

Key Points
Question
Is a reduced-dose glucocorticoid plus rituximab regimen noninferior to the conventional high-dose glucocorticoid plus rituximab regimen in remission induction of antineutrophil cytoplasm antibody (ANCA)–associated vasculitis?
Findings
In this randomized clinical trial that included 140 patients with newly diagnosed ANCA-associated vasculitis, the proportion of patients with disease remission at 6 months was 71.0% in the reduced-dose glucocorticoid plus rituximab group and 69.2% in the high-dose glucocorticoid plus rituximab group, a difference that met the prespecified noninferiority margin of −20 percentage points.
Meaning
Among patients with newly diagnosed ANCA-associated vasculitis, a reduced-dose glucocorticoid plus rituximab regimen was noninferior to a high-dose glucocorticoid plus rituximab regimen with regard to induction of disease remission.
Abstract
Importance
The current standard induction therapy for antineutrophil cytoplasm antibody (ANCA)–associated vasculitis is the combination of high-dose glucocorticoids and cyclophosphamide or rituximab. Although these regimens have high remission rates, they are associated with considerable adverse events presumably due to high-dose glucocorticoids.
Objective
To compare efficacy and adverse events between a reduced-dose glucocorticoid plus rituximab regimen and the standard high-dose glucocorticoid plus rituximab regimen in remission induction of ANCA-associated vasculitis.
Design, Setting, and Participants
This was a phase 4, multicenter, open-label, randomized, noninferiority trial. A total of 140 patients with newly diagnosed ANCA-associated vasculitis without severe glomerulonephritis or alveolar hemorrhage were enrolled between November 2014 and June 2019 at 21 hospitals in Japan. Follow-up ended in December 2019.
Interventions
Patients were randomized to receive reduced-dose prednisolone (0.5 mg/kg/d) plus rituximab (375 mg/m2/wk, 4 doses) (n = 70) or high-dose prednisolone (1 mg/kg/d) plus rituximab (n = 70).
Main Outcomes and Measures
The primary end point was the remission rate at 6 months, and the prespecified noninferiority margin was −20 percentage points. There were 8 secondary efficacy outcomes and 6 secondary safety outcomes, including serious adverse events and infections.
Results
Among 140 patients who were randomized (median age, 73 years; 81 women [57.8%]), 134 (95.7%) completed the trial. At 6 months, 49 of 69 patients (71.0%) in the reduced-dose group and 45 of 65 patients (69.2%) in the high-dose group achieved remission with the protocolized treatments. The treatment difference of 1.8 percentage points (1-sided 97.5% CI, −13.7 to ∞) between the groups met the noninferiority criterion (P = .003 for noninferiority). Twenty-one serious adverse events occurred in 13 patients in the reduced-dose group (18.8%), while 41 occurred in 24 patients in the high-dose group (36.9%) (difference, −18.1% [95% CI, −33.0% to −3.2%]; P = .02). Seven serious infections occurred in 5 patients in the reduced-dose group (7.2%), while 20 occurred in 13 patients in the high-dose group (20.0%) (difference, −12.8% [95% CI, −24.2% to −1.3%]; P = .04).
Conclusions and Relevance
Among patients with newly diagnosed ANCA-associated vasculitis without severe glomerulonephritis or alveolar hemorrhage, a reduced-dose glucocorticoid plus rituximab regimen was noninferior to a high-dose glucocorticoid plus rituximab regimen with regard to induction of disease remission at 6 months.
Trial Registration
ClinicalTrials.gov Identifier: NCT02198248
This randomized trial compares the effect of a reduced-dose glucocorticoid plus rituximab regimen vs the standard high-dose glucocorticoid plus rituximab regimen on remission induction of antineutrophil cytoplasm antibody (ANCA)–associated vasculitis.
Introduction
Antineutrophil cytoplasm antibody (ANCA)–associated vasculitis is characterized by a vasculitis that affects small- and medium-sized vessels and the presence of ANCA. ANCA-associated vasculitis includes microscopic polyangiitis, granulomatosis with polyangiitis, and eosinophilic granulomatosis with polyangiitis. The current standard therapies for remission induction of ANCA-associated vasculitis are the combination of high-dose glucocorticoids and either cyclophosphamide or rituximab.1,2,3 Although those therapies have high remission rates of 80% to 90%, mortality at 5 years is still high at 10% to 20%. Infections and cardiovascular diseases due to treatment are the main causes of death in patients with ANCA-associated vasculitis, along with active vasculitis.4,5 There are also adverse events of treatment that significantly decrease patients’ quality of life, such as osteoporosis, peptic ulcers, myopathy, and cataracts, most of which are associated with high-dose glucocorticoids.
A rationale for B-cell depletion therapy in ANCA-associated vasculitis has emerged from the presence of B cells at sites of inflammation,6,7 the correlation between B-cell activation and disease activity,8 and the presence of pathogenic autoantibodies, myeloperoxidase (MPO) and proteinase 3 (PR3) ANCA.9,10 Rituximab is an anti-CD20 monoclonal antibody depleting B cells. Two randomized clinical trials, the RAVE and RITUXVAS trials,11,12 demonstrated similar remission rates and frequencies of adverse events between rituximab and cyclophosphamide in combination with high-dose glucocorticoids.
Data from the 2 trials suggested that high-dose glucocorticoids are the main contributor to adverse events in the current standard treatment. Although previous studies have shown that reducing glucocorticoid dose in combination with conventional immunosuppressants in remission induction was associated with frequent relapses,13,14 rituximab has a mechanism of action different from conventional immunosuppressants and retrospective studies have suggested that reduced-dose glucocorticoids plus rituximab could sufficiently induce remission of ANCA-associated vasculitis.15 Thus, this trial (Low-Dose Glucocorticoid Vasculitis Induction Study) aimed to compare the efficacy and adverse events between a reduced-dose glucocorticoid plus rituximab regimen and the standard high-dose glucocorticoid plus rituximab regimen in remission induction of ANCA-associated vasculitis.
Methods
Study Design and Participants
The study was an open-label, 2-group, parallel-design, multicenter, randomized trial. The ethics committee at each site approved the protocol and consent form. All patients provided written informed consent. Details on the trial design have been previously published,16 and the trial protocol and statistical analysis plan are available in Supplement 1 and Supplement 2, respectively. Patients were enrolled at 21 hospitals in Japan.
Inclusion in the study required a new diagnosis of ANCA-associated vasculitis (microscopic polyangiitis, granulomatosis with polyangiitis, or renal-limited vasculitis), according to the definition of the 2012 Chapel Hill Consensus Conference,17 and a positive test result for either MPO-ANCA or PR3-ANCA with the enzyme-linked immunosorbent assay, chemiluminescence enzyme immunoassay, or fluorimetric enzyme-linked immunoassay method. Patients with severe glomerulonephritis (estimated glomerular filtration rate18 [eGFR] <15 mL/min/1.73 m2) or alveolar hemorrhage (oxygen inhalation >2 L/min) were excluded. Detailed eligibility criteria are provided in the eMethods in Supplement 3.
