

Abstract
Background
Tooth wear can have a multifactorial aetiology which requires thorough patient assessment and aesthetic management.
Purpose
This case report discusses the management of a young, Egyptian swimmer complaining of tooth sensitivity associated with erosive tooth wear. Anterior teeth were restored using the injection molding technique, also known as the injectable composite resin technique, to overcome the patient’s complaint and enhance the aesthetics of compromised anterior teeth.
Patients and Methods
Thorough patient assessment was followed by impression taking, a diagnostic wax-up and intraoral mock-up fabrication for aesthetic, functional and biological verification. Upon the patient’s agreement on the proposed treatment, an injection molding technique was carried out.
Conclusion
The tooth loss pattern associated with erosive tooth wear in competitive swimmers showed a very characteristic presentation. Detailed patient history is imperative for successful assessment of the risk factors contributing to the condition and treatment planning in such cases. The use of injection molding technique for restoration of anterior teeth is a simple, straightforward and aesthetically pleasing alternative for patients with erosive tooth wear requiring direct composite veneers.
Keywords: composite, erosion, abrasion, erosive tooth wear, case report, aesthetic, competitive swimmer
Introduction
Tooth wear is the cumulative surface loss of mineralized tooth substance due to physical or chemo-physical processes that do not involve caries, trauma or resorption.1 It is a common dental problem with a reported 30% prevalence in Arab countries, including Egypt.2 Competitive swimmers are prone to suffer from tooth erosion due to chemically induced loss of mineralized tooth substance caused by exposure to acids not derived from oral bacteria.1 Dental erosion presented in competitive swimmers has been attributed to extrinsic exposure to heavily chlorinated swimming pool water with lowered pH values as a result of insufficient monitoring or inadequate buffering of the pool water.3,4 Swimmers demonstrating dental erosive lesions typically have loss of hard tooth tissue on the labial surfaces on maxillary incisors due to their regular contact with pool water and diminished protective action from saliva.5 The aetiology of tooth wear can be multifactorial and presented in a variety of clinical appearances. Occasionally, one causative factor may be dominant, but often the clinical appearance is the result of collective damage over a period of time.6 Teeth subjected to erosive insults can be more vulnerable for physical tooth structure loss by foreign objects, for instance, a toothbrush or tooth paste. Several authors recognized a relationship between toothbrush stiffness, toothpaste abrasiveness and hard tooth structure abrasion.7–11 The combined effect of erosive acids and mechanical insults, triggering progressive enamel substance loss, has been known as erosive tooth wear.12 This case report discusses a case of a young, Egyptian, competitive swimmer, complaining from sensitivity to cold and hot related to his anterior teeth. The patient also had an aesthetic concern which he needed resolved before an important event. The patient presented in this case report was diagnosed with erosive tooth wear.
Patient and Methods
Case Presentation
This case report has been described according to the 2013 CARE checklist for case report writing and publishing guidelines.13
Patient Information
A 28-year-old male patient came to the conservative dentistry department outpatient clinic, Cairo University, complaining from hypersensitivity to hot and cold stimuli and an aesthetically unsatisfactory smile.
Thorough patient history was taken and revealed that the patient is a national competitive swimmer living in Cairo, Egypt. He has been swimming for 20 years and goes for four to five swimming sessions per week. The patient has been to the dentist twice throughout his life for a dental hygiene visit, followed by a chemical bleaching session, which was done almost 5 years ago and he had no sensitivity complaint after those visits. The patient maintains his oral hygiene through brushing once to twice daily using a hard toothbrush along with a whitening tooth paste, which he has been using for a couple of years, and in his own words, he “scrubs the teeth vigorously” in a vertical direction.
