

There has been much controversy about the safety or harm associated with the consumption of eggs and meat. In the past, the focus has largely been on the content of cholesterol and saturated fat. In this Viewpoint, we refocus the view of this issue through the lens of the effects of egg and meat consumption on toxic metabolites produced by the intestinal microbiome. Additional references are available in the Supplemental Material.
Problems With Studies Reporting No Harm From Eggs and Meat
A number of articles report no harm, or even benefit, of consuming eggs and red meat. In such reports, this result may be explained wholly or in part by the low risk and young age of the participants; confounders such as smoking, socioeconomic status, and reverse causality; and unmeasured confounders. 1
Huang et al 2 reported an analysis of 416 104 men and women in the US National Institutes of Health–American Association of Retired Persons Diet and Health Study. Substituting plant‐based protein for animal‐based protein, for only 3% of caloric intake, resulted in an overall 10% reduction in mortality. Substituting plant protein for egg protein reduced risk by 24% in men and 21% in women 2 ; substituting plant protein for red meat protein reduced risk by 13% in men and 15% in women. 2 Most of the risk reduction was for cardiovascular disease.
Reasons for the Current Controversy
An important source of the controversy is the role of the food industry in influencing public opinion.
In a commentary about an exposé of the sugar industry by Kearns et al 3 , Nestlé extended the issue to the food industry in general. Barnard et al 4 recently reviewed the influence of industry on cholesterol research. Greger has commented on the origins and approaches of egg industry advertising. 5
The assertion that eggs and meat do not raise fasting serum cholesterol levels by much is mostly true. However, the conclusion that it is therefore safe to consume them is misleading. The average increase in fasting cholesterol that results from dietary cholesterol is about 10%, but with marked individual differences with important public health implications. Furthermore, dietary cholesterol markedly increases the effect of saturated fat on fasting lipids, so bacon and eggs consumed together (as is often the case) will raise the fasting low‐density lipoprotein cholesterol (LDL‐C) by much more than eggs or bacon alone. 6 When cholesterol is consumed from meat, it is always accompanied by saturated fat, although less so in “lean” meats.
More important, there is much more to atherosclerosis and cardiovascular disease than serum cholesterol. In a study of >4000 patients with measurements of carotid plaque burden and LDL‐C in successive years, neither the level of LDL‐C at baseline nor the change in LDL‐C from baseline predicted progression, stable plaque, or regression. On the other hand, age and serum creatinine did predict progression. 7 The authors hypothesized that the relationship of impaired renal function to atherosclerosis may be largely mediated by toxic metabolites produced by the intestinal microbiome, which are renally excreted. 7
Effect of Diet on Fasting Levels of Risk Factors Versus Actual Effects on Cardiovascular Risk
Cardiovascular risk factors such as LDL‐C are indirect and imperfect predictors of risk. Most cardiovascular events occur in people at average risk factor levels who are misclassified by traditional risk factor scoring as low or intermediate risk. The effect of diet on the fasting level of risk factors is probably not what matters most for actual cardiovascular risk. We suggest that the consumption of meat and egg yolk increases cardiovascular risk and that this is probably mainly attributed to their postprandial effects. For ≈4 hours after a high‐fat/high‐cholesterol meal, there is a marked increase in the oxidation of LDL‐C, endothelial dysfunction, and arterial inflammation. There have been many studies over the years indicating that dietary cholesterol causes atherosclerosis in animal models and is associated with increased human coronary artery disease.
When the US dietary guideline for 2015 to 2020 appeared, there were jubilant headlines saying essentially that “it's OK to eat cholesterol now; the new guideline says so!” However, that is not what the guideline said. Previous guidelines said (for good reason 8 ) that people at risk of cardiovascular disease should limit cholesterol intake to <200 mg a day—<1 large (63 g) egg yolk. The press release from that guideline said in the first paragraph that there were insufficient data to identify a numeric limit to cholesterol intake such as 200 to 300 mg/day, so this would no longer be specified. However, the second paragraph said that cholesterol intake should be as low as possible within the recommended eating pattern (page 32 of the full guideline). The 2 paragraphs should have been reversed to avoid the confusion that resulted from that press release. Similar to the recent Canadian guideline, the US guideline recommended a more plant‐based diet.