The trial was conducted in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. To increase reliability of the results, independent monitors visited the sites to review the records and compare them with source documents for all patients. A contract research organization also performed an audit.
Randomization
Registration and allocation for an eligible patient were performed by investigators using an electronic data capture system (DATATRAK ONE version 14.1.0). Eligible patients were randomized to reduced-dose or high-dose glucocorticoid groups at a ratio of 1:1 using a minimization method with probability assignment. The assignment probability was set to 0.9. As with previous trials,11,12 known risk factors for death, namely, age at entry (<65 years vs ≥65 years) and eGFR at entry (<50 mL/min/1.73 m2 vs ≥ 50 mL/min/1.73 m2), and a risk factor for relapse, namely, ANCA subtypes (MPO-ANCA vs PR3-ANCA), were chosen as allocation adjustment factors.
Procedures
Participants were randomly allocated to the reduced-dose or high-dose glucocorticoid groups. Initial doses of prednisolone were 0.5 mg/kg/d in the reduced-dose glucocorticoid group and 1.0 mg/kg/d in the high-dose glucocorticoid group. Prednisolone was stopped at 5 months in the reduced-dose group, while the dose of prednisolone was reduced to a total of 10 mg/d by 5 months in the high-dose group (eTable 1 in Supplement 3). The high-dose regimen was consistent with current standard treatment.1,2,3 Only in cases in which the Birmingham Vasculitis Activity Score (version 3)19,20 did not reach 0 or C-reactive protein (CRP) and ANCA values were not normalized could the investigator postpone the initiation of the prednisolone discontinuation step (tapering from 5 mg/d to stopping the drug over a 14-week period) in the reduced-dose glucocorticoid regimen.
In combination with prednisolone, 4 doses of rituximab (375 mg/m2/wk) were administered via intravenous infusion in both treatment regimens. The first dose of rituximab was administered between day 1 and day 7. Except for the protocolized dose of prednisolone, systemic administration of glucocorticoids, including intravenous methylprednisolone pulse therapy, was not allowed in either treatment group. Topical administration of glucocorticoids (eg, eye drops, nasal drops, and ointment) was allowed if needed. In the absence of contraindication, the concomitant use of trimethoprim-sulfamethoxazole for Pneumocystis pneumonia prophylaxis was recommended.
Study visits were scheduled at 0, 1, 2, 4, and 6 months. At each visit, disease activity of vasculitis was measured using the Birmingham Vasculitis Activity Score (version 3),19,20 which was previously validated and has been used for clinical trials for vasculitis. It consists of a set of each weighted item divided into 9 organ systems (eg, kidney, respiratory, and nervous). Some items are objective features (eg, fever ≥38.0 °C, serum creatinine level ≥500 μmol/L), while physicians’ judgment is involved in scoring other items (eg, uveitis, sensory peripheral neuropathy). The scores range from 0 to 63, and higher scores indicate more active disease.
Outcomes
The primary end point was the remission rate at 6 months. Remission was defined as a state in which the Birmingham Vasculitis Activity Score (version 3)19,20 was 0 (or ≤1, if all items were persistent) and the oral prednisolone dose was 10 mg/d or lower.
The secondary efficacy end points included the proportion of patients who died, the proportion of patients with relapse, and the proportion of patients with end-stage kidney disease (ESKD). Death, relapse, ESKD, and remission were also assessed by time-to-event analyses. Deaths were counted as failures in the analysis of all efficacy end points. Relapse was defined as new emergence or recurrence of 1 or more items of the Birmingham Vasculitis Activity Score (version 3)19,20 after remission. The cumulative dose of prednisolone, disease activity assessed using the Birmingham Vasculitis Activity Score (version 3),19,20 health-related quality of life assessed using the Medical Outcomes Study 36-Item Short Form21,22 (scores range from 0 to 100, with higher scores indicating better health), and self-assessment by patients using 10-cm visual analog scales for overall disease activity and glucocorticoid/rituximab-related treatment toxicity (scores range from 0 cm to 10 cm, with higher scores indicating more severe activity and toxicity) were also assessed.
For secondary safety end points, the number of serious adverse events and the proportion of participants with serious adverse events were evaluated. The first serious adverse event was also assessed by time-to-event analysis. Serious adverse events were defined as adverse events associated with death, disability, hospitalization, and/or prolongation of existing hospitalization. Treatment-relatedness of adverse events was judged by the investigators who were not blinded to the patients’ treatment group. As glucocorticoid-related adverse events, new-onset diabetes, hypertension, dyslipidemia, insomnia, and infection requiring medication were specifically evaluated.
For exploratory end points, vital signs and laboratory tests, including serum CRP, IgG levels, eGFR, and peripheral B-cell count, were assessed.
Disease and treatment damage using the Vasculitis Damage Index (scores range from 0 to 64, with higher scores indicating more severe damage)23 at 6 months was assessed as a post hoc outcome.
Statistical Analysis
Based on the RITUXVAS trial11 and the Cambridge University cohort,15 we assumed 80% of the patients in both treatment groups would achieve remission at 6 months. Given the lack of data regarding the potential benefits of a reduced-dose glucocorticoid regimen for ANCA-associated vasculitis, a noninferiority margin was selected based on the margin used in the RAVE trial12: a noninferiority margin of −20 percentage points for the difference in remission rates and a 1-sided α level of .025. Assuming a 10% dropout rate, we calculated that we would need 140 patients for 80% statistical power to demonstrate noninferiority.24
The primary efficacy analyses were based on the full analysis set, which included all patients who received at least 1 dose of rituximab (full analysis set). Patients who dropped out of the study before 6 months were considered to have a treatment failure with respect to the primary end point. For the primary analysis, the risk difference in the remission induction rate at 6 months between the groups and its 1-sided 97.5% CI were estimated using a Wald statistics–based method. The findings were considered consistent with noninferiority if the lower limit of the 1-sided 97.5% CI of the risk difference exceeded −0.2. As a sensitivity analysis, adjusted risk differences were estimated by the Mantel-Haenszel method. Adjustment factors were the allocation factors.
For the other analyses, patient characteristics were compared using the Pearson χ2 test or Fisher exact test for categorical outcomes and the Wilcoxon rank-sum test for continuous variables, as appropriate. Longitudinal data were compared using analysis of covariance. Time-to-event analyses were performed with the use of log-rank test.
As post hoc analyses, we performed subgroup analyses of the primary outcome according to the minimization groups and an analysis of the mixed-effect model with site as a random effect for the primary outcome. As sensitivity analyses, we replaced dropouts with achieving the primary outcome and also analyzed the per-protocol population.
