

Abstract
Background: Overseas imported cases of COVID-19 continue to increase in China, so we conducted this study to review the epidemiological characteristics of these patients.
Methods: From February 26 to April 4, 2020, the imported cases from abroad were enrolled in this study. The effect of prevention countermeasures in curbing the spread of COVID-19 was assessed in this study. Moreover, we defined incubation period and confirmed time as from the date of leaving the epicenter to date of symptom onset and date of final diagnosed, respectively, and the interval of symptom onset to final diagnosed time was defined as diagnostic time. Categorical variables were summarized as numbers and percentages, and the difference among the variables were analyzed.
Results: For 670 cases imported from abroad, 555 were Chinese and 115 were foreigners. Apparently, confirmed cases had significantly decreased after China was compelled to temporarily suspend the entry of foreign passport holders with valid visas or residence permits; 6 days after implement of controlled measures, the daily new confirmed cases were reduced to 13 cases. Moreover, about 84.3% of patients (166/197) presented symptoms 1 week after leaving the epicenter, and notably seven patients (3.6%) had symptoms 2 weeks after leaving the epicenter. The median incubation period was 3.0 days (inter quartile range, 1.0 to 6.0), the 95th percentile was 11.6 days. Additionally, most of cases (92.9%) were detected positively of nucleic acid after symptom onset with 4 days, the median diagnostic time was 2.0 days (interquartile range, 1.0 to 3.0), and the 95th percentile of the distribution was 5.0 days. Finally, about 5.8% of patients were healthy carriers, and the median confirmed time of asymptomatic patients was 4.0 days (interquartile range, 2.0 to 9.0). The following variables might be associated with confirmed time: symptom type (P = 0.005), exported regions (P < 0.001), and symptom onset time (P < 0.001).
Conclusions: The prevention countermeasures for imported cases implemented by the Chinese government played an indispensable role in curbing the spread of COVID-19; the time of departure from epicenter could provide an estimate of the incubation period; and a confirmed time, 2-week quarantine period might need to be prolonged, while asymptomatic patients should be closely monitored.
Keywords: COVID-19, global pandemic, imported case, epidemiological characteristics, prevention
Introduction
The coronavirus disease (COVID-19) (1) epidemic broken out in Wuhan City of China in December 2019, and it had spread rapidly around the world (2) due to economic globalization. Internationally, on March 11, the epidemic spread worldwide in 114 countries or regions, a total of 118,319 confirmed cases and 4,292 deaths worldwide (3) were reported by WHO. Under this situation, WHO announced COVID-19 as a global pandemic (4). In China mainland, the epidemic was controlled effectively, on March 27, 20 provinces or autonomous regions had reported no domestic cases for more than 4 weeks (5), and some regions of China reduced the public health emergency to Level Three Response (6, 7).
To our disappointment, on February 26, the first imported cases were reported in Ningxia Hui Autonomous Region of China, imported from Iran (8). Epidemic prevention and control measures to guard against imported cases were brought out by the authorities, such as all entering people received temperature test and home quarantine. With the increasing number of imported patients confirmed, on March 18, professor Zhong, a top Chinese epidemiologist, suggested that all entry population from epicenter should undergo nucleic acid testing (9), which resulted in a continuous increase in the number of imported cases, as on March 26, the new imported cases reached 54 cases (10). To more powerfully curb the spread of COVID-19, on March 28, China was compelled to temporarily suspend the entry of foreign passport holders with valid visas or residence permits (11).
Therefore, prevention and treatment measures for imported cases based on the epidemiological characteristics of imported cases can be formulated. However, for imported cases, most of them could not provide the definite exposure time, which was indispensable for infected disease. In real life study, it was important to utilize the available information to predict the outcome of the imported cases. So, we conducted this study to analyze the epidemiological characteristics of COVID-19 cases imported from abroad by using the available information.
Materials and Methods
Study Design
After strict prevention and treatment of COVID-19, on February 29, 20 provinces of China mainland announced no domestic COVID-19 cases (5). However, the confirmed cases outside of China continued to increase, and by March 11, WHO announced COVID-19 as a global pandemic (4). As a result, China's epidemic has reversed, changing from the exporting country to the importing one. The first imported case from Iran was reported on February 26, and China was compelled to temporarily suspend the entry of foreign passport holders with valid visas or residence permits on March 11 to curb the spread of COVID-19. The implementation date of critical public health prevention initiatives is displayed in Figure 1. This study was designed to review the epidemiological characteristics and outcomes of imported cases from abroad (from February 26 to April 4). The study was approved by the Review Board of the Air Force Medical University. Case enrollment needs to meet the following conditions: (1) imported from abroad; (2) underwent quarantine at designated places; (3) diagnosed by the results of nucleic acid test; and (4) adequate clinical information and available follow-up data.
