

Abstract
Background:
Brain abscess usually occurs secondary to trauma, through contiguous spread (e.g.; dental infections, [paranasal] sinusitis, otitis, and mastoiditis), after intracranial neurosurgical procedures, or through hematogenous spread in case of an arteriovenous (AV) shunt, for example; atrial septum defect. Although uncommon, another possible cause of AV shunt which can facilitate brain abscess is a pulmonary arteriovenous malformation (PAVM). We report a case of brain abscess secondary to a solitary PAVM and review the literature.
Case Description:
A 74-year-old male patient presented with headaches, fatigue, low-grade fever, and homonymous hemianopsia. He was diagnosed with a brain abscess in the left occipital lobe. A chest computed tomography (CT) with intravenous (IV) contrast was performed because of fever and respiratory insufficiency in a period where screening for COVID-19 in suspected patients was important. A solitary PAVM of the left lung was diagnosed. Initial stereotactic burr hole drainage of the abscess was insufficient and resection of the abscess was deemed necessary. Routine workup did not reveal any additional pathology apart from the PAVM. After treatment of the cerebral abscess, the PAVM was treated with embolization using an endovascular plug.
Conclusion:
It is recommended to screen for PAVM by chest CT with IV contrast in patients with brain abscess when no obvious source of infection can be identified.
Keywords: Brain abscess, Cryptogenic, Pulmonary arteriovenous malformation

INTRODUCTION
Brain abscess usually results from trauma, hematogenous spread through an atrial septal defect (ASD), contiguous spread from adjacent infections such as (paranasal) sinusitis or otitis media, or infections following intracranial neurosurgical procedures. In 20% of the cases, no source of infection can be identified and the abscess is deemed cryptogenic.[1] Alternative right-to-left shunts, other than an ASD, such as pulmonary arteriovenous malformation (PAVM), is a possible but uncommon etiology of brain abscess. They are low resistance, abnormal direct communications between pulmonary arteries and veins without interposition of a capillary bed, resulting in an intrapulmonary right-to-left shunt, predisposing to complications of paradoxical emboli presenting as transient ischemic attack, and ischemic stroke or brain abscess.[6,13] Overall, 30% of PAVM patients develop these neurological complications.[5] PAVM is not screened for in routine practice.[11] We describe a case of brain abscess due to a solitary PAVM which was an incidental finding. The aim of this report is to emphasize the additional value of routine computed tomography (CT) with intravenous (IV) contrast of the chest in patients with a cryptogenic brain abscess, even without any respiratory event.
CASE REPORT
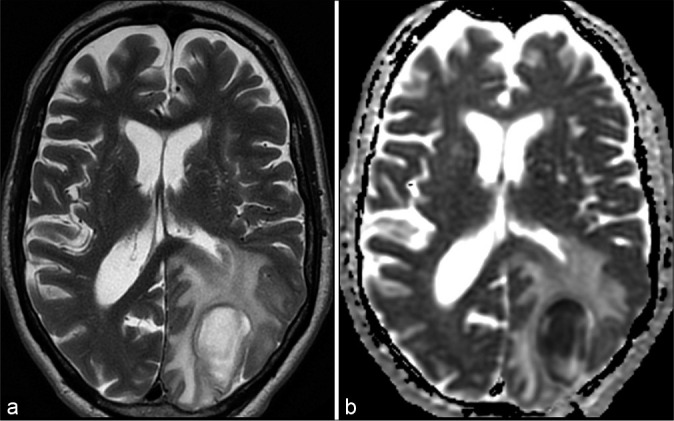
A 74-year-old male patient, without previous medical history, presented with headaches, fatigue, low-grade fever, disorientation, and difficulty conceiving distance. Neurological examination revealed a right-sided homonymous hemianopsia. During observation, body temperature fluctuated between 36.5 and 38°C. Oxygen saturation was 95%. Arterial blood samples showed a PaO2 of 67.9 mmHg, PaCO2 of 31.4 mmHg, and HCO3- of 22.1 mmol/L. Further, blood examination showed a slight raise in CRP (10.9 mg/L) but no leukocytosis. CT of the brain revealed a cystic lesion in the left occipital lobe with surrounding brain edema. Magnetic resonance imaging (MRI) confirmed this lesion, with central diffusion restriction suggestive for brain abscess [Figure 1].
