

Abstract
BACKGROUND AND PURPOSE: Flexion-extension radiography is neither sensitive nor specific in the diagnosis of degenerative spinal instability, a presumed cause of back pain and an indication for spinal fusion. We tested the hypothesis that with MR imaging and a device to rotate the torso, axial rotations of lumbar vertebrae can be measured with sufficient accuracy and that significantly different rotations can be detected between lumbar segments with degenerated disks and those with normal disks.
METHODS: We studied five volunteers without back pain (group 1), five patients who underwent MR imaging because of back pain but were not considered candidates for fusion (group 2), and five patients in whom diskography identified one or more disks with concordant pain (group 3). Each participant was placed on a specially built table that provided separate supports for the torso and for the hips and legs. Series of sagittal images were acquired with a T2-weighted fast spin-echo sequence, with the torso rotated clockwise and then counterclockwise. The amount of rotation was calculated from axial images with use of an automated program.
RESULTS: In the five volunteers, rotations of the lumbar motion segments varied between −1.8° and 5.7°, with an average of 0.8°. The abnormal disks in five patients in group 2 rotated from −0.9° to 5.6°, with an average of 3.2°. In group 3, the disks in which concordant pain was elicited rotated from 0.8° to 4.4°, with an average of 2.2°. Difference in rotation between abnormal and normal disks was statistically significant.
CONCLUSION: Measurements of rotations of lumbar vertebrae with MR imaging may have value for determining levels that move abnormally in axial rotation.
Flexion-extension radiography has been used to detect abnormal motions of the spine in patients with suspected degenerative spinal instability, a presumed cause of back pain and an indication for spinal fusion. Radiography of the spine in patients performing a flexion and extension maneuver is neither sensitive nor specific in the diagnosis of degenerative spinal instability (1–4).
The role of the intervertebral disk in degenerative spinal instability has been clarified by means of biomechanical cadaver studies (5–9). The normal lumbar intervertebral disk resists rotation in the axial plane because of the strong obliquely oriented fibers in the anulus fibrosus. With rupture of these fibers secondary to a radial tear of the anulus fibrosus, the resistance to a rotation in the axial plane is diminished markedly (10, 11). In biomechanical studies, a radial tear reduces the stiffness of the disk to axial rotatory forces by a factor of 2 or more, whereas it affects the stiffness to flexion or extension marginally. Therefore, in theory, abnormal mobility and decreased stiffness of the lumbar spine are detected more effectively by studying the motions of vertebrae subjected to an axial rotatory torque than to a flexion or extension torque.
Several investigators have attempted to measure axial rotations of the lumbar vertebrae. Invasive radiographic techniques have been developed for measuring axial rotation (12). An open design MR magnet has been used to noninvasively measure rotation of lumbar vertebrae in patients (P. K. Hol, M.D., Oslo Norway, personal communication, 2001). Johansen et al (13) used CT to measure the rotation of vertebrae in patients who were placed in positions of rotation by means of cushions. The long-term goal of this study is to develop methods to detect lumbar spinal instability based on measures of rotation of the lumbar vertebrae. The purpose of this preliminary study was to test the hypotheses that, with MR imaging and a table device to produce small rotations of the torso, axial rotations of lumbar vertebrae could be measured and significantly different degrees of rotation could be detected in lumbar segments with degenerated disks compared to segments with normal disks.
Methods
Participants
Three groups of subjects enrolled in the study. Group 1 consisted of five volunteers (three women, two men; mean age, 37 years) without back pain and without a history of severe back pain; these were considered the control subjects. Group 2 consisted of five patients (one woman, four men; mean age, 45 years) who underwent MR imaging because of back pain, but who were not considered surgical candidates for the treatment of back pain. In this group, diminished signal intensity in a lumbar intervertebral disk on a T2-weighted image or diminished disk height were inclusion criteria. Evidence of severe spinal stenosis or a destructive process was an exclusion criterion, but evidence of a disk herniation or bulging of the anulus was not. Group 3 included five patients (four women, one man; mean age, 36 years) who had consulted a neurosurgeon for back pain and who were considered candidates for a surgical fusion procedure. An inclusion criterion was a diskogram in which concordant pain was produced at one or more levels. Exclusion criteria were the same as those in group 2, plus evidence of radiculopathy or a history of treatment for back pain. Three additional patients with back pain were studied and then excluded because of artifacts on the images that precluded accurate measurement of rotation. Informed consent was obtained from each subject and approval for the study was obtained from our institutional review board.
