

Key Points
Question
Is tracheostomy associated with COVID-19 outcomes among patients or SARS-CoV-2 transmission among health care professionals (HCPs)?
Findings
In this systematic review and meta-analysis, 69 nonrandomized studies including 4669 total patients were identified that evaluated tracheostomy in COVID-19. While the use of enhanced personal protective equipment in tracheostomy in patients with COVID-19 was associated with low SARS-CoV-2 transmission among HCPs and early tracheostomy was associated with reduced intensive care unit length of stay but not time to mechanical ventilation wean or decannulation, there was no difference in mortality between surgical and percutaneous tracheostomy.
Meaning
This study suggests that tracheostomy is a relatively effective and safe treatment for patients with COVID-19 and and also safe for the HCPs performing the procedures who are wearing personal protective equipment, but the conclusions are limited by the observational nature of included studies.
Abstract
Importance
Approximately 5% to 15% of patients with COVID-19 require invasive mechanical ventilation (IMV) and, at times, tracheostomy. Details regarding the safety and use of tracheostomy in treating COVID-19 continue to evolve.
Objective
To evaluate the association of tracheostomy with COVID-19 patient outcomes and the risk of SARS-CoV-2 transmission among health care professionals (HCPs).
Data Sources
EMBASE (Ovid), Medline (Ovid), and Web of Science from January 1, 2020, to March 4, 2021.
Study Selection
English-language studies investigating patients with COVID-19 who were receiving IMV and undergoing tracheostomy. Observational and randomized clinical trials were eligible (no randomized clinical trials were found in the search). All screening was performed by 2 reviewers (P.S. and M.L.). Overall, 156 studies underwent full-text review.
Data Extraction and Synthesis
We performed data extraction in accordance with Meta-analysis of Observational Studies in Epidemiology guidelines. We used a random-effects model, and ROBINS-I was used for the risk-of-bias analysis.
Main Outcomes and Measures
SARS-CoV-2 transmission between HCPs and levels of personal protective equipment, in addition to complications, time to decannulation, ventilation weaning, and intensive care unit (ICU) discharge in patients with COVID-19 who underwent tracheostomy.
Results
Of the 156 studies that underwent full-text review, only 69 were included in the qualitative synthesis, and 14 of these 69 studies (20.3%) were included in the meta-analysis. A total of 4669 patients were included in the 69 studies, and the mean (range) patient age across studies was 60.7 (49.1-68.8) years (43 studies [62.3%] with 1856 patients). We found that in all studies, 1854 patients (73.8%) were men and 658 (26.2%) were women. We found that 28 studies (40.6%) investigated either surgical tracheostomy or percutaneous dilatational tracheostomy. Overall, 3 of 58 studies (5.17%) identified a small subset of HCPs who developed COVID-19 that was associated with tracheostomy. Studies did not consistently report the number of HCPs involved in tracheostomy. Among the patients, early tracheostomy was associated with faster ICU discharge (mean difference, 6.17 days; 95% CI, −11.30 to −1.30), but no change in IMV weaning (mean difference, −2.99 days; 95% CI, −8.32 to 2.33) or decannulation (mean difference, −3.12 days; 95% CI, −7.35 to 1.12). There was no association between mortality or perioperative complications and type of tracheostomy. A risk-of-bias evaluation that used ROBINS-I demonstrated notable bias in the confounder and patient selection domains because of a lack of randomization and cohort matching. There was notable heterogeneity in study reporting.
Conclusions and Relevance
The findings of this systematic review and meta-analysis indicate that enhanced personal protective equipment is associated with low rates of SARS-CoV-2 transmission during tracheostomy. Early tracheostomy in patients with COVID-19 may reduce ICU stay, but this finding is limited by the observational nature of the included studies.
This systematic review and meta-analysis examines the association of tracheostomy with COVID-19 patient outcomes and the risk of SARS-CoV-2 transmission among health care professionals.
Introduction
As of March 25, 2021, more than 125 million people worldwide have received a diagnosis of COVID-19, and more than 2.7 million people have died.1 COVID-19 transmission occurs via SARS-CoV-2 and is associated with pneumonia, coagulopathy, and multiorgan failure.2 Up to 70% of patients with COVID-19 who are admitted to critical care units require invasive mechanical ventilation (IMV), which is typically secondary to the development of acute respiratory distress syndrome.3 In patients who require prolonged IMV, evidence is conflicting regarding the association of early tracheostomy with mortality and duration of intensive care unit (ICU) stay and IMV.4,5
However, tracheostomy is an aerosol-generating medical procedure (AGMP) and can increase the risk of viral disease transmission.6 Several COVID-19 guidelines recommended performing tracheostomy after 14 days of IMV to reduce the risk of SARS-CoV-2 transmission.7,8 The purpose of this study is to evaluate the association of tracheostomy with clinical outcomes in COVID-19 and the risk of SARS-CoV-2 transmission among health care professionals (HCPs).
Methods
The study protocol was registered in PROSPERO (CRD42020208129) and was reported in accordance with reporting guidelines for Meta-analysis for Observational Studies in Epidemiology.9 Because this study is a systematic review, it was determined that institutional review board approval was not required.
Study Eligibility
Eligibility criteria included full-text primary research articles that reported clinical outcomes in adult (age, ≥18 years) patients with COVID-19 who were receiving IMV and identified as candidates for tracheostomy. Studies included surgical tracheostomy (ST) and percutaneous dilatational tracheostomy (PDT). We included studies that evaluated clinical end points selected a priori, including mortality, ICU length of stay, and time to decannulation or ventilation weaning. We also included studies that reported SARS-CoV-2 transmission among HCPs. Eligible study designs included observational cohort studies, case series (n ≥ 5), and randomized clinical trials.
Search Methods
Two authors (P.S. and M.L.) searched Cochrane, EMBASE (Ovid), Medline (Ovid), and Web of Science from January 1, 2020, until March 4, 2021, with no restrictions as to publication type. Because of the rate of publishing in COVID-19 research, we included only English-language studies to expedite analysis. The search strategy is included in the eAppendix in the Supplement. We screened the reference lists of included studies. We also searched ClinicalTrials.gov, the Current Controlled Trials (ISRCTN Register), and PROSPERO database.
Study Selection and Data Abstraction
Title and abstract screening were completed in duplicate by 2 reviewers (P.S. and M.L.). Full-text screening of studies was completed by 2 reviewers (P.S. and M.L.). Conflicts were resolved by a third reviewer (T.M.). All studies that met eligibility criteria were included in the systematic review. Data abstraction was performed by 2 independent reviewers (P.S. and M.L.). A data abstraction form was created, reviewed, and piloted by all authors. We abstracted study details, including publication date, location of publication, and study design. We also abstracted patient demographic and clinical information and SARS-CoV-2 HCP transmission findings. We included observational studies in the meta-analysis that investigated 1 or more of the aforementioned clinical end points. We also required that studies report clinical end points in a manner that allowed for pooling, and more than 2 studies were needed to perform a meta-analysis. We excluded studies from the meta-analysis that were published by the same group or included patients who were recruited over the same period and/or at identical institutions. Interreviewer agreement was evaluated using the Cohen κ.
Risk-of-Bias Assessment
We used the ROBINS-I tool, which has been validated in nonrandomized studies, to perform risk-of-bias (RoB) assessment for the studies included within this meta-analysis.10 Total RoB score for the ROBINS-I tool was evaluated as low, moderate, serious, or critical. Risk-of-bias assessment was performed by 2 reviewers (P.S. and M.L.). We were unable to perform funnel plot analyses because of the small number of included studies.
Statistical Analysis
We used a descriptive analysis to evaluate study characteristics. We performed a meta-analysis that compared tracheostomy vs no tracheostomy, early vs late tracheostomy, and surgical vs percutaneous tracheostomy. We defined early tracheostomy as 14 days or less and late tracheostomy as longer than 14 days based on the mean or median time from intubation to tracheostomy. We used a random-effects model, and statistical heterogeneity was evaluated using I2. We measured odds ratios (ORs) for clinical end points and 95% confidence intervals to characterize statistical errors. Statistical analyses were preformed using Microsoft Excel (Microsoft) and Revman, version 5.3 (Cochrane).
