

Abstract
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic, affecting all the individuals across the planet. COVID-19 has gained significant attention due to its high prevalence among individuals with diabetes, nonalcoholic fatty liver disease (NAFLD), and metabolic syndrome. NAFLD is the hepatic manifestation of metabolic syndrome and can be associated with a high risk of developing type 2 diabetes. The association of COVID-19 and NAFLD has also gained more attention because NAFLD is highly associated with the epidemic of obesity. NAFLD is a potential risk factor for SARS-CoV-2 infection and severe COVID-19, independent of metabolic syndrome. Importantly, it is not yet clear whether the epidemics of obesity and NAFLD have perpetuated the current pandemic of COVID-19. Further research is urgently needed to assess the following: (1) Whether NAFLD is a high risk factor for SARS-CoV-2 infection; (2) Whether NAFLD is associated with the severe form of COVID-19; and (3) Whether the presence of NAFLD can explain the racial variation in the morbidity and mortality associated with COVID-19. This review summarizes the interactions between COVID-19 and NAFLD, mechanism of liver injury by COVID-19, and effect of lockdown due to COVID- 19 on patients with NAFLD.
Keywords: Fatty liver, COVID-19, Diabetes, Obesity, Pandemic
Core Tip: Earlier studies suggested that individuals most vulnerable to severe acute respiratory syndrome coronavirus 2 infection suffer from pre-existing disease, including nonalcoholic fatty liver disease (NAFLD). There is an interwoven relationship between NAFLD and the associated high-risk factors for coronavirus disease 2019 (COVID-19). NAFLD can increase risk of infection, lung injury, cardiac impairment, and difficulty with respiratory ventilation, and can be associated with higher risk for COVID-19, especially in the presence of liver fibrosis. The association between high production of interleukin-6 in both NAFLD and COVID-19 merits further research to determine whether NAFLD is directly involved in the cytokine storms.
INTRODUCTION
Coronavirus outbreak caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)[1] led to the unprecedented spread of the novel coronavirus disease 2019 (COVID-19). COVID-19 has become a global pandemic and a serious threat to human life and economy[2]. SARS-CoV-2 is transmitted by droplet means and displays a higher fatality rate in elderly and immunocompromised individuals[3]. COVID-19 has gained significant attention worldwide due to its high fatality rate. Earlier studies suggested that individuals suffering from pre-existing disease, including metabolic syndrome (MetS) and nonalcoholic fatty liver disease (NAFLD), are at greater risk of developing COVID-19.
NAFLD is a worldwide growing chronic pandemic and considered a part of MetS. NAFLD is also a risk factor for SARS-CoV-2 infection[4] and severe COVID-19, independent of MetS[5]. Bats are believed to be the origin of SARS-CoV-2 because the SARS-CoV-2 genome is 88% identical to the SARS-CoV genome derived from bat[6]. Pangolin is likely to be the intermediate mammalian host for SARS-CoV-2 because the genome of pangolin-CoV is 91% similar to the SARS-CoV-2 genome[7]. However, transmission of SARS-CoV-2 from pangolin to human is debatable. Most of the individuals infected are asymptomatic[8]. The typical presentation of COVID-19 is mild to severe pneumonia. However, COVID-19 can affect all the systems of the human body, causing myocarditis, heart failure, acute kidney injury, hypoxic encephalopathy, sepsis, multi-organ failure, and even death[9].
In the initial stage of COVID-19, the viral proteins bind to angiotensin converting enzyme 2 (ACE2) receptors to allow the entry of the viral contents into the host cells. ACE2 receptors are present in the nasopharyngeal epithelium, which is the main site of viral replication, type II alveolar epithelial cells, endothelium of the blood vessels, stomach epithelial cells, the brush border of intestinal enterocytes, colon colonocytes, renal proximal tubules, and cholangiocytes of the liver[10]. Binding of the viral proteins to ACE2 receptors in the stomach and the intestine can lead to malabsorption of food and disturbance in intestinal juice and enteric nervous system activation, evoking diarrhea and digestive system symptoms[11]. SARS-CoV-2 can cause liver damage directly by replication in hepatic cells or indirectly by inducing inflammatory response, causing hypoxia and ischemia of the liver through influencing pre-existing liver disease and drug-related injury of the liver[12].
This review summarizes the interactions between COVID-19 and NAFLD, mechanism of liver injury by COVID-19, and effect of lockdown due to COVID-19 on patients with NAFLD.
NAFLD
NAFLD is a worldwide growing epidemic caused by insulin resistance and obesity, leading to collection of triglycerides and free fatty acids in the liver, and can be associated with greater risk for cardiovascular and liver-related mortality. NAFLD has become an important indication for liver transplantation[13]. The spectrum of NAFLD encompasses conditions ranging from simple accumulation of fat (> 5% of the hepatic parenchyma without injury to hepatocytes) in the liver to more progressive steatosis with associated fibrosis, cirrhosis, hepatitis, and hepatocellular carcinoma in the absence of excess intake of alcohol. NAFLD is composed of nonalcoholic fatty liver and nonalcoholic steatohepatitis (NASH; the necroinflammatory process causing injury of the hepatic cells)[14,15]. A group of experts who aimed to provide more accurate terminology to reflect the pathogenesis and aid in management of patients reached consensus that the term “NAFLD” does not reflect the current knowledge and proposed metabolic (dysfunction) associated fatty liver disease most appropriately[16].
