

Abstract
Underactive bladder and impaired bladder compliance are irreversible problems associated with bladder fibrosis. Remodeling of the extracellular matrix is regarded as an important mechanism associated with bladder fibrosis. However, various risk factors and conditions contribute to the functional impairment of the bladder associated with fibrosis, and there is limited knowledge about bladder fibrosis-associated problems in the field of neurourology. Further studies are thus necessary to elucidate the underlying mechanism of bladder fibrosis and to identify effective treatment.
Keywords: Urinary bladder, Fibrosis, Extracellular matrix, Lower urinary tract symptoms, Collagen
INTRODUCTION
Bladder trabeculation refers to morphological changes of the bladder detrusor, including smooth muscle hypertrophy and increased collagen deposition in the detrusor extracellular matrix (ECM), resulting in fibrosis of the bladder [1,2]. These morphological changes of the bladder can be observed in patients with various voiding problems, such as neurogenic bladder and bladder outlet obstruction (BOO) [3-6]. Lower urinary tract symptoms (LUTS) in the men with benign prostatic hyperplasia (BPH) are associated with BOO, and the increased intravesical pressure that occurs in men with BOO induces hypertrophy of the bladder detrusor to overcome BOO. If BOO is not relieved, irreversible morphological changes of the bladder, such as increased collagen accumulation and fibrosis of the bladder, occur. Fibrosis of the bladder causes the loss of normal detrusor contractility; and therefore, affected patients cannot urinate by themselves [6]. In addition to BOO associated with BPH, many other conditions are associated with fibrotic changes of the bladder, such as dementia, stroke, cerebral hemorrhage, spinal cord injury, diabetes mellitus, and aging [7].
Common LUTS associated with bladder fibrosis are a weak urinary stream, intermittency, increased residual urine sensation, and abdominal straining during urination because the fibrotic bladder loses normal contractility for expelling urine from the bladder. Medical therapies using parasympathomimetics and alpha blockers have been attempted to help urination; however, inconsistent results have been reported regarding the effects of these treatments, and there is no clear evidence that they improve bladder contractility [8-11]. Some patients showed improvement of LUTS and the ability to urinate by themselves, but most patients continue to need indwelling urethral and suprapubic catheters to expel urine from their bladder due to an irreversible loss of bladder contractility [12-15].
At present, no effective treatment methods are available to prevent bladder fibrosis and to recover the impaired bladder contractility associated with bladder fibrosis. Thus, this review deals with the pathophysiology of bladder fibrosis and upcoming treatment based on a literature review.
LUTS AND DECREASED CONTRACTILITY AND COMPLIANCE OF THE BLADDER DETRUSOR ASSOCIATED WITH BLADDER FIBROSIS
Underactive bladder (UAB) is a LUTS complex characterized by incomplete bladder emptying with a decreased urinary flow rate and increased postvoid residual urine volume [15]. UAB is associated with detrusor underactivity (DU) or acontractile detrusor observed in a urodynamic study. Morphological changes such as bladder fibrosis induced by increased collagen deposition in the detrusor ECM can induce DU and impairment of bladder contractility. According to a study reporting urodynamic results in UAB patients, detrusor hyperreflexia with impaired detrusor contractility (DHIC) was observed, as well as DU or acontractile detrusor [16]. Patients with DHIC experienced storage symptoms such as incontinence or urgency with accompanying symptoms induced by incomplete emptying [17]. These findings suggest that contractile changes associated with bladder fibrosis constitute a complicated process that results in impaired bladder contractility with or without detrusor overactivity. Furthermore, the process of a coexistent voiding problem that is not associated with bladder fibrosis (e.g., stress urinary incontinence) can be a factor that induces incontinence [18-20]. Moreover, Uren et al. [21] reported that patients diagnosed with DU using a urodynamic study showed nocturia, frequent daytime urination, urgency, and incontinence, as well as a weak urinary stream, hesitancy, and abdominal straining during urination. However, Uren et al. [21] did not investigate the etiology of DU, making it impossible to know whether the patients with storage LUTS had other voiding problems unrelated to DU.
Decreased bladder compliance is a change associated with bladder fibrosis. Bladder compliance can be conceptualized as the relationship between a change in bladder volume and a change in detrusor pressure. In general, bladder compliance is expressed as an increase in bladder volume per increment of intravesical pressure [22]. Thus, bladder compliance reflects the flexibility of the bladder. Fibrotic changes of the bladder reduce its flexibility and induce stiffness of the bladder and low bladder compliance. As a result, the intravesical pressure of a stiff bladder with low compliance is increased, and prolonged high intravesical pressure adversely affects renal function [23-26]. Therefore, it is important to improve bladder compliance and reduce the intravesical pressure of the bladder to prevent impairment of renal function. Patients with impaired bladder compliance show urge urinary incontinence [27].