Figure 1.
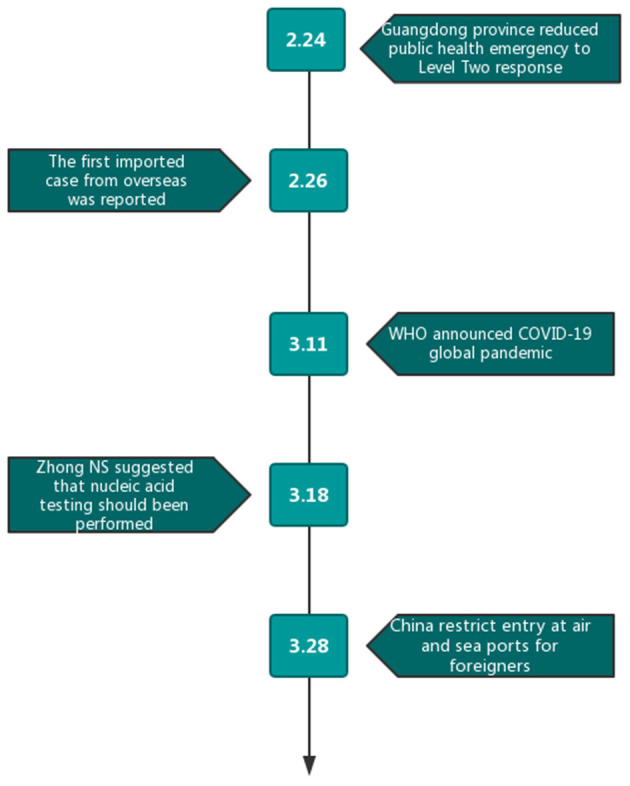
Date of occurrence of important events and implementation of preventive measures.
Data Collection
We collected the departure time and the country or region, the time of entry, symptoms, time of symptom onset, confirmed age and gender from the news reports and press releases reported by National Commission and Chinese Center for Diseases Control and Prevention. The degree of severity and diagnostic criteria refer to the 7th edition of the National New Coronavirus Pneumonia Diagnosis and Treatment Program. The data collection was performed by doctor Zhu, doctor Zhang, and doctor Jia, and any major disagreement among these three doctors was checked by the other two reviewers (doctor Xu and doctor Lei).
Statistical Analysis
Due to lack of definite exposure time, we defined incubation period as from the date of leaving epicenter to date of symptom onset, and the interval of symptom onset to final diagnosed time was defined as diagnostic time (12). We also defined confirmed time as from date of leaving epicenter to date of final diagnosis. The incubation period and diagnostic time were estimated by fitting a Weibull distribution on the date of leaving epicenter and symptom onset. Categorical variables were summarized as numbers and percentages. T test were performed to compare the differences of incubation period among groups, and when the cases were not normal data distribution, Mann-Whitney U test or Kruskal–Wallis H test was used. It was considered statistically significant that P < 0.05. SPSS 20.0 was used to finish the above analyses.
Results
Clinical Characteristics
As of April 4, 2020, 1 week after China suspended the entry of foreign passport holders with valid visas or residence permits (February 28, 2020), cumulative imported cases from abroad increased to 913 cases, with 11 domestic cases related to imported cases. Finally, a total of 670 imported cases (Chinese: 555 cases and foreigners: 115 cases) were enrolled in this study. Europe was the main exported area (59.4%), followed by North America (20.9%) and South America (1.2%) (Table 1). The distribution of cases in exported countries and entry province, autonomous region or municipality was shown in Figure 2, and we show that United Kingdom and United States were main exported countries, and the main imported cities were metropolises, such as Shanghai and Guangzhou. For these cases, 269 cases were male, 209 were female, and 192 cases were unknown. Among 458 patients with clear age information, the oldest patient was 71 years old, the youngest was only 2 months old, and the median age of the patients was 30 years. Figure 3 showed that patients aged between 20 and 49 years accounted for 69.2% (317/458); the main reason may be that a large proportion of the overseas imported cases were students studying abroad (32.8%). The detailed information of the patients is listed in Table 1.
Table 1.
