

Abstract
Background:
Osteonecrosis of the femeral head (ONFH) occurs predominantly in young- and middle-aged people, and the disability rate is high in the late stage of the disease and most patients have to undergo total hip replacement. Clinically, increasing attention is paid to intervening early and middle-stage ONFH so as to delay its progress. Acupuncture and moxibustion (AM) is a unique method for treating ONFH in China. This study aims to summarize the advantages of AM for the treatment of ONFH.
Methods:
A comprehensive literature search was conducted on the database with languages of English and Chinese. The medical subject titles used are “Osteonecrosis of the femoral head” and “acupuncture and moxibustion.” Related words in the title or abstract including but were not limited to “necrosis of the femoral head,” “avascular necrosis of the femoral head,” “ischemic necrosis of the femoral head,” “caput femoris necrosis,” “bone paralysis,” “bone erosion,” and “bone atrophy.”
Results:
Nine randomized controlled trials were identified in this meta-analysis that included 630 subjects. Meta-analysis showed that the trial group that treated with conventional therapy combined with AM had a higher effective rate (Z = 2.27 P = 0.02) and excellent and good rate (Z = 4.85 P < 0.00001) and Harris hip function score (HHS) (Z = 2.31 P = 0.02) and lower incidence of related adverse reactions during treatment (Z = 2.82 P = 0.005) compared with the control group that treated with conventional therapy alone.
Conclusions:
AM for early and middle-stage ONFH is an effective and relatively safe intervention, which can improve the effective rate and excellent and good rate and HHS, and reduce the adverse reaction rate. Clinically, early and middle-stage ONFH can be intervened by combining with AM while taking conventional therapy to improve the efficacy.
Keywords: AM, early and middle stage, effective rate, excellent and good rate, Harris hip function score, meta-analysis, ONFH
1. Introduction
Osteonecrosis of the femeral head (ONFH), formerly known as ischaemic necrosis of the femoral head, characterized by the death of bone cells and bone marrow caused by the insufficient blood supply to the affected segment of subchondral bone, usually occurs in young people and eventually leads to hip destruction, and because of its high disability rate, it is even referred to clinic as “undead cancer.”[1,2] The main clinical manifestation is pain and the pain is mainly concentrated in the hip, buttock, or groin area, and occasionally is accompanied by knee pain and limited internal rotation of the hip joint.[3–5] The number of patients with ONFH is increasing year by year globally, and China alone has approximately 8.12 million patients with ONFH.[3] Early diagnosis and early intervention of ONFH can provide some joint rescue treatments and control the progression of the disease. Total hip replacement is the last resort to relieve pain and restore function, but it is not widely accepted because the patient population is mostly young.[6,7] As a result, there is increasing emphasis on early interventions for ONFH, designed to preserve natural joints to avoid or at least delay total hip replacement.[7] ONFH belongs to the categories of “bone arthritis,” “bone atrophy,” and “bone erosion” in the traditional Chinese medicine (TCM) system.[8] Chinese medicine is commonly used to promote qi and blood circulation, smooth channel to relieve pain, nourish liver and kidney, strengthen muscles and bones, and other treatments to promote blood circulation throughout the body, improve the microcirculation of the lesion, and thus relieve symptoms.[8–10] In China, clinicians apply TCM to treat early and middle-stage femoral head necrosis through differentiation of symptoms and signs to release patient symptoms and delay disease progression.[11,12] The general treatment principle is “activating blood to remove blood stasis,” therefore, salvia miltiorrhiza, ligusticum wallichii, peach nut seed, and safflower are often used for treatment. There have been a large number of clinical studies showing that TCM can greatly relieve patients’ pain.[11–17] And studies also confirmed by magnetic resonance imaging (MRI) that the pathological changes of femoral head necrosis such as effusion and edema of the Joint cavity have also been alleviated through TCM treatment.[18,19] Acupuncture and moxibustion (AM) is a unique treatment method in China, also belongs to TCM. With the development of technology, current AM include not only traditional acupuncture or moxibustion but also electro-acupuncture (EA), intensive acupuncture, etc. And it proves that AM has functions of activating menstrual channels, regulating qi and blood, and nourishing the internal organs, and eventually enhancing body function.[20] It has achieved good clinical effects in the clinical treatment of chronic pain,[21,22] and it can also achieve the effect of decompression and pain relief of the hip joint, and more importantly, there is no side effect of surgery.[23,24] The main purpose of this study is to summarize the efficacy of AM for early and middle-stage ONFH, and to analyze the advantages of combined AM therapy for ONFH, so as to provide recommendations for clinical treatment of early and middle-stage ONFH.
2. Methods
This systematic review has been registered on PROSPERO as ID 195730. This study does not require ethical approval. First, this is a systematic review and meta-analysis of previous studies, not a clinical trial or animal experiment; Secondly, requiring ethical approval of the ethics committee and obtaining the patient's informed consent is the premise of every randomized controlled trial (RCT) study, which also includes in each included RCTs of this paper.
2.1. Source of literature
This meta-analysis was written using Preferred Reporting Items for Systematic Review and Meta-Analysis reporting guidelines and was based on previous studies of AM for ONFH. The selected studies are mainly searched in the following databases: PubMed, EMBASE, Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), Weipu Chinese Science and Technique Journals Database, and the Wanfang database, from the establishment of the database until July 5, 2020.
2.2. Search strategy
Two researchers conducted the independent literature search, mainly searching for English and Chinese literature. The search items were as follows: “osteonecrosis of the femeral head,” “necrosis of the femoral head” OR “avascular necrosis of the femoral head” OR “ischemic necrosis of the femoral head” OR “caput femoris necrosis” OR “bone paralysis” OR “bone erosion” OR “bone atrophy” AND “acupuncture” OR “acupuncture and moxibustion” OR “electro-acupuncture” OR “moxibustion” AND “randomized controlled trial” OR “randomized” OR “randomly” OR “randomized clinical trial” OR “random.”
2.3. Inclusion criteria
All studies we selected are RCTs. We included ONFH patients irrespective of gender, age, but all patients were clearly diagnosed with early and middle-stage ONFH according to the common clinical staging methods. And in the included studies, AM is not included in the interventions of the control group, and the interventions of the trial group are combined with AM on the basis of the control group. Moreover, the patient's observation indicators are mainly the effective rate, excellent and good rate, harris hip function score (HHS), and the adverse reaction rate.
2.4. Exclusion criteria
The exclusion criteria correspond to the selection criteria. First, the study is not RCT and the study is not related to AM for the treatment of ONFH or the study is a comparison between different acupuncture techniques. Next, the stage of ONFH is not early or middle. Further, AM was also included in the interventions of the control group or no suitable outcome. Finally, animal experiments and repeated research also cannot be included.