All statistical tests were 2-sided. P values less than .05 were considered statistically significant. Because of the potential for type I error due to multiple comparisons, findings for analyses of secondary end points should be interpreted as exploratory. All statistical analyses were performed using SAS version 9.4 (SAS Institute) according to the statistical analysis plan (Supplement 2).
Results
Participants
Between November 2014 and June 2019, a total of 140 patients with ANCA-associated vasculitis were enrolled in this study (Figure 1). Of these patients, 70 were randomly assigned to receive the reduced-dose regimen and 70 to receive the high-dose regimen. Five in the high-dose group and 1 in the reduced-dose group were excluded from analysis. There was 1 dropout in each treatment group. Baseline characteristics were similar between the 2 groups (Table 1). The numbers of patients who enrolled at each site are shown in eTable 2 in Supplement 3.
Figure 1. Allocation, Randomization, and Flow of Patients Through the Low-Dose Glucocorticoid Vasculitis Induction Study.

Eligible patients were randomized to reduced-dose or high-dose glucocorticoid groups at a ratio of 1:1 using a minimization method with probability assignment. The assignment probability was set to 0.9. The full analysis set was used for the primary analysis. Patients who did not receive rituximab were excluded from the analysis (1 cerebral hemorrhage before rituximab infusion after randomization in the reduced-dose group; 1 withdrawal of consent and 1 unexpected discovery of cancer before rituximab infusion after randomization in the high-dose group). We failed to collect the data of 3 patients in 1 hospital, thus they were excluded from the analysis. Therapies based on physician preference included 14 increasing doses of prednisolone, 2 azathioprine, 1 plasma exchange, 1 cyclophosphamide, 1 mycophenolate mofetil, and/or 1 rapid reduction of prednisolone dose. ANCA indicates antineutrophil cytoplasm antibody; eGFR, estimated glomerular filtration rate.
Table 1. Baseline Demographics and Characteristics of Evaluated Patients.
| Reduced-dose glucocorticoid plus rituximab (n = 69) | High-dose glucocorticoid plus rituximab (n = 65) | |
|---|---|---|
| Age, median (IQR), y | 73 (66-78) | 74 (68-78) |
| Sex, No. (%) | ||
| Female | 43 (62.3) | 37 (56.9) |
| Male | 26 (37.7) | 28 (43.1) |
| Diagnosis, No. (%) | ||
| Microscopic polyangiitis | 53 (76.8) | 51 (78.5) |
| Granulomatosis with polyangiitis | 16 (23.2) | 13 (20.0) |
| Renal-limited vasculitis | 0 (0.0) | 1 (1.5) |
| ANCA positivity, No. (%) | ||
| MPO-ANCAa | 60 (86.9) | 55 (84.6) |
| PR3-ANCAb | 9 (13.0) | 10 (15.4) |
| Estimated glomerular filtration rate, median (IQR), mL/min/1.73 m2 (normal limits ≥90 mL/min/1.73 m2)c | 52.0 (31.4-74.6) | 55.3 (41.2-72.3) |
| C-reactive protein level, median (IQR), mg/dL(normal limits ≤0.3 mg/dL)d | 7.7 (2.2-12.8) | 7.9 (1.4-12.2) |
| Birmingham Vasculitis Activity Score, median (IQR)e | 15 (10-19) | 13 (8.5-17.5) |
| System involvement, No. (%) | ||
| Constitutional | 59 (86.8) | 57 (89.1) |
| Kidney | 47 (69.1) | 34 (53.1) |
| Respiratory | 40 (58.8) | 38 (59.4) |
| Ear, nose, throat | 28 (41.2) | 21 (32.8) |
| Nervous | 20 (29.4) | 18 (28.1) |
| Cutaneous | 15 (22.1) | 8 (12.5) |
| Eye, mucosa | 8 (11.8) | 9 (14.1) |
| Cardiovascular | 2 (2.9) | 0 (0.0) |
| Gastrointestinal | 1 (1.5) | 2 (3.1) |
Abbreviations: ANCA, antineutrophil cytoplasm antibody; IQR, interquartile range; MPO, myeloperoxidase; PR3, proteinase 3.
MPO-ANCA is an autoantibody binding to myeloperoxidase and is usually associated with microscopic polyangiitis.
PR3-ANCA is an autoantibody binding to proteinase 3 and is usually associated with granulomatosis with polyangiitis.
Estimated glomerular filtration rate is an indicator of kidney dysfunction caused by kidney involvement of vasculitis.
C-reactive protein is an indicator of systemic inflammation caused by vasculitis.
The Birmingham Vasculitis Activity Score is an assessment tool for disease activity of systemic vasculitis and its scores range from 0 to 63, with higher scores indicating more active disease. A median score of approximately 15 indicates high disease activity; a score of 7-8, moderate disease activity; and 4-5, low disease activity.
Primary End Point
At 6 months, 49 in the reduced-dose group (71.0%) and 45 in the high-dose group (69.2%) achieved remission with the protocolized treatments. The difference was 1.8 percentage points (1-sided 97.5% CI, −13.7 to ∞) between groups, and the lower 95% confidence limit for the difference met the criterion for noninferiority (P = .003 for noninferiority) (Table 2). Adjusted analyses that accounted for ANCA subtype, age, and kidney function did not affect primary comparison when examined by the Mantel-Haenszel method.
Table 2. Primary and Secondary Outcomes at 6 Months.
| Outcomes | Reduced-dose glucocorticoid plus rituximab (n = 69) | High-dose glucocorticoid plus rituximab (n = 65) | Absolute difference (95% CI) | P valuea | ||
|---|---|---|---|---|---|---|
| No. (%) with data | Median (IQR) | No. (%) with data | Median (IQR) | |||
| Primary outcomes | ||||||
| Remissionb | 49 (71.0) | 45 (69.2) | 1.8 (−13.7 to ∞)c | .003d | ||
| Secondary outcomes | ||||||
| Remissionb,e | 49 (71.0) | 45 (69.2) | 0.6 (−15.3 to ∞)c,f | .005d | ||
| Relapseb | 3 (4.3) | 0 | 4.4 (−0.5 to 9.2) | .24 | ||
| Deathsb | 2 (2.9) | 3 (4.6) | −1.7 (−4.7 to 8.2) | .67 | ||
| End-stage kidney diseaseb | 0 | 1 (1.5) | −1.5 (−4.5 to 1.5) | .48 | ||
| Prednisolone, mg | ||||||
| Cumulative dose | 65 (94.2) | 1318 (989 to 1770) | 62 (95.4) | 4151.25 (3795.25 to 4376) | −2599.3 (−2856 to −2342)g | <.001 |
| Dose at 6 mo | 65 (94.2) | 2.0 (0 to 7.5) | 62 (95.4) | 10.0 (9.0 to 10.0) | −5.5 (−7.0 to −4.0)g | <.001 |
| SF-36 component summary | ||||||
| Physicalh | 54 (78.2) | 38.3 (21.1 to 47.4) | 49 (75.3) | 31.7 (22.0 to 49.4) | 6.3 (−2.6 to 15.2) | .43 |
| Mentali | 54 (78.2) | 49.8 (45.1 to 56.6) | 49 (75.3) | 50.4 (46.3 to 57.2) | −0.4 (−4.7 to 4.0) | .65 |
| Birmingham Vasculitis Activity Scorej | 65 (94.2) | 0 (0 to 1) | 58 (89.2) | 0 (0 to 0) | 0 (0 to 0) | .65 |
| Patient visual analog scale | ||||||
| Disease activity, mmk | 55 (79.7) | 12 (0 to 50) | 49 (75.3) | 24 (7 to 55) | −12.0 (−29.4 to 5.4) | .17 |
| Treatment toxicity, mml | 54 (78.2) | 2.5 (0 to 24) | 49 (75.3) | 26 (5 to 53) | −23.0 (−39.1 to −6.8) | .003 |
Abbreviations: IQR, interquartile range; SF-36, Medical Outcomes Study 36-Item Short Form.
