

Summary:
Understanding salient environmental determinants of pediatric sleep is essential for informing interventions and public health initiatives. Emerging evidence suggests that the neighborhood environment can impact pediatric sleep, but this evidence has not yet been systematically reviewed. We conducted a systematic review of the scientific literature on associations between neighborhood environments and sleep in young children (0–5 years), school-aged children (6–12 years) and adolescents (13–18 years). We reviewed 85 articles published between 2003 and 2020. The most commonly examined neighborhood exposure was low socioeconomic status (40 studies), which was associated with sleep outcomes in 58% of studies (primarily shorter sleep duration, later sleep timing, or obstructive sleep apnea). Evidence was stronger for neighborhood safety/crime/violence (21 studies), with 86% of studies reporting associations with sleep outcomes (primarily self- or caregiver-reported sleep problems). Fewer studies examined associations of neighborhood physical environment exposures, including noise (15 studies), the built environment (seven studies), and air pollution (six studies). Limitations of the current body of evidence include 1) limited examination of neighborhood exposures other than socioeconomic status or safety, 2) use of primarily cross-sectional observational study designs, 3) lack of objective sleep outcome assessment, and 4) limits of current exposure assessment methods.
Keywords: Neighborhoods, Environment, Pediatric, Adolescents, Sleep, Socioeconomic status
BACKGROUND
Insufficent sleep is highly prevalent among children and adolescents [1], which is concerning given established links between insufficient sleep and adverse physical and mental health outcomes [2, 3]. As a modifiable behavior, sleep is a promising target for public health policies and interventions that aim to prevent future disease burden. However, in order to effectively intervene to improve sleep outcomes among children and adolescents, it is essential to identify key determinants of healthy sleep. An area that has received increasing attention is how neighborhood context influences sleep [4–7]. Due to structural factors including racial residential segregation and socioeconomic inequalities, neighborhoods contain varying levels of physical and social attributes that may influence sleep [4]. The neighborhood physical environment includes ambient factors (e.g. noise, air pollution) and the built environment (e.g. density, physical activity resources). The neighborhood social environment incorporates features related to interactions between people, including safety and social cohesion. Emerging evidence suggests that neighborhood socioeconomic, physical, and social features may influence sleep [4–7].
Although most studies of the relationship between neighborhood context and sleep have focused on adults, a growing body of evidence suggests that neighborhood environments influence sleep among children and adolescents [4–7]. However, there has not been a comprehensive evaluation of the literature on neighborhood determinants of sleep in pediatric populations. To address this gap, we conducted a systematic review of studies examining associations of neighborhood socioeconomic, social, and physical characteristics with sleep outcomes (e.g. duration, quality, variability, timing, problems, diagnoses) among children and adolescents. This paper reports data extracted from 85 studies, summarizes findings, and identifies methodological strengths and weaknesses in the current body of evidence. Using these results, we discuss opportunities for future research to fill key substantive and methodological gaps and advance understanding of the most salient environmental determinants of sleep among children and adolescents.
METHODS
Eligibility criteria
We adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting the systematic review and reporting results. Studies were eligible for inclusion if they were published in peer-reviewed journals in English, assessed associations of a neighborhood-level exposure with a sleep outcome, and included participants aged <18 years. We defined neighborhood-level exposures as area-level exposures assessed at a smaller spatial scale than the city-level (e.g. census tract). Articles that examined exposures only inside participants’ home were excluded. We also excluded articles where the exposure combined neighborhood and home context in the same measure (e.g. exposure to violence in both home and community settings). We included sleep outcomes that were objectively-measured, participant-reported, or caregiver-reported, which included: duration, timing, quality, variability, sleep problems, obstructive sleep apnea (OSA) symptoms, sleep-related impairment, and sleep diagnoses. We excluded articles that only assessed wheezing during sleep among children with asthma, which is indicative of asthma symptom severity rather than underlying sleep issues. We also excluded articles that combined pediatric and adult populations if they did not present subgroup analyses restricted to participants <18 years. Finally, we excluded review articles, published study protocols, non-human studies, and non-peer-reviewed articles.
Development of search terms
We consulted a librarian with expertise in systematic reviews prior to developing our search terms. We developed a preliminary set of search terms that included three concepts: 1) neighborhood environments, 2) sleep, 3) children and adolescents. Using these three concepts, we developed a set of Medical Subject Headings (MeSH) terms and key words for each subject, combined with an “AND” between each concept according to the Boolean search method. We piloted the set of search terms in Medline to determine whether the terms identified an a priori set of 16 benchmark articles that met our inclusion criteria. We reviewed reference lists of all included articles and prior reviews to identify additional eligible articles that were not returned by the initial search. Search terms were iteratively refined to ensure that they identified all benchmark papers and relevant references from included articles and past reviews. Our final set of search terms is available in the Supplemental Appendix.
Search and screening
We completed our search in Medline, PubMed, EMBASE, Web of Science, and PsychInfo on October 9, 2020. We searched titles, abstracts, and keywords, and restricted to English-language articles. No date restrictions were placed on the search. We identified 12,044 records, including duplicates (Figure 1). One additional article was identified through review of literature cited in included articles. After removal of duplicates, 6,733 titles/abstracts were screened to determine whether they met inclusion/exclusion criteria described above, yielding 275 candidate articles for full text review. Full texts were independently reviewed by 2 reviewers each to confirm eligibility. Eligibility ratings were compiled by the lead author (SM), and differences were discussed and resolved by group consensus. A total of 85 articles, published between 2003 and 2020, met eligibility criteria and were included in this review [8–92].
Figure 1.
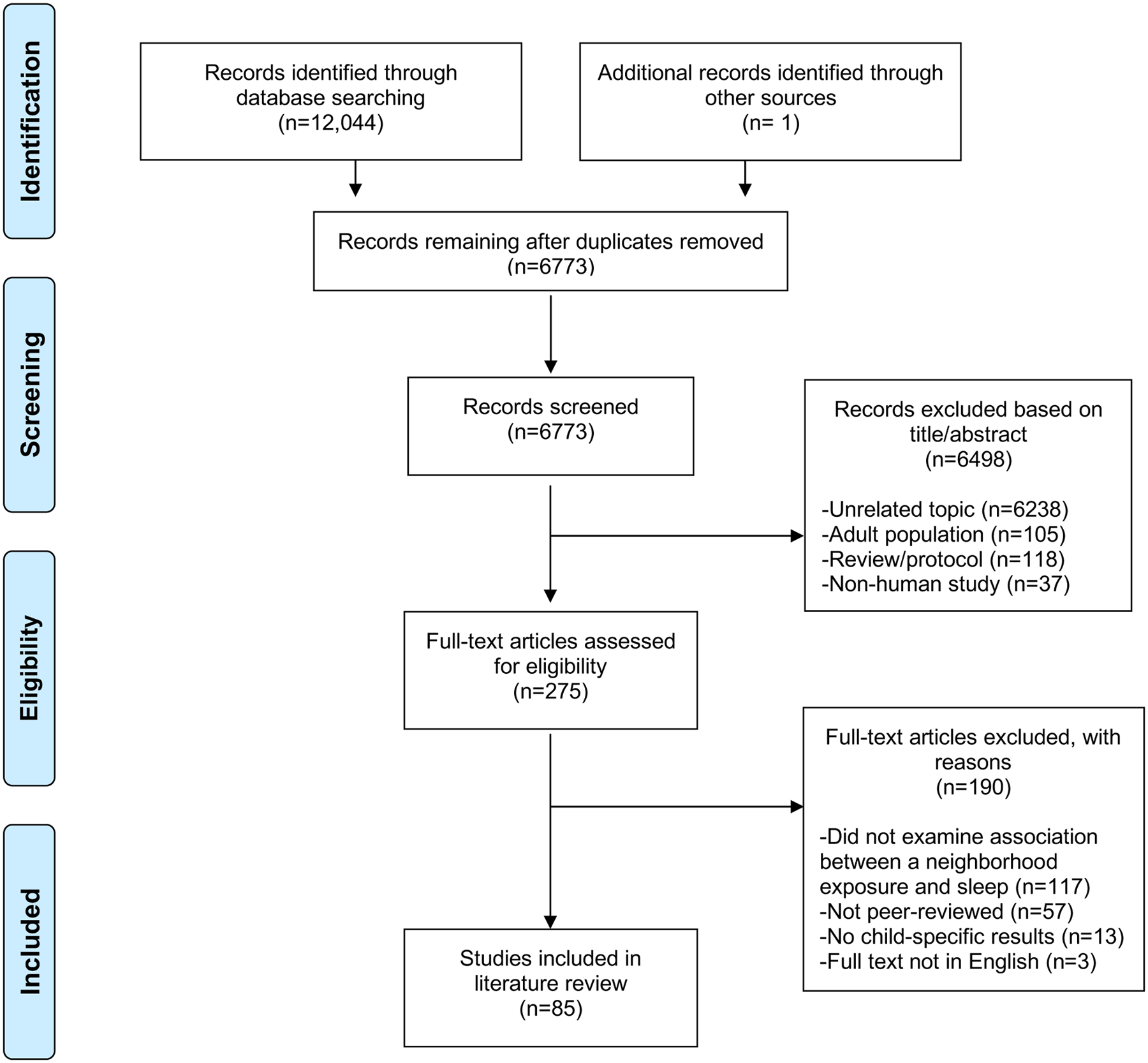
PRISMA 2009 flow diagram.
