

Abstract
目的
探讨改良关节镜下弹性固定 Latarjet 手术治疗伴有明显肩胛盂前缘骨缺损的肩关节复发性前脱位时,移植骨块偏外放置在术后中期对肩关节退变的影响。
方法
回顾分析 2015 年 1 月—2016 年 11 月收治且符合选择标准的 18 例肩关节复发性前脱位伴肩胛盂前缘骨缺损患者临床资料,均接受改良关节镜下弹性固定 Latarjet 手术。男 12 例,女 6 例;年龄 19~37 岁,平均 26.2 岁。肩关节脱位 4~30 次,平均 8.8 次。病程 8~49 个月,平均 23.8 个月。肩胛盂前缘骨缺损为 20%~29%,平均 25.2%。肩关节不稳定严重指数评分(ISIS)为 7~10 分,平均 7.6 分。肩关节退变 Samilson-Prieto 分级:0 级 13 例,Ⅰ级 3 例,Ⅱ级 2 例。手术前后采用疼痛视觉模拟评分(VAS)、美国肩肘外科协会评分(ASES)、Walch-Duplay 评分、Rowe 评分和肩关节活动度评价临床疗效。影像学观察肩关节退变情况以及移植骨块位置、肩胛盂塑形情况。
结果
术后患者均获随访,随访时间 55~62 个月,平均 59.6 个月。无血管神经损伤、感染、固定物和移植骨块相关并发症发生,随访期间无肩关节脱位复发和翻修患者。患者均恢复正常生活,17 例重返运动。末次随访时,VAS 评分较术前明显降低,ASES 评分、Walch-Duplay 评分、Rowe 评分明显提高,差异均有统计学意义(P<0.05);肩关节前屈、外展、外展 90° 外旋、0° 外旋和外展 90° 内旋活动度与术前比较,差异均无统计学意义(P>0.05)。术后即刻三维 CT 显示所有移植骨块中心在肩胛盂 En-face 面上位于 3∶30~4∶30(右肩)或 7∶40~8∶20(左肩)位置,无移植骨块过高或过低;在 CT 横断面上相对于肩胛盂偏外 2.3~4.6 mm,平均 3.5 mm。患者术后 36、48 个月及末次随访时的肩关节退变 Samilson-Prieto 分级与术前一致,均未进展。所有移植骨块在术后 24 个月内塑形达稳定,在三维 CT 肩胛盂 En-face 面显示塑形后的肩胛盂外形为与正常肩胛盂相近的正梨形,在 CT 横断面上为与肩胛盂齐平并形成与肱骨头圆形近似的弧形。末次随访时肩胛盂外形与术后 24 个月比较无明显变化。
结论
改良关节镜下弹性固定 Latarjet 手术中移植骨块偏外放置,术后中期未出现肩关节退变进展的影像学改变。
Keywords: 复发性肩关节前脱位, 改良 Latarjet 手术, 关节镜, 弹性固定, 肩关节退变
Abstract
Objective
To investigate the mid-term effect of lateral placement of bone graft on shoulder joint degeneration after modified arthroscopic Latarjet surgery with elastic fixation for recurrent anterior shoulder dislocation with an anterior glenoid bone defect.
Methods
According to the inclusion and exclusion criteria, 18 patients with recurrent anterior shoulder dislocation and anterior glenoid bone defect who received the modified arthroscopic Latarjet surgery with elastic fixation between January 2015 and November 2016 were enrolled in this study. There were 12 males and 6 females with an average age of 26.2 years (range, 19-37 years). The number of shoulder dislocation ranged from 4 to 30 times (mean, 8.8 times). The disease duration was 8-49 months (mean, 23.8 months). The mean anterior glenoid bone defect was 25.2% of the glenoid surface (range, 20%-29%). The mean preoperative Instability Severity Index Score (ISIS) was 7.6 (range, 7-10). According to Samilson-Prieto classification, the shoulder joint degeneration was rated as grade 0 in 13 cases, grade Ⅰ in 3 cases, and grade Ⅱ in 2 cases. Before and after operation, the visual analogue scale (VAS) score, American Society of Shoulder and Elbow Surgery (ASES) score, Walch-Duplay score, Rowe score, and shoulder mobility were used to evaluate the effectiveness. Imaging examination was performed to observe the shoulder joint degeneration, the position of the bone graft, and the postoperative shaping of the scapular glenoid.