Both UAB and impaired bladder compliance are associated with bladder fibrosis. However, it is unclear about why the consequences of bladder fibrosis sometimes appear as UAB or impaired bladder compliance. Previous studies have suggested that there may be a difference in the subtype of collagen deposition between UAB and impaired bladder compliance, and that increased proteoglycan deposition in the ECM may also be related factor (Fig. 1) [28-31].
Fig. 1.
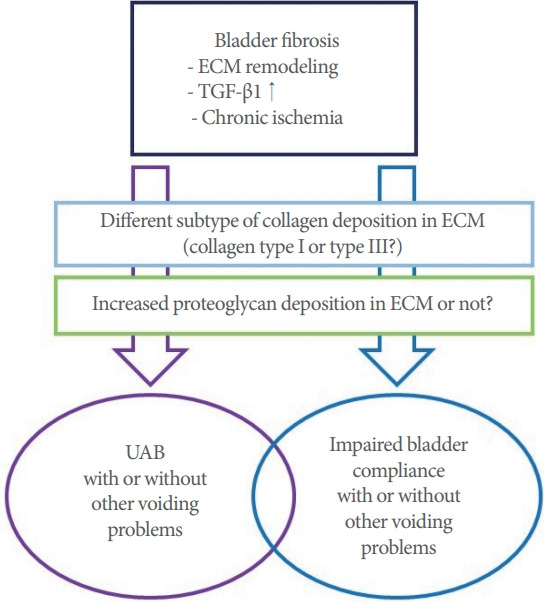
Potential theoretical mechanism of bladder fibrosis-associated voiding problems. ECM, extracelluar matrix; TGF-β1, transforming growth factor-β1; UAB, underactive bladder.
UNDERLYING MECHANISM ASSOCIATED WITH BLADDER FIBROSIS
Remodeling of the ECM and increased levels of transforming growth factor-β1 (TGF-β1) are regarded as the mechanism underlying bladder fibrosis [32]. The ECM of the bladder consists of collagen, elastin, fibronectins, and proteoglycans. Collagen is the major fibrous protein of the ECM and plays a role in providing tensile strength to the bladder. Collagen types I and III are the most important subtypes of collagen in the ECM [33- 35]. Unlike collagen, elastin induces recoil of the ECM after stretching during urination. Conditions such as BOO and neurogenic bladder associated with mechanical or chemical stresses induce fibroblastic and inflammatory responses in the ECM. These responses dysregulate fibroblast secretion of matrix metalloproteinases (MMPs) and tissue inhibitors of MMPs (TIMPs) and increase ECM deposition. Prolonged ECM deposition increases the production of TIMPs which are associated with fibrosis and fibrotic changes of the bladder occur [36-38]. Moreover, increased levels of TGF-β1 induce fibrosis by stimulating collagen production through binding to serine/threonine kinase receptors on the cell surface, cause the phosphorylation of intracellular Smad2/3 transcription factors [39,40].
Chronic bladder ischemia may be a factor associated with bladder fibrosis. Previous studies have suggested that cardiovascular and metabolic diseases related to endothelial dysfunction decrease blood flow to the bladder. In turn, chronic ischemia of the bladder was found to increase oxidative stress and inflammatory cytokine levels, which might be associated with bladder fibrosis induced by nerve damage [41].
UPCOMING THERAPEUTIC METHODS TO PREVENT AND TREAT BLADDER FIBROSIS
There is currently no effective treatment for LUTS associated with bladder fibrosis. Conventional medical treatment fails in most patients with voiding problems induced by bladder fibrosis, and these patients require catheterization to expel urine from the bladder. Therefore, studies have aimed to prevent and restore bladder fibrosis using antifibrotic agent such as relaxin. Ikeda et al. [42] showed that human relaxin-2 reversed fibrosis, decreased collagen deposition, and increased bladder compliance and detrusor contractility in patients with radiation-induced bladder fibrosis. A recent study reported that relaxin receptors were present in the dome and trigone of the human bladder and that in vitro relaxin stimulation upregulated MMP- 2 and decreased TGF-β1 [43].
Efforts have been made to apply stem cell and gene therapy to improve UAB associated with bladder fibrosis [20]. Several preclinical studies used various types of stem cells and showed improvements in detrusor contractility. A pilot study by Levanovich et al. [44] showed enhanced urination and a reduced need for clean intermittent catheterization in a patient with UAB after an intradetrusor injection of autologous muscle-derived stem cells.
