

Supplemental Digital Content is available in the text.
Keywords: Contact matrix, SARS-CoV-2, Social mixing, Social distancing, Transmission potential
Background:
Information about social mixing patterns under heavy social distancing is needed to model the impact of nonpharmaceutical interventions on SARS-CoV-2 transmission.
Methods:
We conducted a survey on daily person-to-person contacts during the early phase of the SARS-CoV-2 epidemic in Finland, one month after strong social distancing measures had been introduced nationwide. We defined a contact as exchange of at least a few words in proximity of another person. We also considered physical (“skin-to-skin”) contacts separately. Based on 3,171 reported contacts by 1,320 participants of 1–79 years of age, we estimated age-stratified contact matrices essential in modeling virus transmission.
Results:
Compared with contacts during prepandemic conditions, as learned from the Finnish part of the Polymod study, there was a 72% (95% credible interval, CI = 71, 74) reduction in the daily number of all contacts and a 69% (95% CI = 66, 73) reduction in the daily number of physical contacts in April 2020. The largest reduction, of almost 90%, occurred in physical contacts by individuals more than 70 years of age. The estimated reduction in the transmission potential of the virus attributable solely to reduced contact frequencies varied between 59% (whole population; physical contacts; 95% CI = 52, 68) and 77% (over 20-year olds; physical contacts; 95% CI = 70, 89).
Conclusions:
We surmise that the large reduction in the daily numbers of social contacts in the early part of the SARS-CoV-2 epidemic in Finland was likely a major contributor to the steady decline of the epidemic in the country since early April.
In Finland, the epidemic caused by the novel SARS-CoV-2 virus started in early March 2020, with a number of introductions identified in travelers returning from Southern and Central Europe.1 On 16 March, when the epidemic had reached an exponential growth phase and individual transmission chains were no longer identifiable, the government imposed strong legal measures and recommendations to endorse social distancing.2 The first SARS-CoV-2-related death in Finland occurred on 20 March. From early April, the epidemic showed a steady decline until late June. As of 24 June 2020, the cumulative incidence of confirmed coronavirus disease (COVID-19) cases and deaths in Finland were 130 per 100,000 and 5.9 per 100,000, respectively.3 More than 80% of hospitalizations and deaths occurred in the extended capital region, with one-fifth of the population.
Close person-to-person contacts are necessary for the spread of SARS-CoV-2.4 With the aim of reducing the virus’s transmission in Finland, the social distancing measures instigated in March included closing schools and universities, encouraging remote working, restricting gatherings up to 10 persons, and closing restaurants and most public places.2 Those over the age of 70 were instructed to reside in quarantine-like conditions, and there was considerable publicity for improved hand hygiene and the importance for social distancing across the whole population.
Social distancing policies can be assessed by surveying the frequency and patterns of person-to-person contacts.5–8 Apart from providing information about the public’s behavior under the pandemic threat, up-to-date information on changes in social contacts provide direct means to envision the impact of social distancing on pathogen transmission.7,8 In 2005, the Polymod survey revealed a similar age-assortative pattern in social contacts across a number of European countries.5 In such normal conditions, the average number of daily contacts in Finland was 11 per person. The number of daily encounters involving skin-to-skin contact, thought to be the most relevant for droplet-spread infections, was four.
We here report results from a survey of person-to-person contacts among the Finnish population in April 2020, 1 month after the implementation of social distancing measures. We characterize all person-to-person contacts as well as physical (“skin-to-skin”) contacts between different age groups. We compare the findings from the new survey with the age-specific patterns of contacts in the Finnish arm of the Polymod study. Finally, we discuss the implications of the new data for the development of the early phase of the SARS-CoV-2 epidemic in Finland from March through June 2020.
METHODS
Survey Set-up
We conducted a survey of social contacts among Finnish residents during the ongoing SARS-CoV-2 epidemic on 20–24 April 2020. Emailed requests to fill in a web-based questionnaire were sent to individuals belonging to an internet panel of a market research company (Taloustutkimus). The questionnaire followed the template of the Polymod study.5 The in-house ethical committee was informed about the study. As the survey participants belonged to an internet panel and no data linkage will occur, no formal ethics review was required.
We asked each member of the survey panel about his or her social contacts made during one preassigned day of the week (the day the participant opened the questionnaire or one of the 2 preceding days). The day was defined to start at 5 am and end 24 hours later. A contact was defined as a two-way conversation with at least a few words exchanged in presence of another person. We recorded each contact only once. For each contact, we asked if it involved a physical contact (e.g., a handshake, embracing, kissing).
For each contact, we asked the respondent to report age, sex, location, and frequency of meeting that person. We entered ages of contacts according to 11 classes (0–9, ..., 80–89, 90+ years; “don’t know”). Because the panel only consisted of adults 18–79 years, we pooled all contacts to individuals more than 70 years into one age class 70+. We collected additional information about the contacts by the oldest child in the panel member’s household. We categorized the children into 0–9 years and 10–19 years. We omitted the “don’t know” category in all analyses requiring known contactee ages. We thus based the analysis of between-age-class contacts on eight 10-year age classes (0–9, ..., 60–69, 70+).
