

Abstract
Purpose
To present a safety-optimized ultrasound-guided minimal invasive carpal tunnel release (CTR) procedure.
Materials and Methods
104 patients (67 female, 37 male; mean age 60.6 ± 14.3 years, 95% CI 57.9 to 63.4 years) with clinical and electrophysiological verified typical carpal tunnel syndrome were referred for a high-resolution ultrasound of the median nerve and were then consecutively assigned for an ultrasound-guided CTR after exclusion of possible secondary causes of carpal tunnel syndrome such as tumors, tendovaginitis, ganglia and possible contraindications (e.g., crossing collateral vessels, nerve variations). Applying a newly adapted and optimized algorithm, basing on the work proposed by Petrover et al. CTR was performed using a button tip cannula which has several safety advantages: On the one hand, the button tip cannula acts as a blunt and atraumatic guiding splint for the subsequent insertion of the hook-knife, and on the other hands, it serves as a “hydro-inflation”-tool, i.e., a fluid-based expansion of the working-space is warranted during the whole procedure whenever needed.
Results
In all patients, successful releases were confirmed by the depiction of a completely transected transverse carpal ligament during and in the postoperative ultrasound-controls two weeks after intervention. All patients reported markedly reduction of symptoms promptly after this safety-optimized ultrasound-guided minimal invasive CTR and at the follow-up examination. No complications were evident.
Conclusion
The here proposed optimized algorithm assures a reliable and safe ultrasound-guided CTR and thus should be taken into account for this minimal invasive interventional procedure.
Supplementary Information
The online version contains supplementary material available at (10.1007/s00270-021-02789-2).
Keywords: Carpal tunnel syndrome, Minimal invasive carpal tunnel release, Ultrasound-guidance
Introduction
Carpal tunnel syndrome (CTS) is the most frequent compressive neuropathy, caused by compression of the median nerve at the level of the transverse carpal ligament (TCL) [1–3]. Diagnosis of CTS is mainly based on typical clinical symptoms, electrodiagnostic testing and high-resolution ultrasound (HRUS) [4].
In mild forms of CTS conservative treatment such as splint wearing at night, physiotherapy or steroid injections can initially be considered, whereas in severe forms or in patients with failed non-surgical treatment, carpal tunnel release (CTR) is indicated with patients showing an improvement in more than 90% [5, 6] of the cases.
Open CTR has been performed successfully for many years [7] with a trend, however, toward less-invasive procedures [7–11]. Over the recent years – most notably by Petrover et al. [8] – the safety and efficacy of real-time HRUS-guided minimally invasive CTR procedures have been demonstrated, leading to a lower invasiveness, less tissue trauma and a lower rate of procedural complications [8, 9, 12–15]. We hereby present a modified HRUS-guided minimally invasive CTR procedure utilizing as a novelty a blunt button tip cannula, which shows several advantages regarding procedural performance and median nerve safety.
Material and Methods
Demographics
One-hundred and four patients (67 female, 37 male; mean age 60.6 ± 14.3 years, 95% CI 57.9 to 63.4 years) were included. No patients had to be excluded due to anatomical variations (Table 1).
Table 1.
Demographic data and CTS findings
| Results | 95% CI$ | |
|---|---|---|
| Age | 60.6 ± 14.3 years | 57.9–63.4 years |
| Sex: male/female | 37/67 (37.6/64.4%) | – |
| Affected side: right | 60 (57.7%) | – |
| CTS severity | ||
| “mild” | 10 (12.1%) | – |
| “moderate” | 43 (51.8%) | – |
| “severe” | 30 (36.1%) | – |
| Median nerve CSA | 20.2 ± 5.4 mm2 | 19.0–21.3 mm2 |
| Wrist-to-forearm ratio | 2.1 ± 0.7 | 2.0–2.3 |
$Confidence interval
Carpal tunnel release procedures
All consecutive patients referred to our department for HRUS-guided CTR with clinically and electrophysiologically verified CTS and failed conservative treatment from December 2019 to October 2020 were included in this study. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Prior to the intervention all patients underwent HRUS-assessment to exclude possible anatomic contraindications (e.g., crossing collateral vessels, tumors) or nerve variations, such as Berrettini branches (anastomoses between the common digital nerves of the median and ulnar nerve) or Riche-Cannieu anastomoses (anastomoses between the thenar motor branch of the median nerve and the deep branch of the ulnar nerve) [16]. Median nerve cross-section areas (CSA) were measured to calculate the wrist-to-forearm ratio [17]. For the according written consent, a weighed explanation of the planned procedure including potential advantages and risks as well as the novel nature of the procedure was addressed.