CONCLUSIONS
Bladder fibrosis is an irreversible change of the bladder that is associated with UAB and impaired bladder compliance. Although bladder fibrosis is a serious problem, it has been difficult to elucidate its exact underlying mechanism and risk factors. Moreover, the progression of voiding problems associated with bladder fibrosis cannot be predicted due to the unknown characteristics of conditions associated with bladder fibrosis. There problematic characteristics are also obstacles to the prevention and treatment of bladder fibrosis. Therefore, further studies are essential to elucidate the underlying mechanism of bladder fibrosis and to identify effective treatments.
Footnotes
Fund/Grant Support
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2018R1D1A3B07048492).
Conflict of Interest
SJK and KHK, associate editors of International Neurourology Journal, are the authors of this article. However, they played no role whatsoever in the editorial evaluation of this article or the decision to publish it. Except for that, no potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization: SJK
·Data curation: JK
·Formal analysis: YGN
·Funding acquisition: KHK
·Methodology: JK
·Project administration: KHK
·Visualization: YGN
·Writing-original draft: SJK
·Writing-review & editing: SJK
REFERENCES
- 1.Barnard RJ, Dixon JS, Gosling JA. A clinical and morphological evaluation of the trabeculated urinary bladder. Prog Clin Biol Res. 1981;78:285–8. [PubMed] [Google Scholar]
- 2.Jung JH, Cho SY, Yoo C, Oh SJ. Establishment of the novel cystoscopic classification for bladder trabeculation of neurogenic bladder. Urology. 2014;84:515–9. doi: 10.1016/j.urology.2014.05.015. [DOI] [PubMed] [Google Scholar]
- 3.Selby B, Hidas G, Chuang KW, Soltani T, Billimek J, Kaplan S, et al. Development and validation of a bladder trabeculation grading system in pediatric neurogenic bladder. J Pediatr Urol. 2020;16:367–70. doi: 10.1016/j.jpurol.2020.03.007. [DOI] [PubMed] [Google Scholar]
- 4.Hoffberg HJ, Cardenas DD. Bladder trabeculation in spinal cord injury. Arch Phys Med Rehabil. 1986;67:750–3. doi: 10.1016/0003-9993(86)90009-2. [DOI] [PubMed] [Google Scholar]
- 5.Bai SW, Park SH, Chung DJ, Park JH, Shin JS, Kim SK, et al. The significance of bladder trabeculation in the female lower urinary system: an objective evaluation by urodynamic studies. Yonsei Med J. 2005;46:673–8. doi: 10.3349/ymj.2005.46.5.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fusco F, Creta M, De Nunzio C, Iacovelli V, Mangiapia F, Li Marzi V, et al. Progressive bladder remodeling due to bladder outlet obstruction: a systematic review of morphological and molecular evidences in humans. BMC Urol. 2018;18:15. doi: 10.1186/s12894-018-0329-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Santos-Pereira M, Charrua A. Understanding underactive bladder: a review of the contemporary literature. Porto Biomed J. 2020;5:e070. doi: 10.1097/j.pbj.0000000000000070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gaitonde S, Malik RD, Christie AL, Zimmern PE. Bethanechol: is it still being prescribed for bladder dysfunction in women? Int J Clin Pract. 2019;73:e13248. doi: 10.1111/ijcp.13248. [DOI] [PubMed] [Google Scholar]
- 9.Osman NI, Chapple CR. Are there pharmacotherapeutic options for underactive bladder? Eur Urol Focus. 2018;4:6–7. doi: 10.1016/j.euf.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 10.Yamanishi T, Yasuda K, Kamai T, Tsujii T, Sakakibara R, Uchiyama T, et al. Combination of a cholinergic drug and an α-blocker is more effective than monotherapy for the treatment of voiding difficulty in patients with underactive detrusor. Int J Urol. 2004;11:88–96. doi: 10.1111/j.1442-2042.2004.00753.x. [DOI] [PubMed] [Google Scholar]
- 11.Chang SJ, Chiang IN, Yu HJ. The effectiveness of tamsulosin in treating women with voiding difficulty. Int J Urol. 2008;15:981–5. doi: 10.1111/j.1442-2042.2008.02134.x. [DOI] [PubMed] [Google Scholar]