Furthermore, the statement that “eggs can be part of a healthy diet for healthy people” is a common slogan in egg advertising. That statement was based on 2 US studies that showed harm from egg consumption only among people who developed diabetes mellitus during follow‐up; among those people, an egg a day doubled coronary risk. Similarly, a meta‐analysis published in 2020 reported that among people with type 2 diabetes mellitus, a high versus low egg intake was associated with increased cardiovascular risk (relative risk, 1.40; 95% CI, 1.00–1.97). 9 However, the American Heart Association statistical report of 2015 stated that only 0.1% of Americans consume a healthy diet. The EAT‐Lancet Commission recommended in 2019 that in a diet providing 2500 kcal, red meat consumption should be limited to 7 g/day and eggs to 13 g/day; they reported that North Americans consume 7 times as much red meat as recommended and nearly 3 times as much eggs. 10
In that setting it is difficult to demonstrate harm from any component of the diet. Long ago, Rose commented on the difficulty of identifying risk factors in sick populations. 11 In Greece, however, where the Mediterranean diet is the norm, the harm from eggs has been more obvious. Egg intake in the Mediterranean diet is low, ranging from 0 to 4 eggs per week on average. Among Greek diabetics, an egg a day was associated with a 5‐fold increase in coronary risk, and even 10 g of an egg per day (a sixth of a large egg) was associated with a 54% increase in coronary risk. 12
Most important, even in the United States, the cardiovascular harm from the consumption of eggs and cholesterol has recently been demonstrated. In a pooled analysis of data in 29 615 Americans followed for a median of 17.5 years, there was a dose‐dependent increase in cardiovascular risk with both dietary cholesterol and egg consumption. 13 In the same cohorts, there was a slight increase in cardiovascular risk with a higher intake of processed meat, unprocessed red meat, or poultry, but not fish. 14 Similar data have been shown for meat in the UK Biobank study; each additional serving per week of red and processed meat was significantly related to increased all‐cause mortality (hazard ratio [HR], 1.037; 95% CI, 1.028–1.047), cardiovascular mortality (HR, 1.03; 95% CI, 1.009–1.051), and cancer mortality (HR, 1.029; 95% CI, 1.016–1.042). 15
What Are the Harmful Constituents in Eggs?
The problem is not the egg white, which is largely the source of the protein that is the reason many people consume eggs; it is the yolk. Besides the very high cholesterol content (237 mg in a 63 g egg; almost as much as in a 12‐ounce beef burger), egg yolk is high in phosphatidylcholine, which is converted by the intestinal bacteria to trimethylamine. Absorbed trimethylamine is oxidized in the liver to trimethylamine N‐oxide (TMAO), which caused atherosclerosis in an animal model. Among 4007 patients referred to the Cleveland Clinic for coronary angiograms, those with TMAO levels in the top quartile had a 2.5‐fold increase in the 3‐year risk of stroke, myocardial infarction, or vascular death. 16 The other dietary substance that is largely responsible for the formation of TMAO is carnitine, mainly from red meat. Among people with impaired kidney function, high levels of TMAO accelerate the decline of renal function and increase mortality. There is a linear dose response of TMAO with egg consumption. 17
Eggs also increase the risk of type 2 diabetes mellitus. This has been known for some time. An increase in the risk of type 2 diabetes mellitus with egg consumption was confirmed in several recent meta‐analyses. In one study, this effect was limited to studies in the United States, but a recent meta‐analysis reported an increased risk of type 2 diabetes mellitus with egg consumption in China. 18
Wang et al 18 reported that TMAO levels were substantially reduced within a month by switching to white meat or nonmeat sources of protein; that may be 1 reason why there is a reduction of cardiovascular risk with vegetarian diets.
Vegetarian Diets
Recent cohort studies have shown that a healthy plant‐based diet relates to major advantages in health compared with an animal produce–based diet. Two studies in Buddhist cohorts in Taiwan reported a significant reduction in stroke risk with vegetarian diets. 19 A recent meta‐analysis of 32 prospective cohort studies in 715 128 participants followed for 3.5 to 32 years reported that the intake of plant protein was significantly associated with a lower risk of cardiovascular disease mortality (pooled HR, 0.88; 95% CI, 0.80–0.96; 12%–63%; P=0.001). 20
A recent analysis of participants in the Atherosclerosis Risk in Communities study provided robust evidence that a plant‐based diet was associated with a substantial reduction in cardiovascular risk. An example of a measured confounder in that report was that people with the most plant‐based diets were also less likely to smoke. An important unmeasured confounder that may actually be on a causal pathway is the intestinal microbiome.