Figure 1:

Magnetic resonance imaging shows typical brain abscess in the left occipital lobe. A T2 (a) hyperintense lesion with hypointense rim surrounded by vasogenic edema. Susceptibility-weighted images show a double rim sign (b), typical for brain abscess. Central diffusion restriction (ADC map – c). T1-weighted images (d and e) after gadolinium show rim enhancement.
A contrast-enhanced CT of the chest, to exclude COVID-19 pneumonia, showed a solitary PAVM of the inferior lobe of the left lung [Figure 2]. Routine workup for the source of the abscess showed no signs of endocarditis, (paranasal) sinusitis, mastoiditis, or dental problems. Although transesophageal echocardiography (TEE) could not visualize an ASD, there was an atrial right to left shunt suggestive of the presence of a pulmonary AV shunt.
Figure 2:
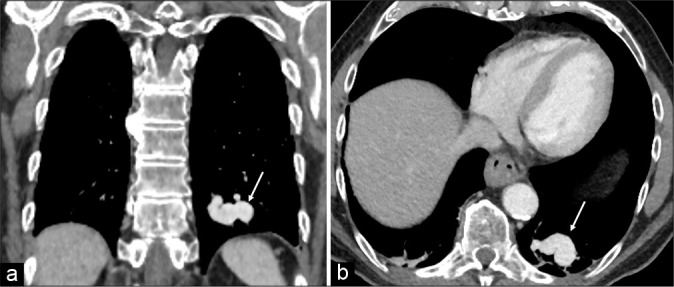
Coronal (a) and axial (b) chest computed tomography with intravenous contract shows large pulmonary arteriovenous malformation (arrow) in the left lower lobe.
Initial treatment consisted of stereotactic burr hole aspiration of 13 ml of purulent material and subsequent IV antibiotic therapy, consisting of ceftriaxone (2 g 2/d) and metronidazole (1.5 g 1/d). The antibiogram showed Streptococcus anginosus and Fusobacterium for which IV penicillin (4 million units 6/d) and metronidazole (1.5 g 1/d) were administered as definitive treatment. Despite a favorable biochemical evolution, the lesion progressively enlarged on MRI scan [Figure 3]. Therefore, a resection of the abscess was performed 17 days after initial presentation. The remaining postoperative period was uneventful. To prevent recurrence of the abscess, the PAVM was embolized using an endovascular plug [Figure 4]. After 4 weeks of IV therapy, another 2 weeks of oral antibiotic therapy were prescribed (Clamoxyl 1 g 3/d and metronidazole 500 mg 3/d) Although hemianopsia persisted, subsequent imaging and laboratory testing showed a positive evolution [Figure 5].
Figure 3:
Control magnetic resonance imaging shows residual abscess in the left occipital lobe after drainage with increased vasogenic edema on T2 (a) and persisted diffusion restriction (ADC map – image b).
Figure 4:

Digital subtraction angiography. Pulmonary arteriovenous malformation in the left lower lobe (a) (*) and confirmation (b) of complete closure of the feeding vessel after embolization with plug (arrow).
Figure 5:

Follow-up magnetic resonance imaging (5 months postoperatively) shows normal postoperative brain tissue loss and gliosis on T2-weighted image (a) in the left occipital lobe after abscess resection. On T1 (b) after gadolinium, there is no pathologic enhancement. There are no signs of diffusion restriction (ADC map – c).