Reciprocity of Reported Contacts
Denote by  ,
,  , the number of contacts participant
, the number of contacts participant  of age class
of age class  reported with individuals of age class j. The average and standard deviation of
reported with individuals of age class j. The average and standard deviation of  are denoted by
are denoted by  and
and  . We inspected the reciprocity of reported contacts by calculating standardized differences of population-level numbers of contacts from age class k to age class j and vice versa9:
. We inspected the reciprocity of reported contacts by calculating standardized differences of population-level numbers of contacts from age class k to age class j and vice versa9:
| (1) |
where  ,
,  , are the sizes of the 8 age classes in 2019. If reciprocity holds for the reported contacts, most standardized differences are between –2 and 2.
, are the sizes of the 8 age classes in 2019. If reciprocity holds for the reported contacts, most standardized differences are between –2 and 2.
Estimation of Contact Matrices
Let  denote the matrix whose elements
denote the matrix whose elements  ,
,  , are the mean numbers of daily contacts an individual in age class k makes with individuals of age class j. The elements of matrix M were parameterized to fulfill the reciprocity condition with respect to the 2019 age distribution, meaning that
, are the mean numbers of daily contacts an individual in age class k makes with individuals of age class j. The elements of matrix M were parameterized to fulfill the reciprocity condition with respect to the 2019 age distribution, meaning that  . Based on a negative binomial model for the numbers of contacts, the log–likelihood function of the three model parameters,
. Based on a negative binomial model for the numbers of contacts, the log–likelihood function of the three model parameters,  ,
,  , and
, and  , pertaining to contacts between-age classes j and k (
, pertaining to contacts between-age classes j and k ( ) is
) is
 |
where  and
and  are overdispersion parameters (i.e., the variance of
are overdispersion parameters (i.e., the variance of  is
is  ). The numbers of participants in the two age classes are
). The numbers of participants in the two age classes are  and
and  . When
. When  , only the first term in the above expression is included. Of note, we assumed the total numbers of contacts made by the adult and child in the same household to be independent, that is, we excluded any between-household heterogeneity in contact numbers.
, only the first term in the above expression is included. Of note, we assumed the total numbers of contacts made by the adult and child in the same household to be independent, that is, we excluded any between-household heterogeneity in contact numbers.
We combined replies from children 10–17 years and respondents 18–19 years into age class 10–19 years when estimating contact matrices. Because the ensuing age distribution in this age class was unbalanced, individual likelihood terms were given weights ( ) to adjust for the population-level age distribution (eAppendix 1; http://links.lww.com/EDE/B806). Likewise, as the survey sample was under-representative of households with children, respondents in the range 20–59 years were given weights by presence/absence of children in the household (eAppendix 1; http://links.lww.com/EDE/B806).
) to adjust for the population-level age distribution (eAppendix 1; http://links.lww.com/EDE/B806). Likewise, as the survey sample was under-representative of households with children, respondents in the range 20–59 years were given weights by presence/absence of children in the household (eAppendix 1; http://links.lww.com/EDE/B806).
The log-likelihood function of all model parameters is
 |
(2) |
The 36 ( ) mean parameters and 64 (=8*8) overdispersion parameters were estimated in the Bayesian context. We gave an uninformative prior
) mean parameters and 64 (=8*8) overdispersion parameters were estimated in the Bayesian context. We gave an uninformative prior  to all mean parameters and independent
to all mean parameters and independent  priors for the overdispersion parameters. The posterior distribution of the parameters is then proportional to the product of the likelihood and the prior densities:
priors for the overdispersion parameters. The posterior distribution of the parameters is then proportional to the product of the likelihood and the prior densities:
 |
The posterior predictive distribution of the number of contacts  (
( ) by an individual in age class k to individuals in age class j is
) by an individual in age class k to individuals in age class j is
 |
where the integration is with respect to the posterior distribution of the model parameters. The reciprocal numbers were obtained as  (
( ).
).
Assessment of Reductions in Contacts
We estimated a contact matrix  from the 1,006 replies in the Finnish arm of the Polymod study by using likelihood (2) with the mean contact numbers made reciprocal with respect to the 2005 age distribution. We then transformed the mean numbers to agree with the current age distribution using a density correction10:
from the 1,006 replies in the Finnish arm of the Polymod study by using likelihood (2) with the mean contact numbers made reciprocal with respect to the 2005 age distribution. We then transformed the mean numbers to agree with the current age distribution using a density correction10:
 |
where  ,
,  , are the population sizes by age class in 2005.
, are the population sizes by age class in 2005.
We evaluated changes in the numbers of between-age-class contacts in terms of ratios 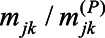 . In addition, we compared the two contact matrices, M and
. In addition, we compared the two contact matrices, M and  , by calculating the ratio of their largest eigenvalues. In the absence of heterogeneity in susceptibility to infection or infectiousness, the ratio can be interpreted as the ratio of the effective reproduction numbers (during vs. before social distancing).6,9
, by calculating the ratio of their largest eigenvalues. In the absence of heterogeneity in susceptibility to infection or infectiousness, the ratio can be interpreted as the ratio of the effective reproduction numbers (during vs. before social distancing).6,9
Retrospectively Reported Contacts
In addition to current contacts, we asked the adult respondents to recall their contacts made during the same day of the week (e.g., Monday) just before social distancing was declared. The reported numbers were compared with those based on the Polymod data.