Results
All patients were followed up 55-62 months, with an average of 59.6 months. There was no neurovascular injuries, infections, fixation-related and bone graft-related complications. No re-dislocation and revision occurred. All patients returned to normal life, 17 of whom returned to sport. The VAS score was significantly decreased and ASES, Walch-Duplay, and Rowe scores were significantly improved at last follow-up (P<0.05). No significant difference was found in range of motion of forward flexion, abduction, lateral rotation at 90° abduction, internal rotation at 90° abduction, or lateral rotation at 0° between pre- and post-operation (P>0.05). Three-dimensional CT showed that the centers of all bone grafts were between 3∶30 and 4∶30 (right shoulder) or between 7∶40 and 8∶20 (left shoulder) and no bone grafts were positioned superiorly or inferiorly in the glenoid En-face view. All bone grafts were positioned lateral to the scapular glenoid with an average distance of 3.5 mm (range, 2.3-4.6 mm) in cross-sectional imaging by CT. Compared with the preoperative Samilson-Prieto classification results, all cases showed no progression of shoulder joint degeneration at 36, 48 months and last follow-up. All bone grafts remodeled to a steady state within 24 months after operation. The bone graft and glenoid finally remodeled analogous to the shape of the intact glenoid in the En-face view and became flush with the glenoid rim, remodeling to a curved shape congruent to the humeral head in cross-sectional imaging by CT. The shape of the remodeled glenoid at last follow-up was not significantly different from that at 24 months after operation.