Relapse, deaths, and end-stage kidney disease were compared by Fisher exact test. Dose of prednisolone was compared by Wilcoxon rank-sum test. SF-36, the Birmingham Vasculitis Activity Score, and visual analog scales were compared by analysis of covariance.
No. (%) with event.
Difference (97.5% CI).
P values for noninferiority.
Covariate (age, estimated glomerular filtration rate, antineutrophil cytoplasm antibody)-adjusted analysis by Mantel-Haenszel methods.
Adjusted difference.
Estimated difference with 95% CI using quantile regression.
SF-36 physical component summary is an assessment tool of physical health status and its scores range from 0 to 100, with higher scores indicating better health. A median of 31.7 to 38.3 indicates physically bad condition.
SF-36 mental component summary is an assessment tool of mental health status and its scores range from 0 to 100, with higher scores indicating better health. A median of 49.8 to 50.4 indicates normal mental health status.
The Birmingham Vasculitis Activity Score is an assessment tool for disease activity of systemic vasculitis and its scores range from 0 to 63, with higher scores indicating more active disease. A median of 0 points indicates disease remission.
Visual analog scale for disease activity of vasculitis is a self-assessment by patients and its scores range from 0 mm to 100 mm, with higher scores indicating more severe disease activity. A median of 12 mm to 24 mm indicates very low disease activity.
Visual analog scale for glucocorticoid/rituximab-related treatment toxicity is a self-assessment by patients and its scores range from 0 mm to 100 mm, with higher scores indicating more severe toxicity. A median of 2.5 mm indicates almost no toxicity and a median of 26 mm indicates mild toxicity.
Secondary Efficacy End Points
Six patients in the reduced-dose group and 8 in the high-dose group who completed the protocolized treatment did not achieve remission (Figure 1). Nine patients in the reduced-dose group and 8 in the high-dose group switched the protocolized treatment to a therapy based on physician preference because of insufficient response to the protocolized treatment except for 1 severe infusion reaction to rituximab and 1 intestinal perforation in the high-dose group. Among patients who switched treatment, 7 of 9 in the reduced-dose group and 5 of 8 in the high-dose group were in remission at 6 months. Early relapse within 6 months occurred in 3 patients in the reduced-dose group (4.3%) (1 major and 2 minor relapses) and none in the high-dose group, though the frequencies were not statistically different between treatment groups (difference, 4.3% [95% CI, −0.5% to 9.3%]; P = .24).
There were 2 deaths in the reduced-dose group (2.9%) and 3 deaths in the high-dose group (4.6%), and the frequencies were not statistically different between treatment groups (difference, −1.7% [95% CI, −4.7% to 8.2%]; P = .67). The causes of death were 1 sudden death of unknown origin (79 years old, day 50 from the study entry) and 1 subarachnoid hemorrhage (58 years old, day 14) in the reduced-dose group, and 1 sepsis case (80 years old, day 32) and 2 gastrointestinal bleedings (75 years old, day 105 and 85 years old, day 12) in the high-dose group. Cumulative survival rates at 6 months were not significantly different between the reduced-dose (97.1%) and the high-dose (95.3%) groups (difference, 1.7% [95% CI, −4.7% to 8.2%]; P = .58) (eFigure 1 in Supplement 3). ESKD occurred in 1 patient in the high-dose group (1.5%) and none in the reduced-dose group, though the frequencies were not statistically different between treatment groups (difference, −1.5% [95% CI, −4.5% to 1.5%]; P = .48).
Prednisolone doses were reduced in both groups in accordance with the protocol (eFigure 2 in Supplement 3). Median cumulative doses over the 6-month period were lower in the reduced-dose group (1318 mg) than in the high-dose group (4151.25 mg) (difference, −2599.3 mg [95% CI, −2856.6 to −2342.0]; P < .001). Median doses at 6 months were lower in the reduced-dose group (2 mg/d) than in the high-dose group (10 mg/d) (difference, −5.5 mg [95% CI, −7 to −4]; P < .001). Prednisolone was completely withdrawn in 27 patients (39.1%) in the reduced-dose group by 6 months. Twenty-two patients in the reduced-dose group postponed the final step of prednisolone tapering due to elevated ANCA titers (n = 17), more than 1 point of the Birmingham Vasculitis Activity Score (n = 11), and/or elevated CRP levels (n = 6).
Regarding quality of life at 6 months, both the physical and mental component summaries of the Medical Outcomes Study 36-Item Short Form did not statistically significantly differ between the 2 groups (difference, 6.3 [95% CI, −2.6 to 15.2], P = .43 and −0.4 [95% CI, −4.7 to 4.0]; P = .65) (eFigure 3 in Supplement 3).
The Birmingham Vasculitis Activity Scores at 6 months were not significantly different between the groups (median, 0 vs 0; difference, 0 [95% CI, 0 to 0]; P = .65) (Figure 2A). The patient visual analog scale for disease activity at 6 months was not significantly different between the reduced-dose group and the high-dose group (median, 12 mm vs 24 mm; difference, −12 mm [95% CI, −29.4 to 5.4]; P = .17), while that for treatment toxicity at 6 months was lower in the reduced-dose group than in the high-dose group (median, 2.5 mm vs 26 mm; difference, −23 mm [95% CI, −39.1 to −6.8]; P = .003) (Figure 2B and C).
Figure 2. Secondary and Exploratory Outcomes Over 6 Months.