Statistical Methods
Results are presented as posterior means and 95% equal-tailed credible intervals (CI) of the model parameters. To estimate the effects of age, sex, and geographical area on the mean number of contacts in a negative binomial regression model, we used the brms package in R.11–13 We used uninformative priors for both the means and the inverses of the overdispersion parameters. To estimate the parameters (  ) of the contact matrices, we implemented a Metropolis-Hastings algorithm in R.13 We inspected the convergence of Markov chain Monte Carlo sampling by running five parallel chains, each of length 45,000. The upper 95% confidence limits of the Gelman, Rubin scale reduction factors for all estimated parameters were below 1.08.
) of the contact matrices, we implemented a Metropolis-Hastings algorithm in R.13 We inspected the convergence of Markov chain Monte Carlo sampling by running five parallel chains, each of length 45,000. The upper 95% confidence limits of the Gelman, Rubin scale reduction factors for all estimated parameters were below 1.08.
RESULTS
Participants
Altogether 1,175 respondents (591 males, 584 females) filled in the questionnaire. The average respondent age of 51 years was higher than the current average of 42 years of the adult population. The replies were distributed among the days of the week relatively evenly, with daily proportions ranging from  (Friday) to 16% (Wednesday).
(Friday) to 16% (Wednesday).
Almost a third of the respondents (28%) lived in a single-person household and 74% of the households consisted of one or two. Only 17% ( ) of participants reported living with children, although the current percentage in Finland is 38%. The proportion of respondents living in the extended capital region (Helsinki–Uusimaa) with a population of 1,690,000 was 28%, comparing well with the actual value of 30%.
) of participants reported living with children, although the current percentage in Finland is 38%. The proportion of respondents living in the extended capital region (Helsinki–Uusimaa) with a population of 1,690,000 was 28%, comparing well with the actual value of 30%.
We additionally obtained information on social contacts from the oldest child in the respondent’s households, if applicable. We included contacts from 88% (145/165) of children, omitting data from 20 children who reported zero contacts. The age distribution of reported contacts in age class 10–19 years was skewed, with more replies from 15–19 years than 10–14 years (69% vs. 31%).
Numbers of Contacts
Figure 1 presents the distribution of the reported numbers of daily contacts. The average number by the 1,175 adult respondents was 2.4 (SD, 2.6), with range 0–29. Altogether 78% of the respondents reported fewer than four contacts, and 86% fewer than five contacts. The average number of physical contacts was 0.75 (SD, 1.2) and 85% had less than 2 physical contacts. The average number of contacts reported for the 145 children was 3.5 (SD, 2.0). The corresponding number of physical contacts was 1.9 (SD, 1.7).
FIGURE 1.
Distribution of the number of reported daily social contacts as reported by the 1,175 participants (18–79 years of age) and 145 children (0–17 years of age) in the households, Finland, April 2020. In adults, the average numbers of reported contacts were 2.4 (all contacts, A) and 0.75 (physical contacts, B). In children, the average numbers of reported contacts were 3.5 (all contacts, A) and 1.9 (physical contacts, B).
Table 1 summarizes the average numbers of reported contacts per respondent’s age. Based on the negative binomial regression model, there was no effect of sex on the number of contacts. Individuals in age class 60–69 years had 20% (95% CI = 4, 33) fewer contacts, and those 70–79 years had 43% (95% CI = 31, 54) fewer contacts than those in the youngest adult age class without children. Individuals with children in the household had 70% (95% CI = 50, 100) more contacts than those without. The number of contacts in the rest of the country was 10% (95% CI = 0, 30) larger than in the Helsinki–Uusimaa region.
TABLE 1.
Estimated Effects of Age, Family Status, Sex, and Geographical Area on the Number of All Reported Contacts
| Parameter | Level | N | Mean (SD) | Effect (95% CI) |
|---|---|---|---|---|
| Age (yrs) | 18–29 | 184 | 2.7 (2.3) | ◊ |
| 30–39 | 158 | 2.6 (2.5) | 0.89 (0.73, 1.1) | |
| 40–49 | 168 | 3.1 (3.6) | 0.99 (0.82, 1.2) | |
| 50–59 | 209 | 2.7 (3.0) | 0.95 (0.79, 1.1) | |
| 60–69 | 238 | 2.0 (2.0) | 0.80 (0.67, 0.96) | |
| 70–79 | 218 | 1.4 (1.4) | 0.57 (0.46, 0.69) | |
| Children | No | 978 | 2.0 (2.3) | ◊ |
| Yes | 197 | 4.0 (3.1) | 1.7 (1.5, 2.0) | |
| Sex | Female | 591 | 2.5 (2.6) | ◊ |
| Male | 584 | 2.2 (2.5) | 0.98 (0.88, 1.1) | |
| Region | Helsinki–Uusimaa | 323 | 2.2 (2.3) | ◊ |
| Rest | 852 | 2.4 (2.7) | 1.1 (1.0, 1.3) | |
| Age (yrs) | 0–4 | 23 | 4.0 (2.7) | * |
| 5–9 | 23 | 3.6 (2.2) | 0.90 (0.66, 1.2) | |
| 10–14 | 46 | 3.3 (1.7) | 0.81 (0.62, 1.1) | |
| 15–17 | 53 | 3.5 (1.8) | 0.87 (0.67, 1.1) |
The relative numbers with respect to the reference class (i.e., effects) are based on a negative binomial regression model. In the 1,175 adults with a total of 2,777 contacts, the reference class (◊) is females without children in the youngest age class (18–29 years) outside the Helsinki–Uusimaa region, with the point estimate of 2.2 contacts per day (95% CI = 1.9, 2.6). The data from the 145 children with 511 contacts were analyzed separately. The reference class (*) is the youngest age class with 4.0 contacts per day (95% CI = 3.1, 5.2).
