

Abstract
More patients are requesting fixed prosthesis to replace missing teeth. More than 5 million dental implants are placed annually in the United States. This number will decrease in 2020 owing to the coronavirus disease-19 pandemic. The edentulous patient has a decreased quality of life. Prosthodontic rehabilitation/reconstruction of edentulism improves overall quality of life. Patient-reported outcome measures are subjective reports of patients’ perceptions of their oral health status and the impact that it has on their quality of life. This chapter contains a variety of prosthodontic principles for the reader to help satisfy the needs and expectations of the patient.
Keywords: Personal protective equipment (PPE), Implant-protective occlusion (IPO), Patient-reported outcome measures (PROM), Quality of life (QOL), Oral rehabilitation/reconstruction, Fixed dental prostheses (FDP), Implant overdentures (IOD), Implant-supported fixed complete dental prostheses (IFCDPs)
Key points
-
•
Since the coronavirus disease 2019 pandemic, several businesses have closed and many people have been left jobless.
-
•
The current recession will have a negative impact on dentists and dental offices in the United States and worldwide.
-
•
The modern-day dentist will need to be conservative and may need to implement payment plans as means to encourage patients to invest in implant treatment.
-
•
Long spanned and/or complex implant cases should have mandatory occlusal-protected appointments.
-
•
The general practitioner is challenged on a daily basis to make clinical decisions based off of the patient’s anatomy, needs, and wishes, in order, to select the best prostheses.
More than 5 million dental implants are placed annually by dentists in the United States, according to the American Dental Association. Oral health enhances a patients' quality of life.1 Pjetursson and colleagues2 , 3 reported that “the survival rates of implant-supported single crowns and fixed dental prostheses (FDPs) range between 89% and 94% at 10 years.
The current pandemic of coronavirus disease 2019 (COVID-19) has caused >1 million deaths worldwide and >230,000 deaths in the United States, and these numbers are growing every day. On a brighter note, more than 30 million people have recovered worldwide. Coronaviruses are a group of viruses that can cause a variety of respiratory illnesses (ie, pneumonia) that can lead to respiratory failure. SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) was renamed COVID-19 (coronavirus disease 2019). Current medical/ dental literature on the COVID-19 pandemic suggests that dentists, oral surgeons, and otolaryngologists–head and neck surgeons are at high risk of contagion owing to the exposure to saliva, blood, aerosol, and droplets.4 , 5 This crisis has resulted in people being quarantined in their homes (in attempts to contain the spread of the virus), schools closing, restaurants closing, businesses cutting staff or closing themselves, and ultimately leading to millions of people losing their jobs (income). More than 30 million people in the United States have claimed themselves jobless (unemployed) at the end of April, 2020. The recession in the United States will eventually rebound in a positive direction with time. At the beginning of the pandemic, the effect on dentists and staff were challenging owing to some office closings and the temporary hold on all elective procedures (recommended by state governors), while only focusing on dental emergencies. The dental implant market in the United States and globally will take a hit financially during the pandemic. There will be patients who were able to afford implants (before the pandemic) who will be unaffected, there may be another working class who (once were able) may not be in a position to afford or consider implants as a necessity. The modern-day dentist should be understanding, may have to be more conservative with their patients’ treatment plan, and suggest to them ways of investing in an implant 1 or 2 at a time. The dental office may need to implement down payments or payment plans (before treatment) as a way of encouraging implant care. This consideration can be extended by the doctor that has a heart for providing quality dentistry for their fellow man or woman, that is, the patient. The modern-day dentist or general practitioner (GP) should implement reproducible treatment protocols, which will propel more successful outcomes.6 The 5 concepts for dental implant success include (1) past medical history, (2) examination and occlusion, (3) dental imaging, (4) fixed verses removable prosthodontics, and (5) surgery, and are reviewed in this article (Fig 1 ).7 The goal is to bring forth proven contributions of evidence based dentistry in the complex discipline of dental implantology in a format that will strengthen the decision making process of the GP in the clinical setting. At the end of this article, the reader will be able to make efficient, intelligent, and methodical treatments based off current scientific research (systemic reviews, randomized controlled trials, meta-analysis, and retrospective studies) and the foundation of textbooks on dental implantology. The objective during this challenging time in our profession is to make dental implants affordable for the patient, enhance their ability to function, improve their aesthetics, and improve their overall quality of life. Pictures (from cases) have been included to describe certain topics discussed, is in no way to lead or influence the GP to use a particular treatment. The pictures are to be used as visual aids to bring light to the literature being discussed. Because there are so many variables mentioned in this article, the reader should always consider whatever works for them or more conservative approaches when it comes to their case(s).
Fig. 1.

The 5 concepts for dental implant success.
(Courtesy of Ricardo A. Boyce, DDS, FICD. © 2015.)
The first discussion will be on the use of personal protective equipment (PPE) for the safety of the doctor(s), dental hygienist, and staff. The Centers for Disease Control and Prevention and other state and local health department have continued to instruct and respond to the outbreak of the COVID-19 respiratory disease. All patients should be triaged over the phone, queried about any recent travel histories, if they have tested positive for COVID-19 (or awaiting test results), if they have a fever (>100.4°F), chills, shaking, body aches, headache, itchy throat, dry throat, dry cough, shortness of breath, or loss of smell or taste. They should also be asked if their family members or loved ones (having contact) have had the virus. The patients should be instructed to wear some sort of mask or face covering to protect themselves and others before their office visit. Please note that the questions mentioned should be followed up on arrival to the dental clinic. All members of the health care team (dentists, dental hygienists, dental assistants, and receptionist) should be wearing masks and washing their hands throughout the day and be prepared to triage all patients (before any treatment). The temperature should be taken with a contact-free forehead thermometer. Patients should have a review of systems and their vitals (temperature) checked before treatment. Those patients that present to the office (or queried over the phone) with a fever (>100.4°F) and any of the other symptoms mentioned should not be treated and given another appointment at least 2 weeks from the date (or until the patient is cleared from the virus/disease).8 , 9 The dentist can prescribe acetaminophen (if the patient does not have in their possession or at home) should any fever exist and be instructed to contact their physicians and/or specialists for medical advice (a medical consult can be written). If the patient presents with symptoms of new confusion, dyspnea, severe dysphagia, airway compromise, bluish lips (or face), persistent pain or pressure in the chest, and fever, then emergency medical services should called immediately. Until more is learned about this virus, appointments should be booked to allow social distancing in the reception area and every patient should be treated as if they were COVID-19 positive. The use of air purifiers or air scrubbers (with HEPA filters and UVC light disinfection) can be considered for each treatment room. The rooms to be allowed to be aired out (or with the windows open) in between cases. Dental procedures can be performed if there is absence of contacts and/or symptoms.5 High-speed handpieces and ultrasonic devices should be minimized; the use of rubber dams are highly recommended.8 , 9
When patients arrive they should be given level 1 masks (if they do not present with one) to wear in waiting room. The goal of the office staff should be to protect all patients and staff. When the procedures are about to start, all staff (in the surgical room) should be wearing N-95 or KN95 or level 3 (depending on the procedure) masks or masks with a face shield or goggles and/or a separate face shield; in addition, a full-length gown should also be worn. The clinician can review a list of guidelines and recommendations from the Centers for Disease Control and Prevention’s website (https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html). Good judgment for PPE should be used for the type of procedure, because it can be adjusted for minor follow-up procedures. The dental staff should perform hand hygiene using alcohol-based hand sanitizer and alcohol hand rubs before and after all patient contact, contact with potentially infectious material, and before putting on and upon removal of PPE, including gloves. The recommendation is to wash hands with soap and water for at least 20 seconds. If hands are visibly soiled, use soap and water before returning to alcohol-based hand sanitizer.
The donning (putting on) and doffing (taking off) should be done by those health care workers who are treating and in direct contact with patients. Those dental professionals who work in a hospital or have to consult COVID-19–infected patients (on the floors) may feel more comfortable using a P 100 or N 100 mask instead of an N-95 mask. Any clinician who will be performing implant procedures in the hospital operating room will be practicing surgical scrubbing, gowning, and gloving, and others can obtain a more detailed description of donning and doffing on the Centers for Disease Control and Prevention’s website (https://www.cdc.gov/hai/pdfs/ppe/ppe-sequence.pdf).
Good oral health is a shared responsibility between the patient and the dental provider. Patients must be informed and motivated to perform their daily home care duties until their next visit (or recall). Prudent safety recommendations for the GP providing care for implants in the ambulatory setting/dental office include but are not limited to (1) placing the patient in an upright position (whenever possible), (2) placement of a 4 × 4 gauze in the area of the oropharynx to protect objects falling (if the office does not have them, a 2 × 2 will be suffice, unfolding it will be even better), and (3) attach dental floss to Hex tools (Fig. 2 ). In the unlikely case an implant part should accidently be swallowed by the patient, they will need to be directed to the nearest hospital for a chest radiograph.
Fig. 2.