Clinical Findings
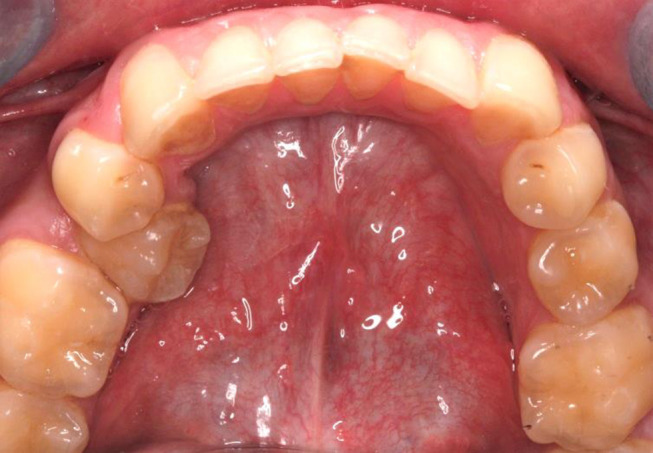
Clinical examination showed tooth wear related to the maxillary and mandibular anterior teeth, more distinctively affecting both upper central incisors and maxillary left lateral incisor. Those teeth presented loss of anatomy affecting their smooth surfaces and were shiny in appearance with the dentine color more evident. The pattern of tooth wear seemed similar to preparations for aesthetic veneers. Moreover, a moderate sized fracture associated with the upper right central incisor was seen, which the patient does not recall how it happened, but it caused the sensitivity complaint to cold and hot stimuli due to frank dentine exposure. The patient has no carious lesions anteriorly or posteriorly. Significant malalignment was observed in the mandibular arch. Plaque deposits and marginal gingivitis were also apparent on periodontal examination (Figures 1–3).
Figure 1.

Frontal view of anterior teeth.
Figure 2.

Occlusal view of the maxillary arch.
Figure 3.
Occlusal view of the mandibular arch.
Diagnosis and Assessment
Caries risk assessment was done as part of the diagnostic visit using the Cariogram®, which placed the patient in a low risk category with an 82% chance to avoid new cavities. The patient’s diet was investigated as part of the caries risk assessment process. The patient stated that he follows a diet of high protein and low carbohydrate content with incorporation of various vegetables in most of his main meals. He does not consume energy or carbonated drinks, but might have some coffee during the day. Salivary pH was measured using a pH indicator strip (MQuant® pH-indicator strip, Merck KGaA, Darmstadt, Germany), showing a pH level of 7, indicating neutrality.
It was extrapolated from the patient’s history that the current lesions are due erosive tooth wear as a result of a combined effect of tooth erosion and toothbrush abrasion. A similar pattern of tooth surface loss in swimmers was reported in other clinical reports.14–16 Although the relationship between handedness and the side on which non-carious cervical lesions may develop is still controversial, yet it is worth mentioning that the patient is right-handed which could explain the incidence of the erosive tooth wear lesions more drastically on the left incisors, in relation to the right.17,18 The maxillary right central incisor seems to have a labio-version position with slight rotation, making it more prone to contact the stiff toothbrush filaments, as the patient brushes his teeth regularly, in relation to anterior teeth in the same quadrant. The marginal gingivitis also confirms the traumatic effect of improper tooth brushing technique.19 The visual analogue scale (VAS) was presented to the patient to score sensitivity and aesthetic concerns. The patient scored 7 for his sensitivity complaint and 6 for aesthetic satisfaction.
Therapeutic Intervention
Patient education covering proper oral hygiene measures was done. The patient was instructed to discard the hard toothbrush and whitening toothpaste and replace them with a soft toothbrush that should be used three times per day with a fluoridated toothpaste. Primary impressions were taken using heavy and light condensation silicone impression material (Silaxil, LASCOD, Florence, Italy) and temporization was done to the fractured maxillary central incisor using a light cured resinous temporary material to overcome the patient’s sensitivity. The restorative treatment plan was discussed with the patient and it was decided to restore only the teeth that are mostly affected by tooth surface loss using direct resin composite restorations. The remaining teeth suffering from some degree of erosive tooth wear, for example incisal thirds of mandibular anterior teeth, presented no complaints whether aesthetically or sensitivity, thus monitoring of those lesions was favored. A diagnostic wax-up was made by the laboratory technician (Figure 4) and a silicone index was used for fabrication of a mock-up (Figure 5).
Figure 4.

Diagnostic wax-up.
Figure 5.

Intraoral mock-up.