CI indicates credible interval.
The elderly had approximately half the number of physical contacts as compared with other adult age classes (Table 2). Males had fewer physical contacts than females. There were double the amount of physical contacts by respondents with children (relative number 2.2, 95% CI = 1.8, 2.6). Notably, older school-aged children had only half the number of physical contacts as compared with younger children.
TABLE 2.
Estimated Effects of Age, Family Status, Sex, and Geographical Area on the Number of Physical Contacts
| Parameter | Level | N | Mean (SD) | Effect (95% CI) |
|---|---|---|---|---|
| Age (yrs) | 18–29 | 184 | 0.84 (1.2) | ◊ |
| 30–39 | 158 | 1.1 (1.1) | 1.2 (0.89, 1.5) | |
| 40–49 | 168 | 1.3 (1.8) | 1.3 (0.97, 1.6) | |
| 50–59 | 209 | 0.68 (1.1) | 0.80 (0.63, 1.0) | |
| 60–69 | 238 | 0.48 (0.68) | 0.70 (0.54, 0.92) | |
| 70–79 | 218 | 0.32 (0.65) | 0.50 (0.36, 0.68) | |
| Children | No | 978 | 0.57 (1.0) | ◊ |
| Yes | 197 | 1.6 (1.3) | 2.2 (1.8, 2.6) | |
| Sex | Female | 591 | 0.92 (1.3) | ◊ |
| Male | 584 | 0.58 (0.97) | 0.71 (0.61, 0.84) | |
| Region | Helsinki–Uusimaa | 323 | 0.76 (0.94) | ◊ |
| Rest | 852 | 0.75 (1.2) | 1.1 (0.94, 1.3) | |
| Age (yrs) | 0–4 | 23 | 3.2 (2.0) | * |
| 5–9 | 23 | 2.7 (1.7) | 0.84 (0.55, 1.3) | |
| 10–14 | 46 | 1.5 (1.4) | 0.46 (0.31, 0.70) | |
| 15–17 | 53 | 1.4 (1.5) | 0.44 (0.30, 0.64) |
The relative numbers with respect to the reference class (i.e., effects) are based on a negative binomial regression model. In the 1,175 adults with a total of 880 contacts, the reference class (◊) is females without children in the youngest age class (18–29 years) outside the Helsinki–Uusimaa region, with the point estimate of 0.74 contacts per day (95% CI = 0.58, 0.92). The data from the 145 children with 276 contacts were analyzed separately. The reference class (*) is the youngest age class with 3.2 contacts per day (95% CI = 2.3, 4.4).
CI indicates credible interval.
Checking Reciprocity
The distribution of standardized differences based on Eq (1) was relatively symmetric. The largest discrepancies occurred in contacts made by 0–9 years to 30–39 years (standardized difference 3.5) and by 10–19 years to 40–49 years (standardized difference 2.9), and by 20–29 years to 70+ years (standardized difference –3.0). Regarding physical contacts, the largest discrepancy was again in contacts made by 0–9 years to 30–39 years (standardized difference 3.7). The larger numbers of contacts reported by children to older age classes than vice versa reflect the fact that adult participants in this survey had fewer children than the general adult population.
The above analysis and the subsequent estimation of contact matrices were based on 3,171 contacts by the 1,320 participants (1,175 adults and 145 children). This excludes 3.6% (117/3,288) of reported contacts due to missing information about the contactee ages. Only two of 1,156 physical contacts were excluded.
Contacts in April 2020
The mean and variability in the between-age-class numbers of contacts were estimated based on likelihood function (2). Figure 2 shows the posterior mean contact matrices for all contacts (Figure 2A) and physical contacts (Figure 2B) between the eight age classes. See eTables 1-4; http://links.lww.com/EDE/B806 for summaries of the posterior distributions of all parameters in the contact matrix models.
FIGURE 2.