Restorative tools with floss attached to prevent aspiration.
The GP often instructs the patient how to maintain their dentition, as well as, having the following extended responsibilities: (1) obtain a good medical history, (2) request a medical consult with the patient’s physician or specialist (when necessary), (3) obtain necessary laboratory tests based on the patient’s past medical history (ie, complete blood count with differential, hemoglobin A1c, international normalized ratio, etc), and (4) inform the patient of their risk factors associated with dental implant placement. An updated list of medical conditions with risk factors for failure or potential complications of implant placement are provided in Box 1 .7
Box 1. Risk factors for implant placement.
| Moderate to severe neutropenia | Atypical odontalgia or atypical facial pain |
| Patients on corticosteroids | Radiation therapy to the head and neck |
| Cancer chemotherapy | Myocardial infarction within 6 mo |
| Patients on IV bisphosphonates | Gravid patient |
| Poorly controlled diabetics | Heavy smoking habits |
| Malignancy/terminal illness | Cluster phenomenon |
| Psychological instability | Parafunctional habits |
| Selective serotonin reuptake inhibitors | Proton Pump Inhibitors |
There are several documented literatures on the cluster phenomenon10, 11, 12 and parafunctional habits associated with implant failure.13 Rose and colleagues14 stated that “meticulous screening and patient selection can help reduce the risk of failure or potential complications during implant treatment.” Potential complications in the risk factor category include to discomfort, pain, and purulence. Patients with multiple comorbidities and taking multiple medications may be potential risks for implant failure. Systematic reviews and meta-analysis have proved that there is a statistically significant increased implant failure rate with patients on selective serotonin reuptake inhibitors and proton pump inhibitors.15 If the patient (symptomatic or asymptomatic) asks for the implant to be removed owing to any of the aforementioned reasons (included in Box 1), the implant is considered to have failed.
Individual risk assessments are necessary before implant surgery.16 In light of COVID-19, geriatric patients with serious chronic diseases (ie, pulmonary, cardiac, etc) may be at increased risk of sudden death; therefore, medical consults should be sent to physicians and specialist before implant surgery (now more than ever). As for these older patients, it may be safe and wise to provide alternative prosthodontic treatment in the form of conventional partial dentures and/or complete dentures.
The GP should be skilled enough to handle the implant case and if not then refer the patient to a dental specialist who can execute surgical strategies for the various hard and soft tissue deficiencies, such as (1) anatomic preconditions, (2) lack of keratinized mucosa, (3) local diseases affecting the teeth and implants, (4) mechanical overload, (5) tissue morphology and phenotype, (6) expansion of the floor of the sinus, (7) extraction(s), (8) trauma to orofacial structures, (9) migration of teeth and malpositioning of implants, and (10) iatrogenic factors.17
Chiapasco and colleagues18 listed 5 main methods to augment the local bone volume at deficient sites as follows: (a) osteoinduction by the use of growth factors; (b) osteoconduction where a grafting material serves as a scaffold; (c) distraction osteogenesis, by which a fracture is surgically induced and then pulled apart; (d) guided bone regeneration, which allows spaces maintained by barrier membranes to be filled with bone; and (e) revascularized bone grafts, where vital bone segment is transferred to its recipient bed with its vascular pedicle. There are different regenerative techniques that can be implemented to reconstruct deficient alveolar ridges, namely, lateral, vertical, or combined bone augmentation.19 The approaches to achieve this reconstruction is by the use of bone blocks, particulated grafts, and/or barrier membranes. There are a variety of biomaterials that can be applied, including autogenous, allogenic, xenogenic, and synthetic bone substitute (resorbable and nonresorbable).20 The goal is to achieve primary stability of the implant and avoid any micro movement, which could lead to poor revascularization of the graft site.
There are no well-documented series of scientific studies that show the superiority of an implant company over another. The most important biological event (of osteointegration) is in the clinical healing phase of the dental implant is cell adhesion at the interface between it and the host tissue.21 A meta-analysis and systematic reviews have showed that rough-surfaced implants demonstrated favorable results compared with machined implants.6 Ogle21 also stated that “the success and failure is more dependent on patient related, procedural, and prosthetic parameters than implant shape.”
Clinicians interested in short implants (≤6 mm) should be mindful that studies have shown higher rates of prosthetic complications (microrotation and rocking).22 , 23 The complications and rotational movements seem to decrease when the prostheses were splinted. Meta-analysis of randomized clinical trials reported that long implants show a higher survival rate than extrashort implants (after a 5-year timeframe).24
Chen and Buser25 published a list of protocols for implant placement after extractions: (a) type 1 (immediate implant placement): the implants are placed on the same day as the extraction; (b) type 2 (early implant placement): the implants are placed 1 to 2 months after the extraction; (c) type 3 (delayed implant placement): the implants are placed 3 to 4 months after the extraction; and (d) type 4 (late or conventional placement): 4 to 6 months or greater after implant placement. The patient who presents with infection in the bone may benefit from the delayed or late/conventional to improve the chances of success. In cases where there is difficulty in achieving primary stability (and challenges to stabilize the implant), good clinical judgment would be to consider a conventional loading approach to avoid micromovements to increase the survival rate, which directly impacts the affect the esthetic outcome. Canellas and colleagues26 showed a statistically significant difference in favor of delayed implant placement in their meta-analysis. Gallucci and colleagues27 created a comprehensive protocol combining implant placement and loading (Fig. 3 , highlighting the well documented and insufficiently documented cases):
-
•
Type 1A: immediate placement and immediate restoration/loading
-
•
Type 1B: immediate placement and early restoration/loading
-
•
Type 1C: immediate placement and conventional restoration/loading
-
•
Type 2A: early placement with soft tissue healing and immediate restoration/loading
-
•
Type 2B: early placement with soft tissue healing and early restoration/loading
-
•
Type 2C: early placement with soft tissue healing and conventional restoration/loading
-
•
Type 3A: early placement with partial bone healing and immediate restoration/loading
-
•
Type 3B: early placement with partial bone healing and early restoration/loading
-
•
Type 3C: early placement with partial bone healing and conventional restoration/loading
-
•
Type 4A: late placement and immediate restoration/loading
-
•
Type 4B: late placement and early restoration/loading
-
•
Type 4C: late placement and conventional restoration/loading
Fig. 3.