- 12.Bayrak Ö, Dmochowski RR. Underactive bladder: a review of the current treatment concepts. Turk J Urol. 2019;45:401–9. doi: 10.5152/tud.2019.37659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aggarwal H, Zimmern PE. Underactive bladder. Curr Urol Rep. 2016;17:17. doi: 10.1007/s11934-016-0582-6. [DOI] [PubMed] [Google Scholar]
- 14.Dewulf K, Abraham N, Lamb LE, Griebling TL, Yoshimura N, Tyagi P, et al. Addressing challenges in underactive bladder: recommendations and insights from the Congress on Underactive Bladder (CURE-UAB) Int Urol Nephrol. 2017;49:777–85. doi: 10.1007/s11255-017-1549-3. [DOI] [PubMed] [Google Scholar]
- 15.Chapple CR, Osman NI, Birder L, Dmochowski R, Drake MJ, van Koeveringe G, et al. Terminology report from the International Continence Society (ICS) Working Group on Underactive Bladder (UAB) Neurourol Urodyn. 2018;37:2928–31. doi: 10.1002/nau.23701. [DOI] [PubMed] [Google Scholar]
- 16.Li X, Liao LM, Chen GQ, Wang ZX, Lu TJ, Deng H. Clinical and urodynamic characteristics of underactive bladder: data analysis of 1726 cases from a single center. Medicine (Baltimore) 2018;97:e9610. doi: 10.1097/MD.0000000000009610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Uren AD, Drake MJ. Definition and symptoms of underactive bladder. Investig Clin Urol. 2017;58(Suppl 2):S61–7. doi: 10.4111/icu.2017.58.S2.S61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Natale F, Illiano E, Zucchi A, Balzarro M, La Penna C, Costantini E. Transobturator mid-urethral sling in females with stress urinary incontinence and detrusor underactivity: effect on voiding phase. Int Urogynecol J. 2019;30:1519–25. doi: 10.1007/s00192-019-03871-7. [DOI] [PubMed] [Google Scholar]
- 19.Ko KJ, Suh YS, Sung HH, Ryu GH, Lee M, Lee KS. Assessing the readjustable sling procedure (Remeex system) for female stress urinary incontinence with detrusor underactivity. Int Neurourol J. 2017;21:116–20. doi: 10.5213/inj.1732682.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cho KJ, Kim JC. Management of urinary incontinence with underactive bladder: a review. Int Neurourol J. 2020;24:111–7. doi: 10.5213/inj.2040076.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Uren AD, Cotterill N, Harding C, Hillary C, Chapple C, Klaver M, et al. Qualitative exploration of the patient experience of underactive bladder. Eur Urol. 2017;72:402–7. doi: 10.1016/j.eururo.2017.03.045. [DOI] [PubMed] [Google Scholar]
- 22.Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21:167–78. doi: 10.1002/nau.10052. [DOI] [PubMed] [Google Scholar]
- 23.Nseyo U, Santiago-Lastra Y. Long-term complications of the neurogenic bladder. Urol Clin North Am. 2017;44:355–66. doi: 10.1016/j.ucl.2017.04.003. [DOI] [PubMed] [Google Scholar]
- 24.Holmdahl G, Sillen U, Hellström AL, Sixt R, Sölsnes E. Does treatment with clean intermittent catheterization in boys with posterior urethral valves affect bladder and renal function? J Urol. 2003;170:1681–5. doi: 10.1097/01.ju.0000084142.71123.b5. [DOI] [PubMed] [Google Scholar]
- 25.Ghoniem GM, Bloom DA, McGuire EJ, Stewart KL. Bladder compliance in meningomyelocele children. J Urol. 1989;141:1404–6. doi: 10.1016/s0022-5347(17)41323-1. [DOI] [PubMed] [Google Scholar]
- 26.Prakash NS, Lopategui DM, Gomez C. Changes in management of poorly compliant bladder in botulinum toxin A era. Curr Urol Rep. 2017;18:64. doi: 10.1007/s11934-017-0707-6. [DOI] [PubMed] [Google Scholar]
- 27.Truss MC, Stief CG, Uckert S, Becker AJ, Schultheiss D, Machtens S, et al. Initial clinical experience with the selective phosphodiesterase- I isoenzyme inhibitor vinpocetine in the treatment of urge incontinence and low compliance bladder. World J Urol. 2000;18:439–43. doi: 10.1007/pl00007088. [DOI] [PubMed] [Google Scholar]
- 28.Lee BR, Perlman EJ, Partin AW, Jeffs RD, Gearhart JP. Evaluation of smooth muscle and collagen subtypes in normal newborns and those with bladder exstrophy. J Urol. 1996;156:2034–6. [PubMed] [Google Scholar]