Clinical characteristics of imported patients of COVID-19.
| Characteristics | Cases | Proportion |
|---|---|---|
| Age, (median: 30 years, range from 2 month to 71 years) | N (670) | (%) |
| Gender | (null: 192) | 28.7% |
| Male | 269 | 40.2% |
| Female | 209 | 31.2% |
| Agea | (null: 212) | 31.6% |
| <30 | 228 | 34.0% |
| ≥30 | 230 | 34.3% |
| Time of entry | ||
| Before the global explosion | 48 | 7.2% |
| Global explosion | 7 | 1.0% |
| After the global explosion | 615 | 91.8% |
| Nationality | ||
| Foreigner | 115 | 17.2% |
| Chinese | 555 | 82.8% |
| Region of cases exported | ||
| Asia | 100 | 14.9% |
| Africa | 24 | 3.6% |
| Europe | 398 | 59.4% |
| South America | 8 | 1.2% |
| North America | 140 | 20.9% |
| Occupation | ||
| International student | 220 | 32.8% |
| Non-international students | 450 | 67.2% |
| Symptoms | ||
| Fever | 107 | 16.0% |
| Respiratory symptoms | 65 | 9.7% |
| Gastrointestinal symptoms | 4 | 0.6% |
| Other symptom | 26 | 3.9% |
| Without symptom | 39 | 5.8% |
| Symptoms unknown | 429 | 64.0% |
Age: median age of all cases.
Figure 2.

Distribution of exported countries and distribution of imported provinces.
Figure 3.

Age distribution of imported cases from abroad.
Public Health Interventions
Since the first imported case from Iran was reported on February 26, China began to be concerned about the imported cases from abroad, with the reversal of domestic and foreign epidemics; on March 11, WHO announced COVID-19 as global pandemic. March 11 was an obvious watershed, the confirmed cases before and after were 28 cases and 642 cases, respectively. With the increase of confirmed cases, on March 18, Zhong Nanshan, a top Chinese epidemiologist, suggested that all entry population from epicenter should undergo nucleic acid testing, and 1 week after nucleic acid test was performed, the daily newly increased imported patients reached a peak with 50 cases. To more powerfully curb the spread of COVID-19, on March 28, China was compelled to temporarily suspend the entry of foreign passport holders with valid visas or residence permits. Apparently both arrived cases and confirmed cases had significant decreased, 6 days after implement of controlled measures, on April 4, and the daily new confirmed cases were reduced to 13 cases. The public health intervention events and related dynamic results are exhibited in Figure 4.
Figure 4.

Time distribution of confirmed cases from abroad.
Epidemiological Characteristics
For symptomatic patients, 37 cases had symptoms before departure, 17 patients had symptoms on the day of departure, and 180 patients had symptoms after leaving the epicenter. About 84.3% of patients (166/197) presented symptoms 1 week after leaving the epicenter, and 7 patients (3.6%) had symptoms 2 weeks after leaving the epicenter. Interesting, the peak of symptom onset emerged was on the first day (42 patients). Incubation period was estimated by fitting Weibull distribution, and patients who presented symptoms before departure had been excluded from the analysis. The median incubation period was 3.0 days (interquartile range, 1.0 to 6.0), and the 95th percentile was 11.6 days (Figure 5A). Moreover, cases exported from Africa presented symptoms later than patients exported from other regions (P = 0.007), which may due to the outbreak time varied in different regions (Table 2). Studies related to the incubation period are listed in Table 3.
Figure 5.

Estimation of incubation period and diagnostic time by fitting Weibull distribution. (A) Incubation period estimated on the date of leaving epicenter; (B) Diagnostic time were estimated on the date of symptom onset.
Table 2.
Epidemiological characteristics of symptomatic patients imported from abroad.
| Variable | Incubation period (days) | IQIb | P | Diagnostic time (days) | IQIb | P |
|---|---|---|---|---|---|---|
| In total (197) | 3.0 | (1.0, 6.0) | 2.0 | (1.0, 2.0) | ||
| Gender | 0.116 | 0.708 | ||||
| Male (87) | 4.0 | (2.0, 7.0) | 1.0 | (1.0, 2.0) | ||
| Female (80) | 3.0 | (1.0, 5.0) | 2.0 | (1.0, 2.0) | ||
| Agea | 0.749 | 0.017 | ||||
| <27 (77) | 4.0 | (2.0, 6.0) | 1.0 | (0.0, 2.0) | ||
| ≥27 (84) | 4.0 | (2.0, 6.0) | 2.0 | (1.0, 2.0) | ||
| Occupation | 0.570 | 0.044 | ||||
| International student (71) | 4.0 | (1.0, 6.0) | 1.0 | (1.0, 2.0) | ||
| Non-international students (126) | 3.0 | (1.0, 6.0) | 2.0 | (1.0, 2.25) | ||
| Symptoms | 0.067 | 0.307 | ||||
| Fever (89) | 4.0 | (2.0, 6.0) | 2.0 | (1.0, 2.0) | ||
| Respiratory symptoms (41) | 2.0 | (1.0, 6.0) | 1.0 | (1.0, 2.0) | ||
| Gastrointestinal symptoms (3) | 3.0 | (2.5, 3.0) | 1.0 | (1.0, 1.5) | ||
| Other symptom (17) | 4.0 | (1.0, 7.0) | 1.0 | (0.5, 2.0) | ||
| Symptoms unknown (47) | 1.0 | (1.0, 5.0) | 2.0 | (1.0, 2.0) | ||
| Nationality | 0.805 | 0.815 | ||||
| Foreigner (27) | 2.0 | (1.0, 8.0) | 1.0 | (1.0, 2.0) | ||
| Chinese (170) | 3.0 | (1.0, 6.0) | 2.0 | (1.0, 2.0) | ||
| Region of cases exported | 0.007 | 0.309 | ||||
| Asia (33) | 2.0 | (0.0,5.0) | 2.0 | (1.0, 3.0) | ||
| Africa (7) | 8.0 | (3.0,14.0) | 1.0 | (1.0, 2.0) | ||
| Europe (114) | 3.0 | (1.0,5.0) | 1.5 | (1.0, 2.0) | ||
| South America (3) | 5.0 | (5.0,5.5) | 1.0 | (1.0, 2.0) | ||
| North America (40) | 4.0 | (2.0,6.0) | 2.0 | (1.0, 3.0) |
Age, median age of symptomatic cases.