Classification according to implant placement and healing protocol.
(From Gallucci GO, Hamilton A, Zhou W, et al. Implant placement and loading protocols in partially edentulous patients: A systemic review. Clin Oral Implants Res. 2018;29(Suppl 16):126; with permission.)
Gallucci and colleagues27 stated that type 1C is the most scientifically and clinically validated approach. The most documented approach, type 4C, is the standard of care when treatment modifiers such as bone augmentation, low insertion torque, reduced diameter implants, and patient local and systemic factors are present. The Group 2 ITI Consensus Report reviewed these new implant protocols for descriptive analysis: (a) immediate implant placement, same day as the extraction(s); (b) early implant placement: (soft tissue healing) 4 to 8 weeks or (partial bone healing) 12 to 16 weeks after the tooth extraction(s); and (c) late implant placement: placed after complete bone healing, more than 6 months after tooth extraction.28 The implant loading protocols defined as follows: (a) immediate loading: dental implants are connected to a prosthesis in occlusion with the opposing arch within 1 week subsequent to implant placement; (b) immediate restoration: dental implants are connected to a prosthesis, held out of occlusion with the opposing arch within 1 week subsequent to implant placement; (c) early loading: dental implants are connected to the prosthesis between 1 week and 2 months after implant placement; and (d) conventional loading: dental implants are allowed a healing period of more than 2 months after implant placement with no connection of the prosthesis.28
Morton and colleagues28 showed the percentage of the survival rates for the new set of protocols (types 1A–4C; see Fig. 3). Their consensus statement on this topic revealed a 98% survival rate with type 1A (yellow); a 98% survival rate with type 1B (yellow); a 96% survival rate with type 1C (green); types 2A and 2B both have clinically insufficient documentation (red); a 96% survival rate with type 2C (green); a 98% survival rate with type 4A (yellow); a 98% survival rate with 4B(green); and a 98% survival rate with type 4C(green). The reader should be mindful there is no gold standard for implant placement after extraction(s); however, the implant placement and loading protocol should be planned before surgery.28
Establishing proper occlusion can dictate the success of each case. Occlusal treatment at the time of delivery and at follow-up visits cannot be overemphasized. Several studies29 , 30 have proven that most reported complications (prosthetic or bony) are associated with occlusion. In dental implantology, another form of dental implant complication(s) refer to “a problem with any of the replaceable components of the implant system.”31 Misch stated that “most common complications of the implant prostheses relate to biomechanical factors, such as porcelain fracture, unretained prostheses (cement or screw), abutment screw loosening, early implant failure after loading, and implant component fracture.32, 33, 34 The GP is encouraged to implement an occlusal plan to provide an implant-protective occlusion to decrease biomechanical complications and improve clinical longevity.32, 33, 34, 35 It has been documented that the implant system handles the stress of mastication and occlusal interferences poorly.32 If occlusal treatment visits are not properly provided for the patient it can result in implant(s) failure. The benefits of implant-protective occlusion are as follows: (1) no premature occlusal contacts or interferences, (2) mutually protected articulation, (3) implant body angle to occlusal load, (4) cusp angle of crowns, (5) cantilever or offset loads, (6) crown height (vertical height), (7) implant crown contour, (8) occlusal contact position, (9) timing of occlusal contacts, and (10) protect the weakest component.32 The screw could fracture as a result of occlusal overload or torqueing beyond the manufacturer’s recommendation. The sequence of internal mechanical complications of the screw that can lead to failure are as follows: the screw loosening leading → screw bending; the screw bending leading → screw fracturing; and screw fracturing leading → fracturing of the platform of the implant, which could ultimately lead to failure of the implant. It is recommended that all bent screws be replaced by new ones before retorqueing, owing to the high risk of breakage (this can be requested by the manufacturer or the dental laboratory). It is important to note that, after the implant placement, the cover screw, healing cap, and temporary crown should be hand torqued until delivery of the final restoration(s) or prostheses when it will be torqued according to the manufacturer’s recommendation. There are a few times when skillful clinicians may be fortunate enough to remove a broken screw embedded within the implant. If not possible, the implant may have to be buried (leaving it nonfunctional) or be removed (trephination) or a cast post/core and crown be cemented. If a problem like one of these described occur in the office then referral to a specialist would be recommended.
Papaspyridakos and colleagues35 revealed in their systematic review that “wears” are the most common minor complication and “fracture of the prosthetic material” are the major complication with implant-supported fixed complete dental prostheses for the edentulous patients. They went further to recommend for patients to wear nightguards to prevent any complications of the prostheses. A more current retrospective study (with 1–12 years of follow-up) of implant-supported fixed complete dental prostheses detailed (the annual rate in percentage) of minor complications as (1) wear of the prosthetic material (9.8%), (2) decementation of cement retained implant-supported fixed complete dental prostheses (2.9%), and (3) loss of the screw access filling material (2.7%).36 The annual rate of major complications from this same study are as follows: (1) fracture of prosthetic material (1.9%), (2) fracture of the occlusal screw (0.3%), and (3) fracture of the framework (0.3%).36 Moreover, to avoid repairs, remakes, and wasted chair time, a nightguard as a part of the final delivery is recommended.36 The use of nightguards and orthodontic retainers have been recommended in the partially dentate patient (with implants) to prevent interproximal contact loss, which could lead to peri-implantitis.37 There are a number of clinical complications published in the literature that may compromise the successful outcome of dental implants (ie, biologic, technical/mechanical, esthetic, or phonetic).38 , 39 Heitz-Mayfield and colleagues16 stated that “Bleeding on probing (BOP) has a positive predictive value (7% to 58%) for the diagnosis of peri-implantitis.” Peri-implant mucositis characteristically includes BOP, and/or suppuration, probing depths of less than 4 mm with no evidence of bone loss (is reversible), is considered a precursor to peri-implantitis.40 A diagnosis of peri-implantitis involves evidence of inflammation, infection, and progressive bone loss (classified as mild, moderate, or severe), if not treated can lead to failure of the implant.
Over the past 2 decades, cone beam computed tomography has proved to become a valuable armamentarium in dental implantology treatment planning (Fig. 4 ).41 , 42 This 3-dimensional imaging modality allows the clinicians the ability to access bone density before implant placement, measure the bone height, and width to properly predict the placement of the implant more accurately.43 This allows the GP (along with the help of the dental laboratory) the ability to develop a more “prosthetically driven” process, to allow the patient the option of receiving a prosthesis on the day of surgery. Moreover, this outcome should never be promised to the patient because of the possibility of complications that can occur somewhere in the case (ie, unsatisfactory aesthetics). It is imperative that the surgeon use cone beam computed tomography scans to assess vital structures in the image of the maxilla and/or mandible. An awareness and knowledge of surgical anatomy is important to the success of the case. Aziz affirmed that “prevention of an inferior alveolar nerve (IAN) injury is directly related to proper and thorough preoperative implant planning. He also stated, “The etiology of IAN injury is usually associated with inadequate planning or overzealous implant placement (ie, miscalculation).44 This miscalculation can also occur in the area of the maxillary sinuses, the mental foramen, nasopalatine canal, and the lingual concavity of the mandible. There are a variety of virtual systems (Figs. 5 and 6 ) on the market for the clinician to choose from to plan for the placement of implant(s). The modern-day GP can use software to select the implant company, choose the length of the implant, platform size, draw the nerve (if needed), choose virtual teeth (and abutment), and position (move and rotate) the implant to prevent any perforations and fenestrations (Fig 6).
Fig. 4.


(A) Cone beam computed tomography. (B) Axial view of cone beam computed tomography.
Fig. 5.

(A) Shows a cone beam computed tomography with a virtual image of paralleling pins. (B) Virtual image of paralleling pins in the cast and with surgical guide.
Fig. 6.

Virtual Imaging of implant in bone.
In this particular case, we used the virtual company Simplant from a cast and the scanned image(s) to a computer-milled template or tooth supported stereolithographic surgical guide was made to fit the patient (Fig. 7, Fig. 8, Fig. 9, Fig. 10, Fig. 11 ). Note that the amount of bone loss (loss of interdental papilla) in the area of #8 and #9 from a history of trauma, bilateral posterior crossbite, anterior open bite, and overjet (appreciated in picture with paralleling pins, in Fig. 11, Fig. 12, Fig. 13 ).
Fig. 7.