Data abstraction and synthesis
Two reviewers independently abstracted data from each included article using a standardized abstraction form. The elements abstracted included the study purpose, design, population, sample size, sampling methodology, sleep outcomes, neighborhood exposures, statistical analysis, covariate adjustment, findings, and subgroup analyses. We classified sleep outcomes as objective (e.g. actigraphy-based) or subjective (e.g. caregiver- or child-reported). We also classified neighborhood exposures as objective (e.g. census variables) or subjective (e.g. perceived safety). The lead author (SM) provided a synthesis of the abstraction results (Supplemental Table 1) for review by the authorship team; disagreements were resolved by consensus. We described patterns overall and across three pre-specified age groups: early childhood (0–5 years), school-aged children (6–12 years), and adolescents (13–17 years). In addition to summarizing the characteristics and key findings of the included studies, we assessed potential risk of bias at the study level according to the following prespecified features: study design (cross-sectional versus longitudinal), sleep assessment method (objectively measured versus caregiver- or child-reported), sampling strategy (probability-based versus non-probability-based), and control for confounding (multivariable modeling versus bivariate analysis).
RESULTS
Of the 85 articles that met inclusion criteria, 15 articles (18%) included young children (aged 0–5), 16 articles (19%) included school-aged children (aged 6–12), 15 articles (18%) included adolescents (aged 13–18), and 38 articles (45%) included multiple age groups. A majority of studies were conducted in the United States (51 studies, 60%). Thirteen studies were conducted in Australia and New Zealand, 10 studies in Europe (Germany, Netherlands, Norway, Poland, England, Sweden), four studies in Canada, two studies in Chile, and one study each in Egypt, Iran, Mexico, China, Taiwan, and South Korea. The median sample size was 436 (range 18 to 196,900).
Tables 1–3 present each study’s neighborhood measures and associations with sleep outcomes. The tables are organized by neighborhood domain: neighborhood socioeconomic status (SES, 40 studies, Table 1), neighborhood social environment (29 studies, Table 2), and neighborhood physical environment (32 studies, Table 3).
Table 1:
Results from studies examining neighborhood socioeconomic status and sleep (40 articles)
| Age group | Associations by sleep outcome | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author/year | Design | N | 0–5 | 6–12 | 13–17 | Exposure | Dur | Tim | Qual | Var | Prob | OSA | DTS | Oth |
| Bagley 2018 [10] | CR | 210 | X | SES index | act(+) | act(+) | ||||||||
| Biggs 2013 [14]a | CR | 1845 | X | X | SES index | par(+) | par(+) | |||||||
| Brouillette 2011 [17] | CR | 436 | X | X | Individual SES variables | psg(+) | ||||||||
| Cheon 2019 [19] | CR | 350 | X | Poverty | self(+) act(0) |
act(+) self(+) |
||||||||
| Côté-Lussier 2020 [20] | CR | 504 | X | % low income, % single parent | act(0) | |||||||||
| Dollman 2007 [22]a | CR | 900 | X | X | SES index | self(×) | ||||||||
| Dollman 2017 [21]a | CR | 1246 | X | X | SES index | self(+) | ||||||||
| Elder 2020 [25]b | CR | 70 | X | % low income | act(0) | act(+) | act(0) | |||||||
| El-Sheikh 2013 [24] | CR | 276 | X | Poverty | act(+) | act(0) | act(0) | self(0) | ||||||
| Gill 2012 [28]b | CR | 823 | X | SES index | par(+) | |||||||||
| Graham 2020 [29]a | CR | 16936 | X | Individual SES variables, economic stress | par(+) par(−) |
|||||||||
| Grimes 2019 [30] | CR | 80 | X | SES index | act(+) | |||||||||
| Hardy 2017 [32]a | CR | 7555 | X | X | X | SES index | self(0) | |||||||
| levers-Landis 2008 [36]a,b | CR | 819 | X | Median income | par(+) | |||||||||
| Jones 2014 [37]b | CR | 84 | X | SES index | par(0) | |||||||||
| Koinis-Mitchell 2015 [40] | CR | 249 | X | SES index | act(×) | act(0) | ||||||||
| MacKinnon 2020 [43] | LO | 2445 | X | SES index | par(0) | par(0) | ||||||||
| Martin 2017 [45] | CR | 346 | X | SES index | act(+) | act(0) | par(0) | |||||||
| McLaughlin 2005 [49]b | CR | 3371 | X | X | Median income | par(+) | par(+) | par(+) | par(+) | |||||
| Moore 2011 [51]a | CR | 247 | X | “Distressed” SES | act(0) | act(0) | ||||||||
| Olds 2010 [53]a | CR | 4032 | X | X | SES index | self(0) | ||||||||
| Orsey 2016 [54] | CR | 50 | X | X | Median income | act(0) | ||||||||
| Pabayo 2014 [56]a | CR | 1375 | X | SES index | self(−) | |||||||||
| Patrick 2016 [59]b | CR | 191 | X | Median income | par(+) | par(+) | ||||||||
| Patte 2017 [60] | CR/LO | 36088 / 7394 | X | Median income | self(+) | |||||||||
| Rubens 2016 [66] | CR | 207 | X | X | X | SES index | clin(0) | clin(0) | clin(×) | |||||
| Saelee 2020 [69]a | LO | 12692 | X | X | SES index | self(×) | ||||||||
| Sheehan 2018 [71] | LO | 2720 | X | X | Poverty | par(+) | ||||||||
| Spilsbury 2006 [75]a | CR | 843 | X | “Distressed” SES | psg(+) | |||||||||
| Spilsbury 2015 [76]a | LO | 490 | X | X | “Distressed” SES | psg(×) | ||||||||
| Street 2018 [78]a | CR | 1614 | X | SES index | self(−) | |||||||||
| Tamanyan 2016 [79]b | CR | 301 | X | X | X | SES index | psg(0) | |||||||
| Troxel 2017 [81] | CR | 2493 | X | Poverty | self(0) | self(−) | self(0) | self(0) | ||||||
| Uebergang 2017 [82]a,b | CR | 4901 | X | X | SES index | par(0) | ||||||||
| Wang 2017 [85] | CR | 774 | X | X | “Distressed” SES | psg(+) | ||||||||
| Williamson 2019 [89]a | LO | 4517 | X | X | SES/Social/Physical index | par(0) | ||||||||
| Williamson 2020a [88] | CR | 205 | X | SES index | par(0) | par(0) | ||||||||
| Xie 2018 [90]b | CR | 158 | X | X | X | Median income | psg(0) | |||||||
| Zhang 2019 [91]a | CR | 173 | X | SES index | act(0) | act(0) | par(0) | |||||||
| Zhao 2019 [92]b | CR | 882 | X | X | SES index | par(+) | ||||||||
CR: cross-sectional; LO: longitudinal; SES: socioeconomic status; dur: sleep duration (continuous or dichotomized to reflect obtaining sufficient versus insufficient sleep duration); tim: sleep timing (bedtime, waketime, onset, offset, delay in sleep onset); qual: sleep quality (e.g. efficiency, wake after sleep onset, latency, night awakenings/wake episodes, self-reported quality); var: variability in sleep duration or timing; prob: subjectively reported sleep problems or disturbances; OSA: obstructive sleep apnea diagnosis, symptoms, snoring; DTS: daytime sleepiness, tiredness, napping; oth: other outcomes (e.g. parasomnias); par: parent/care-giver-reported; self: self-reported; act: assessed using actigraphy; clin: based on clinical assessment; psg: assessed using in-lab polysomnography or in-home overnight cardiorespiratory studies.
