

Abstract
Background:
The spine surgery complexity score (SSCS), previously reported by us, is a simple grading system to predict postoperative complications and hospital length of stay (LOS). This scale is based on the technical difficulty of the spinal procedures being performed.
Methods:
We performed a retrospective chart review to validate SSCS in 671 consecutive patients undergoing spine procedures at a quaternary academic hospital.
Results:
The SSCS was predictive of the hospital LOS and postoperative complications (defined by the ClavienDindo score), based on linear regression analysis (P < 0.001 for both).
Conclusion:
Categorizing procedures according to the SSCS may enable neurosurgeons to assess surgical risk and predict longer LOS courses after spine surgery. Thus, it may prove useful in preoperative patient evaluation/ education and determining a prognosis based on surgical complexity.
Keywords: Hospital length of stay, Outcomes, Postoperative complications, Spine surgery, Surgical complexity scale

INTRODUCTION
Characterizing procedural complexity related to postsurgical outcomes can aid neurosurgeons in patient selection, preoperative counseling, and determining the prognosis.[5] It also helps establish risk models along with surgical outcomes assessment.
Here, we attempt to validate the spine surgery complexity score (SSCS), recently proposed by us,[3] to predict hospital length of stay (LOS) and postoperative complications (i.e., as described by the Clavien-Dindo score [CDS]).[6]
MATERIALS AND METHODS
Data collection
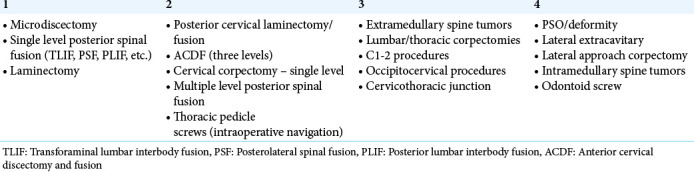
The patients undergoing spine surgery were identified from operating room logs of the Department of Neurosurgery, Westchester Medical Center, 2015–2017. A 4-level subjective complexity scale (SSCS) was devised based on what year of residency trainees typically learn each procedure [Table 1].[3] Patients undergoing spinal procedures were selected, and each was assigned a score from 1 to 4 based on the predefined SSCS categories. Subsequently, the following factors were assessed: hospital LOS and complications (i.e., as defined by CDS – spell out).
Table 1:
Spine surgery complexity score.
Statistical analysis
Spearman’s correlation and univariate linear regression analysis were performed for comparing continuous variables and Likert scale scores. Significance was set at a cutoff of P < 0.05. All statistical analyses were performed using SPSS 24 software (IBM Corp., Armonk, NY).
RESULTS
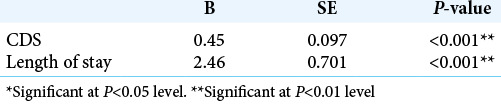
A total of 671 patients were included in this study with average age of 50 ± 17.15 years. Of these patients, 53.6% were men and 46.4% were women. The median SSCS was 2 (IQR:1); the average LOS was 7.14 ± 10.4 days; and the median CDS was 0 (IQR:2) [Figure 1]. The SSCS significantly correlated with both LOS and CDS [Table 2] and was predictive of LOS and CDS in linear regression analysis [Table 3].
Figure 1:

Frequency of cases by the spine surgery complexity score.
Table 2:
Spearman correlation of primary endpoints.
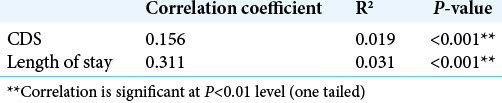
Table 3:
Univariate linear regression of primary endpoints.
DISCUSSION
Agreed-upon scales for both complexity and surgical outcomes are increasingly required for standardized evaluation of procedures, LOS, and outcomes in neurological surgery.[4,5] In 2008, multiple neurosurgical organizations created the NeuroPoint Alliance (NPA) to create a national database for neurosurgical outcomes and to centralize outcome reporting.[1] Although the NPA’s prospective clinical registry, the National Neurosurgery Quality and Outcomes Database (N2QOD), has led to studies assessing validity of lumbar spine surgery, a broadly applicable spine procedure complexity scale has not yet been devised.[2,7-9] The SSCS, validated in this study, is a product of consensus expert opinion based on surgical experience. Compared to other neurosurgical outcome scales, the SSCS offers a middle ground of objectivity, being based both on expert opinion and statistical models. Unique to the SSCS is its basis in resident training timelines. As more complexity scales emerge in this, and other fields, they can also be used to guide and evaluate resident training.
Emphasizing postsurgical complications rather than patient functional impairment, the SSCS is also the only neurosurgical scale to use CDS as an endpoint, instead of, for example, change in Glasgow Coma Score (GCS). The most appropriate outcome measure may vary by subspecialty within neurosurgery. For example, a spine complexity scale that measures change in GCS may not yield important information about the difficulty of the preceding procedure. The most appropriate outcome measure may vary by subspecialty within neurosurgery. Current efforts by the N2QOD spine division are focused on preventing readmission after spine surgery and comparing effectiveness of different approaches to surgical treatment of spondylolisthesis using patient-reported outcome data. They also evaluate the endpoints of blood loss and LOS as reflections of surgical efficiency. Ultimately, future work should include evaluation of multiple endpoints to offer comprehensive analysis of surgical risk and operative complexity. Finally, as national patient databases become increasingly available, statistically derived complexity scales should be devised and compared to existing ones.
CONCLUSION
Stratifying procedures using the SSCS may enable neurosurgeons to assess surgical risk and predict hospital courses and outcomes for patients after spine surgery.
Footnotes
How to cite this article: Azizkhanian I, Alcantara R, Ballinger Z, Cho E, Dore S, Gatzofilas S, et al. Spine surgery complexity score predicts outcomes in 671 consecutive spine surgery patients. Surg Neurol Int 2021;12:206.
Contributor Information
Ida Azizkhanian, Email: iazizkha@nymc.edu.
Ryan Alcantara, Email: ralcanta2@nymc.edu.
Zachary Ballinger, Email: zballing@nymc.edu.
Edward Cho, Email: echo4@nymc.edu.
Silvi Dore, Email: sdore@nymc.edu.
Stergios Gatzofilas, Email: sgatzofl@nymc.edu.
Raeesa Habiba Hossain, Email: rhossain2@nymc.edu.
Jesse Honig, Email: jhonig@nymc.edu.
Nicole Matluck, Email: nmatluck@nymc.edu.
Jonathan V. Ogulnick, Email: jogulnic@student.nymc.edu.
Michael Rothbaum, Email: mrothbau2@nymc.edu.
Iliya Rybkin, Email: ilrybkin@gmail.com.
Harrison Smith, Email: hsmith6@nymc.edu.
Brian Tung, Email: btung@nymc.edu.
Syed Faraz Kazim, Email: skazim@salud.unm.edu.
Ivan Miller, Email: ivan.miller@wmchealth.org.
Meic H. Schmidt, Email: mhschmidt@salud.unm.edu.
Chad D. Cole, Email: cdcole@salud.unm.edu.
Christian A. Bowers, Email: cabowers@salud.unm.edu.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Asher AL, McCormick PC, Selden NR, Ghogawala Z, McGirt MJ. The national neurosurgery quality and outcomes database and neuropoint alliance: Rationale, development, and implementation. Neurosurg Focus. 2013;34:E2. doi: 10.3171/2012.10.FOCUS12311. [DOI] [PubMed] [Google Scholar]
- 2.Asher AL, Speroff T, Dittus RS, Parker SL, Davies JM, Selden N, et al. The national neurosurgery quality and outcomes database (N2QOD): A collaborative north American outcomes registry to advance value-based spine care. Spine (Phila Pa 1976) 2014;39(22) Suppl 1:S106–16. doi: 10.1097/BRS.0000000000000579. [DOI] [PubMed] [Google Scholar]
- 3.Azizkhanian I, Rothbaum M, Alcantara R, Ballinger Z, Cho E, Dore S, et al. Demographics and outcomes of interhospital neurosurgical transfer patients undergoing spine surgery. World Neurosurg. 2020;144:e221–6. doi: 10.1016/j.wneu.2020.08.080. [DOI] [PubMed] [Google Scholar]
- 4.Broggi M, Zattra C, Ferroli P. How to compare outcomes and complications in neurosurgery: We must make the mission possible! Surg Neurol Int. 2018;9:65. doi: 10.4103/sni.sni_424_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dindo D, Clavien PA. Quality assessment in surgery: Mission impossible? Patient Saf Surg. 2010;4:18. doi: 10.1186/1754-9493-4-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13. doi: 10.1097/01.sla.0000133083.54934.ae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McGirt MJ, Speroff T, Dittus RS, Harrell FE, Jr, Asher AL. The national neurosurgery quality and outcomes database (N2QOD): General overview and pilot-year project description. Neurosurg Focus. 2013;34:E6. doi: 10.3171/2012.10.FOCUS12297. [DOI] [PubMed] [Google Scholar]
- 8.Than KD, Curran JN, Resnick DK, Shaffrey CI, Ghogawala Z, Mummaneni PV. How to predict return to work after lumbar discectomy: Answers from the neuropoint-SD registry. J Neurosurg Spine. 2016;25:181–6. doi: 10.3171/2015.10.SPINE15455. [DOI] [PubMed] [Google Scholar]
- 9.Whitmore RG, Curran JN, Ali ZS, Mummaneni PV, Shaffrey CI, Heary RF, et al. Predictive value of 3-month lumbar discectomy outcomes in the neuropoint-SD registry. J Neurosurg Spine. 2015;23:459–66. doi: 10.3171/2015.1.SPINE14890. [DOI] [PubMed] [Google Scholar]