Preoperative preparations
All patients were placed in a supine position with the respective arm extended at 90 degrees and the hand positioned supinated on a supporting cushion. Two belts were used to loosely fix the forearm and the extended fingers, respectively. Under strict aseptic conditions (with the intervening specialist wearing a mask, sterile gloves and a sterile gown) the patient’s arm was cleansed, and sterile drapes were used to cover the region. Using a Canon Aplio i800® system (Canon Medical Systems, Tokyo, Japan) with a linear 18L7 transducer (including a sterile transducer cover and sterile gel) the median nerve, ulnar artery and the superficial palmar arch were marked with a sterile marker on the skin defining thereby the safe release path— “safe zone”(15).
Interventional technique
Subcutaneous local anesthesia at the incision site (approx. 1.5 cm proximal to the dominant flexor crease of the ulnar sided wrist) with a 25G needle and 2 ml of 0.5% Carbostesin (Bucain®).
Hydrodissection of the median nerve with 5 ml of 0.5% Carbostesin (Bucain®) after insertion of a 21G needle into the perineural space from the ulnar aspect while scanning under real-time transaxial guidance.(Fig. 1).
Small incision (approximately 3 mm) of the skin and subcutaneous fascia at the intended entry point of the hook-knife (approx. 1.5 cm proximal to the dominant flexor crease of the ulnar sided wrist) by a sterile standard 11 mm disposable scalpel.
Advancement of a disposable button tip 16F metal cannula (Keysurgical®, Lensahn, Germany) longitudinally under HRUS-control through the safe zone up to the distal edge of the TCL (superficial palmar arch visible in this scan plane) (Fig. 2). The blunt button tip cannula serves as a guiding track and is swayed within the safe zone, to free the carpal tunnel (CT) from possible adhesions and guide the subsequent insertion of the knife.
Further injections of sterile physiologic saline through the button tip cannula to additionally widen the perineural safe zone just before inserting the hook-knife whenever necessary guaranteeing a sufficient widening of the safe zone during the whole dissection procedure.
Subsequent advancement of a hook-knife (Acufex® 3.0-mm hook-knife, Smith & Nephew PLC, London, England) parallel and ulnar to the button tip cannula with the cutting hook oriented ulnar, until the knife-tip reaches the level of the tip of the cannula (“dead end” of the safe procedure) (Figs. 3, 4), depicting a “Double-Dot Sign” in an axial scan plane within the safe zone deep to the TCL (Fig. 5).
The knife is then rotated under HRUS control and “hooks” the distal edge of the TCL – a transection of the TCL is subsequently achieved by continuously retracting the knife longitudinally under HRUS-vision(Fig. 6A).
Removal of the hook-knife after verification of the successful release by tilting the button tip cannula through the transected TLC (Fig. 6B).
Covering of the skin-incision with a band-aid (Steri-Strip®, 3 M Deutschland GmbH Health Care Business) and a compression bandage.
Fig. 1.
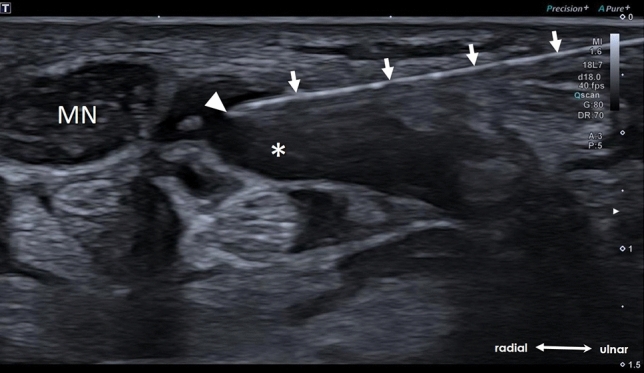
US-axial scan depicting the hydrodissection of the median nerve (MN) using a 21G needle (arrows) and the needle tip (arrowhead) within the “expanded” perineural space (asterisk)
Fig. 2.