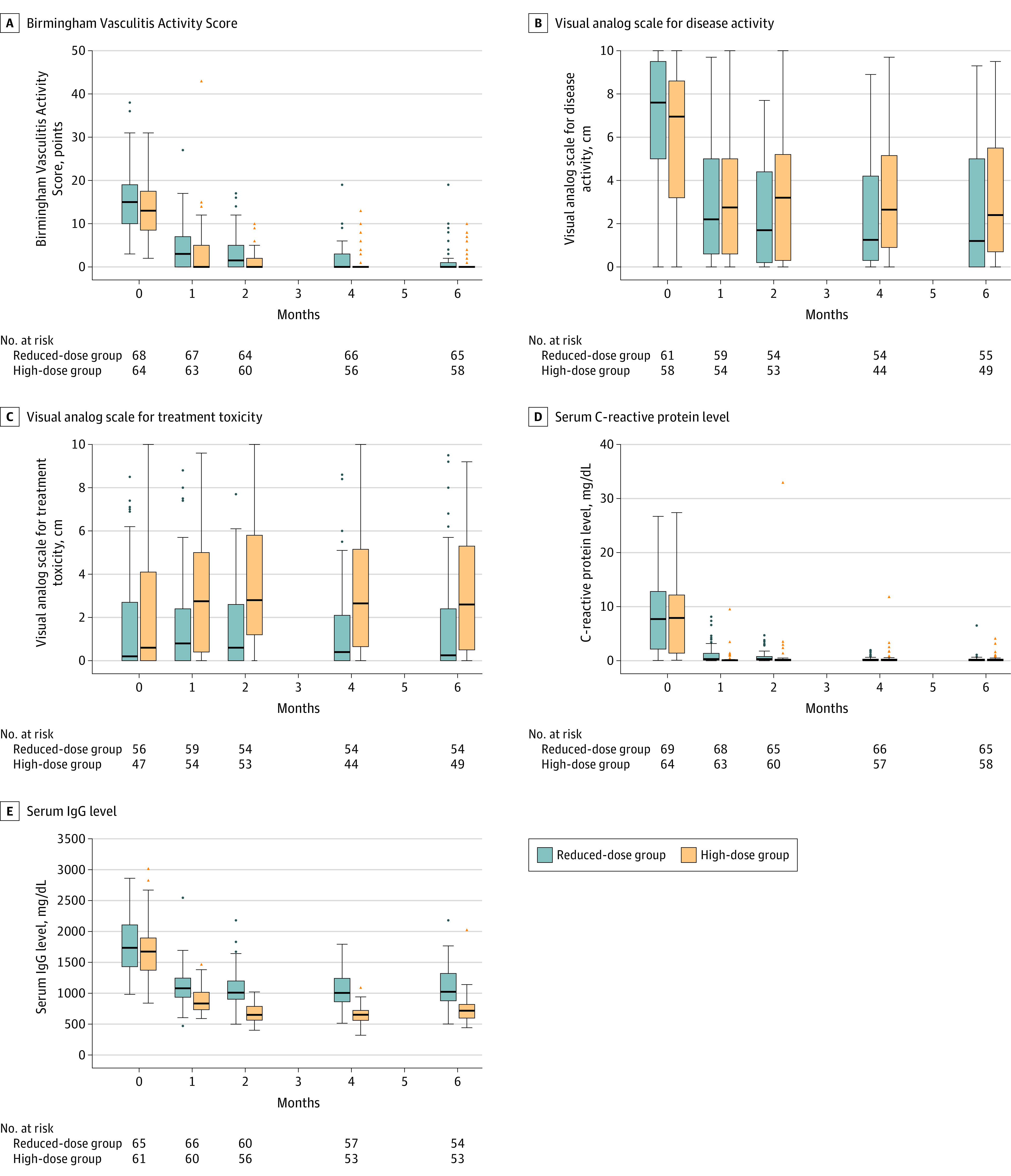
The median time of observation was 180 days (interquartile range, 180-180) for all panels. The boxes indicate the medians and interquartile ranges, the vertical lines indicate the 1.5 interquartile range, and the circles and triangles indicate outliers. A, Disease activity of vasculitis was assessed using the Birmingham Vasculitis Activity Score. The scores range from 0 to 63, and higher scores indicate more active disease. B and C, Visual analog scales based on self-assessment by patients to measure the intensity of overall disease activity and treatment toxicity. The scales range from 0 cm to 10 cm, and higher scores indicate more severe activity and toxicity. D, Normal limit of C-reactive protein level is 0.3 mg/dL or less. E, Serum IgG levels were measured by turbidimetric immunoassay, and the normal range is 870 to 1700 mg/dL.
Exploratory End Points
Median serum CRP levels at 6 months were not significantly different between groups (difference, −0.06 mg/dL [95% CI, −0.22 to 0.35]; P = .67) (Figure 2D). Median eGFR values at 6 months were not significantly different between groups (difference, 3.2 mg/min/1.73 m2 [95% CI, −5.9 to 12.2]; P = .69) (eFigure 4A in Supplement 3). Median serum IgG levels fell after induction in both groups and were higher in the reduced-dose group than in the high-dose group at 6 months (difference, 245.9 mg/dL [95% CI, 91.6 to 400.2]; P < .001) (Figure 2E). All patients who received rituximab achieved B-cell depletion (eFigure 4B in Supplement 3).
Adverse Events (Secondary Safety End Points)
Serious adverse events were less frequent in the reduced-dose group (21 events in 13 patients, 18.8%) than in the high-dose group (41 events in 24 patients, 36.9%) (difference, −18.1% [95% CI, −33.0% to −3.2%]; P = .02) (Table 3). Serious infections were also less frequent in the reduced-dose group (7 events in 5 patients, 7.2%) than in the high-dose group (20 events in 13 patients, 20.0%) (difference, −12.8% [95% CI, −24.2% to −1.3%]; P = .04). As for opportunistic infections, 1 varicella, 1 miliary tuberculosis, and 2 invasive aspergillosis cases occurred in the high-dose group, whereas 2 Pneumocystis pneumonia cases occurred in the reduced-dose group. The patients who had Pneumocystis pneumonia had not received prophylactic treatments.
Table 3. Adverse Events According to the Study Group.
| No. of events (No. of patientsa) | ||
|---|---|---|
| Reduced-dose glucocorticoid plus rituximab (n = 69) | High-dose glucocorticoid plus rituximab (n = 65) | |
| Serious adverse eventsb | 21 (13) | 41 (24) |
| Treatment-related serious adverse eventsc | 15 (9) | 31 (22) |
| Serious infectiond | 7 (5) | 20 (13) |
| Death | 2 (2) | 3 (3) |
| Cancerse | 1 (1) | 1 (1) |
| Predefined adverse eventsf | ||
| Serious and nonserious infection | 15 (11) | 45 (29) |
| New-onset | ||
| Dyslipidemia | 12 (12) | 17 (17) |
| Hypertension | 11 (11) | 14 (14) |
| Insomnia | 10 (10) | 23 (23) |
| Diabetes | 9 (9) | 19 (19) |
Numbers of patients indicate patients who had 1 or more events.