Case #1 of the patients’ occlusion.
Fig. 8.

Surgical guide fitted in the maxilla.
Fig. 9.

Close up image of the surgical guide.
Fig. 10.

Next, the osteotomy being made with surgical guide in place.
Fig. 11.

Placement of the paralleling pins .
Fig. 12.

Sagittal view with paralleling pins.
Fig. 13.

Radiograph of paralleling pins in bone.
In this case, the decision was made to restore at a later date owing to the degree of overjet, which would alter the aesthetics (see Fig. 12). The final placement of implant #8 is shown in Fig. 14 . Implants #8 and #9, completed with postoperative radiograph, are shown in Fig. 15 . The patient's preexisting flipper (Fig. 16 ) was reamed out on the intaglio surface and a soft reline material was placed so that it would not place heavy pressure on the implants #8 and #9. Subsequently, the flipper was taken out of occlusion. Gold custom (UCLA) abutments were milled (Fig.17A ), cotton pellets placed in the vents to protect the screws (see Fig.17B). The occlusion was adjusted, then the connected permanent crowns were cemented (Fig. 18 ).
Fig. 14.

Final placement of the implant #8.
Fig. 15.

Implants #8 and #9 are completed with a postoperative radiograph.
Fig. 16.

Preexistng flipper before taken out of occlusion.
Fig. 17.

Milled Gold custom (UCLA) abutments.
(Courtesy of Milivoj Grego, CDT, MS.)
Fig. 18.

The patient was satisfied with the aesthetic outcome.
(Courtesy of Milivoj Grego, CDT, MS and Ricardo A. Boyce, DDS, FICD.)
The discussion of dental implants are at the forefront of most treatment plans involving any missing tooth or teeth. Today, more patients are requesting edentulous spaces to be restored with FDPs; however, owing to financial constraints (from the current economic recession) it may lead the patient to gradually invest in the fixed partial dentures at a later date. Nonetheless, the GP will need to provide this group of patients with evidenced based knowledge, goals, and treatment to satisfy their needs and expectations.
Many patients may not be ready to lose their periodontally compromised dentition; however, some will eventually transition from removable partial dentures to a complete denture or complete overdentures or implant-supported fixed complete dental prostheses. An early start of implant placement may turn out to be a wise investment for the patient (Fig. 19 ). Wittneben and colleagues45 stated “in partially edentulous patients demanding a fixed rehabilitation, the choice between tooth- or implant-supported fixed dental (FDP’s) needs to be made.” Nonetheless, the patient should be educated about periodontal disease, the “seeding” process of anaerobic bacteria invading the implants which could lead to peri-mucositis or peri-implantitis.7 , 28 This does not mean that their teeth need to be extracted, instead the patient needs to be meticulous about their oral hygiene regimen. The goal of the GP should be to make the oral cavity as clean as possible to receive the initial implant(s), whereas the goal of the patient is to maintain the cleanliness of the oral cavity. Berglundh and colleagues46 stated “there is strong evidence that there is an increased risk of developing peri-implantitis in patients who have a history of severe periodontitis, poor plaque control, and no regular maintenance care after implant therapy.”
Fig. 19.

Upper and lower acrylic removable partial dentures showing retentive elements on the intaglio surface of the RPD. This photo illustrates how the patient may choose to invest incrementally (in Implants) according to their financial budget.
In medicine, patient-reported outcomes are “any report of the status of a patient’s health condition that comes directly from the patient, without interpretation of the patient’s response by a clinician or anyone else.”47 In dentistry, patient-reported outcome measures are “subjective” reports of patients’ perceptions of their oral health status and the impact on the patient’s quality of life.45 , 48 , 49 These are important criteria’s in dental implantology, because patient expectations are increasing and the GP is left with making a decision that must satisfy the patient by the end of the treatment (which could result in additional costs if the patient is not satisfied). A deeper insight and discussion on patient-reported outcome measures is presented elsewhere in this article. Misch32 describes how often times the dental laboratory technician does not get the credit but are largely responsible for the final esthetic result. It is imperative for the restorative dentist or GP to choose a knowledgeable and experienced laboratory technician in the management of complex implant cases. Moreover, the GP should be skilled enough to envision the final outcome of a restoration or prostheses, know how to communicate this vision with the laboratory technician until the finished prosthesis is delivered and the patient is completely satisfied.
Edentulism is considered to be a disability according to the World Health Organizations.50 , 51 The edentulous patient has a reduced quality of life, is at high risk for choking on foods, which could lead to digestive problems or even death. Prosthodontic rehabilitation/reconstruction of edentulism improves a patients’ overall quality of life. In dentistry, the qualities of life include but are not limited to masticatory function, maintenance of weight, reduced gastrointestinal disturbances, psychological well-being, and enhanced esthetics.52 , 53
When there is an improvement in the retention and stability of the implant supported prostheses, it can lead to enhanced speaking, mastication, and swallowing, which can improve the patient’s overall satisfaction.54 The literature suggests for the dentist to consider the patient’s past medical history, risk assessment, expectations, motoric skills, and financial costs before prosthodontic rehabilitation.7 , 55 Even though mandibular implants are considered the standard of care for the edentulous patient, this is not always the case in the maxilla. Edentulous patients with good bony support in the maxilla may not need implant placement. In fact, de Albuquerque Júnior and colleagues,56 stated that “maxillary implant prostheses should not be considered as a general treatment of choice in patients with good bony support,” who are problem free with a maxillary conventional prostheses. This recommendation will be prudent advice for any patient that falls into the high risk category mentioned in Box 1. Removable implant overdentures, along with parts and systems (from the manufacturer or dental laboratory) serves to enhance retention, function, fixation, and stabilization.57 In this particular Cochrane database systemic review, Payne and colleagues52 described the 4 groups of attachment systems for removable implant overdentures as the (1) ball/stud attachment, (2) bar attachment, (3) magnet attachment, and (4) telescopic attachment. The decision of which attachment system to use solely depends on the clinician’s expertise and personal preferences.58 One systematic review brought to light some interesting pearls of wisdom for those who restore overdentures: (1) respect the manufacturers torqueing (screwing) guidelines, (2) share the likelihood of minor complications (ie, adjustments with patients) with the patient to facilitate communication of realistic expectations, (3) a strict follow-up with routine recall should be provided to maintain and improve denture adaptation, and (4) a denture that has to be fabricated after a decade, is not considered a failure; however, if it needs repair within 5 years success has not been achieved.59 Some additional removable prosthodontic pearls for the different types of overdentures have been included in Box 2 .
Box 2. Prosthodontic Pearls for various types of Overdentures.
-
•
The Ball/Stud (locator) attachment can be used with nonparalleled implants.
-
•
The Bar attachment (with clips or riders) have high retentive capacities and reduced loading forces over implants. Also, they can be used with nonparalleled implants.
-
•
The Bar attachments have an increased probability of plaque accumulation; therefore, good oral hygiene maintenance should be practiced. Also, gingival hyperplasia has been reported with bar attachments.
-
•
The magnet attachment is better suited for the elderly patient with limited dexterity. There are reduced loading forces over the implants and can be used with nonparalleled implants.
-
•
The magnet attachment can lose retention over time owing to intraoral corrosion.
-
•
The telescopic attachments allow for high retention and stability of the denture. Oral hygiene is more easily accessible.
Patients should be informed that magnet, bar, and telescopic attachments will have higher fees owing to dental laboratory fees. Assaf and colleagues59 stated that “there is no clear understanding of what the preferred retention system may be, nor which system should be designated as routine maintenance repairs vs complications, as the difference is quantitative and subjective.”60
When the decision has been made by the GP to provide Oral Rehabilitation/Reconstruction for the completely edentulous patient, there should be a few questions to include in the treatment plan. The GP should determine (1) if there is a monetary budget, (2) whether the patient is comfortable with the thought of wearing dentures attached to the implants (some patients do not like the concept of a denture), (3) whether the patient would prefer the ability to remove and clean your denture, and (4) whether the patient prefers the denture to stay in the mouth (without the ability to remove it)? Once these preferences are established, they will help with patient satisfaction at the time of delivery. It should be noted that once the patients’ desires are confirmed, the ultimate plan will be determined by the patient’s bone volume, soft tissue condition, anatomic structures, and interarch space.
The fundamental prosthodontic principles in dental implantology include (1) preliminary and definitive impressions, (2) jaw relation records, (3) wax try-in, (4) metal framework try-in (with and without artificial teeth), and (5) insertion of definitive prostheses.61 The second half of this article discusses the fixed prostheses designed in 3 different ways. They will be displayed according to minimal complications for the clinician, allowing for a passive fit, and ease of hygiene for the patient to the most complex prostheses. Computer-aided designed/computer aided manufacturing are preferred by many clinicians based off of reported accuracy of fit.61
The maxillary posterior region is the most sensitive area of all 4 quadrants owing to its inadequate density and caution is warranted when placing implants in this region. Sinus lifts are commonly performed to facilitate implants in this region; however, many implants fail owing to type IV bone in the region. There are some patients who may be hesitant or afraid at the mere thought of dental implants at or near their sinuses. Should a patient decide not to obtain a sinus lift (when there is a need), or if the patient has pneumatization of the sinuses, then the consideration of intentionally tilted implants could be considered as an option. This option could be given to the patient who does not mind the concept of wearing a denture and prefer the prostheses to be fixed. The “fixed–hybrid” or “all-on-four” concept requires angulation, placement of 2 posterior implants, and placement of 2 anterior implants to allow the denture to attach, function, and the inability to be removed (unless done so by the operator or another trained clinician with the implant parts). Of course, other options can be suggested; nonetheless, the main reason behind offering this first is due to the 45° angulation of the posterior implant, which could limit the addition of other implants in the future (Fig. 20 ). Morton and colleagues28 stated “there is no statistically significant difference in primary outcomes (survival rates for implant prosthesis) or secondary outcomes (peri-implant marginal bone loss, soft and hard tissue complications, prosthetic complications and patient-centered outcomes) for implants placed in a tilted configuration when used to support full arch fixed partial dentures.” The authors went further to state that “the final prosthetic plan should be considered when developing a surgical plan for implant placement.” Even though a 1-piece full-arch fixed prosthesis is acceptable, it may not be the best choice for those patients in the high-risk category for implant loss or complications (ie, smokers). The patient in high-risk categories can be offered a treatment plan with 6, 8, or more in an arch in case there are complications or failures (or simply decline the placement of implants).
Fig. 20.

