

Abstract
Background
Women represent an increasing percentage of interventional cardiologists in Italy compared with other countries. However, gaps exist in understanding and adapting to the impact of these changing demographics.
Methods and Results
We performed a national survey to analyze demographics, gender‐based professional difference, needs in terms of catheterization laboratory (Cath‐Lab) abstention, and radiation safety issues in Italian Cath‐Lab settings. A survey supported by the Italian Society of Interventional Cardiology (Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici SICI‐GISE) was mailed to all SICI‐GISE members. Categorical data were compared using the χ2 test. P<0.05 was considered significant. There were 326 respondents: 20.2% were <35 years old, and 64.4% had >10 years of Cath‐Lab experience. Notably, 26.4% were women. Workload was not gender‐influenced (women performed “on‐call” duty 69.8% versus men 68.3%; P=0.97). Women were more frequently unmarried (22.1% women versus 8.7% men; P=0.002) and childless (43.9% versus 56.1%; P<0.001). Interestingly, 69.8% of women versus 44.6% of men (P<0.001) argued that pregnancy/breastfeeding negatively impacts professional skill development and career advancement. For Cath‐Lab abstention, 38.9% and 69.6% of respondents considered it useful to perform percutaneous coronary intervention robotic simulations and "refresh‐skill" sessions while they were absent or on return to work, respectively, without gender differences. Overall, 80% of respondents described current radioprotection counseling efforts as inadequate and not gender specific. Finally, 26.7% faced some type of job discrimination, a significantly higher proportion of whom were women.
Conclusions
Several gender‐based differences exist or are perceived to exist among interventional cardiologists in Italian Cath‐Labs. Joint strategies addressing Cath‐Lab abstention and radiation exposure education should be developed to promote gender equity in interventional cardiologists.
Keywords: catheterization laboratory, ethics, gender, pregnancy, radiation safety, women
Subject Categories: Catheter-Based Coronary and Valvular Interventions, Percutaneous Coronary Intervention, Women, Pregnancy
Nonstandard Abbreviations and Acronyms
- Cath‐Lab
Catheterization laboratory
- GISE‐young
Gruppo Italiano di Studi Emodinamici Young
- IC
Interventional cardiology
- ICs
Interventional cardiologists
- SICI‐GISE
Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici
Clinical Perspective
What Is New?
Gender gap is still wide in some subspecialties of medicine, such as interventional cardiology (IC), in which radioexposure plays a key role.
This is an important study that surveys and raises awareness about gender differences in personal, family, and professional life among interventional cardiologists in Italy, where the proportion of interventional cardiologists who are women is higher than in other places around the world.
Several recommendations and action items to overcome the gender gap were proposed to adjust to the rising proportion of women in IC and improve radiation prevention globally in IC.
What Are the Clinical Implications?
Gender discrimination in Italian catheterization laboratories remains both a perceived and a real issue.
With the increased prevalence of women in IC, some concerning findings, such as catheterization laboratory abstention and gender‐specific radiation counseling, need to be carefully assessed, organized, and implemented with the development of gender‐specific educational programs.
Education and professional advancement should be pursued and used across the field of IC for both sexes.
Gender represents a topic of increasing importance in medicine. Nearly half of medical students are now women, with an increase of women entering medical subspecialties that have been historically male dominated. 1 , 2 , 3 Compared with other non‐European countries, an area of major change in Italy has been in interventional cardiology (IC), where affiliated women of Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici (SICI‐GISE) now represent 17.7% of catheterization laboratory (Cath‐Lab) operators (SICI‐GISE census of 2019).3‐5 Despite this promising turn, women interventional cardiologists (ICs) remain a small community that needs to be supported, especially in the initial phases of a woman’s career, which coincide with childbearing. 4 , 5 , 6 Furthermore, both sexes need a support in those circumstances of abstention from the Cath‐Lab caused by health conditions. Although prior studies have examined the issue of gender differences in IC, there is a paucity of information available about gender differences among operators within Cath‐Lab settings. The issue of Cath‐Lab abstention also remains a widely understudied topic. 7 , 8 , 9
In 2016, SICI‐GISE established a young interventionalist group called “GISE Young” consisting of young ICs <35 years old. The mission of this group is: (1) to understand the unmet needs of young Italian ICs, (2) to promote the training and support of young Italian ICs, and (3) to develop an active national and international network of young ICs. Another important purpose of GISE Young is to support young women ICs in the early stages of their professional training and education.
To support these missions, a national survey, addressed to all SICI‐GISE members, was developed with the aim of canvassing all Italian Cath‐Labs to assess gender disparities on professional life.
The aims of this survey were to:
Assess differences in demographics in Italian Cath‐Labs according to gender;
Evaluate possible professional and private‐life gender differences in Italian Cath‐Labs;
Identify the need for professional support during and after a period of abstention from the Cath‐Lab for any reason; and
Investigate the need for dedicated radiation safety procedures as perceived by the operators.
Methods
Because of the sensitive nature of the data collected for this study, requests to access the data set from qualified researchers trained in human subject confidentiality protocols may be sent on request and after permission from the SICI‐GISE society.
The survey, named “The Gender Issues and Radiation Risk in the Cath‐Lab,” was sent by e‐mail to all SICI‐GISE members. The survey was sent on August 4, 2018, and was closed on September 30, 2018. The questions were formatted as multiple choice, and some required an open answer or definition of a scale. This was an online survey study using fully anonymized data. It was not mandatory to answer all questions to complete the survey. The survey was designed by a multidisciplinary women team composed of Cath‐Lab heads, senior ICs, and fellows. Finally, we conducted a dedicated systematic review to acknowledge and build on prior works on this topic.