In a study of patients attending vascular prevention clinics, 21 the plasma levels of 4 toxic metabolites of the intestinal microbiome (TMAO, p‐cresylsulfate, p‐cresylglucuronide, and phenylacetylglutamine) were significantly higher in people with severe carotid atherosclerosis not explained by traditional risk factors (unexplained atherosclerosis) than in people who had little or no carotid plaque despite high levels of risk factors (a protected phenotype). The differences were independent of renal function and dietary intake of the nutrient precursors of the metabolites, suggesting that differences in the intestinal microbiome accounted for that finding. In linear regression, levels of both TMAO and p‐cresylsulfate were significant independent predictors of carotid plaque burden and were more significant than sex, diastolic blood pressure, and diabetes mellitus, all of which were excluded from the model in backward regression. 21 Poesen et al 22 had previously reported that intestinally derived phenylacetylglutamine was associated with atherosclerosis. Hazen’s group recently confirmed this, and elegantly demonstrated a mechanism related to adrenergic platelet aggregation. 23
Meat Consumption and Toxic Metabolites of the Intestinal Microbiome
Red meat contains ≈4 times as much carnitine as white meat. Furthermore, other toxic metabolites of the intestinal microbiome, such as p‐cresylsulfate, hippuric acid, indoxyl sulfate, p‐cresylglucuronide, phenylacetylglutamine, and phenylsulfate, are produced from amino acids ingested as part of protein, so consumption of any animal flesh raises their plasma levels, especially when renal function is compromised, a situation that is common in the elderly. A recent report indicated that compared with red meat, the intake of 1 serving per day of combined plant protein sources (nuts, legumes, and soy) was associated with a lower risk of coronary heart disease (HR, 0.86; 95% CI, 0.80–0.93). 24
Patients on dialysis for severe renal failure have blood levels of some of these intestinal metabolites that are 50‐fold to 100‐fold higher than in people with good kidney function. These metabolites increase reactive oxygen species in endothelial cells and increase vascular calcification and mortality in chronic kidney disease. However, even people with modest impairment of kidney function, with an estimated glomerular filtration rate ≤66 mL/min per 1.73 m2, have significantly higher blood levels of all the intestinal metabolites listed previously 25 (Figure [B]). Kidney function declines with age; by age 80, the average estimated glomerular filtration rate is <60 mL/min per 1.73 m2 (Figure [A]). Thus, egg yolk and meat are particularly harmful in people with impaired kidney function, including the elderly.
Figure 1. Decline in renal function with age and the effect of renal function on plasma levels of toxic metabolites of the intestinal microbiome.
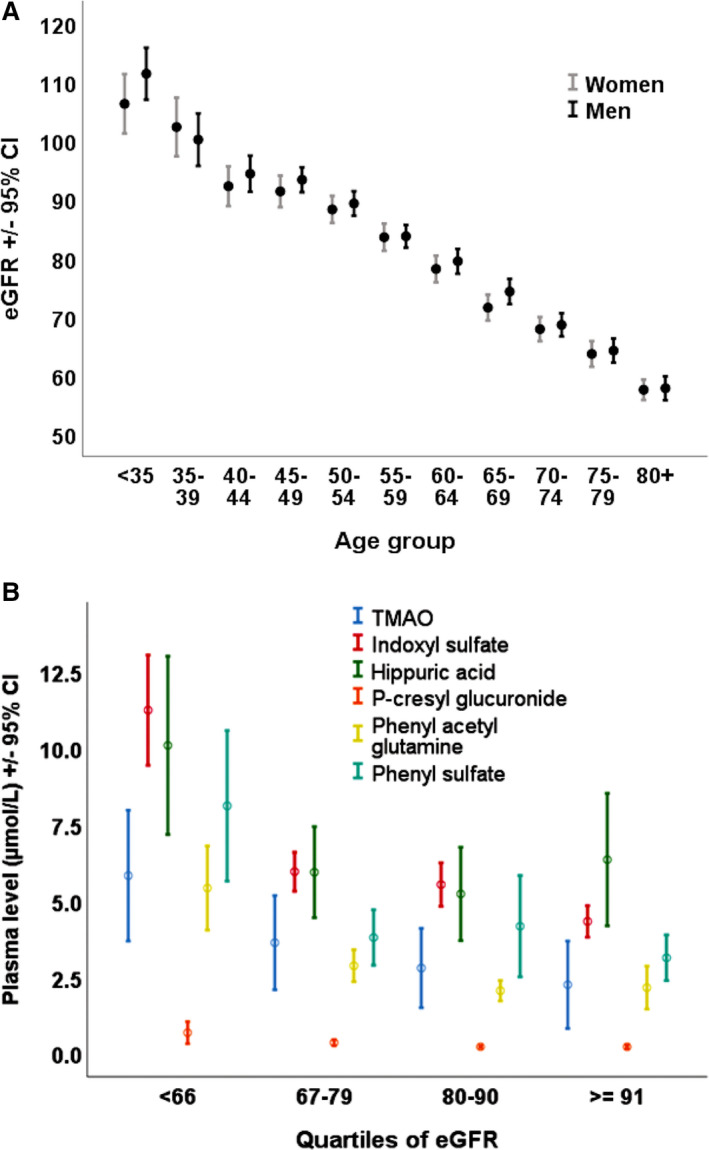
A, Decline in renal function with age. Among patients referred for stroke prevention, renal function declines linearly with age. By age 80, the mean eGFR is <60 mL/min per 1.73 m2 (n=3967). eGFR was computed using the Chronic Kidney Disease Epidemiology Collaboration equations. Reprinted from Spence JD et al with permission of the publisher. Copyright © 2015 Oxford University Press. 26 B, Effect of renal function on plasma levels of toxic intestinal metabolites. Even a modest reduction of renal function to an eGFR <66 mL/min per 1.73 m2 was associated with significantly higher plasma levels of all the intestinal metabolites (analysis of variance P<0.0001 for all except 0.01 for p‐cresylglucuronide and 0.006 for phenyl sulfate). Levels of P‐cresylsulfate were also increased significantly (P<0.0001), but the levels were much higher (increasing from 30 μmol/L in the highest quartile of eGFR to 70 μmol/L in the lowest quartile), so they are omitted from this graph because of scale. eGFR indicates estimated glomerular function; and TMAO, trimethylamine n‐oxide. Reprinted from Spence et al with permission of the publisher. Copyright © 2020, Wolters Kluwer Health. 27