- 29.Imamura M, Kanematsu A, Yamamoto S, Kimura Y, Kanatani I, Ito N, et al. Basic fibroblast growth factor modulates proliferation and collagen expression in urinary bladder smooth muscle cells. Am J Physiol Renal Physiol. 2007;293:F1007–17. doi: 10.1152/ajprenal.00107.2007. [DOI] [PubMed] [Google Scholar]
- 30.Asgari M, Latifi N, Heris HK, Vali H, Mongeau L. In vitro fibrillogenesis of tropocollagen type III in collagen type I affects its relative fibrillar topology and mechanics. Sci Rep. 2017;7:1392. doi: 10.1038/s41598-017-01476-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Iozzo RY, Schaefer L. Proteoglycan form and function: a comprehensive nomenclature of proteoglycans. Matrix Biol. 2015;42:11–55. doi: 10.1016/j.matbio.2015.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Koeck I, Burkhard FC, Monastyrskaya K. Activation of common signaling pathways during remodeling of the heart and the bladder. Biochem Pharmacol. 2016;102:7–19. doi: 10.1016/j.bcp.2015.09.012. [DOI] [PubMed] [Google Scholar]
- 33.Rozario T, DeSimone DW. The extracellular matrix in development and morphogenesis: a dynamic view. Dev Biol. 2010;341:126–40. doi: 10.1016/j.ydbio.2009.10.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Schaefer L, Schaefer RM. Proteoglycans: from structural compounds to signaling molecules. Cell Tissue Res. 2010;339:237–46. doi: 10.1007/s00441-009-0821-y. [DOI] [PubMed] [Google Scholar]
- 35.Almalki SG, Agrawal DK. Effects of matrix metalloproteinases on the fate of mesenchymal stem cells. Stem Cell Res Ther. 2016;7:129. doi: 10.1186/s13287-016-0393-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Craig VJ, Zhang L, Hagood JS, Owen CA. Matrix metalloproteinases as therapeutic targets for idiopathic pulmonary fibrosis. Am J Respir Cell Mol Biol. 2015;53:585–600. doi: 10.1165/rcmb.2015-0020TR. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Arpino V, Brock M, Gill SE. The role of TIMPs in regulation of extracellular matrix proteolysis. Matrix Biol. 2015;44-46:247–54. doi: 10.1016/j.matbio.2015.03.005. [DOI] [PubMed] [Google Scholar]
- 38.da Costa AWF, do Carmo Neto JR, Braga YLL, Silva BA, Lamounier AB, Silva BO, et al. Cardiac Chagas disease: MMPs, TIMPs, Galectins, and TGF-β as tissue remodelling players. Dis Markers. 2019;2019:3632906. doi: 10.1155/2019/3632906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.He R, Zhang J, Luo D, Yu Y, Chen T, Yang Y, et al. Upregulation of transient receptor potential canonical type 3 channel via AT1R/TGF- β1/Smad2/3 induces atrial fibrosis in aging and spontaneously hypertensive rats. Oxid Med Cell Longev. 2019;2019:4025496. doi: 10.1155/2019/4025496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Song S, Zhang R, Cao W, Fang G, Yu Y, Wan Y, et al. Foxm1 is a critical driver of TGF-β-induced EndMT in endothelial cells through Smad2/3 and binds to the Snail promoter. J Cell Physiol. 2019;234:9052–9064. doi: 10.1002/jcp.27583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Yoshida M, Yamaguchi O. Detrusor underactivity: the current concept of the pathophysiology. Low Urin Tract Symptoms. 2014;6:131–7. doi: 10.1111/luts.12070. [DOI] [PubMed] [Google Scholar]
- 42.Ikeda Y, Zabbarova IV, Birder LA, Wipf P, Getchell SE, Tyagi P, et al. Relaxin-2 therapy reverses radiation-induced fibrosis and restores bladder function in mice. Neurourol Urodyn. 2018;37:2441–51. doi: 10.1002/nau.23721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Diaz EC, Briggs M, Wen Y, Zhuang G, Wallace SL, Dobberfuhl AD, et al. Characterizing relaxin receptor expression and exploring relaxin’s effect on tissue remodeling/fibrosis in the human bladder. BMC Urol. 2020;20:44. doi: 10.1186/s12894-020-00607-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Levanovich PE, Diokno A, Hasenau DL, Lajiness M, Pruchnic R, Chancellor MB. Intradetrusor injection of adult muscle-derived cells for the treatment of underactive bladder: pilot study. Int Urol Nephrol. 2015;47:465–7. doi: 10.1007/s11255-015-0924-1. [DOI] [PubMed] [Google Scholar]