(+) indicates a significant positive association (better neighborhood environment associated with better sleep outcomes)
(0) indicates no association
(−) indicates a significant negative association (better neighborhood environment associated with worse sleep outcomes)
(×) indicates an interaction/association only significant in a subgroup of the study population
(+)(0) indicates findings varied based on assessment type (objective or subjective)
Study used probability-based sampling methods (e.g. random selection of households or classrooms)
Results from bivariate analysis only
Table 3:
Results from studies examining the neighborhood physical environment and sleep (32 articles)
| Age group | Associations by sleep outcome | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author/year | Design | N | 0–5 | 6–12 | 13–17 | Exposure | Dur | Tim | Qual | Var | Prob | OSA | DTS | Oth |
| Neighborhood noise (15 articles) | ||||||||||||||
| Belmon 2020 [13]c | QL/CR | 45 / 33 | X | Perceived noise | self(0) par(+) |
|||||||||
| Feng 2020 [26]a | CR | 11916 | X | X | Perceived noise | self(0) | self(×) | |||||||
| Gaarde 2020 [27]c | QL/CR | 142 | X | Perceived noise | self(+) | |||||||||
| Lindsay 2018 [42]c | QL/CR | 37 | X | Perceived noise | par(+) | |||||||||
| Martin-Biggers 2015 [46]c | QL/CR | 139 | X | Perceived noise | par(+) | |||||||||
| Martinez 2015 [47]c | QL/CR | 18 | X | Perceived noise | par(+) | |||||||||
| Ohrstrom 2006 [52]b | CR | 160 (79)* | X | Road traffic noise | act(0) | self(+) act(0) |
self(+) | self(+) | ||||||
| Palimaru 2020 [58]c | QL/CR | 26 | X | X | Perceived noise | self(+) | ||||||||
| Rudolph 2019 [67]a | CR | 4508 | X | Ambient outdoor noise | self(0) | self(+) | ||||||||
| Sadler 2020 [68]c | QL/CR | 25 | X | Perceived noise | par(+) | |||||||||
| Skrzypek 2017 [73] | CR | 5136 | X | X | Road traffic noise | par(+) | ||||||||
| Spilsbury 2016 [74]c | QL/LO | 65 | X | X | Perceived noise | self(+) | ||||||||
| Stansfeld 2010 [77]b | LO | 326 | X | Aircraft noise | self(0) | |||||||||
| Tiesler 2013 [80] | CR | 872 | X | Ambient outdoor noise | par(+) | |||||||||
| Weyde 2017 [86] | CR | 2665 | X | Road traffic noise | par(×) | par(0) | ||||||||
| Neighborhood built environment (7 articles) | ||||||||||||||
| Aguilar-Farias 2020 [9]a | CR | 148 | X | Perceived walkability, distance to places | act(0) | |||||||||
| Bottino 2012 [16] | CR | 1226 | X | Urbanicity, density, distance to major road | par(+) | |||||||||
| Côté-Lussier 2020 [20] | CR | 504 | X | Traffic density, residential density, land use mix | act(0) | |||||||||
| Ha 2020 [31] | CR | 3917 | X | X | X | Distance to major road | par(+) | |||||||
| Marco 2011 [44] | CR | 155 | X | X | Physical condition, street environment | act(0) | act(×) | act(+) | ||||||
| Philbrook 2016 [62] | CR | 231 | X | Perceived recreation facilities | act(+) | act(+) | act(0) | act(0) | ||||||
| Singh 2013 [72]a | CR | 63352 | X | X | Perceived built environment index | par(+) | ||||||||
| Air pollution (6 articles) | ||||||||||||||
| Abou-Khadra 2013 [8]a | CR | 276 | X | X | Air pollution (PM10) | par(+) | ||||||||
| Bose 2019 [15] | LO | 397 | X | Air pollution (PM2.5) | act(+) | act(+) | ||||||||
| Kannan 2017[38] | LO | 609 | X | Traffic-related air pollution | par(+) | |||||||||
| Kheirandish-Gozal 2014 [39]a | CR | 4322 | X | X | Air pollution (multiple types) | par(+) | ||||||||
| Lawrence 2018 [41]a | CR | 59754 | X | X | X | Air pollution (multiple types) | self(+) | |||||||
| Sanchez 2019 [70] | CR | 564 | X | X | Air pollution (multiple types) | par(0) | ||||||||
| Outdoor Light (4 studies) | ||||||||||||||
| Côté-Lussier 2020 [20] | CR | 504 | X | Outdoor light at night | act(0) | |||||||||
| Paksarian 2020 [57]a | CR | 10123 | X | Outdoor light at night | self(+) | self(+) | ||||||||
| Spilsbury 2016 [74]c | QL/LO | 65 | X | X | Perceived outdoor light | self(+) | ||||||||
| Vollmer 2012 [83] | CR | 1507 | X | X | Outdoor light at night | self(+) | ||||||||
| Other Physical Environment Measures (7 articles) | ||||||||||||||
| Feng 2020 [26]a | CR | 11916 | X | X | Green space | self(×) | self(0) | |||||||
| Huss 2016 [35] | LO | 2361 | X | REMF | par(+) | par(0) | par(0) | par(0) | par(−) | |||||
| Williamson 2019 [89]a | LO | 4517 | X | X | SES/Social/Physical index | par(0) | ||||||||
CR: cross-sectional; LO: longitudinal; dur: sleep duration (continuous or dichotomized to reflect obtaining sufficient versus insufficient sleep duration); tim: sleep timing (bedtime, waketime, onset, offset, delay in sleep onset); qual: sleep quality (e.g. efficiency, wake after sleep onset, latency, night awakenings/wake episodes, self-reported quality); var: variability in sleep duration or timing; prob: subjectively reported sleep problems or disturbances; OSA: obstructive sleep apnea diagnosis, symptoms, snoring; DTS: daytime sleepiness, tiredness, napping; oth: other outcomes (e.g. parasomnias, chronotype, qualitative assessment of sleep barriers); par: parent/care-giver -reported; self: self-reported; act: assessed using actigraphy; clin: based on clinical assessment; psg: assessed using in-lab polysomnography or in-home overnight cardiorespiratory studies.
(+) indicates a significant positive association (better neighborhood environment associated with better sleep outcomes)
(0) indicates no association
(−) indicates a significant negative association (better neighborhood environment associated with worse sleep outcomes)
(×) indicates an interaction/association only significant in a subgroup of the study population
(+)(0) indicates findings varied based on assessment type (objective or subjective)
Study used probability-based sampling methods (e.g. random selection of households or classrooms)
Results from bivariate analysis only
Qualitative study assessing perceived barriers and/or facilitators of child sleep
Subsample with actigraphy
Table 2:
Results from studies examining the neighborhood social environment and sleep (29 articles)
| Age group | Associations by sleep outcome | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author/year | Design | N | 0–5 | 6–12 | 13–17 | Exposure | Dur | Tim | Qual | Var | Prob | OSA | DTS | Oth |
| Neighborhood safety/crime/community violence (21 articles) | ||||||||||||||
| Bagley 2016 [11] | CR | 252 | X | Community violence concerns | act(0) | act(×) | self(+) | self(+) | ||||||
| Bailey 2005 [12] | CR | 268 | X | Community violence exposure | self(+) | |||||||||
| Belmon 2020 [13]c | QL/CR | 45 / 33 | X | Perceived safety | self(0) par(+) |
|||||||||
| Chen 2013 [18]a | CR | 2113 | X | Perceived safety | self(+) | |||||||||
| Dowdell 2003 [23]b | CR | 54 | X | X | Perceived safety | self(+) | ||||||||
| Hawkins 2016 [33]a | CR | 196900 | X | X | Perceived safety | par(×) | ||||||||
| Heissel 2017 [34] | LO | 82 | X | X | Objective crime | act(+) | act(+) | act(+) | ||||||
| MacKinnon 2020 [43] | LO | 2445 | X | Perceived safety | par(+) | par(0) | ||||||||
| Martinez 2015 [47]c | QL/CR | 18 | X | Perceived crime | par(+) | |||||||||
| McHale 2011 [48] | CR | 469 | X | X | Perceived crime | self(0) | self(0) | self(+) | ||||||
| Meldrum 2018 [50]a | CR | 7958 | X | X | Perceived safety | self(+) | ||||||||
| Owens 2006 [55]c | QL/CR | 64 | X | X | Perceived safety | self(+) | ||||||||
| Pabayo 2014 [56]a | CR | 1375 | X | Perceived safety | self(0) | |||||||||
| Objective crime | self(−) | |||||||||||||
| Philbrook 2019 [61] | CR | 219 | X | Community violence concerns | act(×) | act(×) | ||||||||
| Rubens 2014 [63] | CR | 144 | X | Community violence exposure | self(+) | |||||||||
| Sadler 2020 [68]c | QL/CR | 25 | X | Perceived safety | par(+) | |||||||||
| Spilsbury 2016 [74]c | QL/LO | 65 | X | X | Perceived safety | self(+) | ||||||||
| Street 2018 [78]a | CR | 1614 | X | Objective crime | self(0) | |||||||||
| Troxel 2017 [81] | CR | 2493 | X | Perceived safety | self(0) | self(0) | self(0) | self(0) | ||||||
| Wamser-Nanney 2018 [84]b | CR | 276 | X | X | Community violence exposure | par(+) | ||||||||
| Williamson 2020b [87]c | QL/CR | 23 | X | Perceived safety | par(+) | |||||||||
| Neighborhood social cohesion/collective efficacy (5 articles) | ||||||||||||||
| Aguilar-Farias 2020 [9]a | CR | 148 | X | Collective efficacy | act(0) | |||||||||
| Hawkins 2016 [33]a | CR | 196900 | X | X | Social cohesion | par(+) | ||||||||
| Pabayo 2014 [56]a | CR | 1375 | X | Social cohesion | self(+) | |||||||||
| Street 2018 [78]a | CR | 1614 | X | Collective efficacy | self(0) | |||||||||
| Troxel 2017 [81] | CR | 2493 | X | Social cohesion | self(0) | self(0) | self(0) | self(+) | ||||||
| Neighborhood Disorder (4 articles) | ||||||||||||||
| Graham 2020 [29]a | CR | 16936 | X | Disorder | par(+) | |||||||||
| MacKinnon 2020 [43] | LO | 2445 | X | Disorder | par(+) | par(0) | ||||||||
| Pabayo 2014 [56]a | CR | 1375 | X | Disorder | self(0) | |||||||||
| Street 2018 [78]a | CR | 1614 | X | Disorder | self(0) | |||||||||
| Neighborhood Social Fragmentation/Disorganization (3 articles) | ||||||||||||||
| Bagley 2018 [10] | CR | 210 | X | Social fragmentation | act(0) | act(+) | ||||||||
| Pabayo 2014 [56]a | CR | 1375 | X | Social fragmentation | self(+) | |||||||||
| Saelee 2020 [69]a | LO | 12692 | X | X | Social disorganization | self(×) | ||||||||
| Neighborhood Social Environment Index (3 articles) | ||||||||||||||
| Rubens 2018 [64] | CR | 144 | X | Social environment index | self(+) | |||||||||
| Rubens 2020 [65] | CR/LO | 44 | X | X | Social environment index | self(0) | self(0) | self(0) | ||||||
| Singh 2013 [72]a | CR | 63352 | X | X | Social environment index | par(+) | ||||||||
| Williamson 2019 [89]a | LO | 4517 | X | X | SES/Social/Physical index | par(0) | ||||||||
CR: cross-sectional; LO: longitudinal; QL: qualitative, dur: sleep duration (continuous or dichotomized to reflect obtaining sufficient versus insufficient sleep duration); tim: sleep timing (bedtime, waketime, onset, offset, delay in sleep onset); qual: sleep quality (e.g. efficiency, wake after sleep onset, latency, night awakenings/wake episodes, self-reported quality); var: variability in sleep duration or timing; prob: subjectively reported sleep problems or disturbances; OSA: obstructive sleep apnea diagnosis, symptoms, snoring; DTS: daytime sleepiness, tiredness, napping; oth: other outcomes (e.g. parasomnias, qualitative assessment of sleep barriers); par: parent/care-giver -reported; self: self-reported; act: assessed using actigraphy; clin: based on clinical assessment; psg: assessed using in-lab polysomnography or in-home overnight cardiorespiratory studies.