Protocol
For the rotation study, each patient or volunteer was placed on a specially built table that provided separate supports for the torso and for the hips and legs (Fig 1). Each support could be rotated 8° in either direction. The table was placed on the gantry of a 1.5-T imager (GE Advantage; GE Medical Systems, Milwaukee, WI). With the patient positioned comfortably on the table and the gantry inserted into the imager, a series of sagittal images was acquired with a fast spin-echo sequence (2000/99/2 [TR/TEeff/NEX], 24-cm field of view, 192 × 256 matrix) for evaluating the signal intensity and morphology of each intervertebral disk. Then the gantry was removed from the imager. The hip support in the table was rotated 8°, right hip down, and the support under the torso was rotated 8°, left shoulder down. The gantry was returned to its former position in the imager, and a series of three-dimensional images was acquired in the sagittal plane with the spoiled gradient recalled acquisition in the steady state ([SPGR] 24/5/1 [TR/TE/NEX], 256 × 192 field of view, 2.0-mm section thickness). The gantry was then removed once more from the imager, and the rotations of the two table parts were reversed. The gantry was returned to the imager once more, and the SPGR sequence was repeated.
Fig 1.

Table insert that provides clockwise and counterclockwise rotation at the lumbar spine. The insert is placed on the MR gantry. The patient is positioned on the insert with head and thorax on the longer segment and hips on the shorter segment. The segments are on rollers that permit them to rotate 8° in a clockwise and a counterclockwise direction, with the axis of rotation centered at a point 10 cm above the segment, so that the spine is at the isocenter of rotation.
The amount of rotation at each lumbar intervertebral disk was calculated with an automated program developed at our institution. The rotation of vertebrae was measured by means of a pixel shift program similar to that used to adjust the masking image in digital subtraction angiography. In the series of images with clockwise rotation of the torso and the series with counterclockwise rotation, a section was chosen through the midportion of each vertebra to include the transverse process of the vertebra, or in the case of S1, the sacral alae (Fig 2A and B). The same section location was chosen for each vertebra in the two image series. One investigator (B.R.) placed a pivot point in the midline on the dorsal aspect of the vertebral body (Fig 2A and B). The program specified a region of interest surrounding the pivot point (illustrated by the cursor in Fig 2A and B and by Fig 2C and D) in which the pixel shift analysis is applied. One image (“floating image”) was then rotated and translated with respect to the other image (reference image) by Powell’s method as the correlation between images was calculated (14–16). Before application of the program, the floating image, when subtracted from the reference image, showed poor registration (2E). When the maximal correlation was achieved, the angle through which the image rotated was reported (illustrated by reference lines in Fig 2F). Alignment of the floating and reference images after rotation reveals improved registration in the subtracted image (2G). The rotation between two adjacent vertebrae was calculated as the difference between the rotations at contiguous levels. The rotation for each level was tabulated and compared with the MR appearance of the disk at that level and the diskographic findings.
Fig 2.
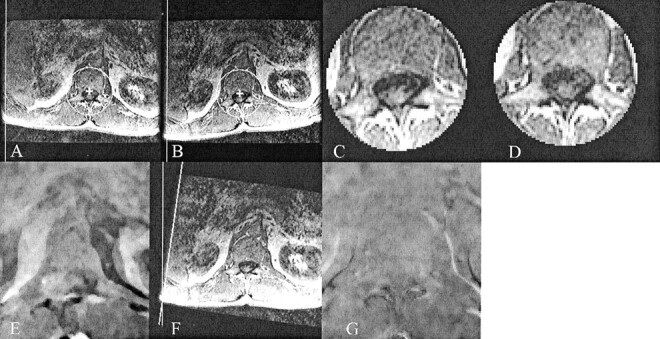
A–G, Images illustrate the application of the pixel shift program to measure rotation. The first step is to choose a vertebral level from each of the image sets with the thorax rotated clockwise (A) and counterclockwise (B). Note the vertical reference line to the left of each image. The next step is to choose the pivot point and region of interest for the pixel shift analysis (crosshairs and circular cursor in A and B). All voxels outside the cursor are excluded from analysis of motion (C and D). Alignment of the one image with the other before pixel shifting is illustrated by a subtraction image (E), which reveals a mismatch. When the one image is rotated with respect to the other to maximize the correlation, the angle of rotation (illustrated by the reference lines in F) is recorded. Alignment of the images after rotation is illustrated by a subtraction image (G), which shows no mismatch for the vertebral bodies.