Results
The database search generated 1877 citations, of which 156 (8.3%) underwent full-text review (Figure 1). Overall, 69 studies (N = 4669 patients) were included within the qualitative synthesis, and 14 studies were included in the meta-analyses.11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79 Interrater reliability between independent reviewers was 0.81 and 0.64 for the abstract screening and full-text stages, respectively.
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-analyses Flow Diagram of Included Studies.

Study Characteristics
Most of the included studies were published in the US (21 [30.4%]), UK (13 [18.8%]), or Italy (12 [17.4%]) (eTable in the Supplement). We found that 58 studies (84.1%) were observational, of which 38 (65.5%) were retrospective and 16 (28.1%) were prospective. Furthermore, 58 studies (84.1%) were performed at single hospital sites, which were mainly tertiary care centers. Overall, 28 studies (40.6%), including 3373 patients, investigated either ST or PDT. We found that 22 studies (31.9%), including 497 patients, investigated ST alone and 15 studies (21.7%), including 594 patients, reported PDT alone. The remaining 4 studies (5.8%) did not report the type of tracheostomy. We identified 7 studies that may have included overlapping patient cohorts: 2 studies by Botti et al,21,22 3 studies by Takhar et al,66,67,79 and 2 studies by Kwak and colleagues and Angel et al.16,37
The mean (range) patient age across studies was 60.7 (49.1-68.8) years (43 studies [62.3%] with 1856 patients). We found that in all studies, 1854 patients (73.8%) were men and 658 (26.2%) were women. The mean (range) body mass index (BMI; calculated as weight in kilograms divided by height in meters squared) was 30.2 (26.9–33; 20 studies [29.0%] with 626 patients). Diabetes and hypertension were most commonly reported baseline comorbidities (44 studies [63.8%]). We found that 53 studies (76.8%) included only COVID-19–positive patients. Eight studies included patients with COVID-19–positive, negative, or unknown status and 8 studies did not report COVID-19 status. One study only included patients who had 2 negative COVID-19 nasopharyngeal swab (NPS) results before tracheostomy.51 There were 36 studies (52.2%) that studied late tracheostomy, 15 (21.7%) that studied early tracheostomy, 12 (17.4%) that did not report the timing of tracheostomy from intubation, and 6 (8.7%) that studied early and late tracheostomy.
SARS-CoV-2 Transmission Among HCPs Following Tracheostomy
We identified 58 studies (84.1%) that investigated SARS-CoV-2 transmission among HCPs, in which 26 studies (44.8%) reported COVID-19 status via NPS and/or blood testing and 32 (55.2%) either used clinical symptoms or did not report testing methods. Studies primarily assessed HCPs for COVID-19 infection within 4 weeks of being involved in a tracheostomy. Overall, we found that 55 studies (94.8%) did not find that any HCPs tested positive or developed COVID-19 symptoms following tracheostomy. One study of PDT alone found that 7 of 91 HCPs (7.7%) who were involved in early tracheostomy had either a positive SARS-CoV-2 test or NPS result after performing the tracheostomies; however, this was similar to 6 of 52 HCPs (11.5%) who were not involved in tracheostomy in this study.58 Another study of ST that did not specifically investigate SARS-CoV-2 transmission among HCPs found that 1 staff member, who was involved in tracheostomy care, developed COVID-19 symptoms.62 A third study of ST and PDT found that 1 of 30 otolaryngology–head and neck surgery physicians involved in performing tracheostomy contracted COVID-19.37 Two (of 3) of these studies reported performing tracheostomies a mean of less than 14 days from intubation. The timing of SARS-CoV-2 testing for HCPs was reported in 8 studies that monitored HCPs for COVID-19 status within a range of 14 to 30 days from tracheostomy. The type of personal protective equipment (PPE) that was used by HCPs was reported in 41 of 69 studies (59.4%). Of these, 13 of 41 (31.7%) reported using either N95 or equivalent masks, 12 of 41 (29.3%) using N99 or equivalent masks, 11 of 41 studies (26.8%) powered air-purifying respirators (PAPRs), and 5 of 41 (12.2%) did not specify type of PPE. We found that 8 of 69 studies (11.6%) performed tracheostomies in a negative-pressure room, while the remaining studies primarily performed ST in an operating theater and PDT at the bedside. Studies also described procedures to reduce aerosol generation during tracheostomy.
RoB Analysis
We used the ROBINS-I tool to perform an RoB analysis for 14 studies that were included in the meta-analysis (Table14,21,23,33,35,38,58,59,60,66,67,73,74,78). Of these, 5 studies (35.7%) had a serious RoB, 5 studies (37.5%) had a moderate RoB, and 4 studies (28.6%) had a low RoB. Notable bias was identified in the confounders and patient selection domains, largely because of the nonrandomized nature of studies and lack of cohort matching. Missing data, outcome measurements, and report result domains demonstrated less RoB because of the objective clinical end points.
Table. Risk-of-Bias Assessment in 14 Studies Using ROBINS-I.
| Study | ROBINS-I domains | |||||||
|---|---|---|---|---|---|---|---|---|
| Confounders | Participant selection | Interventions | Deviation from intended intervention | Missing data | Outcome measurement | Reported result | Overall | |
| Avilés-Jurado et al,14 2020 | Moderate | Low | Low | Low | Low | Moderate | Moderate | Low |
| QEHB CAT,24 2020 | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Botti et al,21 2021 | Serious | Moderate | Serious | Unclear | Unclear | Moderate | Serious | Serious |
| Glibbery et al,33 2020 | Serious | Moderate | Moderate | Low | Moderate | Serious | Moderate | Moderate |
| Krishnamoorthy et al,35 2020 | Moderate | Serious | Serious | Unclear | Serious | Moderate | Serious | Serious |
| Long et al,38 2020 | Serious | Serious | Low | Low | Moderate | Moderate | Serious | Moderate |
| Rosano et al,58 2020 | Moderate | Moderate | Low | Unclear | Low | Low | Moderate | Moderate |
| Rovira et al,59 2021 | Moderate | Moderate | Low | Unclear | Low | Low | Moderate | Low |
| Sancho et al,60 2020 | Moderate | Serious | Low | Unclear | Low | Low | Low | Low |
| Takhar et al,66 2020 | Serious | Serious | Low | Unclear | Low | Low | Low | Low |
| Takhar et al,67 2020 | Serious | Serious | Moderate | Low | Moderate | Serious | Serious | Serious |
| Yeung et al,73 2020 | Serious | Serious | Moderate | Unclear | Moderate | Serious | Serious | Serious |
| Zhang et al,74 2020 | Critical | Critical | Serious | Unclear | Serious | Serious | Serious | Serious |
| Zuazua-Gonzalez et al,78 2020 | Serious | Serious | Moderate | Unclear | Low | Low | Moderate | Moderate |
Abbreviation: QEHB CAT, Queen Elizabeth Hospital Birmingham COVID-19 airway team.