45° intentionally tilted posterior implants, just anterior to the maxillary sinuses.
The key prosthodontic points of all-on-four hybrid system are that (1) there are only 4 implants, (2) it is a prosthetically driven process, where the posterior abutments are torqued at 15 neutons and the anterior abutments are torqued at 30 neutons, (3) there is a collaboration between the restorative dentist and the oral surgeon, (4) the posterior regions are avoided owing to the intentionally (45°) tilted implant, (5) there is use of a cantilever, (6) the intaglio surface should be smooth and convex, (7) and maintenance will be with the use of Superfloss (see Fig. 38) or a floss threader or a Waterpik.
Fig. 38.

Floss threader, soft picks, and super floss.
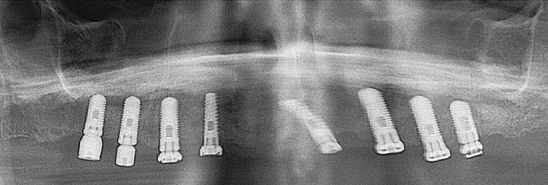
According to the Group 2 ITI Consensus Report, the prosthetic plan should include (a) the prosthetic material, (b) 1-piece (Fig. 21, Fig. 22, Fig. 23, Fig. 24 ) and (Fig. 30, Fig. 31, Fig. 32, Fig. 33, Fig. 34, Fig. 35, Fig. 36, Fig. 37) or segmented prostheses (Fig. 25, Fig. 26, Fig. 27, Fig. 28, Fig. 29 ), (c) aesthetic factors (ie, lip support, smile line), (d) the condition of the opposing dentition, (e) the available space for the prosthesis, (f) the anatomy of the edentulous ridge (maxilla, mandible, bone volume and quality, and anatomic limitations), (g) planned distribution and cantilever length, (h) space availability hygiene and maintenance (see Figs. 38 and 39).28 Morton and colleagues28 mentioned that “a minimum number of 4 appropriately distributed implants are recommended to support a one-piece full arch fixed prosthesis… the impact of future implant loss/complications on prosthesis support should be considered when choosing a number.” The case with the classic implant roundhouse 1-piece, failed after stage 2 of the healing caps being placed on #3 (see Fig. 31). This patient refused to wear an implant overdenture and would only accept a treatment plan with a fixed bridge (see Fig. 31, Fig. 32, Fig. 33, Fig. 34, Fig. 35, Fig. 36, Fig. 37 ). The patient had a history of smoking 1 pack of cigarettes per day for 35 years. There are some patients who will not heed the warnings from the GP and choose various risks (ie, smoking), which could lead to complications or failure.
Fig. 21.

Closed Tray impression copings.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 22.

Excess flanges of acrylic should be trimmed by the GP. These vents will be plugged with cotton pellets and sealed off. The choice of acrylic or composite can be used.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 23.

The intaglio surface can be filled with pink acrylic (retrofitted by the GP) to make the prostheses cleansable for the patient. Special care should be made not to allow any acrylic to enter the metal coping on the intaglio surface, for the screws. The chair time will increase for the GP, but this particular “fixed hybrid” can be made affordable to the patient.
Fig. 24.

The patient was extremely satisfied at the delivery date. The lower anterior teeth were extracted and treated with an immediate removable partial dentures on the day of delivery. (A) Before. (B) After.
Fig. 30.
Eight implants.
Fig. 31.

Implant #3 failed, owing to the patients’ history of cigarette smoking.
Fig. 32.

The connected metal framework may fit perfect on the cast.
(Courtesy of Milivoj Grego, CDT, MS.)
Fig. 33.

One of the disadvantages of the “roundhouse” is misfit on delivery. Management of this problem could be to retake the impression or it could be sectioned, placed back in the mouth, splinted with inlay resin. Note: a pickup impression with PVS should be made, sent to the dental laboratory.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 34.

The soldered “roundhouse” tried in the mouth.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 35.

The GP should request a Bisque–Bake appointment to adjust occlusion. An occlusal-protected appointment.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 36.

Before cementation.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 37.

Satisfied patient on delivery.
(Courtesy of Milivoj Grego, CDT, MS and Ricardo A. Boyce, DDS, FICD.)
Fig. 25.

This case displays the segmented cement retained fixed partial denture.
(Courtesy of Milivoj Grego, CDT, MS.)
Fig. 26.

The connected crowns were cemented first.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 27.

Next, the long spanned bridge was cemented.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 28.

Finally, the last bridge was cemented.
(Courtesy of Ricardo A. Boyce, DDS, FICD.)
Fig. 29.

The patient was satisfied on delivery.
(Courtesy of Milivoj Grego, CDT, MS and Ricardo A. Boyce, DDS, FICD.)
Fig. 39.

Plastic, titanium, and graphite dental instruments.
Mombelli62 stated: “regarding dental implants, as the evolution from peri-implant mucositis to peri-implantitis may be gradual, maintenance therapy has the potential to intercept infection before the bone has been damaged extensively.” He described 3 important components of maintenance care after completion of active periodontal therapy and after dental implant therapy (Fig. 40 ): (1) measures taken by the patient (ie, personal oral hygiene, avoidance of tobacco smoke, management of systemic diseases), (2) preventive procedures carried out by the dental health care professional (ie, removal of subgingival deposits, elimination of plaque retentive factors), and (3) supportive periodontal therapy sensu strictu (ie, interventions addressing the cause, the pathophysiologic mechanisms, or the sequelae of recurrent or residual disease.
Fig. 40.