LITERATURE REVIEW AND DISCUSSION
Brain abscess is a focal infection of the brain that can be caused by several microorganisms including bacteria, mycobacteria, protozoa, helminths, and fungi. Although present only in 20% of cases, the classic triad of symptoms includes headache, fever, and focal neurological deficits.[4] Most patients, however, present with nonspecific symptoms. The diagnosis must be considered in all patients with new-onset progressive headache, signs of increased intracranial pressure, and focal neurologic deficits.[14]
Cranial imaging is crucial in the diagnosis of brain abscess and consists of CT scan with IV contrast enhancement and MRI with diffusion-weighted images to differentiate brain abscess from cystic or necrotic tumors.[4]
Brain abscess is often attributed to predisposing factors, such as disruption of the natural protective surrounding barriers (e.g.; neurosurgical procedure and trauma), an underlying disease, causing immunodeficiency, or a systemic source of infection. Bacteria can enter the brain through contiguous spread from infections of the middle or inner ear and sinuses or hematogenous spread from endocarditis, lung infections, or dental infections.[3]
When the diagnosis of brain abscess is made, a routine workup should be performed to find the source of infection. This includes echocardiography to rule out atrial septal defects, endocarditis, chest X-ray to identify lung infections, and evaluation of the teeth, ear, nose, and throat. [4] Transthoracic echocardiography (TTE) is recommended as initial screening for cardiac abnormalities. If TTE is normal, equivocal or if no other cause had been identified, TEE should be performed since its sensitivity is higher.[15] In 20% of cases, no source will be identified despite all available investigations.[1] Screening for PAVM can be useful in these cases.
PAVM has an estimated prevalence of 1 in 2600 people.[2] About 80–90% of patients with PAVM have underlying hereditary hemorrhagic telangiectasia (HHT) or Rendu-Osler-Weber disease.[13] Our patient, however, had no clinical signs of HHT. Brain abscess affects between 7.8% and 9% of patients with PAVM.
In patients with cryptogenic brain abscess, we should look for clinical symptoms and signs of PAVM. Although often asymptomatic (66%), common symptoms are dyspnea, orthodeoxia, exercise intolerance, palpitations, and chest pain.[1,9] If the thin-walled PAVM ruptures, patients can present with hemoptysis or hemothorax.[19] Systolic murmur, clubbing, cyanosis, low arterial pO2 levels, as in our patient, and polycythemia are clinical signs indicative of PAVM.
Imaging is required for the diagnosis of PAVM. On chest radiographs, PAVM appears as a well-defined round or oval sharply defined nodule or mass. Chest radiographs are normal in 10–40% of cases, however, making routine screening insensitive.[6,7] Transthoracic contrast echocardiography (TTCE) or bubble echocardiography is a rapid, simple, and minimally invasive examination which can be used as initial screening for PAVM, as it has a sensitivity of 93–100%.[12,13] TTCE examines the presence of a pulmonary right-to-left shunt but it does not directly visualize the PAVM. Chest CT with IV contrast is advised for further evaluation of the size and location of the PAVM and is thus considered the gold standard diagnostic tool for PAVM. Pulmonary angiography is no longer a diagnostic tool and is reserved for therapeutic purposes.[6,12,13]