Tracheostomy and No Tracheostomy
A decreased risk of mortality in patients with COVID-19 who underwent tracheostomy (96 of 342 [38.1%]) was observed compared with those who did not undergo tracheostomy (140 of 238 [58.8%]; OR, 0.26; 95% CI, 0.09-0.77; n = 580 patients; 5 studies [7.2%]; Figure 2). However, statistical heterogeneity was high (I2 = 87%). These studies evaluated either ST and/or PDT. The no tracheostomy groups in these studies consisted of critically ill patients with COVID-19 who were not treated with tracheostomy. Despite both groups being qualitatively similar in these studies, they were not defined methodologically as matched cohorts. The mean (SD) age was 60.4 (5.2) and 58.7 (3.8) years in the tracheostomy and no tracheostomy groups, respectively. The mean (SD) BMI was 29.9 (1.6) and 28.9 (0.9) (3 studies [4.3%]) in the tracheostomy and no tracheostomy groups, and Sequential Organ Failure Assessment (SOFA) and/or APACHE II scores were reported in 4 studies (5.8%). Two studies (2.9%) reported significantly higher baseline SOFA and/or APACHE II scores in the tracheostomy compared with no tracheostomy group.60,66 Hypertension was the most common medical comorbidity in all studies. No study commented on the presence of therapeutic anticoagulation at the time of tracheostomy. No study identified any patient in either group who required extracorporeal membrane oxygenation. The timing of tracheostomy from intubation ranged from 6 to 16 days, and follow-up ranged from 28 to 30 days posttracheostomy (3 studies [4.3%]).
Figure 2. Mortality in 5 Studies For Those Who Received Tracheostomy vs Did Not Receive Tracheostomy.
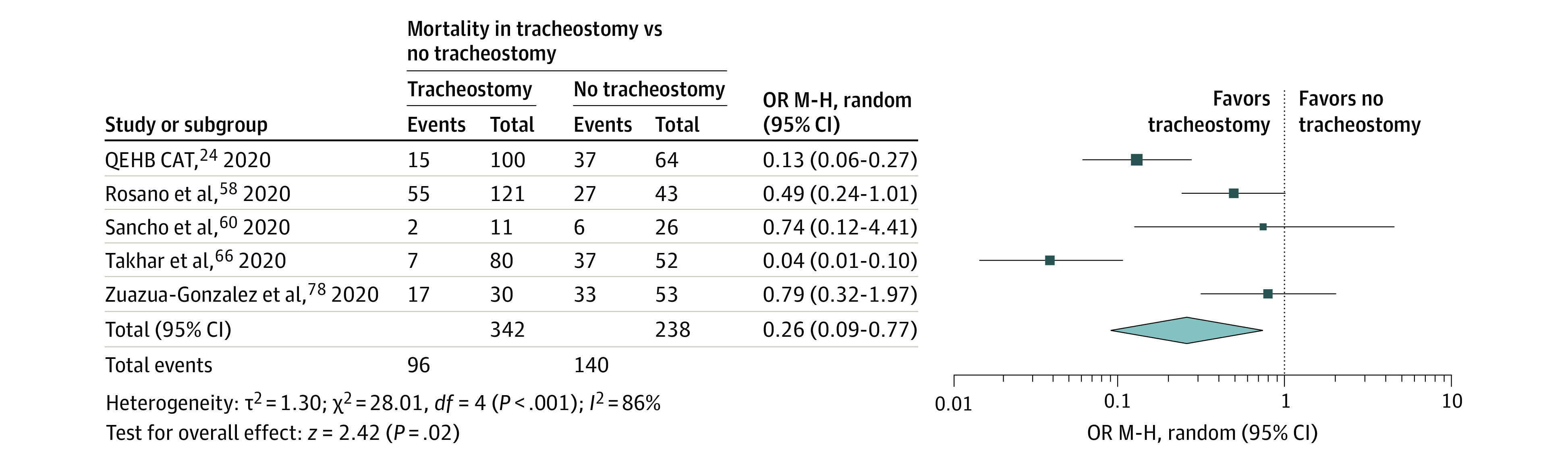
M-H indicates Mantel-Haenszel; QEHB CAT, Queen Elizabeth Hospital Birmingham COVID-19 airway team; OR, odds ratio; random, random effects.
Early and Late Tracheostomy
When evaluating tracheostomy before and after 14 days of intubation, the mean discharge from ICU improved in early compared with late tracheostomy within 209 patients (mean difference, −6.17 days; 95% CI, −11.30 to −1.30) (Figure 3A). In 259 patients who underwent either ST or PDT, the mean time to IMV weaning (mean difference, −2.99 days; 95% CI, −8.32 to 2.33) and decannulation (mean difference, −3.12 days; 95% CI, −7.35 to 1.12) did not differ between the early and late tracheostomy groups (Figure 3, B and C). Statistical heterogeneity was high in these comparisons (I2 = 70%-91%). Two studies (2.9%) investigated either ST and/or PDT, while Avilés-Jurado et al14 investigated only ST and Takhar et al67 investigated only PDT. Early tracheostomy was defined as less than 14 days from intubation in 3 studies and less than <10 days in 1 study.14 Two studies (2.9%) that reported baseline characteristics did not identify any clinically important differences in the early vs late tracheostomy group.14,67
Figure 3. Mean Times in Early vs Late Tracheostomy.
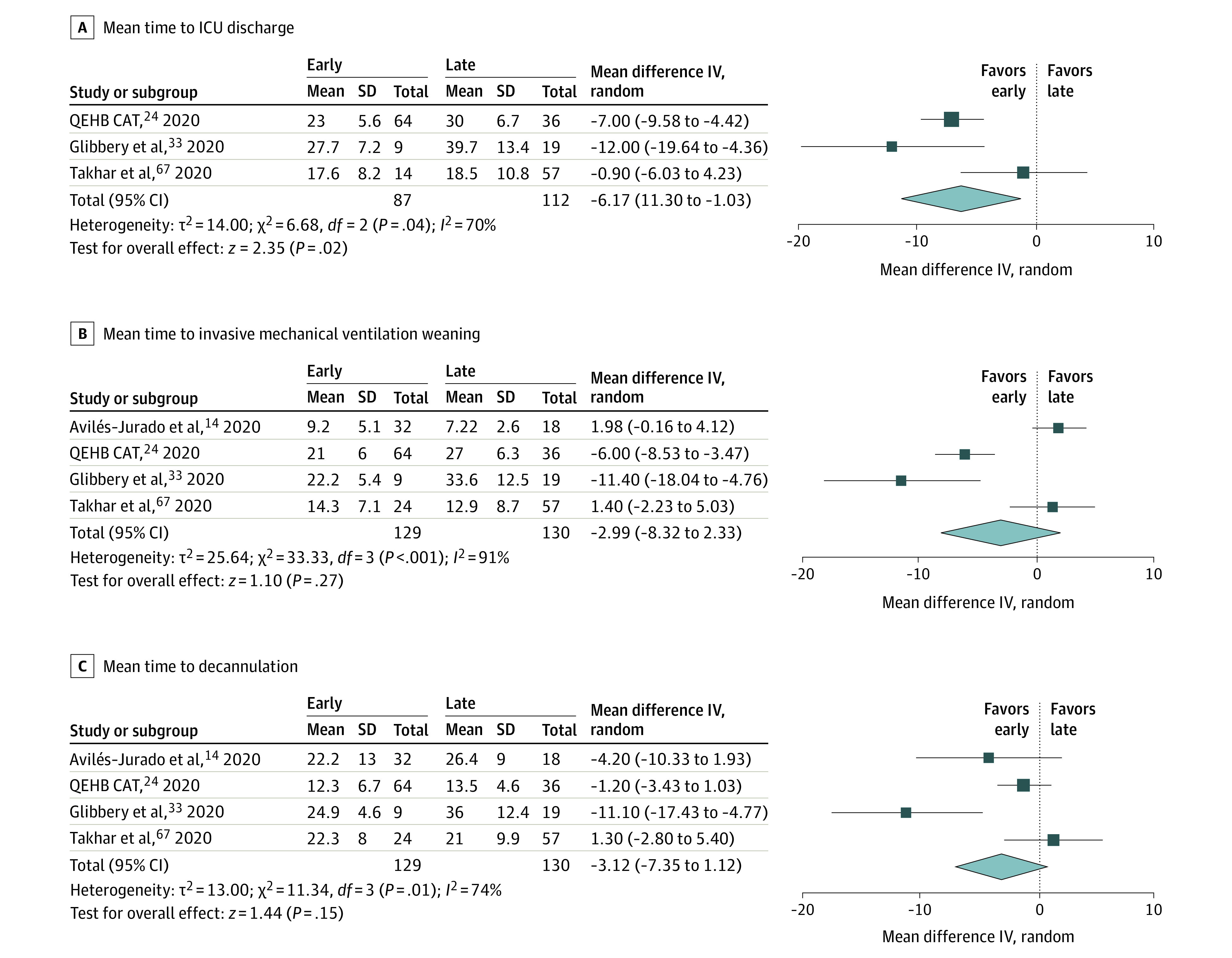
Mean times of intensive care unit (ICU) discharge (4 studies) (A), invasive mechanical ventilation weaning ( 4 studies) (B), and decannulation (3 studies) (C) in early vs late tracheostomy. IV indicates intravenous; QEHB CAT, Queen Elizabeth Hospital Birmingham COVID-19 airway team; random, random effects.