The survey included a total of 46‐item questions focused on 5 sections: (1) generalities and job‐day activities (question 1‐question 12); (2) private life (question 13‐question 18); (3) abstention from the Cath‐Labs for health problems, pregnancy, and breastfeeding (question 19‐question 27); (4) radioexposure (question 28‐question 38); and (5) job discrimination issues (question 39‐question 46). The complete survey is consultable in Table S1. Response enhancement techniques included mailing lists, multiple mailings, and telephone calls. In addition, we encouraged the forwarding of the survey by e‐mail to increase participation. The survey was anonymous, without tracking of the identity personality or other personal features enabling the identification of the respondents.
The study was approved by institutional review committee (institutional review board), and the subjects gave informed consent.
Statistical Analysis
No specific primary hypothesis or end point was outlined. However, the survey was designed to capture several key dimensions of women training in cardiovascular interventions, and to enable several comparative analyses. We did not perform a specific sample size analysis for this work. However, we reasoned that a total of at least 1200 invitations should have yielded a minimum of 300 completed surveys, assuming a 20% to 25% response rate. Accordingly, a 300‐unit sample would have provided acceptably narrow 95% CIs for inferential analysis (eg, a 40% positive response to a given question would have yielded a 95% CI ranging from 33%–47%). Parametric distribution of continuous variables was tested graphically and with Kolmogorov‐Smirnov, and the appropriate analyses were used in accordance with the results. Categorical data were expressed as numbers (percentages) and compared with the use of χ2 test. All data were analyzed using SPSS version 22.0 (IBM SPSS Statistics for Windows, Version 22.0; IBM Corp, Armonk, NY). P<0.05 was considered significant.
Results
Survey Population: Generalities, Job Habits, and Private Life
The survey was sent to a total of 1230 SICI‐GISE members (1070 nonyoung and 160 young members). Table 1 and Figure 1 show the demographic of survey respondents. A total of 326 interventionalists completed the survey, representing a response rate of 26.5%. Sixty‐six (20.2%) were <35 years old, and 29.1% were between 41 and 50 years old. Overall, 86 (26.4%) of the survey responders were women. Women were more likely to be <40 years old compared with men (48.8% women versus 33.8% men; P=0.010). Respondents had >10 years of Cath‐Lab experience in 64.4% of cases, with a significant difference according to gender. Overall, 76.7% were stable consultants, whereas the remaining were cardiologists with atypical job contracts (grant holders, free‐service contracts, and/or temporary contracts). In addition, 79.8% worked in a public hospital.
Figure 1. Demographics of the Gender‐CATH survey recipients.
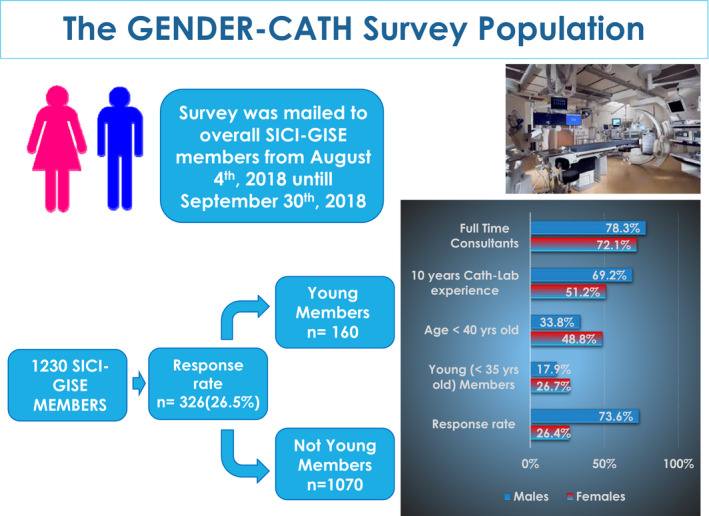
Diagram flow of the survey conducted among Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici (SICI‐GISE) members, and the principal characteristics of the survey responders. CATH indicates Catheterization laboratory; and Cath‐Lab, catheterization laboratory.
Typical Working Day and Private Life According to Gender
Table 2 shows the gender differences for working day and private life. Nearly half (48.8%) of respondents claimed to work <8 hours per day in the Cath‐Lab (45.3% women versus 50.0% men; P=0.459). Furthermore, 68.7% of respondents performed clinical activities with “on‐call” duty without difference between the genders (69.8% women versus 68.3% men; P=0.970). Notably, asking “How much does your job in the Cath‐Lab affect your family management from a scale of 1 to 10?,” both genders indicated that being an IC has a decisively negative impact (>5) on organizing their family life. For private life, women are more frequently single (22.1% versus 8.7% men; P=0.02) and without children (43.9% versus 56.1%; P<0.001). Furthermore, men more frequently have domestic partners who work in the same hospital to them, but who are not part of the medical staff (56.2% men versus 44.8% women; P=0.029).
Abstention From the Cath‐Lab
Table 3 reports the response differences between genders according to themes such as abstention from the Cath‐Lab, radiation exposure, and workplace discrimination. In cases of Cath‐Lab abstention for any reason (pregnancy/illness/injury), 38.9% and 69.6% of respondents believe that it is useful to perform interventions with percutaneous coronary intervention robotics/simulations and to participate in "refresh‐skill" sessions during abstention or on return to work, respectively, without gender differences. Moreover, women indicated a negative impact of pregnancy/breastfeeding on professional skill development and career advancement (women 69.8% versus men 44.6%; P<0.001). In addition, most women, especially those with child, respondents preferred to abstain from the Cath‐Lab altogether during pregnancy/breastfeeding (Figure 2). 8 , 9
Figure 2. Abstention from catheterization laboratories (Cath‐Labs) during pregnancy and/or breastfeeding.