Optimal treatment of brain abscess includes both medical and surgical therapy. All patients should receive prompt empiric antibiotics such as ceftriaxone and metronidazole. The reason for choosing these drugs is their ability to penetrate in the abscess, and they cover both Gram-positive and -negative bacteria.[8] Stereotactic burr hole aspiration has become the intervention of choice. Drainage of the purulent material is necessary for resolution of the abscess, and antibiotic susceptibility patterns can be determined. Complete surgical resection may be considered in particular circumstances. In our case, resection was performed because of progression of the lesion after initial burr hole aspiration. Corticosteroids are not routinely used and are reserved for cases with severe edema that has led to significant clinical mass effect.[14] In addition, the infectious focus must be removed through tooth extraction, cardiac valve replacement, or sinus surgery to prevent further spread of bacteria.[4] When PAVM is present, this should be treated to prevent recurrence of brain abscess and paradoxical brain embolism.[11]
The current preferred treatment for PAVM is embolization, which is safe and effective in experienced hands. It is less invasive than surgical methods and repeatable.[6,11] After successful embolization, feeding arteries occlude and the PAVM does no longer recruit vascular supply. Collateralization and revascularization overtime may occur, making lifelong follow-up important. Dental hygiene and antibiotic prophylaxis before dental or surgical procedures are recommended in all patients with residual right-to-left shunts. Surgical parenchymal resection is indicated in cases with centrally located or large PAVMs or high risk of embolization failure.[2,10,18]
Although prognosis of brain abscess has improved with an all-cause mortality of 5–32%, many patients are unable to return to their former activities due to persistent neurological deficits.[14,17] Screening for the presence of PAVM in patients with cryptogenic brain abscess is valuable to establish the diagnosis and treat the malformation since occlusion of PAVM prevents recurrence of brain abscess. Screening is best performed using contrast-enhanced CT scan of the chest. The main disadvantage of screening includes radiation exposure.[16]
CONCLUSION
This case demonstrates the possibility of PAVM as a cause of brain abscess. Especially in cases of cryptogenic brain abscess, it is important to screen for PAVM. Treatment of PAVM can prevent recurrence of brain abscess. We recommend contrast-enhanced chest CT scan in all patients with cryptogenic brain abscess, particularly with evidence of right to left shunting on clinical examination or contrast echocardiography.
Footnotes
How to cite this article: Rens J, Van Thielen T, Derweduwen A, Goedseels K, Hes R, de Jong L. Screening in cryptogenic brain abscess: Do not forget pulmonary arteriovenous malformations. Surg Neurol Int 2021;12:188.
Contributor Information
Jasmien Rens, Email: jasmien.rens@student.uantwerpen.be.
Thomas Van Thielen, Email: thomas.vanthielen@klina.be.
Aurelie Derweduwen, Email: aurelie.derweduwen@klina.be.
Koen Goedseels, Email: koen.goedseels@klina.be.
Robert Hes, Email: robert.hes@klina.be.
Lars de Jong, Email: ldjone@hotmail.com.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Arivazhagan A, Pandey P, Anandh B, Abraham RG, Indira DB, Sampath S, et al. An unusual etiology of recurrent cerebral abscesses-a report of 3 cases. Surg Neurol. 2009;71:241–4. doi: 10.1016/j.surneu.2007.07.044. discussion 245. [DOI] [PubMed] [Google Scholar]
- 2.Boother EJ, Brownlow S, Tighe HC, Bamford KB, Jackson JE, Shovlin CL. Cerebral abscess associated with odontogenic bacteremias, hypoxemia, and iron loading in immunocompetent patients with right-to-left shunting through pulmonary arteriovenous malformations. Clin Infect Dis. 2017;65:595–603. doi: 10.1093/cid/cix373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brouwer MC, Tunkel AR, McKhann GM, 2nd, van de Beek D. Brain abscess. N Engl J Med. 2014;371:447–56. doi: 10.1056/NEJMra1301635. [DOI] [PubMed] [Google Scholar]