PDT and ST
We found that there was no difference in mortality in patients with COVID-19 who were undergoing either PDT (36 of 287 [12.5%]) or ST (32 of 239 [13.4%]) (OR, 1.00; 95% CI, 0.49-2.04; n = 526 patients; Figure 4A). We also found that there was no difference in complication rates between PDT (42 of 266 [15.8%]) and ST (51 of 203 [25.1%]) (OR, 0.66; 95% CI, 0.40-1.07; n = 469; Figure 4B). Statistical heterogeneity was low in both analyses (I2 = 0%-27%). Despite not being matched cohort studies, patients were demographically and clinically similar across types of tracheostomy. The time to tracheostomy from intubation ranged from 16.8 to 25.0 days. The most common comorbidity was hypertension. Five studies (7.2%) commented on the presence of therapeutic anticoagulation at the time of tracheostomy. Zhang et al74 demonstrated considerable perioperative complication rates (ie, PDT = 16.7%; ST = 40%) in both types of tracheostomy, which is likely because of the low number of tracheostomies that were performed. The follow-up period in these studies ranged from 14 days or less to a maximum of 110 days from intubation. In 13 studies of ST that reported perioperative complications, perioperative hemorrhage was the most commonly reported. One study reported bleeding that required revision surgery, while 3 studies identified anticoagulation status at the time of surgery.36,45,46 In 13 PDT studies that reported perioperative complications, the most common complication was perioperative hemorrhage. Two studies reported bleeding that required revision surgery and/or transfusion, and 4 studies reported anticoagulation status at the time of surgery.16,34,48,64,67
Figure 4. Mortality in 6 Studies and Perioperative Complications in 5 Studies in Surgical vs Percutaneous Dilatational Tracheostomy.
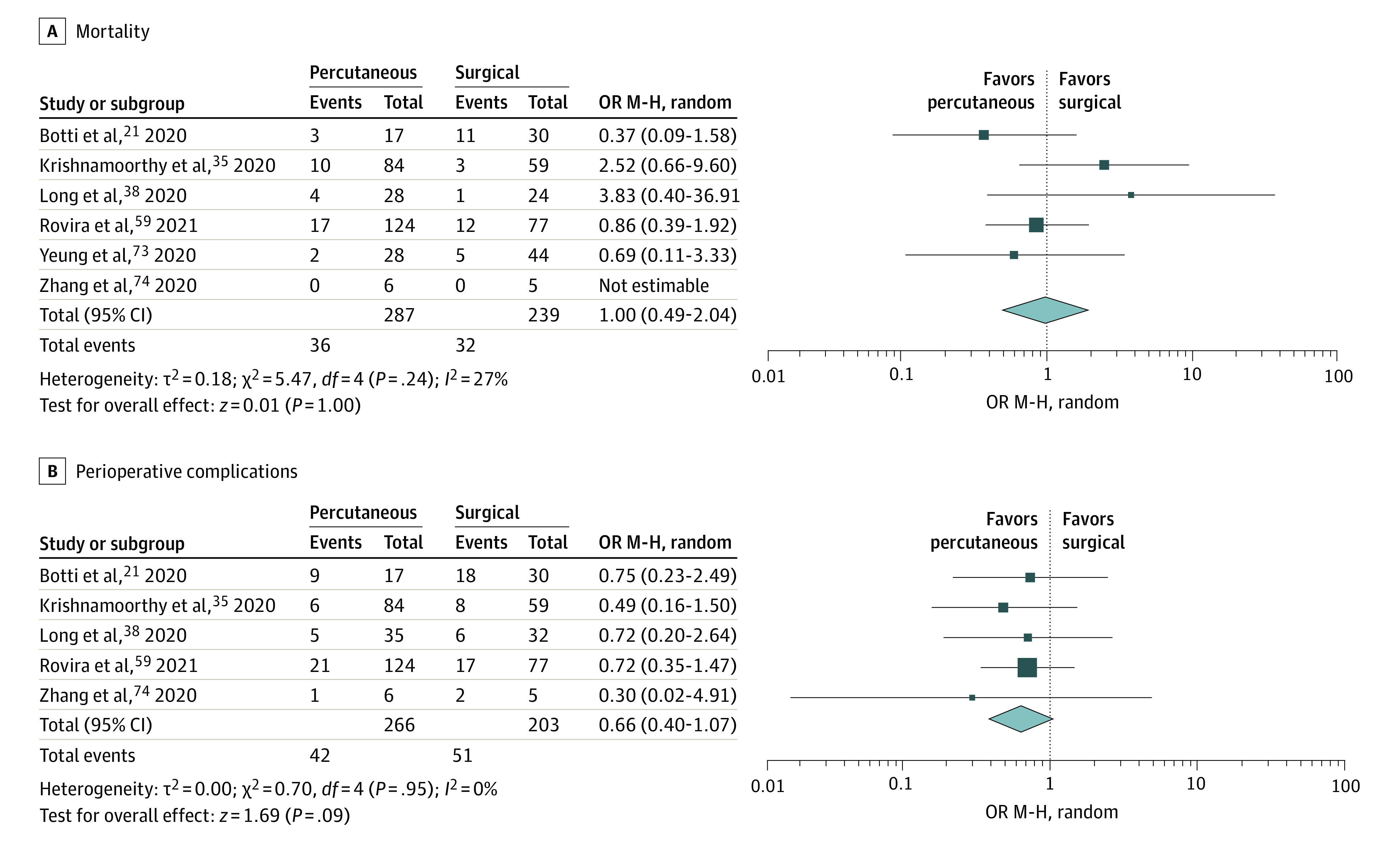
M-H indicates Mantel-Haenszel; OR, odds ratio; random, random effects.
Discussion
Health care systems worldwide continue to respond to the evolving COVID-19 pandemic. Several national COVID-19 guidelines recommend performing tracheostomy after 14 days of IMV to reduce the risk of viral transmission because SARS-CoV-2 is more transmissible early in its course.8 In this study, tracheostomy was found to be associated with reduced mortality in patients with COVID-19; however, these observational findings are likely affected by confounders, selection bias, and a possible survivorship bias in patients who underwent delayed tracheostomy. We also found that early tracheostomy was associated with reduced ICU stay, but not with time to ventilation weaning or decannulation. Early tracheostomy has been shown to shorten ICU stay in critical care populations, but it does not carry a clear mortality benefit, and its clinical use remains controversial.4,80,81,82,83,84 One study has reported that tracheostomy less than 4 days from intubation may lead to improved clinical outcomes, but this has not been established in patients with COVID-19.85 The observed reduction in ICU stay may also be secondary to institutions that allow for patients who are receiving ventilation to be discharged from the ICU following tracheostomy. Benefits of early tracheostomy in COVID-19 may include improved sedation wean, fewer endotracheal intubation complications, and optimization of prolonged ventilation wean, but the evidence remains inconclusive.86 Therefore, surgeons must balance the possible benefits of early tracheostomy with the potential heightened risk of SARS-CoV-2 transmissibility in the earlier stages of COVID-19 infection.