(+) indicates a significant positive association (better neighborhood environment associated with better sleep outcomes)
(0) indicates no association
(−) indicates a significant negative association (better neighborhood environment associated with worse sleep outcomes)
(×) indicates an interaction/association only significant in a subgroup of the study population
(+)(0) indicates findings varied based on assessment type (objective or subjective)
Study used probability-based sampling methods (e.g. random selection of households or classrooms)
Results from bivariate analysis only
Qualitative study assessing perceived barriers and/or facilitators of child sleep
Neighborhood socioeconomic status
Overall, lower neighborhood SES was associated with poorer sleep outcomes in 23 out of 40 studies (58%, Table 2). Specifically, lower SES was associated with shorter sleep duration in 13 out of 25 of studies (52%) [10, 14, 19, 21, 22, 24, 36, 45, 49, 59, 60, 69, 71], later sleep timing in five out of six studies (86%) [14, 25, 29, 49, 92], OSA/snoring in five out of nine studies (56%) [17, 28, 75, 76, 85], and poorer sleep quality (e.g. efficiency) in four out of ten studies (40%) [10, 19, 30, 59]. Studies including 0–5 and 6–12 year old children were more likely to report associations between lower SES and poorer sleep outcomes compared to studies among adolescents. Three studies found results in the opposite direction for adolescents, with teens living in more socioeconomically deprived neighborhoods having longer sleep duration [56, 78] and earlier bedtimes [81] in some models.
All studies that included neighborhood SES exposures used administrative data from the U.S. Census Bureau or similar government organizations. Studies that defined SES using a single indicator (e.g. poverty) were more likely to identify associations for sleep duration, timing, and OSA/snoring than studies defining SES using an index, although this pattern did not hold true for sleep quality. Studies that measured sleep subjectively were more likely to report associations of low SES with shorter sleep duration and poorer sleep quality than studies with objective sleep measurement, while the opposite was true for sleep timing and OSA/snoring.
While most studies used cross-sectional designs, six studies examined neighborhood SES and sleep outcomes longitudinally [43, 60, 69, 71, 76, 89]. Three of the four longitudinal cohorts (75%) that examined SES and self- or caregiver-reported sleep duration identified associations of lower SES with shorter sleep duration, overall [60, 71] or among girls only [69]. Cross-sectional studies were much more numerous but were less likely to identify associations between lower SES and shorter sleep duration (11 out of 22, 50%). However, no longitudinal studies of SES assessed sleep duration objectively, while 41% of cross-sectional studies did (9 out of 22). There was less evidence in longitudinal studies for associations of SES with other outcomes. One community-based US study found low neighborhood SES to be associated with OSA in middle childhood but not in adolescence [76], while a nationally representative Australian birth cohort study found no association between a neighborhood socioeconomic risk index and sleep problem trajectories from age 0–11 [89].
Neighborhood social environment
Table 2 summarizes results from 29 studies that examined neighborhood social environment exposures and sleep, of which 24 studies (86%) found associations between a poorer neighborhood social environment and adverse sleep outcomes. The most commonly examined exposures were neighborhood safety, crime, and community violence (21 studies), followed by neighborhood social cohesion/collective efficacy (five studies), disorder (four studies), and social fragmentation/disorganization (three studies). Four studies constructed indices of multiple neighborhood social environment exposures [64, 65, 72, 89].
Eighteen studies (86%) found that living in a neighborhood with high crime/violence or lower perceived safety was associated with poorer sleep outcomes. Six of these studies were qualitative and identified neighborhood safety as a caregiver- or child-reported barrier to sleep [13, 47, 55, 68, 74, 87]. When examining specific sleep outcomes, lower neighborhood safety was most frequently associated with self-reported sleep problems (five out of six studies, 83% [11, 12, 18, 63, 84]), followed by sleep quality (three out of four studies, 75% [11, 34, 61]), sleep timing (two out of three studies, 67% [23, 34]) and sleep duration (five out of ten studies, 50% [33, 34, 43, 50, 61]). The majority of studies assessing neighborhood neighborhood safety/crime included school-aged or adolescent populations, with significant associations most common among school-aged children.
Few neighborhood social environment studies used actigraphy to assess sleep duration, timing, or quality, but those that did were more likely to identify associations with neighborhood safety/crime compared to studies assessing these outcomes subjectively [11, 34, 61]. Only three studies used police-recorded crime data as opposed to neighborhood perceptions [34, 56, 78], with only one reporting associations between neighborhood violent crime and actigraphy-assessed later bedtime, shorter sleep duration, and greater sleep latency [34]. Two studies of neighborhood crime/safety and sleep used longitudinal designs, which identified associations between lower maternal perceived neighborhood safety and shorter caregiver-reported sleep duration among infants [43] and between objective neighborhood crime and later bedtime assessed via actigraphy among 11–18 year olds [34]. Results for sleep duration and timing were more mixed among cross-sectional studies compared to longitudinal studies, with three out of eight studies reporting associations for sleep duration [33, 50, 61] and one out of two with sleep timing [23]).
Among the remaining neighborhood social exposures, a small number of studies provided evidence of associations with primarily subjectively-measured sleep outcomes. For example, two out of five studies (40%) reported associations between greater social cohesion/collective efficacy and increased self- or caregiver-reported sleep duration [33, 56], but the single study that assessed sleep duration objectively did not report an association [9]. Neighborhood social fragmentation/disorganization was associated with shorter self-reported sleep duration [56, 69], but not with actigraphy-assessed duration [10], among adolescents. All studies of social cohesion and social fragmentation were cross-sectional. Finally, neighborhood disorder was associated with later caregiver-reported bedtime among kindergarteners in a large nationally representative cross-sectional study [29] and with shorter caregiver-reported sleep duration at age 12 months in a large longitudinal birth cohort [43], but not with self-reported sleep duration in teens [56, 78]. No studies of neighborhood disorder assessed sleep outcomes objectively.
Neighborhood physical environment
Table 3 summarizes results for 32 studies that examined neighborhood physical environment exposures, most commonly noise (15 studies) or the built environment (e.g. percent urban land use, access to recreational facilities; seven studies). Other physical environment exposures included air pollution (five studies), nighttime outdoor light (four studies), green space (one study), exposure to radiofrequency electromagnetic fields (REMF) from mobile phone base stations (one study), and an index of neighborhood SES, physical, and social features (one study). In total, 27 of 32 studies (84%) reported associations between a poorer neighborhood physical environment and worse sleep.
There were eight qualitative studies in which children or caregivers mentioned noise outdoors as a potential barrier to sleep [12, 27, 42, 46, 47, 58, 68, 74]. The remaining seven studies that included neighborhood noise assessed quantitative associations with specific sleep outcomes, of which six (86%) identified associations of higher neighborhood noise with poorer sleep [26, 52, 67, 73, 80, 86]. Higher neighborhood noise was most frequently associated with self-reported sleep problems (three out of four studies [52, 73, 80]) and quality (two out of three studies [26, 52]). Increased neighborhood noise was associated with later self-reported bedtimes in a nationally representative survey of U.S. adolescents [67], the only study to examine this sleep outcome. There was less evidence for sleep duration (one out of four studies found an association among girls only [86]). Studies were primarily cross-sectional and based on subjective sleep assessment, with no association found between noise and objectively measured sleep duration in the one study that used actigraphy [52], or between noise and self-reported sleep quality in the single longitudinal study [77]. No studies examining neighborhood noise included children below age 6.
