

Hepatitis B core antibody (HBcAb) is the first antibody to appear following acute hepatitis B infection and will persist in high levels following resolution of infection and in chronically infected patients. Resolved infection is generally recognized by the presence of antibody to hepatitis B surface antigen (HBsAb) in the serum, whereas in chronic infection hepatitis B surface antigen (HBsAg) itself is typically present.
Isolated HBcAb, which is defined as positive HBcAb with undetectable HBsAg and HBsAb, may occur in any of several clinical situations.1 It may be the only serum marker of acute hepatitis B infection during the so-called “window phase” between disappearance of HBsAg and appearance of HBsAb. It may also represent a remote resolved infection with the decline of HBsAb to undetectable levels or ongoing chronic infection with HBsAg that is escaping detection, either because of low levels of HBsAg or because of mutations in the protein that render it undetectable using certain diagnostic assays. It rarely represents a false-positive test. Acute hepatitis B virus (HBV) infection is often recognized by its clinical presentation, and repeat testing after several weeks will generally detect the appearance of HBsAb. The other clinical possibilities are not easily distinguished on routine serological testing but may have important consequences, particularly in situations of chronic infection with no detection of HBsAg.
Cost efficacy considerations led to a recent change in the routine heptatitis B screening algorithm at the Sir Mortimer B. Davis–Jewish General Hospital, a tertiary care, 637-bed teaching hospital in Montreal. Patients are now evaluated initially with serum HBcAb testing. A negative HBcAb test result is reported as HBV-negative, and a positive result is followed by testing for HBsAg and, if this result is negative, HBsAb. HBsAg-positive sera are tested for hepatitis B e antigen (HBeAg) and hepatitis B e antibody (HBeAb).
Between June 1999 and March 2000, 4121 individual patients who were not pregnant were screened for HBV using HBcAb as the initial test. Of these, 3273 patients tested negative (79%), and 848 patients tested positive (21%) for HBcAb. Because there was an insufficient number of samples, 24 HBcAb-positive patients were excluded from further testing. Of the remaining 824 patients, 175 (21%) tested positive for HBsAg and 649 (79%) tested negative. The 649 HBsAg-negative patients were tested for HBsAb. Of these, 446 (69%) had a titre of more than 10 IU (positive), 81 patients (12%) had a titre of less than 1 IU (negative) and 122 patients (19%) had a value ranging between 1.0 and 10 IU (low level). Therefore, 81 (2.0%) of 4121 patients screened during this 10-month period had HBcAb as the only positive marker of infection. Among HBcAb-positive patients, at least 81 (10%) of 848 had both undetectable HBsAg and HBsAb.
Isolated HBcAb has been reported in up to 20% of patients tested.2,3,4,5,6 Dickson and colleagues demonstrated the importance of this entity in the post–liver transplant setting. De novo hepatitis B infection developed in 18 of 23 recipients of liver grafts from HBcAb-positive donors (78%), compared with 3 of 651 recipients of HBcAb-negative donor grafts (0.5%). All donors were negative for HbsAg.7 This illustrates the potential for active hepatitis B infection in patients with isolated HBcAb, particularly in the context of immunosuppression. Among patients with chronic hepatitis C infection and isolated HBcAb, HBV viral sequences are frequently found in the liver.8,9
The presence of isolated HBcAb in a context other than acute HBV infection may relate to the decay of HBsAb levels in patients with remote resolved infection or HBsAg that evades serological detection.10 The detection of HBsAg may be affected by the assay used, especially if a monoclonal capture antibody is used.11 HBV envelope escape mutations have been described in individuals vaccinated with recombinant HBV vaccine, although this phenomenon so far appears to be uncommon.11
It is most important to rule out ongoing chronic HBV infection in the setting of isolated HBcAb, in order to treat patients appropriately and protect their household and sexual contacts. One strategy that has emerged is the use of HBV vaccination in the diagnosis and management of patients with isolated HbcAb.12,13 The main use of vaccination is to differentiate individuals with resolved infection and a low level of HBsAb from chronically infected subjects with low-level viremia or mutated HBsAg, and from false-positive HBcAb results, as proposed in Fig. 1. Patients with resolved infection and subdetectable HBsAb would be expected to display an anamnestic response to HBV vaccination, with protective levels of antibody developing after a single dose of vaccine.12,13
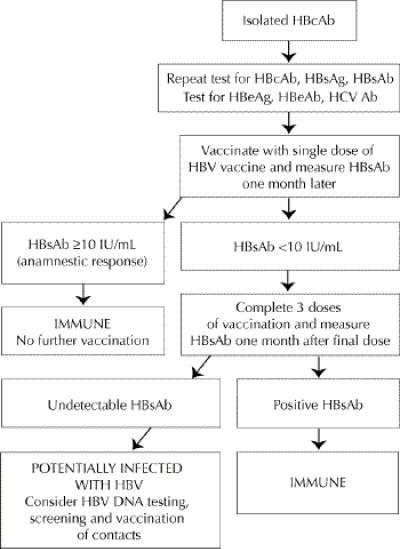
Fig. 1: Suggested algorithm for evaluation of patients with isolated hepatitis B core antibody (HBcAb). HBsAg = hepatitis B surface antigen, HBsAb = antibody to hepatitis B surface antigen, HBeAg = hepatitis B e antigen, HBeAb = hepatitis B e antibody, HCV Ab = antibody to hepatitis C virus, HBV = hepatitis B virus.