The mock-up was left for a week for biological and functional assessment before receiving the permanent restorations. The injection molding technique, also known as the injectable composite resin technique, using highly filled injectable resin composite was chosen for aesthetic restoration of this case. The same wax-up was used for fabrication of a vacuum pressed vinyl sheet splint, which was injected with a clear polyvinyl siloxane material (DENU Trans Sil, HDI Inc., Seoul, Republic of Korea) to record finer details of the wax-up and provide better adaptation and stabilization of the splint (Figure 6). Holes were drilled through the materials to provide a pathway through which the tip of the injectable composite syringe can be inserted.
Figure 6.

Splint injected with clear PVS and seated on the cast.
On the recall visit, shade selection was done and the mock-up was removed, teeth were prepared using abrasive discs (Polishing Discs № 1.071, TOR VM, Moscow, Russia) to remove any debris from the mock-up and provide a better surface for bonding procedures. For isolation, a soft, flexible cheek and lip retractor was used (OptraGate, Ivoclar Vivadent, Schaan, Liechtenstein), this was followed by placement of retraction cords into the gingival sulci and a Teflon napkin gingivally and on every other tooth for maximal isolation (Figures 7 and 8). Teflon tape must cover the teeth adjacent to the one to be restored. Selective enamel etching was done for 15 seconds and the area where dentine was exposed in the maxillary right central was avoided during the etching procedure. A one component light-cured universal adhesive (G-Premio Bond, GC Corp, Tokyo, Japan) was applied on the tooth structure and cured for 10 seconds, according to manufacturer instructions. Afterwards, the splint was placed intraorally and stabilized in place. The injectable resin composite (G-ænial Universal Flo, GC Corp, Tokyo, Japan) was injected through the drilled holes and cured for 20 seconds, according to manufacturer instructions (Figure 9). After the three teeth were restored consecutively, Teflon was removed and finally finishing and polishing procedures were done using abrasive discs and a polishing kit (DIACOMP® PLUS RA, EVE Ernst Vetter GmbH, Germany) (Figures 10–12).
Figure 7.

Isolation of adjacent teeth using Teflon tape during restoration of maxillary right central incisor and left lateral incisor.
Figure 8.

Isolation of adjacent teeth using Teflon tape during restoration of maxillary left central incisor.
Figure 9.

Tip of the injectable composite resin syringe inserted into the space created by the wax-up.
Figure 10.

Final restorations.
Figure 11.

Preoperative smile.
Figure 12.

Postoperative smile.
Postoperatively, the patient was advised to rinse his mouth with freshwater immediately when he comes out of the pool, always use fluoridated toothpaste and follow-up with a dentist every 3 months to monitor the restoration- and any lesion progression.
Patient Perceptive
Directly postoperatively, the patient was presented with a visual analogue scale (VAS) card designed for patient satisfaction with aesthetic treatment and he reported the highest level of satisfaction with the provided treatment.
Follow-Up and Outcomes
After 8 weeks, the patient was asked to come in for a follow-up. He had no complaints and was pleased with the treatment provided. Gingival health was satisfactory with some residual marginal inflammation (Figures 13 and 14). The patient still used the vertical “scrubbing” technique for tooth brushing which could explain the residual gingivitis,; thus, proper oral hygiene measures were, once again, explained to the patient and the correct tooth brushing method was demonstrated in front of the patient.
Figure 13.

Follow-up photograph after 8 weeks.
Figure 14.

Artistic picture showing the patient’s smile.
The VAS for pain and satisfaction with treatment was presented to the patient for the second time to follow-up with his perceptive of treatment. He gave a score of 0 for both treatment satisfaction and pain. He reported complete absence of dentine hypersensitivity.
Discussion
This case report describes a young Egyptian competitive swimmer suffering from tooth surface loss and dentine hypersensitivity as a result of frank dentine exposure. Dentine hypersensitivity is defined as “short, sharp pain that arises from exposed dentin in response to non-noxious stimuli, typically thermal, evaporative, tactile, osmotic or chemical”.20 His complaints were attributed to erosive tooth wear. The frequent exposure of the patient’s dentition to an erosive medium (swimming pool water) has been superimposed with a mechanical insult to the tooth enamel by improper oral hygiene practice. Severe presentations of erosive tooth wear can be puzzling to diagnose. At first sight, the patient was thought to have had preparations done to receive anterior aesthetic veneers, but meticulous patient history played the pivotal role to reach the definitive diagnosis in this case which dictated the most suitable management approach. Although similar erosive lesions’ characteristics were reported in swimmers,14–16 but to our knowledge, none have been managed through the injection molding technique.