For the remaining neighborhood physical environment exposures, the number of studies reporting associations between any particular exposure-outcome pair was small. Among seven studies assessing the built environment, those that assessed sleep duration subjectively were more likely to report associations (two out of two studies [16, 72]) compared to studies assessing duration objectively (one out of four studies [62]). A poorer built environment was also associated with later sleep timing [44, 62], increased variability [44], and OSA symptoms [31]. All built environment studies were cross-sectional. For air pollution, five out of six studies identified associations with poorer sleep outcomes including sleep problems [8, 41], caregiver-reported OSA/snoring [38], and objectively-measured quality and duration [15], which included findings from two longitudinal studies [15, 38]. Exposure to outdoor light at night based on satellite imagery was associated cross-sectionally with shorter self-reported sleep duration and later bedtime [57] and later chronotype [83], but not with objectively-measured sleep duration [20].
Discussion
In this systematic review of the role of neighborhood context in pediatric sleep, the most commonly examined exposure was neighborhood SES, followed neighborhood safety, crime, or violence. Overall, 78% of published studies reported a significant association in the expected direction for at least one outcome (e.g. poorer neighborhood environment associated with worse sleep outcomes). Associations were more consistently positive for the neighborhood social environment (86%) and physical environment (84%) compared to neighborhood SES (58%), but there was high heterogeneity in terms of the types of exposures and sleep outcomes measured.
For neighborhood SES, evidence of associations with sleep outcomes was mixed across all age groups and varied by sleep outcome, with the most consistent findings for later sleep timing. These results align with findings from adult populations. Lower neighborhood SES has been associated with shorter sleep duration [99] and poorer sleep quality [100] in adults, but other studies of adults have not found associations [101, 102]. The mixed findings may relate to the challenge of measuring the underlying construct of neighborhood SES, which is a composite of individual measures such as education, employment, and poverty that may impact individuals within a neighborhood differently. While some studies in our review examined individual elements of SES, others combined multiple indicators into an index. In addition, there may be variation in how sleep outcomes, particularly sleep quality, are defined across studies (e.g. actigraphy derived sleep efficiency versus subjective assessments of sleep quality).
It is also important to note that sleep patterns and the nature of caregiver- or child-reported sleep problems change considerably over development, which may introduce additional variability. Among young children, more proximal child and family-level factors such as child temperament, caregiver-child interactions, and family routines may exert a greater influence on child sleep patterns and caregiver perceptions of child sleep problems [103]. As children age, their sleep becomes increasingly self-regulated and might be more strongly impacted by their neighborhood context. During the transition to adolescence, biological and social factors including puberty, early school start times, and extracurricular demands increasingly impact sleep patterns [104, 105]. This might explain findings from several studies indicating that adolescents in higher SES neighborhoods had shorter sleep durations and later bedtimes [56, 78, 81].
The most consistent evidence among published articles was for an association between neighborhood safety, crime, or community violence and adverse subjectively-measured sleep problems. Neighborhood crime/violence is hypothesized to influence sleep through stress processes, which trigger a state of arousal that could interfere with falling or staying asleep [11]. Concerns about safety may also influence daytime behaviors that impact sleep, by reducing physical activity [106] and increasing time engaged in sedentary, screen-based activities [107]. To increase understanding of how neighborhood crime may impact sleep, future studies should empirically test whether policies and interventions that reduce crime have a positive impact on sleep outcomes. For example, a place-based intervention that converted vacant lots into green spaces increased perceptions of safety among residents and reduced crime rates [108], but it is unknown whether such interventions impact sleep.
The next section will outline four limitations of the current literature on the influence of neighborhood environments on pediatric sleep outcomes: 1) limited examination of neighborhood exposures beyond SES or safety, 2) use of primarily cross-sectional observational study designs, 3) lack of objective sleep outcome assessment, and 4) limits of current exposure assessment methods.
Limited examination of neighborhood exposures beyond SES or safety
While studies included in this review identified significant associations of air pollution, built environment features, and social cohesion with sleep outcomes, the number of studies examining each of these exposures was small. Neighborhood noise was the third most common exposure, but half of these studies were qualitative and did not estimate associations of quantitative noise exposure with specific sleep outcomes. Features of the physical environment deserve increased attention given its potential to be modified through public health policies and interventions (e.g., built environment improvements, noise reduction limits). Also, few studies examined associations of neighborhood social or physical exposures with OSA.
For comparison, we also examined neighborhood exposures in adult studies excluded from our review. Neighborhood exposures examined among adults were similar to those identified in this review, although we identified several additional exposures: neighborhood crowding [93], stigma [94], social capital [95], food environment [96], and proximity to chemical or natural gas pollutants [97, 98]. Neighborhood crowding, stigma, and proximity to shale gas drilling and chemical superfund sites were associated with poorer sleep outcomes in adults. Future studies should examine associations of these exposures with sleep outcomes among children.
Use of primarily cross-sectional observational designs
Another limitation is that most published studies examining neighborhood environments and pediatric sleep have used cross-sectional designs. These studies provide evidence of associations between neighborhood exposures and sleep, but are limited in making causal assertions. Although reverse causality is unlikely, as child sleep outcomes are not likely to impact neighborhood exposures, there is a strong likelihood of residual confounding in cross-sectional studies. Longitudinal studies facilitate adjustment for time-varying covariates and also allow for statistical analyses comparing within-person changes in sleep outcomes in response to within-person changes in neighborhood exposures, whether due to residential relocation or changes in neighborhood characteristics over time. Such designs inherently control for confounding by time-invariant covariates, both measured and unmeasured. Cross-sectional designs also preclude examination of neighborhood exposures that change over time. In our review, only one study examined neighborhood change, by estimating trajectories of neighborhood poverty over a 40-year period [71]. More work is needed to understand the impact of neighborhood change on sleep outcomes.
In addition, all studies in our review used observational data. This is typical for research examining associations of neighborhood environments with health outcomes, as practical and ethical constraints limit randomization of exposure to many environmental exposures. However, some neighborhood features may be manipulated through randomized experiments, such as the urban greening intervention mentioned previously [108]. In addition, the use of natural experiments and quasi-experimental designs could strengthen causal inference by examining how sleep outcomes change in response to policy changes or place-based interventions.
Lack of objective sleep outcome assessment
Another limitation is that relatively few studies used objective sleep assessment. While subjective measurement is important for certain outcomes, such as perceived sleep problems and subjective sleep quality, objective sleep assessment may improve assessment of outcomes including sleep duration, efficiency, and variability. Prior studies have found that adolescents may over-report their sleep duration in comparison to actigraphy [109] and that caregivers and adolescents may under-report child sleep problems despite showing poor sleep patterns [110], leading to substantial variation between objectively and subjectively measured outcomes. Studies with objective sleep assessment tended to be smaller in size; the largest sample size in our review for a study with actigraphy was 397 [15]. The growing number of commercially available wearable sleep trackers may improve capacity for examining sleep objectively on a larger scale and over longer time periods, although validation of wearables against gold standard measurements is needed.
Limits of current exposure assessment methods
Most studies have focused exclusively on participants’ residential neighborhood. However, children and adolescents spend substantial amounts of time at school, in transit, and at other locations, leading to measurement error in exposure assessment when focusing only on the home [111]. Mobile health methods (e.g. GPS tracking; ecological momentary assessment) offer an opportunity to improve exposure assessment by capturing neighborhood exposures across multiple contexts, although privacy concerns must be addressed in the context of this work. In addition, the availability of devices that facilitate personal monitoring of noise and air pollution will improve researchers’ ability to construct person-centric environmental exposure measures.
Limitations of review
Our review was subject to several limitations. First, we focused on peer-reviewed articles and may have omitted null research findings that remain unpublished. Second, given the high level of heterogeneity in neighborhood exposures and sleep outcomes measured, we were unable to conduct a meta-analysis, instead conducting a qualitative evidence synthesis. Third, we restricted to English-language articles, which may have omitted relevant studies published in other languages. However, exclusion of non-English and unpublished studies has been found to have limited effect on the results and conclusions of systematic reviews/meta-analyses [112].
Conclusion
Our review identified evidence to suggest that neighborhood safety/crime/violence impedes sleep among school-aged children and adolescents. There is also emerging evidence to support the importance of noise, the built environment, air pollution and social cohesion, although more research in these areas is needed. Future research should expand investigation to additional physical and social environmental factors. In addition, there is a need for more studies using longitudinal or quasi-experimental designs to understand whether the associations identified in this review are causal, as well as more objective measurement of sleep for outcomes related to sleep duration and timing.
Supplementary Material
Practice Points.
1. Most studies included in our review reported associations between less favorable neighborhood environmental conditions and poorer sleep outcomes among children and adolescents.
2. Neighborhood socioeconomic status has been examined most frequently, and was associated with shorter sleep duration, later sleep timing, and obstructive sleep apnea diagnoses/symptoms in over half of studies.
3. The most consistent evidence is for an association of neighborhood safety/crime/violence with greater perceived sleep problems.
Research Agenda.
In the future, research should focus on:
1. Examining a wider range of neighborhood exposures beyond neighborhood socioeconomic status and safety/crime/community violence, which have been most studied to date.
2. Utilizing longitudinal and experimental study designs to improve causal inference and examine neighborhood change.
3. Greater inclusion of objectively measured sleep outcomes in addition to perceived measures
4. Improving environmental exposure assessment through GPS tracking and personal monitoring of exposures that vary over time (e.g. noise, air pollution).