Intake of Carbohydrates, Saturated Fats, and Risk
Much of the controversy in this field has been about relative harm of a low‐fat/high‐carbohydrate diet, with proponents of low‐carbohydrate/high‐fat diets such as a “keto diet” emerging. It is not that simple; there are healthy and unhealthy versions of both types of diets. Shan et al 28 analyzed cardiovascular risk in 37 233 adults it with 24‐hour dietary recall data from the US National Health and Nutrition Examination Survey from 1999 to 2014. They divided participants into 11 sex‐specific strata each of percentage of energy from fat, protein, and carbohydrate to compute healthy versus unhealthy diet scores for low‐carbohydrate/high‐fat diets and low‐fat/high‐carbohydrate diets. They found that healthy diets of both types were associated with reduced cardiovascular risk, whereas unhealthy diets of both types were associated with increased cardiovascular risk.
What Diet Should Be Consumed by People at Risk of Cardiovascular Disease?
With good reason, there has been much made of the evils of the low‐fat diet, which tends to replace fat with carbohydrates. Although it is true that a high glycemic index high‐carbohydrate diet may be harmful, the appropriate answer to that problem is not the popular low‐carbohydrate high‐fat diets that are high in cholesterol and animal fat, such as the classic Atkins diet. It is not the amount of fat in the diet that matters, it is the kind of fat. On Crete, where 40% of calories were from fat (mainly olive oil), the coronary risk was 1/15th that in Finland at that time, where 38% of calories were from fat (mainly animal fat, accompanied by cholesterol). Although it is possible that a vegetarian diet may be even better (if B12 deficiency were avoided), the best evidence for cardiovascular prevention is for the Cretan Mediterranean diet. Although it is commonly thought that the Mediterranean diet is high in fish and poultry, it was described by Ancel Keys, leader of the Seven Countries Study, as a “mainly vegetarian diet, favoring fruit for dessert instead of pastries, much lower in meat and dairy.” 29 A study in Israel randomized overweight residents of a nuclear facility to a low‐fat diet, a low‐carbohydrate diet similar to the Atkins diet, and the Mediterranean diet. Weight loss was identical on the low‐carbohydrate diet and the Mediterranean diet, and significantly better with both than on the low‐fat diet. Importantly, among diabetics, the Mediterranean diet was clearly the best for lowering blood sugar and fasting insulin levels and insulin resistance. A recent study provided strong evidence that a diet high in fruits, vegetables, and whole grains reduced the risk of diabetes mellitus. 30
Conclusions
Egg yolk and red meat should be avoided, and meat intake limited, to prevent cardiovascular disease and stroke. Because of the interaction of impaired renal function with toxic metabolites of the intestinal microbiome, that advice is particularly important for people with impaired renal function, including the elderly. Adopting a more plant‐based diet would also improve the sustainability of food sources and reduce harm to the environment from a meat‐based diet.