IQI, interquartile intervals.
Table 3.
Study list of incubation period of COVID-19 estimation.
| References | N | Distribution | Mean, days (95% CI) | Median, days (95% CI) | Percentiles |
|---|---|---|---|---|---|
| Zhang et al. (13) | 49 | Log-normal | 5.2 (1.8, 12.4) | - | 95th: 10.5 |
| Li et al. (14) | Null | Gamma | 7.2 (6.8, 7.6) | - | - |
| Leung et al. (15) | 175 | Weibull | (Travelers to Hubei) 1.8 (1.0, 2.7) (Non-travelers) 7.2 (6.1, 8.4) |
- | (Travelers to Hubei) 95th: 3.2 (Non-travelers) 95th: 14.6 |
| Qian et al. (16) | 262 | - | 6.7 | - | - |
| Ping et al. (17) | 758(93) | Log-normal | - | 8.06 (6.9, 9.4). | 95th: 21.9 |
| Qian et al. (16) | 91 | - | - | 6 (3.0, 8.0) | - |
| Wang et al. (18) | 483 | Logarithm normal | 7.4 | 7.0 | - |
| Lu et al. (19) | 265 | Weibull | 6.4 (5.3, 7.6) | - | 5th: 1.0 95th: 13.1 |
| Ki et al. (20) | 28 | - | 3.9 (0, 15.0) | 3.0 | - |
| Guan et al. (21) | 1,099 | - | - | 4.0 (2.0, 7.0) | - |
| Li et al. (14) | 10 | Log-normal | 5.2 (4.1, 7.0) | - | 95th:12.5(9.2, 18) |
| Backer et al. (22) | 88 | Weibull Gamma Lognormal |
6.4 (5.6, 7.7) 6.5 (5.6, 7.9) 6.8 (5.7, 8.8) |
- | 95th:10.3 (8.6, 14.1) 95th:11.3 (9.1, 15.7) 95th:13.3 (9.9, 20.5) |
| Lauer et al. (23) | 181 | Outside mainland China (n = 108). | - | 5.5 (4.4, 7.0) | 95th: (2.1, 14.7) |
| Lauer et al. (23) | 181 | Inside mainland China (n = 73) | - | 4.8 (4.2, 5.6) | 95th: (2.5, 9.2) |
| Lauer et al. (24) | 181 | Lognormal | - | 5.1 (4.5,5.8) | 97.5th: 11.5 (8.2,15.6) |
| Linton et al. (25) | Excluding Wuhan residents (n = 52) | Lognormal Weibull Gamma |
5.0 (4.2, 6.0) 5.4 (4.3, 6.6) 5.3(4.3, 6.6) |
4.3(3.5, 5.1) 4.7(3.6, 5.8) 4.7(3.8,5.7) |
95th:10.6 (8.5, 14.1) 95th:12.0 (9.8, 15.6) 95th:11.3 (9.2, 14.5) |
| Linton et al. (25) | Including Wuhan residents (n = 158). | Lognormal Weibull Gamma |
5.6 (5.0, 6.3) 5.8 (5.2, 6.5) 6.0 (5.3, 6.7) |
5.0(4.4, 5.6) 5.3(4.7, 6.0) 5.6(4.9, 6.4) |
95th:10.8 (9.3, 12.9) 95th:11.0 (9.6, 12.9) 95th:11.7 (10.3, 13.4) |
| Jing et al. (12) | 1,211 | Weibull | 8.6 (8.0, 9.23) | 8.1 (7.4, 8.9) | 90th:14.7 (14.0, 15.3) 99th:20.6(19.5, 21.6) |
| Han et al. (24) | 59 | Monte Carlo simulation | 5.8 | 5.0 | - |
Furthermore, we also researched the serial interval of symptom onset to final diagnosed (positive results of nucleic acid test). Two patients presented symptoms after final diagnosed; most cases (92.9%) were detected positively of nucleic acid after symptom onset with 4 days. For symptomatic patients, the median diagnostic time was 2.0 days (interquartile range, 1.0 to 3.0), the 95th percentile of the distribution was 5.0 days, it was showed in Figure 5B, furthermore, age and occupation were associated with diagnostic time (P = 0.017 and P = 0.044) (Table 2).