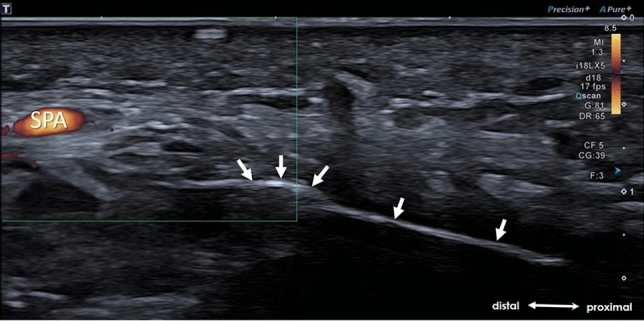
Longitudinal US-scan illustrating the positioning of the button tip cannula (arrows) at the distal reach of the safe zone. Superficial palmar arch (SPA)
Fig. 3.

Depiction of the hook-knife (Acufex® 3.0-mm hook-knife, Smith & Nephew PLC, London, England) (left) and the button tip cannula (Keysurgical®, Lensahn, Germany) (right)
Fig. 4.

A Anatomic specimen depicting the button tip cannula within the carpal tunnel. Median nerve (MN), ulnar nerve (UN), ulnar artery (UA), transverse carpal ligament (TCL), superficial palmar arch (SPA). B After insertion of the hook-knife ulnar to the button tip. C Position of the instruments within the carpal tunnel with a transected TCL. Note that the MN in this specimen shows marked enlargement typical in patients with CTS
Fig. 5.

A Longitudinal US-scan demonstrating the button tip cannula within (arrows) and the hook-knife (arrowheads) entering the carpal tunnel. B Axial US-scan depicting the “Double-Dot Sign” formed by cross-section of the button tip cannula (arrow) and the hook-knife (arrowhead). Median nerve (MN), ulnar artery (UA)
Fig. 6.

A Longitudinal US-scan illustrating the cutting of the TCL by retraction of the hook-knife (arrowheads). Hook (void arrowheads). The button tip cannula (arrows) which serves as a guiding tract, remains within the carpal tunnel during the whole release. B Axial US-scan depicting a successful release by “palpation” of the button tip cannula (arrow) through the transected TCL (dotted arrowheads). Median nerve (MN), ulnar artery (UA)
After the procedure, patients were advised to use their treated hand normally and to perform specific exercises, which were given to them immediately after the procedure.
Results
In all patients (n = 104, 100.0%), a technically successful CT-release could be documented on the basis of (a) a clearly HRUS-proven transected TLC and (b) the movement of the button tip cannula through the gap of the transected TCL. In all patients, 5 ml of physiologic saline was injected through the button tip cannula to widen initially the perineural safe zone. In 16 patients, additional 5 ml of saline was used to widen further a “narrow” perineural space just before inserting the hook-knife. In the postoperative HRUS controls two weeks after intervention (always done by an experienced nerve sonographer not engaged in the HRUS-guided procedure), a fully transected TCL was clearly defined and documented in each patient. Other than sparse hematoma at the incision site, no major complications (vascular or nerve injury) were evident. Applying a simplified Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) all patients reported a marked reduction of their specific symptoms promptly after CT-release and at the follow-up examination.
Discussion
Various studies have been published describing techniques for median nerve decompression by TCL release (5–15). In our study, a successful release was also demonstrated in all of our patients. Although not formally studied, an immediate reduction of their specific symptoms was additionally observed promptly after CT-release and during the follow-up examination. This positive effect with quick improvement of hand function and reduction of hand discomfort was also demonstrated in a recent study by Kamel et al. [18].