Sources of Funding
None.
Disclosures
Professor Spence is a consultant to Amgen and Orphan Technologies and an unpaid Scientific Officer of Vascularis Inc. Professor Jenkins has received research grants from Saskatchewan Pulse Growers, the Agricultural Bioproducts Innovation Program through the Pulse Research Network, the Advanced Foods and Material Network, Loblaw Companies Ltd, Unilever, Barilla, the Almond Board of California, Agriculture and Agri‐food Canada, Pulse Canada, Kellogg's Company, Canada, Quaker Oats, Canada, Procter & Gamble Technical Centre Ltd, Bayer Consumer Care (Springfield, NJ), Pepsi/Quaker, International Nut and Dried Fruit Council Foundation Inc., Soy Foods Association of North America, the Coca‐Cola Company (investigator‐initiated, unrestricted grant), Solae, Haine Celestial, the Sanitarium Company, Orafti, the International Tree Nut Council Nutrition Research and Education Foundation, the Peanut Institute, Soy Nutrition Institute, the Canola and Flax Councils of Canada, the Calorie Control Council, the Canadian Institutes of Health Research, the Canada Foundation for Innovation, and the Ontario Research Fund. He has received in‐kind supplies for trials as a research support from the Almond Board of California, Walnut Council of California, American Peanut Council, Barilla, Unilever, Unico, Primo, Loblaw Companies, Quaker (PepsiCo), Pristine Gourmet, Bunge Limited, Kellogg Canada, and White Wave Foods. He has been on the speaker's panel, served on the scientific advisory board, and/or received travel support and/or honoraria from the Almond Board of California, Canadian Agriculture Policy Institute, Loblaw Companies Ltd, the Griffin Hospital (for the development of the NuVal scoring system), the Coca‐Cola Company, EPICURE, Danone, Diet Quality Photo Navigation, Better Therapeutics (FareWell), Verywell, True Health Initiative, Institute of Food Technologists, Soy Nutrition Institute, Herbalife Nutrition Institute, Saskatchewan Pulse Growers, Sanitarium Company, Orafti, the Almond Board of California, the American Peanut Council, the International Tree Nut Council Nutrition Research and Education Foundation, the Peanut Institute, Herbalife International, Pacific Health Laboratories, Nutritional Fundamentals for Health, Barilla, Metagenics, Bayer Consumer Care, Unilever Canada and Netherlands, Solae, Kellogg, Quaker Oats, Procter & Gamble, the Coca‐Cola Company, the Griffin Hospital, Abbott Laboratories, the Canola Council of Canada, Dean Foods, the California Strawberry Commission, Haine Celestial, PepsiCo, the Alpro Foundation, Pioneer Hi‐Bred International, DuPont Nutrition and Health, Spherix Consulting and White Wave Foods, the Advanced Foods and Material Network, the Canola and Flax Councils of Canada, the Nutritional Fundamentals for Health, Agri‐Culture and Agri‐Food Canada, the Canadian Agri‐Food Policy Institute, Pulse Canada, the Saskatchewan Pulse Growers, the Soy Foods Association of North America, the Nutrition Foundation of Italy, Nutra‐Source Diagnostics, the McDougall Program, the Toronto Knowledge Translation Group (St. Michael's Hospital), the Canadian College of Naturopathic Medicine, The Hospital for Sick Children, the Canadian Nutrition Society, the American Society of Nutrition, Arizona State University, Paolo Sorbini Foundation, and the Institute of Nutrition, Metabolism and Diabetes. He received an honorarium from the US Department of Agriculture to present the 2013 W.O. Atwater Memorial Lecture. He received the 2013 Award for Excellence in Research from the International Nut and Dried Fruit Council. He received funding and travel support from the Canadian Society of Endocrinology and Metabolism to produce mini