Finally, the median confirmed time of all patients was 4.0 days (interquartile range, 2.0 to 6.0). It was worth noting that about 5.8% patients were healthy carriers, and the median confirmed time of asymptomatic patients was 4.0 days (interquartile range, 2.0 to 9.0). Figure 6 showed that the peak of confirmed time was on the third day (139 cases); there were still 37 patients (5.5%) who were final diagnosed 2 weeks after leaving the epicenter. The following variables might be associated with confirmed time: symptom type (P = 0.005), exported regions (P < 0.001), and symptom onset time (P < 0.001) (Table 4).
Figure 6.

Distribution of confirmed time after confirmed cases leave the epidemic area.
Table 4.
Confirmed time of imported COVID-19 patients.
| Variable | Confirmed time (median, days) | IQIb | P |
|---|---|---|---|
| In total (670) | 4.0 | (2.0, 6.0) | |
| Gender | 0.776 | ||
| Male (269) | 4.0 | (2.0, 7.0) | |
| Female (209) | 4.0 | (2.0, 7.0) | |
| Agea | 0.281 | ||
| <30 (228) | 3.0 | (2.0, 6.0) | |
| ≥30 (230) | 4.0 | (2.0, 7.0) | |
| Occupation | 0.1 | ||
| International student (220) | 4.0 | (3.0, 6.0) | |
| Non-international students (450) | 4.0 | (2.0, 6.25) | |
| Symptoms | 0.005 | ||
| Fever (107) | 5.0 | (3.0, 8.0) | |
| Respiratory symptoms (65) | 3.0 | (2.0, 6.0) | |
| Gastrointestinal symptoms (4) | 4.0 | (3.25, 4.75) | |
| Other symptom (26) | 3.0 | (2.0, 5.5) | |
| Without symptom (39) | 4.0 | (2.0, 9.0) | |
| Symptoms unknown (429) | 4.0 | (3.0, 6.0) | |
| Nationality | 0.066 | ||
| Foreigner (115) | 4.0 | (3.0, 8.0) | |
| Chinese (555) | 4.0 | (2.0, 6.0) | |
| Region of cases exported | <0.001 | ||
| Asia (100) | 4.0 | (2.0, 7.0) | |
| Africa (24) | 8.0 | (4.25, 13.75) | |
| Europe (398) | 3.0 | (2.0, 5.0) | |
| South America (8) | 8.5 | (7.25, 9.75) | |
| North America (140) | 4.0 | (3.0, 7.0) | |
| Symptoms onset | <0.001 | ||
| Symptom onset is clear (234) | 4.0 | (3.0, 7.0) | |
| Symptoms during isolation (79) | 6.0 | (4.0, 8.0) | |
| Asymptomatic (39) | 4.0 | (2.0, 9.0) | |
| Unknown time of symptoms (318) | 3.0 | (2.0, 5.0) |
Age, median age of all cases.
IQI, interquartile intervals.
Discussion
With the global outbreak of COVID-19, the confirmed cases and deaths continue to rise globally (26–29). In China, the domestic epidemic was controlled effectively but the challenge of cross-border COVID-19 transmissions emerged. To our knowledge, this study is the first designed to review the epidemiological characteristics of COVID-19 cases imported from abroad in China. Most of them were exported from Europe and North American, which might be related with the economic and academic exchanges between China and these regions.
Internationally, according to statistics, about 145 million tourists traveled to China from abroad in 2019 (30), and most of them came from Europe and North America. We also know that Europe and North America were the most popular areas for Chinese students (31). The distribution of exported regions of COVID-19 was associated with above data, and in this study, about 74.3% cases came from Europe and North America and nearly one-third of exported cases were Chinese overseas students. As exported country, previous studies have shown most cases from China had spread to Asian neighbors, followed by Europe (32). In our study, although there were few cases (4.8%) exported from Africa and South America, the imported cases in these two regions could not be ignored. On February 26, the first imported case from Iran was reported; after that, the confirmed increased steadily, as on March 11, COVID-19 was defined as a global pandemic, and the imported cases increased sharply.