Conclusion
The lateral placement of the bone graft during modified arthroscopic Latarjet surgery with elastic fixation do not accelerate the imaging changes of shoulder joint degeneration.
Keywords: Recurrent anterior shoulder dislocation, modified Latarjet surgery, arthroscopy, elastic fixation, shoulder joint degeneration
Latarjet 手术被视为治疗伴有明显肩胛盂前缘骨缺损的肩关节复发性前脱位的“金标准”,传统 Latarjet 手术采用螺钉硬性固定移植骨块,获得了较好临床疗效[1-3]。然而,随着临床应用增多及随访时间延长,研究发现螺钉硬性固定术后肩关节退变进展率可高达 20%~25%[2]。在诸多引起术后肩关节退变进展的危险因素中,移植骨块偏外放置[2, 4-6]和螺钉相关因素(如螺钉成角[7]、裸露[8]、突出[9]等)的影响尤为明显。2016 年 Boileau 等[10]报道采用关节镜下线袢法 Latarjet 手术治疗此类患者。该术式利用线袢弹性固定代替传统螺钉硬性固定,并采用特制的导向系统进行移植骨块定位,术中 96% 移植骨块固定位置与肩胛盂齐平,降低了移植骨块偏外放置比例,有效避免了引起术后肩关节退变进展的两大主要危险因素。
但 Boileau 等[10]提出的术式是在关节镜下截取喙突且需要 6~7 个关节镜入路,操作相对复杂、费时。因此,我们提出改良关节镜下弹性固定 Latarjet 手术[11],主要改良点包括采用开放小切口截取及修整喙突;术中只需要 3 个关节镜入路;采用套管置线避免在向后牵拉喙突、缝线时造成软组织缠绕;采用骨块防旋装置(防旋转线和锚钉);在交换棒保护腋神经下从后向前、由内到外劈开肩胛下肌腱。以上改良措施使移植骨块愈合面新鲜化更简单彻底、操作更简便、骨块更稳定、对腋神经和肩胛下肌腱损伤更小,同时手术时间也大大缩短。前期临床应用该改良术式并随访 3 年疗效[12]与 Boileau 等[13]报道相似。此外,我们还发现偏外放置的移植骨块术后塑形更好,塑形稳定后的肩胛盂更接近正常形态,而且在 3 年随访中移植骨块偏外放置患者均未见肩关节退变或退变加快的影像学改变。为进一步明确随时间延长此类患者肩关节退变情况,我们进行了进一步随访。报告如下。
1. 临床资料
1.1. 患者选择标准
纳入标准:① 年龄<40 岁;② 外伤性肩关节复发性前脱位;③ 肩胛盂前缘骨缺损>20%、肩胛盂前缘骨缺损>15%+肩关节不稳定严重指数评分(ISIS)>6 分或者肩胛盂前缘骨缺损 10%~15%+有对抗性运动需求;④ 术后 CT 扫描证实移植骨块偏外放置(骨块相对于肩胛盂偏外≥2 mm)。排除标准:① 翻修患者;② 关节松弛症者;③ 癫痫或有基础疾病者。2015 年 1 月—2016 年 11 月,共 18 例患者符合选择标准纳入研究。
1.2. 一般资料
本组男 12 例,女 6 例;年龄 19~37 岁,平均 26.2 岁。左肩 6 例,右肩 12 例。肩关节脱位 4~30 次,平均 8.8 次。病程 8~49 个月,平均 23.8 个月。肩胛盂前缘骨缺损 20%~29%,平均 25.2%。ISIS 评分 7~10 分,平均 7.6 分。肩关节退变 Samilson-Prieto 分级[14]:0 级 13 例,Ⅰ级 3 例,Ⅱ级 2 例。
1.3. 手术方法
手术均由同一组医师于 30° 关节镜下操作完成。全麻联合臂丛阻滞麻醉下,患者取沙滩椅位。