Acknowledgements:
We thank Shannon Kelleher, William Drust, Olivia Cicalese, Gabrielle DiFiore, Chloe Hannan, and Tomiko Hackett for assistance with data abstraction. Stephanie L. Mayne was supported by the Possibilities Project at the Children’s Hospital of Philadelphia. Jonathan A. Mitchell was supported by NIH/NHLBI Career Development Award K01HL123612. Ariel A. Williamson was supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development Career Development Award K23HD094905 and by the Sleep Research Society Foundation.
Abbreviations:
- MeSH
medical subject headings
- OSA
obstructive sleep apnea
- PRISMA
preferred reporting items for systematic reviews and meta-analyses
- REMF
radiofrequency electromagnetic fields
- SES
socioeconomic status
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Financial Disclosure: The authors have no financial relationships relevant to this article to disclosure.
Conflict of Interest: The authors have no conflicts of interests relevant to this article to disclose
References:
- 1.Wheaton AG, Jones SE, Cooper AC, Croft JB. Short Sleep Duration Among Middle School and High School Students - United States, 2015. MMWR Morb Mortal Wkly Rep. 2018;67(3):85–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Roberts RE, Duong HT. Is there an association between short sleep duration and adolescent anxiety disorders? Sleep Med. 2017;30:82–7. [DOI] [PubMed] [Google Scholar]
- 3.Rudnicka AR, Nightingale CM, Donin AS, Sattar N, Cook DG, Whincup PH, et al. Sleep Duration and Risk of Type 2 Diabetes. Pediatrics. 2017;140(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Billings ME, Hale L, Johnson DA. Physical and Social Environment Relationship With Sleep Health and Disorders. Chest. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hale L, Emanuele E, James S. Recent Updates in the Social and Environmental Determinants of Sleep Health. Curr Sleep Med Rep. 2015;1(4):212–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hunter JC, Hayden KM. The association of sleep with neighborhood physical and social environment. Public Health. 2018;162:126–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Johnson DA, Billings ME, Hale L. Environmental Determinants of Insufficient Sleep and Sleep Disorders: Implications for Population Health. Curr Epidemiol Rep. 2018;5(2):61–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abou-Khadra MK. Association between PM(1)(0) exposure and sleep of Egyptian school children. Sleep Breath. 2013;17(2):653–7. [DOI] [PubMed] [Google Scholar]
- 9.Aguilar-Farias N, Martino-Fuentealba P, Chandia-Poblete D. Correlates of device-measured physical activity, sedentary behaviour and sleeping in children aged 9–11 years from Chile: ESPACIOS study. Retos-Nuevas Tendencias En Educacion Fisica Deporte Y Recreacion. 2020(37):1–10. [Google Scholar]
- 10.Bagley EJ, Fuller-Rowell TE, Saini EK, Philbrook LE, El-Sheikh M. Neighborhood Economic Deprivation and Social Fragmentation: Associations With Children’s Sleep. Behav Sleep Med. 2018;16(6):542–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bagley EJ, Tu KM, Buckhalt JA, El-Sheikh M. Community violence concerns and adolescent sleep. Sleep Health. 2016;2(1):57–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bailey BN, Delaney-Black V, Hannigan JH, Ager J, Sokol RJ, Covington CY. Somatic complaints in children and community violence exposure. J Dev Behav Pediatr. 2005;26(5):341–8. [DOI] [PubMed] [Google Scholar]
- 13.Belmon LS, Busch V, van Stralen MM, Stijnman DPM, Hidding LM, Harmsen IA, et al. Child and Parent Perceived Determinants of Children’s Inadequate Sleep Health. A Concept Mapping Study. Int J Environ Res Public Health. 2020;17(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Biggs SN, Lushington K, James Martin A, van den Heuvel C, Declan Kennedy J. Gender, socioeconomic, and ethnic differences in sleep patterns in school-aged children. Sleep Med. 2013;14(12):1304–9. [DOI] [PubMed] [Google Scholar]
- 15.Bose S, Ross KR, Rosa MJ, Chiu YM, Just A, Kloog I, et al. Prenatal particulate air pollution exposure and sleep disruption in preschoolers: Windows of susceptibility. Environ Int. 2019;124:329–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bottino CJ, Rifas-Shiman SL, Kleinman KP, Oken E, Redline S, Gold D, et al. The association of urbanicity with infant sleep duration. Health Place. 2012;18(5):1000–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Brouillette RT, Horwood L, Constantin E, Brown K, Ross NA. Childhood sleep apnea and neighborhood disadvantage. J Pediatr. 2011;158(5):789–95 e1. [DOI] [PubMed] [Google Scholar]
- 18.Chen DR, Truong KD, Tsai MJ. Prevalence of poor sleep quality and its relationship with body mass index among teenagers: evidence from Taiwan. J Sch Health. 2013;83(8):582–8. [DOI] [PubMed] [Google Scholar]
- 19.Cheon YM, Ip PS, Yip T. Adolescent profiles of ethnicity/race and socioeconomic status: Implications for sleep and the role of discrimination and ethnic/racial identity. Adv Child Dev Behav. 2019;57:195–233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cote-Lussier C, Knudby A, Barnett TA. A novel low-cost method for assessing intraurban variation in night time light and applications to public health. Social Science & Medicine. 2020;248. [DOI] [PubMed] [Google Scholar]
- 21.Dollman J, Matricciani L, Booth V, Blunden S. Secular trends in Australian school children’s sleep and perceived importance of sleep between 1985 and 2013. Acta Paediatr. 2017;106(8):1341–7. [DOI] [PubMed] [Google Scholar]
- 22.Dollman J, Ridley K, Olds T, Lowe E. Trends in the duration of school-day sleep among 10- to 15-year-old South Australians between 1985 and 2004. Acta Paediatr. 2007;96(7):1011–4. [DOI] [PubMed] [Google Scholar]
- 23.Dowdell EB, Santucci ME. The relationship between health risk behaviors and fear in one urban seventh grade class. J Pediatr Nurs. 2003;18(3):187–94. [DOI] [PubMed] [Google Scholar]
- *24.El-Sheikh M, Bagley EJ, Keiley M, Elmore-Staton L, Chen E, Buckhalt JA. Economic adversity and children’s sleep problems: multiple indicators and moderation of effects. Health Psychol. 2013;32(8):849–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Elder D, McDowall P, Sim D, Campbell A. Sleep in New Zealand children aged 7–9: associations with ethnicity, socioeconomic status, and achievement in reading and mathematics. J Clin Sleep Med. 2020;16(6):847–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Feng X, Flexeder C, Markevych I, Standl M, Heinrich J, Schikowski T, et al. Impact of Residential Green Space on Sleep Quality and Sufficiency in Children and Adolescents Residing in Australia and Germany. Int J Environ Res Public Health. 2020;17(13). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gaarde J, Hoyt LT, Ozer EJ, Maslowsky J, Deardorff J, Kyauk CK. So Much to Do Before I Sleep: Investigating Adolescent-Perceived Barriers and Facilitators to Sleep. Youth & Society. 2020;52(4):592–617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gill AI, Schaughency E, Galland BC. Prevalence and factors associated with snoring in 3-year olds: early links with behavioral adjustment. Sleep Med. 2012;13(9):1191–7. [DOI] [PubMed] [Google Scholar]
- 29.Graham C, Reither EN, Ciciurkaite G, Dev DA, Fargo J. Does context matter? A multilevel analysis of neighborhood disadvantage and children’s sleep health. Sleep Health. 2020;6(5):578–86. [DOI] [PubMed] [Google Scholar]
- 30.Grimes M, Camerota M, Propper CB. Neighborhood deprivation predicts infant sleep quality. Sleep Health. 2019;5(2):148–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ha EK, Park JH, Lee SJ, Yon DK, Kim JH, Jee HM, et al. Shared and unique individual risk factors and clinical biomarkers in children with allergic rhinitis and obstructive sleep apnea syndrome. Clinical Respiratory Journal. 2020;14(3):250–9. [DOI] [PubMed] [Google Scholar]
- 32.Hardy LL, Mihrshahi S, Bellew W, Bauman A, Ding D. Children’s adherence to health behavior recommendations associated with reducing risk of non-communicable disease. Prev Med Rep. 2017;8:279–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hawkins SS, Takeuchi DT. Social determinants of inadequate sleep in US children and adolescents. Public Health. 2016;138:119–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *34.Heissel JA, Sharkey PT, Torrats-Espinosa G, Grant K, Adam EK. Violence and Vigilance: The Acute Effects of Community Violent Crime on Sleep and Cortisol. Child Dev. 2018;89(4):e323–e31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Huss A, van Eijsden M, Guxens M, Beekhuizen J, van Strien R, Kromhout H, et al. Environmental Radiofrequency Electromagnetic Fields Exposure at Home, Mobile and Cordless Phone Use, and Sleep Problems in 7-Year-Old Children. PLoS One. 2015;10(10):e0139869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ievers-Landis CE, Storfer-Isser A, Rosen C, Johnson NL, Redline S. Relationship of sleep parameters, child psychological functioning, and parenting stress to obesity status among preadolescent children. J Dev Behav Pediatr. 2008;29(4):243–52. [DOI] [PubMed] [Google Scholar]