The 3 components of maintenance after completion of active periodontal therapy and after dental implant therapy.
(From Mombelli A. Maintenance therapy for teeth and implants. Periodontol 2000. 2019;79(1):191; with permission.)
Baseline radiographs and probing depths (with a plastic periodontal probe) should be taken on delivery of the implant-supported prostheses and at subsequent follow-up visits to establish the bone level and follow the remodeling process.63, 64, 65, 66
Patient satisfaction (with overall treatment, aesthetics) is the primary goal of the dentist/GP providing any prosthodontic procedure and has been viewed equally important as implant survival.45 The 4 most frequently used parameters for measuring the success of dental implants include (1) the implant level, (2) peri-implant soft tissue level, (3) prosthesis level, and (4) the patient’s subject assessment.67 Wittenben45 used the visual analogue scale to determine the patient-reported outcome measures to evaluate how patients felt about their overall treatment and esthetics. Their systematic review concluded that (1) the aesthetics of implant-supported FDPs are highly rated by patients (visual analogue scale = 90.0; 87.9–92.2); (2) the appearance of the mucosa surrounding the implant-supported FDP's was highly rated (visual analogue scale = 84.7; minimum of 73.0 to maximum of 92.0) by patient-reported outcome measures; (3) patient-reported outcome measures ratings were higher with patients having soft tissue level implants compared with the ones with bone level type implants however without being statistically significant (P = .128); (4) individual restorative materials had no influence on ratings of PROMs focusing on the aesthetics of implant-supported FDPs; and (5) the use of a provisional restoration had no effect on aesthetic ratings of the definitive restorations on implant-supported FDPs evaluated by PROMs. An even more interesting point that was made when it comes to aesthetics, are that the studies that have proved the worse critics in the aesthetic outcome to be prosthodontists and general dentists, while patients shown to be less critical and often times highly satisfied with their overall treatment and aesthetics.68, 69, 70, 71, 72
Summary
The current COVID-19 pandemic has been a challenge for dentists and their dental offices owing to the consequent economic recession. The modern day dentist may need to be more conservative (ie, down payments, offer payment plans) with their patients’ treatment plans involving implants. All members of the dental health team should be wearing appropriate PPE and practicing hand hygiene throughout the day. Patients are requesting edentulous spaces to be restored with FDP. The 10-year survival rate of implant crowns and FDPs range between 89% and 94%. The GP is encouraged to implement an occlusal plan to provide an implant protective occlusion, to reduce biomechanical complications and improve clinical outcomes. There is no gold standard for implant placement after extraction(s). The GP can use their own techniques or choose between the immediate, early, or late protocols with the higher percentages of survival rates. The surgical plan will be determined by the patients’ risk factors (past medical history, medications, social habits, etc), bone volume (need for bone grafting), soft tissue conditions, anatomic structures, and interarch space. The prosthetic plan should involve the prostheses (type, material), aesthetic factors, condition of the opposing dentition, space for the prostheses, anatomy of the edentulous ridge, planned distribution, hygiene, and maintenance. A nightguard is recommended as a part of the final delivery for crown(s) and long spanned prostheses. The modern-day dentist will need to provide patients who are interested in implants with evidenced-based knowledge, goals, and treatment to satisfy their needs and expectations.
Clinics care points
-
•
All patients should be queried over the phone (before) and on the day of their arrival in the clinic (ie, recent travel histories and test results for coronavirus, fever, respiratory symptoms, etc.).
-
•
The patient and family who accompany them should be instructed to wear masks to their appointments.
-
•
The goal of the GP should be to protect all patients and staff from coronavirus.
-
•
Attach dental floss to restorative tools to avoid an uneventful aspiration by the patient.
-
•
Risk factors for failure or potential complications should be discussed with the patient before treatment.
-
•
There is no gold standard for Implant placement after extraction(s); however, the implant placement and loading protocol should be planned before surgery.
-
•
Respect the manufacturer’s torqueing guidelines.
-
•
The surgical plan will be determined by the patient’ risk factors, bone volume, soft tissue conditions, anatomic structures, and interarch space.
-
•
The prosthetic plan should involve the prostheses (type material), aesthetic factors, condition of the opposing dentition, space for the prostheses, anatomy of the edentulous ridge, planned distribution, hygiene, and maintenance.
-
•
Nightguards should be recommended in long spanned and/complex cases.
Acknowledgments
Disclosure
The author has nothing to disclose.
References
- 1.Zembic A., Tahmaseb A., Jung R.E. Patient reported outcomes of maxillary edentulous patients wearing overdentures retained by two implants from insertion to 4 years. Int J Oral Maxillofac Implants. 2019;34:481–488. doi: 10.11607/jomi.6980. [DOI] [PubMed] [Google Scholar]
- 2.Pjetursson B.E., Zarauz C., Strasding M. A systematic review of the influence of the implant abutment connection on the clinical outcomes of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin Oral Implants Res. 2018;29(Suppl.18):160–183. doi: 10.1111/clr.13362. [DOI] [PubMed] [Google Scholar]
- 3.Jung R.E., Zembic A., Pjetursson B.E. Systemic review of the Survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res. 2012;23(Suppl 6):2–21. doi: 10.1111/j.1600-0501.2012.02547.x. [DOI] [PubMed] [Google Scholar]
- 4.Givi B., Schiff B.A., Chinn S.B. Safety Recommendations for Evaluation and Surgery of the Head and Neck during the COVID-19 Pandemic. JAMA Otolarygol Head Neck Surg. 2020;146(6):579–584. doi: 10.1001/jamaoto.2020.0780. [DOI] [PubMed] [Google Scholar]
- 5.Izzetti R., Nisi M., Gabriele M. COVID-19 transmission in the dental practice: brief review of prospective measures in Italy. J Dent Res. 2020 doi: 10.1177/0022034520920580. [DOI] [PubMed] [Google Scholar]
- 6.Kern J.-S., Kern T., Wolfart S. A systemic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: post- loading implant loss. Clin Oral Implants Res. 2016;27:174–195. doi: 10.1111/clr.12531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Boyce R.A., Klemons G. Treatment Planning for Restorative Implantology. Dent Clin North Am. 2015;59:291–304. doi: 10.1016/j.cden.2014.10.009. [DOI] [PubMed] [Google Scholar]