cases for the Canadian Diabetes Association. He is a member of the International Carbohydrate Quality Consortium. His wife, Alexandra L. Jenkins, is a director and partner of INQUIS Clinical Research for the Food Industry, his 2 daughters, Wendy Jenkins and Amy Jenkins, have published a vegetarian book that promotes the use of the low glycemic index plant foods advocated here, The Portfolio Diet for Cardiovascular Risk Reduction (Academic Press/Elsevier 2020) and his sister, Caroline Brydson, received funding through a grant from the St. Michael's Hospital Foundation to develop a cookbook for 1 of his studies. Sievenpiper has received research support from the Canadian Foundation for Innovation, Ontario Research Fund, Province of Ontario Ministry of Research and Innovation and Science, Canadian Institutes of Health Research, Diabetes Canada, PSI Foundation, Banting and Best Diabetes Centre, American Society or Nutrition, INC International Nut and Dried Fruit Council Foundation, National Dried Fruit Trade Association, National Honey Board, International Life Sciences Institute, The Tate and Lyle Nutritional Research Fund at the University of Toronto, The Glycemic Control and Cardiovascular Disease in Type 2 Diabetes Fund at the University of Toronto (a fund established by the Alberta Pulse Growers), and the Nutrition Trialists Fund at the University of Toronto (a fund established by an inaugural donation from the Calorie Control Council). He has received in‐kind food donations to support a randomized controlled trial from the Almond Board of California, California Walnut Commission, American Peanut Council, Barilla, Unilever, Upfield, Unico/Primo, Loblaw Companies, Quaker, Kellogg Canada, WhiteWave Foods, and Nutrartis. He has received travel support, speaker fees, and/or honoraria from Diabetes Canada, Dairy Farmers of Canada, FoodMinds LLC, International Sweeteners Association, Nestlé, Pulse Canada, Canadian Society for Endocrinology and Metabolism, GI Foundation, Abbott, Biofortis, American Society or Nutrition, Northern Ontario School of Medicine, INC Nutrition Research & Education Foundation, European Food Safety Authority, Comité Européen des Fabricants de Sucre, and Physicians Committee for Responsible Medicine. He has or has had ad hoc consulting arrangements with Perkins Coie LLP, Tate & Lyle, Wirtschaftliche Vereinigung Zucker e.V., and Inquis Clinical Research. He is a member of the European Fruit Juice Association Scientific Expert Panel and Soy Nutrition Institute Scientific Advisory Committee. He is on the Clinical Practice Guidelines Expert Committees of Diabetes Canada, European Association for the Study of Diabetes, Canadian Cardiovascular Society, and Obesity Canada. He serves or has served as an unpaid scientific advisor for the Food, Nutrition, and Safety Program and the Technical Committee on Carbohydrates of International Life Sciences Institute North America. He is a member of the International Carbohydrate Quality Consortium, Executive Board Member of the Diabetes and Nutrition Study Group of the European Association for the Study of Diabetes, and Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. His wife is an employee of AB InBev. Dr Srichaikul has no disclosures to report. Additional information is available from the corresponding author on request.
Supporting information
Supplemental References
(J Am Heart Assoc. 2021;10:e017066. DOI: 10.1161/JAHA.120.017066.)
The opinions expressed in this article are not necessarily those of the editors or of the American Heart Association.
Supplementary Material for this article is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.120.017066
For Sources of Funding and Disclosures, see page 5.