Chronically infected patients would not be expected to respond to the vaccine with the development of HBsAb. These patients have been labelled as “cryptic HBV carriers,” and testing for HBV DNA by sensitive polymerase chain reaction (PCR) techniques (but not necessarily the direct detection techniques in general clinical use) is positive in the majority of patients.14 With false-positive HBcAb results, normal response to vaccination has been demonstrated after a full 3-dose course.14 It may also be useful to test for HBeAg and HBeAb in patients with isolated HBcAb. The absence of both HBeAg and HBeAb would be anticipated in patients with false-positive HBcAb results.
We have found that in an urban North American teaching hospital isolated HBcAb is a relatively frequent phenomenon. These patients may have otherwise undetectable chronic HBV infection and should be investigated further. The application of the HBV vaccination strategy outlined here will identify patients with resolved infections and false-positive results for whom no specific follow-up is required. Those patients with isolated HBcAb who fail to develop HBsAb after a standard course of HBV vaccination should be considered to be potentially chronically infected with the virus, which should trigger appropriate public and personal health measures.
Footnotes
This article has been peer reviewed.
Competing interests: None declared.
Correspondence to: Dr. Averell H. Sherker, Director, Liver Center, Washington Hospital Center, 110 Irving St. NW, Washington DC 20010, USA; fax 202 877 8163; A.H.Sherker@medstar.net
References
- 1.Krugman S, Hoofnagle JH, Gerety RJ, Kaplan PM, Gerin JL. Viral hepatitis type B. DNA polymerase activity and antibody to hepatitis B core antigen. N Engl J Med 1974;290:1331-5. [DOI] [PubMed]
- 2.McMahon BJ, Parkinson AJ, Helminiak C, Wainwright RB, Bulkow L, Kellerman-Douglas A, et al. Response to hepatitis B vaccine of persons positive for antibody to hepatitis B core antigen. Gastroenterology 1992;103(2):590-4. [DOI] [PubMed]
- 3.Hu M, Schenzle D, Deinhardt F, Scheid R. Epidemiology of hepatitis A and B in Shanghai area: prevalence of serum markers. Am J Epidemiol 1984; 120: 404-13. [DOI] [PubMed]
- 4.Hadler SC, Murphy BL, Schable CA, Heyward WL, Francis DP, Kane MA. Epidemiological analysis of the significance of low positive test results for antibody to hepatitis B surface and core antigens. J Clin Microbiol 1984;19:521-5. [DOI] [PMC free article] [PubMed]
- 5.Feret E, Larauze B, Diop B, Sow M, London WT, Blumberg BS. Epidemiology of hepatitis B virus infection in the rural community of Tip, Senegal. Am J Epidemiol 1987;125:140-9. [DOI] [PubMed]
- 6.Lok ASF, Lai CL, Wu PC. Prevalence of isolated antibody to hepatitis B core antigen in an area endemic for hepatitis B virus infection: implications in hepatitis B vaccination programs. Hepatology 1987;8:766-70. [DOI] [PubMed]
- 7.Dickson RC, Everhart JE, Lake JR, Wei Y, Seaberg EC, Wiesner RH, et al. Transmission of hepatitis B by transplantation of livers from donors positive for antibody to hepatitis B core antigen. Gastroenterology 1997;113(5):1668-74. [DOI] [PubMed]
- 8.Cacciola I, Pollicino T, Squadrito G, Cerenzia G, Orlando ME, Raimondo G. Occult hepatitis B virus infection in patients with chronic hepatitis C liver disease. N Engl J Med 1999;341:22-6. [DOI] [PubMed]
- 9.Koike K, Kobayashi M, Gondo M, Hayashi I, Osuga T, Takada S. Hepatitis B virus DNA is frequently found in liver biopsy samples from hepatitis C virus infected chronic hepatitis patients. J Med Virol 1998;54:249-55. [PubMed]
- 10.Carman WF, Thomas HC. Genetic variation in hepatitis B virus. Gastroenterology 1992;102:711-9. [DOI] [PubMed]
- 11.Carman WF, Korula J, Wallace L, MacPhee R, Mimms L, Decker R. Fulminant reactivation of hepatitis B due to envelope protein mutant that escaped detection by monoclonal HbsAg ELISA. Lancet 1995;345:1406-7. [DOI] [PubMed]
- 12.McIntyre A, Nimmo GR, Wood GM, Tinniswood RD, Kerlin P. Isolated hepatitis B core antibody — can response to hepatitis B vaccine help elucidate the cause? Aust N Z J Med 1992;22(1):19-22. [DOI] [PubMed]
- 13.Draelos M, Morgan T, Schifman RB, Sampliner RE. Significance of isolated antibody to hepatitis B core antigen determined by immune response to hepatitis B vaccination. JAMA 1987;258:1193-5. [PubMed]
- 14.Luo KX, Zhou R, He Chao, Liang ZS, Jiang S. Hepatitis B virus DNA in sera of virus carriers positive exclusively for antibodies to the hepatitis B core antigen. J Med Virol 1991;35:55-9. [DOI] [PubMed]