Professional swimmers, like the case presented, are prone to erosive tooth wear due to the environmental factors which they face on regular basis. It has been reported by Ashley et al21 that the prevalence of tooth tissue loss due to erosive challenges in athletes, range from 36% to 85%. Swimmers are regularly exposed to chlorinated water.22 Chlorine compounds are added to swimming pool water as a means of disinfection, resulting in drastic changes in pH values that can drop up to a pH level of 4 in a short period of time.23 The WHO sets the standard of pH for swimming pool water to be maintained between 7.2 and 7.8 for chlorine disinfectants,24 which is the most commonly used method for disinfection in Egypt. Similarly, the Egyptian Ministry of Health Decree no. 418 for the year 1995 states the same range as the WHO. However, some violations concerning swimming pool water pH have been reported in Egypt.25 It has been stated in the literature over the years, that the critical pH for enamel dissolution ranges from 5.5 to 5.7.23,26 However, Lussi and Carvalho27 debated that this range is only specific to the carious process and there is no clear-cut critical pH for enamel dissolution during other erosive challenges, since it depends not only on the pH of the solution but also on the concentration of the relevant mineral constituents (calcium, phosphate and fluoride) in each erosive solution. They finally concluded that the critical pH for enamel dissolution can have a wider range starting at 6.5 up to 3.9. Unfortunately, pH levels of some of the reported swimming pool water samples reported in Egypt fell below this critical pH.25 Upon exposure of enamel and dentine to an acidic insult, demineralization occurs in a centripetal process starting with partial loss of surface minerals simultaneously with softening at the surface layer, which progresses with a continuous acidic attack and makes eroded enamel surfaces vulnerable to physical impacts.28 The continuous exposure of the patient presented in this report to low pH levels for long durations, was probably the primary causative factor for initiation of erosive tooth wear.
Individual tooth wear mechanisms rarely act alone but interact with each other. The most important interaction is the potentiation of erosive damage by abrasion to the dental hard tissues.29 In the case currently discussed, the patient has been practicing improper oral hygiene measures for at least 2 years where he used a combination of whitening toothpaste along with a hard bristle toothbrush. In vitro studies observed that softened dental tissues are more susceptible to abrasion by the toothbrush and paste.8–10 This could explain the pattern of tooth surface loss presented in this case, where enamel was softened by the acidic insult from the swimming pool water followed by vigorous brushing of the tooth surface resulting in wearing off, of enamel layers.
The choice of toothbrush filament stiffness and toothpaste type for proper oral hygiene maintenance are key players for maintaining healthy soft and hard dental tissues. The selection of toothpaste is primarily more significant than the toothbrush filament stiffness. Abrasive wear of eroded dental hard tissues increases with increasing abrasivity of the toothpaste.10 Abrasives have been added to toothpastes by manufacturers for two reasons; 1') to contribute to the toothpaste rheology and 2) for aesthetic purposes.30 Those abrasives act by removing plaque and stains from the surfaces of teeth.31 This is because, abrasives are physically harder than stains; thus, when they get trapped between the toothbrush bristles and the tooth surface, they remove those stains and clean the surface.32 The case described in this article reported the use of whitening toothpaste for some time. Whitening toothpastes include different active ingredients in their composition, such as chemical and optical agents, and normally contain higher amounts of abrasives and detergents than their conventional counterparts.33,34 After viewing the components of the used toothpastes by the above mentioned patient, all of them contained one or more of the following: silica, sodium bicarbonate, phosphate compounds or charcoal powder. Those components are capable of soft and hard tissue damage, especially in cases where acid erosion is also present. Therefore, such toothpastes should be avoided in cases suffering from erosive tooth wear.31,35–37
Toothbrush filament stiffness has shown little effect on enamel and dentine surfaces, when analyzed without toothpastes. In other words, it plays a secondary role in tooth structure abrasion.7,8,38,39 It has been debatable whether soft or hard toothbrushes cause more hard dental tissue loss.8,9,38 However, when an erosive challenge weighs in, its’ not just the bristle stiffness that plays a role, but also the applied load.12 The patient discussed in this report mentioned vigorous scrubbing of the tooth structure using a hard bristle tooth brush. According to an in vitro study by Souza et al, in 2021,12 the authors recommended that patients with erosive tooth wear, exerting loads normally applied by healthy individuals should avoid hard bristle dental brushes to avoid further tooth loss. This could explain the exaggerated pattern of erosive tooth wear presented in this case, considering that the present case might even be applying higher than the usual load during tooth brushing procedures according to his description of his tooth brushing regimen. Moreover, hard toothbrushes have shown to cause soft tissue trauma,19,40 which could explain the marginal gingivitis seen in this case.