2.5. Outcome measures
In several studies, the efficacy according to the HHS criterion after treatment was judged into 4 grades: excellent with 90–100 points, good with 80–90 points, moderate with 70–80 points, and poor with less than 70 points.[25–27] In 2 studies, according to the “Diagnosis and Curative Effect Criteria for Diseases of Traditional Chinese Medicine” to determine the efficacy as cured, improved, and not cured by the symptoms and X-ray before and after treatment.[28,29] In Jin study, according to the “National Symposium on Avascular Necrosis of the Femoral Head Joint Function Standards” to formulate efficacy standards.[30] Score based on joint range of motion, pain, living ability, walking distance, and X-ray, the efficacy was judged into 4 grades: excellent with 90–100 points, good with 60–80 points, moderate with 40–60 points, and poor with less than 40 points. In the other 2 studies, the curative effect was determined with reference to the “Draft of Evaluation of Curative Effect on Avascular Necrosis of the Femoral Head in Adults (Percentage),” which was divided into 4 levels according to the score: excellent with 85–100 points, good with 75–85 points, moderate with 60–75 points, and poor with less than 60 points.[31,32] The effective rate means the ratios of “excellent, good and moderate” or “cured and improved.” The excellent and good rate includes the ratios of excellent and good. HHS is currently the most universal hip joint function scoring system in the world.[33] It is used to quantitatively evaluate the functional state of the hip joint. The full score is 100 points and is mainly composed of 4 parts: deformity (4 points), pain (44 points), movement scope (5 points), and functional activities (47 points).[34] Adverse reaction rate refers to the incidence of adverse reactions related to treatment or disease that occur during treatment.
2.6. Literature screening and data extraction
Two researchers independently extracted data and used a pre-designed collection form to collect study title, first author, year of publication; sample size, age, and gender of patients; intervention measures and intervention frequency; and clinical outcome measures and adverse reactions. Finally, these 2 researchers aggregated this information together. Discrepancies in the process are confirmed by consensus or by a third party.
2.7. Literature quality evaluation
We used the Cochrane Risk Bias Evaluation Tool to evaluate the quality of the literature, which mainly includes random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias.[35] The evaluation was conducted independently by 2 researchers and finally summarized. Discrepancies in the evaluation process were confirmed by consensus or by a third party.
2.8. Assessment of evidence quality
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method to evaluate the quality of evidence for each outcome, and evaluation criteria mainly include design, risk of bias, inconsistency, indirectness, imprecision, and other considerations. Randomized trials are regarded as high-quality evidence, and observational studies are regarded as low-quality evidence. According to the GRADE, outcomes of an intervention are classified into the following 4 levels of evidence quality: high, moderate, low, and very low, and are correspondingly expressed as, and.
2.9. Assessment of publication bias
We evaluate the publication bias by directly observing the funnel plots, which are made in Rev Man 5.3 software.
2.10. Data statistics and analysis
We used Rev Man 5.3 software to integrate these 10 studies for data analysis, which came from Cochrane Collaboration. For dichotomous outcomes, we used the Mantel–Haenszel (M–H) method to calculate risk ratios (RRs) as the effect scale, and while the outcomes are continuous variables, we used the inverse variance (IV) method to calculate the weighted mean differences (MDs) as the effect scale. And we computed the 95% confidence intervals (95%CI) as the effect amount. We used the I-squared statistic (I2) as a heterogeneity indicator, when I2 value is more than 50%, it means that the heterogeneity is significant, and then we choose the random-effects (RE) mode; contrarily, when I2 is no more than 50%, it means that the data heterogeneity is not significant, and we choose the fixed-effects (FE) model. Sensitivity and subgroup analyses were used to assess the stability of the evidence to the outcomes.
3. Results
3.1. Literature search
The literature search methods and screening criteria are all shown in the flow diagram (Fig. 1). A total of 474 relevant records were obtained by searching the database. By observing the title and abstract, 353 non-RCT studies were excluded, 74 duplicates were further excluded, 47 papers remained, and then according to the excluded criteria in the method as mentioned above, excluded 38 articles. Finally, 9 studies were obtained for the meta-analysis.[25–32,36]
Figure 1.
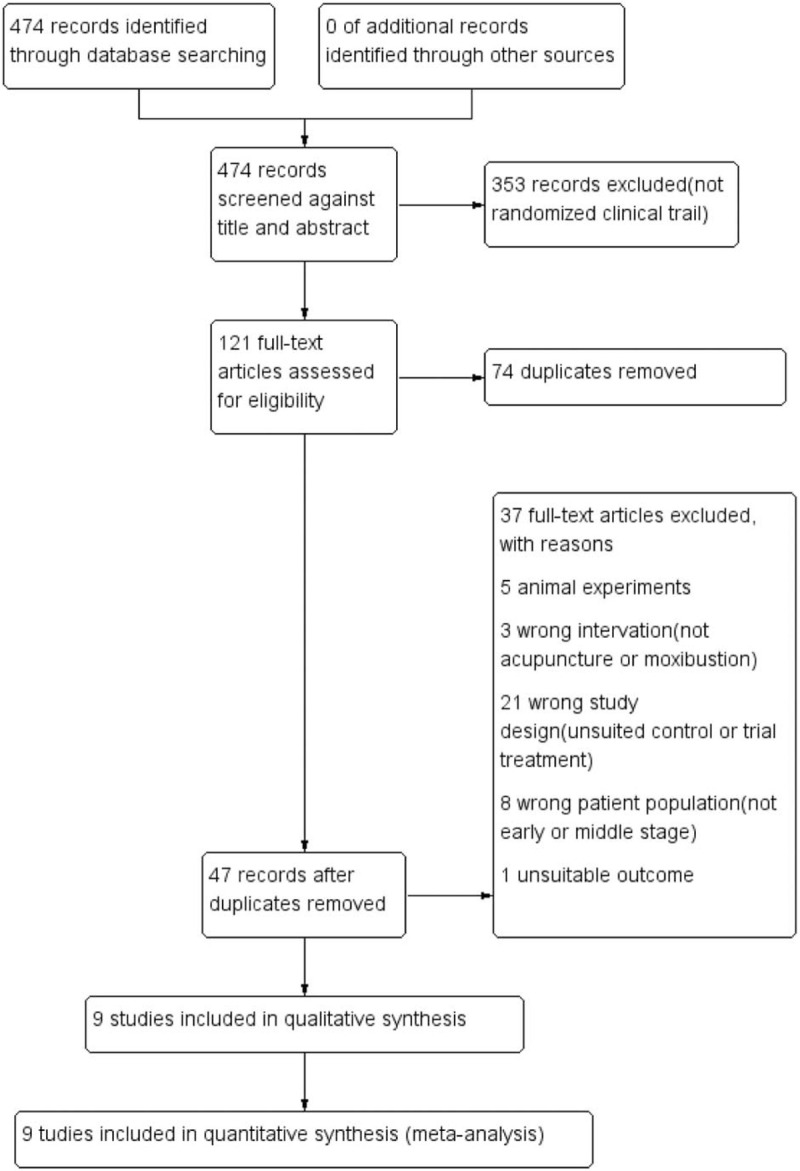
PRISMA flowchart of the literature.
3.2. Study characteristics
The basic characteristics of these studies are summarized in Tables 1 and 2. These literature were published in the past 10 years, from 2011 to 2020. The sample size of these trials ranges from 30 to 96. A total of 630 participants, aged between 18 and 79 years, were collected, with half of the control and trial groups. The treatment time ranges from 1 to 3 months. Of 9 included trials, the intervention measures are as follows: on the basis of 5 mL Guanxinning injection was injected into the hip joint cavity combined with AM (4 studies),[25–27,36] TCM internal and conventional treatment combined with AM (1 study),[28] oral steonecrosis apsule combined with AM (2 studies),[31,32] core decompression combined with EA (1 study),[30] and TCM comprehensive treatment combined with AM (1 study).[29]
Table 1.