Most of the patients with NAFLD have both insulin resistance and obesity that play a key role in the pathogenesis of MetS[17,18]. Thus, NAFLD is considered to be the liver manifestation of MetS. MetS is defined as a group of metabolic abnormalities including central obesity, hypertension, hyperglycemia, and dyslipidemia that increase risk of cardiovascular disease, stroke, and type 2 diabetes[19]. MetS affects more than one-fifth of the population in the United States, and is very common in both Mexican Americans and African Americans, affecting women more than men in the two latter ethnic groups. Caucasian women and men are affected equally. The prevalence of MetS is highest among Mexican Americans, followed by African Americans and Caucasians. With regard to the components of MetS, insulin resistance is the most common in Hispanics, with hypertension being the most common in African-Americans and atherogenic dyslipidemia in White people[20]. MetS affects about 25% of the people in Europe. The prevalence of the disease is low in Southeast Asia, but it is rising towards the rates of Europe and United States and high in the Middle East and sub-Saharan Africa[21].
NAFLD prevalence is estimated to be about 20%-30% in the Western world and 5%-18% in Asian countries. The prevalence of NAFLD is 80%-90% among obese adults, up to 90% among patients with hyperlipidemia, 30%-50% among diabetic patients, and about 3%-10% among children, increasing to 40%-70% among obese children. The most important risk factors for developing NAFLD are obesity, insulin resistance, male sex, older age, and the cardiometabolic abnormalities of MetS[14,22]. Accumulation of free fatty acids and triglycerides are due, at least partially, to insulin resistance, and obesity is the key feature of the disease[23].
After liver transplantation, patients can develop obesity, insulin resistance, diabetes mellitus, hypertension, hyperlipidemia, and hyperglycemia. Metabolic abnormalities develop partially due to use of medications such as corticosteroids, calcineurin inhibitors, and sirolimus after liver transplantation[24]. Hence, recurrence or de novo NAFLD/NASH after liver transplantation is common[25]. It has been reported that 26.3% of patients with liver transplant become obese in 3 years[26] and 10%-64% of the transplant patients develop diabetes mellitus[27]. The prevalence of MetS following liver transplantation is about 50%-60%[28]. Sprinzl et al[29] performed a cohort study including 170 patients with liver transplant followed for 2 years and reported the development of MetS in one-third of the patients. The incidence of NAFLD following liver transplantation is about 18%-40%. Post-liver transplant development of NAFLD might contribute to the high cardiovascular mortality seen in these cases[30].
INTERACTIONS BETWEEN NAFLD AND COVID-19
ACE2 receptors are present in liver endothelial cells and cholangiocytes[31,32]. The incidence of acute liver injury during COVID-19 was reported to be about 15.4% in Wuhan, China[33]. Interestingly, liver involvement has been reported in about 60% of the patients[34]. Importantly, impairment of liver enzymes was seen in more than one-third to one-half of the patients with COVID-19[35-39]. Furthermore, there is higher incidence of liver function abnormality in patients with severe COVID-19[37]. Feng et al[40] hypothesized in a review that there is an association between older age and higher risk of liver damage/dysfunction during COVID-19 disease. Ji et al[41] performed a retrospective study to evaluate the status of NAFLD in 202 confirmed COVID-19 patients, and reported liver injury in half of the cases on admission and in 75% of the patients during their stay in the hospital, mainly presenting as mild hepatocellular injury indicated by increased serum level of alanine aminotransferase (ALT), and 3% with ductular or mixed pattern; about one-third of the patients had continual liver function abnormality from admission to the last day of follow-up. There is an association between the progression of COVID-19 disease and older age (> 60 years), male sex, higher body mass index, NAFLD, and higher percentage of comorbidity. The authors concluded that NAFLD is an independent risk factor for COVID-19 disease progression and is associated with higher probability of liver function abnormalities in patients from their admission until their discharge[41]. Zheng et al[42] in a study that included 45 obese and 21 nonobese patients with COVID-19 and NAFLD reported that the severity of COVID-19 is increased by the presence of obesity and NAFLD. They proposed interleukin (i.e., IL–6) as a major contributor in triggering the inflammatory storm in COVID-19 patients. Obese NAFLD patients have an increased inflammatory activity in the liver and abdominal adipose tissue that is independently associated with higher levels of IL-6 which could have an additional contribution in increasing the severity of COVID-19[42].