The technique described by Petrover et al. [8] was optimized in our study by initially inserting a button tip cannula prior to the hook-knife which offers clear advantages: On the one hand, a blunt cannula is used to widen the safe zone of the CT and to free it from possible adhesions and serves on the other hands as a guiding splint for the subsequent insertion of the hook-knife which enables a relative smooth insertion of the knife along the button tip cannula: this is especially in elderly patients with, e.g., arthritic changes and habitual radiocarpal extension a great advantage, as in such cases the hook-knife alone often deviates or slides below the median nerve with a greater risk of unintended nerve injury by repositioning. Additionally the button tip cannula serves as a clear marker indicating the most distal reach of the safe zone prior to the insertion of the knife avoiding thus any unintended injury of the superficial palmar arch artery when advancing the hook-knife beyond that point. A further advantage of the button tip cannula is the possibility of “hydro-inflating” the safe zone at any time during our CTR procedure if needed. Initially injected local anesthetics, displace within the CT: Due to the confined space and proximal and distal open nature of the CT, the injected fluid spreads and thus tunnel expansion decays gradually and rather prompt during the procedure, which might complicate the insertion of the hook-knife. This problem is minimized as additional saline can be injected at any time especially immediately before starting the cutting procedure itself. At the end of the procedure, documentation of a successfully transected TCL is mandatory and can be done by either moving the hook-knife through the transected TCL or as described by Petrover et al. [8] by secondarily injecting physiologic saline to distend and thus proof the released TCL or by introducing a cannula into the tunnel by a separate step to directly show the release by “HRUS-palpation”: Although the convex side of the hook-knife is blunt, the tip of the hook is spiky and may again unintendedly injure surrounding tissues by “palpating” the divided TCL. Thus, in our proposed algorithm, the explicit “procedure-success-control” can simply be done by using the atraumatic button tip cannula being still in place avoiding any unnecessary trauma.
Although the intention of our study was to describe this new modified algorithm which definitely optimizes the technique proposed by Petrover regarding procedural performance and safety, a limiting factor was the missing inclusion of a control group.
Conclusion
This proposed algorithm which is an evolution of a previously described technique by Petrover et al. [8] assures a reliable and safe ultrasound-guided CTR and thus should be considered when performing percutaneous HRUS-guided carpal tunnel release.
Supplementary Information
Funding
Open access funding provided by University of Innsbruck and Medical University of Innsbruck.. This study was not supported by any funding.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Information Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Alfonso C, Jann S, Massa R, Torreggiani A. Diagnosis, treatment and follow-up of the carpal tunnel syndrome: a review. NeurolSci. 2010;31(3):243–252. doi: 10.1007/s10072-009-0213-9. [DOI] [PubMed] [Google Scholar]
- 2.Nordstrom DL, DeStefano F, Vierkant RA, Layde PM. Incidence of diagnosed carpal tunnel syndrome in a general population. Epidemiology. 1998;9(3):342–345. doi: 10.1097/00001648-199805000-00021. [DOI] [PubMed] [Google Scholar]
- 3.Seror P. Sonography and electrodiagnosis in carpal tunnel syndrome diagnosis, an analysis of the literature. Eur J Radiol. 2008;67(1):146–152. doi: 10.1016/j.ejrad.2007.06.017. [DOI] [PubMed] [Google Scholar]
- 4.Kopf H, Loizides A, Mostbeck GH, Gruber H. Diagnostic sonography of peripheral nerves: indications, examination techniques and pathological findings. Ultraschall Med. 2011;32(3):242–263. doi: 10.1055/s-0031-1273309. [DOI] [PubMed] [Google Scholar]