1.3.1. 喙突截取
于喙突尖端向下作长 2.5 cm 小切口,分离后暴露喙突,切断喙肩韧带与大部分胸小肌,喙突截骨长度 2 cm,喙突蒂长 4~5 cm。用摆锯新鲜化喙突底面后,于底面中心向上表面钻制直径 2.5 mm 骨道,上表面放置 Endobutton(施乐辉公司,美国),从 Endobutton 中央 2 孔穿入 3 条高强线并穿过喙突中央骨道,备用。在距喙突截骨端 3 mm 侧方钻制直径 1.5 mm 骨道(与喙突中央骨道垂直),放置防旋转线备用,必要时可以在联合腱根部放置 1 条牵引线。喙突修整完毕后,将喙突、喙突上预置的所有缝线置入套管并置入切口内。将该切口部分缝合关闭,作为前侧入路使用。
1.3.2. 肩胛下肌腱劈开与肩胛盂骨床准备
建立关节镜常规后侧入路并置入关节镜,在关节镜引导下建立前外侧入路,观察肩胛盂缺损及 Hill-Sachs 病变,清理肩袖间隙组织,保留不影响视野的关节囊和滑膜,用射频标记肩胛盂右肩 4∶00、左肩 8∶00 位置(相当于肩胛下肌腱上缘与肩胛盂缺损下缘中点)。
采用由后向前、由内向外方法劈开肩胛下肌腱。首先在肩关节中立位,于肩胛盂右肩 4∶30、左肩 8∶30 位置用射频劈开肩胛下肌腱后方关节囊、肌膜和肌腹,直达肩胛下肌腱前方肌膜并开一个小窗;于前侧入路置入交换棒,穿过肩胛下肌腱劈开的小窗并向上牵引肩胛下肌腱,将其放置在肩胛盂平面以保护内侧腋神经,用射频继续由内向外劈开肩胛下肌腱至宽 1.2 cm 即可。然后从前外侧入路置入关节镜,观察并新鲜化肩胛盂。
1.3.3. 肩胛盂骨道钻制、喙突转位与固定
于前外侧入路置入关节镜,后侧入路置入交换棒,放置特制的 8 mm 双筒定位器;在交换棒引导下,于标记的肩胛盂位置钻入 2.4 mm 导针,用 4.5 mm Endobutton 钻扩孔后穿入 PDS 导线,并将该导线经肩胛下肌腱裂口从前侧入路拉出,引导预先留置的喙突 Endobutton 3 条高强线及防旋转线经肩胛盂骨道从后侧入路拉出,并将喙突骨块经肩胛下肌腱拉入关节并贴合至肩胛盂。用防旋转线调节喙突位置,并用 Pushlock锚钉(锐适公司,美国)将其固定于右肩 3∶00、左肩 9∶00 位置,使喙突与肩胛盂紧密贴合,防止喙突旋转。最后从后侧入路观察移植骨块表面与肩胛盂的关系,关节囊无需再缝合处理。
1.4. 术后处理
术后采用肩关节外展 30°、外旋 0° 支具固定 6 周;2 周后开始肩关节被动钟摆锻炼;6 周去除支具后,在医师指导下进行主动康复训练,并逐渐恢复正常生活。术后 6 个月内避免肱二头肌腱主动大幅度锻炼。
1.5. 疗效评价指标
术前以及术后 6 个月、1 年及之后每年 1 次,对患者进行定期随访。
1.5.1. 临床疗效评估
观察患者运动水平恢复程度以及并发症发生情况,测量肩关节前屈、外展、外展 90° 外旋、0° 外旋和外展 90° 内旋活动度,采用疼痛视觉模拟评分(VAS)、美国肩肘外科协会评分(ASES)、Walch-Duplay 评分和 Rowe 评分,综合评估临床疗效。
1.5.2. 影像学评估
术后即刻行三维 CT 检查,其中在肩胛盂 En-face 面上观察移植骨块的中心位置,以右肩 3∶00~5∶00、左肩 7∶00~9∶00 为最佳位置,右肩高于 3∶00 表示过高、低于 5∶00 表示过低,左肩高于 9∶00 表示过高、低于 7∶00 表示过低[15];根据 Samim 等[16]提出的方法在 CT 肩胛盂横断面上观察移植骨块相对于肩胛盂位置。随访期间,采用肩胛骨前后位(肩关节切线位)X 线片联合三维 CT 观察肩关节间隙和骨赘增生情况,并参照 Samilson-Prieto 分级[14]评估肩关节退变情况;CT 观察移植骨块的塑形情况。
1.6. 统计学方法
采用 SPSS25.0 统计软件进行分析。数据以均数±标准差表示,手术前后比较采用配对 t 检验;检验水准 α=0.05。