Gao et al[43] performed a cohort study including 65 COVID-19 patients with NAFLD and 201 COVID-19 patients without NAFLD and reported that the presence of NAFLD was associated with a 4-fold increased risk of severe COVID-19; increasing the metabolic risk factors increased the risk of severity of COVID-19; and the association with severe COVID-19 disease persisted after adjusting for sex, age, and other coexisting morbid conditions. Zhou et al[44] performed a multicentral preliminary analysis that included 327 adult patients and reported that NAFLD patients younger than 60 years of age had more severe COVID-19 disease compared to patients older than 60 years of age, independent of other risk factors that increase the severity of COVID-19. Singh et al[45] conducted a meta-analysis to identify the diseases that increase the susceptibility to SARS-CoV-2 infection. They studied the gene expression signatures in 30 widely prevalent acute, chronic, and infectious diseases that could promote the pathogenesis of COVID-19. The authors found that patients with leukemia are most susceptible to SARS-CoV-2 infection, followed by NAFLD, pulmonary arterial hypertension, type 2 diabetes, and psoriasis[45]. Targher et al[46] performed a cohort study including 310 patients with COVID-19 and reported that the severity of COVID-19 disease increased in patients with NAFLD with high or intermediate fibrosis-4 index scores. Limitations of that study are a small sample size, homogeneous ethnicity of the study population, and lack of histopathological diagnosis of liver fibrosis[46]. Patients with NAFLD are vulnerable to severe COVID-19 disease because they harbor associated risk factors. First among these is the high incidence of type-2 diabetes in NAFLD patients, increasing their susceptibility to infection[47]. Second among these is the high incidence of obesity in patients with NAFLD; these patients might present with chronic lung diseases leading to difficulty in intubation and poor response to ventilation[48]. Third is the higher incidence of cardiovascular disease in patients with NAFLD, who might present with a reduction in cardiac reserve and an impairment in their response in the intensive care unit[49,50]. In addition, deficiency of vitamin D is frequent in NAFLD and is associated with greater risk for infection[51]. Furthermore, NAFLD is associated with high 30-d mortality in community-acquired pneumonia patients[52].
MECHANISM OF LIVER INJURY BY COVID-19
Binding of SARS-CoV-2 to the target cells is initiated by interactions between the spike glycoprotein (termed ‘S’) and ACE2 receptors. Following receptor binding, SARS-CoV-2 S is processed by a plasma membrane-associated type II transmembrane serine protease to release the viral material into the host cells. This mechanism is supported by the rapid increase of SARS-CoV-2 genomic RNAs in liver ductal organoids 24 h after infection[53,54]. Hepatocellular injury seen in COVID-19 is likely due to temporary damage to liver cells by nonviral agents and impairment of regeneration of the liver by cholangiocyte precursor cells, leading to deterioration of liver function[55]. However, various mechanisms have been proposed to explain the altered liver function in COVID-19. One of these proposed mechanisms is direct liver damage by SARS-CoV-2 due to replication of the virus in hepatic cells after binding to ACE2 receptors. This effect is not related to increased uptake of SARS-CoV-2 by the liver because NAFLD does not alter expression of hepatic genes in COVID-19. Biquard et al[56] conducted a study to investigate whether NAFLD is associated with alteration in hepatic expression of SARS-CoV-2 critical entry proteins. They found that uptake of SARS-CoV-2 by the liver is not increased in NAFLD[56]. However, the observation of normal serum levels of alkaline phosphatase in most of the patients does not support this hypothesis. Another mechanism is increased expression of ACE2 receptors in liver injury due to hepatocellular hypoxia in patients with COVID-19[32]. Hypoxia activates hypoxia-inducible factors (i.e., HIFs). Increased HIF1 alpha and HIF2 alpha signaling promotes metabolic diseases, such as NAFLD and MetS[57]; hence, hypoxia could aggravate the progression of NAFLD. However, the dramatic rise in plasma levels of aspartate and ALT (aspartate aminotransferase/ALT) by one to two times the upper limit of normal does not support hypoxic liver injury. The cytokine storm mechanism includes immune-mediated liver damage caused by severe inflammatory response following SARS-CoV-2 infection. This mechanism is supported by the higher serum levels of the inflammatory markers [IL-6, IL-2, C-reactive protein (CRP), and serum ferritin][58]. In addition, postmortem liver biopsy obtained from patients deceased from COVID-19 showed hyperactivation of T cells and microvesicular steatosis, suggesting that the liver injury is most likely immune-mediated.
Another mechanism is drug-induced liver injury (commonly referred to as DILI). The use of antiviral medications such as tocilizumab, remdesivir, hydroxychloroquine, azithromycin, and Chinese traditional medicine was recommended for the treatment of COVID-19. All these agents have the potential to induce hepatotoxicity in some patients. Moreover, the presence of NAFLD increases the risk of developing DILI[41,59-61]. Another suggested mechanism is hepatic lipid metabolism. There is an association between hepatic lipid metabolism and diabetes mellitus, fatty liver, and hepatic fibrosis. Metabolic dysfunction caused by multiple processes can lead to hepatic steatosis. Hepatic lipid accumulation caused by increased uptake of lipid by the liver and de novo lipogenesis or decreased oxidation and export of lipid is the initial process; then, additional factors induce inflammation and insulin resistance, and promote hepatic steatosis progression. Evidence has indicated that these factors functioning within the liver can cause activation of innate immunity and induce inflammatory response in the liver, possibly influencing the development of hepatic fibrosis in NAFLD[62]. Another proposed mechanism is pre-existing liver disease reactivation. Ji et al[63] performed a study to investigate the prevalence of acute-on-chronic liver failure in COVID-19 patients with pre-existing compensated chronic liver disease and reported that the patients with pre-existing chronic liver disease could be at higher risk for liver injury by COVID-19 and that COVID-19 increases the progression of the chronic liver disease leading to deterioration of the liver function (Figure 1).
Figure 1.