The European consensus statement on management guidelines for severe tooth wear published in 2017,41 states that a restorative intervention is only necessary if the patient has one or more of the following complaints: 1) sensitivity or pain, 2) impairment of function, 3) impairment of aesthetics due to loss of hard dental tissues and 4) “crumbling” of dental hard tissues and/or restorations which threatens the integrity of the remaining tooth structure. The patient described in this case report complained from sensitivity and aesthetic concerns, which indicated that a restorative intervention must take place. In regards to the restorative materials indicated for such cases, a systematic review by Mesko et al42 concluded that there is no specific material that is favored over the other. Direct and indirect materials are both viable option for treatment of worn dentition. However, the European Federation of Conservative Dentistry reported in their consensus report covering erosive tooth wear in 2015 that direct restorative approaches are less invasive than indirect ones, and composites have been recommended for treatment of such lesions.43
The injection molding technique was the restorative approach chosen for this case. This technique can be utilized for fabrication of temporary or permanent restorations applied in several clinical scenarios including 1) changes in occlusal relations, 2) establishment of a new vertical dimension and 3) restoration of fractured or worn dentition. Restorative dentistry nowadays is focused on minimum intervention protocols that employ additive restorative approaches. This technique involves an indirect/direct method using a transparent silicone index for transformation of a diagnostic wax-up into composite restorations with maximum tooth structure conservation.44 The technique utilizes the use of a highly filled injectable composite as a restorative material and a clear polyvinyl siloxane material for index construction. Although this technique demands a laboratory step for diagnostic wax-up fabrication and two dental visits: one for assessment, patient education and impression taking and the second for the actual restorative treatment. Yet, it ensures conservation of valuable dental tissues, decreased chair side time (in relation to a free hand technique) and the production of predictable restorations that are highly aesthetic. Moreover, this restorative approach is more economically accepted by patients in comparison to indirect ceramic veneers and most importantly in case of wear or fracture of such restorations, it can be easily and conservatively repaired unlike ceramic materials.45 Highly filled restorative injectable composites have gained popularity due to their ease of manipulation and have proven clinical success up to 24–36 months in clinical trials.46,47
Conclusion
The tooth loss pattern associated with erosive tooth wear in competitive swimmers showed a very characteristic presentation.
Detailed patient history is imperative for successful assessment of the risk factors contributing to the condition and treatment planning in such cases.
The use of injection molding technique for restoration of anterior teeth is a simple, straightforward and aesthetically pleasing alternative for patients with erosive tooth wear requiring direct composite veneers.
Recommendations
Professional swimmers must be kept on close follow-up periods and dental check-ups to assess and manage early signs of erosive tooth wear.
Swimming pool water should be closely supervised for its pH and kept close to the national and international standards for the safety of athletes.
Clinical trials involving professional swimmers are required to evaluate the durability of the proposed restorative approach “injection molding technique” as a line of treatment in comparison to the conventional restorative methods using ceramic materials or conventional composite layering.
Abbreviation
VAS, visual analogue scale.
Informed Consent
The institution’s research ethics committee requires a written informed consent to allow this case report to be published. However, in the case of clinical trials, a research ethics committee approval is mandatory. The authors acknowledge the patient who provided written informed consent to allow this case report to be published along with the accompanying images.