We also reported no association between the type of tracheostomy and perioperative complications or mortality rates in COVID-19. Studies have shown similar trends in critically ill patients without COVID-19 who underwent ST or PDT.87,88 The perioperative complication rates for ST and PDT were 25.1% and 15.8%, respectively. These complication rates are similar to those published in the critical care literature, but are affected by patient- and study-specific factors.89,90,91 This difference in complication rates may be because of a lack of randomization, the likelihood for less stable patients to undergo ST, and likelihood for patients with a high BMI with a worse COVID-19 prognosis to undergo ST.92 We also confirmed that the most common tracheostomy complication was perioperative hemorrhage, which is often cited in the literature.93 The observed noteworthy perioperative bleeding risk may also be secondary to therapeutic anticoagulation in COVID-19, but reporting of coagulation status was not standardized and remains a notable confounder.94 Both ST and PDT appear to be relatively safe in the setting of COVID-19 and therefore should be selected by clinicians based on patient-specific and logistical factors, in addition to any risk of viral transmission.
Tracheostomy is associated with low rates of SARS-CoV-2 transmission among HCPs. However, viral transmission was investigated primarily using clinical symptoms, and given that up to 20% of patients with COVID-19 are asymptomatic, there may have been missed transmission events.95 A COVID-19 air sampling study suggested that tracheostomy less than 14 days from intubation may be associated with viral shedding within the surgical field and may be a higher transmission risk than delayed tracheostomy.96 A study reporting on otolaryngologists who contracted COVID-19 noted that disease transmission can occur via tracheostomy.97 Another recent study demonstrated low rates of SARS-CoV-2 transmission within tracheostomy irrespective of polymerase chain reaction status.98 Overall, while tracheostomy has not been demonstrated to be a high-risk procedure for SARS-CoV-2 transmission, further studies are needed to establish the role of timing in viral transmission within HCPs.6,99 The relative safety of tracheostomy in the COVID-19 population is likely associated with the use of aerosol-grade PPE. Studies have suggested that N95 respirators are sufficient for respiratory protection within AGMPs, while N99 or P100 are helpful in procedures with heightened risks for viral transmission.100 Powered air-purifying respirators have been shown to also be beneficial in AGMPs and improved wearer comfort, but they are also associated with communication issues, and inadequate training on their use may lead to self-contamination during doffing.101 Powered air-purifying respirators have shown superior protection (ie, 0% transmission) compared with N95 respirators (ie, 10% transmission) in a study of 58 participants who were exposed to influenza virus, but it is not known if this extends to SARS-CoV-2 transmission.102 A recent study suggests that SARS-CoV-2 viral aerosolization is not a high transmission risk in surgical cautery plume.103 Enhanced PPE is associated with reduced infectivity in COVID-19; however, surgical teams performing tracheostomy must select the timing of the procedure based on patient-specific factors and the conceptual risk of SARS-CoV-2 transmission.86 Recent directions in determining the risk of infectivity in patients with COVID-19 have been moving toward relying on the duration since the first positive RT-PCR test result or first date of symptoms.104,105 A recent publication has suggested that antibody titers may also serve as a useful measure for assessing infectivity in the tracheostomy population.98 It remains unclear how the effects of vaccination and variant SARS-CoV-2 strains will affect these evolving considerations.
Limitations
This study’s main limitation is the small number of and nonrandomized nature of included studies, which are prone to selection bias and heterogeneity.106 Therefore, these studies are unable to account for confounders in comparisons of the type and timing of tracheostomy, including age, BMI, comorbid conditions, coagulopathies, infection severity, and ventilatory settings. The RoB analysis demonstrated a serious level of bias in the confounders and participant selection domains of ROBINS-I tool because of the lack of randomization and cohort matching. The exclusion of non-English studies potentially precludes extrapolation of these findings to low- and middle-income countries that are burdened by COVID-19. We also cannot extend these SARS-CoV-2 transmission findings broadly to proceduralists or anesthetists during tracheostomy.
Conclusions
SARS-CoV-2 transmission is low in HCPs who perform tracheostomy using enhanced PPE. Early tracheostomy may be associated with reduced ICU length of stay, but further studies are needed to establish the importance of timing in optimizing clinical outcomes and minimizing viral transmission in COVID-19. Despite being limited by the quality of the current COVID-19 tracheostomy literature, these conclusions will inform future randomized clinical trials that evaluate the safety and effectiveness of tracheostomy in COVID-19.
eAppendix A. Ovid search strategy
eTable. Summary of all included studies (N = 69).
References
- 1.Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis. 2020;20(5):533-534. doi: 10.1016/S1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pascarella G, Strumia A, Piliego C, et al. COVID-19 diagnosis and management: a comprehensive review. J Intern Med. 2020;288(2):192-206. doi: 10.1111/joim.13091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Luo M, Cao S, Wei L, et al. Intubation, mortality, and risk factors in critically ill Covid-19 patients: a pilot study. J Clin Anesth. 2020;67:110039. doi: 10.1016/j.jclinane.2020.110039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Andriolo BN, Andriolo RB, Saconato H, Atallah AN, Valente O. Early versus late tracheostomy for critically ill patients. Cochrane Database Syst Rev. 2015;1:CD007271. doi: 10.1002/14651858.CD007271.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Meng L, Wang C, Li J, Zhang J. Early vs late tracheostomy in critically ill patients: a systematic review and meta-analysis. Clin Respir J. 2016;10(6):684-692. doi: 10.1111/crj.12286 [DOI] [PubMed] [Google Scholar]
- 6.Thamboo A, Lea J, Sommer DD, et al. Clinical evidence based review and recommendations of aerosol generating medical procedures in otolaryngology—head and neck surgery during the COVID-19 pandemic. J Otolaryngol Head Neck Surg. 2020;49(1):28. doi: 10.1186/s40463-020-00425-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chiesa-Estomba CM, Lechien JR, Calvo-Henríquez C, et al. Systematic review of international guidelines for tracheostomy in COVID-19 patients. Oral Oncol. 2020;108:104844. doi: 10.1016/j.oraloncology.2020.104844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bier-Laning C, Cramer JD, Roy S, et al. Tracheostomy during the COVID-19 pandemic: comparison of international perioperative care protocols and practices in 26 countries. Otolaryngol Head Neck Surg. 2020;194599820961985. [DOI] [PubMed] [Google Scholar]
- 9.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) Group. JAMA. 2000;283(15):2008-2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 10.Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi: 10.1136/bmj.i4919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ahmed Y, Cao A, Thal A, et al. Tracheotomy outcomes in 64 ventilated COVID-19 patients at a high-volume center in Bronx, NY. Laryngoscope. 2021. Published online January 7, 2021. doi: 10.1002/lary.29391 [DOI] [PubMed] [Google Scholar]