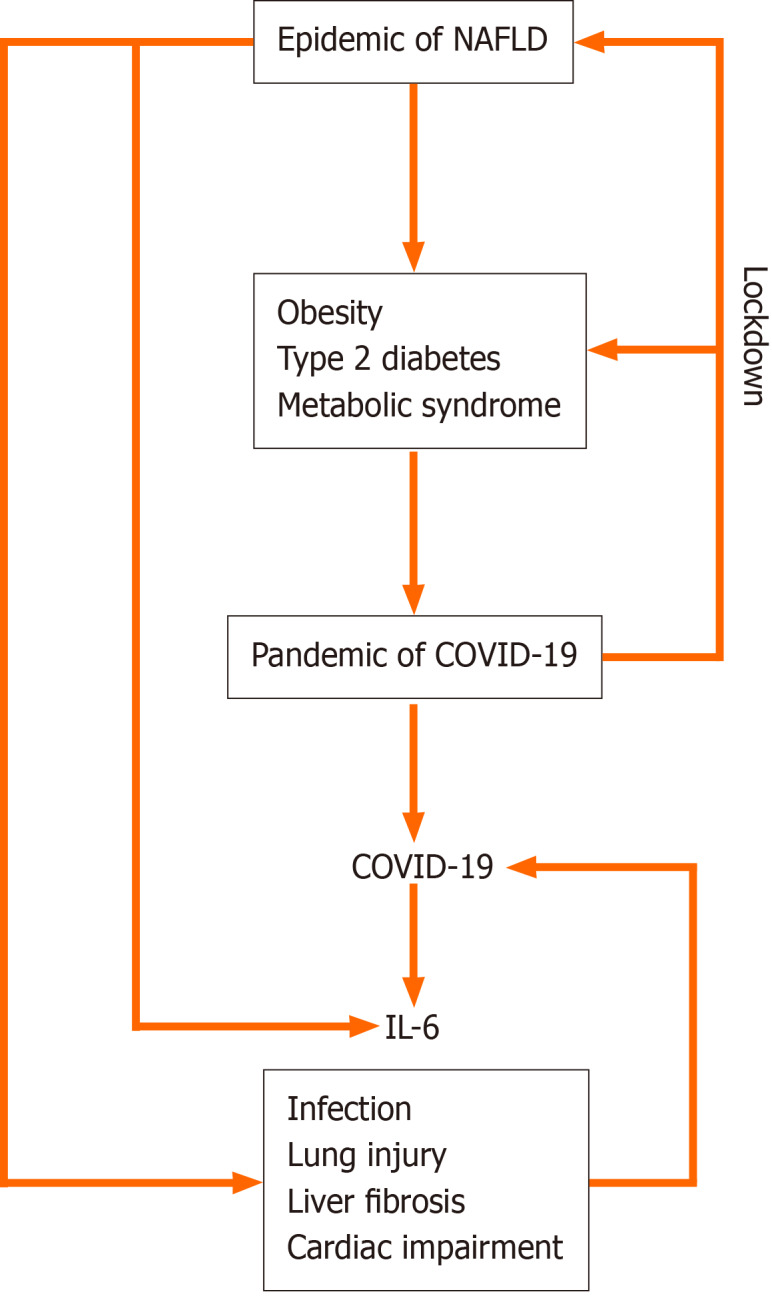
Interwoven relationships between nonalcoholic fatty liver disease, coronavirus disease 2019, interleukin-6, risk factors for coronavirus disease 2019, and effect of lockdown. The risk factors for coronavirus disease 2019 (COVID-19) are infection, lung injury, liver fibrosis, and cardiac impairment. IL-6: Interleukin–6; NAFLD: Nonalcoholic fatty liver disease.
It is not yet clear whether NAFLD can aggravate or precipitate the cytokine storm. Dysregulated hepatic innate immunity in NAFLD patients could contribute to the pathogenesis of COVID-19. Hepatic innate immunity cells are active cytokine producers. NAFLD and obesity are associated with high production of pro-inflammatory cytokines by adipocytes and Kupffer cells. This might increase the risk of symptomatic COVID-19 and the prevalence of NAFLD[64]. The plasma levels of inflammatory markers, including ferritin, lactate dehydrogenase, D-dimer, CRP, IL-2, IL-10, and IL-6, are high in severe COVID-19 disease[58]. IL-6 plays a key role in cytokine storm initiation and progression in patients with COVID-19[40] and high plasma levels of IL-6 have been reported in patients with NAFLD[65]. This means that the progression of NAFLD could be accelerated by COVID-19[66].
EFFECT OF LOCKDOWN DUE TO COVID-19 ON PATIENTS WITH NAFLD
Due to the increased number of reported cases and the high fatality rate of COVID-19, lockdowns were imposed and the activities of clinical care centers were suspended for the benefit of COVID-19 patients. These actions have adverse effects on the management of the NAFLD and follow-up, ultimately leading to increased liver-related mortality. Moreover, fear of many patients from the risk of acquiring SARS-CoV-2 infection in the hospital setting prevented them from seeking or participating in proper management by hepatologists[67].
Liver transplantation has become very challenging during the ongoing pandemic of COVID-19 because many transplantation centers stopped or reduced the transplantation surgeries due to a decrease in the number of donors and the conversion of many healthcare facilities into units for treating COVID-19 patients. Testing of SARS-CoV-2 for liver transplantation donors and recipients has been applied in many hospitals, but the influence of COVID-19 on liver transplantation outcome is still unknown. It is likely that the COVID-19 pandemic will cause a negative effect on the increase in liver-related morbidity and mortality that will become obvious in the upcoming months[67].
For instance, the increase in financial constrains associated with social isolation and job losses will cause an increase in alcohol addiction, drug use, depression, and overeating. This may ultimately increase the burden of NAFLD and associated morbidity and mortality. These unavoidable effects of the COVID-19 pandemic will likely be seen in the years to come. Prevention of liver-related mortality after the pandemic of COVID-19 requires rapid reopening of healthcare facilities for patients with liver diseases and for patients in need of liver transplantation. Governments need to adopt social measures to alleviate the health consequences of the global economic crisis and provide more funds to healthcare systems[67].