Serious adverse events were defined as adverse events related to death, disability, hospitalization, and/or prolongation of existing hospitalization.
Treatment-related serious adverse events were treatment-related and serious adverse events. Treatment-relatedness was judged by the investigators who were not blinded to treatment group membership.
Serious infections were infections related to death, disability, hospitalization, and/or prolongation of existing hospitalization.
Two cancers were 1 colon cancer case in the reduced-dose group and 1 lung cancer case in the high-dose group.
As glucocorticoid-related adverse effects, infections and new-onset insomnia, diabetes, dyslipidemia, and hypertension requiring medication were evaluated. Patients who were receiving treatment for diabetes, hypertension, dyslipidemia, and insomnia at the study entry were not counted as patients with the new-onset ones. The investigators who were not blinded to treatment group membership were able to initiate medication for those adverse events without specific criteria.
Among the predefined glucocorticoid-related adverse events, diabetes (difference, −20.8% [95% CI, −34.8% to −6.8%]; P < .001), insomnia (difference, −16.2% [95% CI −29.8% to −2.6%]; P = .02), and all infections (difference, −28.7% [95% CI −43.5% to −13.8%]; P < .001) occurred less frequently in the reduced-dose group than in the high-dose group.
Two patients developed cancer: 1 patient developed colon cancer at 2 months in the reduced-dose group and 1 patient developed lung cancer at 1 month in the high-dose group.
Post Hoc Analyses
Vasculitis Damage Index scores at 6 months were not significantly different between treatment groups (difference, −0.1 [95% CI, −0.7 to 0.4]; P = .62).
Subgroup analyses of the primary outcome are shown in eFigure 5 in Supplement 3. There were no statistically significant interactions by age, eGFR value, or ANCA subtype.
An odds ratio for the primary outcome of remission calculated by the mixed-effect model with site as a random effect was 1.09 (95% CI, 0.51 to 2.31; P = .82). The results of sensitivity analyses supported those of the primary analyses (eTable 3 in Supplement 3).
Discussion
In this randomized clinical trial of patients with newly diagnosed ANCA-associated vasculitis, a reduced-dose prednisolone regimen was noninferior to a conventional high-dose prednisolone regimen when combined with rituximab with respect to disease remission rate at 6 months. The reduced dose of prednisolone resulted in significantly reduced serious adverse events including serious infections as well as predefined glucocorticoid-related adverse effects.
In addition to the conventional end points, patient visual analog scales were also assessed as patient-oriented outcomes, which are increasingly viewed as an essential component in developing efficient therapies. Patient visual analog scale for disease activity at 6 months was not significantly different between the groups, while that for treatment toxicity was significantly in favor of the reduced-dose group compared with the high-dose group. Although patient visual analog scales have not been validated in trials for ANCA-associated vasculitis, the results of patient visual analog scales were consistent with other end points in this trial.
Recently, the results of the PEXIVAS trial have been published,25 which used a 2 × 2 factorial design to evaluate plasma exchange and rapid or standard glucocorticoid tapering in patients with the most severe ANCA-associated vasculitis with a median serum creatinine level of 327 μmol/L. The researchers reported that the rapid tapering was noninferior to the standard tapering with respect to death or ESKD. Moreover, although the choice of glucocorticoids dosage was left to each physician’s discretion, the RITAZAREM trial suggested a reduced-dose prednisolone regimen with starting dose of 0.5 mg/kg/d had a similar remission rate to a high-dose regimen in combination with rituximab in relapsing ANCA-associated vasculitis.26 Regardless of different concomitant therapies, these emerging studies and this trial collectively demonstrated that the total dose of glucocorticoids during the remission induction phase could be reduced in most patients with ANCA-associated vasculitis when combined with appropriate, potent treatment.
Among the previously mentioned trials, this trial and the PEXIVAS trial shared the concept of reducing glucocorticoid dose during the remission induction period. However, these 2 trials had distinct differences from each other. The patient population in this trial had a higher age (median, 73 years) and higher MPO-ANCA positivity (85.8%) than those in the PEXIVAS trial (median age, 63 years; MPO-ANCA positivity, 59.4%). While this study excluded severe glomerulonephritis (eGFR <15 mL/min/1.73 m2) and alveolar hemorrhage (oxygen inhalation >2 L/min), the patients in the PEXIVAS trial were limited to those patients with severe glomerulonephritis (eGFR <50 mL/min/1.73 m2) and/or alveolar hemorrhage. Accordingly, their prednisolone dose in the rapid-tapering regimen involved much higher glucocorticoid doses than that of this trial. In addition, intravenous methylprednisolone pulse therapy was administered to all patients in the PEXIVAS trial, while this trial did not allow it. Rituximab was administered in all patients in this trial, while either cyclophosphamide or rituximab was administered in the PEXIVAS trial. Achieving similar results in a different patient population increases the generalizability of the findings in support of the reduced-dose prednisolone regimen.
The ADVOCATE trial27 evaluating the efficacy of avacopan, a C5a receptor inhibitor, demonstrated that avacopan was noninferior to high-dose prednisolone in remission at week 26 and was superior to high-dose prednisone in sustained remission at week 52 in patients with ANCA-associated vasculitis. However, the avacopan group in the ADVOCATE trial still used a mean of 1349 mg of prednisolone during the remission induction phase, which was similar to the dose in the reduced-dose group in this trial (median, 1318 mg). In addition, frequencies of serious adverse events were similar between the avacopan group (37.3%) and the prednisolone group (39.0%) in the ADVOCATE trial, while the frequency was lower in the reduced-dose group (18.8%) than that in the high-dose group (36.9%) in this trial. A trial comparing avacopan and the reduced-dose prednisolone regimen in this trial will be needed.
In this trial, postponement of the initiation of the prednisolone discontinuation step in the reduced-dose group was allowed if the predefined conditions were met and an investigator suspected persistent low disease activity. This postponement occurred in 22 of 49 patients who achieved remission in the reduced-dose group. This allowance was set in the study protocol because the study aim was lowering the cumulative dose of prednisolone rather than early complete withdrawal of prednisolone. A combination of vasculitis symptoms (the Birmingham Vasculitis Activity Score), serum CRP levels, and ANCA titers was selected as a tool for assessing a possibility of persistent low disease activity. The same combination is often used in daily clinical practice, though it was not established in the clinical trial setting and not well supported by prior data.