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Schlueter N, Amaechi BT, Bartlett D, et al. Terminology of erosive tooth wear: consensus report of a workshop organized by the ORCA and the Cariology Research Group of the IADR. Caries Res. 2020;54(1):2–6. doi: 10.1159/000503308 [DOI] [PubMed] [Google Scholar]
- 2.Awad MA, El Kassas D, Al Harthi L, et al. Prevalence, severity and explanatory factors of tooth wear in Arab populations. J Dent. 2019;80:69–74. doi: 10.1016/j.jdent.2018.09.011 [DOI] [PubMed] [Google Scholar]
- 3.Wiegand A, Attin T. Occupational dental erosion from exposure to acids - a review. Occup Med. 2007;57(3):169–176. doi: 10.1093/occmed/kql163 [DOI] [PubMed] [Google Scholar]
- 4.Schlueter N, Tveit AB. Prevalence of erosive tooth wear in risk groups. Monogr Oral Sci Basel. 2014;25:74–98. doi: 10.1159/000359938 [DOI] [PubMed] [Google Scholar]
- 5.Buczkowska-Radlińska J, Łagocka R, Kaczmarek W, Górski M, Nowicka A. Prevalence of dental erosion in adolescent competitive swimmers exposed to gas-chlorinated swimming pool water. Clin Oral Invest. 2013;17:579–583. doi: 10.1007/s00784-012-0720-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hemmings K, Truman A, Shah S, Chauhan R. Tooth wear guidelines for the BSRD part 3: removable management of tooth wear. Dent Update. 2018;45(8):687–696. doi: 10.12968/denu.2018.45.8.687 [DOI] [Google Scholar]
- 7.Lippert F, Arrageg MA, Eckert GJ, Hara AT. Interaction between toothpaste abrasivity and toothbrush fi lament stiffness on the development of erosive/abrasive lesions in vitro. Int Dent J. 2017;67(6):344–350. doi: 10.1111/idj.12305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wiegand A, Schwerzmann M, Sener B, et al. Impact of toothpaste slurry abrasivity and toothbrush filament stiffness on abrasion of eroded enamel - an in vitro study. Acta Odontol Scand. 2008;66(4):231–235. doi: 10.1080/00016350802195041 [DOI] [PubMed] [Google Scholar]
- 9.Bizhang M, Riemer K, Arnold WH, Domin J. Influence of bristle stiffness of manual toothbrushes on eroded and sound human dentin – an in vitro study. PLoS One. 2016;11(4):1–13. doi: 10.1371/journal.pone.0153250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nakamura M, Kitasako Y, Nakashima S, Sadr A, Tagami J. Impact of toothpaste on abrasion of sound and eroded enamel: an in vitro white light interferometer study. Am J Dent. 2015;28(5):268–272. [PubMed] [Google Scholar]
- 11.Brandini DA, De Sousa ALB, Trevisan CL, et al. Noncarious cervical lesions and their association with toothbrushing practices: in vivo evaluation. Oper Dent. 2011;36(6):581–589. doi: 10.2341/10-152-S [DOI] [PubMed] [Google Scholar]
- 12.Souza CD, Sakae L, Carneiro P, Esteves R, Scaramucci T. Interplay between different manual toothbrushes and brushing loads on erosive tooth wear. J Dent. 2021;105(August2020):103577. doi: 10.1016/j.jdent.2020.103577 [DOI] [PubMed] [Google Scholar]
- 13.Riley DS, Barber MS, Kienle GS, et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017;89:218–235. doi: 10.1016/j.jclinepi.2017.04.026 [DOI] [PubMed] [Google Scholar]
- 14.Jahangiri L, Pigliacelli S, Kerr AR. Severe and rapid erosion of dental enamel from swimming: a clinical report. J Prosthet Dent. 2011;106(4):219–223. doi: 10.1016/S0022-3913(11)60126-1 [DOI] [PubMed] [Google Scholar]