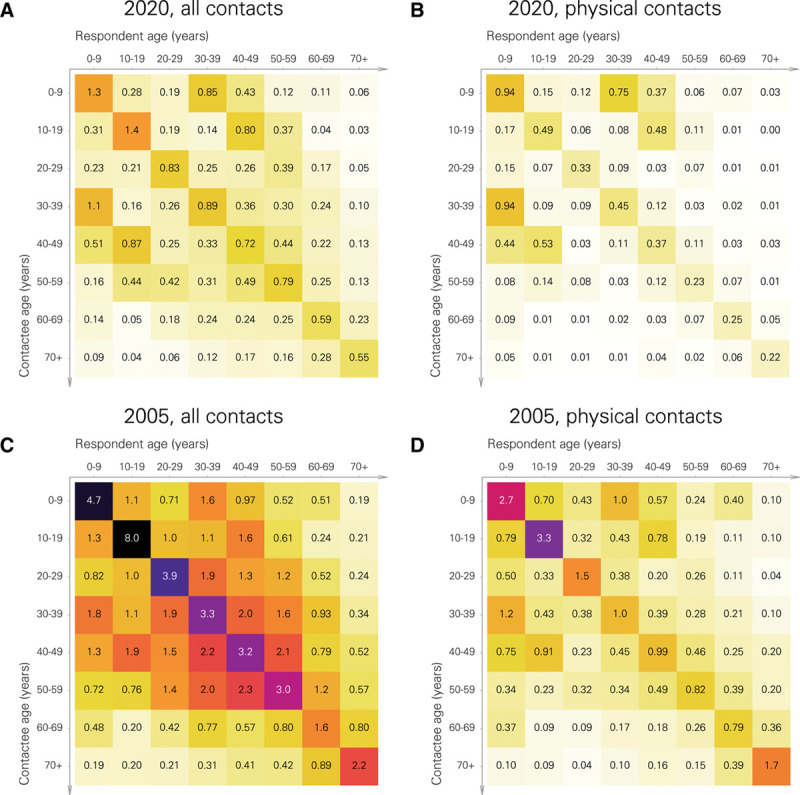
Mean numbers of daily contacts between the eight 10-year age classes in April 2020 and under normal conditions, Finland. A, All contacts (April 2020); B, physical contacts (April 2020); C (all contacts, Polymod data); D (physical contacts, Polymod data). The respondent’s age class (years) is on the top row. The rows correspond to contactees age classes (years). The numbers are posterior expectations of the mean numbers of contacts  . See eTables 1; http://links.lww.com/EDE/B806 and 3; http://links.lww.com/EDE/B806 for the 95% posterior intervals of the mean numbers as given in the April 2020 matrices.
. See eTables 1; http://links.lww.com/EDE/B806 and 3; http://links.lww.com/EDE/B806 for the 95% posterior intervals of the mean numbers as given in the April 2020 matrices.
The patterns of age-specific assortativeness and contacts between children and their parents are evident in both types of contacts (Figure 2). eFigure 1; http://links.lww.com/EDE/B806 shows the posterior predictive distributions of the numbers of all and physical contacts. eFigure 2; http://links.lww.com/EDE/B806 displays the predictive distributions as a network where the strength of connection between each pair of age classes depends on the reciprocal population-level number of contacts between them. The prominent role of children in bridging other age classes is evident, especially in physical contacts.
Reductions in the Numbers of Contacts and Transmission Potential
Based on the Polymod survey, the average numbers of all and physical contacts under normal conditions in Finland would have been 9.7 (SD, 0.9) and 3.7 (SD, 0.5), respectively. In April 2020, the corresponding numbers were 2.7 (SD, 0.3) and 1.1 (SD, 0.3). The reductions in the numbers of all contacts and physical contacts thus were 72% (95% CI = 71, 74) and 69% (95% CI = 66, 73), respectively, when comparing the period under strong social distancing with the normal conditions.
Figure 3 shows the reductions in the contact numbers by age class. Regarding all contacts, the reductions varied between 64% (0–9 years) and 77% (20–29 years and 70+years). The age-specific pattern was more pronounced in physical contacts, with the smallest reductions in 0–9 years (55%), 30–39 years (58%), and 40–49 years (54%). The reduction was as large as 88% in 70+ years.
FIGURE 3.
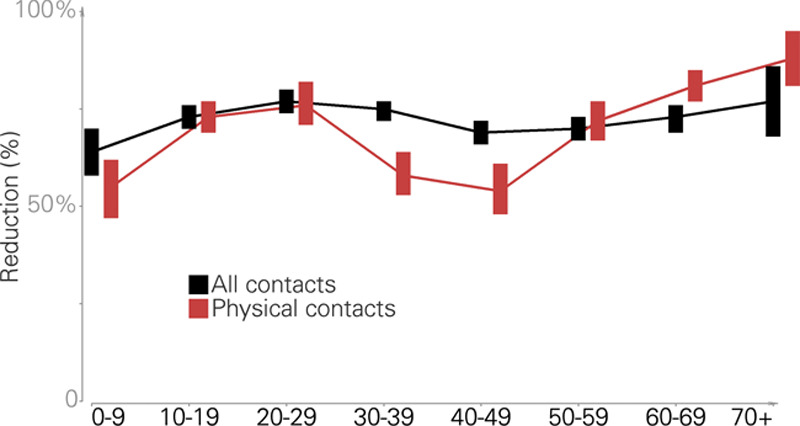
Age-class-specific relative reductions in the mean numbers of daily contacts when comparing April 2020 (strong social distancing) with the normal conditions as based on the Polymod survey data. The posterior means and 95% credible intervals are shown. Black = all contacts; red = physical contacts.