- 8.Peng X., Xu X., Li Y. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020;12(1):9. doi: 10.1038/s41368-020-0075-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Meng L., Hua F., Bian Z. Response to the Letter to the Editor: how to deal with suspended oral treatment during the COVID-19 epidemic. J Dent Res. 2020;99(8):988. doi: 10.1177/0022034520920166. [DOI] [PubMed] [Google Scholar]
- 10.Ekfelt A., Christiansson U., ErikssonT A Retrospective analysis of factors associated with multiple implant failures in the maxillae. Clin Oral Implants Res. 2001;12:462–467. doi: 10.1034/j.1600-0501.2001.120505.x. [DOI] [PubMed] [Google Scholar]
- 11.Minsk L., Polson A.M., Weisgold A. Outcome failures of endosseous implants from a clinical training center. Compend Contin Educ Dent. 1996;17:848–859. [PubMed] [Google Scholar]
- 12.Mombell A. Microbiology of the Dental Implant. Adv Dent Res. 1993;7(2):202–206. doi: 10.1177/08959374930070021201. [DOI] [PubMed] [Google Scholar]
- 13.Balshi T.J. Analysis and management of fractured implants: a clinical report. Int J Oral Maxillofac Implants. 1996;11:660–666. [PubMed] [Google Scholar]
- 14.Rose L.F., Mealy B., Genco R. Elsevier Mosby; St Louis (MO): 2004. Periodontics: medicine, surgery, and implants; pp. 611–674. [Google Scholar]
- 15.Chappuis V., Avila-Ortiz G., Araújo M.G. Medication-related dental implant failure: systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl. 16):55–68. doi: 10.1111/clr.13137. [DOI] [PubMed] [Google Scholar]
- 16.Heitz-Mayfield L.J., Aaboe M., Araujo M. Group 4 ITI consensus report: risks and biologic complications associated with implant dentistry. Clin Oral Implants Res. 2018;29(Suppl. 16):351–358. doi: 10.1111/clr.13307. [DOI] [PubMed] [Google Scholar]
- 17.Hämmerle C.H.F., Tarnow D. The etiology of hard- and soft-tissue deficiencies at dental implants. J Periodontol. 2018;89(Suppl 1):S291–S303. doi: 10.1002/JPER.16-0810. [DOI] [PubMed] [Google Scholar]
- 18.Chiapasco M., Zaniboni M., Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 2006;17(Suppl. 2):136–159. doi: 10.1111/j.1600-0501.2006.01357.x. [DOI] [PubMed] [Google Scholar]
- 19.Sanz-Sanchez I., Carrilllo de Albornoz A., Figuero E. Effects of lateral bone augmentation procedures on peri-implant health or disease: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl. 15):18–31. doi: 10.1111/clr.13126. [DOI] [PubMed] [Google Scholar]
- 20.Thoma D.S., Bienz S.P., Figuero E. Efficacy of lateral bone augmentation performed simultaneously with dental implant placement: a systematic review and meta-analysis. J Clin Periodontol. 2019;46(Suppl. 21):257–276. doi: 10.1111/jcpe.13050. [DOI] [PubMed] [Google Scholar]
- 21.Ogle O.E. Implant Surface Material, Design, and Osseointegration. Dent Clin North Am. 2015;59:505–520. doi: 10.1016/j.cden.2014.12.003. [DOI] [PubMed] [Google Scholar]
- 22.Pohl V., Thoma D.S., Sporniak-Tutak K. Short dental implants (6mm) versus long dental implants (11-15)mm) in combination with sinus floor elevation procedures: 3 year results from multicenter, randomized, controlled clinical trial. J Clin Periodontol. 2017;44:438–445. doi: 10.1111/jcpe.12694. [DOI] [PubMed] [Google Scholar]
- 23.Bidez M.W., Misch C.E. Clinical biomechanics in implant dentistry. In: Misch C.E., editor. Contemporary implant dentistry. 3rd edition. Mosby; St. Louis (MO): 2008. pp. 543–555. [Google Scholar]
- 24.Ravidà A., Wang I.-C., Barootchi S. Meta-analysis of randomized clinical trials comparing clinical and patient-reported outcomes between extra –short (≤ 6 mm) and longer (≥10 mm) implants. J Clin Periodontol. 2019;46:118–142. doi: 10.1111/jcpe.13026. [DOI] [PubMed] [Google Scholar]
- 25.Chen S.T., Buser D. Clinical and esthetic outcomes of implants placed in posterior extraction sites. Int J Oral Maxillofac Implants. 2009;24(Suppl):186–217. [PubMed] [Google Scholar]
- 26.Canellas J.V.D.S., Medeiros P.J.D., Figueredo C.M.D.S. Which is the best choice after extraction, immediate implant placement or delayed placement with alveolar ridge preservation? A systematic review and meta-analysis. Craniomaxillofac Surg. 2019;47(11):1793–1802. doi: 10.1016/j.jcms.2019.08.004. [DOI] [PubMed] [Google Scholar]
- 27.Gallucci G.O., Hamilton A., Zhou W. Implant placement and loading protocols in partially edentulous patients: a systemic review. Clin Oral Implants Res. 2018 Oct;29(Suppl 16):106–134. doi: 10.1111/clr.13276. [DOI] [PubMed] [Google Scholar]
- 28.Morton D., Gallucci G., Lin W. Group 2 ITI Consensus Report: prosthodontics and implant dentistry. Clin Oral Implants Res. 2018;29(Suppl. 16):215–223. doi: 10.1111/clr.13298. [DOI] [PubMed] [Google Scholar]
- 29.Isidor R. Histological evaluation of peri-implant bone at implants subjected to occlusal overload or plaque accumulation. Clin Oral Implants Res. 1997;8:1–9. doi: 10.1111/j.1600-0501.1997.tb00001.x. [DOI] [PubMed] [Google Scholar]
- 30.Rangert B., Krogh P.H., Langer B. Bending overload and implant fracture: a retrospective clinical analysis. Int J Oral Maxillofac Implants. 1995;7:40–44. [PubMed] [Google Scholar]
- 31.Fuentealba R., Jofŕe J. Esthetic Failure in Implant Dentistry. Dent Clin North Am. 2015;59:227–246. doi: 10.1016/j.cden.2014.08.006. [DOI] [PubMed] [Google Scholar]
- 32.Misch C., editor. Rationale for dental implants. 2nd edition. Elsevier (Mosby); St. Louis (MO): 2015. Misch CE. Dental Implant Prosthetics; pp. 874–937. [Google Scholar]
- 33.Misch C., editor. Occlusal considerations for implant-supported prostheses. Contemporary implant dentistry. Mosby; St. Louis (MO): 1993. [Google Scholar]
- 34.Misch C.E., Bidez M.W. Implant protected occlusion: a biomechanical rationale. Compend Contin Dent Educ. 1994;15:1330–1343. [PubMed] [Google Scholar]
- 35.Papaspyridakos P., Chen C.-J., Chuang S.K. A systematic review of biologic and technical complications with fixed implant rehabilitation for edentulous patients. Int J Oral Maxillofac Implants. 2012;27(1):102–110. [PubMed] [Google Scholar]
- 36.Papspyridakos P., Bordin T.B., Kim Y.J. Technical complications and prosthesis survival rates with implant-supported fixed complete dental prostheses: a retrospective study with 1 to 12 year follow-up. J Prosthodont. 2020;29(1):3–11. doi: 10.1111/jopr.13119. [DOI] [PubMed] [Google Scholar]
- 37.Varthis S., Tarnow D., Randi A. Interproximal open contacts between implant restorations and adjacent teeth. Prevalence – causes – possible solutions. J Prosthodont. 2019;28:e806–e810. doi: 10.1111/jopr.12980. [DOI] [PubMed] [Google Scholar]
- 38.Sadid-Zadeh R., Kutkut A., Kim H. Prosthetic failure in Implant Dentistry. Dent Clin North Am. 2015;59:195–214. doi: 10.1016/j.cden.2014.08.008. [DOI] [PubMed] [Google Scholar]
- 39.Goodacre C.J., Bernal G., Rungcharassaeng K. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90:121–132. doi: 10.1016/S0022-3913(03)00212-9. [DOI] [PubMed] [Google Scholar]
- 40.Romanos G.E., Javed F., Delgado-Ruiz R.A. Peri-implant diseases: a review of treatment interventions. Dent Clin North Am. 2015;59:157–178. doi: 10.1016/j.cden.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 41.Scarfe W., Farman A., Sukovic P. Clinical applications of cone-beamed computed tomography in the dental practice. J Can Dent Assoc. 2006;72(1):75–80. [PubMed] [Google Scholar]