- 15.Peampring C. Restorative management using hybrid ceramic of a patient with severe tooth erosion from swimming: a clinical report. J Adv Prosthodont. 2014;6(5):423–426. doi: 10.4047/jap.2014.6.5.423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baghele ON, Majumdar IA, Thorat MS, Nawar R, Baghele MO, Makkad S. Prevalence of dental erosion among young competitive swimmers: a pilot study. Compend Contin Educ Dent. 2013;34(2):20–24. [PubMed] [Google Scholar]
- 17.Özgöz M, Arabaci T, Sümbüllü MA, Demir T. Relationship between handedness and toothbrush-related cervical dental abrasion in left- and right-handed individuals. J Dent Sci. 2010;5(4):177–182. doi: 10.1016/j.jds.2010.11.001 [DOI] [Google Scholar]
- 18.Heasman PA, Holliday R, Bryant A, Preshaw PM. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. J Clin Periodontol. 2015;42(S16):S237–S255. doi: 10.1111/jcpe.12330 [DOI] [PubMed] [Google Scholar]
- 19.Zimmer S, Metin Ö, Barthel CR, Bizhang M, Ra J. Cleaning efficacy and soft tissue trauma after use of manual toothbrushes with different bristle stiffness. J Periodontol. 2011;82(2):267–271. doi: 10.1902/jop.2010.100328 [DOI] [PubMed] [Google Scholar]
- 20.Liu XX, Tenenbaum HC, Wilder RS, Quock R, Hewlett ER, Ren YF. Pathogenesis, diagnosis and management of dentin hypersensitivity: an evidence-based overview for dental practitioners. BMC Oral Health. 2020;20(1):1–10. doi: 10.1186/s12903-020-01199-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ashley P, Di Iorio A, Cole E, Tanday A, Needleman I. Oral health of elite athletes and association with performance: a systematic review. Br J Sports Med. 2015;49(1):14–19. doi: 10.1136/bjsports-2014-093617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schlueter N, Luka B. Erosive tooth wear – a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018;224(5):364–370. doi: 10.1038/sj.bdj.2018.167 [DOI] [PubMed] [Google Scholar]
- 23.Zebrauskas A, Birskute R, Maciulskiene V. Prevalence of dental erosion among the young regular swimmers in Kaunas, Lithuania. J Oral Maxillofac Surg. 2014;5(2):1–7. doi: 10.5037/jomr.2014.5206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.WHO. Guidelines for Safe Recreational Water Environments: Swimming Pools and Similar Environments. 2006:3505–3518 [Google Scholar]
- 25.Abd El-Salam MM. Assessment of water quality of some swimming pools: a case study in Alexandria, Egypt. Environ Monit Assess. 2012;184(12):7395–7406. doi: 10.1007/s10661-011-2508-6 [DOI] [PubMed] [Google Scholar]
- 26.Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries enamel structure and the caries process in the dynamic process of demineralization and remineralization (part 2). J Clin Pediatr Dent. 2004;28(2):119–124. doi: 10.17796/jcpd.28.2.617404w302446411 [DOI] [PubMed] [Google Scholar]
- 27.Lussi A, Carvalho TS. Erosive tooth wear: a Multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2014;25:1–15. doi: 10.1159/000360380 [DOI] [PubMed] [Google Scholar]
- 28.Lussi A, Schlueter N, Rakhmatullina E, Ganss C. Dental erosion - an overview with emphasis on chemical and histopathological aspects. Caries Res. 2011;45(SUPPL. 1):2–12. doi: 10.1159/000325915 [DOI] [PubMed] [Google Scholar]
- 29.Addy M, Shellis P. Interaction between attrition, abrasion and erosion in tooth wear. Dent Eros. 2006;20:17–31. [DOI] [PubMed] [Google Scholar]
- 30.Lippert F. An introduction to toothpaste – its purpose, history and ingredients. Monogr Oral Sci Basel. 2013;23:1–14. doi: 10.1159/000350456 [DOI] [PubMed] [Google Scholar]
- 31.Ali S, Farooq I, Shahid F, Hassan U, Zafar MS. Common toothpastes abrasives and methods of evaluating their abrasivity. J Oral Res. 2020;9–15. doi: 10.17126/joralres [DOI] [Google Scholar]
- 32.Joiner A. Whitening toothpastes: a review of the literature. J Dent. 2010;38(suppl 2):e17–e24. doi: 10.1016/j.jdent.2010.05.017 [DOI] [PubMed] [Google Scholar]
- 33.Turssi CP, Messias DCF, De Menezes M, Hara AT, Serra MC. Role of dentifrices on abrasion of enamel exposed to an acidic drink. Am J Dent. 2005;18(4):251–255. [PubMed] [Google Scholar]
- 34.Pintado-Palomino K, Vasconcelos CVM, Silva RJD, et al. Effect of whitening dentifrices: a double-blind randomized controlled trial. Braz Oral Res. 2016;30(1):e82. doi: 10.1590/1807-3107BOR-2016.vol30.0082 [DOI] [PubMed] [Google Scholar]
- 35.Brooks JK, Bashirelahi N, Reynolds MA. Charcoal and charcoal-based dentifrices: a literature review. J Am Dent Assoc. 2017;148(9):661–670. doi: 10.1016/j.adaj.2017.05.001 [DOI] [PubMed] [Google Scholar]
- 36.Hunter ML, Addy M, Pickles MJ, Joiner A. The role of toothpastes and toothbrushes in the aetiology of tooth wear. Int Dent J. 2002;52(5):399–405. doi: 10.1111/j.1875-595X.2002.tb00729.x [DOI] [Google Scholar]
- 37.Subramanian S, Appukuttan D, Tadepalli A, Gnana PPS, Victor DJ. The role of abrasives in dentifrices. J Pharm Sci Res. 2017;9(2):221–224. [Google Scholar]
- 38.Kumar S, Kumar Singh S, Gupta A, Roy S, Sareen M, Khajuria S. A profilometric study to assess the role of toothbrush and toothpaste in abrasion process. J Dent. 2015;16(3Suppl):267–273. [PMC free article] [PubMed] [Google Scholar]
- 39.Tellefsen G, Liljeborg A, Johannsen A, Johannsen G. The role of the toothbrush in the abrasion process. Int J Dent Hyg. 2011;9(4):284–290. doi: 10.1111/j.1601-5037.2011.00505.x [DOI] [PubMed] [Google Scholar]
- 40.Ranzan N, Muniz F, Rosing C. Are bristle stiffness and bristle end-shape related to adverse effects on soft tissues during toothbrushing? A systematic review. Int Dent J. 2019;69:171–182. doi: 10.1111/idj.12421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Loomans B, Opdam N, Attin T, et al. Severe tooth wear: European consensus statement on management guidelines. J Adhes Dent. 2017;19(2):111–119. doi: 10.3290/j.jad.a38102 [DOI] [PubMed] [Google Scholar]
- 42.Mesko ME, Sarkis-Onofre R, Cenci MS, Opdam NJ, Loomans B, Pereira-Cenci T. Rehabilitation of severely worn teeth: a systematic review. J Dent. 2016;48:9–15. doi: 10.1016/j.jdent.2016.03.003 [DOI] [PubMed] [Google Scholar]
- 43.Carvalho TS, Colon P, Ganss C, et al. Consensus report of the European federation of conservative dentistry: erosive tooth wear—diagnosis and management. Clin Oral Investig. 2015;19(7):1557–1561. doi: 10.1007/s00784-015-1511-7 [DOI] [PubMed] [Google Scholar]
- 44.Geštakovski D. The injectable composite resin technique: minimally invasive reconstruction of esthetics and function. Quintessence Int. 2019;50(9):712–720. doi: 10.3290/j.qi.a43089 [DOI] [PubMed] [Google Scholar]
- 45.Hosaka K, Mizutani K, Tagami J, et al. Post-orthodontic recontouring of anterior teeth using composite injection technique with a digital workflow. J Esthet Restor Dent. 2020;32(7):638–644. doi: 10.1111/jerd.12619 [DOI] [PubMed] [Google Scholar]
- 46.Kemaloglu H, Ozkaya CA, Ergucu Z, Onal B. Follow-up of flowable resin composites performed with a universal adhesive system in non-carious cervical lesions: a randomized, controlled 24-month clinical trial. Am J Dent. 2020;33(1):39–42. [PubMed] [Google Scholar]
- 47.Kitasako Y, Sadr A, Burrow MF, Tagami J. Thirty-six month clinical evaluation of a highly filled flowable composite for direct posterior restorations. Aust Dent J. 2016;61(3):366–373. doi: 10.1111/adj.12387 [DOI] [PubMed] [Google Scholar]