CONCLUSION
Earlier studies have suggested that the most vulnerable individuals to SARS-CoV-2 infection suffer from pre-existing disease, including MetS, NAFLD, diabetes, obesity, and visceral obesity. In Figure 1, we have highlighted the plausibility that the prevalence of NAFLD is more than that currently estimated, due to the high prevalence of diabetes, MetS, and visceral obesity. It is not yet clear whether the COVID-19 pandemic was related to the high prevalence of NAFLD in different populations[14,22,45] — in other words, whether the pandemic of COVID-19 has uncovered a heretofore un-noticeable high prevalence of NAFLD, obesity, and diabetes. These observations can be endorsed by the interwoven relationship between NAFLD and the associated high-risk factors for COVID-19. For instance, NAFLD can increase the risk of infection, lung injury, cardiac impairment, and difficulty with respiratory ventilation. Importantly, NAFLD can be associated with higher risk for COVID-19, especially in the presence of liver fibrosis. The association between high production of IL-6 in both NAFLD and COVID-19 may raise the need for further research to determine whether NAFLD can be involved directly in the cytokine storms (Figure 1). It is worth mentioning that these observations may also help in part to enhance our understanding of why COVID-19 is more prevalent in Black and other ethnic minorities[68].
Footnotes
Conflict-of-interest statement: The authors declare no conflict of interest related to this manuscript.
Manuscript source: Invited manuscript
Corresponding Author's Membership in Professional Societies: The British Geriatric Society.
Peer-review started: January 13, 2021
First decision: February 10, 2021
Article in press: April 26, 2021
Specialty type: Gastroenterology and hepatology
Country/Territory of origin: United Kingdom
Peer-review report’s scientific quality classification
Grade A (Excellent): A
Grade B (Very good): 0
Grade C (Good): C, C, C
Grade D (Fair): D
Grade E (Poor): 0
P-Reviewer: Chen H, Di Pasqua LG, Kim D, Malnick SD S-Editor: Liu M L-Editor: Wang TQ P-Editor: Xing YX
Contributor Information
Musaab Ahmed, College of Medicine, Ajman University, Ajman 346, United Arab Emirates.
Mohamed H Ahmed, Department of Medicine and HIV Metabolic Clinic, Milton Keynes University Hospital NHS Foundation Trust, Milton Keynes MK5 6LD, United Kingdom. mohamed.hassan-ahmed@mkuh.nhs.uk.
References
- 1.Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395:470–473. doi: 10.1016/S0140-6736(20)30185-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Di Gennaro F, Pizzol D, Marotta C, Antunes M, Racalbuto V, Veronese N, Smith L. Coronavirus Diseases (COVID-19) Current Status and Future Perspectives: A Narrative Review. Int J Environ Res Public Health. 2020;17:2690. doi: 10.3390/ijerph17082690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J Infect. 2020;80:e14–e18. doi: 10.1016/j.jinf.2020.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sachdeva S, Khandait H, Kopel J, Aloysius MM, Desai R, Goyal H. NAFLD and COVID-19: a Pooled Analysis. SN Compr Clin Med. 2020:1–4. doi: 10.1007/s42399-020-00631-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mahamid M, Nseir W, Khoury T, Mahamid B, Nubania A, Sub-Laban K, Schifter J, Mari A, Sbeit W, Goldin E. Nonalcoholic fatty liver disease is associated with COVID-19 severity independently of metabolic syndrome: a retrospective case-control study. Eur J Gastroenterol Hepatol. :2020 epub ahead of print. doi: 10.1097/MEG.0000000000001902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Panyod S, Ho CT, Sheen LY. Dietary therapy and herbal medicine for COVID-19 prevention: A review and perspective. J Tradit Complement Med. 2020;10:420–427. doi: 10.1016/j.jtcme.2020.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhang T, Wu Q, Zhang Z. Probable Pangolin Origin of SARS-CoV-2 Associated with the COVID-19 Outbreak. Curr Biol. 2020;30:1578. doi: 10.1016/j.cub.2020.03.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Albano D, Bertagna F, Bertoli M, Bosio G, Lucchini S, Motta F, Panarotto MB, Peli A, Camoni L, Bengel FM, Giubbini R. Incidental Findings Suggestive of COVID-19 in Asymptomatic Patients Undergoing Nuclear Medicine Procedures in a High-Prevalence Region. J Nucl Med. 2020;61:632–636. doi: 10.2967/jnumed.120.246256. [DOI] [PubMed] [Google Scholar]
- 9.Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, Ma K, Xu D, Yu H, Wang H, Wang T, Guo W, Chen J, Ding C, Zhang X, Huang J, Han M, Li S, Luo X, Zhao J, Ning Q. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi: 10.1136/bmj.m1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Qi F, Qian S, Zhang S, Zhang Z. Single cell RNA sequencing of 13 human tissues identify cell types and receptors of human coronaviruses. Biochem Biophys Res Commun. 2020;526:135–140. doi: 10.1016/j.bbrc.2020.03.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liang W, Feng Z, Rao S, Xiao C, Xue X, Lin Z, Zhang Q, Qi W. Diarrhoea may be underestimated: a missing link in 2019 novel coronavirus. Gut. 2020;69:1141–1143. doi: 10.1136/gutjnl-2020-320832. [DOI] [PubMed] [Google Scholar]