- 4.Brouwer MC, van de Beek D. Epidemiology, diagnosis, and treatment of brain abscesses. Curr Opin Infect Dis. 2017;30:129–34. doi: 10.1097/QCO.0000000000000334. [DOI] [PubMed] [Google Scholar]
- 5.Cappa R, Du J, Carrera JF, Berthaud JV, Southerland AM. Ischemic stroke secondary to paradoxical embolism through a pulmonary arteriovenous malformation: Case report and review of the literature. J Stroke Cerebrovasc Dis. 2018;27:e125–e127. doi: 10.1016/j.jstrokecerebrovasdis.2018.02.015. [DOI] [PubMed] [Google Scholar]
- 6.Cartin-Ceba R, Swanson KL, Krowka MJ. Pulmonary arteriovenous malformations. Chest. 2013;144:1033–44. doi: 10.1378/chest.12-0924. [DOI] [PubMed] [Google Scholar]
- 7.Cox M, Patel M, Deshmukh S, Roth CG, Flanders AE. Contrast-enhanced chest computed tomography reveals treatable causes of cerebral abscesses in patients without antecedent surgery or trauma. World Neurosurg. 2017;101:144–8. doi: 10.1016/j.wneu.2017.01.068. [DOI] [PubMed] [Google Scholar]
- 8.Dong SL, Reynolds SF, Steiner IP. Brain abscess in patients with hereditary hemorrhagic telangiectasia: Case report and literature review. J Emerg Med. 2001;20:247–51. doi: 10.1016/s0736-4679(00)00315-2. [DOI] [PubMed] [Google Scholar]
- 9.Holzer RJ, Cua CL. Pulmonary arteriovenous malformations and risk of stroke. Cardiol Clin. 2016;34:241–6. doi: 10.1016/j.ccl.2016.01.001. [DOI] [PubMed] [Google Scholar]
- 10.Ibrahim I, Rabiou S, Laila B, Zahra AF, Jamal G, Marouane L, et al. Cerebral abscesses revealing pulmonary arteriovenous malformations. Chin Med J (Engl) 2016;129:2253–5. doi: 10.4103/0366-6999.189905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kaido T, Moriyama Y, Ueda K, Higashiura W, Sakaguchi H, Kichikawa K. Recurrent brain abscess induced by pulmonary arteriovenous fistula. J Infect Chemother. 2011;17:552–4. doi: 10.1007/s10156-011-0210-9. [DOI] [PubMed] [Google Scholar]
- 12.Kroon S, Snijder RJ, Faughnan ME, Mager HJ. Systematic screening in hereditary hemorrhagic telangiectasia: A review. Curr Opin Pulm Med. 2018;24:260–8. doi: 10.1097/MCP.0000000000000472. [DOI] [PubMed] [Google Scholar]
- 13.Lacombe P, Lacout A, Marcy PY, Binsse S, Sellier J, Bensalah M, et al. Diagnosis and treatment of pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: An overview. Diagn Interv Imaging. 2013;94:835–48. doi: 10.1016/j.diii.2013.03.014. [DOI] [PubMed] [Google Scholar]
- 14.Patel K, Clifford DB. Bacterial brain abscess. Neurohospitalist. 2014;4:196–204. doi: 10.1177/1941874414540684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pearson AC. Transthoracic echocardiography versus transesophageal echocardiography in detecting cardiac sources of embolism. Echocardiography. 1993;10:397–403. doi: 10.1111/j.1540-8175.1993.tb00051.x. [DOI] [PubMed] [Google Scholar]
- 16.Shovlin CL, Condliffe R, Donaldson JW, Kiely DG, Wort SJ, British Thoracic Society British thoracic society clinical statement on pulmonary arteriovenous malformations. Thorax. 2017;72:1154–63. doi: 10.1136/thoraxjnl-2017-210764. [DOI] [PubMed] [Google Scholar]
- 17.Shovlin CL, Jackson JE, Bamford KB, Jenkins IH, Benjamin AR, Ramadan H, et al. Primary determinants of ischaemic stroke/ brain abscess risks are independent of severity of pulmonary arteriovenous malformations in hereditary haemorrhagic telangiectasia. Thorax. 2008;63:259–66. doi: 10.1136/thx.2007.087452. [DOI] [PubMed] [Google Scholar]
- 18.Shovlin CL. Pulmonary arteriovenous malformations. Am J Respir Crit Care Med. 2014;190:1217–28. doi: 10.1164/rccm.201407-1254CI. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tabakow P, Jarmundowicz W, Czapiga B, Czapiga E. Brain abscess as the first clinical manifestation of multiple pulmonary arteriovenous malformations in a patient with hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber disease) Folia Neuropathol. 2005;43:41–4. [PubMed] [Google Scholar]