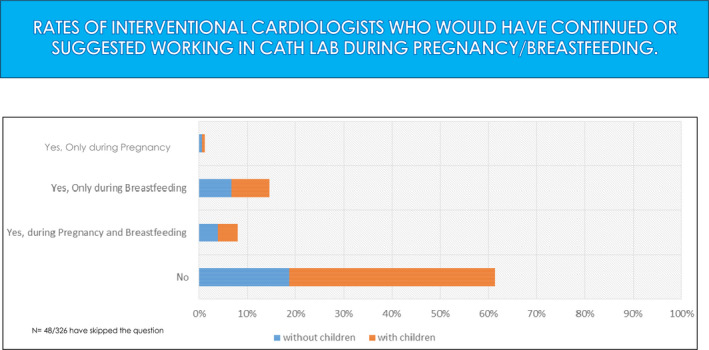
Percentage rate of responders who would continue to work in Cath‐Labs during pregnancy, breastfeeding, or in both periods. The quote of interventional cardiologists with and without child is also depicted.
Radiation Exposure
For radiation exposure, only 46.6% of respondents felt that their hospital counseling service is adequate, without any gender difference (Table 3). Overall, 85.9% of respondents believe that national professional organizations should have a direct role in developing dedicated radiation protection counseling programs. In addition, 80% of the survey’s respondents retain that the current radiation exposure counseling is not specific to gender and age. Only 12.3% of respondents reported that there are campaigns designed to prevent infertility and reduce exposure to gonads and/or highly radiosensitive tissue, such as breast tissue. Almost all respondents reported that workers should have appropriate apron lead protections, such as side sleeve for the breasts, with significantly more women in agreement (88.3% women versus 73.8% men; P=0.028). Finally, 12.0% of respondents reported that they are not equipped with a table suspended lead ceiling. As expected, there was a significant gender difference in the knowledge of the legislative principles governing access to Cath‐Labs during pregnancy. Notably, only 22.1% and 18.6% of women reported to have received detailed information from their employer on radiation exposure during the first trimester of pregnancy and during breastfeeding, respectively.
Discrimination in the Workplace
One of the survey’s introductory questions was related to the perception of gender as a limitation to pursuing a career in IC: “Do you think that the female gender can preclude or render a more difficult training course in IC?” There was an important gender difference in answering this question (74.4% women answered positively versus 35.4% of men; P<0.001). Furthermore, there was a significant gender difference in assuming that greater support of women by the scientific societies could support women in their choice of an interventional career (83.7% women versus 64.6% men; P=0.008). Interestingly, 26.7% of the entire population reported to have experienced some type of workplace discrimination, with significant differences between genders (62.8% women versus 13.8% men; P<0.001) (Table 3). Overall, 8.9% of respondents reported being subject to physical harassment, and 18.4% to verbal harassment.
Discussion
This national survey, to our knowledge, represents the first assessment of professional gender differences as perceived by Italian ICs. The main findings of the survey are the following: (1) there are no gender‐based workload differences in performing “on‐call duty” or clinical activity; (2) however, several important gender differences in private life exist between ICs; (3) both genders desire professional support in cases of abstention from/return to the Cath‐Lab through training, education, “refresh‐skill” and hands‐on sessions, aimed to facilitate re‐entry into interventional activity; (4) there is a major need for radiation safety training and the development of gender‐specific educational programs; (5) there is a significant gender perception difference in evaluating different topics; and (6) women reported more career discrimination and harassment compared with men.
Gender and Age Classes in Interventional Italian Cath‐Labs
The proportion of women IC SICI‐GISE members in Italy has increased over time, reducing the demographic gender gap in Italian Cath‐Labs. Indeed, in Italy, the rate of IC women is clearly higher than other countries, such as United States and Australia. 3 , 4 , 5 Furthermore, in the past 4 years, the number of Italian women ICs affiliated with SICI‐GISE increased from 15.7% in 2015 to 17.7% in 2019, faster compared with other countries. 3 , 4 , 5 These data are encouraging, especially when compared with the United States, where the number of practicing female interventionalists is 7%, and in line with the recently published European Association of Percutaneous Coronary Interventions Women’s survey, where European female operators accounted for 18% (n=353) of 1952 interventionalists, with a similar proportion across rank, whatever the type of institution. European Association of Percutaneous Coronary Interventions data further reported that female fellows accounted for 24.5% (n=147) of the total 599 fellows (P<0.01), suggesting that the proportion of women is likely to increase further. 9 , 10
A growing number of women in IC therefore requires a more detailed understanding of the gender‐based needs and requirements within the Cath‐Lab to ensure operator safety. This survey demonstrated that gender topic is important between both sexes and various age groups of IC generations. Indeed, although the survey was an initiative conceived and launched by the GISE Young group, it included participation from all ICs in Italy. However, the women who participated in the survey were younger overall than the male participants. There was a significantly greater female preponderance in the respondent group of <40 year olds. These results may be partly justified and linked to a selection bias: more young women could have participated because the survey assessed a relevant topic to women of childbearing age or harboring more concern about the future of their career. However, these results also potentially suggest that we are beginning an era of “gender change” in the Cath‐Lab, with a growing percentage of women willing and wanting to share their opinions and strive for positive professional change.
Gender Disparities: Job, Private Life
This survey evaluated the work and private life of ICs according to gender. Importantly, the typical workday performing clinical activities and “on‐call” duty for ICs is similar between the 2 genders. Similarly, work position (eg, full‐time consultants) was not different according to gender. Nevertheless, compensation was not addressed. However, the fact that women perform the same amount of “on‐call duty” does not mean their workload is the same. In fact, women are more often asked to complete additional work‐related tasks apart from their clinical activities. Indeed, despite a similar or higher workload, women are often paid less and promoted less often than their male counterparts. 4 , 7
Notably, on the contrary to workload, a major gap in private life exists. Women continue to be more frequently single. In addition, male respondents more frequently have domestic partners working in the same hospital, but who are not part of the medical staff, whereas women more often have domestic partners who work outside of the health system or have partners who are also physicians and usually working in the same structure.