- 5.Keith MW, Masear V, Amadio PC, Andary M, Barth RW, Graham B, Chung K, Maupin K, Watters WC, 3rd, Haralson RH, 3rd, Turkelson CM, Wies JL, McGowan R. Treatment of carpal tunnel syndrome. J Am AcadOrthopSurg. 2009;17(6):397–405. doi: 10.5435/00124635-200906000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Huisstede BM, Randsdorp MS, Coert JH, Glerum S, van Middelkoop M, Koes BW. Carpal tunnel syndrome. Part II: effectiveness of surgical treatments–a systematic review. Arch Phys Med Rehabil. 2010;91(7):1005–1024. doi: 10.1016/j.apmr.2010.03.023. [DOI] [PubMed] [Google Scholar]
- 7.Scholten RJ, Mink van der Molen A, Uitdehaag BM, Bouter LM, de Vet HC. Surgical treatment options for carpal tunnel syndrome. Cochrane Database Syst Rev. 2007 doi: 10.1002/14651858.CD003905.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Petrover D, Silvera J, De Baere T, Vigan M, Hakimé A. Percutaneous ultrasound-guided carpal tunnel release: study upon clinical efficacy and safety. CardiovascInterventRadiol. 2017;40(4):568–575. doi: 10.1007/s00270-016-1545-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Petrover D, Hakime A, Silvera J, Richette P, Nizard R. Ultrasound-guided surgery for carpal tunnel syndrome: a new interventional procedure. SeminInterventRadiol. 2018;35(4):248–254. doi: 10.1055/s-0038-1673360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sayegh ET, Strauch RJ. Open versus endoscopic carpal tunnel release: a meta-analysis of randomized controlled trials. ClinOrthopRelat Res. 2015;473(3):1120–1132. doi: 10.1007/s11999-014-3835-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vasiliadis HS, Nikolakopoulou A, Shrier I, Lunn MP, Brassington R, Scholten RJ, Salanti G. Endoscopic and open release similarly safe for the treatment of carpal tunnel syndrome. a systematic review and meta-analysis. PLoS ONE. 2015;10(12):e0143683. doi: 10.1371/journal.pone.0143683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Henning PT, Yang L, Awan T, Lueders D, Pourcho AM. Minimally invasive ultrasound-guided carpal tunnel release: preliminary clinical results. J Ultrasound Med. 2018;37(11):2699–2706. doi: 10.1002/jum.14618. [DOI] [PubMed] [Google Scholar]
- 13.Rojo-Manaute JM, Capa-Grasa A, Chana-Rodríguez F, Perez-Mañanes R, Rodriguez-Maruri G, Sanz-Ruiz P, Muñoz-Ledesma J, Aburto-Bernardo M, Esparragoza-Cabrera L, Cerro-Gutiérrez MD, Vaquero-Martín J. Ultra-minimally invasive ultrasound-guided carpal tunnel release: a randomized clinical trial. J Ultrasound Med. 2016;35(6):1149–1157. doi: 10.7863/ultra.15.07001. [DOI] [PubMed] [Google Scholar]
- 14.Guo XY, Xiong MX, Lu M, Cheng XQ, Wu YY, Chen SY, Chen K, Zhou QD, Wang L, Tan L, Quan JR, He FD, Chen Q. Ultrasound-guided needle release of the transverse carpal ligament with and without corticosteroid injection for the treatment of carpal tunnel syndrome. J OrthopSurg Res. 2018;13(1):69. doi: 10.1186/s13018-018-0771-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nakamichi K, Tachibana S, Yamamoto S, Ida M. Percutaneous carpal tunnel release compared with mini-open release using ultrasonographic guidance for both techniques. J Hand Surg Am. 2010;35(3):437–445. doi: 10.1016/j.jhsa.2009.12.016. [DOI] [PubMed] [Google Scholar]
- 16.Roy J, Henry BM, PĘkala PA, Vikse J, Saganiak K, Walocha JA, Tomaszewski KA, Median and ulnar nerve anastomoses in the upper limb: A meta-analysis. Muscle Nerve. 2016;54(1):36–47. doi: 10.1002/mus.24993. [DOI] [PubMed] [Google Scholar]
- 17.Hobson-Webb LD, Massey JM, Juel VC, Sanders DB. The ultrasonographic wrist-to-forearm median nerve area ratio in carpal tunnel syndrome. ClinNeurophysiol. 2008;119(6):1353–1357. doi: 10.1016/j.clinph.2008.01.101. [DOI] [PubMed] [Google Scholar]
- 18.Kamel SI, Freid B, Pomeranz C, Halpern EJ, de Nazarian LN. Minimally invasive ultrasound-guided carpal tunnel release improves long-term clinical outcomes in carpal tunnel syndrome. AJR Am J Roentgenol. 2020 doi: 10.2214/AJR.20.24383. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.