Incubation period, from the earliest exposure time to the time of symptoms onset, was necessary for preventing and controlling the epidemic, so numerous studies were focused on this issue. The median incubation period was ranged from 3.9 days to 8.6 days due to the different definition of exposure time (13, 14, 16–19, 21–25, 33, 34). However, in a real world study, most patients could not provide the specific exposure time. It was significant to estimate the incubation period by using the available information. Jing et al. (12) estimated the median incubation period of COVID-19 was 8.13 days (95% CI: 7.37–8.91), and they defined it as from the time of departure from Wuhan City to the symptom onset by using the well-known renewal theory in probability. For the imported cases, preventive measures were formulated based on the incubation period; unfortunately, we could not obtain the definite exposure time, and we supposed that the time of leaving epicenter could predict the progression of COVID-19. In this study, we found that the median incubation of the imported COVID-19 cases was 3.0 days (interquartile range, 1.0 to 6.0) after they leaving the epicenter, shorter than the previous study. The following reasons can explain its short incubation period: a minority of them were infected on the way to China, or the mutations in the novel coronavirus (35). Notably, there were still 3.6% of patients who had symptom 2 weeks after leaving the epicenter, which indicated that the 2-week quarantine period might need to be prolonged. The outbreak of sporadic epidemics since mid-2020 were related to the onset of imported cases after the 2-week quarantine period; therefore, the Chinese government had formulated a 2-week plus 7-day quarantine policy for overseas cases.
We also explored the optimal nucleic acid detection time for imported cases in this study. For the symptomatic patients, the median diagnostic time was 2.0 days after they presented symptoms. A study from South Korea (20) showed that the median of symptom-onset to diagnosis was 5.2 days, the longest time of symptom-onset to diagnosis was 16.0 days reported by Xiao, and a total of 301 patients were analyzed (36). In this study, the positive results of nucleic acid test were detected earlier than the related studies, which might be due to that all inbound population from epicenter were suggested to underwent nucleic acid test when they arrived in China.
Moreover, our experience of fighting the COVID-19 indicated that public health intervention could reduce its transmission (37). The public health intervention, including strictly enforced segregation and travel bans, entry screening, suspension of public transportation in the city, closure of entertainment venues, and bans on public gatherings, played an important role in controlling the epidemic (38–40). One study proved that the Wuhan City shutdown delayed the spread of COVID-19 to other cities for 2.91days (95% CI: 2.54–3.29) (39). Therefore, on March 28 (11), China was compelled to temporarily suspend the entry of foreign passport holders with valid visas or residence permits. Apparently both arrived cases and confirmed cases had significantly decreased.
Finally, with asymptomatic patients, because the condition was hidden and might be contagious, we should be more vigilant. In our study, 39 asymptomatic patients were detected during their quarantine. A study about a health carrier from Wuhan caused widespread concern, she transmitted new coronavirus to her five family relatives, but she did not present any symptoms during her disease course (41). A series of subsequent studies confirmed that asymptomatic patients were infectious (42–45). The median of confirmed of asymptomatic patients was 4.0 days, basically consistent with symptomatic patients. Therefore, nucleic acid testing of all immigrants was essential for screening asymptomatic patients.
The shortcoming of this study was that the retrospective study did not include all people returning from overseas (243 cases were lost), so it could not represent the epidemiological characteristics of all imported confirmed cases; secondly, we estimated the incubation period for COVID-19; the departure time from the epidemic area was recognized as the exposure time, which may lead to a reduction in the real incubation period. Third, we could not quantify that interventions had multiple indirect effects on changes in human behavior. Finally, most patients were still in hospital, so the clinical outcomes had not been analyzed.
It is important to plan for the early stages of imported cases from overseas during a pandemic to avoid a national outbreak. In this study, we investigated the epidemiological characteristics of COVID-19 imported from overseas and observed interventions implemented by the government. We found that the departure time from epicenter could be used to predict the progression of the COVID-19. Promulgation of a ban on entry, a combination of quarantine, and quarantine methods was effective. For imported cases, the 2-week quarantine period might need to be prolonged and asymptomatic patients should be closely monitored.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Tangdu Hospital. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
TJ, JZha, and WuW participated in study design and study conception. JZhu, QZ, CJ, SX, JL, HW, and ZZ performed data analysis. JZhu, QZ, CJ, SX, JC, YX, WeW, XW, and MW recruited patients. JZhu, QZ, CJ, WuW, and JC drafted the manuscript. All authors provided critical review of the manuscript and approved the final draft for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
Funding. This research was supported by grants from the Wu Jieping Medical Foundation (320.6750.17527) and the Provincial Key R & D Program of Shaanxi (2017ZDCXL-SF-01-04-01).
References
- 1.Novel Coronavirus–China. (2020). Available online at: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed January 12, 2020).