To estimate the error due to inexact selection of the pivot point, we repeated the analysis with the “floating” and “reference” images reversed; we then repeated this sequence six more times with the pivot points moved by approximately 5 mm in a different direction each time. This gave 14 results, from which we estimated the error. The computations took about 5 minutes per subject. The measurements had a precision of about 0.5°, a higher degree of precision than that achieved by manual measurements previously described (13, 17).
The intervertebral disks in each participant were classified on the basis of the sagittal MR images. Disks with normal height, signal intensity, and annular borders were classified as normal. Disks with diminished signal intensity or height or both were classified as abnormal. These were further subdivided into those that had evidence on the sagittal and axial images of a bulging disk or herniation based on American Society of Neuroradioloy criteria (18). Evidence of endplate destruction, vertebral body destruction, or increased signal intensity 2in the disk was an exclusion criterion.
For diskography, standard techniques were employed (19). The selected disks were cannulated under fluoroscopic monitoring. Saline was injected, and the patient was asked to report the type of pain, if any. Pain produced by the injection that resembled the pain regularly experienced was classified as concordant pain. If no pain was produced or pain was not of the concordant type, the diskographic findings were classified as having no concordant pain at that level.
Each patient in group 3 was examined by the treating neurosurgeon 6 months after diskography. In those patients who underwent fusion after diskography, the level of fusion was noted, and the postoperative results were tabulated. The level of the concordant pain and the motions were compared.
The rotations for each level in the control subjects were averaged. Rotations for normal and abnormal disks in the volunteers and in the two patient groups were compared. Differences in mean rotation were tested for significance by means of a Student t test, with unequal variances assumed and significance set at .05.
Results
In the control subjects of group 1, 24 disks were classified as normal and one as abnormal (bulging disk). In the group 2 patients, 14 disks were classified as normal, three as herniated disks, and eight as bulging anulus. In this group, four of the abnormal disks were at L4-L5, four at L5-S1, and one each at L1-L2, L2-L3, and L3-L4. In group 3 patients, 18 disks were classified as normal and seven as bulging anulus (Fig 3). None had evidence of a herniation. Four of the abnormal disks were at L4-L5 and three at L5-S1.
Fig 3.

Sagittal T2-weighted image in a 29-year-old woman with chronic back pain. Intervertebral disks at L4–L5 and L5–S1 have diminished height, diminished signal intensity, and bulging of the posterior anulus fibrosus. No herniations are evident. Diskography subsequently showed concordant pain at the L4–L5 level only. The rotations were 0.3° at L1–L2, 1.3° at L2–L3, -0.1° at L3–L4, 2.2° at L4–L5, and 1.9° at L5–S1.
In the control subjects, rotations of the lumbar motion segments varied between −1.8° and 5.7°. Average rotation in this group was 0.8° (Table 1). The amount of rotation varied with level and increased toward the sacrum (Fig 4), from an average of −0.2° at L1-L2 to an average of 1.6° at L5-S1. This rostrocaudal increase in rotation was significant in this small sample (P < .005). The largest rotations in the control subjects were measured in the subject with a degenerated disk at L5-S1. This 23-year-old asymptomatic woman gave no history of back pain. In this volunteer, rotations at L5-S1 and three other levels exceeded the averages by a substantial amount. The rotation at L4-L5, 5.7°, exceeded the rotation of all other disks, normal or abnormal, in this series.
