

Abstract
Despite demonstrated efficacy for HIV prevention, substantial challenges remain for successful rollout of oral pre-exposure prophylaxis (PrEP), especially among adolescent girls and young women (AGYW). We characterized trajectories of PrEP adherence among 200 AGYW in South Africa and analyzed data from 22 qualitative interviews and 3 focus group discussions for explanatory purposes. Two adherence trajectory groups were identified: 52% with high early adherence that decreased after month three and 48% with low adherence throughout. Adherence in the consistently low group was related to social support and logistical concerns, while the decrease in the high declining group corresponded to a change in the frequency of study visits from monthly to quarterly. PrEP support should be differentiated for those who need more frequent visits and adherence support initially versus later in PrEP use. Visits every month when needed should be considered for AGYW who need sustained support later into use.
Keywords: Adolescent girls and young women, Pre-exposure prophylaxis, HIV prevention, Trajectory analysis, Adherence
Introduction:
Adolescent girls and young women (AGYW) ages 15–24 years have a high incidence of HIV infection which is up to six times higher than their male counterparts.1 Oral antiretroviral pre-exposure prophylaxis (PrEP) is over 90% effective at preventing HIV in women and men2,3 and is a promising prevention strategy for AGYW at high risk of HIV acquisition. However, low adherence and persistence has undermined the effective use of PrEP to prevent HIV particularly among AGYW.4–7
PrEP demonstration projects across southern and East Africa show substantial declines in daily oral PrEP persistence among AGYW over time. In the POWER study in Kenya and South Africa, only 51% of AGYW were still taking PrEP one month after initiation despite high initial uptake (90%), decreasing to just 25% at month three.8 In the HPTN 082 study in South Africa, 25% of enrolled AGYW had high adherence at month three, decreasing significantly through the remainder of the study when the frequency of prescribed visits changed from monthly to quarterly.9 The 3Ps (Perception, Partners, Pills) for Prevention study, from which this analysis originates, was an open label PrEP demonstration project in South Africa that also demonstrated high initial uptake with rapid declines in persistence and adherence observed shortly after initiation.10,11 The study found that early on, PrEP adherence was high (80% had medium/high adherence at 2–3 months) but declined rapidly over time.
Given the substantial declines and overall low adherence observed in 3P, we aimed to further understand patterns of declining PrEP adherence in this prospective longitudinal cohort. A better understanding of when and why declines in adherence occur could inform the development of adherence support interventions that are implemented at critical times during PrEP use. Here, we use group-based trajectory modelling to characterize trajectories of adherence among AGYW enrolled in 3P over one-year. We then use additional quantitative and qualitative data to contextualize these trajectories and assess how intervention approaches might differ for these groups.
Methods:
Study Setting, Population, and Procedures
A total of 200 young women were enrolled in 3P between March 2017 and March 2018 who were between the ages 16–25, HIV-negative (blood test) and living in a Cape Town township in South Africa.11 Additional inclusion criteria included vaginal or anal sex in the month prior to screening or planning to be sexually active in the next three months, willingness to take PrEP, not pregnant, and normal renal function (creatinine clearance >60 ml/min). Young women were followed for a year with study visits at months 1, 2, 3, 6, 9 and 12. Dried blood spots (DBS) were obtained at each visit to measure intracellular tenofovir diphosphate (TFV-DP) levels as a measure of PrEP adherence. All participants received adherence counseling at each study visit and retrospective feedback about their adherence based on drug levels obtained at months 1, 2, and 3. All young women received 100 ZAR per study visit. Half were randomized to an incentive arm where they received an additional 200 ZAR shopping voucher at months 2, 3 and 4 upon demonstration of high adherence (>500 fmol/punch at Month 1 and >700 fmol/punch at Months 2 and 3).11,12 AGYW completed a questionnaire at each visit with questions about demographics, sexual behaviors, PrEP disclosure, alcohol use and HIV risk. Study retention across visits was 73–89%.11 Additional study details, including all recruitment and enrollment procedures, are available in the main study paper.11
In addition to the quantitative surveys, serial qualitative in-depth interviews (IDI) were administered over the study period to better understand AGYW experiences using PrEP. Participants were purposively selected at enrollment (stratified by incentive arm and age) and were interviewed at months 1, 3, and 12 (N=22). Early interviews explored interest, motivation, and initial experiences using PrEP, while later interviews explored patterns of adherence, reasons for stopping/persisting on PrEP, social experiences, and participants’ reflections on their overall journey. Interviews were audio-recorded, transcribed and translated, and underwent quality control by the team in South Africa and the United States. In addition, three focus groups discussions (FGDs) were conducted at the end of the study; two were conducted with participants who stopped PrEP before the end of follow-up (N=7) and one (N=5) with those who remained on PrEP for the entire study and expressed interest in using PrEP in the future (persisters).