- 2.Hui DS, Azhar EI, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health-The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. (2020) 91:264–6. 10.1016/j.ijid.2020.01.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Coronavirus Disease (COVID-2019) Situation. Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed March 11, 2020).
- 4.Coronavirus Outbreak is a Pandemic, Says WHO. Available online at: https://www.who.int/zh/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020 (accessed March 11, 2020).
- 5.China Daily in March 28, 2020. Available online at: https://www.chinadaily.com.cn/a/202003/28/WS5e7f2ba6a310128217282b8c.html (accessed March 28, 2020).
- 6.Chongqing Center for Disease Control and Prevention. Available online at: http://www.cqcdc.org/html/content/20/03/4617.shtml (accessed March 25, 2020).
- 7.Shanxi Provincial Center for Disease Control and Prevention. Avavailble online at: http://www.sxcdc.cn/Article/20196.html (accessed March 10, 2020).
- 8.The Confirmed Cases of Imported New Coronary Pneumonia in Ningxia were Isolated After Arriving in Zhongwei City, and Have Been Intensively Treated on the 26th. Available online at: https://wap.peopleapp.com/article/5208841/5110610 (accessed February 26, 2020).
- 9.Press Conference of Guangzhou Municipal Government. Available online at: http://www.gz.gov.cn/zt/gzsrmzfxwfbh/fbt/content/post_5744314.html (accessed March 18, 2020).
- 10.National Health Commission of the People's Republic of China. Available online at: http://www.nhc.gov.cn/xcs/yqtb/202003/c521093a01734df3b3fbc156064ba19f.shtml (accessed March 27, 2020).
- 11.People's Republic of China Ministry of Foreign Affairs. Available online at: https://www.mfa.gov.cn/web/zyxw/t1761858.shtml (accessed March 26, 2020).
- 12.Jing Q, You C, Lin QS, Hu TJ, Yu SC, Zhou XH, et al. Estimation of incubation period distribution of COVID-19 using disease onset forward time: a novel cross-sectional and forward follow-up study. Sci Adv. (2020). 6:c1202. 10.1126/sciadv.abc1202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhang JJ, Litvinova M, Wang W, Wang Y, Deng XW, Chen XH, et al. Evolving epidemiology and transmission dynamics of coronavirus disease 2019 outside Hubei province, China: a descriptive and modelling study. Lancet Infect Dis. (2020) 20:93–802. 10.1016/S1473-3099(20)30230-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li Q, Guan X, Wu P, Wang XY, Zhou L, Tong YQ, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. (2020) 382:1199–207. 10.1056/NEJMoa2001316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leung C. The difference in the incubation period of 2019 novel coronavirus (SARS-CoV-2) infection between travelers to Hubei and nontravelers: the need for a longer quarantine period. Infect Control Hosp Epidemiol. (2020) 41:594–6. 10.1017/ice.2020.81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Qian GQ, Yang NB, Ding F, Ma AHY, Wang ZY, Shen YF, et al. Epidemiologic and clinical characteristics of 91 hospitalized patients with COVID-19 in Zhejiang, China: a retrospective, multi-centre case series. QJM. (2020) 113:474–81. 10.1093/qjmed/hcaa089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ping KK, Lei MY, Gou Y. Epidemiologic characteristics of COVID-19 in Guizhou, China. J Infect Dev Ctries. (2021). 15:389–97. 10.3855/jidc.12818 [DOI] [PubMed] [Google Scholar]
- 18.Wang P, Lu J-a, Jin Y, Zhu M, Wang L, Chen S. Statistical and network analysis of 1212 COVID-19 patients in Henan, China. Int J Infect Dis. (2020) 95:391–8. 10.1016/j.ijid.2020.04.051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lu HZ, Ai JW, Shen YZ, Li Y, Li T, Zhou X, et al. A descriptive study of the impact of diseases control and prevention on the epidemics dynamics and clinical features of SARS-CoV-2 outbreak in Shanghai, lessons learned for metropolis epidemics prevention. medRxiv [Preprint]. (2020). 10.1101/2020.02.19.20025031 [DOI] [Google Scholar]
- 20.Ki M. Task Force for-nCo V Epidemiologic characteristics of early cases with 2019 novel coronavirus(2019-nCoV) disease in Korea. Epidemiol Health. (2020) 42:e2020007. 10.4178/epih.e2020007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. 10.1056/NEJMoa2002032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus(2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill. (2020) 25:2000062. 10.2807/1560-7917.ES.2020.25.5.2000062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng QL, Meredith HR, et al. The incubation period of coronavirus disease 2019(COVID-19)from publicly reported confirmed cases: estimation and application. Ann Intern Med. (2020) 172:577–82. 10.7326/M20-0504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Han H. Exploring the association between compliance with measures to prevent the spread of COVID-19 and big five traits with Bayesian generalized linear model. Pers Individ Dif. (2021) 176:110787. 