2. 结果
2.1. 临床疗效评估
术后患者均获随访,随访时间 55~62 个月,平均 59.6 个月。术后均无血管神经损伤、感染、固定物和移植骨块相关并发症发生。患者均恢复正常生活,17 例(94.4%)重返运动且恢复伤前运动水平,其中 15 例(83.3%)可进行较术前更剧烈的运动。随访期间无肩关节脱位复发和翻修患者。
末次随访时,VAS 评分较术前明显降低,ASES 评分、Walch-Duplay 评分及 Rowe 评分明显提高,差异均有统计学意义(P<0.05)。见表 1。肩关节前屈、外展、外展 90° 外旋、0° 外旋和外展 90° 内旋活动度与术前比较,差异均无统计学意义(P>0.05)。见表 2。
表 1.
Comparison of effectiveness scores between pre- and post-operation (n=18,
 )
)
患者手术前后临床疗效评分比较(n=18,
 )
)
| 时间
Time |
VAS | ASES | Rowe | Walch-Duplay |
| 术前
Preoperative |
3.3±0.7 | 79.6±3.9 | 40.3±6.7 | 67.5±5.8 |
| 末次随访
Last follow-up |
1.0±0.7 | 92.6±3.2 | 93.3±2.4 | 94.3±3.0 |
| 统计值
Statistic |
t=20.968
P=0.000 |
t=–26.800
P=0.000 |
t=–46.007
P=0.000 |
t=–32.353
P=0.000 |
表 2.
Comparison of range of motion of should joint between pre- and post-operation (n=18,
 , °)
, °)
患者手术前后肩关节活动度比较(n=18,
 ,°)
,°)
| 时间
Time |
前屈
Forward flexion |
外展
Abduction |
外展 90° 外旋
Lateral rotation at 90° abduction |
0° 外旋
Lateral rotation at 0° |
外展 90° 内旋
Internal rotation at 90° abduction |
| 术前
Preoperative |
175.2±1.7 | 125.2±7.1 | 77.8±5.6 | 78.3±4.9 | 65.6±2.1 |
| 末次随访
Last follow-up |
174.9±2.2 | 124.7±7.8 | 77.2±6.1 | 78.0±5.3 | 65.3±2.7 |
| 统计值
Statistic |
t=2.051
P=0.056 |
t=1.932
P=0.070 |
t=1.944
P=0.069 |
t=1.844
P=0.083 |
t=2.062
P=0.055 |
2.2. 影像学评估
术后即刻三维 CT 显示所有移植骨块中心在肩胛盂 En-face 面上位于 3∶30~4∶30(右肩)或 7∶40~8∶20(左肩)位置,无移植骨块过高或过低。在 CT 横断面上,所有移植骨块相对于肩胛盂偏外 2.3~4.6 mm,平均 3.5 mm。
术后 36、48 个月及末次随访时,肩关节退变 Samilson-Prieto 分级与术前一致,均未进展。术后 24 个月移植骨块形态趋于稳定,在三维 CT 肩胛盂 En-face 面上显示塑形后的肩胛盂外形为与正常肩胛盂相近的正梨形,在 CT 横断面上显示为与肩胛盂齐平并形成与肱骨头圆形近似的弧形。末次随访时,肩胛盂外形与术后 24 个月比较无明显变化。见图 1。
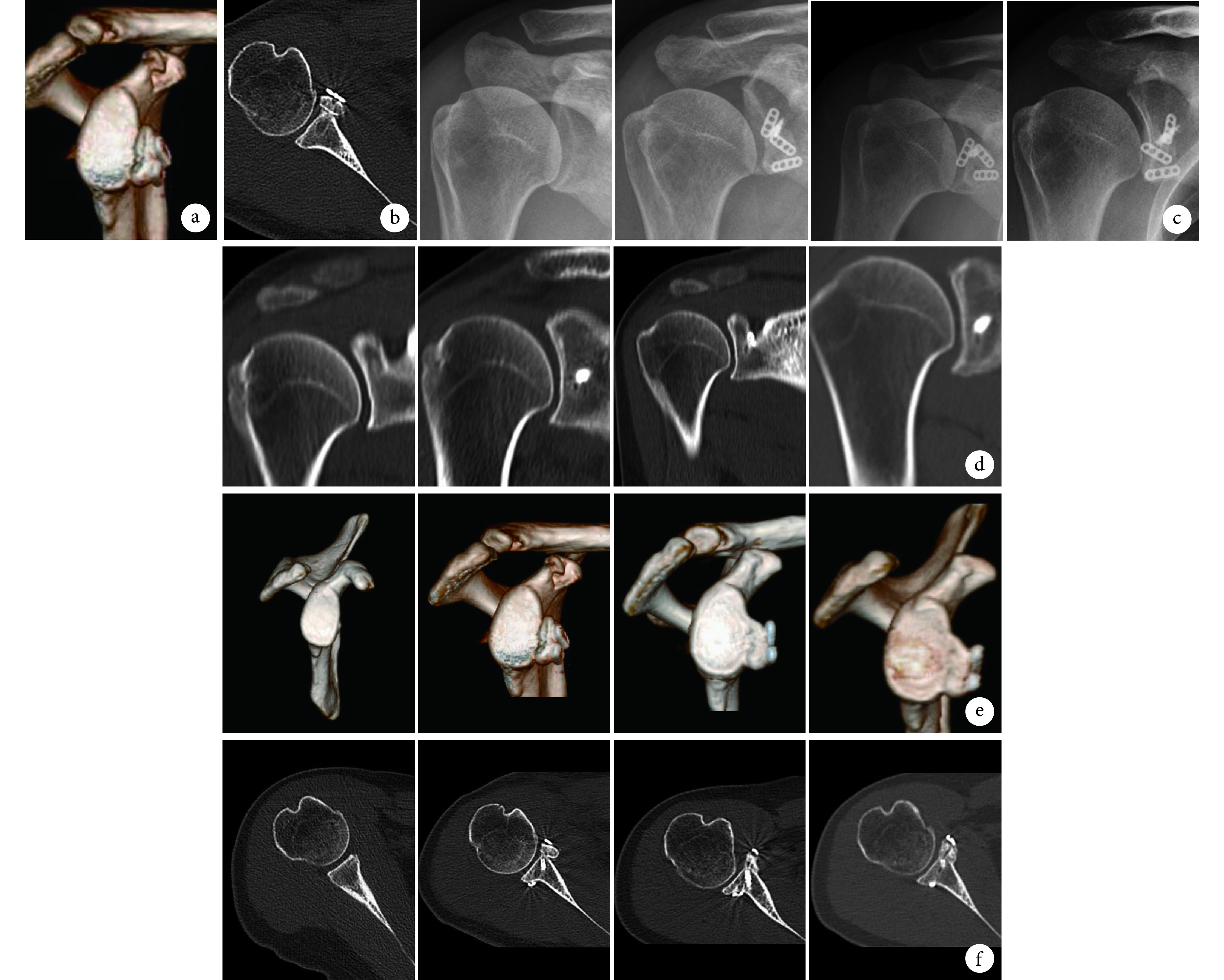
图 1.