Quantitative Analysis:
The outcome of PrEP adherence in our analysis was defined using continuous levels of TFV-DP from DBS.11 We coded the young women who missed a visit or did not obtain a refill as having a 0 value for adherence. In a sensitivity analyses, we coded missed visits as 0.5 to account for leftover drug from the prior month and, in another analysis, did not recode missed values. All approaches resulted in the identification of the same two trajectory groups. Therefore, we decided to code the young women who missed a visit or did not get a refill as having a 0 value for adherence, increasing the likelihood of model convergence. We used continuous rather than dichotomous adherence throughout the analysis to leverage all data available and because the two trajectory groups that emerged were similar when defining adherence both ways.
Baseline characteristics that were examined in relation to trajectory group membership included age, sexual behaviors and relationship characteristics (number of partners, intimate partner violence (IPV; yes/no), transactional sex (yes/no), any alcohol use (yes/no), HIV testing (yes/no), and partner HIV status (negative/positive/unknown), incentive randomization arm, worry a lot about HIV (a lot versus no/some worry) and disclosure of PrEP use to anyone (yes/no) and to a sex partner (yes/no). Variable definitions were consistent with those used in prior analyses of these data.11
We used group-based trajectory modelling to identify trajectories of PrEP adherence over one year.13–15 Group-based trajectory modelling is a data driven approach whereby the study data are used to identify latent groups of individuals whose outcomes of interest follow a similar pattern over time. We first fit a series of unconditional trajectory models for PrEP adherence to identify the most appropriate number of trajectory groups.15 Model fit was determined using seven criteria13,15: (1) How groups corresponded with substantive literature about trends in adherence; (2) average posterior class probabilities of class membership; (3) Akaike Information Criteria (AIC; smaller values indicating better fit); (4) Bayesian Information Criteria (BIC; smaller values indicating better fit); (5) entropy (use class probabilities for each variable and values closer to one indicate accurate classifications); (6) percentage and size of smallest trajectory group; and (7) the log-likelihood of each model. After the optimal number of trajectories was selected, we then considered constant, linear, quadratic, and cubic specifications for the shape of each trajectory group, selecting a final model through visual inspection of the data and using fit statistics described above.
Next, we assigned each young woman to an adherence group using a maximum probability assignment rule and calculated descriptive statistics to examine relationships between individual and partner characteristics at enrollment and trajectory group membership.16 We used relative frequencies for categorical variables and medians with the interquartile range (IQR) for continuous measures. Analyses were done using Stata version 16.17
Qualitative Analysis:
Qualitative data was analyzed to further explain findings from the quantitative trajectory analysis. Transcripts were coded in Dedoose (version 8.2.18, Los Angeles, CA). All 22 participants who joined the qualitative interview cohort were analyzed in concordance with their assigned trajectory group. For both the consistently low and high declining trajectory groups, we reviewed each participant’s “PrEP journey” using a case analysis approach.18 To explore additional barriers to adherence, we also examined the following codes (alone and in combination) from the IDI and FGD transcripts: “3P”, “adherence”, “discontinuation,” “counseling,” “PrEP Journey,” and/or “persistence.” We focused on three key areas for further explanation: 1) In the consistently low adherence group, we examined barriers to ever achieving high adherence; 2) In the high declining adherence group, we examined reasons for declines in adherence later in the study; and 3) Reasons for high adherence for those in the high declining group that persisted throughout the study.
Results:
A total of 200 AGYW in Cape Town, South Africa were included in the analysis cohort to examine trajectories of PrEP adherence over one year. The median age at baseline was 19 (range 16–25), approximately half reported being worried a lot about HIV (N=110, 55%), 86% had a sex partner (N=172), 91% disclosed their PrEP plan to someone (N=182) and 19% had ever experienced IPV (N=37) (Table 1). Most participants had only one partner in the last 3 months (N=161, 81%), and about a third had previously tested for HIV (N=60, 33%). Roughly 50% had high adherence at month 3 and less than 10% had high adherence at month 12. Persistence over the study period was high with 44% still refilling a PrEP prescription through month 12 and another 20% restarting PrEP after discontinuation.