- 42.Hutlin H., Svensson K., Trulsson M. Clinical advantages of computer-guided implant placement: a systemic review. Clin Oral Implants Res. 2012;23(Suppl 6):124–138. doi: 10.1111/j.1600-0501.2012.02545.x. [DOI] [PubMed] [Google Scholar]
- 43.Block M.S. 3rd edition. Saunders (Elsevier); 2011. Color Atlas of implant surgery; pp. 58–114. [Google Scholar]
- 44.Aziz S.R. Hard and soft tissue surgical complications in dental implantology. Oral Maxillofacial Surg Clin N Am. 2015;27:313–318. doi: 10.1016/j.coms.2015.01.006. [DOI] [PubMed] [Google Scholar]
- 45.Wittneben J.-G., Wismeijer D., Brägger U. Patient-reported outcome measures focusing on aesthetics of implant- and tooth-supported fixed dental prostheses: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl. 16):224–240. doi: 10.1111/clr.13295. [DOI] [PubMed] [Google Scholar]
- 46.Berglundh T., Armitage G., Araujo M.G. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(Suppl 1):S313–S318. doi: 10.1002/JPER.17-0739. [DOI] [PubMed] [Google Scholar]
- 47.Mittal H., John M.T., Sekulić S. Patient- Reported Outcome Measures for Adult Dental Patients: a systemic review. J Evid Based Dent Pract. 2019;19(1):53–70. doi: 10.1016/j.jebdp.2018.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lang N.P., Zitzmann N.U. Working Group 3 of the VIII European Workshop on Periodontology. Clinical research in implant dentistry: evaluation of implant-supported restorations, aesthetic and patient-reported outcomes. J Clin Periodontol. 2012;39(Suppl. 12):133–138. doi: 10.1111/j.1600-051X.2011.01842.x. [DOI] [PubMed] [Google Scholar]
- 49.Cosyn J., Thoma D.S., Hämmerle C.H. Esthetic assessments in implant dentistry: objective and subjective criteria for clinicians and patients. Periodontol 2000. 2017;73(1):193–202. doi: 10.1111/prd.12163. [DOI] [PubMed] [Google Scholar]
- 50.Petersen P.E., Bourgeois D., Ogawa H. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661–669. [PMC free article] [PubMed] [Google Scholar]
- 51.Peterson P.E., Yamamoto T. Improving the Oral health of older people: the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2005;33(2):81–92. doi: 10.1111/j.1600-0528.2004.00219.x. [DOI] [PubMed] [Google Scholar]
- 52.Payne A.G.T., Alsabeeha N.H.M., Atieh M.A. Interventions for replacing missing teeth : attachment systems for Implant over-dentures in edentulous jaws. Cochrane Database Syst Rev. 2018;(10) doi: 10.1002/14651858.CD008001.pub2. CD008001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Babush C.A. Post-treatment quantification of patient experiences with full-arch implant treatment using a modification of the OHID – 14 questionnaire. J Oral Implant. 2012;38(3):251–260. doi: 10.1563/AAID-JOI-D-12-00001. [DOI] [PubMed] [Google Scholar]
- 54.Lopez C.S., Saka C.H., Rada G. Impact of fixed implant supported prostheses in edentulous patients: protocol for a systemic review. BJM Open. 2016;6:e009288. doi: 10.1136/bmjopen-2015-009288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sykess D. Medico-legal aspects of dental implants. Ann R Australas Coll Dent Surg. 2000;15:309–314. [PubMed] [Google Scholar]
- 56.de Albuquerque Júnior R.F., Lund J.P., Tang L. Within-subject comparison of maxillary long-bar implant-retained prostheses with and without palatal coverage: patient-based outcome. Clin Oral Implants Res. 2000;11:555–565. doi: 10.1034/j.1600-0501.2000.011006555.x. [DOI] [PubMed] [Google Scholar]
- 57.Fero K.J., Morgano S.M., Driscoll C.F. the Glossary of Prosthodontic Terms: Ninth Edition GPT-9. J Prosthet Dent. 2017;117(5 Suppl):e1–e105. doi: 10.1016/j.prosdent.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 58.Naert I. The influence of attachment systems on implant-retained mandibular overdentures. In: Feine J.S., Carsson G.E., editors. vol. 13. Quintessence Publishing Co Inc; Chicago, Illinois, USA: 2003. pp. 238–243. (Implant overdentures: the standard of care for the edentulous patients). [Google Scholar]
- 59.Assaf A., Daas M., Boittin A. Prosthetic maintenance of different mandibular implant overdentures: a systematic review. Prosthet Dent. 2017;118(2):144–152. doi: 10.1016/j.prosdent.2016.10.037. [DOI] [PubMed] [Google Scholar]
- 60.Attard N.J., Zarb G.A., Laporte A. Long-term treatment outcomes in edentulous patients with implant overdentures: the Toronto study. Int J Prosthodont. 2004;17:425–433. [PubMed] [Google Scholar]
- 61.Drago C., Howell K. Concepts for Designing and Fabricating Metal Implant Frameworks for Hybrid Implant Prostheses. J Prosthodont. 2012;21:413–424. doi: 10.1111/j.1532-849X.2012.00835.x. [DOI] [PubMed] [Google Scholar]
- 62.Momelli A. Maintenance therapy for teeth and implants. Perodontol 2000. 2019;79:190–199. doi: 10.1111/prd.12255. [DOI] [PubMed] [Google Scholar]
- 63.Araujo M.G., Lindhe J. Peri-implant health. J Periodontol. 2018;89(Suppl 1):S249–S256. doi: 10.1002/JPER.16-0424. [DOI] [PubMed] [Google Scholar]
- 64.Heitz-Mayfiel L.J.A., Salvi G.E. Peri-implant mucositis. J Periodontol. 2018;(Suppl 1):S257–S266. doi: 10.1002/JPER.16-0488. [DOI] [PubMed] [Google Scholar]
- 65.Schwartz F., DerksJ Monje A., Wang H.-L. Per-implamtitis. J Periodontol. 2018;89(Suppl1):S267–S290. doi: 10.1002/JPER.16-0350. [DOI] [PubMed] [Google Scholar]
- 66.Renevert S., Perrson G.R., Pirih F.Q. Peri-implant health, peri-implant mucositis: case definitions and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S304–S312. doi: 10.1002/JPER.17-0588. [DOI] [PubMed] [Google Scholar]
- 67.Papaspyridakos P., Chen C.J., Singh M. Success criteria in implant dentistry: a systemic review. J Dent Res. 2012;91(3):253–260. doi: 10.1177/0022034511431252. [DOI] [PubMed] [Google Scholar]
- 68.Chang M., Odman P., Wennström J.L. Esthetic outcome of implant-supported single-tooth replacements assessed by the patient and by prosthodontists. Int J Prosthodont. 1999;12(4):335–341. [PubMed] [Google Scholar]
- 69.Tettamanti S., Millen C., Gavric J. Esthetic evaluation of implant crowns and peri-implant soft tissue in the anterior maxilla: comparison and reproducibility of three different indices. Clin Implant Dent Relat Res. 2016;18(3):517–526. doi: 10.1111/cid.12306. [DOI] [PubMed] [Google Scholar]
- 70.Hartlev J., Kohberg P., Ahlmann S. Patient satisfaction and esthetic outcome after immediate placement and provisionalization of single-tooth implants involving a definitive individual abutment. Clin Oral Implants Res. 2014;25(11):1245–1250. doi: 10.1111/clr.12260. [DOI] [PubMed] [Google Scholar]
- 71.Cosyn J., Eghbali A., De Bruyn H. Single implant treatment in healing versus healed sites of the anterior maxilla: an aesthetic evaluation. Clin Implant Dent Relat Res. 2012;14(4):517–526. doi: 10.1111/j.1708-8208.2010.00300.x. [DOI] [PubMed] [Google Scholar]
- 72.Cosyn J., Eghbali A., Hanselaer L. Four modalities of single implant treatment in the anterior maxilla: a clinical, radiographic, and esthetic evaluation. Clin Implant Dentistry Relat Res. 2013;15(4):517–530. doi: 10.1111/j.1708-8208.2011.00417.x. [DOI] [PubMed] [Google Scholar]