A 37-year-old female patient with recurrent anterior dislocation of the right shoulder and an anterior glenoid bone defect of 24% of the glenoid surface
患者,女,37 岁,右侧肩关节复发性前脱位伴肩胛盂前缘骨缺损 24%
a. 术后即刻三维 CT 示移植骨块中心在肩胛盂 En-face 面上位于 3∶30 位置;b. 术后即刻 CT 示在肩胛盂横断面上移植骨块相对于肩胛盂偏外 2.5 mm;c、d. 肩关节 X 线片及三维 CT 示肩关节退变无进展 从左至右分别为术前及术后 36、48、60 个月;e、f. 三维 CT En-face 面和 CT 横断面示肩胛盂达正常形态 从左至右分别为术前及术后即刻、24、60 个月
a. Three-dimensional CT of the glenoid En-face view showed that the center of bone graft was at 3∶30 immediately after operation; b. CT of the cross-section view showed that the bone graft were positioned lateral to the glenoid rim with 2.5 mm immediately after operation; c, d. X-ray films and three-dimensional CT of the shoulder joint showed no progression of shoulder joint degeneration From left to right for preoperatively and 36, 48, and 60 months postoperatively, respectively; e, f. Three-dimensional CT of En-face and CT of cross-section views showed that the shape of scapular glenoid was normal From left to right for preoperatively and immediately, 24, and 60 months postoperatively, respectively
3. 讨论
3.1. 螺钉固定 Latarjet 手术中移植骨块偏外放置对肩关节退变的影响
Lädermann 等[17]对一组患者螺钉固定 Latarjet 手术后随访 16 年,在移植骨块位置不偏外的患者中有 30.4% 出现肩关节退变进展,而在移植骨块偏外放置的患者中该比例高达 82.4%。Kee 等[4]回顾性分析了 110 例接受螺钉固定 Latarjet 手术治疗的患者,经多元回归分析发现移植骨块偏外放置与术后肩关节退变进展显著相关。因此,有学者建议将骨块平行放置于与肩胛盂软骨面齐平或稍偏内侧的位置,以预防关节退变[9]。然而,由于技术操作偏差和关节镜下视觉差异,移植骨块位置偏外情况仍无法完全避免,引起术后肩关节退变加快的风险依旧存在。
大部分肩关节退变进展在术后远期才能观察到,但有研究发现部分患者在术后早中期即出现肩关节退变进展。Hovelius 等[9]的研究中术前 22 例患者有轻度关节退变,术后 2 年轻度关节退变患者增加至 26 例。Minkus 等[18]的研究中术前 8 例有关节退变,术后 27 个月关节退变患者增至 12 例,其中轻度 10 例、中度 2 例。Willemot 等[19]的研究也发现术后随访(43.7±27.7)个月时,肩关节退变进展率高达 34.6%。由此可见,在某些危险因素影响下,螺钉固定 Latarjet 手术后肩关节退变进展可提前到术后早中期发生。
3.2. 弹性固定 Latarjet 手术中移植骨块偏外放置对肩关节退变的影响
尽管移植骨块偏外放置是引起 Latarjet 手术后肩关节退变进展的显著危险因素,但我们前期研究发现[11, 13],在改良关节镜下弹性固定 Latarjet 手术中移植骨块偏外放置的患者,术后早期均未出现肩关节退变进展的影像学改变,而且骨块塑形效果更好。同时,本次研究发现直至术后中期,移植骨块偏外放置患者也未出现肩关节退变进展的影像学改变。分析可能有以下三方面原因:① 改良术式避免了引起术后肩关节退变进展的螺钉相关危险因素,继而降低相关风险。② 术后早期骨块未愈合前,弹性固定方式使偏外放置的移植骨块在受到肱骨头撞击时在肩胛盂附着处产生了微动,对肱骨头的撞击起到弹性缓冲作用,加上肱骨头软骨的韧性缓冲作用,减小了肱骨头和骨块的应力,最大程度降低了术后肩关节活动中的肱骨头软骨磨损,进一步降低引起肩关节退变进展的风险。③ 根据 Wolff 定律[20],骨骼生长会受到力学刺激影响而改变其外部形状和内部结构。正常肩胛盂外形近似正梨形,移植骨块位于肩胛盂正梨形范围内的部分受到肱骨头挤压应力较大,因此骨痂产生较多,而位于正梨形范围外的部分受到挤压应力较小甚至未受到挤压应力,因此骨痂产生较少,骨质发生废用性萎缩并吸收,从而导致移植骨块上半部分骨质吸收较多、位于肩胛盂正梨形范围内的骨质吸收较少,最终在 En-face 面上塑形成与正常肩胛盂相近的正梨形外形。同时,由于骨块偏外距离并不是太大,随着骨质愈合,骨块偏外部分逐渐被吸收或磨平,位于肱骨头活动轨迹外的骨质也被吸收,而位于肱骨头活动轨迹内的部分则良好塑形,最终骨块与肩胛盂骨质愈合并塑形至与肩胛盂齐平,同时形成符合肱骨头活动轨迹的与肱骨头圆形近似的弧形。骨块塑形稳定后,肱骨头在近似正常形态的肩胛盂内转动、滑动,不再与移植骨块撞击,降低了肱骨头撞击导致肩关节退变进展的风险。
综上述,改良关节镜下弹性固定 Latarjet 手术中移植骨块偏外放置在术后中期未出现肩关节退变加快的影像学改变。因此,我们建议在采用改良关节镜下弹性固定 Latarjet 手术时,移植骨块固定位置应偏外 3~5 mm,使骨块与肩胛盂的塑形更好,而且不增加肩关节退变进展的风险。
3.3. 本研究不足