TABLE 1:
Rotations at each lumbar level in the control subjects
| Subject No. | Level | Rotation (degrees) | MR Appearance of Intervertebral Disk |
|---|---|---|---|
| 1 | L1-L2 | −1.0 | Normal |
| L2-L3 | 2.1 | Normal | |
| L3-L4 | 1.8 | Normal | |
| L4-L5 | 0.8 | Normal | |
| L5-S1 | 0.8 | Normal | |
| 2 | L1-L2 | −0.5 | Normal |
| L2-L3 | 0.3 | Normal | |
| L3-L4 | 1.7 | Normal | |
| L4-L5 | −0.4 | Normal | |
| L5-S1 | 1.9 | Normal | |
| 3 | L1-L2 | 0.5 | Normal |
| L2-L3 | 0.8 | Normal | |
| L3-L4 | −0.1 | Normal | |
| L4-L5 | 1.3 | Normal | |
| L5-S1 | 2.6 | Normal | |
| 4 | L1-L2 | 0.1 | Normal |
| L2-L3 | 0.9 | Normal | |
| L3-L4 | 1.0 | Normal | |
| L4-L5 | 1.3 | Normal | |
| L5-S1 | 1.2 | Normal | |
| 5 | L1-L2 | 3.0 | Normal |
| L2-L3 | −1.8 | Normal | |
| L3-L4 | −0.2 | Normal | |
| L4-L5 | 5.7 | Normal | |
| L5-S1 | 2.8 | Abnormal |
Fig 4.

Average rotation occurring at the five lumbar levels in the five control subjects as the gantry table is rotated left and right.
In group 2 patients, the rotations varied from −0.9° to 5.6°. Average rotation in the normal disks in this group was 1.1° and in the abnormal disks was 3.2° (Table 2).
TABLE 2:
Rotations at each lumbar level in patients with back pain and abnormal intervertebral disks
| Group 2 Patient No. | Level | Rotation (degrees) | MR Appearance of Intervertebral Disk |
|---|---|---|---|
| 1 | L1-L2 | −0.5 | Normal |
| L2-L3 | 1.0 | Normal | |
| L3-L4 | 2.3 | Normal | |
| L4-L5 | 0.6 | Abnormal | |
| L5-S1 | 4.2 | Abnormal | |
| 2 | L1-L2 | 3.7 | Abnormal |
| L2-L3 | 2.5 | Normal | |
| L3-L4 | 1.4 | Normal | |
| L4-L5 | −0.9 | Abnormal | |
| L5-S1 | 3.9 | Abnormal | |
| 3 | L1-L2 | 1.6 | Normal |
| L2-L3 | 1.1 | Normal | |
| L3-L4 | 5.6 | Abnormal | |
| L4-L5 | 0.0 | Normal | |
| L5-S1 | 1.5 | Normal | |
| 4 | L1-L2 | 2.2 | Normal |
| L2-L3 | 0.8 | Normal | |
| L3-L4 | −0.1 | Normal | |
| L4-L5 | 3.2 | Abnormal | |
| L5-S1 | 4.7 | Abnormal | |
| 5 | L1-L2 | 0.1 | Normal |
| L2-L3 | 2.2 | Abnormal | |
| L3-L4 | 2.0 | Normal | |
| L4-L5 | 3.4 | Abnormal | |
| L5-S1 | 3.1 | Abnormal |
In group 3 patients, the rotation varied from −1.9° to 4.4°. Average rotation for the normal disks in this group was 0.4° and for the abnormal disks was 2.2° (Table 3). For the disks in this group that had concordant pain, rotations were 0.8° to 4.4°. The abnormal disks were at L4-L5 and L5-S1. The two normal L5-S1 motion segments rotated an average of 1.6°, and the three motion segments at L5-S1 with concordant pain in this group rotated a mean of 3.3° (Fig 5). The difference was not significant (P = .07).