- 12.Ahn D, Lee GJ, Choi YS, et al. Timing and clinical outcomes of tracheostomy in patients with COVID-19. Br J Surg. 2021;108(1):e27-e28. doi: 10.1093/bjs/znaa064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aodeng S, Wang W, Chen Y, et al. Safety and efficacy of tracheotomy for critically ill patients with coronavirus disease 2019 (COVID-19) in Wuhan: a case series of 14 patients. Eur J Cardiothorac Surg. 2020;58(4):745-751. doi: 10.1093/ejcts/ezaa312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Avilés-Jurado FX, Prieto-Alhambra D, González-Sánchez N, et al. Timing, complications, and safety of tracheotomy in critically ill patients with COVID-19. JAMA Otolaryngol Head Neck Surg. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Aissaoui O, Nsiri A, Fehdi MA, Mouhaoui M, Alharrar R. Surgical tracheostomy in COVID-19 patients: report of 5 cases. Pan Afr Med J. 2020;35(suppl 2):55. doi: 10.11604/pamj.supp.2020.35.2.23615 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Angel L, Kon ZN, Chang SH, et al. Novel percutaneous tracheostomy for critically ill patients with COVID-19. Ann Thorac Surg. 2020;110(3):1006-1011. doi: 10.1016/j.athoracsur.2020.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bassily-Marcus A, Leibner ES, Kohli-Seth R. Tracheostomy for coronavirus disease 2019 patients: maintaining the standard of care. Crit Care Explor. 2020;2(8):e0190-e0190. doi: 10.1097/CCE.0000000000000190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bertini P, Forfori F, Bruschini L, et al. Percutaneous tracheostomy in COVID-19 critically ill patients: experience from 30 consecutive procedures. Int Arch Otorhinolaryngol. 2021;25(1):e135-e140. doi: 10.1055/s-0040-1718528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Betancourt-Ramirez A, Yelon JA, Boland P, Amaturo M. A technique to minimize aerosolization during percutaneous tracheostomy in COVID-19 patients. Am Surg. 2020;86(8):904-906. doi: 10.1177/0003134820943102 [DOI] [PubMed] [Google Scholar]
- 20.Bhavana K, S AS, Ouseph S, Suneha S, Prakash R, Bharti B. Modifying ways to perform ICU tracheostomies in COVID-19 patients: approach to a safe and secure method. Indian J Otolaryngol Head Neck Surg. 2020;1-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Botti C, Lusetti F, Peroni S, et al. The role of tracheotomy and timing of weaning and decannulation in patients affected by severe COVID-19. Ear Nose Throat J. 2021;100(2_suppl)(suppl 2):116S-119S. doi: 10.1177/0145561320965196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Botti C, Lusetti F, Neri T, et al. Comparison of percutaneous dilatational tracheotomy versus open surgical technique in severe COVID-19: complication rates, relative risks and benefits. Auris Nasus Larynx. 2020;S0385-8146(20)30296-0. doi: 10.1016/j.anl.2020.10.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Boujaoude Z, Madisi N, Patel B, Rachoin JS, Dellinger RP, Abouzgheib W. Safety and feasibility of a novel protocol for percutaneous dilatational tracheostomy in patients with respiratory failure due to COVID-19 infection: a single center experience. Pulm Med. 2021;2021:8815925. doi: 10.1155/2021/8815925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Queen Elizabeth Hospital Birmingham COVID-19 airway team . Safety and 30-day outcomes of tracheostomy for COVID-19: a prospective observational cohort study. Br J Anaesth. 2020;125(6):872-879. doi: 10.1016/j.bja.2020.08.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Briatore R, Aprile F, Roasio A, et al. Surgical tracheotomy in COVID-19 patients: an Italian single centre experience. Eur Arch Otorhinolaryngol. 2021. doi: 10.1007/s00405-021-06697-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Broderick D, Kyzas P, Baldwin AJ, et al. Surgical tracheostomies in COVID-19 patients: a multidisciplinary approach and lessons learned. Oral Oncol. 2020;106:104767. doi: 10.1016/j.oraloncology.2020.104767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cardasis JJ, Rasamny JK, Berzofsky CE, Bello JA, Multz AS. Outcomes after tracheostomy for patients with respiratory failure due to COVID-19. Ear Nose Throat J. 2021;145561321993567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Courtney A, Lignos L, Ward PA, Vizcaychipi MP. Surgical tracheostomy outcomes in COVID-19–positive patients. OTO Open. 2021;5(1):X20984998. doi: 10.1177/2473974X20984998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chao TN, Harbison SP, Braslow BM, et al. Outcomes after tracheostomy in COVID-19 patients. Ann Surg. 2020;272(3):e181-e186. doi: 10.1097/SLA.0000000000004166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cui C, Yao Q, Zhang D, et al. Approaching otolaryngology patients during the COVID-19 pandemic. Otolaryngol Head Neck Surg. 2020;163(1):121-131. doi: 10.1177/0194599820926144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ferri E, Boscolo Nata F, Pedruzzi B, et al. Indications and timing for tracheostomy in patients with SARS CoV2-related. Eur Arch Otorhinolaryngol. 2020;277(8):2403-2404. doi: 10.1007/s00405-020-06068-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Floyd E, Harris SS, Lim JW, Edelstein DR, Filangeri B, Bruni M. Early data from case series of tracheostomy in patients with SARS-CoV-2. Otolaryngol Head Neck Surg. 2020;163(6):1150-1152. doi: 10.1177/0194599820940655 [DOI] [PubMed] [Google Scholar]
- 33.Glibbery N, Karamali K, Walker C, Fitzgerald O’Connor I, Fish B, Irune E. Tracheostomy in the coronavirus disease 2019 patient: evaluating feasibility, challenges and early outcomes of the 14-day guidance. J Laryngol Otol. 2020;134(8):688-695. doi: 10.1017/S0022215120001759 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kim EJ, Yoo EH, Jung CY, Kim KC. Experience of percutaneous tracheostomy in critically ill COVID-19 patients. Acute Crit Care. 2020;35(4):263-270. doi: 10.4266/acc.2020.00444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Krishnamoorthy S, Polanco A, Coleman N, et al. The safety and efficacy of tracheostomy in patients diagnosed with COVID-19: an analysis of 143 patients at a Major NYC medical center. Ann Surg. 2020. doi: 10.1097/SLA.0000000000004612 [DOI] [PubMed] [Google Scholar]
- 36.Kumar Swain S, Ranjan Das S, Sahu A. Performing bedside surgical tracheostomy on COVID-19 patients at intensive care unit—our experiences at a tertiary care Indian teaching hospital. Eur J Mol Clin Med. 2020;7(11):1208-1217. https://ejmcm.com/article_5592.html [Google Scholar]
- 37.Kwak PE, Connors JR, Benedict PA, et al. Early outcomes from early tracheostomy for patients with COVID-19. JAMA Otolaryngol Head Neck Surg. 2021;147(3):239-244. doi: 10.1001/jamaoto.2020.4837 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Long SM, Chern A, Feit NZ, et al. Percutaneous and open tracheostomy in patients with COVID-19: comparison and outcomes of an institutional series in New York City. Ann Surg. 2021;273(3):403-409. doi: 10.1097/SLA.0000000000004428 [DOI] [PubMed] [Google Scholar]
- 39.Loube DI, Hassan KZ, Lee SH, Davidson BL. Bedside tracheostomy for a COVID-19 cohort. Respir Med Case Rep. 2021;32:101346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Martínez-Téllez E, Orús Dotú C, Trujillo-Reyes JC, et al. Traqueotomía en pacientes COVID-19: un procedimiento necesario de alto riesgo: experiencia de dos centros. Arch Bronconeumol. 2020;56(10):673-674. doi: 10.1016/j.arbres.2020.05.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Marchioni D, Bisi N, Molteni G, Rubini A. Covid-19 and ENT practice: our experience: ENT outpatient department, ward and operating room management during the SARS-CoV-2 pandemic. Am J Otolaryngol. 2020;41(6):102676. doi: 10.1016/j.amjoto.2020.102676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Martin-Villares C, Perez Molina-Ramirez C, Bartolome-Benito M, Bernal-Sprekelsen M; COVID ORL ESP Collaborative Group . Outcome of 1890 tracheostomies for critical COVID-19 patients: a national cohort study in Spain. Eur Arch Otorhinolaryngol. 2020;278:1605-1612. doi: 10.1007/s00405-020-06220-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Mattioli F, Fermi M, Ghirelli M, et al. Tracheostomy in the COVID-19 pandemic. Eur Arch Otorhinolaryngol. 2020;277(7):2133-2135. doi: 10.1007/s00405-020-05982-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mata-Castro N, Sanz-López L, Pinacho-Martínez P, Varillas-Delgado D, Miró-Murillo M, Martín-Delgado MC. Tracheostomy in patients with SARS-CoV-2 reduces time on mechanical ventilation but not intensive care unit stay. Am J Otolaryngol. 2021;42(2):102867. doi: 10.1016/j.amjoto.2020.102867 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Meyer CD, Capra GG, Strange RG, Weimerskirch BP, Santiago GF. Airway management of COVID-19 positive patients aboard USNS COMFORT mission to New York City. J Craniofac Surg. 2020;31(6):e660-e661. doi: 10.1097/SCS.0000000000006891 [DOI] [PubMed] [Google Scholar]