- 12.Méndez-Sánchez N, Valencia-Rodríguez A, Qi X, Yoshida EM, Romero-Gómez M, George J, Eslam M, Abenavoli L, Xie W, Teschke R, Carrion AF, Keaveny AP. What Has the COVID-19 Pandemic Taught Us so Far? J Clin Transl Hepatol. 2020;8:0024. doi: 10.14218/JCTH.2020.00024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Benedict M, Zhang X. Non-alcoholic fatty liver disease: An expanded review. World J Hepatol. 2017;9:715–732. doi: 10.4254/wjh.v9.i16.715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sayiner M, Koenig A, Henry L, Younossi ZM. Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis in the United States and the Rest of the World. Clin Liver Dis. 2016;20:205–214. doi: 10.1016/j.cld.2015.10.001. [DOI] [PubMed] [Google Scholar]
- 15.Kanwar P, Kowdley KV. The Metabolic Syndrome and Its Influence on Nonalcoholic Steatohepatitis. Clin Liver Dis. 2016;20:225–243. doi: 10.1016/j.cld.2015.10.002. [DOI] [PubMed] [Google Scholar]
- 16.Eslam M, Sanyal AJ, George J International Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020; 158: 1999-2014. :e1. doi: 10.1053/j.gastro.2019.11.312. [DOI] [PubMed] [Google Scholar]
- 17.Lomonaco R, Ortiz-Lopez C, Orsak B, Webb A, Hardies J, Darland C, Finch J, Gastaldelli A, Harrison S, Tio F, Cusi K. Effect of adipose tissue insulin resistance on metabolic parameters and liver histology in obese patients with nonalcoholic fatty liver disease. Hepatology. 2012;55:1389–1397. doi: 10.1002/hep.25539. [DOI] [PubMed] [Google Scholar]
- 18.Pagano G, Pacini G, Musso G, Gambino R, Mecca F, Depetris N, Cassader M, David E, Cavallo-Perin P, Rizzetto M. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367–372. doi: 10.1053/jhep.2002.30690. [DOI] [PubMed] [Google Scholar]
- 19.Dumas ME, Kinross J, Nicholson JK. Metabolic phenotyping and systems biology approaches to understanding metabolic syndrome and fatty liver disease. Gastroenterology. 2014;146:46–62. doi: 10.1053/j.gastro.2013.11.001. [DOI] [PubMed] [Google Scholar]
- 20.Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28:629–636. doi: 10.1161/ATVBAHA.107.151092. [DOI] [PubMed] [Google Scholar]
- 21.Gupta A, Gupta V. Metabolic syndrome: what are the risks for humans? Biosci Trends. 2010;4:204–212. [PubMed] [Google Scholar]
- 22.Bellentani S, Scaglioni F, Marino M, Bedogni G. Epidemiology of non-alcoholic fatty liver disease. Dig Dis. 2010;28:155–161. doi: 10.1159/000282080. [DOI] [PubMed] [Google Scholar]
- 23.Townsend SA, Newsome PN. Non-alcoholic fatty liver disease in 2016. Br Med Bull. 2016;119:143–156. doi: 10.1093/bmb/ldw031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Watt KD, Pedersen RA, Kremers WK, Heimbach JK, Charlton MR. Evolution of causes and risk factors for mortality post-liver transplant: results of the NIDDK long-term follow-up study. Am J Transplant. 2010;10:1420–1427. doi: 10.1111/j.1600-6143.2010.03126.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bhagat V, Mindikoglu AL, Nudo CG, Schiff ER, Tzakis A, Regev A. Outcomes of liver transplantation in patients with cirrhosis due to nonalcoholic steatohepatitis vs patients with cirrhosis due to alcoholic liver disease. Liver Transpl. 2009;15:1814–1820. doi: 10.1002/lt.21927. [DOI] [PubMed] [Google Scholar]
- 26.Richards J, Gunson B, Johnson J, Neuberger J. Weight gain and obesity after liver transplantation. Transpl Int. 2005;18:461–466. doi: 10.1111/j.1432-2277.2004.00067.x. [DOI] [PubMed] [Google Scholar]
- 27.Lane JT, Dagogo-Jack S. Approach to the patient with new-onset diabetes after transplant (NODAT) J Clin Endocrinol Metab. 2011;96:3289–3297. doi: 10.1210/jc.2011-0657. [DOI] [PubMed] [Google Scholar]
- 28.Gitto S, Villa E. Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome after Liver Transplant. Int J Mol Sci. 2016;17:490. doi: 10.3390/ijms17040490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sprinzl MF, Weinmann A, Lohse N, Tönissen H, Koch S, Schattenberg J, Hoppe-Lotichius M, Zimmermann T, Galle PR, Hansen T, Otto G, Schuchmann M. Metabolic syndrome and its association with fatty liver disease after orthotopic liver transplantation. Transpl Int. 2013;26:67–74. doi: 10.1111/j.1432-2277.2012.01576.x. [DOI] [PubMed] [Google Scholar]
- 30.Mikolasevic I, Orlic L, Hrstic I, Milic S. Metabolic syndrome and non-alcoholic fatty liver disease after liver or kidney transplantation. Hepatol Res. 2016;46:841–852. doi: 10.1111/hepr.12642. [DOI] [PubMed] [Google Scholar]