Using the Polymod contact matrix (Figure 2C) as a reference for normal conditions, the largest eigenvalue of the April 2020 all-contact matrix (Figure 2A) was 71% smaller (95% CI = 69, 73). For physical contacts (Figure 2B and D), the reduction was 59% (95% CI = 52, 68). When restricting the analysis to over 20-year-olds, the corresponding reductions were 76% (95% CI = 74, 78, all contacts) and 77% (95% CI = 70, 89, physical contacts). Among adults, the largest eigenvalues of both contact matrices were thus reduced to approximately one-fourth of their basic levels.
Figure 4 shows the posterior expectations of element-wise relative reductions  . For all contacts, the greatest reductions took place between 10–19 years and 30–39 years (85% reduction) and 20–29 years and 30–39 years (86%). In general, the greatest drops in the numbers of physical contacts occurred between 60+ and the rest of the age classes, with most reductions being more than 80%. See eTable 5; http://links.lww.com/EDE/B806 and eTable 6; http://links.lww.com/EDE/B806 for the posterior summaries of all 64 element-wise reductions. More information about contacts at home, work/school or leasure is provided in eAppendix 2; http://links.lww.com/EDE/B806.
. For all contacts, the greatest reductions took place between 10–19 years and 30–39 years (85% reduction) and 20–29 years and 30–39 years (86%). In general, the greatest drops in the numbers of physical contacts occurred between 60+ and the rest of the age classes, with most reductions being more than 80%. See eTable 5; http://links.lww.com/EDE/B806 and eTable 6; http://links.lww.com/EDE/B806 for the posterior summaries of all 64 element-wise reductions. More information about contacts at home, work/school or leasure is provided in eAppendix 2; http://links.lww.com/EDE/B806.
FIGURE 4.
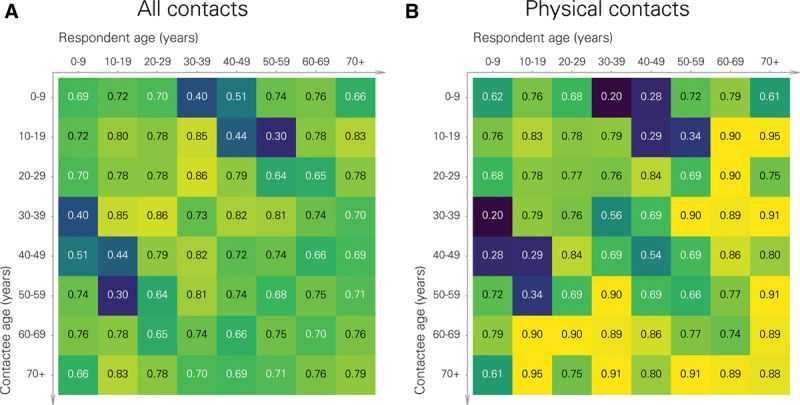
Relative reductions in the mean numbers of daily contacts (during vs. before social distancing) between the eight 10-year age classes. A, all types of contacts; B, physical contacts. The respondent’s age class (years) is on the top row. The rows correspond to the contactees’ age classes (years). The numbers are posterior expectations.
Comparison to Contacts Before Social Distancing
The 1,175 adult participants were asked about their social contacts made on 1 day 1 month before onset of social distancing. The age-standardized average number of reported daily contacts was 13 (SD, 0.64). The format of the questionnaire allowed very large numbers to be reported. If replies with >30 contacts (N = 121) were censored at 30, the average was 9.8 (SD, 0.28). The above numbers compare reasonably well with the average of 9.7 contacts as based on the Polymod data. The ratio of the largest eigenvalues of the contact matrices (prior social distancing vs. Polymod-based matrix) was 1.3.
DISCUSSION
We collected data on person-to-person contacts in Finland 1 month after the adoption of strong social distancing to reduce the spread of the new coronavirus, SARS-CoV-2. Compared with the frequency of contacts under prepandemic conditions, as based on data from the Polymod study, the average number of daily contacts had reduced from 9.7 to 2.7. The average number of physical (“skin-to-skin”) contacts had reduced from 3.7 to 1.1. Accordingly, the numbers of all types of contacts had reduced by 72% (95% CI = 71, 74) and physical contacts by 69% (95% CI = 66, 73). The reductions were most prominent in physical contacts made by adolescents (10–19 years), young adults (20–29 years), and the elderly. In particular, individuals over 70 years of age reported almost 90% fewer physical contacts as compared to normal conditions.
A reduction in the frequency of social contacts can be interpreted as reduction in the transmission potential of the pathogen. In particular, in absence of heterogeneity in susceptibility or infectiousness, the largest eigenvalue of a contact matrix is proportional to the reproduction number.10 The findings about the frequency and pattern of physical contacts in Finland in April 2020 suggest that the reproduction number of the new coronavirus may have been 59% (95% CI = 52, 68) smaller than its basic level. If one considers all types of contacts, the reduction was even larger (71%, 95% CI = 69, 73).