- 37.Jones CH, Ball H. Exploring Socioeconomic Differences in Bedtime Behaviours and Sleep Duration in English Preschool Children. Infant Child Dev. 2014;23(5):518–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kannan JA, Brokamp C, Bernstein DI, LeMasters GK, Hershey GKK, Villareal MS, et al. Parental Snoring and Environmental Pollutants, but Not Aeroallergen Sensitization, Are Associated with Childhood Snoring in a Birth Cohort. Pediatr Allergy Immunol Pulmonol. 2017;30(1):31–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kheirandish-Gozal L, Ghalebandi M, Salehi M, Salarifar MH, Gozal D. Neighbourhood air quality and snoring in school-aged children. Eur Respir J. 2014;43(3):824–32. [DOI] [PubMed] [Google Scholar]
- 40.Koinis-Mitchell D, Kopel SJ, Boergers J, McQuaid EL, Esteban CA, Seifer R, et al. Good Sleep Health in Urban Children With Asthma: A Risk and Resilience Approach. J Pediatr Psychol. 2015;40(9):888–903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lawrence WR, Yang M, Zhang C, Liu RQ, Lin S, Wang SQ, et al. Association between long-term exposure to air pollution and sleep disorder in Chinese children: the Seven Northeastern Cities study. Sleep. 2018;41(9). [DOI] [PubMed] [Google Scholar]
- 42.Lindsay AC, Moura Arruda CA, Tavares Machado MM, De Andrade GP, Greaney ML. Exploring Brazilian Immigrant Mothers’ Beliefs, Attitudes, and Practices Related to Their Preschool-Age Children’s Sleep and Bedtime Routines: A Qualitative Study Conducted in the United States. Int J Environ Res Public Health. 2018;15(9). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.MacKinnon AL, Tomfohr-Madsen L, Tough S. Neighborhood Socio-Economic Factors and Associations with Infant Sleep Health. Behav Sleep Med. 2020:1–13. [DOI] [PubMed] [Google Scholar]
- *44.Marco CA, Wolfson AR, Sparling M, Azuaje A. Family socioeconomic status and sleep patterns of young adolescents. Behav Sleep Med. 2011;10(1):70–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Martin SR, Boergers J, Kopel SJ, McQuaid EL, Seifer R, LeBourgeois M, et al. Sleep Hygiene and Sleep Outcomes in a Sample of Urban Children With and Without Asthma. J Pediatr Psychol. 2017;42(8):825–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Martin-Biggers J, Spaccarotella K, Hongu N, Alleman G, Worobey J, Byrd-Bredbenner C. Translating it into real life: a qualitative study of the cognitions, barriers and supports for key obesogenic behaviors of parents of preschoolers. BMC Public Health. 2015;15:189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Martinez SM, Thompson-Lastad A. Latino Parents’ Insight on Optimal Sleep for Their Preschool-Age Child: Does Context Matter? Acad Pediatr. 2015;15(6):636–43. [DOI] [PubMed] [Google Scholar]
- *48.McHale SM, Kim JY, Kan M, Updegraff KA. Sleep in Mexican-American adolescents: social ecological and well-being correlates. J Youth Adolesc. 2011;40(6):666–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *49.McLaughlin Crabtree V, Beal Korhonen J, Montgomery-Downs HE, Faye Jones V, O’Brien LM, Gozal D. Cultural influences on the bedtime behaviors of young children. Sleep Med. 2005;6(4):319–24. [DOI] [PubMed] [Google Scholar]
- 50.Meldrum RC, Jackson DB, Archer R, Ammons-Blanfort C. Perceived school safety, perceived neighborhood safety, and insufficient sleep among adolescents. Sleep Health. 2018;4(5):429–35. [DOI] [PubMed] [Google Scholar]
- *51.Moore M, Kirchner HL, Drotar D, Johnson N, Rosen C, Redline S. Correlates of adolescent sleep time and variability in sleep time: the role of individual and health related characteristics. Sleep Med. 2011;12(3):239–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *52.Ohrstrom E, Hadzibajramovic E, Holmes M, Svensson H. Effects of road traffic noise on sleep: Studies on children and adults. J Environ Psychol. 2006;26(2):116–26. [Google Scholar]
- 53.Olds T, Maher C, Blunden S, Matricciani L. Normative data on the sleep habits of Australian children and adolescents. Sleep. 2010;33(10):1381–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Orsey AD, Wakefield DB. Does socioeconomic status impact physical activity and sleep among children with cancer? Pediatr Blood Cancer. 2016;63(11):2004–10. [DOI] [PubMed] [Google Scholar]
- 55.Owens JA, Stahl J, Patton A, Reddy U, Crouch M. Sleep practices, attitudes, and beliefs in inner city middle school children: a mixed-methods study. Behav Sleep Med. 2006;4(2):114–34. [DOI] [PubMed] [Google Scholar]
- 56.Pabayo R, Molnar BE, Street N, Kawachi I. The relationship between social fragmentation and sleep among adolescents living in Boston, Massachusetts. J Public Health (Oxf). 2014;36(4):587–98. [DOI] [PubMed] [Google Scholar]
- 57.Paksarian D, Rudolph KE, Stapp EK, Dunster GP, He J, Mennitt D, et al. Association of Outdoor Artificial Light at Night With Mental Disorders and Sleep Patterns Among US Adolescents. JAMA Psychiatry. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Palimaru AI, Brown RA, Troxel WM, Dickerson DL, Johnson CL, D’Amico EJ. Understanding sleep facilitators, barriers, and cultural dimensions in Native American urban youth. Sleep Health. 2020;6(4):478–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Patrick KE, Millet G, Mindell JA. Sleep Differences by Race in Preschool Children: The Roles of Parenting Behaviors and Socioeconomic Status. Behav Sleep Med. 2016;14(5):467–79. [DOI] [PubMed] [Google Scholar]
- 60.Patte KA, Qian W, Leatherdale ST. Sleep duration trends and trajectories among youth in the COMPASS study. Sleep Health. 2017;3(5):309–16. [DOI] [PubMed] [Google Scholar]
- 61.Philbrook LE, Buckhalt JA, El-Sheikh M. Community violence concerns and adolescent sleep: Physiological regulation and race as moderators. J Sleep Res. 2019:e12897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Philbrook LE, El-Sheikh M. Associations between Neighborhood Context, Physical Activity, and Sleep in Adolescents. Sleep Health. 2016;2(3):205–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rubens SL, Fite PJ, Cooley JL, Canter KS. The Role of Sleep in the Relation between Community Violence Exposure and Delinquency among Latino Adolescents. Journal of Community Psychology. 2014;42(6):723–34. [Google Scholar]
- 64.Rubens SL, Gudino OG, Fite PJ, Grande JM. Individual and neighborhood stressors, sleep problems, and symptoms of anxiety and depression among Latino youth. Am J Orthopsychiatry. 2018;88(2):161–8. [DOI] [PubMed] [Google Scholar]
- 65.Rubens SL, Gudino OG, Ford LM, Soliemannjad RR, Contreras PD. Association between the sleep environment and sleep problems in low-income Latinx youth. Childrens Health Care. 2020. [Google Scholar]
- 66.Rubens SL, Patrick KE, Williamson AA, Moore M, Mindell JA. Individual and socio-demographic factors related to presenting problem and diagnostic impressions at a pediatric sleep clinic. Sleep Med. 2016;25:67–72. [DOI] [PubMed] [Google Scholar]
- 67.Rudolph KE, Shev A, Paksarian D, Merikangas KR, Mennitt DJ, James P, et al. Environmental noise and sleep and mental health outcomes in a nationally representative sample of urban US adolescents. Environ Epidemiol. 2019;3(4):e056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Sadler LS, Banasiak N, Canapari C, Crowley AA, Fenick A, OʼConnell M, et al. Perspectives on Sleep from Multiethnic Community Parents, Pediatric Providers, and Childcare Providers. J Dev Behav Pediatr. 2020;41(7):540–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Saelee R, Gazmararian JA, Haardörfer R, Suglia SF. Associations between the neighborhood social environment and obesity among adolescents: Do physical activity, screen time, and sleep play a role? Health Place. 2020;64:102380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Sánchez T, Gozal D, Smith DL, Foncea C, Betancur C, Brockmann PE. Association between air pollution and sleep disordered breathing in children. Pediatr Pulmonol. 2019;54(5):544–50. [DOI] [PubMed] [Google Scholar]
- 71.Sheehan C, Powers D, Margerison-Zilko C, McDevitt T, Cubbin C. Historical neighborhood poverty trajectories and child sleep. Sleep Health. 2018;4(2):127–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *72.Singh GK, Kenney MK. Rising Prevalence and Neighborhood, Social, and Behavioral Determinants of Sleep Problems in US Children and Adolescents, 2003–2012. Sleep Disord. 2013;2013:394320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Skrzypek M, Kowalska M, Czech EM, Niewiadomska E, Zejda JE. Impact of road traffic noise on sleep disturbances and attention disorders amongst school children living in Upper Silesian Industrial Zone, Poland. Int J Occup Med Environ Health. 2017;30(3):511–20. [DOI] [PubMed] [Google Scholar]