Basic characteristics of included studies.
| Author | Year | Study type | Age (year) | Sample size male/female | Hips | Staging method | Treatment course (month) | Therapies |
| Bi[25] | 2011 | RCT | 18–70 | 60 | Early | 3 | ||
| C:56.78 | C:16/14 | C:42 | ARCO: | C:IAIG | ||||
| T:54.36 | T:19/11 | T:38 | I/II | T:IAIG+AM | ||||
| Guo[28] | 2015 | RCT | 60 | Early | 2 | |||
| C:44.167 ± 8.93 | C: 20/10 | ARCO: | C:TCM | |||||
| T: 43.933 ± 8.99 | T: 21/9 | 0/1/2 | T:TCM+AM | |||||
| Hu[27] | 2016 | RCT | 45–78 | 90 | Early | 3 | ||
| C: 61.3 ± 8.2 | C: 26/19 | C: IAIG | ||||||
| T: 61.8 ± 8.1 | T: 28/17 | T:IAIG+AM | ||||||
| Zhang[26] | 2018 | RCT | 44–79 | 72 | Early | 3 | ||
| C: 61.3 ± 8.2 | C:26/19 | C: IAIG | ||||||
| T: 61.8 ± 8.1 | T: 28/17 | T:IAIG+AM | ||||||
| Jin[30] | 2019 | RCT | 20–70 | 60 | Early&Middle | 3 | ||
| C: 39.8 ± 7.34 | C:18/12 | C:38 | Ficat: | C: CD | ||||
| T: 37.7 ± 6.8 | T:16/14 | T:36 | I/II | T: CD+EA | ||||
| Li[36] | 2019 | RCT | 55–77 | 30 | Early | 3 | ||
| C:66.32 ± 11.34 | C:10/5 | C: IAIG | ||||||
| T:66.47 ± 11.22 | T:11/4 | T:IAIG+AM | ||||||
| Mo[32] | 2020 | RCT | 20–60 | 96 | Middle | 2 | ||
| C: 45 ± 5 | C: 29/19 | C:57 | Ficat: | C: OC | ||||
| T: 45 ± 5 | T: 31/17 | T: 55 | II/III | T: OC+AM | ||||
| Mo[31] | 2020 | RCT | 22–55 | 82 | Early&Middle | 3 | ||
| C: 46 ± 9 | C: 27/14 | C:48 | ARCO: | C: OC | ||||
| T: 47 ± 10 | T: 25/16 | T: 47 | I/II/III | T: OC+IA | ||||
| Zhao[29] | 2020 | RCT | 24–75 | 60 | Early&Middle | 1 | ||
| C: 39.7 ± 6.74 | C: 18/12 | C:39 | China: | C: RT | ||||
| T: 41.9 ± 5.96 | T: 20/10 | T: 41 | I/II/III | T: RT+AM |
Table 2.
Therapies and clinical outcomes of included studies.
| Author Year | Therapies | Acupoints selection | Outcome |
| Bi 2011[25] | C:IAIG5 ml Guanxinning injection was injected into the hip joint cavity, twice a week for 12 weeks.T:IAIG+AMOn the basis of control group treatment, and combined with acupuncture treatment, 5 times a week (once a day) for 12 weeks | Zusanli (ST36), Huantiao (GB30), Sanyinjiao (SP6), Yanglingquan (GB34) | Effective rate; Excellent and good rate; Harris Hip Function Score |
| Guo 2015[28] | C:TCMTraditional Chinese medicine internal and conventional treatment for 2 months.T:TCM+AMOn the basis of control group treatment, combined with acupuncture and moxibustion, 5 times a week for 2 months | Huantiao (GB30), Huanzhong (extra point), Yanglingquan (GB34), Juliao (GB29), Xuanzhong (GB39) | Harris Hip Function Score; Effective rate; Visual Analogue Scale (VAS);Clinical efficacy standard (Cured, improved, not cured) according to Standards for diagnosis and treatment of traditional Chinese medicine |
| Hu 2016[27] | C: IAIG5 ml Guanxinning injection was injected into the hip joint cavity, twice a week for 3 months.T:IAIG+AMOn the basis of control group treatment, combined with acupuncture and moxibustion, 5 times a week for 3 months | Zusanli (ST36), Huantiao (GB30), Sanyinjiao (SP6), Yanglingquan (GB34) | Effective rate; excellent and good rate; hip joint function recovery time; incidence of related adverse reactions during treatment; total treatment time |
| Zhang 2018[26] | C: IAIG5 ml Guanxinning injection was injected into the hip joint cavity, twice a week for 3 months.T:IAIG+AMOn the basis of control group treatment, combined with acupuncture, 5 times a week for 3 months | Zusanli (ST36), Huantiao (GB30), Sanyinjiao (SP6), Yanglingquan (GB34) | Excellent and good rate; Harris Hip Function Score; Total treatment time; Hip joint function recovery time; Incidence of related adverse reactions during treatment |
| Jin 2019[30] | C: CDCore decompressionT: CD+EACombined electro-acupuncture after 2 weeks of core decompression for 3 months. | Juliao (GB29), Biguan (ST31), Xuehai (SP10), Fengshi (GB31), Zusanli (ST36), Yanglingquan (GB34), Weizhong (BL40), Sanyinjiao (SP6), Xuanzhong (GB39), Shenshu (BL23), Zhibian (BL54), Huantiao (GB30) | Effective rate; excellent and good rate; Harris hip function score; radiographic score |
| Li 2019[36] | C: IAIG5 ml Guanxinning injection was injected into the hip joint cavity, twice a week for 3 months.T:IAIG+AMOn the basis of control group treatment, combined with acupuncture, 5 times a week for 3 months | Not mentioned | Effective rate; Harris hip function score; incidence of related adverse reactions during treatment |
| Mo 2020[32] | C: OCoral Osteonecrosis Capsule, 5 capsules each time, 3 times a day for 2 months.T: OC+AMOn the basis of control group treatment, combined with acupuncture and moxibustion, 5 times a week for 2 months | Pain point, Huanzhong (extra point), Yanglingquan (GB34), Wuanzhong (GB39), Zusanli (ST36), Shenshu (BL23), Taixi (KI3), Xuehai (SP10), Sanyinjiao (SP6), Taichong (LR3) | Effective rate; excellent and good rate; plasma specific viscosity; ehole blood high shear viscosity; the volume of osteonecrosis; The grayscale of osteonecrosis area; the grayscale of femoral head |
| Mo 2020[31] | C: OCoral steonecrosis apsule, 5 capsules each time, 3 times a day, with regular exercise for 1 month. And in the next 2 months, change to 2 times a day.T: OC+IAOn the basis of control group treatment, combined with acupuncture and moxibustion, once a month for 3 months | Not mentioned | Effective rate; excellent and good rate; Harris hip function score; serum VEGF and BMP-2 levels; recurrence rate |
| Zhao 2020[29] | C: RTTraditional Chinese medicine comprehensive treatment.T: RT+AMOn the basis of control group treatment, combined with acupuncture, once a day for 1 month | Pain point, Dazhu (BL11), Yangfu (GB38), Neiting (ST44), Shangqiu (SP5), Xingjian (LR2), Taibai (SP3), Gongsun (SP4), Taichong (LR3), Neiting (ST44), Xiangu (ST43), Xiaxi (GB43), Diwuhui (GB42), Waiqiu (GB36), Zhongdu (LR6), Liangqiu (ST34), Jinmen (BL63), Yinlingquan (SP9), Zusanli (ST36), Lidui (ST45), Neiting (ST44), Zulinqi (GB41), Yanglingquan (GB34), Dadun (LR1) | Effective rate; clinical efficacy standard (cured, improved, not cured) according to Standards for diagnosis and treatment of traditional Chinese medicine |
3.3. Quality assessment (risk of bias assessment)
According to the evaluation criteria of quality assessment in the method as mentioned above, each risk of bias item is shown in Figures 2 and 3. One article was determined to have a high risk of allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), and selective reporting (reporting bias).[29] All other 8 articles were low risk or unclear risk of each bias item.
Figure 2.
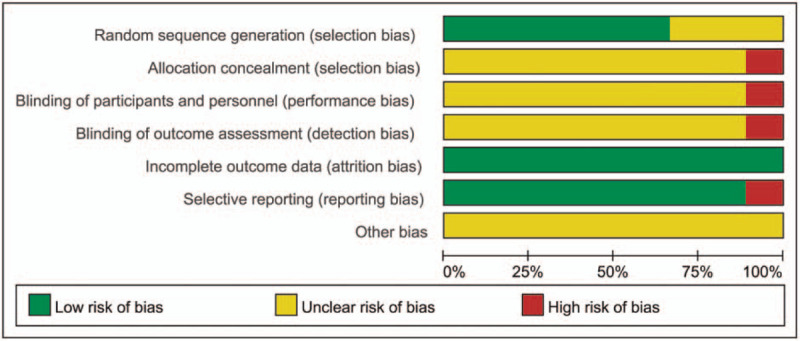
Risk of bias graph.
Figure 3.
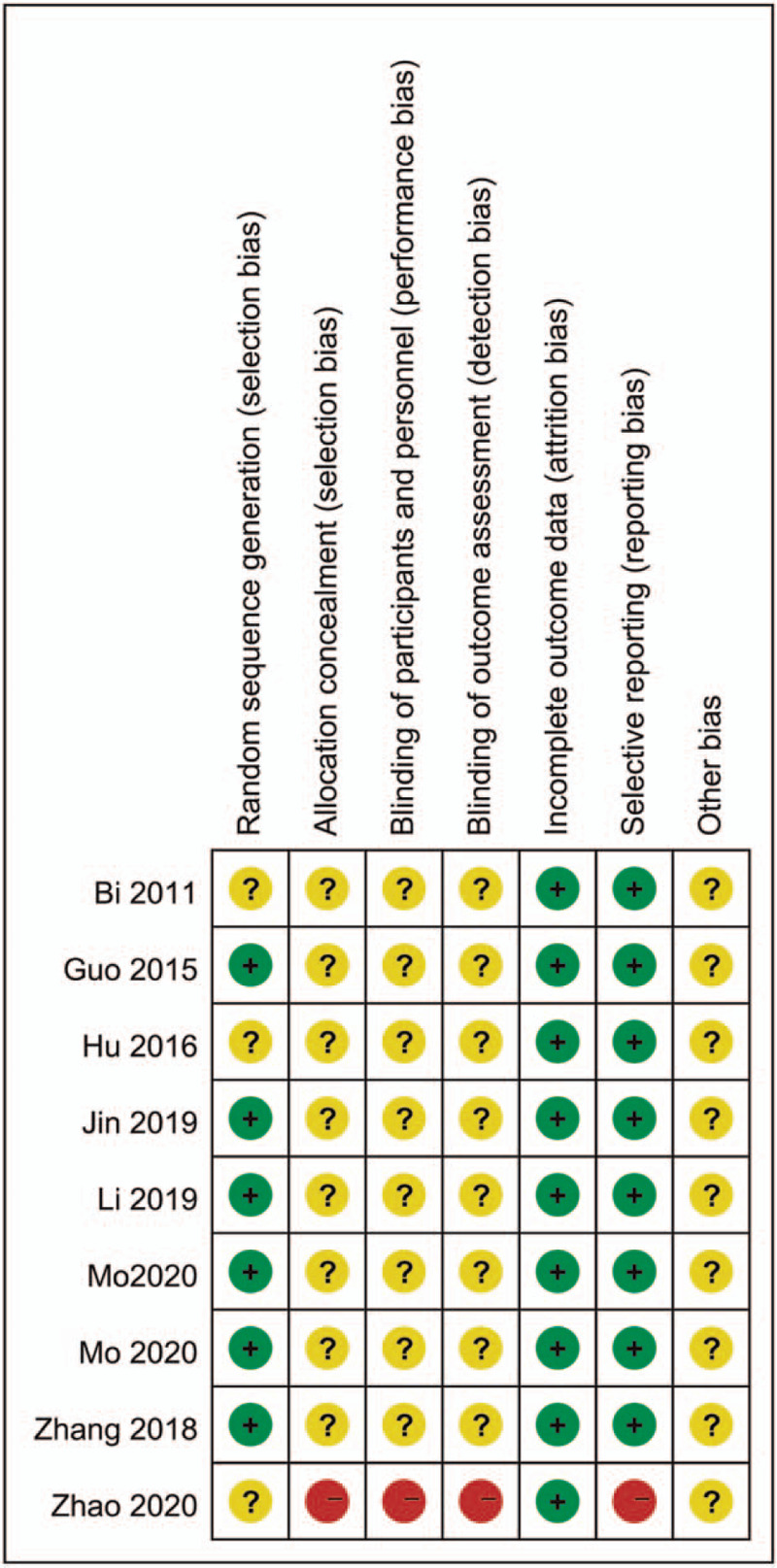
Risk of bias summary.
3.4. Clinical outcomes
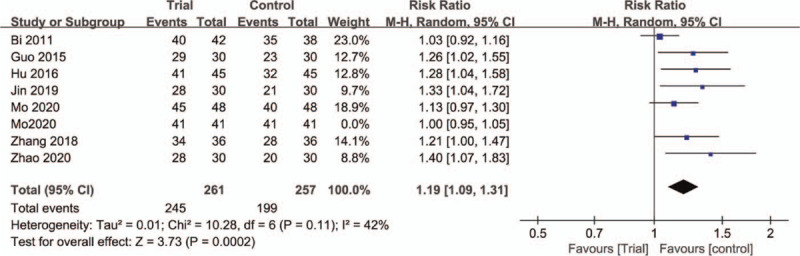
3.4.1. Effective rate
Eight trials reported on the effective rate of ONFH in the groups, and these trials showed high heterogeneity (I2 = 87% > 50%, χ2 = 53.91, df = 7, P < 0.00001); therefore, a random effect model was used for statistical analysis. Meta-analysis showed that overall effect – Z = 2.27 (P = .02), RR = 1.18, 95%CI [1.02–1.36] – indicated there was a significant difference found to benefit the trial group (Fig. 4).
Figure 4.
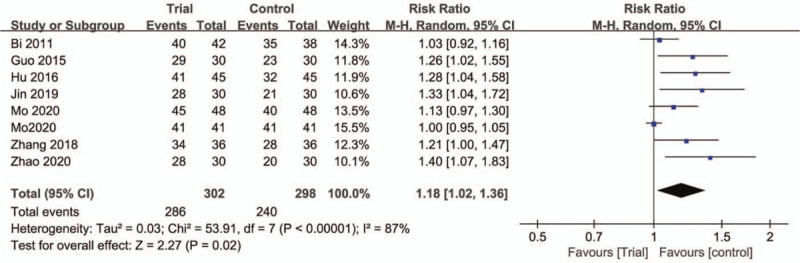
Forest plots of comparison of effective rate between trial group and control group.