Most important, besides being single, a high proportion of Italian IC women have no children. In addition, the rate of women with >1 child was extremely low compared with the male counterparts. Several factors could have contributed to this. First, the age of childbearing in most cases coincides with the IC fellowship, which starts at 29 years old in Italy. The choice to have a child often represents a criticism for young women who plan to become ICs, because pregnancy is perceived as negatively impacting on career development. Duly, Cath‐Lab directors often evaluate the “risk of a pregnancy” when choosing candidates for fellowship or recommendation for a permanent position. 10 In addition, a considerable concern among female ICs is that early skills training is known to be crucial in the learning curve, and an interruption in this training during or after pregnancy can have a negative impact. 10 , 11 , 12 , 13 , 14 , 15
Second, in the early stages of their career, pregnant women ICs have no stable job and therefore are usually not adequately supported with structured parental leave, postpartum/return‐to‐work policies, and childcare support/options.
Third, and most important, in Italy, pregnant staff members are excluded from Cath‐Lab, compared with other countries. This could represent a causative factor in justifying the absence of pregnancy or a low number of children in Italian women who wish to continue working in Cath‐Lab.
Finally, for the reasons above, many women postpone the planning of a pregnancy after IC fellowship and until their position is stable from a working point of view. It is clear, however, that the impact of delayed parenthood until after IC training may result in problems with fertility by biological age per se and because of the potential damage of radiation on reproductive system. 4 , 16 , 17
Cath‐Lab Abstention
This survey evaluated, for the first time, the need of professional support as perceived by interventionalists, during and/or after periods of abstention from activity in the Cath‐Lab, for any circumstance, including pregnancy, illness, or injury.
The use of simulators to reduce the effects of a Cath‐Lab abstention on a trainee’s ability to advance his or her skills without radiation exposure could be useful in such select cases and could also be used in general for all interventionalists who are not able to be exposed to radiation for any temporary reason. Indeed, the percutaneous coronary intervention robotic simulator had been proposed for pregnant operators. 15 Furthermore, the issue of Cath‐Lab abstention was also reported as a concern for male operators who consider it necessary to implement resources to maintain skills in circumstances of abstention from interventional activity (eg, through hands‐on sessions, refresh skills, boot camps, and percutaneous coronary intervention robotics). However, at present, percutaneous coronary intervention robotic simulators are far from being widely used in routine Cath‐Lab practice. This technology could be a part of future development in IC to address several circumstances.
Both genders retain that their institutions and national professional organizations should support all interventionalists during periods of abstention from the Cath‐Lab. The potential alternatives suggested during the Cath‐Lab abstention periods include ambulatory activity (24.5%), intensive care unit and/or general cardiology clinical care (31.3%), clinical research (14.9%), and a combination of these activities (29.8%).
Radiation Exposure
The topic of radiation exposure remains critical. Professional radiation exposure is associated with a nonnegligible lifetime attributable risk of developing malignancy; however, the prevalence of cancer among ICs has not been elucidated. 9 Furthermore, long‐term occupational exposure is correlated with a risk of noncancer health problems, such as orthopedic problems, cataracts, and premature vascular and neurocognitive aging. 18 , 19 , 20 Therefore, related training for Cath‐Lab operators and IC fellows is crucial to learning and applying strategies toward reducing radiation dose exposure. For this topic, survey respondents noted that the type of counseling currently provided by hospitals is inadequate. Furthermore, they felt it necessary to render gender‐specific radiation safety counseling programs and to include information on related infertility. To date, the only data available on the effects of long‐term radiation exposure in fertility are relative to spermatogenesis. 21 It is also necessary to increase operator awareness, promoting and encouraging more extensive use of protective devices, such as dedicated lead aprons. In line with previous reports, women, compared with men, are more concerned with the topic of personalized and dedicated lead aprons (eg, left lateral protection to the breasts). 22 , 23 These results, together with previous data coming from a European Association of Percutaneous Coronary Interventions survey, suggest that Cath‐Lab department policies should be more accurate and more stringent to improve radiation prevention and protection. 10 In this survey, only 28% of responders declared to have specific and customized lead equipment. Furthermore, 12% declared to not have wall hangings at the table for protection of the pelvis.
In regard to occupational radiation exposure during pregnancy, the data currently available do not suggest a significant increase in the risk of abortion, malformation, or fetal neoplasm in women working in Cath‐Labs. 12 , 22 , 23 However, women cardiologists are increasingly concerned about radiation exposure during pregnancy. 16 European and Italian directives on radiation risk and pregnancy are illustrated in Figure 3. 24 , 25 , 26 Although these Italian laws have been dated for 20 years, a large number of women in the survey did not know the legislative principles regulating radiation exposure and pregnancy. Therefore, concerns over radiation exposure during pregnancy remain as education in this area is lacking. Notably, despite data showing that ICs could safely continue their activity in the Cath‐Lab during pregnancy, most surveyed preferred not to work during this time. About 70% of women are reported to abstain from the Cath‐Lab during pregnancy‐breastfeeding, with higher proportion in women having a child. This reflects the lack of adequate information and could be considered a hidden subject. With a likely continued increase in the number of female interventionalists, it is necessary to carefully assess the potential risk of infertility related to pelvic radiation during IC procedures and to address the effects of radioexposure during pregnancy in detail, especially during the first trimester of pregnancy, on the effect on the fetus.
Figure 3. Italian and European radiation laws on radioexposure and pregnancy.
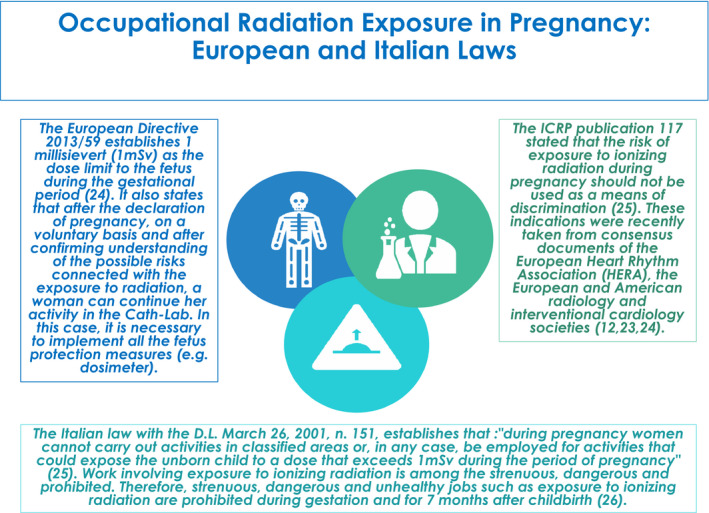
Principal laws that regulate radioexposure and pregnancy in Italy and Europe. Cath‐Lab indicates catheterization laboratory; and ICRP, International Commission on Radiological Protection.