Regarding adverse events, serious adverse events and serious infections were reduced in the reduced-dose group. To our knowledge, this is the first trial in ANCA-associated vasculitis showing that a lower glucocorticoid dose may reduce serious adverse events. In the PEXIVAS trial, frequencies of serious adverse events were similar between the reduced-dose and the standard-dose groups. Among various types of serious adverse events, only serious infection within 1 year was less frequent in the reduced-dose group than in the standard-dose group in the PEXIVAS trial. The use of intravenous methylprednisolone pulse therapy and lower baseline kidney function in the PEXIVAS trial might be the cause of different results from this trial. In addition to serious adverse events, this trial also assessed some of the typical early-phase glucocorticoid-related adverse effects. New-onset diabetes, insomnia, and infections were more frequently observed in the high-dose group than in the reduced-dose group.
Limitations
This study has several limitations. First, this was an open-label trial. Because it would be difficult to blind the effects of high-dose glucocorticoid on patients’ appearance (eg, Cushingoid facies) and blood tests (eg, cholesterol levels), the glucocorticoid intervention was not blinded in this trial. Regarding the primary end point, the Birmingham Vasculitis Activity Score consists of both subjective and objective items. Although the disease remission based on the Birmingham Vasculitis Activity Score has been shown to be a relatively objective end point,11,28,29,30 it might be influenced by the subjectivity of some components. Other end points, including death, ESKD, and serious adverse events, were objective. However, assessment of glucocorticoid-related adverse effects might be influenced by an open-label design. Knowledge of how much prednisolone a patient received could affect the investigators’ decision of initiation of treatments for glucocorticoid-related adverse effects and the reported numbers of patients with new-onset adverse effects requiring treatment.
Second, this was a nationwide but not an international study. As a result, the disease phenotypes in this trial were typical of Japanese patients with ANCA-associated vasculitis,5,31,32 including more frequent microscopic polyangiitis/MPO-ANCA positivity, more frequent lung involvement, and older onset age than patients with ANCA-associated vasculitis in North America and Europe. However, previous studies have shown that treatment responses are similar between Japan and other countries. Furthermore, most trials suggest that ANCA subtypes were not associated with remission rates in induction phase of ANCA-associated vasculitis,11,12,28,29 supporting the generalizability of remission rates of this trial. On the other hand, granulomatosis with polyangiitis/PR3-ANCA positivity is associated with a higher relapse risk. The generalizability of relapse rates of this trial might be limited to patients with microscopic polyangiitis/MPO-ANCA positivity.
Third, only newly diagnosed patients without comorbidity requiring glucocorticoids were included in this trial. It is unclear whether patients already being treated with glucocorticoids would benefit from the reduced-dose regimen.
Fourth, the basis of setting the noninferiority margin in this trial was weak, and the margin that was selected might have been too wide.
Conclusions
Among patients with newly diagnosed ANCA-associated vasculitis without severe glomerulonephritis or alveolar hemorrhage, a reduced-dose glucocorticoid plus rituximab regimen was noninferior to a high-dose glucocorticoid plus rituximab regimen with regard to induction of disease remission at 6 months.
Trial Protocol
Statistical Analysis Plan
eMethods. List of All Inclusion and Exclusion Criteria
eTable 1. Dose of Prednisolone According to the Reduced-Dose and High-Dose Regimens
eTable 2. Enrollment by Site in Each Group
eTable 3. Sensitivity Analyses as Post-Hoc Analyses
eFigure 1. Cumulative Mortality Rates of the Two Groups
eFigure 2. Changes in Dose of Prednisolone
eFigure 3. Changes in the Physical and Mental Component Summaries of the Medical Outcomes Study 36-Item Short Form of the Two Groups
eFigure 4. Changes in Estimated Glomerular Filtration Rate and Peripheral B Cell Count of the Two Groups
eFigure 5. Subgroup Analysis
Nonauthor Collaborators. LoVAS Collaborators
Data Sharing Statement
References
- 1.Yates M, Watts RA, Bajema IM, et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann Rheum Dis. 2016;75(9):1583-1594. doi: 10.1136/annrheumdis-2016-209133 [DOI] [PubMed] [Google Scholar]
- 2.Ntatsaki E, Carruthers D, Chakravarty K, et al. ; BSR and BHPR Standards, Guidelines and Audit Working Group . BSR and BHPR guideline for the management of adults with ANCA-associated vasculitis. Rheumatology (Oxford). 2014;53(12):2306-2309. doi: 10.1093/rheumatology/ket445 [DOI] [PubMed] [Google Scholar]
- 3.Harigai M, Nagasaka K, Amano K, et al. 2017 Clinical practice guidelines of the Japan Research Committee of the Ministry of Health, Labour, and Welfare for Intractable Vasculitis for the management of ANCA-associated vasculitis. Mod Rheumatol. 2019;29(1):20-30. doi: 10.1080/14397595.2018.1500437 [DOI] [PubMed] [Google Scholar]
- 4.Flossmann O, Berden A, de Groot K, et al. ; European Vasculitis Study Group . Long-term patient survival in ANCA-associated vasculitis. Ann Rheum Dis. 2011;70(3):488-494. doi: 10.1136/ard.2010.137778 [DOI] [PubMed] [Google Scholar]
- 5.Furuta S, Chaudhry AN, Hamano Y, et al. Comparison of phenotype and outcome in microscopic polyangiitis between Europe and Japan. J Rheumatol. 2014;41(2):325-333. doi: 10.3899/jrheum.130602 [DOI] [PubMed] [Google Scholar]
- 6.Voswinkel J, Müller A, Lamprecht P. Is PR3-ANCA formation initiated in Wegener’s granulomatosis lesions? granulomas as potential lymphoid tissue maintaining autoantibody production. Ann N Y Acad Sci. 2005;1051:12-19. doi: 10.1196/annals.1361.042 [DOI] [PubMed] [Google Scholar]
- 7.Voswinkel J, Mueller A, Kraemer JA, et al. B lymphocyte maturation in Wegener’s granulomatosis: a comparative analysis of VH genes from endonasal lesions. Ann Rheum Dis. 2006;65(7):859-864. doi: 10.1136/ard.2005.044909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Krumbholz M, Specks U, Wick M, Kalled SL, Jenne D, Meinl E. BAFF is elevated in serum of patients with Wegener’s granulomatosis. J Autoimmun. 2005;25(4):298-302. doi: 10.1016/j.jaut.2005.08.004 [DOI] [PubMed] [Google Scholar]