① 本研究样本量及随访时间有限,本术式骨块偏外放置不引起肩关节退变进展的效果还需要长期随访来进一步证实。② 本研究并未与移植骨块齐平放置、偏内放置患者进行比较,偏外放置的临床效果、塑形效果、降低肩关节退变风险的有效性是否更优,仍需要更多随机对照试验来进一步证实。③ 本研究仅通过 CT 及 X 线片来评估术后肩关节退变情况,需进一步完善和采用更为精确的评估手段,如 MRI、关节镜检查等进行明确。④ 本研究的骨块塑形机制和未引起肩关节退变进展的原因需生物力学研究进一步证实。
作者贡献:覃其煌、梁新枝、陆伟参与实验设计;梁达强、梁新枝、李瑛参与实验实施;邓桢翰、丘志河、李盛、吴冰负责数据收集、统计分析;覃其煌负责文章撰写;李皓、柳海峰、陆伟对文章的知识性内容作批评性审阅。
利益冲突:所有作者声明,在课题研究和文章撰写过程中不存在利益冲突。课题经费支持没有影响文章观点和对研究数据客观结果的统计分析及其报道。
机构伦理问题:研究方案经深圳大学第一附属医院(深圳市第二人民医院)伦理委员会批准。
Funding Statement
广东省自然科学基金资助项目(2018A030313834)
Contributor Information
海峰 柳 (Haifeng LIU), Email: 819811255@qq.com.
伟 陆 (Wei LU), Email: 13922855513@139.com.
References
- 1.Hurley ET, Montgomery C, Jamal MS, et al Return to play after the Latarjet procedure for anterior shoulder instability: a systematic review. Am J Sports Med. 2019;47(12):3002–3008. doi: 10.1177/0363546519831005. [DOI] [PubMed] [Google Scholar]
- 2.Hurley ET, Jamal MS, Ali ZS, et al Long-term outcomes of the Latarjet procedure for anterior shoulder instability: a systematic review of studies at 10-year follow-up. J Shoulder Elbow Surg. 2019;28(2):e33–e39. doi: 10.1016/j.jse.2018.08.028. [DOI] [PubMed] [Google Scholar]
- 3.Gilat R, Lavoie-Gagne O, Haunschild ED, et al Outcomes of the Latarjet procedure with minimum 5- and 10-year follow-up: A systematic review. Shoulder Elbow. 2020;12(5):315–329. doi: 10.1177/1758573220945318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kee YM, Kim HJ, Kim JY, et al Glenohumeral arthritis after Latarjet procedure: Progression and it’s clinical significance. J Orthop Sci. 2017;22(5):846–851. doi: 10.1016/j.jos.2017.06.008. [DOI] [PubMed] [Google Scholar]
- 5.Vezeridis PS, Ishmael CR, Jones KJ, et al Glenohumeral dislocation arthropathy: etiology, diagnosis, and management. J Am Acad Orthop Surg. 2019;27(7):227–235. doi: 10.5435/JAAOS-D-17-00056. [DOI] [PubMed] [Google Scholar]
- 6.Filho JG, Leite MC, Borges ACW, et al Clinical and radiographic evaluation of patients operated by the Bristow-Latarjet technique with a minimum follow-up of 20 years. Rev Bras Ortop (Sao Paulo) 2020;55(4):455–462. doi: 10.1055/s-0039-3402455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Allain J, Goutallier D, Glorion C Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg (Am) 1998;80(6):841–852. doi: 10.2106/00004623-199806000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Balestro JC, Young A, Maccioni C, et al Graft osteolysis and recurrent instability after the Latarjet procedure performed with bioabsorbable screw fixation. J Shoulder Elbow Surg. 2015;24(5):711–718. doi: 10.1016/j.jse.2014.07.014. [DOI] [PubMed] [Google Scholar]
