

A 53-year-old man with HIV-1 and heterotaxy syndrome with polysplenism and left atrial isomerism presented to HIV clinic to establish care. Prior imaging revealed dextrocardia on chest radiograph (Fig. 1). Computed tomography of the chest, abdomen, and pelvis demonstrated a midline liver and right upper quadrant polysplenism (Fig. 2).
Figure 1.
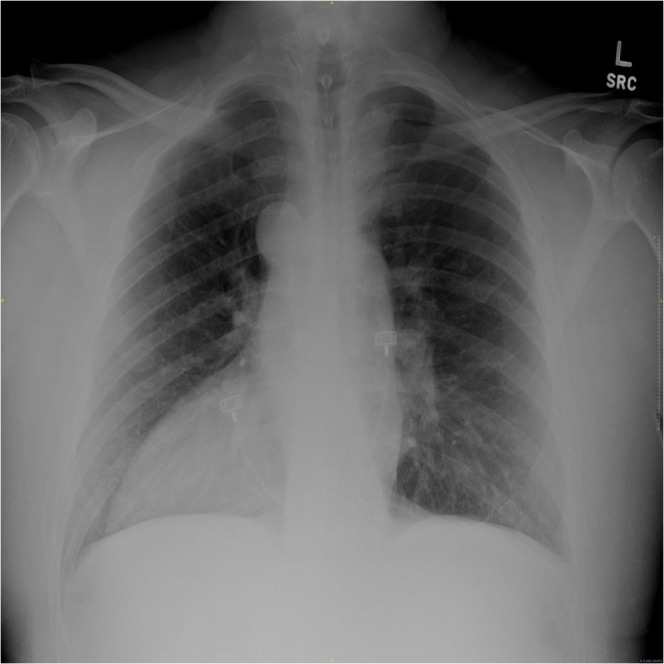
Chest radiograph demonstrating dextrocardia.
Figure 2.

Axial cross-section of a computed tomography abdomen pelvis showing polysplenia (*) in the right upper quadrant and white arrows pointing to a right-sided stomach and midline liver.
Situs solitus is the typical internal anatomy consisting of a right-sided tri-lobed lung, liver, gallbladder, inferior vena cava and left-sided bi-lobed lung, spleen, and aorta. The mirror-image to situs solitus is situs inversus totalis. In contrast, situs ambiguus, or heterotaxy syndrome, refers to variable arrangements of visceral malposition without a single pathognomic anomaly.1 Heterotaxy is stratified by its atrial isomerism, defined as abnormal internal symmetry with either bilateral paired right or left cardiac atria.2 Dextrocardia may accompany any of these conditions.1
Heterotaxy with right atrial isomerism generally exhibits bilateral tri-lobed lungs, asplenia, and severe cardiac abnormalities.2 Heterotaxy with left atrial isomerism includes bilateral bi-lobed lungs, midline or right-sided liver, polysplenism, and mild cardiac defects.2–4 Prognosis depends on the degree of cardiac malformation. Right atrial isomerism portends 85% mortality in the first year, compared to 50% for left atrial isomerism, while most patients with situs inversus can lead healthy lives relatively unaffected.4, 5
Declarations
Conflict of Interest
The authors declare that there are no conflicts to report.
Footnotes
Prior Presentations
None.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002;22:1439–56. doi: 10.1148/rg.226025016. [DOI] [PubMed] [Google Scholar]
- 2.Jacobs JP, Anderson RH, Weinberg PM, et al. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. Cardiol Young. 2007;17(Suppl 2):1–28. doi: 10.1017/S1047951107001138. [DOI] [PubMed] [Google Scholar]
- 3.Winer-Muram HT, Tonkin IL. The spectrum of heterotaxic syndromes. Radiol Clin North Am. 1989;27:1147–70. [PubMed] [Google Scholar]
- 4.Kim SJ. Heterotaxy syndrome. Korean Circ J. 2011;41:227–32. doi: 10.4070/kcj.2011.41.5.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Garofano-Jerez JM, Benedicto-Hernandez E, Gila JDLG, et al. Imaging evaluation of the heterotaxy syndrome. Gastroenterol Hepatol Open Access. 2019;10(2):75–80. doi: 10.15406/ghoa.2019.10.00359. [DOI] [Google Scholar]