- 9.Xiao H, Heeringa P, Hu P, et al. Antineutrophil cytoplasmic autoantibodies specific for myeloperoxidase cause glomerulonephritis and vasculitis in mice. J Clin Invest. 2002;110(7):955-963. doi: 10.1172/JCI0215918 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Little MA, Al-Ani B, Ren S, et al. Anti-proteinase 3 anti-neutrophil cytoplasm autoantibodies recapitulate systemic vasculitis in mice with a humanized immune system. PLoS One. 2012;7(1):e28626. doi: 10.1371/journal.pone.0028626 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jones RB, Tervaert JW, Hauser T, et al. ; European Vasculitis Study Group . Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med. 2010;363(3):211-220. doi: 10.1056/NEJMoa0909169 [DOI] [PubMed] [Google Scholar]
- 12.Stone JH, Merkel PA, Spiera R, et al. ; RAVE-ITN Research Group . Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010;363(3):221-232. doi: 10.1056/NEJMoa0909905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Walsh M, Merkel PA, Mahr A, Jayne D. Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: a meta-analysis. Arthritis Care Res (Hoboken). 2010;62(8):1166-1173. doi: 10.1002/acr.20176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wada T, Hara A, Arimura Y, Sada KE, Makino H; Research Group of Intractable Vasculitis, Ministry of Health, Labor, and Welfare of Japan . Risk factors associated with relapse in Japanese patients with microscopic polyangiitis. J Rheumatol. 2012;39(3):545-551. doi: 10.3899/jrheum.110705 [DOI] [PubMed] [Google Scholar]
- 15.Smith RM, Jones RB, Guerry MJ, et al. Rituximab for remission maintenance in relapsing antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum. 2012;64(11):3760-3769. doi: 10.1002/art.34583 [DOI] [PubMed] [Google Scholar]
- 16.Furuta S, Sugiyama T, Umibe T, et al. ; LoVAS Trial study investigators . Low-dose glucocorticoids plus rituximab versus high-dose glucocorticoids plus rituximab for remission induction in ANCA-associated vasculitis (LoVAS): protocol for a multicentre, open-label, randomised controlled trial. BMJ Open. 2017;7(12):e018748. doi: 10.1136/bmjopen-2017-018748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jennette JC, Falk RJ, Bacon PA, et al. 2012 Revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1-11. doi: 10.1002/art.37715 [DOI] [PubMed] [Google Scholar]
- 18.Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D; Modification of Diet in Renal Disease Study Group . A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999;130(6):461-470. doi: 10.7326/0003-4819-130-6-199903160-00002 [DOI] [PubMed] [Google Scholar]
- 19.Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann Rheum Dis. 2009;68(12):1827-1832. doi: 10.1136/ard.2008.101279 [DOI] [PubMed] [Google Scholar]
- 20.Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences. Birmingham Vasculitis Activity Score (version 3). Accessed March 21, 2021. http://golem.ndorms.ox.ac.uk/calculators/bvas.html
- 21.McHorney CA, Ware JE Jr, Rogers W, Raczek AE, Lu JF. The validity and relative precision of MOS short- and long-form health status scales and Dartmouth COOP charts: results from the Medical Outcomes Study. Med Care. 1992;30(5)(suppl):MS253-MS265. doi: 10.1097/00005650-199205001-00025 [DOI] [PubMed] [Google Scholar]
- 22.Fukuhara S, Bito S, Green J, Hsiao A, Kurokawa K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J Clin Epidemiol. 1998;51(11):1037-1044. doi: 10.1016/S0895-4356(98)00095-X [DOI] [PubMed] [Google Scholar]
- 23.Exley AR, Bacon PA, Luqmani RA, et al. Development and initial validation of the Vasculitis Damage Index for the standardized clinical assessment of damage in the systemic vasculitides. Arthritis Rheum. 1997;40(2):371-380. doi: 10.1002/art.1780400222 [DOI] [PubMed] [Google Scholar]
- 24.Fleiss JL, Tytun A, Ury HK. A simple approximation for calculating sample sizes for comparing independent proportions. Biometrics. 1980;36(2):343-346. doi: 10.2307/2529990 [DOI] [PubMed] [Google Scholar]
- 25.Walsh M, Merkel PA, Peh CA, et al. ; PEXIVAS Investigators . Plasma exchange and glucocorticoids in severe ANCA-associated vasculitis. N Engl J Med. 2020;382(7):622-631. doi: 10.1056/NEJMoa1803537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Smith RM, Jones RB, Specks U, et al. ; RITAZAREM coinvestigators; RITAZAREM co-investigators . Rituximab as therapy to induce remission after relapse in ANCA-associated vasculitis. Ann Rheum Dis. 2020;79(9):1243-1249. doi: 10.1136/annrheumdis-2019-216863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jayne DRW, Merkel PA, Schall TJ, Bekker P; ADVOCATE Study Group . Avacopan for the treatment of ANCA-associated vasculitis. N Engl J Med. 2021;384(7):599-609. doi: 10.1056/NEJMoa2023386 [DOI] [PubMed] [Google Scholar]
- 28.de Groot K, Harper L, Jayne DRW, et al. ; EUVAS (European Vasculitis Study Group) . Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med. 2009;150(10):670-680. doi: 10.7326/0003-4819-150-10-200905190-00004 [DOI] [PubMed] [Google Scholar]
- 29.Jones RB, Hiemstra TF, Ballarin J, et al. ; European Vasculitis Study Group (EUVAS) . Mycophenolate mofetil versus cyclophosphamide for remission induction in ANCA-associated vasculitis: a randomised, non-inferiority trial. Ann Rheum Dis. 2019;78(3):399-405. doi: 10.1136/annrheumdis-2018-214245 [DOI] [PubMed] [Google Scholar]
- 30.Guillevin L, Pagnoux C, Karras A, et al. ; French Vasculitis Study Group . Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis. N Engl J Med. 2014;371(19):1771-1780. doi: 10.1056/NEJMoa1404231 [DOI] [PubMed] [Google Scholar]
- 31.Fujimoto S, Watts RA, Kobayashi S, et al. Comparison of the epidemiology of anti-neutrophil cytoplasmic antibody-associated vasculitis between Japan and the U.K. Rheumatology (Oxford). 2011;50(10):1916-1920. doi: 10.1093/rheumatology/ker205 [DOI] [PubMed] [Google Scholar]
- 32.Furuta S, Chaudhry AN, Arimura Y, et al. Comparison of the phenotype and outcome of granulomatosis with polyangiitis between UK and Japanese cohorts. J Rheumatol. 2017;44(2):216-222. doi: 10.3899/jrheum.160005 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
Statistical Analysis Plan
eMethods. List of All Inclusion and Exclusion Criteria
eTable 1. Dose of Prednisolone According to the Reduced-Dose and High-Dose Regimens
eTable 2. Enrollment by Site in Each Group
eTable 3. Sensitivity Analyses as Post-Hoc Analyses
eFigure 1. Cumulative Mortality Rates of the Two Groups
eFigure 2. Changes in Dose of Prednisolone
eFigure 3. Changes in the Physical and Mental Component Summaries of the Medical Outcomes Study 36-Item Short Form of the Two Groups
eFigure 4. Changes in Estimated Glomerular Filtration Rate and Peripheral B Cell Count of the Two Groups
eFigure 5. Subgroup Analysis
Nonauthor Collaborators. LoVAS Collaborators
Data Sharing Statement