- 46.Mishra P, Jedge P, Kaushik M, Artham P, Kumari S. Our experience of tracheostomy in COVID-19 patients. Indian J Otolaryngol Head Neck Surg. 2020;1-4. doi: 10.1007/s12070-020-02036-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Murphy P, Holler E, Lindroth H, et al. Short-term outcomes for patients and providers after elective tracheostomy in COVID-19–positive patients. J Surg Res. 2021;260:38-45. doi: 10.1016/j.jss.2020.10.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Morvan JB, Rivière D, Danguy des Déserts M, Bonfort G, Mathais Q, Pasquier P. Percutaneous dilatational tracheostomy for saturating influx of COVID-19 patients: experience of military ENT physicians deployed in Mulhouse, France. Eur Ann Otorhinolaryngol Head Neck Dis. 2020;137(4):263-268. doi: 10.1016/j.anorl.2020.06.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Niroula A, Van Nostrand KM, Khullar OV, et al. Percutaneous tracheostomy with apnea during coronavirus disease 2019 era: a protocol and brief report of cases. Crit Care Explor. 2020;2(5):e0134. doi: 10.1097/CCE.0000000000000134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Nishio N, Hiramatsu M, Goto Y, et al. Surgical strategy and optimal timing of tracheostomy in patients with COVID-19: early experiences in Japan. Auris Nasus Larynx. 2020;S0385-8146(20)30306-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Obata K, Miyata R, Yamamoto K, et al. Tracheostomy in patients with COVID-19: a single-center experience. In Vivo. 2020;34(6):3747-3751. doi: 10.21873/invivo.12224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Okuyemi OT, Spinner A, Elkins T, Bigcas JL, Ng M, Wang RC. Safe and efficient performance of open tracheostomies in patients with COVID-19—the fenestrated technique. JAMA Otolaryngol Head Neck Surg. 2021;147(3):301-302. doi: 10.1001/jamaoto.2020.4432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Picetti E, Fornaciari A, Taccone FS, et al. Safety of bedside surgical tracheostomy during COVID-19 pandemic: a retrospective observational study. PLoS One. 2020;15(9):e0240014. doi: 10.1371/journal.pone.0240014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Piccin O, Albertini R, Caliceti U, et al. Early experience in tracheostomy and tracheostomy tube management in Covid-19 patients. Am J Otolaryngol. 2020;41(4):102535. doi: 10.1016/j.amjoto.2020.102535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Prabhakaran K, Malcom R, Choi J, et al. Open tracheostomy for COVID-19-positive patients: a method to minimize aerosolization and reduce risk of exposure. J Trauma Acute Care Surg. 2020;89(2):265-271. doi: 10.1097/TA.0000000000002780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Pradhan P, Mishra AK, Mittal Y, et al. Tracheostomy in the COVID19 patients: our experience in 12 cases. Indian J Otolaryngol Head Neck Surg. 2021;1-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Riestra-Ayora J, Yanes-Diaz J, Penuelas O, Molina-Quiros C, Sanz-Fernández R, Martin-Sanz E. Safety and prognosis in percutaneous vs surgical tracheostomy in 27 patients with COVID-19. Otolaryngol Head Neck Surg. 2020;163(3):462-464. doi: 10.1177/0194599820931801 [DOI] [PubMed] [Google Scholar]
- 58.Rosano A, Martinelli E, Fusina F, et al. Early percutaneous tracheostomy in coronavirus disease 2019: association with hospital mortality and factors associated with removal of tracheostomy tube at ICU discharge: a cohort study on 121 patients. Crit Care Med. 2021;49(2):261-270. doi: 10.1097/CCM.0000000000004752 [DOI] [PubMed] [Google Scholar]
- 59.Rovira A, Tricklebank S, Surda P, et al. Open versus percutaneous tracheostomy in COVID-19: a multicentre comparison and recommendation for future resource utilisation. Eur Arch Otorhinolaryngol. 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Sancho J, Ferrer S, Lahosa C, et al. Tracheostomy in patients with COVID-19: predictors and clinical features. Eur Arch Otorhinolaryngol. 2021. doi: 10.1007/s00405-020-06555-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Sood RN, Dudiki N, Alape D, Maxfiel MW. Healthcare personnel safety during percutaneous tracheostomy in patients with COVID-19: proof-of-concept study. J Intensive Care Med. 2020;885066620980384. [DOI] [PubMed] [Google Scholar]
- 62.Singh S, Hind M, Jordan S, et al. Weaning by surgical tracheostomy and portable ventilators released ICU ventilators during coronavirus disease 2019 surge in London. Crit Care Explor. 2020;2(8):e0193. doi: 10.1097/CCE.0000000000000193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Stubington TJ, Mallick AS, Garas G, Stubington E, Reddy C, Mansuri MS. Tracheotomy in COVID-19 patients: optimizing patient selection and identifying prognostic indicators. Head Neck. 2020;42(7):1386-1391. doi: 10.1002/hed.26280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Sun B, Wolff C, Bechtold H, et al. Modified percutaneous tracheostomy in patients with COVID-19. Trauma Surg Acute Care Open. 2020;5(1):e000625. doi: 10.1136/tsaco-2020-000625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Taboada M, Vazquez S, Regueira J, et al. Safe percutaneous dilational tracheostomy in 5 patients with ARDS by Covid-19. J Clin Anesth. 2020;67:109977. doi: 10.1016/j.jclinane.2020.109977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Takhar A, Surda P, Ahmad I, et al. Timing of tracheostomy for prolonged respiratory wean in critically ill coronavirus disease 2019 patients: a machine learning approach. Crit Care Explor. 2020;2(11):e0279. doi: 10.1097/CCE.0000000000000279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Takhar A, Tornari C, Amin N, et al. Safety and outcomes of percutaneous tracheostomy in coronavirus disease 2019 pneumonitis patients requiring prolonged mechanical ventilation. J Laryngol Otol. 2020;1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Tang Y, Wu Y, Zhu F, et al. Tracheostomy in 80 COVID-19 patients: a multicenter, retrospective, observational study. Front Med (Lausanne). 2020;7:615845. doi: 10.3389/fmed.2020.615845 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Thal AG, Schiff BA, Ahmed Y, et al. Tracheotomy in a high-volume center during the COVID-19 pandemic: evaluating the surgeon’s risk. Otolaryngol Head Neck Surg. 2021;164(3):522-527. doi: 10.1177/0194599820955174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Tornari C, Surda P, Takhar A, et al. Tracheostomy, ventilatory wean, and decannulation in COVID-19 patients. Eur Arch Otorhinolaryngol. 2021;278(5):1595-1604. doi: 10.1007/s00405-020-06187-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Turri-Zanoni M, Battaglia P, Czaczkes C, Pelosi P, Castelnuovo P, Cabrini L. Elective tracheostomy during mechanical ventilation in patients affected by COVID-19: preliminary case series from Lombardy, Italy. Otolaryngol Head Neck Surg. 2020;163(1):135-137. doi: 10.1177/0194599820928963 [DOI] [PubMed] [Google Scholar]
- 72.Volo T, Stritoni P, Battel I, et al. Elective tracheostomy during COVID-19 outbreak: to whom, when, how? Early experience from Venice, Italy. Eur Arch Otorhinolaryngol. 2021;278(3):781-789. doi: 10.1007/s00405-020-06190-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Yeung E, Hopkins P, Auzinger G, Fan K. Challenges of tracheostomy in COVID-19 patients in a tertiary centre in inner city London. Int J Oral Maxillofac Surg. 2020;49(11):1385-1391. doi: 10.1016/j.ijom.2020.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Zhang X, Huang Q, Niu X, et al. Safe and effective management of tracheostomy in COVID-19 patients. Head Neck. 2020;42(7):1374-1381. doi: 10.1002/hed.26261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Weiss KD, Coppolino A, 3rd, Wiener DC, et al. Controlled Apneic Tracheostomy in Patients with COVID-19. JTCVS Tech, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Williamson A, Roberts MT, Phillips J, Saha R. Early percutaneous tracheostomy for patients with COVID-19. Anaesthesia. 2021;76(1):138-139. doi: 10.1111/anae.15197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Yokokawa T, Ariizumi Y, Hiramatsu M, et al. Management of tracheostomy in COVID-19 patients: The Japanese experience. Auris Nasus Larynx. 2021;48(3):525-529. doi: 10.1016/j.anl.2021.01.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Zuazua-Gonzalez A, Collazo-Lorduy T, Coello-Casariego G, et al. Surgical tracheostomies in COVID-19 patients: indications, technique, and results in a second-level Spanish hospital. OTO Open. 2020;4(3):X20957636. doi: 10.1177/2473974X20957636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Takhar A, Tornari C, Amin N, et al. Percutaneous tracheostomy in COVID-19 pneumonitis patients requiring prolonged mechanical ventilation: initial experience in 51 patients and preliminary outcomes. Int J Oral Maxillofac Surg. Published online April 27, 2020. doi: 10.22541/au.158801954.4753876232912655 [DOI] [Google Scholar]
- 80.Siempos II, Ntaidou TK, Filippidis FT, Choi AMK. Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(2):150-158. doi: 10.1016/S2213-2600(15)00007-7 [DOI] [PubMed] [Google Scholar]
- 81.Young D, Harrison DA, Cuthbertson BH, Rowan K; TracMan Collaborators . Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA. 2013;309(20):2121-2129. doi: 10.1001/jama.2013.5154 [DOI] [PubMed] [Google Scholar]
- 82.Cinotti R, Voicu S, Jaber S, et al. ; FROG-ICU investigators . Tracheostomy and long-term mortality in ICU patients undergoing prolonged mechanical ventilation. PLoS One. 2019;14(10):e0220399. doi: 10.1371/journal.pone.0220399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Adly A, Youssef TA, El-Begermy MM, Younis HM. Timing of tracheostomy in patients with prolonged endotracheal intubation: a systematic review. Eur Arch Otorhinolaryngol. 2018;275(3):679-690. doi: 10.1007/s00405-017-4838-7 [DOI] [PubMed] [Google Scholar]
- 84.Herritt B, Chaudhuri D, Thavorn K, Kubelik D, Kyeremanteng K. Early vs. late tracheostomy in intensive care settings: impact on ICU and hospital costs. J Crit Care. 2018;44:285-288. doi: 10.1016/j.jcrc.2017.11.037 [DOI] [PubMed] [Google Scholar]
- 85.Hosokawa K, Nishimura M, Egi M, Vincent JL. Timing of tracheotomy in ICU patients: a systematic review of randomized controlled trials. Crit Care. 2015;19:424. doi: 10.1186/s13054-015-1138-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.McGrath BA, Brenner MJ, Warrillow SJ, et al. Tracheostomy in the COVID-19 era: global and multidisciplinary guidance. Lancet Respir Med. 2020;8(7):717-725. doi: 10.1016/S2213-2600(20)30230-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Johnson-Obaseki S, Veljkovic A, Javidnia H. Complication rates of open surgical versus percutaneous tracheostomy in critically ill patients. Laryngoscope. 2016;126(11):2459-2467. doi: 10.1002/lary.26019 [DOI] [PubMed] [Google Scholar]
- 88.Klotz R, Probst P, Deininger M, et al. Percutaneous versus surgical strategy for tracheostomy: a systematic review and meta-analysis of perioperative and postoperative complications. Langenbecks Arch Surg. 2018;403(2):137-149. [DOI] [PubMed] [Google Scholar]
- 89.Wahla AS, Mallat J, Zoumot Z, et al. Complications of surgical and percutaneous tracheostomies, and factors leading to decannulation success in a unique Middle Eastern population. PLoS One. 2020;15(7):e0236093. doi: 10.1371/journal.pone.0236093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Straetmans J, Schlöndorff G, Herzhoff G, Windfuhr JP, Kremer B. Complications of midline-open tracheotomy in adults. Laryngoscope. 2010;120(1):84-92. doi: 10.1002/lary.20703 [DOI] [PubMed] [Google Scholar]
- 91.El Solh AA, Jaafar W. A comparative study of the complications of surgical tracheostomy in morbidly obese critically ill patients. Crit Care. 2007;11(1):R3. doi: 10.1186/cc5147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Popkin BM, Du S, Green WD, et al. Individuals with obesity and COVID-19: a global perspective on the epidemiology and biological relationships. Obes Rev. 2020;21(11):e13128. doi: 10.1111/obr.13128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Cipriano A, Mao ML, Hon HH, et al. An overview of complications associated with open and percutaneous tracheostomy procedures. Int J Crit Illn Inj Sci. 2015;5(3):179-188. doi: 10.4103/2229-5151.164994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Godoy LC, Goligher EC, Lawler PR, Slutsky AS, Zarychanski R. Anticipating and managing coagulopathy and thrombotic manifestations of severe COVID-19. CMAJ. 2020;192(40):E1156-E1161. doi: 10.1503/cmaj.201240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Buitrago-Garcia D, Egli-Gany D, Counotte MJ, et al. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis. PLoS Med. 2020;17(9):e1003346. doi: 10.1371/journal.pmed.1003346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Xu K, Zhang XH, Long XB, Lu X, Liu Z. An environmental study of tracheostomy on eight COVID-19 patients. J Otolaryngol Head Neck Surg. 2021;50(1):3. doi: 10.1186/s40463-021-00494-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Sowerby LJ, Stephenson K, Dickie A, et al. International registry of otolaryngologist-head and neck surgeons with COVID-19. Int Forum Allergy Rhinol. 2020;10(11):1201-1208. doi: 10.1002/alr.22677 [DOI] [PubMed] [Google Scholar]
- 98.George MM, McIntyre CJ, Zhou J, et al. Viral infectivity in patients undergoing tracheotomy with COVID-19: a preliminary study. Otolaryngol Head Neck Surg. 2021;1945998211004255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. doi: 10.1371/journal.pone.0035797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Howard BE. High-risk aerosol-generating procedures in COVID-19: respiratory protective equipment considerations. Otolaryngol Head Neck Surg. 2020;163(1):98-103. doi: 10.1177/0194599820927335 [DOI] [PubMed] [Google Scholar]
- 101.Licina A, Silvers A, Stuart RL. Use of powered air-purifying respirator (PAPR) by healthcare workers for preventing highly infectious viral diseases-a systematic review of evidence. Syst Rev. 2020;9(1):173. doi: 10.1186/s13643-020-01431-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Bischoff WE, Turner J, Russell G, Blevins M, Missaiel E, Stehle J. How well do N95 respirators protect healthcare providers against aerosolized influenza virus? Infect Control Hosp Epidemiol. 2018;1-3. [DOI] [PubMed] [Google Scholar]
- 103.Robertson-More C, Wu T. A knowledge gap unmasked: viral transmission in surgical smoke: a systematic review. Surg Endosc. 2021. doi: 10.1007/s00464-020-08261-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.van Kampen JJA, van de Vijver DAMC, Fraaij PLA, et al. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nat Commun. 2021;12(1):267. doi: 10.1038/s41467-020-20568-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.US Centers for Disease Control and Prevention . Interim guidance on duration of isolation and precautions for adults with COVID-19. Accessed March 29, 2021. https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html
- 106.Metelli S, Chaimani A. Challenges in meta-analyses with observational studies. Evid Based Ment Health. 2020;23(2):83-87. doi: 10.1136/ebmental-2019-300129 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix A. Ovid search strategy
eTable. Summary of all included studies (N = 69).