- 31.Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. 2004;203:631–637. doi: 10.1002/path.1570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Paizis G, Tikellis C, Cooper ME, Schembri JM, Lew RA, Smith AI, Shaw T, Warner FJ, Zuilli A, Burrell LM, Angus PW. Chronic liver injury in rats and humans upregulates the novel enzyme angiotensin converting enzyme 2. Gut. 2005;54:1790–1796. doi: 10.1136/gut.2004.062398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, Wang H, Wan J, Wang X, Lu Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19) JAMA Cardiol. 2020;5:811–818. doi: 10.1001/jamacardio.2020.1017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zhang C, Shi L, Wang FS. Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. 2020;5:428–430. doi: 10.1016/S2468-1253(20)30057-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382:1708–1720. doi: 10.1056/NEJMoa2002032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Xu XW, Wu XX, Jiang XG, Xu KJ, Ying LJ, Ma CL, Li SB, Wang HY, Zhang S, Gao HN, Sheng JF, Cai HL, Qiu YQ, Li LJ. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ. 2020;368:m606. doi: 10.1136/bmj.m606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069. doi: 10.1001/jama.2020.1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020;40:2095–2103. doi: 10.1111/liv.14455. [DOI] [PubMed] [Google Scholar]
- 40.Feng G, Zheng KI, Yan QQ, Rios RS, Targher G, Byrne CD, Poucke SV, Liu WY, Zheng MH. COVID-19 and Liver Dysfunction: Current Insights and Emergent Therapeutic Strategies. J Clin Transl Hepatol. 2020;8:18–24. doi: 10.14218/JCTH.2020.00018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ji D, Qin E, Xu J, Zhang D, Cheng G, Wang Y, Lau G. Non-alcoholic fatty liver diseases in patients with COVID-19: A retrospective study. J Hepatol. 2020;73:451–453. doi: 10.1016/j.jhep.2020.03.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zheng KI, Gao F, Wang XB, Sun QF, Pan KH, Wang TY, Ma HL, Chen YP, Liu WY, George J, Zheng MH. Letter to the Editor: Obesity as a risk factor for greater severity of COVID-19 in patients with metabolic associated fatty liver disease. Metabolism. 2020;108:154244. doi: 10.1016/j.metabol.2020.154244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gao F, Zheng KI, Wang XB, Yan HD, Sun QF, Pan KH, Wang TY, Chen YP, George J, Zheng MH. Metabolic associated fatty liver disease increases coronavirus disease 2019 disease severity in nondiabetic patients. J Gastroenterol Hepatol. 2021;36:204–207. doi: 10.1111/jgh.15112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Zhou YJ, Zheng KI, Wang XB, Yan HD, Sun QF, Pan KH, Wang TY, Ma HL, Chen YP, George J, Zheng MH. Younger patients with MAFLD are at increased risk of severe COVID-19 illness: A multicenter preliminary analysis. J Hepatol. 2020;73:719–721. doi: 10.1016/j.jhep.2020.04.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Singh MK, Mobeen A, Chandra A, Joshi S, Ramachandran S. A meta-analysis of comorbidities in COVID-19: Which diseases increase the susceptibility of SARS-CoV-2 infection? Comput Biol Med. 2021;130:104219. doi: 10.1016/j.compbiomed.2021.104219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Targher G, Mantovani A, Byrne CD, Wang XB, Yan HD, Sun QF, Pan KH, Zheng KI, Chen YP, Eslam M, George J, Zheng MH. Risk of severe illness from COVID-19 in patients with metabolic dysfunction-associated fatty liver disease and increased fibrosis scores. Gut. 2020;69:1545–1547. doi: 10.1136/gutjnl-2020-321611. [DOI] [PubMed] [Google Scholar]
- 47.Carey IM, Critchley JA, DeWilde S, Harris T, Hosking FJ, Cook DG. Risk of Infection in Type 1 and Type 2 Diabetes Compared With the General Population: A Matched Cohort Study. Diabetes Care. 2018;41:513–521. doi: 10.2337/dc17-2131. [DOI] [PubMed] [Google Scholar]
- 48.De Jong A, Molinari N, Pouzeratte Y, Verzilli D, Chanques G, Jung B, Futier E, Perrigault PF, Colson P, Capdevila X, Jaber S. Difficult intubation in obese patients: incidence, risk factors, and complications in the operating theatre and in intensive care units. Br J Anaesth. 2015;114:297–306. doi: 10.1093/bja/aeu373. [DOI] [PubMed] [Google Scholar]
- 49.Abeles RD, Mullish BH, Forlano R, Kimhofer T, Adler M, Tzallas A, Giannakeas N, Yee M, Mayet J, Goldin RD, Thursz MR, Manousou P. Derivation and validation of a cardiovascular risk score for prediction of major acute cardiovascular events in non-alcoholic fatty liver disease; the importance of an elevated mean platelet volume. Aliment Pharmacol Ther. 2019;49:1077–1085. doi: 10.1111/apt.15192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Forlano R, Mullish BH, Nathwani R, Dhar A, Thursz MR, Manousou P. Non-Alcoholic Fatty Liver Disease and Vascular Disease. Curr Vasc Pharmacol. 2021;19:269–279. doi: 10.2174/1570161118666200318103001. [DOI] [PubMed] [Google Scholar]