REFERENCES
- 1. Spence JD, Jenkins D. Cardiovascular benefit of egg consumption is most unlikely. Heart. 2018;104:1805–1806. DOI: 10.1136/heartjnl-2018-313687. [DOI] [PubMed] [Google Scholar]
- 2. Huang J, Liao LM, Weinstein SJ, Sinha R, Graubard BI, Albanes D. Association between plant and animal protein intake and overall and cause‐specific mortality. JAMA Intern Med. 2020;180:1173–1184. DOI: 10.1001/jamainternmed.2020.2790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kearns CE, Schmidt LA, Glantz SA. Sugar industry and coronary heart disease research: a historical analysis of internal industry documents. JAMA Intern Med. 2016;176:1680–1685. DOI: 10.1001/jamainternmed.2016.5394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Barnard ND, Long MB, Ferguson JM, Flores R, Kahleova H. Industry funding and cholesterol research: a systematic review. Am J Lifestyle Med. 2020. DOI: 10.1177/1559827619892198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Greger M. False and misleading claims by egg marketers. 2013. Available at: http://nutritionfacts.org/video/eggs‐and‐cholesterol‐patently‐false‐and‐misleading‐claims/. Accessed May 20, 2015.
- 6. Fielding CJ, Havel RJ, Todd KM, Yeo KE, Schloetter MC, Weinberg V, Frost PH. Effects of dietary cholesterol and fat saturation on plasma lipoproteins in an ethnically diverse population of healthy young men. J Clin Invest. 1995;95:611–618. DOI: 10.1172/JCI117705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Spence JD, Solo K. Resistant atherosclerosis: the need for monitoring of plaque burden. Stroke. 2017;48:1624–1629. DOI: 10.1161/STROKEAHA.117.017392. [DOI] [PubMed] [Google Scholar]
- 8. Spence JD, Jenkins DJ, Davignon J. Dietary cholesterol and egg yolks: not for patients at risk of vascular disease. Can J Cardiol. 2010;26:e336–e339. DOI: 10.1016/s0828-282x(10)70456-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Drouin‐Chartier JP, Chen S, Li Y, Schwab AL, Stampfer MJ, Sacks FM, Rosner B, Willett WC, Hu FB, Bhupathiraju SN. Egg consumption and risk of cardiovascular disease: three large prospective US cohort studies, systematic review, and updated meta‐analysis. BMJ. 2020;368:m513. DOI: 10.1136/bmj.m513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Willett W, Rockstrom J, Loken B, Springmann M, Lang T, Vermeulen S, Garnett T, Tilman D, DeClerck F, Wood A, et al. Food in the Anthropocene: the EAT‐Lancet Commission on healthy diets from sustainable food systems. Lancet. 2019;393:447–492. DOI: 10.1016/S0140-6736(18)31788-4. [DOI] [PubMed] [Google Scholar]
- 11. Rose G. Sick individuals and sick populations. Int J Epidemiol. 2001;30:427–432. DOI: 10.1093/ije/30.3.427. [DOI] [PubMed] [Google Scholar]
- 12. Trichopoulou A, Psaltopoulou T, Orfanos P, Trichopoulos D. Diet and physical activity in relation to overall mortality amongst adult diabetics in a general population cohort. J Intern Med. 2006;259:583–591. DOI: 10.1111/j.1365-2796.2006.01638.x. [DOI] [PubMed] [Google Scholar]
- 13. Zhong VW, Van Horn L, Cornelis MC, Wilkins JT, Ning H, Carnethon MR, Greenland P, Mentz RJ, Tucker KL, Zhao L, et al. Associations of dietary cholesterol or egg consumption with incident cardiovascular disease and mortality. JAMA. 2019;321:1081–1095. DOI: 10.1001/jama.2019.1572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhong VW, Van Horn L, Greenland P, Carnethon MR, Ning H, Wilkins JT, Lloyd‐Jones DM, Allen NB. Associations of processed meat, unprocessed red meat, poultry, or fish intake with incident cardiovascular disease and all‐cause mortality. JAMA Intern Med. 2020;180:503–512. DOI: 10.1001/jamainternmed.2019.6969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Argyridou S, Zaccardi F, Davies MJ, Khunti K, Yates T. Relevance of physical function in the association of red and processed meat intake with all‐cause, cardiovascular, and cancer mortality. Nutr Metab Cardiovasc Dis. 2019;29:1308–1315. DOI: 10.1016/j.numecd.2019.06.019. [DOI] [PubMed] [Google Scholar]