Gender Perception and Discrimination
As expected, we observed a significant gender‐based difference on several topics. The most concerning finding was that gender remains a limitation to pursuing a career in IC. Even though we are living in an era characterized by an ideal equality between genders, the perception that female gender is detrimental toward career goals is a current reality. This is still a static concept we have yet to overcome, and a burden experienced most acutely by women. Being a woman is perceived by both men and women as being detrimental toward starting a training program in IC, to developing career goals in IC, and to compensation.
Notably, in this survey, there was an important difference in considering female gender as a perceived discriminating factor for career purposes: slightly more than half of men believe that female gender is discriminatory with respect to IC careers as opposed to 90% of women. Indeed, concerns about radiation exposure, lack of flexibility in work hours, and insufficient family support are more readily apparent to women and substantiate their belief that women cannot succeed in IC. 14 Furthermore, 64.3% of respondents retained that gender does not influence compensation, despite there being substantial evidence to support workplace compensation disparities. Therefore, the perception of what is real does not always match the reality. Harassment and discrimination are another area of actual difference. Almost a quarter of survey respondents reported to have experienced some type of workplace harassment, with 8.9% of respondents having experienced physical advances, and 18.4% having received verbal harassment. However, women significantly reported more career discrimination and harassment compared with men.
Future Directives and Recommendations Based on Survey Perceptions
One of the main objectives of this survey is to promote its distribution in other countries to evaluate possible national differences and, above all, to stimulate the formation of working groups aimed at generating greater awareness of and action around these issues. On the basis of the survey results, potential strategies to reduce gender gaps in the field of IC, to adjust to the rising proportion of women in the field, and to improve radiation prevention globally are summarized in Figure 4.
Figure 4. Proposed future directives in the field of gender gap in interventional cardiology (IC).
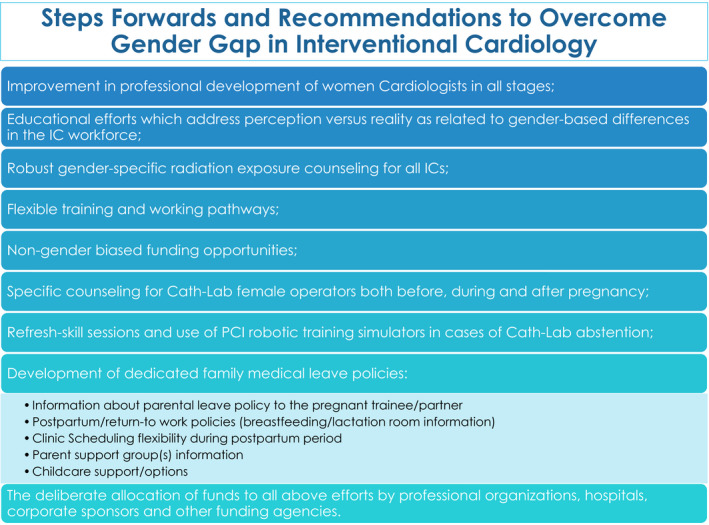
Potential recommendations to overcome gender gap in IC. Cath‐Lab indicates catheterization laboratory; ICs, interventional cardiologists; and PCI, percutaneous coronary intervention.
Limitations
The main limitation of our study is that the survey was conducted only in Italy. Furthermore, the sampling bias, caused by the voluntary nature of the survey, and consequently the sample may not necessarily reflect the entire Italian IC community. Therefore, the results are not generalizable to the wider IC population in Italy because of sampling bias. However, the response rate is satisfactory, and the results may be considered representative despite a slight bias in favor of women. In addition, women responded to the survey at a disproportionate rate to the number of female ICs in Italy, potentially creating a bias in the survey results. The results of the survey, however, are worth considering seriously for several reasons.
In the evaluation of the working day, the survey does not evaluate the other tasks outside the Cath‐Lab, which could lead to an increased workload for women.
Another limitation of this survey is that we could not evaluate the demographic differences between respondents and nonrespondents. Finally, the fact that women are paid less and less often promoted was unfortunately not addressed in this survey.
Conclusions
The results of this survey show several important novel findings. Although women represent an increasing number of ICs in Italy, gender discrimination remains both a perceived and a real issue, and these perceptions and realities, which are both important to address, do not align. It also shows that Cath‐Lab abstention and X‐ray protection are still inadequately addressed. There is a major need for attention to radiation safety in general and for counseling more specific to operator gender. Strategies for education and professional advancement should be developed in cases of Cath‐Lab abstention, and gender‐specific radiation safety programs should be used across the field of IC.
Sources of Funding
This study was supported by the Italian Society of Interventional Cardiology (Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici [SICI‐GISE]). SICI‐GISE also supports the publication charges.
Disclosures
Dr Giuseppe Tarantini received lecture fees for Edwards Lifesciences, Boston Scientific, Medtronic, Abbott Vascular, GADA, Astrazeneca, Abiomed, Cardia, Daichii Sankyo, Eli Lilly, Chiesi, Servier, Byosensor, and Bhoeringer. Dr Mehran received advisory board fees and consulting fees from Sanofi‐Aventis and Janssen, received lecture fees from Bayer, received grant support, paid to her institution, and lecture fees from Daiichi Sankyo, and has previous holding equity in Medtronic. The remaining authors have no disclosures to report.
Table 1.