TABLE 3:
Rotations at each lumbar level in patients with concordant pain at diskography
| Group 3 Patient No. | Level | Rotation (degrees) | MR Appearance of Intervertebral Disk | Disk Abnormality | Level with Concordant Pain at Diskography | Level Fused | Follow-up after Fusion |
|---|---|---|---|---|---|---|---|
| 1 | L1-2 | 0.2 | Normal | Asymptomatic | |||
| L2-3 | 0.9 | Normal | |||||
| L3-4 | 0.8 | Normal | |||||
| L4-5 | 1.1 | Normal | |||||
| L5-S1 | 2.1 | Abnormal | Bulging anulus | X | X | ||
| 2 | L1-2 | 0.4 | Normal | Asymptomatic | |||
| L2-3 | 0.7 | Normal | |||||
| L3-4 | 0.7 | Normal | |||||
| L4-5 | 0.8 | Abnormal | Bulging anulus | X | X | ||
| L5-S1 | 1.0 | Normal | |||||
| 3 | L1-2 | 0.3 | Normal | Asymptomatic | |||
| L2-3 | 1.2 | Normal | |||||
| L3-4 | −0.1 | Normal | |||||
| L4-5 | 2.2 | Abnormal | Bulging anulus | X | X | ||
| L5-S1 | 1.9 | Normal | |||||
| 4 | L1-2 | −1.9 | Normal | Asymptomatic | |||
| L2-3 | 2.2 | Normal | |||||
| L3-4 | −1.3 | Normal | |||||
| L4-5 | 1.3 | Abnormal | Bulging anulus | ||||
| L5-S1 | 4.4 | Abnormal | Bulging anulus | X | X | ||
| 5 | L1-2 | 0.4 | Normal | Not applicable | |||
| L2-3 | 1.7 | Normal | |||||
| L3-4 | 0.8 | Normal | |||||
| L4-5 | 1.3 | Abnormal | Bulging anulus | X | |||
| L5-S1 | 3.4 | Abnormal | Bulging anulus | X |
Fig 5.

Average rotation at the two lower lumbar levels with normal disks (gray line) and those with concordant pain (black line) elicited at diskography in group 3 patients.
The five motion segments at L5-S1 in groups 2 and 3 with normal intervertebral disks rotated an average of 1.6°; the seven motion segments with abnormal disks in groups 2 and 3 rotated an average of 3.7°. The difference was significant at P = .0005. The three motion segments at L4-L5 in which concordant pain was identified in group 3 rotated an average of 1.4°, and the two motion segments with normal disks in group 3 rotated an average of 0.6° (Fig 5). The difference was not significant (P = .16). The five L4-L5 motion segments in groups 2 and 3 with normal disks rotated an average of 0.6°; the eight motion segments in groups 2 and 3 with abnormal disks rotated an average of 1.3°. The difference was significant at P = .03.
Five patients in group 3 had a diskogram at one or more levels that demonstrated concordant pain. Fusion was performed in four patients at the level with concordant pain. These four patients were pain-free after surgery, although one required revision owing to a pseudarthrosis. The criterion that the greatest rotation predicts the level at which concordant pain will be discovered with diskography yielded 18 true-negative, four true-positive, two false-negative, and one false-positive findings in group 3. The positive predictive value of the greatest rotation value for a positive diskogram was 80% and the negative predictive value was 90%. The fifth patient did not undergo spinal fusion.
Discussion
This preliminary study shows that with MR imaging and a device to produce a clockwise and counterclockwise rotation of the torso, rotations of the lumbar vertebrae can be measured. The rotations between vertebrae that have degenerated disks exceed those between vertebrae that have normal disks.
This study is a preliminary one, to assess a methodology. Neither age nor sex was controlled in this study, and either may have a small confounding effect on axial rotations. Normative data were obtained by selecting subjects without a history or complaint of back pain. However, this selection method does not ensure that biomechanically normal spines were included. One of our control subjects had evidence of disk degeneration at one level and evidence of hypermobility at multiple levels. The significance of this finding is speculative at the moment. We did not control for medication or spinal muscle spasm. We did not make comparisons with flexion and extension radiographs. The effect of facet joints on the rotations of the lumbar vertebrae was disregarded. In biomechanical studies (20), facet joints did not appear to limit or oppose rotations of the amount seen in this study. Patients were selected to include some with intervertebral disk degeneration and nonspecific signs and symptoms (group 2) and some with probable degenerative instability (group 3). There is no criterion standard at the moment for confirming that instability is present or not. Diskography is used to detect spinal instability, but the validity of the method is questioned (21). In our cases, the diagnosis of instability was suggested by diskography, by the clinical evaluation, and by the satisfactory results from fusion.
In this study, measurements agreed in general with our hypotheses and assumptions. We found significant differences in rotations between normal and abnormal intervertebral disks, as others have found (10, 11, 20). Abnormal rotation in the group 3 patients predicted an abnormal diskogram with some accuracy. The axial rotation measurements did not have a high predictive value of instability in patients in group 2, who had a low pretest probability of instability or abnormal motions as a cause of back pain. In group 2, abnormal disks had greater rotations than those of normal disks. We found that the rotations calculated with this method varied with level in the control subjects, as they do in spines of cadavers (5) and live humans (13). All these data suggest that the measurements of axial rotations in vivo with MR imaging provide accurate information about the motions of the lumbar motion segments.
The axial rotations measured in this study were in general less than those measured in the lumbar spine by others with other techniques. The cumulative rotation produced in the lumbar spine in our study averaged 4.7°, compared with 11° in subjects who performed an axial rotation while sitting (20) and 18° while standing (22). In a study of patients who were recumbent, with axial rotation applied by means of cushions and rotations measured with CT, the cumulative rotation was 16° (13). Johansen et al (13) found an average rotation of 2.6° in normal disks and 3.8° in abnormal disks. In comparison, we found average rotations of normal disks of 0.4° to 1.3°, depending on the group, and average rotation of 2.2° for abnormal disks with concordant pain. The differences between the results in our study and those previously reported are likely explained by the relatively mild degree of rotation applied in our study. The milder degree of rotation has the advantage that it is well tolerated by patients who have back pain.
Conclusions regarding the mobility of the spine in cases of an abnormal diskogram cannot be drawn at this time. In the absence of a reliable functional imaging technique for the detection of hypermobility or instability in the spine, investigators have attempted to identify imaging findings to predict instability. Correlations have been found between signal intensity in the lumbar intervertebral disks or vertebral body marrow and the presence of instability (23, 24). For the characterization of spinal instability or hypermobility, a noninvasive functional method is still sought (25). A method that identifies hypermobility between lumbar vertebrae might have value in selecting patients for spinal fusion. In some clinical settings, a measurement of spinal motions, if accurate and reliable, might replace some diskograms. Additional studies are warranted. With similar methods and CT, greater precision may be achieved than with MR imaging. Future study with carefully controlled patient groups and comparison of imaging techniques is warranted.
Conclusion
The results of this study show that rotations of lumbar vertebrae in patients or subjects rotated about the spinal axis may be measured with a specially designed table and MR imaging. Differences in mobility can be distinguished between disks that have a normal MR imaging appearance and those that have an abnormal appearance. An increase in rotation is detected in disks that produce “concordant pain” at diskography. Such measurements hypothetically have greater value than measurements from flexion-extension radiographs for studying the motions of spinal vertebrae in vivo. Further evaluation is warranted.
References
- 1.Quinnell R, Stockdale HR. Flexion and extension radiography of the lumbar spine: comparison with lumbar discography. Clin Radiol 1983;34:405–411 [DOI] [PubMed] [Google Scholar]
- 2.McCormick PC. Selection criteria for degenerative lumbar spine instability. Clin Neurosurg 1997;44:29–39 [PubMed] [Google Scholar]
- 3.Posner I, White AA, Edwards WT, Hayes WC. A biomechanical analysis of the clinical stability of the lumbar and lumbosacral spine. Spine 1982;7:374–389 [DOI] [PubMed] [Google Scholar]
- 4.Stokes IA, Frymoyer JW. Segmental motion and instability. Spine 1987;12:688–691 [DOI] [PubMed] [Google Scholar]
- 5.Nowicki BH, Haughton VM, Schmidt T, et al. Occult lumbar lateral spinal stenosis in neural foramina subjected to physiologic loading. AJNR Am J Neuroradiol 1996;17:1605–1614 [PMC free article] [PubMed] [Google Scholar]
- 6.Panjabi MM, Oxland TR, Yamamoto I, Crisco JJ. Mechanical behavior of the human lumbar and lumbosacral spine as shown by three dimensional load-displacement curves. J Bone Joint Surg Am 1994;76:413–424 [DOI] [PubMed] [Google Scholar]
- 7.Schultz AB, Warwick DN, Berkson MH, Nachemson A. 1979. Mechanical properties of human lumbar spine motion segments, I: responses in flexion, extension, lateral bending and torsion. J Biomech Eng 1979;10:46–52 [Google Scholar]
- 8.Mimura M, Panjabi MM, Oxland TR, Crisco JJ, Yamamoto I, Vasavada A. 1994. Disc degeneration affects the multidirectional flexibility of the lumbar spine. Spine 1994;19:1371–1380 [DOI] [PubMed] [Google Scholar]
- 9.Panjabi MM, Thibodeau LL, Crisco JJ 3rd, et al. What constitutes spinal instability? Clin Neurosurg 1988;34:313–319 [PubMed] [Google Scholar]
- 10.An HS, Haughton VM, Lim TH. 1996. The relationship between disc degeneration and kinematic characteristics of the lumbar motion segments [abstract]. Orthop Res Soc Proc 1996;42:663 [Google Scholar]
- 11.Haughton VM, Schmidt TA, Keele K, An HS, Lim TH. Flexibility of lumbar spinal motion segments correlated to type of tears in the annulus fibrosus. J Neurosurgery 2000;92:81–86 [DOI] [PubMed] [Google Scholar]
- 12.Lumsden RM 3rd, Morris JM. An in vivo study of axial rotation and immobilization at the lumbosacral joint. J Bone Joint Surg Am 1968;50:1591–1602 [PubMed] [Google Scholar]
- 13.Johansen JG, Nork M, Grand F. Torsional instability of the lumbar spine. Rivista di Neuroradiologia 1999;12 (suppl 2):193–195 [Google Scholar]
- 14.Penney GP, Weese J, Little JA, Desmedt P, Hill DLG, Hawkes DJ. A comparison of similarity measures for use in 2-D-3-D medical image registration. IEEE Trans Med Imaging 1998;17:586–595 [DOI] [PubMed] [Google Scholar]
- 15.Press WH, Teukolsky SA, Vettering WT, Flannery BP. Numerical Recipes in C . 2nd ed. New York: Cambridge University Press;1992. :994 ,412–420 [Google Scholar]
- 16.Acton FS. Mathematical Methods That Work (corrected edition). Washington, DC: Mathematical Association of America;1990. :464–467
- 17.Aaro S, Dahlborn M, Svensson L. Estimation of vertebral rotation in structural scoliosis by computer tomography. Acta Radiol 1978;19:990–992 [DOI] [PubMed] [Google Scholar]
- 18.Fardon DF, Milette PC, Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine 2001;26:E93–E113 [DOI] [PubMed] [Google Scholar]
- 19.Milette PC, Melanson D. A reappraisal of lumbar discography. JCAR 1982;33:176–182 [PubMed] [Google Scholar]
- 20.Schmidt TA, An HS, Lim TH, Nowicki BH, Haughton VM. The stiffness of lumbar spinal motion segments with a high-intensity zone in the anulus fibrosus. Spine 1998;23:216721–73 [DOI] [PubMed] [Google Scholar]
- 21.Krismer M, Haid C, Rabl W. The contribution of anulus fibers to torque resistance. Spine 1996;21:2551–2557 [DOI] [PubMed] [Google Scholar]
- 22.Gregersen GG, Lucas DB. An in vivo study of the axial rotation of the human thoracolumbar spine. J Bone Joint Surg Am 1967;49:247–262 [PubMed] [Google Scholar]
- 23.Bram J, Zanetti M, Min K, Hodler J. MR abnormalities of the lumbar intervertebral disks and adjacent bone marrow as predictors of segmental instability of the lumbar spine. Acta Radiol 1988;39:18–23 [DOI] [PubMed] [Google Scholar]
- 24.Toyone T, Takahashi K, Kitahara H, Yamagata M, Murakami M, Moriya H. 1995. Vertebral bone marrow changes in degenerative lumbar disc disease. J Bone Joint Surg 1995;765:757–764 [PubMed] [Google Scholar]
- 25.Nachemson A. Instability of the lumbar spine: pathology, treatment and clinical evaluation. Neurosurg Clin N Am 1991;2:785–790 [PubMed] [Google Scholar]