Scholar]
- Merrill KL, Smith SW, Cumming MM, & Daunic AP (2017). A review of social problem-solving interventions: Past findings, current status, and future directions. Review of Educational Research, 87(1), 71–102. 10.3102/0034654316652943 [DOI] [Google Scholar]
- Moberg DP, Finch AJ, & Lindsley SM (2014). Recovery high schools: Students and responsive academic and therapeutic services. Peabody Journal of Education, 89(2), 165–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moberg DP, & Finch AJ (2008). Recovery high schools: A descriptive study of school programs and students. Journal of Groups in Addiction & Recovery, 2, 128–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musu L, Zhang A, Wang K, Zhang J, & Oudekerk BA (2019). Indicators of school crime and safety: 2018. Washington, D.C.: Institute of Education Sciences. Retrieved from https://nces.ed.gov/pubs2019/2019047.pdf. [Google Scholar]
- Nezu AM (2004). Problem solving and behavior therapy revisited. Behavior therapy, 35(1), 1–33. 10.1016/S0005-7894(04)80002-9. [DOI] [Google Scholar]
- Office of Juvenile Justice and Delinquency Prevention (OJJDP). (2019). OJJDP statistical briefing book. Online. Retrieved from: https://www.ojjdp.gov/ojstatbb/special_topics/qa11501.asp?qaDate=2018. [Google Scholar]
- Passetti LL, Godley MD, & Kaminer Y (2016). Continuing care for adolescents in treatment for substance use disorders. Child and Adolescent Psychiatric Clinics, 25(4), 669–684. doi: 10.1016/j.chc.2016.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piehler TF, & Winters KC (2017). Decision-making style and response to parental involvement in brief interventions for adolescent substance use. Journal of Family Psychology, 31(3), 336–346. 10.1037/fam0000266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinecke MA, DuBois DL, & Schultz TM (2001). Social problem solving, mood, and suicidality among inpatient adolescents. Cognitive Therapy and Research, 25(6), 743–756. 10.1023/A:1012971423547 [DOI] [Google Scholar]
- Rubin DB (1987). Multiple imputation for nonresponse in surveys. New York, NY, J. Wiley & Sons. [Google Scholar]
- Schafer JL, & Graham JW (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177. doi: 10.1037//1082-989X.7.2.147 [DOI] [PubMed] [Google Scholar]
- Shadish WR, & Steiner PM (2010). A primer on propensity score analysis. Newborn and Infant Nursing Reviews, 10(1), 19–26. 10.1053/j.nainr.2009.12.010 [DOI] [Google Scholar]
- Simington SR (2020). Evidence based treatment for co-occurring disorders in adolescent alternative integrated education. Available from ProQuest Dissertations & Theses A&I. (UMI No. 27737103). [Google Scholar]
- Sobell LC, & Sobell MB (1995). Alcohol consumption measures. In Allen JP & Wilson VB (Eds.), Assessing alcohol problems: A guide for clinicians and researchers (Vol. 2, pp. 75–99). [Google Scholar]
- StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2019). Results from the 2018 National Survey on Drug Use and Health: Detailed tables. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/ [Google Scholar]
- Tanner-Smith EE, & Lipsey MW (2014). Identifying baseline covariates for use in propensity scores: A novel approach illustrated for a nonrandomized study of recovery high schools. Peabody Journal of Education, 89(2), 183–196. doi: 10.1080/0161956X.2014.895647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner-Smith EE, Finch AJ, Hennessy EA, & Moberg DP (2018). Who attends recovery high schools after substance use treatment? A descriptive analysis of school aged youth. Journal of Substance Abuse Treatment, 89, 20–27. doi: 10.1016/j.jsat.2018.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner-Smith EE, Finch AJ, Hennessy EA, & Moberg DP (2019). Effects of recovery high school attendance on students’ mental health symptoms. International Journal of Mental Health and Addiction, 17(2), 181–190. doi: 10.1007/s11469-017-9863-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thornberry TP, & Krohn MD (2000). The self-report method for measuring delinquency and crime. In Measurement and Analysis of Crime and Justice: Criminal Justice, vol. 4 (pp. 33–83). Washington, DC: National Institute of Justice, Office of Justice Programs, U.S. Department of Justice. [Google Scholar]
- Titus JC, Feeney T, Smith DC, Rivers TL, Kelly LL, & Dennis MD (2013). GAIN-Q3 3.2: Administration, clinical interpretation, and brief intervention. Normal (IL): Chestnut Health Systems. http://gaincc.org/GAINQ3 [Google Scholar]
- Utržan DS, & Piehler TF (2016). Peer Contagion/Deviancy. In Lebow J, Chambers A, & Breunlin DC (Eds.), Encyclopedia of Couple and Family Therapy. New York, NY: Springer. [Google Scholar]
- Weimer DL, Moberg DP, French F, Tanner-Smith EE, & Finch AJ (2019). Net benefits of recovery high schools: Higher cost but increased sobriety and educational attainment. Journal of Mental Health Policy and Economics, 22(3), 109–120. [PMC free article] [PubMed] [Google Scholar]
- White W, & Finch A (2006). The recovery school movement: Its history and future. Counselor, 7(2), 54–58. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.