Young children should play an important role in virus transmission as their contacts link other age groups, thus facilitating virus circulation within the population (eFigure 2; http://links.lww.com/EDE/B806). This is particularly true for physical contacts, generally thought to be the likely at-risk events for transmission. In this study, the total number of physical contacts made by children 0–9 years of age decreased by 55% (Figure 3). The largest eigenvalue of the physical-contacts matrix for the whole population decreased by 59%, which alone would not have been enough to reduce a reproduction number much higher than 2.4 to below one. If children are less susceptible to acquiring the virus or less infectious in passing it forward compared with older age groups,14 the role of social distancing in mitigating the epidemic would have been greater. In fact, if restricted to the adult population, the SARS-CoV-2 transmission potential would have been reduced to one-fourth irrespective of the type of contacts.
Because of the early-phased intervention and the unknown number of parallel introductions of the virus to the country, reliable estimates of the SARS-CoV-2 basic reproduction number ( ) in Finland are still lacking. However, depending on which types of person-to-person contacts are relevant for SARS-CoV-2 transmission, the above reductions would have been enough to take basic reproduction numbers in the range of 2.4–4.0 down to or below one. While the sustained decline of the epidemic since early April through June signifies that the virus’s effective reproduction number in Finland has been below one, the role of other factors, including improved hand hygiene, is not clear. Nevertheless, the low levels of population-immunity indicate that herd immunity has not been decisive in damping the epidemic.15
) in Finland are still lacking. However, depending on which types of person-to-person contacts are relevant for SARS-CoV-2 transmission, the above reductions would have been enough to take basic reproduction numbers in the range of 2.4–4.0 down to or below one. While the sustained decline of the epidemic since early April through June signifies that the virus’s effective reproduction number in Finland has been below one, the role of other factors, including improved hand hygiene, is not clear. Nevertheless, the low levels of population-immunity indicate that herd immunity has not been decisive in damping the epidemic.15
It is notable that 85% of physical contacts were reported to have taken place at home. This can be understood in the backdrop of the official endorsement at the time to avoid unnecessary contacts, with most public places closed and gatherings, sports events, concerts, and other activities canceled nationwide. The large reductions in contacts by school-aged children and young adults are concordant with school closure and transition to remote working.
As the severity of disease caused by SARS-CoV-2 increases strongly with age, reducing contacts to the elderly population is essential in alleviating the epidemic’s public health burden. Our data show that the largest reductions occurred between the elderly individuals and the younger age classes (Figure 4). By June 2020, there had been a relatively small number of COVID-19-related deaths in Finland, which can be at least partly be attributed to succesful shielding of the elderly. At the same time, the similar age distributions of COVID-19-related fatalities in Finland and some other countries (e.g., Sweden) with larger epidemics suggest that the reduction of contacts among the entire population has decisively contributed to alleviating the disease burden in Finland.16,17
Because of the more intense epidemic in the area, the Helsinki–Uusimaa region was locked down from the rest of the country for 2 and a half weeks in April 2020. It is possible that the risk perception associated with the action is linked to that the frequency of social contacts in Helsinki–Uusimaa during the lock down was smaller than in the rest of the country (Table 1). When the region was reopened, the epidemic situation continued to be milder in the other areas.
Our results are remarkably concordant with those in a similar study in the United Kingdom, where a 73% reduction in the number of all types of contacts took place immediately after the lockdown was issued in March 2020.7 Much stronger social distancing measures were apparently issued in the United Kingdom as compared to Finland.2,18 Nevertheless, it is difficult to make clearcut comparisons due to the different timings of the two surveys with respect to the onsets of social distancing policies in the two countries.
There are a number of caveats in our study. First, it was not possible to properly validate the web-based questionnaire used in the current survey. Moreover, the Polymod data are 15 years old and do not necessarily correspond to current social mixing patterns. For example, it is possible that face-to-face communication has diminished in some age groups in the era of social media.8,19 The fact that the population in Finland has aged considerably over the past 15 years was taken into account by transforming the Polymod contact matrix into the current age distribution by a density-dependent way.10 As a partial validation, we compared the concordance of the transformed Polymod contact pattern with that based on information about the respondent’s contacts 1 month before the current survey. We found the agreement to be good.
Second, the survey respondents were older and had fewer children as compared with the general population. The respondents were asked to report contacts on behalf of their oldest child, which distorted the age distribution among under 20-year olds. We dealt with these problems by weighting the individual likelihood contributions. We also parameterized the model to produce contact matrices that are symmetric in the sense that the expected total number of contacts from any one age class to another is the same as vice versa.
Third, there was some missing or partial information on age. The proportion (3.6%) of discarded contacts, however, was small. We did not have the opportunity to ask specifically about contacts made by over 80-year olds, the most vulnerable group for disease caused by SARS-CoV-2. In particular, we based the analysis on the assumption that all individuals 70 years of age or more share the same frequency and pattern of contacts.
Finally, we obtained data about children’s contacts as additional information from the oldest children in the respondents’ households. The quality of these data may be suboptimal, as evidenced by the proportion of children for whom no contacts were actually reported (12%, 20/165). Discarding these children from the analysis makes the numbers of contacts greater and would tend to be a conservative choice when comparing the reduction of contacts due to social distancing.