Table 1:
Characteristics at Enrollment or Screening by Adherence Trajectory Group Membership
| Adherence Trajectory Group | |||||||
|---|---|---|---|---|---|---|---|
| Group 1- Low (N=94, 49%)) | Group 2- High declining (N=106, 52%) | Total | P- value | ||||
| N (%) | Median (range) | N (%) | Median (IQR) | N (%) | Median (range) | ||
| Age | 19 (16–25) | 19 (17–21) | 19 (16–25) | ||||
| Worry a lot about HIV | 52 (55.9) | 58 (54.7) | 110 (55.3) | 0.559 | |||
| Incentive Randomization Arm | 42 (44.7) | 59 (55.7) | 101 (50.5) | 0.121 | |||
| Transactional sex | 2 (2.1) | 3 (2.8) | 5 (2.5) | 0.751 | |||
| Any alcohol use | 19 (20.2) | 23 (21.7) | 42 (21.0) | 0.797 | |||
| Has a sexual partner | 80 (85.1) | 92 (86.8) | 172 (86.0) | 0.732 | |||
| Disclosed PrEP plan | 81 (86.2) | 101 (95.3) | 182 (91.0) | 0.025 | |||
| Disclosed PrEP use to partner | 52 (55.3) | 51 (48.1) | 103 (51.5) | 0.309 | |||
| Sex partner has other partners | |||||||
| No | 32 (34.0) | 26 (24.5) | 58 (29.0) | 0.072 | |||
| Yes | 10 (10.6) | 23 (21.7) | 33 (16.5) | ||||
| Don’t know | 52 (55.3) | 57 (53.8) | 109 (54.5) | ||||
| Any IPV | 21 (22.3) | 16 (15.1) | 37 (18.5) | 0.188 | |||
| Sex Partners in last 3 month | |||||||
| 0 | 12 (12.8) | 15 (14.1) | 27 (13.5) | 0.943 | |||
| 1 | 76 (80.9) | 85 (80.2) | 161 (80.5) | ||||
| >1 | 6 (6.4) | 6 (5.7) | 12 (6.0) | ||||
| Tested with partner | 10 (10.6) | 10 (9.4) | 20 (10.0) | 0.777 | |||
| Partner tested alone | 34 (40.5) | 26 (27.1) | 60 (33.3) | 0.158 | |||
| Partner HIV status | |||||||
| Negative | 59 (62.8) | 51 (48.1) | 110 (55.0) | 0.073 | |||
| Positive | 0 (0) | 1 (0.9) | 1 (0.5) | ||||
| Don’t know | 35 (37.2) | 54 (50.9) | 89 (44.5) | ||||
Bold <0.05
Figure 1a shows the average trajectories of adherence over one year in the study. We identified two trajectories of adherence (BIC= −4937; Entropy 0.90; Appendix Table 1). The first trajectory group, “high declining adherence,” comprising 52% of the sample, demonstrated high levels of adherence at the month 1 study visit (median 744 fmol/punch, interquartile range (IQR) 527,946) that persisted through month 3 followed by a rapid decline in adherence thereafter to a median of 350 fmol/punch (IQR 40,588) at month 6. The second group, “consistently low adherence,” comprising 48% of the sample, exhibited moderate adherence beginning from month 1 (median 295 fmol/punch, IQR 17, 558) with more modest declines in adherence over the remainder of the study period. While model fit was good overall, variation was evident in the individual observed patterns of PrEP use that individuals followed within these groups (Figure 1b).
Figure 1. A) Average trajectory groups based on latent groupings of continuous TVF drug levels from group-based trajectory models, and B) Descriptive observed patterns for PrEP adherence at each study visit for all AGYW in the study, by trajectory group.