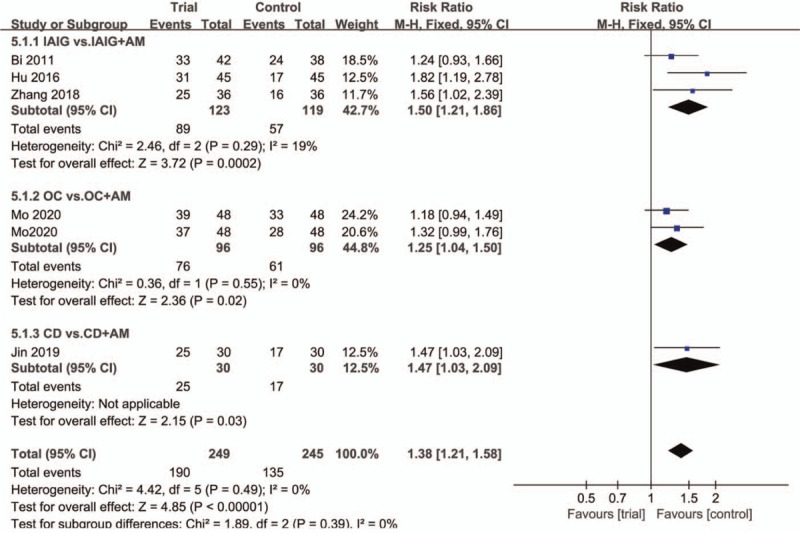
3.4.2. Excellent and good rate
Six trials reported on the excellent and good rate of ONFH in the groups, and these trials showed homogeneity (I2 = 0, χ2 = 4.42, df = 5, P = 0.49); therefore, an FE model was used for statistical analysis. Meta-analysis showed that overall effect – Z = 4.85 (P < 0.00001), RR = 1.38, 95%CI [1.21–1.58] – indicated there was a significant difference found to benefit the trial group (Fig. 5).
Figure 5.
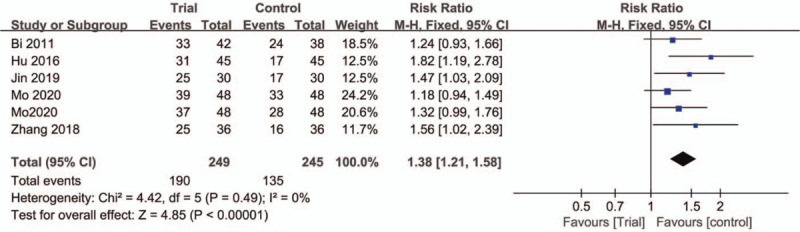
Forest plots of comparison of excellent and good rate between trial group and control group.
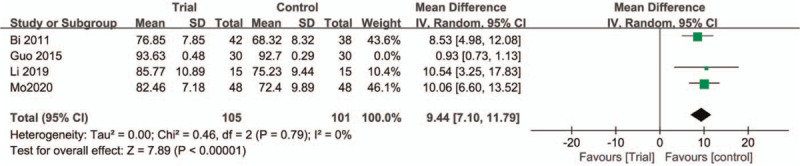
3.4.3. Harris hip function score
Four trials reported on HHS of ONFH in the groups, and these trials showed high heterogeneity (I2 = 94% > 50%, χ2 = 50.65, df = 3, P < 0.00001); therefore, a random effect model was used for statistical analysis. Meta-analysis showed that overall effect – Z = 2.31 (P < 0.02), MD = 7.19, 95%CI [1.08–13.29] – indicated there was a significant difference found to benefit the trial group (Fig. 6).
Figure 6.
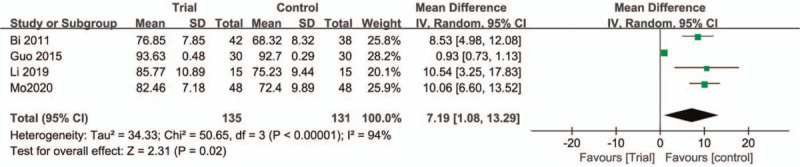
Forest plots of comparison of HHS between trial group and control group. HHS = Harris hip function score.
3.4.4. Adverse reaction rate
Three trials reported on the adverse reaction rate of ONFH in the groups, and these trials showed homogeneity (I2 = 0, χ2 = 0.17, df = 2, P = 0.92); therefore, an FE model was used for statistical analysis. Li group showed muscle cramps and pain occurred during treatment in several patients.[36] And Zhang study showed muscle numbness, pain, and skin itching occurred in several patients.[26] Meta-analysis showed that overall effect – Z = 2.82 (P = 0.005), RR = 0.22, 95%CI [0.08–0.63] – indicated combined AM treatment can reduce the adverse reaction rate of basic treatment alone for ONFH (Fig. 7).
Figure 7.
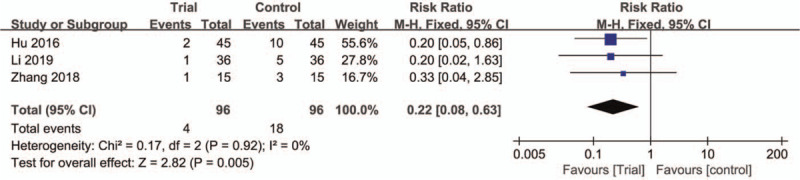
Forest plots of comparison of adverse reaction rate between trial group and control group.
3.5. Subgroup analysis and sensitivity analysis
To ensure the stability of the results, we conducted sensitivity analysis through the outcomes with high heterogeneity of effective rate (Fig. 8) and HHS (Fig. 9) and subgroup analysis through excellent and good rate (Fig. 10).
Figure 8.
Forest plots of comparison of effective rate between trial group and control group. “—”” represents the excluded study.[31]
Figure 9.
Forest plots of comparison of HHS between trial group and control group. “—” represents the excluded study.[28]
Figure 10.
Subgroup analysis of the excellent and good rate.
According to the forest plot of the effective rate that removed Mo study, we found the heterogeneity is significantly reduced (I2 decreased from 87% to 42%) (Figs. 4 and 8), indicating that Mo study is the main source of heterogeneity in the 8 studies included in the combined effective rate. Through a detailed analysis of the entire article, we found that the effective rate of treatment in the study was 100%, whether it was the control group or the trial group, this may be the main reason for the heterogeneity. According to the forest plot of HHS that removed Guo study, we found the I2 value decreased from 94% to 0% (Figs. 5 and 9), indicating that Guo study is the main source of heterogeneity in the 4 studies included in the HHS. Analyzing the reasons for the heterogeneity, we found that the Harris scores in Guo study before and after treatment were generally higher than the other 3 studies. It may be because the patient's condition was better, or the HHP of more than 80 points before treatment was an included criteria in Guo study, but this was not mentioned in Guo study, or the researcher himself has a higher estimate of the score.
Through the subgroup analysis of the excellent and good rate, we found that among the 3different interventions: 3 IAIG vs IAIG, 2 OC vs OC + AM, 1CD vs CD + AM, all showed the trial group had higher-excellent and good rate with a significant difference as follows: P = 0.0002, P = 0.02, and P = 0.03, and there was no significant difference between the subgroups (P = 0.39). These results indicated that combined AM can significantly improve the therapeutic effect, regardless of what the basic measure is (Fig. 10).
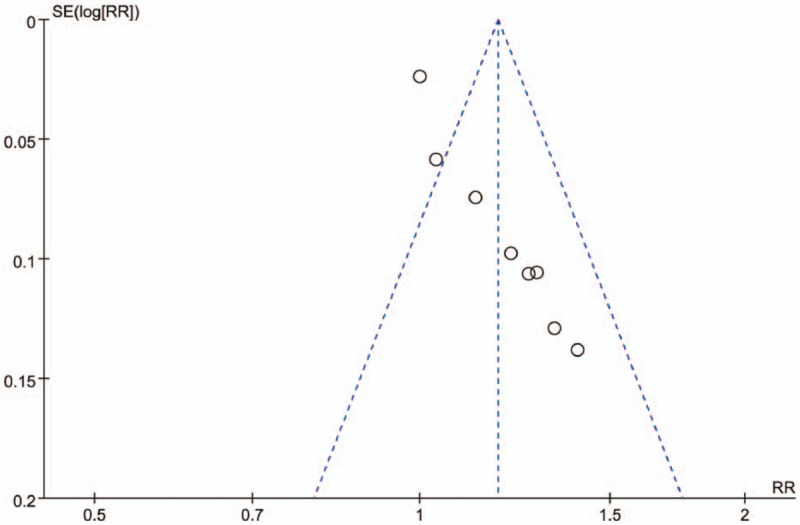
3.6. Publication bias
We used the inverted funnel diagram which indicated the effective rate and excellent and good rate to assess the publication bias. It seems that the funnel shape of the plot is not completely symmetrical, which indicated potential publication bias (Figs. 11 and 12).
Figure 11.
Funnel plot of the trials that compared the trial group with a control group of effective rate.
Figure 12.

Funnel plot of the trials that compared the trial group with a control group of excellent and good rate.
3.7. Evaluation of quality of evidence
The evaluation of the evidence quality for each outcome is shown in Figure 13. The results showed that the quality of evidence is moderate for each outcome.
Figure 13.
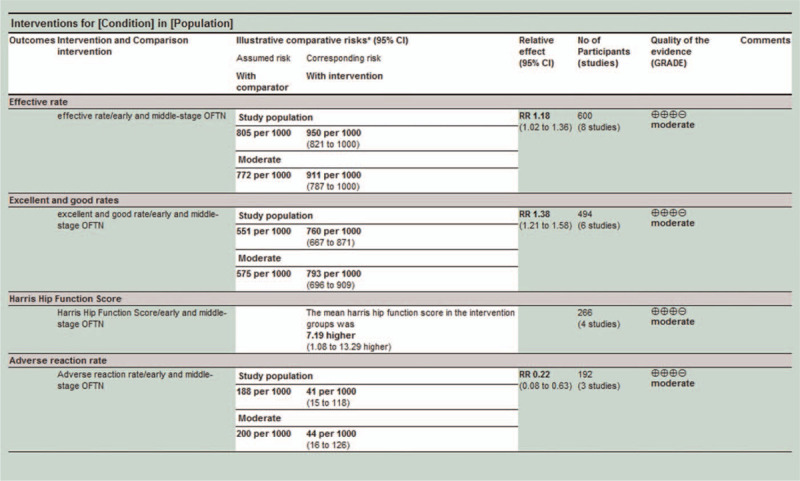
Assessment of quality of evidence.
4. Discussion
In this meta-analysis, all the selected studies are combined with AM on the basis of conventional therapy of the control group to summarize the advantages of AM. In all included studies, both the control group and the trial group were effective, and the symptoms of pain disappeared or alleviated, the range of motion and the function of the marrow joint were significantly increased. We found that the effective rate of the combined AM treatment group was significantly higher than that of the control group (Fig. 4). However, the heterogeneity of these 8 studies is significantly high. We thought that conventional therapy is also effective in the early and middle-stage ONFH, but the effect was improved after combined with AM. Therefore, the analysis of excellent and good rates should better reflect the advantages of combined AM (Fig. 5). The results showed that the excellent and good rate of the trial group was significantly higher than that of the control group, and these 6 trials showed a high degree of homogeneity. Then, subgroup analysis found that regardless of whether the treatment of the control group was the intra-articular injection of Guanxinning (IAIG) or oral Osteonecrosis Capsule or core decompression, the excellent and good rate after combined AM treatment was significantly increased, which indicated the stability of this result (Fig. 10). The HHS result also illustrated the advantages of AM treatment of ONFH, which can significantly improve the patient's HHS score, indicating that AM plays a positive role in alleviating the patient's pain and restoring function (Fig. 6). Moreover, in the hip joint injection of Guanxinning injection treatment group, patients occasionally developed local adverse reactions such as muscle cramps and numbness, pain, and skin itching. On this basis, combined with AM, the adverse reaction rate was significantly reduced (Fig. 7). This implied that AM can improve safety. Furthermore, the results of the assessment of evidence quality indicated that these outcomes were reliable (Fig. 13). These results have reached a consistent conclusion that AM has a beneficial effect in the treatment of early and middle-stage ONFH and can promote the improvement of efficacy.
In recent years, AM has achieved good results in the treatment of chronic pain,[21,37–39] tumors,[40] inflammatory bowel disease,[41] primary osteoporosis,[42–44] etc. In addition, studies have shown that AM can clear the meridians, promote qi and blood circulation, relieve pain, dispel evil, reconcile yin and yang, dispel cold and insufficiency, warm-up vitality, reconcile qi and blood, improve local blood circulation, and have a great effect on necrotic tissue.[20,23,24,45]
In the TCM system, ONFH belongs to the categories of “bone arthritis,” “bone atrophy,” and “bone erosion.”[8] The main pathogeneses are a trauma caused by blood stasis, insufficient blood supply, chronic strain, muscle and bone damage, or cold and dampness, blockage of qi and blood, or heat and blood stasis, skeletal dystrophy, or liver and kidney deficiency, insufficient blood supply, and muscles and bones loss of support. Blood stasis and liver and kidney deficiency are the most critical, and the most important treatment principle is to promote blood circulation to remove blood stasis and to replenish the liver and kidney.[45] In the studies included in this meta-analysis, the treatment of TCM whether it is an IAIG or oral Osteonecrosis Capsule or TCM internal also follows this principle.[25–28,31,32,36]
In modern medicine, ONFH is common in post-traumatic patients who have suffered proximal femoral fractures, especially fractures below the femoral neck or hip dislocation.[46] It also occurs in patients with long-term use of glucocorticoids, alcoholism, lupus, sickle cell disease, leukemia-lymphoma, and AIDS.[47–50] During treatment, firstly intervene the cause of the disease, and then reduce the weight-bearing and walking, reduce the load on the weight-bearing area of the femoral head, and avoid the weakened bone tissue from microfracture and collapse. At the same time, drugs or other measures are used to promote bone regeneration and diseased tissue repair.[51] At present, the most commonly used clinical treatments are core decompression surgery and transplantation of bone marrow cells.[52–54] In this meta-analysis, a study on the treatment of ONFH with CD was also included. In this study, the excellent and good rates were 70% when treated with CD alone, and increased to 93.33% after combined AM treatment.[30] It indicated that even if the intervention of early and middle-stage ONFH through modern medical methods, and combined AM can also play a good role in improving the efficacy. Clinically, in the treatment of early and middle-stage ONFH, conventional therapy can be combined with AM to improve efficacy.
4.1. Limitation
There are some shortcomings in this meta-analysis. First, the included studies have potential publication bias. Second, the effective rate and HHS showed high heterogeneity, which may lead to unreliable results. Third, the outcomes in the included studies are all detected immediately after the end of the treatment course, and the follow-up time and the number of follow-ups are not shown, so it is impossible to determine the long-term effect of the patient after receiving the treatment. AM is also necessary for the long-term effect of treating ONFH. Fourth, detailed imaging results, such as X-ray or MRI, should be added to the judgment of the curative effect of ONFH. Fifth, the included study should be based on more modern medical methods and combined with AM to fully explain the advantages of AM of ONFH. Finally, the included studies are all Chinese studies, and there are only 9 papers, and the results may not be comprehensive. Therefore, the research results may not be applicable to regions outside of China and should be interpreted with caution.
5. Conclusion
The available evidence shows AM combined with conventional therapy can significantly improve the efficacy of early and middle-stage ONFH compared with conventional therapy alone, mainly manifested as increased effective rate, excellent and good rate and HHS, and AM can also be considered as an adjuvant treatment for early and middle-stage ONFH because it can reduce the adverse reaction rate. However, the quantity and quality of the existing data are insufficient, and future studies need larger sample sizes, better designs, and high-quality RCTs to provide stronger evidence for research.
Author contributions
Data curation: Yong Fu, Hongguang Jin.
Formal analysis: Yong Fu, Hongguang Jin, Wen Yu.
Funding acquisition: Hongguang Jin, Yong Fu.
Investigation: Hongguang Jin, Linhui Li, Yong Fu.
Project administration: Yong Fu, Hongguang Jin, Linhui Li.
Supervision: Yong Fu, Hongguang Jin, Linhui Li, Wen Yu.
Writing – original draft: Yong Fu, Hongguang Jin.
Writing – review & editing: Hongguang Jin, Yong Fu.
Footnotes
Abbreviations: AM = acupuncture and moxibustion, CD = core decompression, EA = electro-acupuncture, HHS = Harris hip function score, IA = intensive acupuncture, IAIG = intra-articular injection of Guanxinning, OC = Osteonecrosis Capsule, ONFH = osteonecrosis of the femeral head, RCT = randomized controlled trial, RT = rehabilitation training, TCM = traditional Chinese medicine.
How to cite this article: Jin H, Li L, Yu W, Fu Y. The efficacy of acupuncture and moxibustion for early and middle-stage osteonecrosis of the femeral head: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2021;100:22(e26210).
This study is supported by a grant from the General Project of Natural Science Foundation of Inner Mongolia Autonomous Region (Grant no. 2018MS08035).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the present study are available from the corresponding author on reasonable request.
AM = acupuncture and moxibustion, ARCO = Association Research Circulation Osseous (ARCO) staging criteria, C = control Group, CD = core decompression, China = femoral head necrosis China staging criteria, EA = electro-acupuncture, Ficat = ficat staging criteria, IA = intensive acupuncture, IAIG = intra-articular injection of Guanxinning, OC = steonecrosis apsule, RCT = randomized controlled trial, RT = rehabilitation training, T = trail group, TCM = traditional Chinese medicine.
AM = acupuncture and moxibustion, CD = core decompression, EA = electro-acupuncture, IA = intensive acupuncture, IAIG = intra-articular injection of Guanxinning, OC = Osteonecrosis Capsule, RT = rehabilitation training, TCM = traditional Chinese medicine.
References
- [1].Zhao DW, Hu YC. Chinese experts’ consensus on the diagnosis and treatment of osteonecrosis of the femoral head in adults. Orthop Surg 2012;4:125–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Mont MA, Zywiel MG, Marker DR, McGrath MS, Delanois RE. The natural history of untreated asymptomatic osteonecrosis of the femoral head: a systematic literature review. J Bone Joint Surg Am 2010;92:2165–70. [DOI] [PubMed] [Google Scholar]
- [3].Zhao D, Zhang F, Wang B, et al. Guidelines for clinical diagnosis and treatment of osteonecrosis of the femoral head in adults (2019 version). J Orthop Translat 2020;21:100–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: where do we stand today? A ten-year update. J Bone Joint Surg Am 2015;97:1604–27. [DOI] [PubMed] [Google Scholar]
- [5].Panteli M, Rodham P, Giannoudis PV. Biomechanical rationale for implant choices in femoral neck fracture fixation in the non-elderly. Injury 2015;46:445–52. [DOI] [PubMed] [Google Scholar]
- [6].Malizos KN, Karantanas AH, Varitimidis SE, Dailiana ZH, Bargiotas K, Maris T. Osteonecrosis of the femoral head: etiology, imaging and treatment. Eur J Radiol 2007;63:16–28. [DOI] [PubMed] [Google Scholar]
- [7].Sun Y, Feng Y, Zhang C. The effect of bone marrow mononuclear cells on vascularization and bone regeneration in steroid-induced osteonecrosis of the femoral head. Joint Bone Spine 2009;76:685–90. [DOI] [PubMed] [Google Scholar]
- [8].Xiaoyang L. Analysis on professor BI Rong-Xiu's herbal prescription experience for steroid-induced avascular necrosis of femoral head based on traditional Chinese medicine inheritance support system. (Chinese). Chin J Exp Tradit Med Formulae 2016;22:177–81. [Google Scholar]
- [9].Zhonghua G. Clinical efficacy and safety of da huoluowan in treatment of osteonecrosis with phlegm stasis Syndrome. (Chinese). Chin J Exp Tradit Med Formulae 2018;24:172–7. [Google Scholar]
- [10].Yi-fei L. Exploration of the etiology and mechanism of femoral head necrosis based on “collateral disease theory.” (Chinese). Lishizhen Med Mater Med Res 2019;30:1939–41. [Google Scholar]
- [11].Qinghua X. Observation on curative effect of 240 cases of avascular necrosis of femoral head treated by chinese herbal medicine. (Chinese). Chin J Tradit Med Traumatol Orthop 2012. [Google Scholar]
- [12].Tao G. Observation on therapeutic effect of TCM syndrome differentiation on avascular necrosis of femoral head. (Chinese). Inner Mongolia J Tradit Chin Med 2017;12:22–3. [Google Scholar]
- [13].Shipeng H. A Randomized controlled study of TCM treatment of non-traumatic avascular necrosis of femoral head. (Chinese). Guangming J Chin Med 2020;35:2977–80. [Google Scholar]
- [14].Weidong B. Advances in hip-preserving treatment with traditional Chinese medicine for early and mid-term adult femoral head necrosis. (Chinese). Rheum Arthritis 2019;8:73–6. [Google Scholar]
- [15].Xiaoqing Z. Observation on the curative effect of tongmai bugu decoction combined with electroacupuncture on femoral head necrosis. (Chinese). Shanxi J Tradit Chin Med 2017;39:12254–55. [Google Scholar]
- [16].Yiqun L. Clinical observation on the treatment of early avascular necrosis of femoral head by external application of huoxue powder and sanqi huayu oral liquid. (Chinese). Chin J Tradit Med Traumatol Orthop 2016;24:13–9. [Google Scholar]