- 9.Hovelius L, Sandström B, Saebö M One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: study Ⅱ-the evolution of dislocation arthropathy. J Shoulder Elbow Surg. 2006;15(3):279–289. doi: 10.1016/j.jse.2005.09.014. [DOI] [PubMed] [Google Scholar]
- 10.Boileau P, Gendre P, Baba M, et al A guided surgical approach and novel fixation method for arthroscopic Latarjet. J Shoulder Elbow Surg. 2016;25(1):78–89. doi: 10.1016/j.jse.2015.06.001. [DOI] [PubMed] [Google Scholar]
- 11.Xu J, Liu H, Lu W, et al Clinical outcomes and radiologic assessment of a modified suture button arthroscopic Latarjet procedure. BMC Musculoskelet Disord. 2019;20(1):173. doi: 10.1186/s12891-019-2544-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Xu J, Liu H, Lu W, et al Modified arthroscopic Latarjet procedure: suture-button fixation achieves excellent remodeling at 3-year follow-up. Am J Sports Med. 2020;48(1):39–47. doi: 10.1177/0363546519887959. [DOI] [PubMed] [Google Scholar]
- 13.Boileau P, Saliken D, Gendre P, et al Arthroscopic Latarjet: suture-button fixation is a safe and reliable alternative to screw fixation. Arthroscopy. 2019;35(4):1050–1061. doi: 10.1016/j.arthro.2018.11.012. [DOI] [PubMed] [Google Scholar]
- 14.Samilson RL, Prieto V Dislocation arthropathy of the shoulder. J Bone Joint Surg (Am) 1983;65(4):456–460. doi: 10.2106/00004623-198365040-00005. [DOI] [PubMed] [Google Scholar]
- 15.Lafosse L, Boyle S, Gutierrez-Aramberri M, et al Arthroscopic latarjet procedure. Orthop Clin North Am. 2010;41(3):393–405. doi: 10.1016/j.ocl.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 16.Samim M, Small KM, Higgins LD Coracoid graft union: a quantitative assessment by computed tomography in primary and revision Latarjet procedure. J Shoulder Elbow Surg. 2018;27(8):1475–1482. doi: 10.1016/j.jse.2018.01.008. [DOI] [PubMed] [Google Scholar]
- 17.Lädermann A, Lubbeke A, Stern R, et al Risk factors for dislocation arthropathy after Latarjet procedure: a long-term study. Int Orthop. 2013;37(6):1093–1098. doi: 10.1007/s00264-013-1848-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Minkus M, Wolke J, Fischer P, et al Analysis of complication after open coracoid transfer as a revision surgery for failed soft tissue stabilization in recurrent anterior shoulder instability. Arch Orthop Trauma Surg. 2019;139(10):1435–1444. doi: 10.1007/s00402-019-03220-9. [DOI] [PubMed] [Google Scholar]
- 19.Willemot L, De Boey S, Van Tongel A, et al Analysis of failures after the Bristow-Latarjet procedure for recurrent shoulder instability. Int Orthop. 2019;43(8):1899–1907. doi: 10.1007/s00264-018-4105-6. [DOI] [PubMed] [Google Scholar]
- 20.Prendergast PJ, Huiskes R The biomechanics of Wolff’s law: recent advances. Ir J Med Sci. 1995;164(2):152–154. doi: 10.1007/BF02973285. [DOI] [PubMed] [Google Scholar]