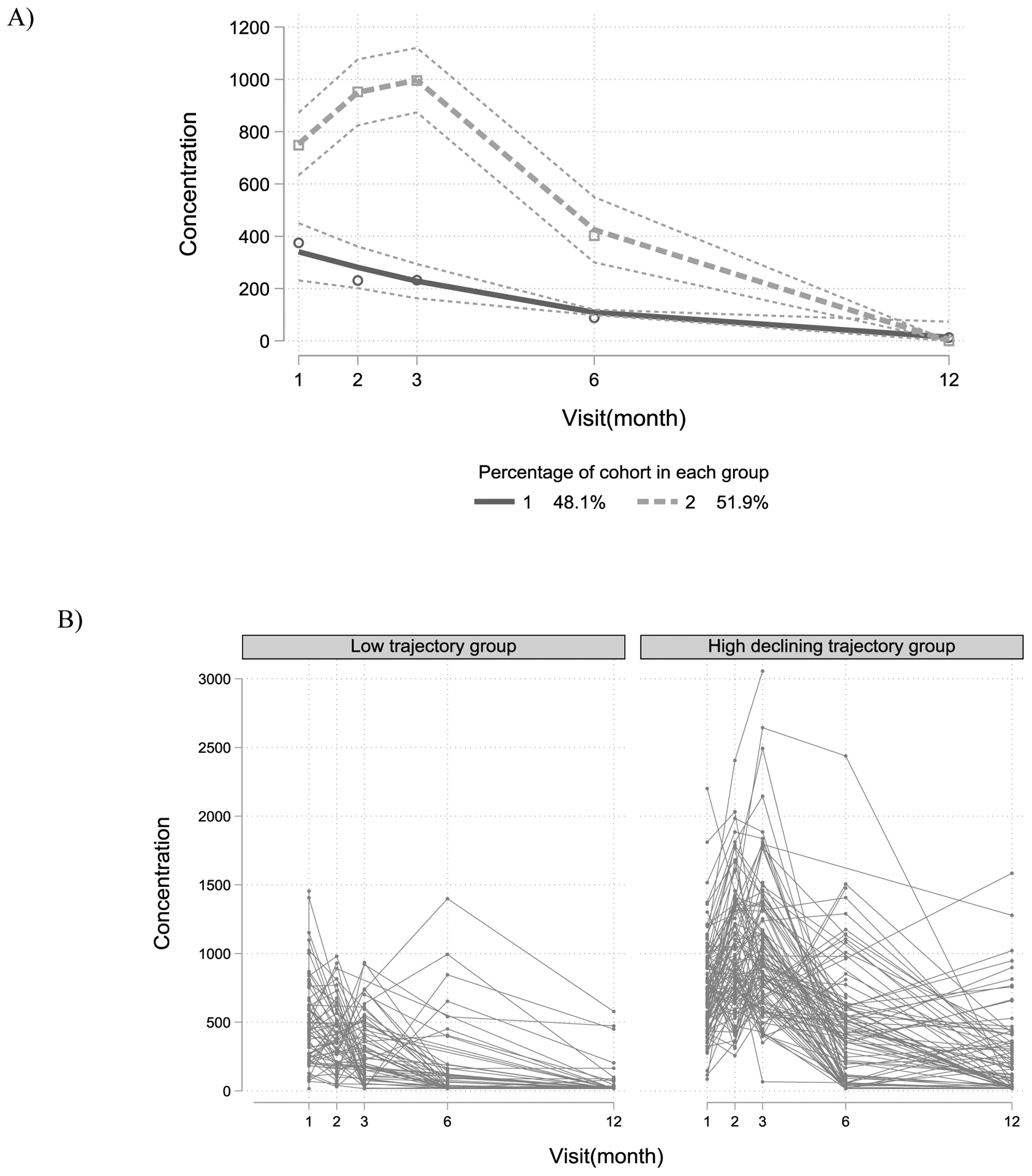
Trajectory groups were estimated using group-based trajectory models and are latent groups of individuals whose outcomes of interest follow a similar pattern over time. Individual longitudinal patterns are plots of observed adherence values at each visit for all 200 participants, split the trajectory group to which they were assigned. These individual patterns show that there is still variation of the individual patterns within each trajectory group.
Table 1 compares the characteristics of AGYW assigned to each trajectory group using a maximum probability assignment rule. Those in the high declining adherence group were more likely to disclose their PrEP plan at enrollment (95% versus 86% in the low adherence group). They were also somewhat more likely to receive the conditional incentive (56% versus 45%), and somewhat less likely to experience IPV (15% versus 22%), although these differences were not statistically significant (p-value of >0.05). They were also less likely to know their partner’s HIV status (51% versus 37%), and more likely to have a non-monogamous partner (22% versus 11%), although these again did not reach statistical significance because the study was not powered to examine these effects.
Drop in pill taking among those in the high declining group:
Thirteen participants in the qualitative cohort were in the high declining trajectory group (59%); five of these young women discontinued PrEP use before the end of the study but were still included in the qualitative analysis. The most common reasons that young women cited for discontinuation and declining adherence were lack of support from family or a partner, traumatic events, and changes in partnership. Among this group, logistical concerns were discussed, but mostly in conjunction with other competing priorities. Importantly, participants overwhelmingly described that the decline in adherence between visits three and six was due to the decreased frequency of visits after three months (from monthly to multi-month dispensing for three months). This is exemplified by an excerpt from one of the FGD with the young women who discontinued PrEP.
Participant 1: The month when you get three bottles!
Participant 2: Hey! Yho, those three bottles!
Interviewer: That was month three; did you stop at month three?
Participant 2: It was three bottles! [Murmurs in the room, everyone seems to have been overwhelmed by the three bottles] I put them in the wardrobe.
Interviewer: Everyone seems to have struggled with the three bottles; what could have helped you guys? What would have helped you guys to not miss any doses?
Participant 1: They should have given them to us one by one, like once a month.
Similarly, IDI participants indicated that they were overwhelmed by having three bottles. One participant (age 17) described her struggle by saying “I would feel motivated because I have finished a bottle so I would go and get another one. So, with the three bottles it was difficult because even if you hide the rest of the bottles you know that you still have them on the premises”. Another participant (age 22) echoed, “I struggled because I was not used [to] having more than one bottle at once so I was still adjusting to that asking myself many questions like when am I going to finish them.” Overall, the participants explained that it difficult to both store and finish three bottles on their own without support from study staff.
In contrast, the eight young women who persisted with PrEP (but were in the high declining group), seemed relatively unaffected by this change in the frequency of visits after month three. In the FGDs with persisters, most participants said that they were not worried about adherence issues and had already developed strategies to take their pills over the three-month period. One participant in the FGD stated
“What I would do is take one bottle and put it next to my bedside table, and when it was finished, I would put another one there. I wouldn’t put them all on the table; that would be too much! I did this so I wouldn’t be discouraged.”
(unidentified participant in Persister FGD)
One participant (age 21) who persisted through the end of the study described a positive experience with receiving three bottles in her IDI at month 12 by saying “three months was better because month to month was not easy sometimes you are lazy to come and take them [from the clinic] so it was better three monthly.” When asked more about any difficulties with the change in visit frequency she said, “It was easy for me because I knew that there is a pill that I must take every day.” Overall, the young women who persisted until the end of the study seemed to have established PrEP routines that made it easier for them to overcome challenges with the quarterly visits.
Barriers to pill taking within the low adherence trajectory group:
Nine of the 22 participants (41%) in the qualitative cohort were matched to the consistently low adherence group based on their posterior probability of group membership. Overall, all of these young women described that they were initially very motivated and engaged in PrEP. Most had support for PrEP use from family and friends, although two young women described challenges with their mothers. Their explanations for low adherence and eventual PrEP discontinuation centered around waning motivation and logistical barriers related to establishing a PrEP routine, leading to forgetfulness. Reasons included being busy, getting sick, moving/relocating, childcare, participation in cultural activities and difficulty attending clinics visits. For example, one participant (age 19), had high adherence the first month, followed by low adherence through month 6 and then stopped using altogether before month 12. She said that she ‘was forgetting them [the pills] most of the time’ because she was busy. Further, she had lost her pills but did not report it to the clinic because she “did not have time to come back here.” Another participant (age 19), struggled with adherence throughout the study due to motivation, logistical concerns and ultimately, problems with her partner. At the first interview she stated “you’re not sick, so you don’t actually see the whole point of taking a pill and being not sick. But I did take it, but I didn’t take it really, really well.” She later described that it was hard to establish a routine, especially when she would travel or have any type of change in her life. She said, “my routine started changing; I started to work and so I had to change things and sometimes I would forget to take my pills.” While the participants in the consistently low adherence group did struggle with other issues, such as practical skills for swallowing, stigma, or lack of support from family and partners, the biggest challenge was establishing a routine that was flexible enough to incorporate unexpected changes in their lives.
Discussion:
PrEP adherence was moderate in the first three months among this cohort of 200 young women in Cape Town, with median drug levels comparable to those that demonstrated 100% protection among MSM in the iPrEX open label extension study.19 However, about half of the cohort did not sustain adherence after month 3. In the consistently low group, poor adherence was related to social support and challenges around developing a routine for PrEP use. The group with high adherence had a steep decline at three months that corresponded to a decrease in the prescribed frequency of visits.
We observed one trajectory group with consistently low adherence over time, which is comparable with other studies.8,9,20 However, our study is the first to examine more nuanced trajectories of PrEP adherence. AGYW in the consistently low adherence group had lower PrEP disclosure at enrollment, which is similar to other studies showing that low adherence and persistence are associated with a lack of social support.21–23In addition, we found that young women in the low adherence group mentioned issues around establishing a routine for PrEP use, particularly one that was flexible enough to accommodate changes such as work schedules and moving. Adherence support interventions for AGYW immediately after PrEP initiation should focus on social support and providing strategies for establishing a routine including tips related to travel, staying away from home and storage of pill bottles.
The second trajectory group had high adherence initially which declined after three months. In quantitative analysis, young women with high declining adherence were slightly more likely to have received the cash incentive, showing that perhaps the cash incentive reinforced their motivation as they were establishing a PrEP routine,11 and were slightly more likely to have a higher risk partner (e.g. of unknown HIV status, with known other partners). In qualitative interviews, the theme that corresponded most strongly with the steep decline in adherence after three months was the change in the visit frequency. AGYW who discontinued or had low adherence after the month 3 visit felt unsupported, overwhelmed, and discouraged by having to store and finish three bottles on their own. In contrast, AGYW who had high adherence after three months developed routines that made it easier to adjust to the change in visit frequency. Our findings concur with evidence from the United States and South Africa showing that quarterly clinic visits are associated with poorer medication adherence among adolescents than initial monthly visits.20,24,25 Adherence support interventions for AGYW with high declining adherence should focus on providing consistent support to address issues as they emerge after an initial routine has been established. AGYW who may need more ongoing frequent input should be identified separately from those who can be seen less often perhaps by changes in routine (moves) or other life events. A monthly supply of PrEP may be preferable to a three-month supply for AGYW who need more frequent input and struggle with correctly implementing a daily dosage regimen.
Group-based trajectory models are an informative way to examine longitudinal patterns, but this approach is data driven and therefore the trajectories that emerge are dependent on duration of the study and sample size. Our study includes data from a one-year period of 200 AGYW.11 We may have identified a larger number of trajectories if we had a larger sample. However, average posterior probability of group membership was high in both groups (>0.9) showing good model fit and the patterns that we observed are similar to those seen in other larger studies. We also lacked power to estimate precise relationships between predictors both at baseline and over time in relation to trajectory group membership. Additionally, this study was done in the context of a randomized intervention study. Our findings may differ from what we would observe among AGYW that were not provided additional support like adherence counseling, adherence clubs and a conditional incentive. We also do not know exactly when declines occurred between month three and six since no drug data was collected between these time points. Yet, our results provide an enhanced understanding of frequency of contact and support that may be needed for different groups of AGYW over time. Lastly, our sample of 22 for the qualitative analysis was relatively modest and was not designed as part of this trajectory analysis. However, data saturation can be reached in as little as 12 interviews,26 and we were able to conduct longitudinal interviews at three different time points for each individual, creating a rich data set that showcased the different trajectories of PrEP use. Qualitative interview participants were also distributed across both trajectory groups and included 13 participants in the high declining group and 9 in the consistently low trajectory groups.
In summary, we identified two distinct trajectories of PrEP adherence among AGYW in South Africa over one-year: one with consistently low adherence and one with high adherence that declined after three months. PrEP support for these two groups should be differentiated between those who need more frequent interaction and support initially, versus later in PrEP use. Adherence in the consistently low group was related to social support and logistical concerns. Adherence support interventions after PrEP initiation should focus on social support and providing strategies for establishing a PrEP routine. Among the group that initially had high adherence, steep declines corresponded with a change in the frequency of clinic visits. Adherence support interventions in this group should focus on providing consistent support, every month when needed, to address issues as they emerge after an initial routine has been established.
Acknowledgements:
This study was funded by the NIH through award number R01HD07578. We would like to thank all of the young women who participated in this study and the study teams at the Desmond Tutu HIV Centre and the University of Washington.
Funding: The study was funded by the United States National Institute of Mental Health, award MH107251.
The study protocol was approved by the Health Science ethics review committee at University of Cape Town. All participants provided written informed consent in English or Xhosa. A parental consent waiver was granted for participants ages 16-17. Dr. Connie Celum reports grants from NIH and has served as a scientific advisor to Merck and Gilead Science. Other coauthors have no conflicts of interest.
app
Appendix Table 1:
Model fit statistics for trajectory groups*
| Shape Parameter | K | BIC (N=967) | BIC (N=200) | AIC | LL | Entropy | Smallest group (%) | Smallest group (N) | Avg Posterior probability, per group | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 3 | 1 | −4906.1 | −5004.7 | −4996.5 | −4991.5 | 1 | 1 | ||||
| 3, 3 | 2 | −4934.1 | −4926.2 | −4909.7 | −4899.7 | 0.91 | 42% | 85 | 0.91 | 0.93 | |
| 3, 3, 3 | 3 | −4914.1 | −4902.3 | −4877.6 | −4862.6 | 0.91 | 17% | 35 | 0.92 | 0.93 | 0.12 |
| 2, 3 | 2 | −4937.1 | −4937.1 | −4915.1 | −4906.1 | 0.90 | 46% | 94 | 0.920 | 0.90 | |
| 2, 2 | 2 | −4943.3 | −4937.0 | −4923.8 | −4915.8 | 0.90 | 37% | 75 | 0.89 | 0.94 | |
| 1, 3 | 2 | −4933.7 | −4927.3 | −4914.1 | −4906.1 | 0.90 | 47% | 95 | 0.92 | 0.91 | |
Models with over 4 groups do not converge; Grey indicates selected model
References:
- 1.Birdthistle I, Tanton C, Tomita A, et al. Recent levels and trends in HIV incidence rates among adolescent girls and young women in ten high-prevalence African countries: a systematic review and meta-analysis. Lancet Glob Heal. 2019;7(11):E1521–E1540. doi: 10.1016/S2214-109X(19)30410-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grant RM, Lama JR, Anderson PL, et al. Preexposure Chemoprophylaxis for HIV Prevention in Men Who Have Sex with Men. N Engl J Med. 2010;363(27):2587–2599. doi: 10.1056/NEJMoa1011205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fonner VA, Dalglish SL, Kennedy CE, et al. Effectiveness and safety of oral HIV preexposure prophylaxis for all populations. AIDS. 2016;30(12):1973–1983. doi: 10.1097/QAD.0000000000001145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baeten JM, Palanee-Phillips T, Brown ER, et al. Use of a vaginal ring containing dapivirine for HIV-1 prevention in women. N Engl J Med. 2016;375:2121–2132. doi: 10.1056/NEJMoa1506110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Marrazzo JM, Ramjee G, Richardson BA, et al. Tenofovir-Based Preexposure Prophylaxis for HIV Infection among African Women. N Engl J Med. 2015;372(6):509–518. doi: 10.1056/NEJMoa1402269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Van Damme L, Corneli A, Ahmed K, et al. Preexposure prophylaxis for HIV infection among African women. N Engl J Med. 2012;367(5):411–422. doi: 10.1056/NEJMoa1202614 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baeten JM, Donnell D, Ndase P, et al. Antiretroviral Prophylaxis for HIV Prevention in Heterosexual Men and Women. N Engl J Med. 2012;367(5):399–410. doi: 10.1056/NEJMoa1108524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rousseau-Jemwa E, Bekker L-G, Bukusi E, et al. Early persistence of HIV Pre-exposure prophylaxis (PrEP) in african adolescent girls and young women (AGYW) from Kenya and South Africa. AIDS Res Hum Retroviruses. 2018;34:68. doi: 10.1089/aid.2018.5000.abstracts [DOI] [Google Scholar]
- 9.Celum C, Mgodi N, Bekker L, et al. PrEP adherence and effect of drug level feedback among young African women in HPTN 082. In: IAS 2019: 10th IAS Conference on HIV Science. Mexico City, Mexico; 2019:Abstract TUAC0301. [Google Scholar]
- 10.Celum C, Gill K, Morton J, et al. Incentives conditioned on tenofovir levels to increase adherence among young women on PrEP in Cape Town, in 10th IAS Conference on HIV Science. In: 10th IAS Conference on HIV Science. Mexico City, Mexico; 2019:MOPEB134. [Google Scholar]
- 11.Celum CL, Gill K, Morton J, et al. Incentives conditioned on tenofovir levels to support PrEP adherence among young South African women: a randomized trial. J Int AIDS Soc Int AIDS Soc. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anderson PL, Liu AY, Castillo-Mancilla JR, et al. Intracellular tenofovir-diphosphate and emtricitabine-triphosphate in dried blood spots following directly observed therapy. Antimicrob Agents Chemother. 2018;62(1):e01710–17. doi: 10.1128/AAC.01710-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nagin DS. Group-based trajectory modeling: An overview. Ann Nutr Metab. 2014;65(2–3):205–210. doi: 10.1159/000360229 [DOI] [PubMed] [Google Scholar]
- 14.Nagin DS, Jones BL, Passos VL, Tremblay RE. Group-based multi-trajectory modeling. Stat Methods Med Res. 2018;27(7):2015–2023. doi: 10.1177/0962280216673085 [DOI] [PubMed] [Google Scholar]
- 15.Jones BL, Nagin DS. A Note on a Stata Plugin for Estimating Group-based Trajectory Models. Sociol Methods Res. 2013;42(4). doi: 10.1177/0049124113503141 [DOI] [Google Scholar]
- 16.Rucinski KB, Powers KA, Schwartz SR, et al. Longitudinal patterns of unmet need for contraception among women living with HIV on antiretroviral therapy in South Africa. PLoS One. 2018;13(12):e0209114. doi: 10.1371/journal.pone.0209114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Press Stata. Stata Statistical Software: Release 16. StataCorp LLC. 2019. [Google Scholar]
- 18.O’Rourke S, Hartmann M, Myers L, et al. The PrEP journey: Understanding how internal drivers and external circumstances impact the PrEP trajectory of adolescent girls and young women in Cape Town, South Africa. AIDS Behav. 2020;(Under Rev. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Grant RM, Anderson PL, McMahan V, et al. Uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: A cohort study. Lancet Infect Dis. 2014;14(9):820–829. doi: 10.1016/S1473-3099(14)70847-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gill K, Dietrich J, Gray G, et al. Pluspills: an open-label, safety and feasibility study of oral pre-exposure prophylaxis (PrEP) in 15–19-year-old adolescents in two sites in South Africa. In: 9th International AIDS Society Conference on HIV Science (IAS 2017). Paris, France; 2017:TUAC0207LB-Oral Abstract. [Google Scholar]
- 21.Wagner LD, Roberts ST, O’Rourke S, et al. Challenges with oral pre-exposure prophylaxis (PrEP) disclosure among adolescent girls and young women (AGYW) in Kenya and South Africa. JAIDS Res Hum Retroviruses. 2018;34:373. doi:// 10.1089/aid.2018.5000.abstracts [DOI] [Google Scholar]
- 22.Roberts ST, Haberer J, Celum C, et al. Intimate Partner Violence and Adherence to HIV Pre-exposure Prophylaxis (PrEP) in African Women in HIV Serodiscordant Relationships: A Prospective Cohort Study. J Acquir Immune Defic Syndr. 2016;73(3):313–322. doi: 10.1097/QAI.0000000000001093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Velloza J, Khoza N, Scorgie F, et al. The influence of HIV-related stigma on PrEP disclosure and adherence among adolescent girls and young women in HPTN 082: a qualitative study. J Int AIDS Soc. 2020;23(3):e25463. doi: 10.1002/jia2.25463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hosek SG, Rudy B, Landovitz R, et al. An HIV Preexposure Prophylaxis Demonstration Project and Safety Study for Young MSM. J Acquir Immune Defic Syndr. 2017;74(1):21–29. doi: 10.1097/QAI.0000000000001179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hosek SG, Landovitz RJ, Kapogiannis B, et al. Safety and Feasibility of Antiretroviral Preexposure Prophylaxis for Adolescent Men Who Have Sex With Men Aged 15 to 17 Years in the United States. JAMA Pediatr. 2017;171(11):1063–1071. doi: 10.1001/jamapediatrics.2017.2007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Guest G, Bunce A, Johnson L. How Many Interviews Are Enough? Field methods. 2006;18(1):59–82. doi: 10.1177/1525822×05279903 [DOI] [Google Scholar]