10.1016/j.paid.2021.110787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Linton NM, Kobayashi T, Yang Y, Hayashi K, Akhmetzhanov AR, Jung S, et al. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: a statistical analysis of publicly available case data. J Clin Med. (2020) 9:538. 10.3390/jcm9020538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhao S, Zhuang Z, Cao P, Cao PH, Ran JJ, Gao DZ, et al. Quantifying the association between domestic travel and the exportation of novel coronavirus(2019-nCoV)cases from Wuhan, China in 2020: a correlational analysis. J Travel Med. (2020) 27:taaa022. 10.1093/jtm/taaa022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bogoch, II, Watts A, Thomas-Bachli A, Huber C, Kraemer M, Khan K, et al. Pneumonia of unknown aetiology in Wuhan, China: potential for international spread via commercial air travel. J Travel Med. (2020) 27:taaa008. 10.1093/jtm/taaa008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wu JT, Leung K, Leung GM. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. Lancet. (2020) 395:689–97. 10.1016/S0140-6736(20)30260-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Findlater A, Bogoch, II. Human mobility and the global spread of infectious diseases: a focus on air travel. Trends Parasitol. (2018) 34:772–83. 10.1016/j.pt.2018.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Basic Situation of the Tourism Market in 2019. Available online at: https://mp.weixin.qq.com/s/VQ4VVeV-rmiZoq8oAUWN9Q (accessed March 10, 2020).
- 31.Overseas Chinese Students. Available online at: http://zz.sll.cn/news/01083742.html (accessed October 31, 2019).
- 32.Haider N, Yavlinsky A, Simons D, Osman AY, Ntoumi F, Zumla A, et al. Passengers' destinations from China: low risk of Novel Coronavirus (2019-nCoV)transmission into Africa and South America. Epidemiol Infect. (2020) 148:e41. 10.1017/S0950268820000424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Li ML, Chen P, Yuan QQ. Transmission characteristics of the COVID-19 outbreak in China: a study driven by data. medRxiv. (2020). 32834640 [Google Scholar]
- 34.Tian S, Hu N, Lou J, Chen K, Kang XQ, Xiang ZJ, et al. Characteristics of COVID-19 infection in Beijing. J Infect. (2020) 80:401–6. 10.1016/j.jinf.2020.02.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Forster P, Forster L, Renfrew C, Forster M. Phylogenetic network analysis of SARS-CoV-2 genomes. Proc Natl Acad Sci USA. (2020) 117:9241–3. 10.1073/pnas.2004999117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Xiao AT. Tong YX, Gao C. Dynamic profile of RT-PCR findings from 301 COVID-19 patients in Wuhan, China: a descriptive study. SSRN. (2020)127:104346. 10.2139/ssrn.3548769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Iwata K, Miyakoshi C. A simulation on potential secondary spread of novel coronavirus in an exported country using a stochastic epidemic SEIR model. J Clin Med. (2020) 9:E944. 10.3390/jcm9040944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Boldog P, Tekeli T, Vizi Z, Dénes A, Bartha FA, Röst G. Risk assessment of novel coronavirus COVID-19 outbreaks outside China. J Clin Med. (2020) 9:571. 10.3390/jcm9020571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tian H, Liu Y, Li Y, Wu C, Chen B, Kraemer M, et al. An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science. (2020) 368:638–42. 10.1126/science.abb6105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Zhou XK, Wu ZG, Yu RR, Cao SN, Fang W, Jiang Z, et al. Modelling-based evaluation of the effect of quarantine control by the Chinese government in the coronavirus disease 2019 outbreak. Sci China Life Sci. (2020) 63:1–4. 10.1007/s11427-020-1717-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. (2020) 323:1406–7. 10.1001/jama.2020.2565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Wolfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. (2020) 581:465–9. 10.1038/s41586-020-2196-x [DOI] [PubMed] [Google Scholar]
- 43.Lai CC, Liu YH, Wang CY, Wang Y-H, Hsueh S-C, Yen M-Y, et al. Asymptomatic carrier state, acute respiratory disease, and pneumonia due to severe acute respiratory syndrome coronavirus 2(SARS-CoV-2): facts and myths. J Microbiol Immunol Infect. (2020) 53:404–12. 10.1016/j.jmii.2020.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Huang R, Xia J, Chen YX, Wang YH, Hsueh SC, Yen M, et al. A family cluster of SARS-CoV-2 infection involving 11 patients in Nanjing, China. Lancet Infect Dis. (2020) 20:534–5. 10.1016/S1473-3099(20)30147-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. (2020) 382:970–1. 10.1056/NEJMc2001468 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.