- 51.Nseir W, Taha H, Khateeb J, Grosovski M, Assy N. Fatty liver is associated with recurrent bacterial infections independent of metabolic syndrome. Dig Dis Sci. 2011;56:3328–3334. doi: 10.1007/s10620-011-1736-5. [DOI] [PubMed] [Google Scholar]
- 52.Nseir WB, Mograbi JM, Amara AE, Abu Elheja OH, Mahamid MN. Non-alcoholic fatty liver disease and 30-day all-cause mortality in adult patients with community-acquired pneumonia. QJM. 2019;112:95–99. doi: 10.1093/qjmed/hcy227. [DOI] [PubMed] [Google Scholar]
- 53.Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020; 181: 271-280. :e8. doi: 10.1016/j.cell.2020.02.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Zhao B, Ni C, Gao R, Wang Y, Yang L, Wei J, Lv T, Liang J, Zhang Q, Xu W, Xie Y, Wang X, Yuan Z, Zhang R, Lin X. Recapitulation of SARS-CoV-2 infection and cholangiocyte damage with human liver ductal organoids. Protein Cell. 2020;11:771–775. doi: 10.1007/s13238-020-00718-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Praveen S, Ashish K, Anikhindi SA, Naresh B, Vikas S, Khare S, Anil A. Effect of COVID-19 on pre-existing liver disease: What Hepatologist should know? J Clin Exp Hepatol. 2020:epub ahead of print. doi: 10.1016/j.jceh.2020.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Biquard L, Valla D, Rautou PE. No evidence for an increased liver uptake of SARS-CoV-2 in metabolic-associated fatty liver disease. J Hepatol. 2020;73:717–718. doi: 10.1016/j.jhep.2020.04.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gonzalez FJ, Xie C, Jiang C. The role of hypoxia-inducible factors in metabolic diseases. Nat Rev Endocrinol. 2018;15:21–32. doi: 10.1038/s41574-018-0096-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Liu J, Li S, Liu J, Liang B, Wang X, Wang H, Li W, Tong Q, Yi J, Zhao L, Xiong L, Guo C, Tian J, Luo J, Yao J, Pang R, Shen H, Peng C, Liu T, Zhang Q, Wu J, Xu L, Lu S, Wang B, Weng Z, Han C, Zhu H, Zhou R, Zhou H, Chen X, Ye P, Zhu B, Wang L, Zhou W, He S, He Y, Jie S, Wei P, Zhang J, Lu Y, Wang W, Zhang L, Li L, Zhou F, Wang J, Dittmer U, Lu M, Hu Y, Yang D, Zheng X. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763. doi: 10.1016/j.ebiom.2020.102763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Boeckmans J, Rodrigues RM, Demuyser T, Piérard D, Vanhaecke T, Rogiers V. COVID-19 and drug-induced liver injury: a problem of plenty or a petty point? Arch Toxicol. 2020;94:1367–1369. doi: 10.1007/s00204-020-02734-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, Liu S, Zhao P, Liu H, Zhu L, Tai Y, Bai C, Gao T, Song J, Xia P, Dong J, Zhao J, Wang FS. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420–422. doi: 10.1016/S2213-2600(20)30076-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Cai Q, Huang D, Yu H, Zhu Z, Xia Z, Su Y, Li Z, Zhou G, Gou J, Qu J, Sun Y, Liu Y, He Q, Chen J, Liu L, Xu L. COVID-19: Abnormal liver function tests. J Hepatol. 2020;73:566–574. doi: 10.1016/j.jhep.2020.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bai L, Li H. Innate immune regulatory networks in hepatic lipid metabolism. J Mol Med (Berl) 2019;97:593–604. doi: 10.1007/s00109-019-01765-1. [DOI] [PubMed] [Google Scholar]
- 63.Ji D, Zhang D, Yang T, Mu J, Zhao P, Xu J, Li C, Cheng G, Wang Y, Chen Z, Qin E, Lau G. Effect of COVID-19 on patients with compensated chronic liver diseases. Hepatol Int. 2020;14:701–710. doi: 10.1007/s12072-020-10058-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ji D, Xu J, Qin E, Zhang D, Cheng G, Wang Y, Lau G. Reply to: 'No evidence for an increased liver uptake of SARS-CoV-2 in metabolic-associated fatty liver disease'. J Hepatol. 2020;73:718–719. doi: 10.1016/j.jhep.2020.04.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Simon TG, Trejo MEP, McClelland R, Bradley R, Blaha MJ, Zeb I, Corey KE, Budoff MJ, Chung RT. Circulating Interleukin-6 is a biomarker for coronary atherosclerosis in nonalcoholic fatty liver disease: Results from the Multi-Ethnic Study of Atherosclerosis. Int J Cardiol. 2018;259:198–204. doi: 10.1016/j.ijcard.2018.01.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Prins GH, Olinga P. Potential implications of COVID-19 in non-alcoholic fatty liver disease. Liver Int. 2020;40:2568. doi: 10.1111/liv.14484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Pawlotsky JM. COVID-19 and the liver-related deaths to come. Nat Rev Gastroenterol Hepatol. 2020;17:523–525. doi: 10.1038/s41575-020-0328-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Morlock R, Morlock A, Downen M, Shah SN. COVID-19 prevalence and predictors in United States adults during peak stay-at-home orders. PLoS One. 2021;16:e0245586. doi: 10.1371/journal.pone.0245586. [DOI] [PMC free article] [PubMed] [Google Scholar]