- [17].Yeh YA, Chiang JH, Wu MY, et al. Association of traditional chinese medicine therapy with risk of total hip replacement in patients with nontraumatic osteonecrosis of the femoral head: a population-based cohort study. Evid Based Complement Alternat Med 2019;2019:5870179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Guanghui L. Comparative observation of MRI before and after TCM treatment of avascular necrosis of femoral head. (Chinese). J Pract Tradit Chin Intern Med 2019;33:19–21. [Google Scholar]
- [19].Huanzhen L. Evaluation of the effect of MRI on the treatment of early avascular necrosis of the femoral head with traditional Chinese medicine. (Chinese). Chin Imag J Integr Tradit West Med 2017;15:186–8. [Google Scholar]
- [20].Zhang HW, Lin ZX, Cheung F, Cho WC, Tang JL. Moxibustion for alleviating side effects of chemotherapy or radiotherapy in people with cancer. Cochrane Database Syst Rev 2018;11:CD010559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain 2018;19:455–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med 2012;172:1444–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Yushui H. Acupuncture and moxibustion treatment of sterile ischemic femoral head necrosis. (Chinese). Shanghai J Acup Mox 1996;15:262. [Google Scholar]
- [24].Fufu Z. Retrospective analysis of 44 cases of femoral head necrosis treated with floating needle. (Chinese). Chin Acup Mox 2017;36:722–4. [Google Scholar]
- [25].Diankui B. Clinical observation on the treatment of femoral head necrosis by injection of Guanxinning into the hip joint cavity combined with acupuncture. (Chinese). Med Innov China 2011;8:19–20. [Google Scholar]
- [26].Zhirong Z. Acupuncture combined with Guanxinning for intra-articular injection of hip joint cavity for early non-traumatic femoral head necrosis: a randomized parallel controlled study. (Chinese). J Pract Tradit Chin Intern Med 2018;32:66–8. [Google Scholar]
- [27].Jianghong H. Analysis on the therapeutic effect of acupuncture and moxibustion in the treatment of early non-traumatic femoral head. (Chinese). Guangming J Chin Med 2016;31:3470–1. [Google Scholar]
- [28].Shengnan G. CIinical efficacy of early osteonecros is treated by warm acupuncture. (Chinese). Guangzhou Univ Chin Med 2015;01–25. [Google Scholar]
- [29].Hongqiang Z. Observation on the effect of acupuncture and moxibustion combined with rehabilitation in the treatment of early femoral head necrosis. (Chinese). J Front Med 2020;10:212–4. [Google Scholar]
- [30].Chenghui J. Electro-acupuncture combined with core decompression in treating 30 cases of avascular necrosis of femoral head in early and middle stages. (Chinese). J Shandong Univ TCM 2019;43:369–72. [Google Scholar]
- [31].Xiangtao M. Observations on the efficacy of intensive acupuncture plus medication for avascular necrosis of femoral head. (Chinese). Shanghai J Acup Mox 2020;39:589–93. [Google Scholar]
- [32].Xiangtao M. Effect of warm needling moxibustion plus Osteonecrosis Capsule on hip function and imaging indicators in patients with middle-stage avascular necrosis of femoral head. (Chinese). Shanghai J Acup Mox 2020;391:70–4. [Google Scholar]
- [33].Lopez-Lopez JA, Humphriss RL, Beswick AD, et al. Choice of implant combinations in total hip replacement: systematic review and network meta-analysis. BMJ 2017;359:j4651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Cooper AP, Basheer SZ, Maheshwari R, Regan L, Madan SS. Outcomes of hip arthroscopy. A prospective analysis and comparison between patients under 25 and over 25 years of age. Br J Sports Med 2013;47:234–8. [DOI] [PubMed] [Google Scholar]
- [35].Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Lei L. Observation on the clinical efficacy and adverse reactions of acupuncture and moxibustion treatment in patients with femoral head necrosis. (Chinese). Renowned Doctor 2016;31:3470–1. [Google Scholar]
- [37].Yun M, Shao Y, Zhang Y, et al. Hegu acupuncture for chronic low-back pain: a randomized controlled trial. J Altern Complement Med 2012;18:130–6. [DOI] [PubMed] [Google Scholar]
- [38].Weiss J, Quante S, Xue F, Muche R, Reuss-Borst M. Effectiveness and acceptance of acupuncture in patients with chronic low back pain: results of a prospective, randomized, controlled trial. J Altern Complement Med 2013;19:935–41. [DOI] [PubMed] [Google Scholar]
- [39].Gadau M, Yeung WF, Liu H, et al. Acupuncture and moxibustion for lateral elbow pain: a systematic review of randomized controlled trials. BMC Complement Altern Med 2014;14:136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Wu X, Chung VCH, Hui EP, et al. Effectiveness of acupuncture and related therapies for palliative care of cancer: overview of systematic reviews. Sci Rep 2015;5:16776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Stein DJ. Massage acupuncture, moxibustion, and other forms of complementary and alternative medicine in inflammatory bowel disease. Gastroenterol Clin North Am 2017;46:875–80. [DOI] [PubMed] [Google Scholar]
- [42].Xu G, Xiao Q, Zhou J, et al. Acupuncture and moxibustion for primary osteoporosis: an overview of systematic review. Medicine (Baltimore) 2020;99:e19334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Mak JC. Acupuncture in osteoporosis: more evidence is needed. Acupunct Med 2015;33:440–1. [DOI] [PubMed] [Google Scholar]
- [44].Inoue M, Nakajima M, Hojo T, Itoi M, Kitakoji H. The effect of electroacupuncture on osteotomy gap healing in a rat fibula model. Acupunct Med 2013;31:222–7. [DOI] [PubMed] [Google Scholar]
- [45].Shaochuan H. Experience of TCM treatment of early femoral head necrosis. J Pract Tradit Chin Intern Med 2012;28:790–1. [Google Scholar]
- [46].Scaglione M, Fabbri L, Celli F, Casella F, Guido G. Hip replacement in femoral head osteonecrosis: current concepts. Clin Cases Miner Bone Metab 2015;12:51–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Larson E, Jones LC, Goodman SB, Koo KH, Cui Q. Early-stage osteonecrosis of the femoral head: where are we and where are we going in year 2018? Int Orthop 2018;42:1723–8. [DOI] [PubMed] [Google Scholar]
- [48].Cohen-Rosenblum A, Cui Q. Osteonecrosis of the femoral head. Orthop Clin North Am 2019;50:139–49. [DOI] [PubMed] [Google Scholar]
- [49].Karimova EJ, Rai SN, Howard SC, et al. Femoral head osteonecrosis in pediatric and young adult patients with leukemia or lymphoma. J Clin Oncol 2007;25:1525–31. [DOI] [PubMed] [Google Scholar]
- [50].Lamb JN, Holton C, O’Connor P, Giannoudis PV. Avascular necrosis of the hip. BMJ 2019;365:l2178. [DOI] [PubMed] [Google Scholar]
- [51].Roth A, Beckmann J, Bohndorf K, et al. S3-guideline non-traumatic adult femoral head necrosis. Arch Orthop Trauma Surg 2016;136:165–74. [DOI] [PubMed] [Google Scholar]
- [52].Chughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J 2017;99-B:1267–79. [DOI] [PubMed] [Google Scholar]
- [53].Villa JC, Husain S, van der List JP, Gianakos A, Lane J. Treatment of pre-collapse stages of osteonecrosis of the femoral head: a systematic review of randomized control trials. HSS J 2016;12:261–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Theruvath AJ, Nejadnikh H, Muehe AM, et al. Tracking cell transplants in femoral osteonecrosis with magnetic resonance imaging: a proof-of-concept study in patients. Clin Cancer Res 2018;24:6223–9. [DOI] [PMC free article] [PubMed] [Google Scholar]