Gender‐CATH Study: Demographic and Working Characteristics of the Survey Population
| Generalities | Overall (326/1230) |
Women (86/326) |
Men (240/326) |
P Value |
|---|---|---|---|---|
| Age, y | ||||
| <35 | 66 (20.2) | 23 (26.7) | 43 (17.9) | 0.095 |
| 36–40 | 59 (18.1) | 20 (23.2) | 39 (16.2) | |
| 41–50 | 95 (29.1) | 26 (30.2) | 69 (28.7) | |
| >50 | 70 (21.5) | 12 (14.0) | 58 (24.2) | |
| >60 | 31 (9.5) | 4 (4.7) | 28 (11.7) | |
| Missing answer | 4 (1.2) | 1 (1.2) | 3 (1.2) | |
| Population aged <40 y | 123 (37.7) | 42 (48.8) | 81 (33.8) | 0.010 |
| Cath‐Lab experience, y | ||||
| 1–≤3 | 29 (8.9) | 8 (9.3) | 21 (8.7) | 0.033 |
| 3–5 | 30 (9.2) | 12 (13.9) | 18 (7.5) | |
| >5 | 52 (15.9) | 20 (23.2) | 32 (13.3) | |
| >10 | 210 (64.4) | 44 (51.2) | 166 (69.2) | |
| Missing answer | 5 (1.5) | 1 (1.2) | 3 (1.2) | |
| Working position | ||||
| Scholarship | 10 (3.1) | 2 (2.3) | 8 (3.3) | 0.760 |
| Freelance contract | 28 (8.6) | 9 (10.5) | 19 (7.9) | |
| Full‐time consultant | 250 (76.7) | 62 (72.1) | 188 (78.3) | |
| Fixed‐term consultant | 35 (10.7) | 12 (14.0) | 23 (9.6) | |
| Missing answer | 3 (0.9) | 1 (1.2) | 2 (0.83) | |
| Working structure | ||||
| Affiliated private hospital | 56 (17.2) | 19 (22.1) | 37 (15.4) | 0.530 |
| Public hospital | 260 (79.8) | 65 (76.8) | 195 (81.3) | |
| Private facility | 6 (1.8) | 1 (1.2) | 5 (2.1) | |
| Missing answer | 4 (1.2) | 1 (1.2) | 3 (1.3) | |
| Working in university structure (+ answer) | 94 (28.9) | 30 (34.9) | 64 (26.7) | 0.353 |
| Geographical origin | ||||
| North | 159 (48.8) | 45 (52.3) | 114 (47.5) | 0.498 |
| Center‐south | 167 (51.2) | 41 (47.7) | 126 (52.5) | |
Values are number (percentage). CATH indicates Catheterization laboratory; and Cath‐Lab, catheterization laboratory.
Table 2.
Gender‐CATH Study: Working Characteristics and Private Life of the Survey Population
| Job and Private Life Features | Overall (n=326) | Women (n=86) | Men (n=240) | P Value |
|---|---|---|---|---|
| Cath‐Lab experience >10 y | 262 (80.4) | 64 (74.4) | 198 (82.5) | 0.101 |
| Full‐time consultant position | 250 (76.7) | 62 (72.1) | 188 (78.3) | 0.153 |
| Cath‐Lab worked <8 h/d | 159 (48.8) | 39 (45.3) | 120 (50.0) | 0.459 |
| Cardiology “on call” | 224 (68.7) | 60 (69.8) | 164 (68.3) | 0.970 |
| Time dedicated to clinical activity >50% | 46 (14.1) | 14 (16.3) | 32 (13.3) | 0.839 |
| Single | 40 (12.3) | 19 (22.1) | 21 (8.7) | 0.002 |
| Not single | 286 (87.7) | 67 (77.9) | 219 (91.2) | |
|
153/286 (53.5) | 30/67 (44.8) | 123/219 (56.2) | 0.029 |
|
62/286 (21.7) | 20/67 (29.8) | 42/219 (19.2) | 0.001 |
|
36/286 (12.6) | 25/67 (40.3) | 11/219 (5.02) | 0.721 |
| Childless | 114/326 (35.0) | 50/114 (43.9) | 64/114 (56.1) | <0.001 |
| With child | 212/326 (65.0) | 36/212 (17.0) | 176/212 (83.0) | |
| 1 Child | 67/212 (31.6) | 21/67 (31.3) | 46/67 (68.7) | |
| >1 Child | 145/212 (68.4) | 15/145 (10.3) | 130/145 (89.7) | |
| Child during residency in cardiology | 43/212 (20.3) | 5/36 (13.9) | 38/176 (21.6) | 0.003 |
Values are number (percentage) or number/total (percentage). CATH indicates catheterization laboratory; and Cath‐Lab, catheterization laboratory.
Table 3.
Gender‐CATH Study: Abstentions From Cath‐Labs, Radiation Exposure, and Work Discrimination of the Survey Population
| Features on Cath‐Lab Abstention, Radiation Exposure, and Work Discrimination | Overall (n=326) | Women (n=86) | Men (n=240) | P Value |
|---|---|---|---|---|
| Do you think that pregnancy can influence negatively the future employment intake? | 167 (51.2) | 60 (69.8) | 107 (44.6) | <0.001 |
| Are you aware of the laws that regulate access to the Cath‐Labs during the period of pregnancy? | 159 (48.8) | 62 (72.1) | 97 (40.4) | <0.001 |
| Do you think that the SICI‐GISE scientific society should create resources to maintain the skills in case of Cath‐Lab abstention? | 198 (60.3) | 62 (72.1) | 136 (56.7) | 0.057 |
| Do you think that a greater protection and support of women by the scientific societies can favor the woman in the choice of an interventional career? | 227 (69.6) | 72 (83.7) | 155 (64.6) | 0.008 |
| Do you believe that your hospital counseling service is enough to provide exhaustive information in the field of radiation exposure? | 152 (46.6) | 38 (44.2) | 114 (47.5) | 0.864 |
| Do you believe that our scientific society must also take charge of counseling programs of related to radioprotection? | 280 (85.9) | 77 (89.5) | 203 (84.6) | 0.244 |
| In your hospital, are there awareness campaigns designed to prevent infertility and to reduce the exposure of gonads and highly radiosensitive tissues, such as the breast? | 40 (12.3) | 7 (8.1) | 33 (13.8) | 0.202 |
| Do you think that female operators should have lateral protection of the breasts? | 253 (77.6) | 76 (88.3) | 177 (73.8) | 0.028 |
| Are there customized lead aprons available in your Cath‐Lab? | 92 (28.2) | 25 (29.1) | 67 (27.9) | 0.091 |
| Do you have wall hangings at the table for protection of the pelvis in your Cath‐Lab? | 287 (88.0) | 74 (86.0) | 213 (88.8) | 0.926 |
| Was the health physics service able to provide detailed information for women exposed in the first trimester of pregnancy? | (‐) Answers 110 (33.7) | 46 (53.5) | 64 (26.7) | 0.001 |
| (+) Answers 77 (23.6) |
19 (22.1) |
58 (24.2) |
||
| “Don’t know” answers 134 (41.1) | 20 (23.3) | 114 (47.5) | ||
| Missing answers 5 (1.5) | 1 (1.2) | 4 (1.7) | ||
| Was the health physics service able to provide detailed information for breastfeeding and radiation exposure? | (‐) Answers 72 (21.1) | 31 (36.0) | 41 (17.1) | 0.001 |
| (+) Answers 50 (15.3) | 16 (18.6) | 34 (14.2) | ||
| “Don’t know” answers 197 (60.4) | 38 (44.2) | 159 (66.3) | ||
| Missing answers 7 (2.1) | 2 (2.3) | 5 (2.1) | ||
| Have you ever experienced discrimination in the workplace? | 87 (26.7) | 54 (62.8) | 33 (13.8) | <0.001 |
| Have you ever perceived to be the subject of behaviors like harassment or advances in the workplace? | 29 (8.9) | 20 (23.3) | 9 (3.75) | <0.001 |
| Have you ever felt you were being subjected to verbal harassment in the workplace? | 60 (18.4) | 25 (29.1) | 35 (14.5) | 0.009 |
| Have you ever felt you were subject to physical harassment in the workplace? | 6 (1.8) | 3 (3.5) | 3 (1.25) | 0.345 |
| Do you believe that female gender is discriminatory for career purposes? | 191 (58.6) | 78 (90.7) | 113 (47.1) | <0.001 |
| Do you believe that being a woman can be discriminatory for the purposes of work compensation? | 74 (22.7) | 46/74 (62.2) | 28/74 (37.8) | <0.001 |
Values are number (percentage) or number/total (percentage). CATH indicates catheterization laboratory; Cath‐Lab, catheterization laboratory; and SICI‐GISE, Società Italiana di Cardiologia Interventistica–Gruppo Italiano di Studi Emodinamici.
Supporting information
Table S1
(J Am Heart Assoc 2021;10:e05603. DOI: 10.1161/JAHA.120.017537.)
Supplementary Material for this article is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.120.017537
For Sources of Funding and Disclosures, see page 11.
See Editorial by Grines et al.
References
- 1. Darves B. Women physicians in the specialties: making gains. NEJM Career Center. September 19, 2012. http://www.nejmcareercenter.org/article/women‐physicians‐in‐the‐specialtiesmaking‐gains/. Accessed September 19, 2012.
- 2. Hlatky MA, Shaw LJ. Women in cardiology: very few, different work, different pay. J Am Coll Cardiol. 2016;67:542–544. [DOI] [PubMed] [Google Scholar]
- 3. Khan MS, Mahmood S, Khan SU, Fatima K, Khosa F, Sharma G, Michos ED. Women training in cardiology and its subspecialties in the United States: a decade of little progress in representation. Circulation. 2020;141:609–611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Burgess S, Shaw E, Ellenberger K, Thomas L, Grines C, Zaman S. Women in medicine: addressing the gender gap in interventional cardiology. J Am Coll Cardiol. 2018;72:2663–2667. [DOI] [PubMed] [Google Scholar]
- 5. Burgess S, Shaw E, Zaman S. Women in cardiology. Circulation. 2019;139:1001–1002. [DOI] [PubMed] [Google Scholar]
- 6. Douglas PS, Rzeszut AK, Bairey Merz CN, Duvernoy CS, Lewis SJ, Walsh MN, Gillam L. Career preferences and perceptions of cardiology among US internal medicine trainees: factors influencing cardiology career choice. JAMA Cardiol. 2018;3:682–691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lewis SJ, Mehta LS, Douglas PS, Gulati M, Limacher MC, Poppas A, Walsh MN, Rzeszut AK, Duvernoy CS. American College of Cardiology Women in Cardiology Leadership Council: changes in the professional lives of cardiologists over 2 decades. J Am Coll Cardiol. 2017;69:452–462. [DOI] [PubMed] [Google Scholar]
- 8. Capranzano P, Kunadian V, Mauri J, Petronio AS, Salvatella N, Appelman Y, Gilard M, Mikhail GW, Schüpke S, Radu MD, et al. Motivations for and barriers to choosing an interventional cardiology career path: results from the EAPCI Women Committee worldwide survey. EuroIntervention. 2016;12:53–59. [DOI] [PubMed] [Google Scholar]
- 9. Yong CM, Abnousi F, Rzeszut AK, Douglas PS, Harrington RA, Mehran R, Grines C, Altin SE, Duvernoy CS. Gender differences in the pursuit of interventional cardiology as a subspecialty among cardiovascular fellows‐in‐training. American College of Cardiology Women in Cardiology Leadership Council (ACC WIC); Society for Cardiovascular Angiography and Interventions Women in Innovations (SCAI WIN). JACC Cardiovasc Interv. 2019;12:219–228. [DOI] [PubMed] [Google Scholar]
- 10. Manzo‐Silberman S, Piccaluga E, Radu MD, James SK, Schüpke S, Vaquerizo B, Kunadian V, Capranzano P, Mehilli J, Buchanan GL, et al. Radiation protection measures and gender distribution in European interventional catheterization laboratories: results from the EAPCI women's survey. EuroIntervention. 2019;19:18–01044. [DOI] [PubMed] [Google Scholar]
- 11. Valentin J . 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007;37:1–332. [DOI] [PubMed]
- 12. Sarkozy A, De Potter T, Heidbuchel H, Ernst S, Kosiuk J, Vano E, Picano E, Arbelo E, Tedrow U. Occupational radiation exposure in the electrophysiology laboratory with a focus on personnel with reproductive potential and during pregnancy: a European Heart Rhythm Association (EHRA) consensus document endorsed by the Heart Rhythm Society (HRS). Europace. 2017;19:1909–1922. [DOI] [PubMed] [Google Scholar]
- 13. Wang TY, Grines C, Ortega R, Dai D, Jacobs AK, Skelding KA, Mauri L, Mehran R. Women in interventional cardiology: update in percutaneous coronary intervention practice patterns and outcomes of female operators from the National Cardiovascular Data Registry. Catheter Cardiovasc Interv. 2016;87:663–668. [DOI] [PubMed] [Google Scholar]
- 14. AAMC . 2016 Physician specialty data report. https://www.aamc.org/data/workforce/reports/457712/2016‐specialty‐databook.html. Accessed September 11, 2018.
- 15. Hauguel‐Moreau M, Adjedj J. Managing pregnancy as an interventional cardiologist fellow‐in‐training: my experience with a simulator. J Am Coll Cardiol. 2016;68:1916–1919. [DOI] [PubMed] [Google Scholar]
- 16. Sarma AA, Nkonde‐Price C, Gulati M, Duvernoy CS, Lewis SJ, Wood MJ. Cardiovascular medicine and society: the pregnant cardiologist. J Am Coll Cardiol. 2017;69:92–101. [DOI] [PubMed] [Google Scholar]
- 17. Best PJ, Skelding KA, Mehran R, Chieffo A, Kunadian V, Madan M, Mikhail GW, Mauri F, Takahashi S, Honye J. For the Society for Cardiovascular Angiography & Interventions’ Women in Innovations (WIN) Group. SCAI consensus document on occupational radiation exposure to the pregnant cardiologist and technical personnel. Catheter Cardiovasc Interv. 2011;77:232–241. [DOI] [PubMed] [Google Scholar]
- 18. Klein LW, Miller DL, Balter S, Laskey W, Naito N, Haines D, Ross A, Mauro MA, Goldstein JA. Occupational health hazards in the interventional laboratory: time for a safer environment. Catheter Cardiovasc Interv. 2009;73:432–438. [DOI] [PubMed] [Google Scholar]
- 19. Andreassi MG, Piccaluga E, Guagliumi G, Del Greco M, Gaita F, Picano E. Occupational health risks in cardiac catheterization laboratory workers. Circ Cardiovasc Interv. 2016;9:e003273. 10.1161/CIRCINTERVENTIONS.115.003273. [DOI] [PubMed] [Google Scholar]
- 20. Andreassi MG, Piccaluga E, Gargani L, Sabatino L, Borghini A, Faita F, Bruno RM, Padovani R, Guagliumi G, Picano E. Subclinical carotid atherosclerosis and early vascular aging from long‐term low‐dose ionizing radiation exposure: a genetic, telomere, and vascular ultrasound study in cardiac catheterization laboratory staff. JACC Cardiovasc Interv. 2015;8:616–627. [DOI] [PubMed] [Google Scholar]
- 21. Kumar D, Salian SR, Kalthur G, Uppangala S, Kumari S, Challapalli S, Chandraguthi SG, Jain N, Krishnamurthy H, Kumar P, et al. Semen abnormalities, sperm DNA damage and global hypermethylation in health workers occupationally exposed to ionizing radiation. PLoS One. 2013;8:e69927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Buchanan GL, Chieffo A, Mehilli J, Mikhail GW, Mauri F, Presbitero P, Grinfeld L, Petronio AS, Skelding KA, Hoye A, et al. The occupational effects of interventional cardiology: results from the WIN for Safety survey. EuroIntervention. 2012;8:658–663. [DOI] [PubMed] [Google Scholar]
- 23. Dauer LT, Miller DL, Schueler B, Silberzweig J, Balter S, Bartal G, Chambers C, Collins JD, Damilakis J, Dixon RG, et al. Society of Interventional Radiology Safety and Health Committee. Cardiovascular and Interventional Cardiological Society of Europe Standards of Practice Committee Occupational radiation protection of pregnant or potentially pregnant workers in IR: a joint guideline of the Society of Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J Vasc Interv Radiol. 2015;26:171–181. [DOI] [PubMed] [Google Scholar]
- 24. European Council . Council Directive 2013/59/Euratom of 5 December 2013 laying down basic safety standards for protection against the dangers arising from exposure to ionising radiation, and repealing Directives 89/618/Euratom, 90/641/ Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom. Official Journal of the European Union. 2014;57:1–73. [Google Scholar]
- 25. Rehani MM, Ciraj‐Bjelac O, Van ~o ´ E, Miller DL, Walsh S, Giordano BD, Persliden J. ICRP Publication 117. Radiological protection in fluoroscopically guided procedures performed outside the imaging department. Ann ICRP. 2010;40:1–102. [DOI] [PubMed] [Google Scholar]
- 26. Decreto Legislativo 26 marzo 2001 , n. 151. Testo unico delle disposizioni legislative in materia di tutela e sostegno della maternita' e della paternita', a norma dell'articolo 15 della legge 8 marzo 2000, n. 53. (Pubblicato nella G.U. 26 aprile 2001, n. 96, S.O.).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1