- 74.Spilsbury JC, Frame J, Magtanong R, Rork K. Sleep Environments of Children in an Urban U.S. Setting Exposed to Interpersonal Violence. Behav Sleep Med. 2016;14(6):585–601. [DOI] [PubMed] [Google Scholar]
- *75.Spilsbury JC, Storfer-Isser A, Kirchner HL, Nelson L, Rosen CL, Drotar D, et al. Neighborhood disadvantage as a risk factor for pediatric obstructive sleep apnea. J Pediatr. 2006;149(3):342–7. [DOI] [PubMed] [Google Scholar]
- 76.Spilsbury JC, Storfer-Isser A, Rosen CL, Redline S. Remission and incidence of obstructive sleep apnea from middle childhood to late adolescence. Sleep. 2015;38(1):23–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Stansfeld S, Hygge S, Clark C, Alfred T. Night time aircraft noise exposure and children’s cognitive performance. Noise Health. 2010;12(49):255–62. [DOI] [PubMed] [Google Scholar]
- 78.Street NW, McCormick MC, Austin SB, Slopen N, Habre R, Molnar BE. Examining family and neighborhood level predictors of sleep duration in urban youth. Fam Syst Health. 2018;36(4):439–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Tamanyan K, Walter LM, Davey MJ, Nixon GM, Horne RS, Biggs SN. Risk factors for obstructive sleep apnoea in Australian children. J Paediatr Child Health. 2016;52(5):512–7. [DOI] [PubMed] [Google Scholar]
- *80.Tiesler CM, Birk M, Thiering E, Kohlbock G, Koletzko S, Bauer CP, et al. Exposure to road traffic noise and children’s behavioural problems and sleep disturbance: results from the GINIplus and LISAplus studies. Environ Res. 2013;123:1–8. [DOI] [PubMed] [Google Scholar]
- 81.Troxel WM, Shih RA, Ewing B, Tucker JS, Nugroho A, D’Amico EJ. Examination of neighborhood disadvantage and sleep in a multi-ethnic cohort of adolescents. Health Place. 2017;45:39–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Uebergang LK, Arnup SJ, Hiscock H, Care E, Quach J. Sleep problems in the first year of elementary school: The role of sleep hygiene, gender and socioeconomic status. Sleep Health. 2017;3(3):142–7. [DOI] [PubMed] [Google Scholar]
- 83.Vollmer C, Michel U, Randler C. Outdoor light at night (LAN) is correlated with eveningness in adolescents. Chronobiol Int. 2012;29(4):502–8. [DOI] [PubMed] [Google Scholar]
- 84.Wamser-Nanney R, Chesher RE. Trauma characteristics and sleep impairment among trauma-exposed children. Child Abuse Negl. 2018;76:469–79. [DOI] [PubMed] [Google Scholar]
- 85.Wang R, Dong Y, Weng J, Kontos EZ, Chervin RD, Rosen CL, et al. Associations among Neighborhood, Race, and Sleep Apnea Severity in Children. A Six-City Analysis. Ann Am Thorac Soc. 2017;14(1):76–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Weyde KV, Krog NH, Oftedal B, Evandt J, Magnus P, Overland S, et al. Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems. Int J Environ Res Public Health. 2017;14(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Williamson AA, Milaniak I, Watson B, Cicalese O, Fiks AG, Power TJ, et al. Early Childhood Sleep Intervention in Urban Primary Care: Caregiver and Clinician Perspectives. J Pediatr Psychol. 2020;45(8):933–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Williamson AA, Mindell JA. Cumulative socio-demographic risk factors and sleep outcomes in early childhood. Sleep. 2020;43(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Williamson AA, Mindell JA, Hiscock H, Quach J. Sleep Problem Trajectories and Cumulative Socio-Ecological Risks: Birth to School-Age. J Pediatr. 2019;215:229–37.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Xie DX, Wang RY, Penn EB, Chinnadurai S, Shannon CN, Wootten CT. Understanding sociodemographic factors related to health outcomes in pediatric obstructive sleep apnea. Int J Pediatr Otorhinolaryngol. 2018;111:138–41. [DOI] [PubMed] [Google Scholar]
- 91.Zhang Z, Sousa-Sá E, Pereira J, Chaput JP, Okely A, Feng X, et al. Correlates of nocturnal sleep duration, nocturnal sleep variability, and nocturnal sleep problems in toddlers: results from the GET UP! Study. Sleep Med. 2019;53:124–32. [DOI] [PubMed] [Google Scholar]
- 92.Zhao J, Mackay L, Chang K, Mavoa S, Stewart T, Ikeda E, et al. Visualising Combined Time Use Patterns of Children’s Activities and Their Association with Weight Status and Neighbourhood Context. Int J Environ Res Public Health. 2019;16(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Johnson DA, Drake C, Joseph CL, Krajenta R, Hudgel DW, Cassidy-Bushrow AE. Influence of neighbourhood-level crowding on sleep-disordered breathing severity: mediation by body size. J Sleep Res. 2015;24(5):559–65. [DOI] [PubMed] [Google Scholar]
- 94.Ruff RR, Ng J, Jean-Louis G, Elbel B, Chaix B, Duncan DT. Neighborhood Stigma and Sleep: Findings from a Pilot Study of Low-Income Housing Residents in New York City. Behav Med. 2018;44(1):48–53. [DOI] [PubMed] [Google Scholar]
- 95.Mohnen SM, Völker B, Flap H, Groenewegen PP. Health-related behavior as a mechanism behind the relationship between neighborhood social capital and individual health--a multilevel analysis. BMC Public Health. 2012;12:116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Testa A The association between food deserts and short sleep duration among young adults in the United States: variation by race and ethnicity. Sleep Health. 2019;5(2):128–34. [DOI] [PubMed] [Google Scholar]
- 97.Weinberger B, Greiner LH, Walleigh L, Brown D. Health symptoms in residents living near shale gas activity: A retrospective record review from the Environmental Health Project. Prev Med Rep. 2017;8:112–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Logue JN, Fox JM. Residential health study of families living near the Drake Chemical Superfund site in Lock Haven, Pennsylvania. Arch Environ Health. 1986;41(4):222–8. [DOI] [PubMed] [Google Scholar]
- 99.Watson NF, Horn E, Duncan GE, Buchwald D, Vitiello MV, Turkheimer E. Sleep Duration and Area-Level Deprivation in Twins. Sleep. 2016;39(1):67–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Fuller-Rowell TE, Curtis DS, El-Sheikh M, Chae DH, Boylan JM, Ryff CD. Racial disparities in sleep: the role of neighborhood disadvantage. Sleep Med. 2016;27–28:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Johnson DA, Brown DL, Morgenstern LB, Meurer WJ, Lisabeth LD. The association of neighborhood characteristics with sleep duration and daytime sleepiness. Sleep Health. 2015;1(3):148–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Johnson DA, Lisabeth L, Hickson D, Johnson-Lawrence V, Samdarshi T, Taylor H, et al. The Social Patterning of Sleep in African Americans: Associations of Socioeconomic Position and Neighborhood Characteristics with Sleep in the Jackson Heart Study. Sleep. 2016;39(9):1749–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Newton AT, Honaker SM, Reid GJ. Risk and protective factors and processes for behavioral sleep problems among preschool and early school-aged children: A systematic review. Sleep Med Rev. 2020;52:101303. [DOI] [PubMed] [Google Scholar]
- 104.Carskadon MA, Vieira C Fau - Acebo C, Acebo C. Association between puberty and delayed phase preference. Sleep. 1993;16(3):258–62. [DOI] [PubMed] [Google Scholar]
- 105.Paksarian D, Rudolph KE, He JP, Merikangas KR. School Start Time and Adolescent Sleep Patterns: Results From the U.S. National Comorbidity Survey--Adolescent Supplement. Am J Public Health. 2015;105(7):1351–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Chaparro MP, Bilfield A, Theall KP. Exposure to Neighborhood Crime Is Associated with Lower Levels of Physical Activity and Higher Obesity Risk among Adolescent Girls, but Not Boys. Child Obes. 2019;15(2):87–92. [DOI] [PubMed] [Google Scholar]
- 107.Carson V, Janssen I. Neighborhood disorder and screen time among 10–16 year old Canadian youth: a cross-sectional study. Int J Behav Nutr Phys Act. 2012;9:66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Branas CC, South E, Kondo MC, Hohl BC, Bourgois P, Wiebe DJ, et al. Citywide cluster randomized trial to restore blighted vacant land and its effects on violence, crime, and fear. Proc Natl Acad Sci U S A. 2018;115(12):2946–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Wolfson AR, Carskadon MA, Acebo C, Seifer R, Fallone G, Labyak SE, et al. Evidence for the validity of a sleep habits survey for adolescents. Sleep. 2003;26(2):213–6. [DOI] [PubMed] [Google Scholar]
- 110.Short MA, Gradisar M, Gill J, Camfferman D. Identifying adolescent sleep problems. PLoS One. 2013;8(9):e75301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Basta LA, Richmond TS, Wiebe DJ. Neighborhoods, daily activities, and measuring health risks experienced in urban environments. Soc Sci Med. 2010;71(11):1943–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Hartling L, Featherstone R, Nuspl M, Shave K, Dryden DM, Vandermeer B. Grey literature in systematic reviews: a cross-sectional study of the contribution of non-English reports, unpublished studies and dissertations to the results of meta-analyses in child-relevant reviews. BMC Med Res Methodol. 2017;17(1):64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.