In summary, we found that person-to-person contacts among the adult population had decreased to one-fourth during April 2020, 1 month after social distancing policies were declared in Finland. We estimate that these policies contributed to the greatly decreased SARS-CoV-2 transmission potential and thus to the steady decline of the epidemic that started 2 to 3 weeks after the policies were implemented. To distinguish the effects of the frequency contacts from their quality and from other potential reasons for reduced transmission will require a more dynamic modeling approach. Moreover, new data about more recent changes in person-to-person contacts will offer a more complete picture. As of late June 2020, the epidemic was at a stand-still, with many restrictions already lifted.
Supplementary Material
Footnotes
The main analysis code is available at http://doi.org/10.5281/zenodo.4541838. The individual-level data are confidential according to Finnish legislation. Access to the data can be requested from the Health and Social Data Permit Authority at http://www.findata.fi/en.
The authors report no funding and conflicts of interest.
Supplemental digital content is available through direct URL citations in the HTML and PDF versions of this article (www.epidem.com).
REFERENCES
- 1.Finnish Government. Report on the first phase of the working group on the coronavirus exit and reconstruction strategy (in Finnish). Available at: https://valtioneuvosto.fi/documents/10616/21411573/VN_2020_12.pdf. 2020. Accessed June 20, 2020.
- 2.Finnish Government. Press release regarding the declaration of a state of emergency in Finland over coronavirus outbreak. 2020. Available at: https://valtioneuvosto.fi/-/10616/hallitus-totesi-suomen-olevan-poikkeusoloissa-koronavirustilanteen-vuoksi?languageId=en–US. Accessed June 25, 2020.
- 3.Finnish Institute for Health and Welfare (THL). Situation update on coronavirus. 2020. Available at: https://thl.fi/fi/web/infektiotaudit-ja-rokotukset/ajankohtaista/ajankohtaista-koronaviruksesta-covid-19/tilannekatsaus-koronaviruksesta. Accessed June 24, 2020.
- 4.Liu J, Liao X, Qian S, et al. Community transmission of severe acute respiratory syndrome Coronavirus 2, Shenzhen, China, 2020. Emerg Infect Dis. 2020;26:1320–1323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mossong J, Hens N, Jit M, et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008;5:e74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hoang T, Coletti P, Melegaro A, et al. A systematic review of social contact surveys to inform transmission models of close-contact infections. Epidemiology. 2019;30:723–736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jarvis CI, van Zandvoort K, Gimma A, Prem K; Klepac P, Edmunds WJ. CMMID COVID-19 working group Quantifying the impact of physical distance measures on the transmission of COVID-19 in the UK. BMC Med. 2020;18:124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Klepac P, Kucharski AJ, Conlan A, et al. Contacts in context: large-scale setting-specific social mixing patterns from the BBC pandemic project. medRxiv. 2020. doi: 10.1101/2020.02.16.20023754. [Google Scholar]
- 9.Wallinga J, Teunis P, Kretzschmar M. Using data on social contacts to estimate age-specific transmission parameters for respiratory-spread infectious agents. Am J Epidemiol. 2006;164:936–944. [DOI] [PubMed] [Google Scholar]
- 10.Arregui S, Aleta A, Sanz J, Moreno Y. Projecting social contact matrices to different demographic structures. PLoS Comput Biol. 2018;14:e1006638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bürkner P-C. brms: an R package for Bayesian multilevel models using Stan. J Stat Softw. 2017;80:1–28. [Google Scholar]
- 12.Stan Development Team. RStan. RStan: the R interface to Stan. R package version 2.17.3. 2018. Available at: http://mc-stan.org.
- 13.R Core Team. R: A language and environment for statistical computing. 2017Vienna, Austria: R Core Team. R Foundation for Statistical Computing; Available at: https://www.R-project.org/. [Google Scholar]
- 14.Davies NG, Klepac P, Liu Y, Prem K, Jit M, Eggo RM; CMMID COVID-19 working group. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat Med. 2020;26:1205–1211. [DOI] [PubMed] [Google Scholar]
- 15.Finnish Institute for Health and Welfare (THL). Weekly report of THL serological population study of the coronavirus epidemic. 2020Finnish Insititute for Health and Welfare; Available at: https://www.thl.fi/roko/cov-vaestoserologia/sero_report_weekly_en.html. Accessed July 2, 2020. [Google Scholar]
- 16.Finnish Institute for Health and Welfare (THL). Situation update on coronavirus. 2020. Available at: https://thl.fi/en/web/infectious-diseases-and-vaccinations/what-s-new/coronavirus-covid-19-latest-updates/situation-update-on-coronavirus. Accessed July 2, 2020.
- 17.Statista. Number of coronavirus (COVID-19) deaths in Sweden in 2020, by age groups. 2020. Available at: https://www.statista.com/statistics/1107913/number-of-coronavirus-deaths-in-sweden-by-age-groups/. Accessed July 2, 2020.
- 18.UK Government. Guidance: staying at home and away from others (social distancing). 2020. Available at: https://www.gov.uk/government/publications/full-guidance-on-staying-at-home-and-away-from-others. Accessed July, 2020.
- 19.Rideout V, Robb MB. Social media, social life: teens reveal their experiences. Technical report. 2018. Common Sense. https://www.commonsensemedia.org/sites/default/files/uploads/research/2018_cs_socialmediasociallife_executivesummary-final-release. Accessed July 4, 2020. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.