- 16. Tang WHW, Wang Z, Levinson BS, Koeth RA, Britt EB, Fu X, Wu Y, Hazen SL. Intestinal microbiota metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368:1575–1584. DOI: 10.1056/NEJMoa1109400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Miller CA, Corbin KD, da Costa KA, Zhang S, Zhao X, Galanko JA, Blevins T, Bennett BJ, O'Connor A, Zeisel SH. Effect of egg ingestion on trimethylamine‐N‐oxide production in humans: a randomized, controlled, dose‐response study. Am J Clin Nutr. 2014;100:778–786. DOI: 10.3945/ajcn.114.087692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Wang Z, Bergeron N, Levison BS, Li XS, Chiu S, Jia X, Koeth RA, Li L, Wu Y, Tang WHW, et al. Impact of chronic dietary red meat, white meat, or non‐meat protein on trimethylamine N‐oxide metabolism and renal excretion in healthy men and women. Eur Heart J. 2019;40:583–594. DOI: 10.1093/eurheartj/ehy799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Spence JD, Tangney C. Lower risk of stroke with a vegetarian diet. Neurology. 2020;94:463–464. DOI: 10.1212/WNL.0000000000009092. [DOI] [PubMed] [Google Scholar]
- 20. Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: systematic review and dose‐response meta‐analysis of prospective cohort studies. BMJ. 2020;370:m2412. DOI: 10.1136/bmj.m2412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Bogiatzi C, Gloor G, Allen‐Vercoe E, Reid G, Wong RG, Urquhart BL, Dinculescu V, Ruetz KN, Velenosi TJ, Pignanelli M, et al. Metabolic products of the intestinal microbiome and extremes of atherosclerosis. Atherosclerosis. 2018;273:91–97. DOI: 10.1016/j.atherosclerosis.2018.04.015. [DOI] [PubMed] [Google Scholar]
- 22. Poesen R, Claes K, Evenepoel P, de Loor H, Augustijns P, Kuypers D, Meijers B. Microbiota‐derived phenylacetylglutamine associates with overall mortality and cardiovascular disease in patients with CKD. J Am Soc Nephrol. 2016;27:3479–3487. DOI: 10.1681/ASN.2015121302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Nemet I, Saha PP, Gupta N, Zhu W, Romano KA, Skye SM, Cajka T, Mohan ML, Li L, Wu Y, et al. A cardiovascular disease‐linked gut microbial metabolite acts via adrenergic receptors. Cell. 2020;180:862–877.e22. DOI: 10.1016/j.cell.2020.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Al‐Shaar L, Satija A, Wang DD, Rimm EB, Smith‐Warner SA, Stampfer MJ, Hu FB, Willett WC. Red meat intake and risk of coronary heart disease among US men: prospective cohort study. BMJ. 2020;371:m4141. DOI: 10.1136/bmj.m4141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Pignanelli M, Bogiatzi C, Gloor G, Allen‐Vercoe E, Reid G, Urquhart BL, Ruetz KN, Velenosi TJ, Spence JD. Moderate renal impairment and toxic metabolites produced by the intestinal microbiome: dietary implications. J Ren Nutr. 2019;29:55–64. DOI: 10.1053/j.jrn.2018.05.007. [DOI] [PubMed] [Google Scholar]
- 26. Spence JD, Urquhart BL, Bang H. Effect of renal impairment on atherosclerosis: only partially mediated by homocysteine. Nephrol Dial Transplant. 2016;31:937–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Spence JD, Azarpazhooh MR, Larsson SC, Bogiatzi C, Hankey GJ. Stroke prevention in older adults: recent advances. Stroke. 2020;51:3770–3777. DOI: 10.1161/STROKEAHA.120.031707. [DOI] [PubMed] [Google Scholar]
- 28. Shan Z, Li Y, Baden MY, Bhupathiraju SN, Wang DD, Sun Q, Rexrode KM, Rimm EB, Qi L, Willett WC, et al. Association between healthy eating patterns and risk of cardiovascular disease. JAMA Intern Med. 2020;180:1090–1100. DOI: 10.1001/jamainternmed.2020.2176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Keys A. Mediterranean diet and public health: personal reflections. Am J Clin Nutr. 1995;61:1321S–1323S. DOI: 10.1093/ajcn/61.6.1321S. [DOI] [PubMed] [Google Scholar]
- 30. Hu Y, Ding M, Sampson L, Willett WC, Manson JE, Wang M, Rosner B, Hu FB, Sun Q. Intake of whole grain foods and risk of type 2 diabetes: results from three prospective cohort studies. BMJ. 2020;370:m2206. DOI: 10.1136/bmj.m2206. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental References