

Abstract
Background
Length of postnatal hospital stay has declined dramatically in the past 50 years. There is ongoing controversy about whether staying less time in hospital is harmful or beneficial. This is an update of a Cochrane Review first published in 2002, and previously updated in 2009.
Objectives
To assess the effects of a policy of early postnatal discharge from hospital for healthy mothers and term infants in terms of important maternal, infant and paternal health and related outcomes.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register, ClinicalTrials.gov, the WHO International Clinical Trials Registry Platform (ICTRP) (21 May 2021) and the reference lists of retrieved articles.
Selection criteria
Randomised controlled trials comparing early discharge from hospital of healthy mothers and term infants (at least 37 weeks' gestation and greater than or equal to 2500 g), with the standard care in the respective settings in which trials were conducted. Trials using allocation methods that were not truly random (e.g. based on patient number or day of the week), trials with a cluster‐randomisation design and trials published only in abstract form were also eligible for inclusion.
Data collection and analysis
Two review authors independently assessed trials for inclusion and risk of bias, extracted and checked data for accuracy, and assessed the certainty of evidence using the GRADE approach. We contacted authors of ongoing trials for additional information.
Main results
We identified 17 trials (involving 9409 women) that met our inclusion criteria. We did not identify any trials from low‐income countries. There was substantial variation in the definition of 'early discharge', ranging from six hours to four to five days. The extent of antenatal preparation and midwifery home care offered to women following discharge in intervention and control groups also varied considerably among trials. Nine trials recruited and randomised women in pregnancy, seven trials randomised women following childbirth and one did not report whether randomisation took place before or after childbirth.
Risk of bias was generally unclear in most domains due to insufficient reporting of trial methods. The certainty of evidence is moderate to low and the reasons for downgrading were high or unclear risk of bias, imprecision (low numbers of events or wide 95% confidence intervals (CI)), and inconsistency (heterogeneity in direction and size of effect).
Infant outcomes
Early discharge probably slightly increases the number of infants readmitted within 28 days for neonatal morbidity (including jaundice, dehydration, infections) (risk ratio (RR) 1.59, 95% CI 1.27 to 1.98; 6918 infants; 10 studies; moderate‐certainty evidence). In the early discharge group, the risk of infant readmission was 69 per 1000 infants compared to 43 per 1000 infants in the standard care group. It is uncertain whether early discharge has any effect on the risk of infant mortality within 28 days (RR 0.39, 95% CI 0.04 to 3.74; 4882 infants; two studies; low‐certainty evidence). Early postnatal discharge probably makes little to no difference in the number of infants having at least one unscheduled medical consultation or contact with health professionals within the first four weeks after birth (RR 0.88, 95% CI 0.67 to 1.16; 639 infants; four studies; moderate‐certainty evidence).
Maternal outcomes
Early discharge probably results in little to no difference in women readmitted within six weeks postpartum for complications related to childbirth (RR 1.12, 95% CI 0.82 to 1.54; 6992 women; 11 studies; moderate‐certainty evidence) but the wide 95% CI indicates the possibility that the true effect is either an increase or a reduction in risk. Similarly, early discharge may result in little to no difference in the risk of depression within six months postpartum (RR 0.80, 95% CI 0.46 to 1.42; 4333 women; five studies; low‐certainty evidence) but the wide 95% CI suggests the possibility that the true effect is either an increase or a reduction in risk.
Early discharge probably results in little to no difference in women breastfeeding at six weeks postpartum (RR 1.04, 95% CI 0.96 to 1.13; 7156 women; 10 studies; moderate‐certainty evidence) or in the number of women having at least one unscheduled medical consultation or contact with health professionals (RR 0.72, 95% CI 0.43 to 1.20; 464 women; two studies; moderate‐certainty evidence).
Maternal mortality within six weeks postpartum was not reported in any of the studies.
Costs
Early discharge may slightly reduce the costs of hospital care in the period immediately following the birth up to the time of discharge (low‐certainty evidence; data not pooled) but it may result in little to no difference in costs of postnatal care following discharge from hospital, in the period up to six weeks after the birth (low‐certainty evidence; data not pooled).
Authors' conclusions
The definition of 'early discharge' varied considerably among trials, which made interpretation of results challenging. Early discharge probably leads to a higher risk of infant readmission within 28 days of birth, but probably makes little to no difference to the risk of maternal readmission within six weeks postpartum. We are uncertain if early discharge has any effect on the risk of infant or maternal mortality. With regard to maternal depression, breastfeeding, the number of contacts with health professionals, and costs of care, there may be little to no difference between early discharge and standard discharge but further trials measuring these outcomes are needed in order to enhance the level of certainty of the evidence. Large well‐designed trials of early discharge policies, incorporating process evaluation and using standardized approaches to outcome assessment, are needed to assess the uptake of co‐interventions. Since none of the evidence presented here comes from low‐income countries, where infant and maternal mortality may be higher, it is important to conduct future trials in low‐income settings.
Keywords: Female; Humans; Infant; Pregnancy; Bias; Breast Feeding; Breast Feeding/statistics & numerical data; Depression, Postpartum; Depression, Postpartum/epidemiology; Infant Mortality; Length of Stay; Patient Discharge; Patient Readmission; Patient Readmission/statistics & numerical data; Postpartum Period; Term Birth; Time Factors
Plain language summary
Early postnatal discharge from hospital for healthy mothers and term infants
We set out to determine from randomised controlled trials the effects of a policy of early postnatal discharge from hospital for healthy mothers and term infants (born at 37 weeks of pregnancy or later) on maternal, infant and paternal health and related outcomes.
What is the issue?
Problems can develop or become clear after the birth of a baby. For example, women can experience excessive bleeding and infections, have problems with initiating breast feeding, and lack confidence in the care of their infants, and the baby may not thrive. In years gone by, women were kept in hospital to prevent or deal with these issues. The length of time women spend in hospital after childbirth has fallen dramatically in many countries over the past 50 years.
Why is this important?
It is not known whether having a shorter stay in hospital after birth is beneficial or harmful to women and their newborn infants. Earlier discharge of mothers and their babies has potential advantages, including a familiar environment and better sleep, less exposure to artificial schedules imposed in the hospital environment and decreased exposure to infection risks. However, leaving hospital earlier may result in missed opportunities for breastfeeding and infant care support and identification of infant and maternal health problems following birth. This review of trials compared the policy of early discharge after childbirth with standard length of stay and care at the time of the study.
What evidence did we find?
We searched for evidence in May 2021 and identified 17 trials involving 9409 women. The evidence is of low to moderate certainty because of limitations in the ways the studies were conducted. There was considerable variation in how early discharge was defined, ranging from six hours to four to five days. In most of the trials included in this review, early discharge was accompanied by some level of nursing or midwifery support. None of the trials took place in low‐income countries.
Early discharge probably slightly increases the number of babies readmitted to hospital within 28 days of being born (10 studies, 6918 babies, moderate‐certainty evidence). It is uncertain whether early discharge has any effect on the risk of babies dying within 28 days (two studies, 4882 babies). Early postnatal discharge probably makes little to no difference to the number of babies having at least one unscheduled medical consultation or contact with health professionals within the first four weeks after birth (four studies, 639 babies, moderate‐certainty evidence).
Early discharge probably results in little to no difference in the number of women readmitted to hospital within six weeks of giving birth for complications related to childbirth (11 studies, 6992 women, moderate‐certainty evidence). No deaths were reported. The number of women having at least one unscheduled medical consultation or contact with health professionals was not clearly different (two studies, 464 women, moderate‐certainty evidence). Similarly, early discharge may result in little to no difference in the risk of depression within six months after giving birth (five studies, 4333 women, low‐certainty evidence).
Early discharge probably results in little to no difference in the number of women breastfeeding at six weeks after giving birth or in the number of women having at least one unscheduled medical consultation or contact with health professionals.
Early discharge may slightly reduce the costs of hospital care with little to no difference in the cost of care from discharge to six weeks after the birth.
What does this mean?
The risk of babies being readmitted to hospital is probably higher following early discharge of mothers and their babies from hospital after the birth, but is probably not higher for women being readmitted to hospital after early discharge. We are uncertain about the risk of death for babies and mothers following early discharge, because these are uncommon events. Differences between early discharge and standard discharge in terms of maternal depression, breastfeeding, the number of contacts with health professionals and costs of care are not clearly different, and until further studies are done to investigate these factors, the evidence remains of low certainty.
Summary of findings
Summary of findings 1. Early discharge compared to standard discharge for healthy mothers and term infants.
| Early discharge compared to standard discharge for healthy mothers and term infants | ||||||
| Patient or population: healthy mothers and term infants Setting: maternity units Intervention: early discharge Comparison: standard discharge | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with standard discharge | Risk with early discharge | |||||
| Infants readmitted for neonatal morbidity within 28 days | Study population | RR 1.59 (1.27 to 1.98) | 6918 (10 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | Removing four trials with a high level of missing data in sensitivity analysis suggests that it is uncertain whether early discharge, compared with standard discharge, has any effect on the risk of infant readmission within 28 days (RR 1.10, 95% CI 0.67 to 1.81; 3647 infants). | |
| 43 per 1000 | 68 per 1000 (54 to 85) | |||||
| Infant mortality within 1 year | Study population | RR 0.45 (0.07 to 2.77) | 4984 (3 RCTs) | ⊕⊕⊝⊝ LOW 2 3 | ||
| 1 per 1000 | 1 per 1000 (0 to 3) | |||||
| Number of infants having contact with healthcare professionals regarding infant health issues within 4 weeks of birth | Study population | RR 0.88 (0.67 to 1.16) | 639 (3 RCTs) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 242 per 1000 | 213 per 1000 (162 to 281) | |||||
| Women readmitted within 6 weeks | Study population | RR 1.12 (0.82 to 1.54) | 6992 (11 RCTs) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 25 per 1000 | 28 per 1000 (21 to 39) | |||||
| Maternal mortality within 6 weeks ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Women probably depressed within 6 months | Study population | RR 0.80 (0.46 to 1.42) | 4333 (5 RCTs) | ⊕⊕⊝⊝ LOW 4 5 | ||
| 437 per 1000 | 349 per 1000 (201 to 620) | |||||
| Women breastfeeding (exclusively or partially) at 6 weeks postpartum | Study population | RR 1.04 (0.96 to 1.13) | 7156 (10 RCTs) | ⊕⊕⊕⊝ MODERATE 6 | ||
| 644 per 1000 | 670 per 1000 (619 to 728) | |||||
| Number of women having contact with healthcare professionals regarding maternal health issues within 6 weeks of giving birth | Study population | RR 0.72 (0.43 to 1.20) | 464 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 133 per 1000 | 96 per 1000 (57 to 160) | |||||
| Costs of hospital care in the period immediately following the birth up to the time of discharge | 3 studies reported lower hospital care costs for women in the early discharge groups compared to standard care group but the data were not suitable for analysis. | ‐ | 1011 (3 RCTs) | ⊕⊕⊝⊝ LOW 7 | ||
| Costs of postnatal care following discharge from hospital in the period up to 6 weeks after the birth | One study (459 women) reported higher postnatal care costs in the early discharge group. Another 2 studies (552 women) reported slightly lower postnatal care costs in the early discharge group. | ‐ | 1011 (3 RCTs) | ⊕⊕⊝⊝ LOW 7 | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: Randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Downgraded one level for risk of bias: some domains at high risk due to inadequate random sequence generation, lack of blinding of outcome assessors and differential attrition
2Downgraded one level for risk of bias: high or unclear risk of bias in random sequence generation, high risk of attrition bias
3Downgraded one level due to imprecision: very few events
4Downgraded one level due to imprecision: 95% confidence interval is consistent with possible benefit and possible harm
5Downgraded one level due to inconsistency: heterogeneity in direction and size of effect
6Downgraded half a level for risk of bias (unclear risk for random sequence generation, allocation concealment and selective reporting) and half a level for inconsistency (unexplained statistical heterogeneity)
7Downgraded two levels for imprecision: no overall effect estimate and no confidence intervals
Background
Since the 1970s, and earlier in some Western countries, there has been a steady decline in the length of time mothers spend in hospital after giving birth. From a standard hospital lying‐in period of between eight to 14 days in the 1950s (Rush 1989), length of postnatal hospital stay for an uncomplicated vaginal birth in Australia, Canada, Sweden and the USA is now around two to three days or less (Campbell 2016). Within the UK context, postnatal hospital stay has been decreasing since the 1970s (NHS Digital 2019). In 1975, 42% of postnatal women in England remained in hospital for seven days or more after birth, and in 2018‐19 this proportion had declined to 2%. Currently, 20% of women go home the same day of birth, with a further 38% on day one and 23% on day two, making a total of 82% being discharged within three days of birth. In parts of the USA, hospital stays of 12 to 24 hours for uncomplicated vaginal births, and 48 to 72 hours for uncomplicated caesarean births, had become standard by the mid‐1990s (Braveman 1995; Declerq 1997). Concern about possible adverse outcomes of early discharge led the USA Congress to pass legislation in 1996 mandating that private insurers cover postnatal stays of at least 48 hours after a vaginal birth, and 96 hours after a caesarean section. However, four years later, the majority of newborn term (at least 37 weeks' gestation) infants were still being discharged 'early' (Lansky 2006).
Description of the condition
The standard length of time a woman stays in hospital after giving birth varies between countries. In Australia, a five to seven day stay was the norm until the mid‐1990s (Day 1997), but in most other Western countries a shorter length of postnatal hospital stay had become standard well before this time (Braveman 1995; Rush 1989). As a result of these variations in practice, a length of stay of less than three days postpartum, which would have been considered standard in the late 1980s in countries such as the UK and the USA, would have been considered 'early discharge' in a country like Australia, at the same time point in history. This variation is reflected in the published literature on early discharge, with study participants discharged as early as six to 12 hours postpartum and as late as three to four days after the birth being considered in the early discharge category (Boulvain 2004; Yanover 1976).
Traditionally, women have been kept in hospital to prevent a number of possible adverse outcomes, which include delays in detecting and treating infant and maternal morbidity, greater occurrence of breastfeeding problems leading to earlier weaning, decreased maternal confidence due to lack of professional support, less maternal satisfaction with postnatal hospital care, higher prevalence of maternal depression, and increased infant and maternal readmissions (Braveman 1995; Britton 1994).
A series of population‐based cohort studies and case‐control studies have been conducted to assess the relationship between length of postnatal hospital stay and maternal and infant health‐related outcomes. These studies have produced conflicting results. Two studies exploring breastfeeding initiation and duration in Australia and Sweden found no association (Brown 2004; Waldenström 2004), whereas a study in California, USA found that women who left hospital earlier than the standard length of stay of two nights for a vaginal birth, and four nights for a caesarean section, were at a slightly increased risk of ceasing breastfeeding earlier (Heck 2003).
Studies examining the association between length of stay and hospital infant readmissions also report conflicting results. Liu 1997, Liu 2000 and Danielson 2000 found an association between shorter length of postnatal stay and increased rates of hospital readmission. In contrast, Edmonson 1997, Kotagol 1999 and Mandl 1997 reported no evidence of an association between shorter hospital stay and readmissions. The most recent study by Harron 2017 and colleagues found no association between postnatal length of stay and risk of readmission within 30 days for term infants. However, for premature infants between 34 and 36 weeks gestation, each additional day of postnatal stay in hospital was associated with a 8.6% decreased risk of readmission (95% confidence interval (CI) 6.1% to 10.5%). Another study conducted by Lain and colleagues found an association between longer length of birth hospitalisation and risk of readmission (Lain 2014).
Several studies have also examined the relationship between postnatal length of stay and jaundice‐related readmissions. The most recent population‐based study found that infants discharged from hospital in the first two days after birth were more likely to be readmitted for jaundice than infants who had a postnatal length of stay of three days or more (Lain 2015). Older studies raised concerns about early discharge leading to an increase in the number of infants developing severe hyperbilirubinaemia (Catz 1995; Maisels 1995). However, each of these reports was based on a very small number of cases, with no adequate comparison group for assessing the contribution early discharge may have made. Another large retrospective cohort study in the state of Washington, USA using routinely collected data for births between 1989 and 1990 found that newborns discharged before 30 hours of age had a significantly higher rate of mortality in the first month of life, and in the first year of life, than those newborns who stayed in hospital longer (Malkin 2000).
One important factor, which makes comparisons between studies conducted in different countries problematic, is the extent to which earlier discharge is accompanied by co‐interventions (for example, varying levels of antenatal preparation and post‐discharge support). An early discharge programme that includes frequent home visits from a health professional is likely to produce different results to an early discharge policy that does not include any after care in the community. The level of primary care support available to postnatal women once they leave hospital irrespective of the timing of discharge varies considerably between countries. In the UK, access to medical care from general practitioners and community midwives is universal and free at the point of service, and whilst the number of postnatal contacts in the community has decreased from seven to four over the last 30 years (Care Quality Commisson 2017; MacArthur 2002), community postnatal care provision is still deemed a critical aspect of postnatal care. This high level of service provision is possibly the reason there has been much less concern about the impact of earlier discharge of mothers and babies in the UK than in countries where access to primary care after discharge from hospital is limited (World Health Organization 2013). A population‐based study of postnatal care provided to healthy newborns conducted in 19 US states found that 11% to 49% of newborn infants discharged 'early' did not receive a follow‐up home visit within one week postpartum (Lansky 2006).
Description of the intervention
Shorter length of stay has been promoted in midwifery‐led care settings (for women and infants at low risk of complications) such as birth centres and is consistent with a move away from an illness orientation in maternity care towards a more family‐centred approach (Rush 1989; Waldenström 1987). From this perspective, earlier discharge of mothers and babies affords many potential advantages. These include the opportunity for all family members to be together as they get to know the baby, which would contribute to improved bonding, greater involvement of the father and less sibling rivalry (Britton 1994); the possibility that mothers may obtain more rest and sleep in their own home environments, where they are not exposed to constant interruptions and noise associated with hospital routines (Rush 1989); decreased exposure of the mother and the infant to nosocomial infections (Hellman 1962); enhanced maternal confidence in caring for the baby in the home environment (Rush 1989); and potentially fewer breastfeeding problems due to less conflicting advice and less exposure of the infant to the artificial schedules imposed in the hospital environment (Hellman 1962). The potential advantages of shorter postnatal hospital stays are in many respects the mirror image of the adverse outcomes identified by those with concerns for the safety of mothers and babies. There have been concerns that early discharge from hospital leaves insufficient time to establishing breastfeeding with direct support from health care professionals, resulting in an increase in feeding‐related problems such as weight loss, dehydration and jaundice (Gupta 2006). Concerns have also been raised that in the absence of further community support, early discharge may increase the delay in identification and treatment of maternal and infant morbidity including cardiac defects, as well as vitamin K administration and provision of contraceptive advice.
How the intervention might work
This review will look at the evidence comparing a policy of early discharge following birth with a standard length of stay in hospital. There is uncertainty whether the length of stay may be of benefit or otherwise to women and their families. While staying in hospital under the direct supervision of healthcare professionals may prevent potential morbidities and reduce re‐admission rates, earlier discharge home may mean more positive experiences of the first few days postpartum, improved bonding and higher breastfeeding rates.
Why it is important to do this review
While there are several other published reviews on this topic, the continuing reduction of length of postnatal stay in a number of countries and absence of clear evidence regarding safety, potential benefits for families, and costs associated with earlier postnatal discharge warrant the publication of a systematic review assessing current evidence from randomised controlled trials (RCTs).
Several systematic reviews of early postnatal discharge have been published (Beck 1991; Benahmed 2017; Braveman 1995; CETS 1997; Grullon 1997; Jones 2020; Margolis 1995; Norr 1987). Due to the lack of trial evidence in this area of study, the most recent of these have reviewed data from randomised controlled trials and non‐randomised studies to consider the effects on neonatal and maternal morbidity, maternal and infant readmissions and women's views of care (Benahmed 2017; Jones 2020). Whilst Benahmed and colleagues concluded that a link between early discharge and neonatal and maternal morbidity could neither be confirmed nor ruled out (Benahmed 2017), Jones and colleagues found that infants discharged early after birth were more likely to be admitted within 28 days. Furthermore, evidence from meta‐analysed interrupted times series data showed that the introduction of postnatal minimum length of stay policies in the United States between 1990‐2000 was associated with a long‐term reduction in neonatal hospital readmission rates (Jones 2020).
Due to the paucity of published trials in the review's earlier version, there was inadequate statistical power to detect increases in maternal or infant readmissions or rarer mortality outcomes (Brown 2002). Since the original review, new trials have been conducted which will contribute to the evidence base.
Objectives
To assess the effects of a policy of early postnatal discharge from hospital for healthy mothers and term infants in terms of important maternal, infant and paternal health, and related outcomes.
Methods
Criteria for considering studies for this review
Types of studies
All trials in which women or caregivers or institutions are allocated randomly or quasi‐randomly (e.g. alternate allocation) to different policies in relation to the timing of postnatal discharge of healthy mothers and term infants. Trials with a cluster‐randomisation design were eligible for inclusion. Studies with a cross‐over design would not be appropriate for this clinical question, so we did not include them. We included all RCTs regardless of publication status.
Types of participants
Women who give birth in hospital to a healthy infant of at least 2500 g at term (37 to 42 weeks) who are deemed eligible for 'early discharge'.
Types of interventions
A policy of early postnatal discharge from hospital for healthy mothers and infants born at term where 'early discharge' refers to discharge that is earlier than standard care in the setting in which the intervention is implemented. Standard care refers to the normal postnatal discharge policy in the setting in which the trial is implemented.
Types of outcome measures
Primary outcomes
Infant outcomes
Infants readmitted for neonatal morbidity (including jaundice, dehydration, infections) within seven days, and within 28 days after birth.
Maternal outcomes
Women readmitted for complications related to childbirth (including postpartum haemorrhage, retained products of conception, infection, postpartum psychosis) in the first six weeks after giving birth.
Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after giving birth.
Women breastfeeding (exclusively or partially) at six weeks, 12 weeks and six months after giving birth.
Secondary outcomes
Infant outcomes
Infant mortality within 28 days and within one year after birth.
Duration of infant readmissions for infants readmitted within seven days, and within the first 28 days after the birth.
Total duration of infant hospitalisation over the first 28 days.
Infants attending hospital casualty or emergency department within seven days, and the first six weeks after birth.
Number of contacts with health professionals regarding infant health issues within seven days, and the first six weeks after birth.
Maternal outcomes
Maternal mortality within six weeks and within one year after giving birth.
Duration of readmissions for women readmitted within first six weeks after giving birth.
Total duration of maternal hospitalisation over the first six weeks after giving birth (including period immediately after giving birth in addition to any readmissions).
Women attending hospital casualty or emergency department within first six weeks after giving birth.
Number of contacts with health professionals regarding maternal health issues within the first six weeks after giving birth.
Women reporting tiredness or exhaustion in the first six weeks after giving birth.
Women reporting physical health problems (including perineal pain, perineal infection, breast soreness, breast infection, caesarean wound pain, caesarean wound infection) in the first six weeks after giving birth.
Women reporting that they lacked confidence about caring for their baby in the first month and the first six months after being discharged from hospital.
Women reporting infant feeding problems in the first six weeks after giving birth.
Women reporting they received conflicting advice regarding breastfeeding in the first six weeks giving birth.
Women satisfied with overall postnatal care (including in hospital and/or post‐discharge care).
Women who perceive their length of hospital stay as too short.
Women who perceive their length of hospital stay as too long.
Partner outcomes
Partners reporting that they lacked confidence about caring for their baby in the first month and the first six months after the baby came home from hospital.
Partners reporting a high level of involvement with their baby in the first month and in the first six months after the birth.
Economic outcomes
Costs of hospital care in the period immediately following the birth up to the time of discharge.
Costs of postnatal care following discharge from hospital in the period up to six weeks after the birth, including community midwife, lactation consultant, general practice, specialist and outpatient visits; readmissions to hospital; attendances at day‐stay programs; in‐patient stays in mother and baby units.
Costs of practical support following discharge from hospital in the period up to six weeks after the birth, including paid and unpaid home help, care of the baby and of siblings.
Search methods for identification of studies
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
For this update, we searched Cochrane Pregnancy and Childbirth’s Trials Register by contacting their Information Specialist (21 May 2021).
The Register is a database containing over 25,000 reports of controlled trials in the field of pregnancy and childbirth. It represents over 30 years of searching. For full current search methods used to populate Pregnancy and Childbirth’s Trials Register including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL; the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service, please follow this link.
Briefly, Cochrane Pregnancy and Childbirth’s Trials Register is maintained by their Information Specialist and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Search results were screened by two people and the full text of all relevant trial reports identified through the searching activities described above were reviewed. Based on the intervention described, each trial report was assigned a number that corresponded to a specific Pregnancy and Childbirth review topic (or topics), and was then added to the Register. The Information Specialist searched the Register for each review using this topic number rather than keywords. This resulted in a more specific search set that has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Ongoing studies).
In addition, we searched ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform (ICTRP) for unpublished, planned and ongoing trial reports (21 May 2021), using the search methods detailed in Appendix 1.
Searching other resources
We also searched the reference lists of all retrieved articles.
We did not apply any language restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeBrown 2002.
For this update, the following methods were used for assessing the reports that were identified as a result of the updated search.
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Selection of studies
Two review authors independently assessed for inclusion all the potential studies identified as a result of the search strategy. We resolved any disagreement through discussion or, if required, we consulted the third review author.
Data extraction and management
We designed a form to extract data. For eligible studies, two review authors extracted the data using the agreed form. We resolved discrepancies through discussion and if required, the third review author was consulted. Data were entered into Review Manager 5 software (RevMan 2014) and checked for accuracy.
When information regarding any of the above was unclear, we planned to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2019). Any disagreement was resolved by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible selection bias)
For each included study, we described the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
For each included study, we described the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
For each included study, we described the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
For each included study, we described the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we planned to re‐include missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we had about other possible sources of bias.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as a summary risk ratio (RR) with its 95% CI.
Continuous data
We presented continuous data using the mean difference (MD) and 95% CIs where the outcome was measured in the same way in different trials. Where different scales were used to measure continuous outcomes, we combined the data using the standardised mean difference (SMD), with the following interpretation:
small effect: SMD ≥ 0.2 and < 0.5;
moderate effect: SMD ≥ 0.5 and < 0.8;
large effect: SMD ≥ 0.8.
Unit of analysis issues
Since all the data come from parallel group RCTs, the unit of analysis for maternal outcomes is per woman randomised. For infant outcomes, the unit of analysis is per infant. For multi‐arm trials where there are two groups defined as 'early discharge' and a third defined as 'standard discharge', e.g. with one group discharged at 12 to 24 hours after giving birth, another group discharged at 25 to 48 hours, and a third group discharged at three days, we analysed the two early discharge groups as one combined group.
We did not identify any cluster‐RCTs, but if we have data from such trials in future updates, we will include it in the analysis, along with individually randomised trials. We will adjust either their sample sizes or standard errors by using an estimate of the intracluster correlation coefficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population, as described in the CochraneHandbook (Higgins 2019). If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
Dealing with missing data
For included studies, we noted the levels of attrition. Many trials of early postnatal discharge had high levels of missing data due to women being excluded from the study after giving birth, because the circumstances of the birth meant they were no longer eligible for early discharge. We described the extent of missing data in the included studies, clearly distinguishing between data missing due to women no longer meeting the eligibility criteria and data missing due to women who were lost to follow‐up, women who chose to withdraw from the trial, or those who were excluded by the trialists for any other reason.
For all outcomes, analyses were carried out, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised, minus any women whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed heterogeneity in each meta‐analysis by visual inspection of forest plots and consideration of the I² statistic. Since strict thresholds to interpret I2 are not recommended, we used the following as a guide:
0% to 40%: might not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%: may represent substantial heterogeneity;
75% to 100%: considerable heterogeneity.
Where we identified evidence of heterogeneity, we explored it and described its possible causes.
Assessment of reporting biases
We investigated reporting biases (such as publication bias) using funnel plots for all meta‐analyses where 10 or more studies contributed data. When funnel plot asymmetry was detected, it was described and possible causes explored. If asymmetry was suggested by a visual assessment, we performed exploratory analyses to investigate it.
Data synthesis
Statistical analysis was carried out using the Review Manager 5 software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials were examining the same intervention, and the trials’ populations and methods were judged sufficiently similar.
If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discussed the clinical implications of treatment effects differing among trials. Where the average treatment effect was not clinically meaningful, we did not combine trials. If random‐effects analyses were used, the results were presented as the average treatment effect with 95% CIs, and the estimates of Tau2 and I2.
Subgroup analysis and investigation of heterogeneity
Substantial heterogeneity was investigated using subgroup analyses and sensitivity analyses. Where we identified substantial heterogeneity, we considered whether an overall summary was meaningful, and if it was, we used random‐effects analysis.
We carried out the following subgroup analyses.
Early discharge (less than 24/48 hours) versus later discharge.
Mode of birth (vaginal versus caesarean section).
To investigate the possible influence of changing clinical practice over time we also carried out post‐hoc subgroup analysis according to the decade when the trials were conducted.
Where data were sufficient, we carried out subgroup analyses for the following outcomes.
Infant outcomes
Infants readmitted for neonatal morbidity (including jaundice, dehydration, infections) within 28 days after birth.
Infant mortality within a year after birth.
Maternal outcomes
Women readmitted for complications related to childbirth (including postpartum haemorrhage, retained products of conception, infection, postpartum psychosis) in the first six weeks after giving birth.
Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after giving birth.
Women breastfeeding (exclusively or partially) at six weeks after giving birth.
We assessed subgroup differences by interaction tests available within RevMan 5 (RevMan 2014) and by investigating the extent of overlap between 95% CIs of the effect estimates belonging to each subgroup. We reported the results of subgroup analyses quoting the P value of the Chi2 statistic and the interaction test I2 value.
Sensitivity analysis
We performed sensitivity analyses to explore the effect of risk of bias assessed by random sequence generation, allocation concealment, and differential attrition, with studies at high risk of bias in those domains being excluded from the analyses in order to assess whether this made any difference to the overall result.
Sensitivity analyses were also planned to explore the impact of including studies with high levels of missing data, regardless of whether or not the proportion with missing data was balanced across treatment groups. This enabled us to address the issue of women being excluded from analyses after randomisation due to no longer meeting the criteria for early discharge (for example, some studies excluded women after randomisation if they had given birth via caesarean section). We considered a study to have a high level of missing data if 20% or more of the women randomised were not included in the analysis.
We performed sensitivity analyses on the following outcomes.
Infant outcomes
Infants readmitted for neonatal morbidity (including jaundice, dehydration, infections) within 28 days after birth.
Infant mortality within a year after birth.
Maternal outcomes
Women readmitted for complications related to childbirth (including postpartum haemorrhage, retained products of conception, infection, postpartum psychosis) in the first six weeks after giving birth.
Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after giving birth.
Women breastfeeding (exclusively or partially) at six weeks after giving birth.
Summary of findings and assessment of the certainty of the evidence
For this update, we assessed the certainty of the evidence using the GRADE approach, as outlined in the GRADE Handbook (Schünemann 2013). We assessed the certainty of the body of evidence relating to the following outcomes, for the main comparison of a policy of early discharge compared with standard discharge from hospital.
RCT data are initially considered to provide high‐certainty evidence but can be downgraded by one or two levels (for serious or very serious concerns, respectively) in the presence of study limitations (high risk of bias), indirectness of evidence, inconsistency of effect estimates and imprecision of effect estimates, as well as the potential of publication bias.
Infant outcomes
Infants readmitted to hospital for neonatal morbidity (including jaundice, dehydration, infections) within 28 days of birth.
Infant mortality within one year after birth.
Number of contacts with health professionals regarding infant health issues within the first four weeks after birth.
Maternal outcomes
Women readmitted for complications related to childbirth (including postpartum haemorrhage, retained products of conception, infection, postpartum psychosis) in the first six weeks after giving birth.
Maternal mortality within six weeks after giving birth.
Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after giving birth
Women breastfeeding (exclusively or partially) at six weeks after giving birth.
Number of contacts with health professionals regarding maternal health issues within the first six weeks after giving birth.
Costs of hospital care in the period immediately following the birth up to the time of discharge.
Costs of postnatal care following discharge from hospital in the period up to six weeks after the birth, including community midwife, lactation consultant, general practice, specialist and outpatient visits; readmissions to hospital; attendances at day‐stay programs; in‐patient stays in mother and baby units.
We used the GRADEpro Guideline Development Tool (GRADEpro GDT) to import data from Review Manager 5.3 (RevMan 2014) in order to create 'Summary of findings’ tables. A summary of the intervention effect and a measure of certainty for each of the above outcomes was produced using the GRADE approach. The GRADE approach has five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the certainty of the body of evidence for each outcome. The evidence was downgraded from 'high certainty' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, inconsistency of effect estimates, imprecision of effect estimates or potential publication bias.
Results
Description of studies
Results of the search
Figure 1 depicts our screening process.
1.
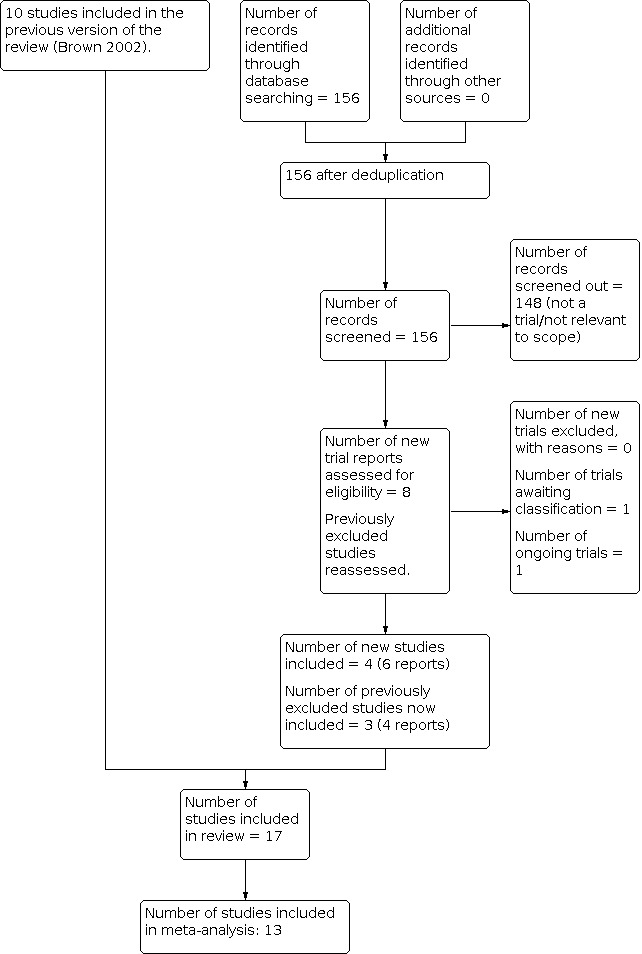
Study flow diagram.
The updated search retrieved 156 reports. We screened out 148 records and assessed eight reports. We also reassessed the excluded studies from the previous version of the review (Brown 2002). We included four new trials (six reports) (Bayoumi 2016; Chiong 2012; Kruse 2021; Taiba 2012), plus three trials that were previously excluded on the basis of lack of relevant outcomes (Burnell 1982; McKeever 2002; Thompson 1999). To adhere to current Cochrane standards we included these three excluded trials in this review because although they did not have useable outcome data, they meet our inclusion criteria.
One trial is ongoing (Namagembe 2014) and we added one trial to Studies awaiting classification for assessment at the next update, as there were no published results available (NCT04422041 2020)
Included studies
We identified 17 trials eligible for inclusion, involving 9409 randomised women. For details of each study, see Characteristics of included studies.
Design
All the included studies were RCTs that randomised women to different treatment groups. We did not identify any cluster‐RCTs. One trial was only available in abstract form.
Sample sizes
The largest trial included 3687 women (Bayoumi 2016). The other 16 trials recruited between 50 women (Thompson 1999) and 2257 women (Hellman 1962).
Many trials reported large differences in the numbers of eligible women willing to participate and the numbers of eligible women who declined participation in the trials. Most trials reported the proportion of women eligible to participate in the study in addition to the number of women randomised (Bayoumi 2016; Boulvain 2004; Burnell 1982; Carty 1990; Chiong 2012; Gagnon 1997; Kruse 2021; McKeever 2002; Smith‐Hanrahan 1995; Taiba 2012; Thompson 1999; Waldenström 1987). Five of the trials reported a participation rate less than 50% (Boulvain 2004; Gagnon 1997; Kruse 2021; Thompson 1999; Waldenström 1987). A further three trials recruited and randomised between 69% and 90% of women eligible (Burnell 1982; McKeever 2002; Smith‐Hanrahan 1995) and the remaining three trials reported 100% uptake to the trial (Carty 1990; Chiong 2012; Taiba 2012).
Setting
The trials included in this review compare 'early postnatal discharge' with standard length of hospital stay as defined in the time and place they were conducted. The trials were undertaken between 1959 (Hellman 1962) and 2019 (Kruse 2021).
We identified no studies from low‐income countries. Thirteen studies were from high‐income countries; four took place in Canada (Carty 1990; Gagnon 1997; McKeever 2002; Smith‐Hanrahan 1995), three in the USA (Brooten 1994; Hellman 1962; Yanover 1976), two in the United Kingdom (Burnell 1982; Winterburn 2000), and one each in Australia (Thompson 1999) Denmark (Kruse 2021), Spain (Sainz Bueno 2005), Sweden (Waldenström 1987), and Switzerland (Boulvain 2004). The remaining three studies took place in middle‐income countries; one each in Bangladesh (Taiba 2012), Egypt (Bayoumi 2016) and Malaysia (Chiong 2012).
Participants
The study populations differed considerably among trials. Five trials only included women who were planning, or already had, a caesarean section birth (Bayoumi 2016; Brooten 1994; Chiong 2012; Kruse 2021; Taiba 2012). Ten studies only included women who had given birth vaginally (Burnell 1982; Carty 1990; Gagnon 1997; Hellman 1962; McKeever 2002; Sainz Bueno 2005; Smith‐Hanrahan 1995; Thompson 1999; Waldenström 1987; Yanover 1976) and the final two studies included women who had given birth via caesarean section or vaginally (Boulvain 2004; Winterburn 2000).
In nine trials, randomisation took place in pregnancy, usually between 30 weeks and 38 weeks' gestation (Boulvain 2004; Burnell 1982; Carty 1990; Gagnon 1997; Kruse 2021; Thompson 1999; Waldenström 1987; Winterburn 2000; Yanover 1976). Seven trials randomised women immediately after the birth (Bayoumi 2016; Brooten 1994; Chiong 2012; Hellman 1962; McKeever 2002; Sainz Bueno 2005; Smith‐Hanrahan 1995). One trial did not describe whether randomisation took place before or after birth.
Most trials specified eligibility criteria designed to limit participation to women at lower risk of complications, although five of the trials included only women who had a caesarean section (Bayoumi 2016; Brooten 1994; Chiong 2012; Kruse 2021; Taiba 2012). In nine trials, pre‐randomisation inclusion criteria were designed to select women at low medical risk (Boulvain 2004; Carty 1990; Gagnon 1997; Sainz Bueno 2005; Smith‐Hanrahan 1995; Waldenström 1987; Winterburn 2000; Yanover 1976). Eight of these trials recruited both women having their first or subsequent children. The trial conducted by Winterburn and colleagues recruited only women having their first child and planning to breastfeed (Winterburn 2000). Yanover and colleagues specified a number of social eligibility criteria including a requirement that prospective parents currently live together, completion of the final year of high school by mothers, and willingness of fathers to attend prenatal classes (Yanover 1976). Two trials were designed to select women at higher medical risk; the first was the study by Brooten and colleagues that recruited women who had an unplanned caesarean section (Brooten 1994) and the second (Chiong 2012) recruited women after 37 weeks' gestation undergoing planned caesarean section.
Follow‐up of participants varied from seven days (Taiba 2012) to one year following childbirth (Bayoumi 2016; Hellman 1962; Waldenström 1987).
Interventions and comparisons
There was substantial heterogeneity in what constituted 'early discharge', to the extent that a length of postnatal hospital stay defined as 'early discharge' in one study was the standard length of postnatal stay in other settings. Standard discharge policies also varied greatly.
We have summarised the interventions and comparisons in Table 2.
1. Description of interventions.
| Study | Early discharge | Standard discharge |
| Bayoumi 2016 | 24 hours after delivery (caesarean births only) | 72 hours after delivery (caesarean births only) |
| Boulvain 2004 | 24 to 48 hours following vaginal births 72 to 84 hours after caesarean births plus home based postnatal care |
hospital based postnatal care then discharge at 4 to 5 days following vaginal births, 6 to 7 days following caesareans births |
| Brooten 1994 | 'earlier than usual' (mean stay of 3.6 days) plus minimum of 2 home visits post discharge, plus 10 phone calls to 8 weeks, plus women had phone number to nurse and physician |
'routine hospital practice' (mean stay of 4.8 days) no routine follow‐up care at home post discharge |
| Burnell 1982 | 48 hours after delivery (vaginal births only) plus postnatal care at home |
conventional hospital stay of 8 to 9 days |
| Carty 1990 | Group 1: 12 to 24 hours after delivery (vaginal births only) plus 5 home visits post discharge Group 2: 25 to 48 hours after delivery (vaginal births only) plus 3 home visits post discharge |
4 days after delivery (vaginal births only) plus 1 home visit post discharge |
| Chiong 2012 | 1 day after delivery (caesarean births only) | 2 days after delivery (caesarean births only) |
| Gagnon 1997 | 6 to 36 hours after delivery (vaginal births only) plus antenatal nursing care at home, at 34 to 38 weeks' gestation, postnatal nursing care by telephone, within 48 hours pp and at 10 days pp, and also at home at 3 and 5 days pp. |
48 to 72 hours after delivery (vaginal births only) plus follow‐up as determined by the woman's and infant's physicians. |
| Hellman 1962 | before 72 hours after delivery (vaginal births only) | 5 days after delivery (vaginal births only) |
| Kruse 2021 | at 28 hours after delivery (caesarean births only) | 48 hours or later after delivery (caesarean births only) |
| McKeever 2002 | 24 to 36 hours after delivery (vaginal births only) plus up to 3 home visits from community nurses qualified as lactation consultants. |
“standard length of hospitalisation” (vaginal births only) |
| Sainz Bueno 2005 | before 24 hours after delivery (vaginal births only) plus home visit by nurse during first 24 to 48 hours |
at least 48 hours after delivery (vaginal births only) |
| Smith‐Hanrahan 1995 | before 60 hours after delivery (vaginal births only) plus telephone call from nurse within 24 hours of discharge leading to a decision to visit or continue to consult by phone; also received phone number for postnatal follow‐up service which could be called at any time |
after 60 hours after delivery (vaginal births only) |
| Taiba 2012 | 72 hours after delivery (caesarean births only) | 7 days after delivery (caesarean births only) |
| Thompson 1999 | before 36 hours after delivery (vaginal births only) | 37‐72 hours after delivery (vaginal births only) |
| Waldenström 1987 | 24 to 48 hours after delivery (vaginal births only) | 6 days after delivery (vaginal births only) |
| Winterburn 2000 | 6 to 48 hours after delivery (vaginal and caesarean births) plus community midwife home visits to support breastfeeding |
between 48 hours and 7 days after delivery (vaginal and caesarean births) |
| Yanover 1976 | 12 to 48 hours after delivery (vaginal births only) | after 48 hours after delivery (vaginal births only) |
pp: postpartum
Definition of early discharge
The definition of 'early discharge' differed across the trials, reflecting standard practice in the settings in which they were conducted. Three trials defined early as 24 hours or less (Bayoumi 2016; Chiong 2012; Sainz Bueno 2005), one as 28 hours or less (Kruse 2021) and one as 36 hours or less (Thompson 1999). Five trials defined early discharge as a range: between six hours and 36 hours (Gagnon 1997); between six hours and 48 hours (Winterburn 2000); between 12 hours and 48 hours (Yanover 1976); between 24 and 36 hours (McKeever 2002); and between 24 and 48 hours (Waldenström 1987).
One trial defined early discharge as between 24 and 48 hours for vaginal birth and between 72 and 84 hours after caesarean section (Boulvain 2004).
One trial allocated women to two different early discharge groups; one for discharge at 12 to 24 hours and another for discharge at 25 to 48 hours (Carty 1990).
Five of the 17 trials defined early discharge as 48 hours or longer after giving birth (Brooten 1994; Burnell 1982; Hellman 1962; Smith‐Hanrahan 1995; Taiba 2012).
Definition of standard care
Most trials included in the review stated a standard postnatal length of stay at least 48 hours after birth (Bayoumi 2016; Boulvain 2004; Brooten 1994; Burnell 1982; Carty 1990; Chiong 2012; Gagnon 1997; Hellman 1962; Kruse 2021; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976). One study did not state the standard length of stay for the control group (McKeever 2002) and the final trial reported a standard care length of stay as between 37 hours and 48 hours after birth (Thompson 1999).
In several studies, the duration of hospital stay in the comparator group was equal to or shorter than the definition of early discharge in other studies. For instance, women in the comparator groups in four vaginal birth‐only studies (Gagnon 1997; Sainz Bueno 2005; Smith‐Hanrahan 1995; Thompson 1999) were allocated to hospital stays that were shorter than or equal to the early discharge period of up to 72 hours in one other vaginal birth‐only study (Hellman 1962). Similarly, in two caesarean‐only studies (Bayoumi 2016; Kruse 2021) early discharge was shorter than standard discharge of 72 hours in another caesarean‐only study (Taiba 2012).
Co‐interventions
The intensity of antenatal preparation and frequency of midwife home care following discharge offered to women in intervention and control groups differed considerably among trials. Two studies included antenatal home visits for women randomised to early discharge (Carty 1990; Waldenström 1987), and a third offered a prenatal 'preparation for discharge' class for women in both intervention and control arms of the study (Yanover 1976). Home visits by study nurses or nurse‐midwives were made to women in the early discharge arms of 13 trials, although in the largest trial (Hellman 1962) study nurses were intended to collect information only and were requested not to provide actual nursing care or support. There was substantial variation in the nature and extent of nurse‐midwife support specified in study protocols. Some trials offered a mixture of home visits and phone calls (Boulvain 2004; Gagnon 1997; Smith‐Hanrahan 1995) while others included a home visit during pregnancy as well as home visits after the birth (Carty 1990; Waldenström 1987). Six trials restricted midwife home visits to the early discharge group (Brooten 1994; Sainz Bueno 2005; Smith‐Hanrahan 1995; Waldenström 1987; Winterburn 2000; Yanover 1976). The other four trials provided a limited number of midwife home visits to women in the control group (Boulvain 2004; Carty 1990; Hellman 1962) or provided home visits on referral by a physician (Gagnon 1997). Two studies did not provide home visits to either arm, but participants could access the clinics and acute care facilities as required (Bayoumi 2016; Chiong 2012). None of the studies provide detailed information about access to primary care services in the settings in which the studies were conducted.
Outcomes
Thirteen trials reported our primary outcomes:
Infants readmitted for neonatal morbidity (Bayoumi 2016; Boulvain 2004; Brooten 1994; Chiong 2012; Hellman 1962; Kruse 2021; Sainz Bueno 2005; Smith‐Hanrahan 1995; Waldenström 1987; Yanover 1976).
Women readmitted for complications related to childbirth in the first six weeks after giving birth (Bayoumi 2016; Boulvain 2004; Carty 1990; Chiong 2012; Hellman 1962; Kruse 2021; Sainz Bueno 2005; Waldenström 1987; Yanover 1976).
Women scoring above the cut‐off score, indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after giving birth (Bayoumi 2016; Boulvain 2004; Chiong 2012; Sainz Bueno 2005; Waldenström 1987).
Women breastfeeding at six weeks, 12 weeks and six months after giving birth (Bayoumi 2016; Boulvain 2004; Carty 1990; Chiong 2012; Gagnon 1997; Hellman 1962; Sainz Bueno 2005; Waldenström 1987; Winterburn 2000).
The following outcomes were not reported by any of the studies.
Infants attending hospital casualty or emergency department within seven days, and the first 28 days after the birth.
Number of contacts with health professionals regarding infant health issues within seven days after the birth.
Maternal mortality within six weeks.
Duration of readmissions for women readmitted within the first six weeks after the birth.
Total duration of maternal hospitalisation over the first six weeks after the birth.
Women attending hospital casualty or emergency department within the first six weeks after the birth.
Funding sources
Ten trials reported that their funding was from government, university or hospital sources (Boulvain 2004; Brooten 1994; Chiong 2012; Gagnon 1997; Hellman 1962; McKeever 2002; Smith‐Hanrahan 1995; Waldenström 1987; Winterburn 2000; Yanover 1976).
Five trials did not report any information about their funding sources (Bayoumi 2016; Burnell 1982; Carty 1990; Sainz Bueno 2005; Taiba 2012).
Two trials reported funding from other sources: Brodene Hartmanns Foundation (Kruse 2021); the Salaried Specialists (Thompson 1999).
Declarations of interest
Fourteen trials did not report any information about the authors' declarations of interest (Boulvain 2004; Brooten 1994; Burnell 1982; Carty 1990; Gagnon 1997; Hellman 1962; McKeever 2002; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Thompson 1999; Waldenström 1987; Winterburn 2000; Yanover 1976).
Three trials explicitly stated that the authors had no conflicts of interest or had nothing to declare (Bayoumi 2016; Chiong 2012; Kruse 2021).
No trials reported any conflicts of interest.
Missing data
Six trials reported the numbers of women excluded from analysis because they no longer met either the trial eligibility criteria or the criteria for early discharge. The proportion of women excluded for this reason ranged from 0.22% (Boulvain 2004) to 44% (Gagnon 1997). The number of women excluded for this reason was generally balanced between the treatment groups in the trials, with the exception of one trial (Thompson 1999) where 13/24 and 5/24 women were excluded because they no longer fulfilled the early discharge criteria. Eight trials did not report whether any women were excluded because they no longer met either the trial eligibility criteria or the criteria for early discharge (Bayoumi 2016; Brooten 1994; Burnell 1982; Carty 1990; Hellman 1962; Sainz Bueno 2005; Taiba 2012; Yanover 1976). Three trials reported that no women were excluded for no longer meeting either the trial eligibility criteria or the criteria for early discharge (Kruse 2021; McKeever 2002; Winterburn 2000).
All but four trials (Brooten 1994; Burnell 1982; Hellman 1962; Taiba 2012) reported the number of women who did not adhere to the treatment group to which they were allocated, i.e. the number of women who either stayed beyond the early discharge time or who were discharged before the standard discharge time. The proportion of women not adhering to the treatment group ranged from zero (McKeever 2002; Yanover 1976) to 61% (Boulvain 2004). The number of women not adhering to the treatment group was generally balanced between the treatment groups in the trials, except in one trial (Winterburn 2000), where 90/121 and 20/127 women either stayed for a longer or a shorter time than the treatment to which they were allocated. Six trials reported that the women who did not adhere to their treatment group were included in the final analysis according to their allocated group (Boulvain 2004; Chiong 2012; Gagnon 1997; Kruse 2021; Sainz Bueno 2005; Winterburn 2000). One trial (Waldenström 1987) analysed all women in the control group according their allocated group, regardless of whether or not they adhered to it; but this trial analysed the women in the early discharge on a per‐protocol basis, i.e. those who did not adhere were not included in the analysis.
Nine trials had a high level of missing data, where 20% or more the women who were randomised were not included in the final analysis (Bayoumi 2016; Carty 1990; Gagnon 1997; McKeever 2002; Smith‐Hanrahan 1995; Taiba 2012; Thompson 1999; Waldenström 1987; Yanover 1976). Five trials had no missing data (Brooten 1994; Burnell 1982; Hellman 1962; Kruse 2021; Sainz Bueno 2005), although one of these did not report the number of women who were originally randomised; therefore, it is not clear if any data were missing from the final analysis (Brooten 1994).
Excluded studies
We excluded three trials because they were not designed to measure the effect of early discharge compared with longer length of hospital stay (see Characteristics of excluded studies).
Risk of bias in included studies
The summary risk of bias across all studies for each domain is presented in Figure 2. Risk of bias per domain, per study is presented in Figure 3.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
See Characteristics of included studies for full details.
Allocation
Random sequence generation
Random sequence generation was detailed in six of the trials in sufficient detail to be judged at low risk of bias (Boulvain 2004; Brooten 1994; Carty 1990; Chiong 2012; Gagnon 1997; Kruse 2021; McKeever 2002; Thompson 1999). Random sequence generation was not clear in eight of the trials (Bayoumi 2016; Burnell 1982; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976). We judged one trial as high risk of bias because it did not use any randomisation process to allocate women to the intervention group, while the control group allocation was done in a randomised fashion that was not described in detail (Hellman 1962).
Allocation concealment
We judged nine trials as low risk of bias because methods to ensure allocation concealment were clearly documented (Bayoumi 2016; Boulvain 2004; Brooten 1994; Carty 1990; Chiong 2012; Gagnon 1997; Kruse 2021; Sainz Bueno 2005; Thompson 1999). There was insufficient information available to determine the adequacy of concealment prior to randomisation for the other eight trials so we judged them as unclear risk of bias (Burnell 1982; Hellman 1962; McKeever 2002; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976).
Blinding
Blinding of participants and caregivers
It was not possible to blind participants or caregivers to allocation status for this intervention. However, studies were judged at low risk of bias if the main outcomes were unlikely to be affected by lack of blinding (for example, readmission rates to hospital) and high risk if the main outcomes were likely to be affected by the lack of participant blinding (for example, participant satisfaction). Fifteen studies were considered to be at low risk of performance bias (Bayoumi 2016; Boulvain 2004; Brooten 1994; Carty 1990; Chiong 2012; Gagnon 1997; Hellman 1962; Kruse 2021; McKeever 2002; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976) and a further two studies were judged at high risk of performance bias due to lack of participant blinding (Burnell 1982; Thompson 1999).
Blinding of outcome assessors
We judged three studies as low risk of detection bias because clear methods to blind the outcome assessment to participant allocation were described (Bayoumi 2016; McKeever 2002; Thompson 1999). It was unclear whether outcome assessment was blinded to allocation status in a further 13 studies (Boulvain 2004; Brooten 1994; Burnell 1982; Carty 1990; Chiong 2012; Gagnon 1997; Hellman 1962; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976). We judged one study as high risk of detection bias because the outcome assessors were not blinded to participant allocation (Kruse 2021).
Incomplete outcome data
Low attrition rates, which were balanced across both arms of the trial, were described in seven of the studies and we judged them to be at low risk of bias (Bayoumi 2016; Boulvain 2004; Chiong 2012; Kruse 2021; Smith‐Hanrahan 1995; Thompson 1999; Winterburn 2000). Levels of attrition and how missing data were accounted for was not clear in five trials and we judged these as unclear risk of bias (Brooten 1994; Burnell 1982; Hellman 1962; Sainz Bueno 2005; Yanover 1976) The remaining six trials we judged at high risk of attrition bias either due to differential attrition rates between the early discharge group and standard care group (Carty 1990; Gagnon 1997; McKeever 2002; Taiba 2012; Waldenström 1987) or high attrition rates in the trial overall (Smith‐Hanrahan 1995).
Selective reporting
None of the studies had published protocols, although the majority of included studies were published at a time when this was not a requirement. We judged these studies as unclear risk of reporting bias (Bayoumi 2016; Boulvain 2004; Brooten 1994; Carty 1990; Chiong 2012; Gagnon 1997; Hellman 1962; Sainz Bueno 2005; Smith‐Hanrahan 1995; Taiba 2012; Waldenström 1987; Winterburn 2000; Yanover 1976). Two of the trials did not report outcomes that were specified in the methods section and we judged these to be at high risk of reporting bias (Burnell 1982; McKeever 2002; Thompson 1999). Kruse 2021 and colleagues did not publish a protocol but the trial was registered prospectively and not all pre‐specified outcomes were reported in full; however, correspondence with the trial author confirmed that the outcomes were measured and the data analysis is in progress. We judged this trial to be at low risk of reporting bias.
Other potential sources of bias
All 17 studies included in the review appeared to be at low risk of any other sources of bias.
Effects of interventions
See: Table 1
Primary infant outcomes
Infants readmitted for neonatal morbidity (including jaundice, dehydration, infections) within seven days
We are uncertain if early discharge, compared with standard discharge, has any effect on the risk of infant readmission within seven days (RR 1.15, 95% CI 0.42 to 3.16; 247 participants; two studies; I2 = 0%; Analysis 1.1).
1.1. Analysis.

Comparison 1: Early versus standard discharge, Outcome 1: Infants readmitted for neonatal morbidity within 7 days
Infants readmitted for neonatal morbidity (including jaundice, dehydration, infections) within 28 days
Early discharge probably slightly increases the number of infants readmitted within 28 days compared to infants in the standard care group (RR 1.59, 95% CI 1.27 to 1.98; 6918 participants; 10 studies; I2 = 12%; Analysis 1.2; moderate‐certainty evidence; Table 1). The risk of infant readmission in the early discharge group was 69 per 1000 infants compared to 43 per 1000 infants in the standard care group.
1.2. Analysis.

Comparison 1: Early versus standard discharge, Outcome 2: Infants readmitted for neonatal morbidity within 28 days
The tests for subgroup differences did not suggest evidence of a difference in effect between different decades when the trials took place (P = 0.24, I2 = 26.3%), different modes of birth (P = 0.65, I2 = 0%; Analysis 1.3) or the varying definitions of early discharge (P = 0.55, I2 = 0%; Analysis 1.4).
1.3. Analysis.

Comparison 1: Early versus standard discharge, Outcome 3: Infants readmitted for neonatal morbidity within 28 days: mode of birth subgroups
1.4. Analysis.

Comparison 1: Early versus standard discharge, Outcome 4: Infants readmitted for neonatal morbidity within 28 days: subgroups < 24h vs > 24h
The sensitivity analysis, removing two trials at high risk of bias in the random sequence generation and differential attrition domains (Hellman 1962; Waldenström 1987), did not change the effect estimate substantially (RR 1.58, 95% CI 1.26 to 1.99; 4663 participants; I2 = 33%).
A second sensitivity analysis, removing trials with a high level of missing data (defined as 20% or more of the infants of women randomised were not included in the analysis), suggests that it is uncertain whether early discharge, compared with standard discharge, has any effect on the risk of infant readmission within 28 days (RR 1.10, 95% CI 0.67 to 1.81; 3647 participants; I2 = 16%). Four trials were removed in order to conduct this sensitivity analysis (Bayoumi 2016; Smith‐Hanrahan 1995; Waldenström 1987; Yanover 1976).
Primary maternal outcomes
Women readmitted for complications related to childbirth (including postpartum haemorrhage, retained products of conception, infection, postpartum psychosis) within six weeks postpartum
Early discharge probably results in little to no difference in women readmitted within six weeks but the 95% CI suggests that the true effect may be either an increase or decrease in risk (RR 1.12, 95% CI 0.82 to 1.54; 6992 participants; 11 studies; I2 = 0%; moderate‐certainty evidence; Analysis 1.5; Table 1).
1.5. Analysis.

Comparison 1: Early versus standard discharge, Outcome 5: Women readmitted within six weeks
The tests for subgroup differences did not suggest evidence of a difference in effect between different decades when the trials took place (P = 0.25, I2 = 25.4%), mode of birth (P = 0.69; I2 = 0%; Analysis 1.6) or definition of early discharge (P = 0.66; I2 = 0%; Analysis 1.7).
1.6. Analysis.

Comparison 1: Early versus standard discharge, Outcome 6: Women readmitted within six weeks: mode of birth subgroups
1.7. Analysis.

Comparison 1: Early versus standard discharge, Outcome 7: Women readmitted within six weeks: subgroups < 24 hours vs > 24hrs
Sensitivity analysis removing three trials at high risk of bias in the random sequence generation, allocation concealment or differential attrition domains (Carty 1990; Hellman 1962; Waldenström 1987), did not change the effect estimate substantially (RR 1.07, 95% CI 0.77 to 1.48; 4663 participants; I2 = 0%).
A second sensitivity analysis, removing three trials with a high level of missing data (defined as 20% or more of the women randomised were not included in the analysis) (Bayoumi 2016; Carty 1990; Waldenström 1987) made the effect estimate more imprecise, with a substantially wider 95% CI (RR 1.28, 95% CI 0.69 to 2.40; 3590 participants; I2 = 0%).
Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression within six months after the birth
Early discharge may result in little to no difference in the risk of depression within six months but the wide 95% CI suggests the possibility that the true effect is either an increase or a reduction in risk (RR 0.80, 95% CI 0.46 to 1.42; 4333 participants; five studies; I2 = 58%; Analysis 1.8; low‐certainty evidence; Table 1).
1.8. Analysis.

Comparison 1: Early versus standard discharge, Outcome 8: Women probably depressed within six months
The tests for subgroup differences did not suggest evidence of a difference in effect between different decades when the trials took place (P = 0.46, I2 = 0%), different modes of birth (P = 0.41, I2 = 0%; Analysis 1.9) or time of early discharge (P = 0.79, I² = 0%, Analysis 1.10).
1.9. Analysis.

Comparison 1: Early versus standard discharge, Outcome 9: Women probably depressed within six months: mode of birth subgroups
1.10. Analysis.

Comparison 1: Early versus standard discharge, Outcome 10: Women probably depressed within six months: subgroups < 24 h vs < 24 hrs
Sensitivity analysis removing one trial at high risk of bias in the differential attrition domain (Waldenström 1987) did not change the effect estimate substantially (RR 0.81, 95% CI 0.43 to 1.53).
A second sensitivity analysis removing trials with a high level of missing data, where 20% or more of the women randomised were not included in the analysis (Bayoumi 2016; Waldenström 1987), did not change the effect estimate substantially (RR 0.62, 95% CI 0.34 to 1.12).
Additionally, one study reported mean scores on the Beck Depression Inventory at one month postpartum favouring early discharge (Carty 1990). The mean score for women randomised to discharge within 24 hours of the birth was 4.5 (standard deviation (SD) 2.54) versus a mean score of 7.8 (SD 6.46) for women randomised to discharge four or more days after the birth (P < 0.05). Higher scores on this scale indicate poorer emotional well‐being. It was not possible to include these data in the meta‐analysis because there was insufficient data provided in the paper.
Women breastfeeding (exclusively or partially) at six weeks after giving birth
Early discharge probably results in little to no difference in women breastfeeding at six weeks after giving birth (RR 1.04, 95% CI 0.96 to 1.13; 7156 participants; 10 studies; I2 = 79%; Analysis 1.11; moderate‐certainty evidence; Table 1).
1.11. Analysis.

Comparison 1: Early versus standard discharge, Outcome 11: Women breastfeeding (exclusively or partially) at six weeks postpartum
The test for subgroup differences suggested a difference in effect between trials taking place in different decades (P = 0.004, I2 = 73.8%). This difference appears to be due to one trial that took place in the early 1960s where more women in the early discharge group were breastfeeding at six weeks compared to women in the standard discharge group, while the trials taking place in the decades since the 1960s did not observe a clear difference between groups.
The tests for subgroup differences did not suggest evidence of a difference in effect between different modes of birth (P = 0.61, I2 = 0%, Analysis 1.12) or time of early discharge did not indicate evidence of a difference in effect between groups (P = 0.74, I2 = 0%, overlapping CIs; Analysis 1.13).
1.12. Analysis.

Comparison 1: Early versus standard discharge, Outcome 12: Women breastfeeding (exclusively or partially) at six weeks postpartum: mode of birth subgroups
1.13. Analysis.

Comparison 1: Early versus standard discharge, Outcome 13: Women breastfeeding (exclusively or partially) at six weeks postpartum: subgroups < 24hr vs > 24 hrs
The symmetry of the funnel plot (Figure 4) did not suggest evidence of data missing due to non‐publication of studies with statistically insignificant findings.
4.

Funnel plot of comparison: 1 Early versus standard discharge, outcome: 1.13 Women breastfeeding (exclusively or partially) at six weeks postpartum.
Sensitivity analysis removing four trials at high risk of bias in the random sequence generation, allocation concealment or differential attrition domains (Carty 1990; Chiong 2012; Hellman 1962; Waldenström 1987) did not substantially change the effect estimate (RR 1.01, 95% CI 0.92 to 1.09).
A second sensitivity analysis removing five trials with a high level of missing data (defined as 20% or more of the women randomised were not included in the analysis) (Bayoumi 2016; Carty 1990; Gagnon 1997; Smith‐Hanrahan 1995; Waldenström 1987), did not change the effect estimate substantially (RR 1.09, 95% CI 0.98 to 1.21).
Women breastfeeding (exclusively or partially) 12 weeks after giving birth
One study measured the number of women breastfeeding at 12 weeks after giving birth and found more women in the early discharge group were breastfeeding (RR 1.21, 95% CI 1.03 to 1.41; 430 participants; Analysis 1.14).
1.14. Analysis.

Comparison 1: Early versus standard discharge, Outcome 14: Women breastfeeding (exclusively or partially) at 12 weeks postpartum
Women breastfeeding (exclusively or partially) at six months after giving birth
There may be little to no difference between early discharge and later discharge in the number of women breastfeeding at six months (RR 1.12, 95% CI 0.94 to 1.32; 973 participants; three studies; I2 = 52%; Analysis 1.15). To investigate the moderate level of heterogeneity in the analysis we performed the analysis again with random‐effects and the effect estimate did not change substantially (RR 1.11, 95% CI 0.87 to 1.43).
1.15. Analysis.

Comparison 1: Early versus standard discharge, Outcome 15: Women breastfeeding (partially or exclusively) at six months postpartum
Secondary infant outcomes
Infant mortality within 28 days
It is uncertain whether early discharge, compared with standard discharge, has any effect on the risk of infant mortality within 28 days (RR 0.39, 95% CI 0.04 to 3.74; 4882 participants; two studies; I2 = 0%; Analysis 1.16).
1.16. Analysis.

Comparison 1: Early versus standard discharge, Outcome 16: Infant mortality within 28 days
Infant mortality within one year
It is uncertain whether early discharge, compared with standard discharge, has any effect on the risk of infant mortality within one year because the certainty of evidence is low and 95% CI is consistent with possible benefit and possible harm (RR 0.45, 95% CI 0.07 to 2.77; 4984 participants; three studies; I2 = 0%; Analysis 1.17; low‐certainty evidence; Table 1).
1.17. Analysis.

Comparison 1: Early versus standard discharge, Outcome 17: Infant mortality within one year
Subgroup analysis on the basis of mode of birth was not possible because there was only trial in the caesarean birth group and it had zero events in both arms. For the same reason we could not perform subgroup analysis with regard to time of early discharge.
Sensitivity analysis removing one trial at high risk of bias due to random sequence generation (Hellman 1962) did not change the effect estimate substantially but made the CI wider (RR 0.36, 95% CI 0.02 to 8.63). Similarly, sensitivity analysis removing one trial with high levels of missing data (Waldenström 1987) did not change the effect estimate substantially but made the CI wider (RR 0.52, 95% CI 0.06 to 4.64).
Duration of infant readmissions for infants readmitted within seven days after the birth
One study reported that the single infant in the study that was readmitted within seven days stayed in hospital for two days (Waldenström 1987). The infant was in the early discharge group (n = 50). No infants in the later discharge group were readmitted (n = 54).
No other studies reported duration of infant readmissions in the first seven days.
Duration of infant readmissions for infants readmitted within the first 28 days after the birth
One study reported that 1/50 and 1/54 infants each spent two days in hospital in the first 28 days (Waldenström 1987).
No other studies reported duration of infant readmissions in the first 28 days.
Total duration of infant hospitalisation over the first 28 days
One study reported total duration of infant hospitalisation over the first 28 days. However it only reported the mean number of days for the control group (two days). No data were reported for mean duration of infant hospitalisation for the early discharge group (Waldenström 1987).
Infants attending hospital casualty or emergency department within seven days, and the first 28 days after the birth
Not reported.
Number of contacts with health professionals regarding infant health issues within seven days after the birth
Not reported.
Number of contacts with health professionals regarding infant health issues within the first four weeks after the birth
Early postnatal discharge, compared with later discharge, probably makes little to no difference in the number of infants having at least one unscheduled medical consultation or contact with health professionals within the first four weeks after birth (RR 0.88, 95% CI 0.67 to 1.16; 639 participants; three studies; I2 = 0%; Analysis 1.18; moderate‐certainty evidence; Table 1) (Brooten 1994; Chiong 2012; Gagnon 1997).
1.18. Analysis.

Comparison 1: Early versus standard discharge, Outcome 18: Number of contacts with healthcare professionals regarding infant health issues within four weeks of birth
Two other studies reported data that could not be included in the meta‐analysis (Kruse 2021; Waldenström 1987). The results indicated little to no difference between the groups in terms of number of contacts with health professionals regarding infant health issues (Table 3).
2. Number of contacts with health professionals regarding infant health issues.
| Trial | Early discharge | Laterdischarge | Notes |
| Kruse 2021 | Median (range): 3 (0‐10) 54 women |
Median (range): 3 (0‐9) 52 women |
Contacts regarding infant and maternal health issues were counted together. |
| Waldenström 1987 | 452 contacts (49 infants) | 537 contacts (50 infants) | 6 month follow‐up. Number of contacts with child health centre (home visits by CHC nurse, visits to CHC nurse, visits to CHC paediatrician) |
Secondary maternal outcomes
Maternal mortality within six weeks postpartum
Not reported.
Maternal mortality within one year postpartum
Two studies reported maternal mortality within one year (Bayoumi 2016; Taiba 2012). Of 1545 women allocated to early discharge and 1653 women allocated to standard discharge, there were no maternal deaths within one year.
Duration of readmissions for women readmitted within the first six weeks after the birth
Not reported.
Total duration of maternal hospitalisation over the first six weeks after the birth
Not reported.
Women attending hospital casualty or emergency department within first six weeks after the birth
Not reported.
Number of contacts with health professionals regarding maternal health issues within the first six weeks after the birth
Two studies reported the number of women having at least one unscheduled medical consultation or contact with health professional (Brooten 1994; Chiong 2012), with both studies including women following caesarean section. There is probably little to no difference in the number of women who have at least one unscheduled medical consultation after having been discharged early, compared with later discharge (RR 0.72, 95% CI 0.43 to 1.20; 464 participants; two studies; I2 = 29%; Analysis 1.19; moderate‐certainty evidence; Table 1).
1.19. Analysis.

Comparison 1: Early versus standard discharge, Outcome 19: Number of contacts with healthcare professionals regarding maternal health issues within six weeks of birth
Two other studies reported data suggesting little difference between the groups in terms of contact with health professionals for maternal health issues but they were not suitable for inclusion in the meta‐analysis (Boulvain 2004; Kruse 2021; see Table 4).
3. Number of contacts with health professionals regarding maternal health issues.
| Trial | Early discharge | Laterdischarge | Notes |
| Kruse 2021 | Median (range): 3 (0‐10) 54 women |
Median (range): 3 (0‐9) 52 women |
Contacts regarding infant and maternal health issues were counted together. |
| Boulvain 2004 | 33/228 | 48/231 | Number of women reporting 1 or more visits to a gynaecologist during the first month. |
Women reporting tiredness or exhaustion in the first six weeks after the birth
Three trials reported measures of tiredness and exhaustion in the first six weeks after the birth but they reported no data that were suitable for pooled analysis. Waldenström and colleagues compared mean values on a five‐point scale that rated fatigue and alertness from 'very alert' to 'very tired' for the first 14 days postpartum. No evidence of a difference was found between groups, but women in both groups were most tired on the day following discharge (Waldenström 1987). Smith‐Hanrahan and colleagues used a 10 centimetre visual analogue scale with anchors ranging from zero (not tired, full of energy, peppy) to 10 (total exhaustion) with assessments at two to three days, one week and six weeks after the birth. No significant differences in mean scores were found between intervention and control groups (Smith‐Hanrahan 1995). Sainz Bueno and colleagues report the increase in puerperal fatigue at one month compared with one week postpartum and found no differences between groups (Sainz Bueno 2005).
Women reporting physical health problems (including perineal pain, perineal infection, breast soreness, breast infection, caesarean wound pain, caesarean wound infection) in the first six weeks after the birth
In one trial fewer women in the early discharge group reported physical health problems in the first six weeks after giving birth compared with the standard discharge group (RR 0.25, 95% CI 0.11 to 0.59; 200 participants; one study; Analysis 1.20; Taiba 2012).
1.20. Analysis.

Comparison 1: Early versus standard discharge, Outcome 20: Women reporting health problems (including perineal pain, perineal infection, breast soreness, breast infection, caesarean wound pain, caesarean wound infection) in the first six weeks postpartum
Women reporting that they lacked confidence about caring for their baby in the first month and the first six months after being discharged from hospital
Not reported.
Women reporting infant feeding problems in the first four weeks after the birth
Two trials reported data on infant feeding problems (Boulvain 2004; Hellman 1962). We are uncertain whether there is any difference between early discharge and standard care for women reporting infant feeding problems in the first four weeks after the birth (RR 0.89, 95% CI 0.43 to 1.86; 2405 participants; two studies; I2 = 88%; Analysis 1.21). Random effects analysis was used to combine trials, due to substantial heterogeneity, which may be due to different modes of births in different trial populations. The estimate of fixed‐effect analysis was not substantially different: RR 0.87, 95% CI 0.68 to 1.11).
1.21. Analysis.

Comparison 1: Early versus standard discharge, Outcome 21: Women reporting infant feeding problems
Women reporting they received conflicting advice regarding breastfeeding in the first six weeks after birth
Not reported.
Women who express satisfaction with their postnatal care (including in hospital and/or post‐discharge care)
Six trials used various methods to measure women's satisfaction with postnatal care in hospital (Boulvain 2004; Carty 1990; Gagnon 1997; Hellman 1962; Sainz Bueno 2005; Waldenström 1987). Four studies used dichotomous measures (Boulvain 2004; Hellman 1962; Sainz Bueno 2005; Waldenström 1987) and two used numerical scales (Carty 1990; Gagnon 1997).
There may be little to no difference in number of women satisfied between women who were discharged early and women discharged according to standard protocol (RR 1.10, 95% CI 0.95 to 1.29; 3098 participants; four studies; I2 = 93%; Analysis 1.22).
1.22. Analysis.

Comparison 1: Early versus standard discharge, Outcome 22: Women satisfied with postnatal care ‐ dichotomous data
The high I2 statistic may be due to variations in the trials' definition of early discharge and/or standard discharge. The early discharge groups ranged from discharge within 24 hours (Sainz Bueno 2005), between 24 and 48 hours (Boulvain 2004; Waldenström 1987), to up to 72 hours (Hellman 1962). In all of the studies standard discharge was considerably later than early discharge; two to three days later (Boulvain 2004), one day later (Sainz Bueno 2005), at least two days later (Hellman 1962), four to five days later (Waldenström 1987).
One study (Carty 1990) measured women's satisfaction with nursing care using a questionnaire with a maximum score of 110 (higher score = greater satisfaction). Another study (Gagnon 1997) used a 5‐point Likert scale to measure women's satisfaction with health care in first day 10 days postpartum (higher score = greater satisfaction). Combining these studies using standardized mean difference indicated substantially greater satisfaction with early discharge compared with standard discharge (SMD 0.74, 95% CI 0.50 to 0.98; 306 participants; two studies; I2 = 0%; Analysis 1.23).
1.23. Analysis.

Comparison 1: Early versus standard discharge, Outcome 23: Satisfaction with postnatal care ‐ continuous data
No trials included measures specifically focusing on women's views of postnatal care after they left hospital.
Women who perceive their length of hospital stay as too short
Only one trial reported on the proportion of women who perceived their length of hospital as too short (Yanover 1976). Very few women in the trial conducted by Yanover and colleagues thought their length of stay too short (2/41 in the early discharge group and 1/41 in the group randomised to standard care (RR 2.00, 95% CI 0.19 to 21.21; 82 participants; Analysis 1.24).
1.24. Analysis.

Comparison 1: Early versus standard discharge, Outcome 24: Women who perceive their length of hospital stay as too short
Women who perceive their length of hospital stay as too long
Two trials reported on the proportion of women who perceived their length of stay as too long. Yanover and colleagues found slightly fewer women in the early discharge group that thought their stay was 'too long' (5/41 in the early discharge group versus 9/41 in the standard care group (RR 0.56, 95% CI 0.20 to 1.52; 82 participants; Analysis 1.25). One study (Sainz Bueno 2005) only reported the proportion of women who perceived their length of stay as too long in the control group (54/125) but no data were reported for the intervention group.
1.25. Analysis.

Comparison 1: Early versus standard discharge, Outcome 25: Women perceive their length of hospital stay as too long
Partner outcomes
None of the trials reported any of our pre‐specified partner outcomes. One trial measured outcomes related to fathers' involvement in infant care but it did not report any data that we could use for analysis (Waldenström 1987). They found that fathers' involvement was higher in the first few days after the birth in the early discharge group, both among first‐time fathers and those having their second or a subsequent child. First‐time fathers in the early discharge group spent an average of 183 minutes per day with their baby in the first two to four days, compared with 71 minutes for the control group (student's t test = 4.5, P < 0.001). Fathers with two or more children spent an average of 89 minutes with the new baby in the early discharge group, compared with 44 minutes in the control group (t = 2.9, P < 0.01). These differences were no longer apparent at two weeks and six weeks after the birth.
Economic outcomes
Costs of hospital care in the period immediately following the birth up to the time of discharge
Three trials reported mean costs of hospitalisation (see Table 5; Boulvain 2004; Brooten 1994; Sainz Bueno 2005). Early discharge may slightly reduce the costs of hospital care in the period immediately following the birth up to the time of discharge (low‐certainty evidence; Table 1).
4. Costs of hospital care in the period immediately following the birth up to the time of discharge.
| Trial | Early discharge | Later discharge | Difference |
| Boulvain 2004 | CHF 5218 228 women |
CHF 6772 231 women |
CHF ‐1554 |
| Brooten 1994 | USD 7648 61 women |
USD 10,971 61 women |
USD ‐3323 |
| Sainz Bueno 2005 | USD 382.22 213 women |
USD 647.67 217 women |
USD ‐265.45 |
CHF: Swiss francs USD: USA dollars
Costs of postnatal care following discharge from hospital in the period up to six weeks after the birth, including community midwife, lactation consultant, general practice, specialist and outpatient visits; readmissions to hospital; attendances at day‐stay programs; in‐patient stays in mother and baby units
Three trials reported data on costs of postnatal care (see Table 6; Boulvain 2004; Brooten 1994; Sainz Bueno 2005). Early discharge may result in little to no difference in costs of postnatal care following discharge from hospital in the six weeks after the birth (low‐certainty evidence; Table 1).
5. Costs of postnatal care following discharge from hospital in the period up to six weeks after the birth.
| Trial | Type of cost | Early discharge | Later discharge | Difference |
| Boulvain 2004 | mean cost of all postnatal care | CHF 932 228 women |
CHF 481 231 women |
CHF 451 |
| Boulvain 2004 | mean cost of community care (including midwifery, medical and allied health care) | CHF 528 (SD 267) 228 women |
CHF 234 (SD 273) 231 women |
CHF 294 |
| Boulvain 2004 | total mean (SD) costs including:
|
CHF 7798 (SD 6419) 228 women |
CHF 9019 (SD 4345) 231 women |
CHF ‐1221 |
| Brooten 1994 | mean cost of nurse‐specialist visits (in hospital and at home), home caregiver charges, acute care visits (following discharge) and rehospitalisation charges | USD 516 61 women |
USD 519 61 women |
USD ‐3 |
| Brooten 1994 | total mean costs including
|
USD 8164 | USD 11,490 | USD ‐3326 |
| Sainz Bueno 2005 | combined cost of community care (including maternal and neonatal consultations and telephone calls) and maternal and neonatal readmissions | USD 125.24 213 women |
USD 153.90 217 women |
USD ‐28.66 |
CHF: Swiss francs USD: USA dollars SD: standard deviation
One trial reported that early discharge was associated with a higher mean cost of all postnatal care and a higher mean cost of community care but that the overall mean cost of all care, including hospitalisation, was lower with early discharge than later discharge (Boulvain 2004). The same trial also measured non‐medical costs attributable to health care in the first six weeks after birth (travel to healthcare providers, childcare support for siblings) and also the costs associated with loss of income if a partner required time off work. They found no differences between the groups in these non‐medical and indirect costs.
Costs of practical support following discharge from hospital in the period up to six weeks after the birth, including paid and unpaid home help, care of the baby and of siblings
Not reported.
Discussion
Summary of main results
The 17 trials we identified, with 9409 randomised women, help to consolidate the evidence base on the safety of early postnatal discharge for women and infants.
Infant outcomes
Early discharge of healthy mothers and term infants probably slightly increases the number of infants readmitted within 28 days for neonatal morbidity (moderate‐certainty evidence). It is uncertain whether early discharge has any effect on the risk of infant mortality within 28 days (low‐certainty evidence). Early postnatal discharge probably makes little to no difference in the number of infants having at least one unscheduled medical consultation or contact with health professionals within the first four weeks after birth.
Maternal outcomes
Early discharge probably results in little to no difference in women readmitted within six weeks postpartum for complications related to childbirth (moderate‐certainty evidence) but the wide 95% CI indicates the possibility that the true effect is either an increase or decrease in risk. Similarly, early discharge may result in little to no difference in the risk of depression within six months postpartum (low‐certainty evidence) but the wide 95% CI suggests the possibility that the true effect is either an increase or a reduction in risk.
Early discharge probably results in little to no difference in women breastfeeding at six weeks postpartum (moderate‐certainty evidence) or in the number of women having at least one unscheduled medical consultation or contact with health professionals (moderate‐certainty evidence).
Maternal mortality within six weeks postpartum was not reported in any of the studies.
Costs
Early discharge may slightly reduce the costs of hospital care in the period immediately following the birth up to the time of discharge (low‐certainty evidence) but it may result in little to no difference in costs of postnatal care following discharge from hospital in the period up to six weeks after the birth (low‐certainty evidence).
Overall completeness and applicability of evidence
We identified evidence for all but one of our pre‐specified GRADE outcomes; none of the studies reported maternal mortality within six weeks postpartum. It is not clear if this is because the outcome was not measured or if there were no deaths and the trialists simply have not reported such a rare outcome in the settings where the trials were conducted.
Several of our pre‐specified secondary outcomes were not reported at all, and there is a notable absence of evidence relating to partner outcomes. Furthermore, it is difficult to draw conclusions and generalise from the limited costs data that we identified.
The definition of early discharge differed considerably between trials and mirrored the differences in standard discharge policies in each context. In most of the trials included in this review, early discharge was accompanied by some level of post‐discharge nursing or midwifery support. In practice, policies promoting shorter length of stay may not always be implemented with accompanying primary care support in the days following discharge. It remains unclear how important home midwifery or nursing support is to the safety and acceptability of early discharge programs.
Quality of the evidence
We assessed the risk of bias in terms of random sequence generation to be generally low or unclear. Risk of bias related to blinding of participants was generally low because we judged that lack of blinding would be unlikely to affect the outcomes measured. In contrast, risk of bias related to outcome assessment was unclear because most trials did not report whether or not outcome assessors were blinded. Risk of bias related to missing data was high in several trials due to differential attrition, low in others because they reported data in full or did not have differential attrition, and unclear in several studies due to insufficient information. Overall, we judged the risk of selective reporting bias to be unclear because the majority of the studies were published before protocol publication became common practice.
The certainty of evidence was downgraded because of risk of bias in one outcome. For other outcomes, we downgraded the certainty of evidence due to imprecision, where there were few events, or the 95% CI was consistent with possible benefit and possible harm. We also downgraded the evidence in some places where there was heterogeneity in the direction and size of effect. Finally, we downgraded the evidence relating to costs of care because we deemed it to be imprecise, due to the lack of pooled data and effect estimates.
Potential biases in the review process
We made every attempt to reduce bias in the review process by conducting a comprehensive literature search without restrictions in terms of language or publication status. We also ensured that we did double independent screening of search results, data extraction, risk of bias assessment and GRADE assessment, in order to reduce bias. We contacted trial authors to seek clarification and/or obtain missing data where necessary.
In this updated review, we identified outcomes for the 'Summary of findings' tables. Two review authors were already aware of some of the trials that were included in the previously published version of the review, and this could have had an impact on the outcomes selected, resulting in a potential source of bias in this current update of the review.
Agreements and disagreements with other studies or reviews
The two other reviews that provide a quantitative synthesis on the effects of early postnatal discharge could neither confirm nor rule out the link between early discharge and neonatal and maternal morbidity and readmissions to hospital (Benahmed 2017; CETS 1997). Whilst this review found similar results for maternal readmissions within six weeks after giving birth, we found that early discharge probably slightly increases the number of infants readmitted within 28 days for neonatal morbidity. Other outcomes including maternal and infant health contacts, breastfeeding, and depression within six months align with findings from existing reviews, which conclude little to no difference between early discharge and standard length of stay. For the outcomes related to cost, we found that early discharge may slightly reduce the costs of hospital care in the period immediately following the birth up to the time of discharge (low‐certainty evidence) but it may result in little to no difference in costs of postnatal care following discharge from hospital in the period up to six weeks after the birth (low‐certainty evidence). This is a similar finding to the Conseil d'évaluation des technologies de la santé du Québec (CETS) review, which found that there are potential savings through early discharge only if there are no maternal or neonatal complications (CETS 1997).
Observational studies have mainly focused on the association between early discharge and infant morbidity and readmission to hospital. Our findings that early discharge probably slightly increases the number of infants readmitted within 28 days corresponds with a recent population based study by Lain and colleagues, which found that infants discharged from hospital in the first two days after birth were more likely to be readmitted for jaundice than infants who had a postnatal length of stay of three days or more (Lain 2015); although a previous study by the same author concluded that when considering all hospital related admissions (not just potentially avoidable conditions such as jaundice, which could be amenable to earlier intervention in the care pathway), a longer length of birth hospitalisation was associated with a higher risk of readmission (Lain 2014). Another recent study by Harron and colleagues found no association between postnatal length of stay and risk of readmission within 30 days for term infants. However, for premature infants between 34 weeks and 36 weeks gestation, each additional day of postnatal stay in hospital was associated with an 8.6% decreased risk of readmission (Harron 2017).
Authors' conclusions
Implications for practice.
In this review, we wanted to answer the following questions in order to help women, clinicians and policymakers make informed decisions.
1. Does a policy of early postnatal discharge for healthy mothers and term infants increase infant mortality, readmissions and contacts with health services after leaving hospital?
Low‐certainty evidence and wide confidence intervals mean that we are uncertain whether early discharge, compared with standard discharge has any effect on the risk of infant mortality within one year. Moderate‐certainty evidence shows that early discharge, compared with standard discharge probably slightly increases infants readmitted within 28 days compared to those discharged according to standard protocol. We are uncertain whether early discharge has any effect on readmissions within seven days. Moderate‐certainty evidence shows that early discharge compared with standard discharge probably makes little to no difference in the number of infants having at least one unscheduled medical consultation or contact with health professionals, although this finding must be interpreted with caution due to the considerable variation in co‐interventions and support available to families at home following discharge. No trials reported on infants attending hospital casualty or emergency department within 28 days.
2. Does a policy of early postnatal discharge for healthy mothers and term infants increase maternal mortality, readmissions and contacts with health services after leaving hospital?
No studies reported on maternal mortality within six weeks postpartum, although two studies reported maternal mortality within one year, finding that no maternal deaths in either the early discharge or control group. Moderate‐certainty evidence indicates that early discharge probably results in little to no difference in women readmitted within six weeks, and probably little to no difference in the number of women having at least one unscheduled contact with health professionals. The proportion of women attending hospital casualty or emergency department within six weeks after birth was not reported by any of the trials.
3. Does a policy of early postnatal discharge for healthy mothers and term infants increase breastfeeding problems, and/or decrease the duration of breastfeeding?
Moderate‐certainty evidence shows that early discharge probably results in little to no difference in women breastfeeding at six weeks. When considering duration of breastfeeding, we found that there is also little to no difference between early discharge and standard discharge in the proportion of women breastfeeding at six months.
4. Does a policy of early postnatal discharge for healthy mothers and term infants influence women's satisfaction with postnatal care in hospital and following discharge?
Findings suggest that there may be little to no difference in satisfaction scores between women who were discharged early and women discharged according to standard protocol. No trials reported on women's satisfaction with their postnatal care in the community following discharge although this would likely depend on the quality of community support available to women in the community.
5. Does a policy of early postnatal discharge for healthy mothers and term infants increase the costs of hospital and/or community postnatal care?
Low‐certainty evidence suggests that early discharge may slightly reduce costs of hospital postnatal care and that early discharge may result in little to no difference in the cost of postnatal care following discharge from hospital in the six weeks after the birth. The latter is likely to depend considerably on the provision of postnatal community support available to women who are discharged early.
Implications for research.
Given the limitations of the evidence to support the practice of early postnatal discharge, there continues to be a need for well‐designed trials of this intervention to inform current practice. However, future studies should be large enough to detect important differences taking into account the likelihood of attrition resulting from post‐randomisation exclusions, protocol deviations (cross‐over) and withdrawals. The role of co‐interventions in addition to early discharge is of particular importance in light of the COVID‐19 pandemic, where many women and infants have not received the standard postnatal care following discharge from hospital, due to restrictions on home visiting (MacGregor 2020). Process evaluation to assess the nature and uptake of any co‐interventions is of critical importance as this is likely to affect satisfaction with postnatal care and utilisation of community health services. Use of standardized approaches to outcome assessment would greatly improve the capacity to interpret results, particularly for outcomes regarding utilisation of health services following discharge from hospital, and compare the findings of future studies.
We only identified one small ongoing trial (Namagembe 2014), and in the absence of further trials (due to the difficultly of conducting them in this area of study), it is likely that observational studies would help to make the evidence more certain. Additionally, meta‐analysis of individual patient data from the existing randomised trials would help to resolve some of the difficulties in analysing studies with such heterogenous interventions. Future reviews may benefit from approaching the analysis using alternative methods of comparison, based on time, to overcome the issue of heterogeneous definitions of early and late discharge.
What's new
| Date | Event | Description |
|---|---|---|
| 21 May 2021 | New search has been performed | Search updated. We included four new trials (Bayoumi 2016; Chiong 2012; Kruse 2021; Taiba 2012), plus three trials that were previously excluded (Burnell 1982; McKeever 2002; Thompson 1999). |
| 21 May 2021 | New citation required and conclusions have changed | Early discharge probably leads to a higher risk of infant readmission within 28 days of birth but probably makes little to no difference to the risk of maternal readmission within six weeks postpartum. We are uncertain if early discharge has any effect on the risk of infant or maternal mortality. |
History
Protocol first published: Issue 1, 2001 Review first published: Issue 3, 2002
| Date | Event | Description |
|---|---|---|
| 1 December 2008 | New search has been performed | Update. New search identified two additional studies for inclusion (Boulvain 2004; Sainz Bueno 2005). Two studies previously awaiting classification were excluded (Burnell 1982a; Thompson 1999a), and a further four studies were also excluded (Escobar 2001; Lieu 2000; McKeever 2002a; Steel O'Connor 2003). Main results and conclusions remain unchanged. |
| 19 August 2008 | Amended | Converted to new review format. |
Acknowledgements
Our thanks to Caroline Crowther, Judith Lumley and Lyn Watson for comments on the review protocol, and Judith Lumley for comments on the original review. Our thanks also to Rhonda Small, Ann Krastev, Sara Kenyon and Brenda Argus for their involvement in the previous update of the review. We are also grateful to Dr Anne Kruse for providing information about her trial.
As part of the prepublication editorial process, this updated review has been commented on by three peers (an editor and two referees who are external to the editorial team), a member of the Pregnancy and Childbirth Group's international panel of consumers and the Group's Statistical Adviser. The authors are grateful to the following peer reviewers for their time and comments: Dr Edgardo Abalos, Vice Director, Centro Rosarino de Estudios Perinatales (CREP), Rosario, Argentina; Dr Andrew G Symon; University of Dundee; and Rachel Plachcinski, Cochrane Consumer.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Evidence Synthesis Programme, the NIHR, National Health Service (NHS) or the Department of Health and Social Care.
Appendices
Appendix 1. Search terms for ICTRP and ClinicalTrials.gov
ICTRP
each line was run separately
early AND discharge AND birth
early AND discharge AND childbirth
early AND discharge AND postpartum
early AND discharge AND postnatal
hospital AND discharge AND caesarean
hospital AND discharge AND cesarean
timing AND discharge AND caesarean
hospital AND discharge AND cesarean
ClinicalTrials.gov
Advanced search
childbirth | Interventional Studies | early discharge
childbirth | Interventional Studies | care pathway
postnatal | early discharge
postpartum | early discharge
cesarean | early discharge
Data and analyses
Comparison 1. Early versus standard discharge.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Infants readmitted for neonatal morbidity within 7 days | 2 | 247 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.42, 3.16] |
| 1.2 Infants readmitted for neonatal morbidity within 28 days | 10 | 6918 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.27, 1.98] |
| 1.2.1 Trials conducted in 1960s | 1 | 2151 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.83 [0.43, 7.80] |
| 1.2.2 Trials conducted in 1970s | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.00 [0.25, 101.25] |
| 1.2.3 Trials conducted in 1980s | 2 | 226 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.44 [0.12, 1.63] |
| 1.2.4 Trials conducted in 1990s | 2 | 540 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.43 [0.87, 6.79] |
| 1.2.5 Trials conducted in 2000s | 1 | 430 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.15, 2.53] |
| 1.2.6 Trials conducted in 2010s | 3 | 3483 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.65 [1.30, 2.10] |
| 1.3 Infants readmitted for neonatal morbidity within 28 days: mode of birth subgroups | 10 | 6918 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.27, 1.98] |
| 1.3.1 Vaginal birth | 5 | 2854 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.30 [0.55, 3.09] |
| 1.3.2 Caesarean birth | 4 | 3605 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.57 [1.24, 1.99] |
| 1.3.3 Vaginal or caesarean | 1 | 459 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.43 [0.87, 6.79] |
| 1.4 Infants readmitted for neonatal morbidity within 28 days: subgroups < 24h vs > 24h | 10 | 6918 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.27, 1.98] |
| 1.4.1 Early discharge < 24 hours | 3 | 3770 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.64 [1.28, 2.09] |
| 1.4.2 Early discharge > 24 hours | 6 | 3060 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.28 [0.73, 2.25] |
| 1.4.3 Early discharge range < 24 hours and > 24 hours | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.00 [0.25, 101.25] |
| 1.5 Women readmitted within six weeks | 11 | 6992 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.82, 1.54] |
| 1.5.1 Trials conducted in 1960s | 1 | 2094 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.84 [0.68, 11.81] |
| 1.5.2 Trials conducted in 1970s | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.5.3 Trials conducted in 1980s | 3 | 357 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.05, 1.36] |
| 1.5.4 Trials conducted in 1990s | 2 | 540 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.03 [0.37, 10.95] |
| 1.5.5 Trials conducted in 2000s | 1 | 430 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.22, 2.99] |
| 1.5.6 Trials conducted in 2010s | 3 | 3483 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.78, 1.58] |
| 1.6 Women readmitted within six weeks: mode of birth subgroups | 11 | 6992 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.82, 1.54] |
| 1.6.1 Vaginal birth | 6 | 2928 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.58, 3.02] |
| 1.6.2 Caesarean section | 4 | 3605 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.74, 1.49] |
| 1.6.3 Vaginal and caesarean | 1 | 459 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.03 [0.37, 10.95] |
| 1.7 Women readmitted within six weeks: subgroups < 24 hours vs > 24hrs | 11 | 6992 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.82, 1.54] |
| 1.7.1 Early discharge < 24 hours | 4 | 3858 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.76, 1.54] |
| 1.7.2 Early discharge > 24 hours | 7 | 3134 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.28 [0.65, 2.55] |
| 1.8 Women probably depressed within six months | 5 | 4333 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.46, 1.42] |
| 1.8.1 Trials conducted in 1980s | 1 | 104 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.16, 2.57] |
| 1.8.2 Trials conducted in 1990s | 1 | 459 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.41, 1.44] |
| 1.8.3 Trials conducted in 2000s | 1 | 430 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.05, 1.19] |
| 1.8.4 Trials conducted in 2010s | 2 | 3340 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.44, 2.64] |
| 1.9 Women probably depressed within six months: mode of birth subgroups | 5 | 4333 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.46, 1.42] |
| 1.9.1 Vaginal birth | 2 | 534 | Risk Ratio (M‐H, Random, 95% CI) | 0.43 [0.15, 1.19] |
| 1.9.2 Caesarean birth | 2 | 3340 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.44, 2.64] |
| 1.9.3 Vaginal or caesarean birth | 1 | 459 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.41, 1.44] |
| 1.10 Women probably depressed within six months: subgroups < 24 h vs < 24 hrs | 5 | 4333 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.46, 1.42] |
| 1.10.1 Early discharge < 24 hours | 3 | 3770 | Risk Ratio (M‐H, Random, 95% CI) | 0.62 [0.18, 2.16] |
| 1.10.2 Early discharge > 24 hours | 2 | 563 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.42, 1.32] |
| 1.11 Women breastfeeding (exclusively or partially) at six weeks postpartum | 10 | 7156 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.96, 1.13] |
| 1.11.1 Trials conducted in 1960s | 1 | 2257 | Risk Ratio (M‐H, Random, 95% CI) | 2.49 [1.59, 3.91] |
| 1.11.2 Trials conducted in 1980s | 2 | 198 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.78, 1.21] |
| 1.11.3 Trials conducted in 1990s | 4 | 931 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.90, 1.19] |
| 1.11.4 Trials conducted in 2000s | 1 | 430 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.99, 1.15] |
| 1.11.5 Trials conducted in 2010s | 2 | 3340 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.83, 1.18] |
| 1.12 Women breastfeeding (exclusively or partially) at six weeks postpartum: mode of birth subgroups | 10 | 7156 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.96, 1.13] |
| 1.12.1 Vaginal birth | 6 | 3112 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.90, 1.47] |
| 1.12.2 Caesarean birth | 2 | 3340 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.83, 1.18] |
| 1.12.3 Vaginal or caesarean birth or not specified | 2 | 704 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.95, 1.11] |
| 1.13 Women breastfeeding (exclusively or partially) at six weeks postpartum: subgroups < 24hr vs > 24 hrs | 10 | 7156 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.96, 1.13] |
| 1.13.1 Early discharge < 24 hours | 3 | 3770 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.90, 1.15] |
| 1.13.2 Early discharge > 24 hours | 4 | 2866 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.77, 1.63] |
| 1.13.3 Early discharge range < 24 hours and > 24 hours | 3 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.90, 1.34] |
| 1.14 Women breastfeeding (exclusively or partially) at 12 weeks postpartum | 1 | 430 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.21 [1.03, 1.41] |
| 1.15 Women breastfeeding (partially or exclusively) at six months postpartum | 3 | 973 | Risk Ratio (M‐H, Random, 95% CI) | 1.11 [0.87, 1.43] |
| 1.16 Infant mortality within 28 days | 2 | 4882 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.39 [0.04, 3.74] |
| 1.17 Infant mortality within one year | 2 | 1986 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.07, 2.77] |
| 1.18 Number of contacts with healthcare professionals regarding infant health issues within four weeks of birth | 3 | 639 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.67, 1.16] |
| 1.19 Number of contacts with healthcare professionals regarding maternal health issues within six weeks of birth | 2 | 464 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.43, 1.20] |
| 1.20 Women reporting health problems (including perineal pain, perineal infection, breast soreness, breast infection, caesarean wound pain, caesarean wound infection) in the first six weeks postpartum | 1 | 200 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.11, 0.59] |
| 1.21 Women reporting infant feeding problems | 2 | 2405 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.43, 1.86] |
| 1.22 Women satisfied with postnatal care ‐ dichotomous data | 4 | 3098 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.95, 1.29] |
| 1.23 Satisfaction with postnatal care ‐ continuous data | 2 | 306 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.74 [0.50, 0.98] |
| 1.24 Women who perceive their length of hospital stay as too short | 1 | 82 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.00 [0.19, 21.21] |
| 1.25 Women perceive their length of hospital stay as too long | 1 | 82 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.56 [0.20, 1.52] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bayoumi 2016.
| Study characteristics | ||
| Methods | Design: RCT Location: Maternity Hospital, Faculty of Medicine, Cairo University, Egypt PN recruitment: “All patients were assessed after 24 h, those fulfilling our discharge criteria were randomised using sealed envelopes” | |
| Participants | Number of women eligible: 3786 Number of participants randomised to treatment groups: A: 1890; B 1896. Number of post‐randomisation exclusions: A: 132/1890 refused to be discharged after 24 hours; B: 188/1896 refused to be discharged after 72 hours. (all women in both groups were still eligible for early discharge) Number of withdrawals: A: 263/1758 lost to follow‐up B 205/1708 lost to follow‐up Number of women analysed: A: 1495 B: 1503 Maternal age (years) (mean (SD)) (per group if available): A: 30.6 (6.2); B: 30.9 (5.7) Gestational age at birth (per group if available): A: 39.44 (1.47); B: 39.07 (1.28) Inclusion criteria: caesarean section, age from 20 to 40 years; no known medical condition, e.g. diabetes, hypertension, renal, cardiac, chest problems or connective tissue disease; no obstetric complications, e.g. placenta previa, placenta accreta, accidental hemorrhage or preeclampsia; all term pregnancies 37 weeks or more; no fetal problems, e.g. intrauterine growth retardation or major congenital anomalies; and all patients who are discharged with their newborn. Exclusion criteria: age less than 20 years or more than 40 years; patients with a known medical problem; patients with any obstetric complication; any preterm delivery; any fetal problem diagnosed after delivery or patients and newborns who did not meet our criteria of discharge at the 24 or 72 h interval chosen for their discharge. |
|
| Interventions | A: (n = 1890) discharge 24 hours after caesarean delivery B: (n = 1896) discharge 72 hours after caesarean delivery Duration of follow‐up: 6 weeks |
|
| Outcomes | Wound infection Abdominal pain Secondary postpartum haemorrhage Successful breastfeeding Breast engorgement Intestinal ileus Fever above 38 C Stress incontinence Chest infection Deep venous thrombosis Pulmonary embolism Mood swings measure by Edinburgh Postnatal Depression Scale Hospital readmission |
|
| Notes | Co‐interventions: “Before being discharged, all patients were given strict instructions about wound care and breast feeding. We could not offer home visits by healthcare professionals but patients could access medical help through our morning outpatient clinics or through the 24‐h emergency department.”
Dates of study: June 2012 to February 2014. Funding sources: not reported Declarations of interest: “The authors report no declarations of interest” |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “randomised using sealed envelopes, containing the discharge protocol, attached to the file of each patient, these envelopes were opened after 24 h and patients were discharged according to the chosen protocol and those who did not fulfil the criteria of discharge after 24 h were excluded from the study” Random sequence generation not reported. |
| Allocation concealment (selection bias) | Low risk | “randomised using sealed envelopes, containing the discharge protocol, attached to the file of each patient, these envelopes were opened after 24 h and patients were discharged according to the chosen protocol and those who did not fulfil the criteria of discharge after 24 h were excluded from the study” |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmission |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | “All the outcome measures in the study were largely self‐reported and were not confirmed by medical personnel. However, the outcome measures were not controversial and there was no reason for the participants to be dishonest in their responses” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No differential attrition but no ITT analysis. 1495/1890 and 1503/1896 women were included in the analysis “All the patients came after 6 weeks for postpartum check‐up, patients who did not attend this postpartum visit were excluded from our study” |
| Selective reporting (reporting bias) | Unclear risk | No indication that the trial was registered prospectively. No mention of protocol. We do not have enough information to know if the trialists measured and reported all the outcomes that they pre‐specified |
| Other bias | Low risk | No indication of any other sources of bias |
Boulvain 2004.
| Study characteristics | ||
| Methods | AN recruitment Randomisation: by telephone, using sealed envelopes. Recruitment and randomisation at > 37 weeks' gestation. Blinding: caregivers, women and outcome assessment unblinded. Follow‐up to 6 months pp. Analysis: intention to treat. Loss to follow‐up: 16/459 = 3.5% comprising 11 in early discharge arm and 5 in comparison arm. Duration: November 1998 to October 2000. Setting: urban tertiary level hospital, Switzerland. |
|
| Participants | Number of women eligible: 2324
Number of participants randomised to treatment groups: 459 (A: 228; B: 231)
Number of post‐randomisation exclusions: A: 1; B: 0.
Number of women who remained in trial: A: 227; B: 231.
Number of women analysis: A: 227; B: 231. Inclusion criteria: primiparous and multiparous women at low risk of caesarean delivery and/or postnatal complications > 37 weeks' gestation. Exclusion criteria: women with a strong preference for long or short length of stay; placenta praevia; pre‐eclampsia; diabetes treated with insulin; medical complications of pregnancy requiring postnatal surveillance; past history of postnatal complications (e.g. postnatal depression); difficult socio‐economic situation; multiple pregnancy; suspected intrauterine growth retardation or large infant for gestational age; fetal malformation or genetic disease. Characteristics: maternal age: A: mean 29 years (SD 4.8); B: mean 29 years (SD 5.5); primiparous A: 60%; B: 57%; married A: 83%; B: 82%; income < 50,000 CHF A: 27%; B: 24%; tertiary education A: 48%; B: 49%; Swiss origin A: 31%; B: 30%; current smoker A: 25%; B: 17%, infant birthweight A: 3420 (SD 435); B: 3480 (SD 405). |
|
| Interventions | A: (n = 228): home based postnatal care with discharge planned for 24 < 48 hours following vaginal births and 72 < 84 hours after caesarean. B: (n = 231): hospital based postnatal care with discharge planned 4 to 5 days postpartum (pp) following vaginal births and 6 to 7 days pp following caesareans. Co‐intervention (A and B): minimum of 2 nurse home visits and 10 phone calls; number and timing determined by the family. |
|
| Outcomes | Infant readmissions within 28 days and in first 6 months pp. Maternal readmissions within 28 days and in first 6 months pp. Proportion of women depressed at 28 days pp. Proportion of women breastfeeding at 7 days and 28 days pp. Proportion of women reporting breastfeeding problems. Maternal satisfaction with postnatal care. Costs of hospital care post birth to discharge. Costs of postnatal care post discharge to 6 weeks pp. |
|
| Notes | Significant non‐compliance in A group; mean length of stay A: 65 hours; B: 106 hours. Dates of study: November 1998 to October 2000 Funding sources: "The study received financial support from the Swiss National Science Foundation (grant #32‐52954.97) and from the Quality of Care Program, Geneva University Hospitals." Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The allocation sequence was prepared with a computer program generating a random sequence of numbers in blocks of varying size (four, six and eight participants), arranged in random order” |
| Allocation concealment (selection bias) | Low risk | "Consenting women were allocated to home or hospital care postpartum by opening a consecutively numbered, opaque, sealed envelope. The envelopes were opened by a third party, usually the trial co‐ordinator during a telephone call with the research midwife” |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmission |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low attrition and not differential |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time. |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Brooten 1994.
| Study characteristics | ||
| Methods | Method of randomisation: sealed envelopes, recruitment and randomisation 24 hours post caesarean. Blinding: caregivers and women unblinded, blinding of outcome assessment unclear. Loss to follow‐up: not reported Analysis: by intention to treat. Follow‐up: 8 weeks pp. Duration: August 1988 to January 1991. Setting: urban tertiary‐level hospital, US. |
|
| Participants | Number of women eligible: not reported Number of participants randomised to treatment groups: not reported Number of post‐randomisation exclusions: not reported. Number of withdrawals: not reported Number of women analysed (per group if available): A: 61; B: 61. Inclusion criteria: unplanned caesarean delivery in hospital, English speaking; healthy mother and infant (range: 2270 to 4680 g; 36 to 43 weeks' gestation). Characteristics: Maternal age: early mean 29 (SD 6), standard 28 (SD 6); Marital status: early 67% married, standard 56% married; Income (< $10,000) early 29%, standard 33%. Education (< high school) early 15%, standard 21%. 'Race' (African American and 'non‐white') early 53%, standard 61%. Birthweight: early mean 3305 g (SD 483), standard 3440 g (SD 572). Gestation: early mean 39 weeks (SD 1.5), standard 39 weeks (SD 1.7). |
|
| Interventions | A: discharge 'earlier than usual' (mean stay of 3.6 days); B: discharge according to 'routine hospital practice' (mean stay of 4.8 days). Co‐interventions: A had minimum of 2 home visits post discharge, plus 10 phone calls to 8 weeks, plus women had phone number to nurse and physician. B had no routine follow‐up care at home post discharge. |
|
| Outcomes | Infant and maternal re‐admissions. Infant and maternal acute care visits. Maternal satisfaction with care. Proportion of infants immunized. Mean cost per woman for care from birth to discharge and for post discharge care. | |
| Notes | Women in standard care considered ready for discharge if: ambulatory, voiding, tolerating normal diet, passing flatus, experiencing normal uterine involution, afebrile for 24 hours, uncomplicated wound healing, removal of sutures and an adequate blood count. Women in early group had same criteria except: staple removal and afebrile status for at least 24 hours. If women in early group did not meet these criteria, they were not discharged early but still received co‐interventions and were analysed with early group. Dates of study: August 1988 to January 1991 Funding sources: "This study was supported by a grant (Pol‐NR‐01859) from the National Institute for Nursing Research, National Institutes of Health" Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation list prepared in advance by a statistician. |
| Allocation concealment (selection bias) | Low risk | Adequate.Sequence of sealed envelopes containing cards with the name of the next treatment group |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Loss to follow‐up not reported. |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Burnell 1982.
| Study characteristics | ||
| Methods | Design: 4‐arm study, 2 arms allocated by randomisation, 2 arms allocated according to woman’s preference AN recruitment Setting: Oxford, UK | |
| Participants | Number of women eligible: “242 women were considered at booking for inclusion in the study”
Number of participants randomised to treatment groups: A: 23; B: 19. (only those who did not express a preference for short or long stay in hospital were allocated randomly)
Number of post‐randomisation exclusions: not reported
Number of women who remained in trial: 153 (106 participants were self‐selecting not randomised: 33 in early discharge group, 73 in standard stay group)
Number of withdrawals: not reported
Number of women analysed (per group if available): 148
Maternal age (years) (mean (SD)): not reported
Gestational age at delivery (weeks): A: 39.44 (1.47); B: 39.07 (1.28) Inclusion criteria: All women over 18 of any parity, ethnic background and social class were included. Exclusion criteria: women with major clinical disorders and those to be delivered by caesarean section |
|
| Interventions | A: (n = 23) transfer to postnatal care at home 48 hours after delivery B: (n = 19) conventional hospital stay of 8 to 9 days Duration of follow‐up: 6 weeks |
|
| Outcomes | Physical problems of mother and child Feeding and related problems Emotional state of the mother Mother's attitude towards her ability to cope, to her baby and to postnatal care |
|
| Notes | Co‐interventions: not reported Dates of study: not reported Funding sources: not reported Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Allocated to either (c) early discharge: randomised. or (d) usual stay: randomised.” No details reported about how randomisation was done |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not possible to blind women. Lack of blinding could have an effect on outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No data reported per randomised group so we do not know how many women withdrew per group |
| Selective reporting (reporting bias) | High risk | No outcomes reported per randomised group |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Carty 1990.
| Study characteristics | ||
| Methods | Method of randomisation: sealed envelopes placed on file prior to home visit at 38 weeks.
Recruitment and randomisation at 37 weeks' gestation. Blinding: caregivers, women and outcome assessment unblinded. Follow‐up to 1 month pp (most outcomes). Loss to follow‐up: 58/189 (30.7%), including 46 post‐randomisation exclusions, 10 not compliant with randomisation outcome, 2 withdrawals; 97/131 returned 1 month questionnaires. Analysis: not intention to treat. Duration: not reported. Setting: urban tertiary‐level hospital, Canada. |
|
| Participants | Number of women eligible: 189 Number of participants randomised: 189 (not reported per group) Number of post‐randomisation exclusions: 45 no longer met the inclusion criteria Number of withdrawals: 1 home birth, 2 reversed their decision to participate, 10 chose to go home at times other than the discharge times to which they had been assessed. Number of women analysed: A: 44; B: 49. C 38 Inclusion criteria: normal labour and hospital birth. Exclusion criteria: caesarean, forceps delivery. Participants were 53% primiparous; mean maternal age 30.2 (SD 3.8); 93% married or living with partner; 58% combined family income > $40,000; 65% completed junior college or university; 95% 'Caucasian'; mean paternal age 32.9 (SD 5.5). No significant group differences found on demographic characteristics (but no data provided by group). |
|
| Interventions | 3 groups, discharge at: 12 to 24 hours (n = 44), 25 to 48 hours (n = 49) or
4 days (n = 38). Co‐interventions:
|
|
| Outcomes | Infant and maternal re‐admissions. Maternal depression, anxiety and confidence. Maternal satisfaction with nursing care. Breastfeeding at 1 month pp. Referrals to physicians for maternal and infant health issues. | |
| Notes | Mean length of stay: 12 to 24 hrs:1.12 days (SD 0.4). 25 to 48 hrs: 2.06 days (SD 0.6). 4 days: 4.03 days (SD 0.7). Study nurses participated in 2 weeks special training for the early discharge program. Dates of study: not reported Funding sources: not reported Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Using a table of random numbers. |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes containing the assignment was placed on the file of each prospective participant and opened by the nurse. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Differential attrition (82%, 74% and 66% returned follow‐up questionnaires) |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Chiong 2012.
| Study characteristics | ||
| Methods | Design: RCT PN recruitment: “The envelope was opened on post cesarean day 1 morning ward round by the health care provider to reveal the allocation” Location: A university hospital in Kuala Lumpur, Malaysia | |
| Participants | Number of women eligible: 360
Number of participants randomised to treatment groups: 360 (A: 179; B: 181)
Number of post‐randomisation exclusions: A: 9/179; B: 9/181
Number of women who remained in trial: A: 170; B: 172
Number of withdrawals: A: 28/170 (9 declined discharge, 19 either mother or baby not fit for discharge) B: 24/172 (12 took discharge on day 1, 12 either mother or baby not fit for discharge)
Number of women analysed: A: 142; B: 148. Maternal age (years) (mean (SD)): A: 31.8 (4.6); B: 31.5 (4.1) Gestational age at birth (per group if available): A: 38.8 (1.0); B: 38.7 (0.9) Inclusion criteria: planned caesarean delivery, age 18 years or older, and gestation 37 weeks or greater with a singleton pregnancy Exclusion criteria: grossly abnormal fetus, established medical problems, or operative factors likely to preclude day 1 discharge (e.g., pre gestational diabetes, preeclampsia, epilepsy, cardiac disease, renal disease, connective tissue disease, antiphospholipid syndrome, 2 or more previous caesarean deliveries, and major previa). Protocol predefined discharge criteria which were; surgically uncomplicated caesarean, blood loss 800 mL or less, post operative haemoglobin of 80 g/L or greater, unassisted ambulation to the bathroom, established urination, tolerated at least 1 normal meal, afebrile (temperature less that 380C in the last 24 hours), normal blood pressure and healthcare professional willing to discharge. Neonatal discharge was predicated on standard paediatric practice. Characteristics: similar between the arms for maternal age (31.8 versus 31.5 years); gestational age 38.8 versus 38.7 weeks; parity both 1; ethnicity; Malay 104 (58.1%) versus 100 (55.2%), Indian 29 (16.2%) versus 43 (23.8%), Chinese 35 (19.6%) versus 28 (15.5%), other 11 (6.1%) versus 10 (5.5%). Employed: 134 (74.9%) versus 137 (75.7%), Homemaker or student 45 (25.1%) versus 44 (24.3%); Education: primary 9 (5.0%) versus 2 (1.1%), secondary 67 (37.4%) versus 76 (42%), and Tertiary 103 (57.5%) versus 103 (56.9%). |
|
| Interventions | A: (n = 179) discharge 1 day after caesarean B: (n = 181) discharge 2 days after caesarean Duration of follow‐up: 6 weeks | |
| Outcomes | Primary outcomes: satisfaction with discharge protocol at 2 weeks after discharge by means of a 5 point Likert scale (top 2 responses taken as demonstrating satisfaction and other 3 responses as non satisfaction) and self reported breastfeeding at 6 weeks. Secondary outcomes assessed at 2 weeks: Double check to see and add readmissions
Secondary outcomes assessed at 6 weeks after discharge:
|
|
| Notes | Co‐interventions: “Home visit by health care professionals from our center were not on offer but our patients have free access to our clinics and acute care facilities, which were opened at all hours. An appointment was routinely given for maternal and newborn follow‐up at 2 weeks after caesarean delivery. After this, another routine appointment would be given at 6 weeks postdelivery. Additional appointments may be scheduled as clinically required” Dates of study: November 2010 to February 2012 Funding sources: University of Malaya Declarations of interest: "Financial Disclosure: The authors did not report any potential conflicts of interest." |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "online random number generator (www.random.org) in random blocks of 4 to 8 on a 1:1 ratio" |
| Allocation concealment (selection bias) | Low risk | "A sealed numbered opaque envelope containing the allocated discharge protocol was then attached to the chart of each participant. The envelope was opened on post cesarean day 1 morning ward round by the health care provider to reveal the allocation” |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No differential attrition; the analysis included data from women who did not adhere to the allocated group and from women who were no longer eligible for early discharge but they did not ana lyze data from women who no longer met the trial eligibility criteria. Overall level of missing data for any reason: 5% |
| Selective reporting (reporting bias) | Unclear risk | No protocol available, retrospectively registered. Insufficient information to judge whether all pre‐specified outcomes were reported |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Gagnon 1997.
| Study characteristics | ||
| Methods | Randomised controlled trial Antenatal recruitment Setting: urban university hospital, Canada. |
|
| Participants | Number of women eligible: 938
Number of participants randomised to treatment groups: 360 (A: 183; B: 177)
Number of post‐randomisation exclusions: A: 85/183; B: 74/177.
Number of women who remained in trial: A: 80; B: 100.
Number of withdrawals: A: 18/98; B: 3/103 (no explanations given for these withdrawals)
Number of women analysed: A: 78; B: 97. Inclusion criteria at randomisation: parity 0 to 4; normal pregnancy (no medical conditions, not breech); English, French or Spanish speaking. intrapartum exclusion criteria were rupture of membranes ‐‐> 24 hours before birth, caesarean delivery, intrapartum blood loss > 500 mL, and third‐ or 4th‐degree perineal laceration. Postpartum exclusion criteria for the mother were soft fundus with excessive bleeding, inability to void adequately, inability to ambulate easily or to care for herself and her infant, non receipt of RhoGAM when indicated, and medical conditions requiring close supervision; for the infant they were multiple birth, birth weight < 2500 g, gestational age < 36 completed weeks, abnormal newborn physical examination, and intolerance to feedings (breast or bottle) in hospital. Characteristics of participants: Mean maternal age (SD): early 29.6 (4.7), standard 29.1 (5.3). Parity (% nulliparous): early 38%, standard 34%. Living with a partner: early 85.5%, standard 93.8%. % 'blue collar': early 21.8%, standard 16.5%. Mean years of maternal education (SD): early 13.8 (3.8), standard 14.0 (3.9). % recent immigrants: early 14.7%, standard 24.7%. Mean birthweight (SD): early 3389g (419), standard 3496g (364). Mean gestation (SD): early 39.3 (1.3), standard 39.5 (1.1). Planned to breastfeed: early 70.5%, standard 54.6%. Smoking in pregnancy: early 23.1%,standard 9.3%. |
|
| Interventions | A: (n = 183 randomised, 98 remained eligible after giving birth) “The early postpartum discharge program consisted of a postpartum hospital stay of 6 to 36 hours and nursing care by telephone, within 48 hours pp and at 10 days pp, and also at home, at 34 to 38 weeks' gestation and at 3 and 5 days pp. 2 part‐time nurses made the visits, which lasted a maximum of 1 hour. The postnatal intervention was offered only to women who had left the hospital within 36 hours of the birth to encourage them to leave the hospital early if they had been randomised into this group and to maximize the generalisability of the intervention” B: (n = 177 randomised, 103 remained eligible after giving birth) postpartum stay of 48 to 72 hours and follow‐up as determined by the woman's and infant's physicians. Duration of follow‐up: 1 month | |
| Outcomes | Breastfeeding Infant health contacts post discharge. Maternal satisfaction with care to day 10 pp. Perceived maternal competency. | |
| Notes | Significant non‐compliance with early discharge allocation in the early group ‐ mean length of stay 37.5 hours (26 women ‐ 33% went home later than planned). Dates of study: January to December 1990 Funding sources: "Funded by a grant from Le Fonds de la Recherche en Santé du Québec. A.J.G. was supported by the Medical Research Counil and the National Health Research and Development Program of Canada" Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Subjects were stratified by date of immigration and parity and randomised 32‐38 weeks' gestation in blocks of 8 according to a random number table |
| Allocation concealment (selection bias) | Low risk | Group assignment was placed in sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | No blinding and the outcome is likely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Differential withdrawals across groups: A: 18/98; B: 3/103 (no explanations given for these withdrawals) |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Hellman 1962.
| Study characteristics | ||
| Methods | Postnatal recruitment Blinding: caregivers, women and outcome assessment unblinded. Follow‐up to 3 weeks pp. Loss to follow‐up: not reported. Analysis: by intention to treat. Duration: 1 July 1959 to 30 June 1960. Setting: urban hospital, New York, US. |
|
| Participants | Number of women eligible: not reported Number of participants randomised to treatment groups: 2257 (A: 1941; B: 316) Number of post‐randomisation exclusions: not reported Number of women analysed: A: 1941; B: 316 Inclusion criteria: hospital birth, mothers deemed eligible for early discharge, babies predominantly > 2500 g, baby gestation not specified. Exclusion criteria: caesarean section, stillbirth, no English. Characteristics of participants: Median age: early 23.6 yrs, standard 23.8 yrs. No living children: early 28%, standard 29%. Married: early 70%, standard 73%. Welfare/no income: early 16%, standard 13%. Ethnicity: Negro/Puerto Rican early 81%, standard 85%. Few details available on babies. |
|
| Interventions | A: (n = 1941): discharge before 72 hrs.
B: (n = 316): discharge after 5 days. Co‐interventions: midwife home visits post discharge (3 in A, 2 in B) for examination of mother and baby and other data collection (not for 'helping' mothers). Duration of follow‐up: 3‐4 weeks after discharge |
|
| Outcomes | Infant and maternal re‐admissions within 3 weeks. Infants deaths. Proportion of women breastfeeding at 3 weeks. Reported infant feeding problems. Proportion of women dissatisfied with hospital postnatal care. Proportion of women dissatisfied with length of stay. Proportion of fathers thinking stay too short. Proportion of fathers thinking stay too long. Limited cost data. | |
| Notes | Dates of study: not reported Funding sources: 'United States Public Service Grant' Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | “Included in the experimental group was every patient who was discharged from the hospital within 72 hours during a five‐day work week” control group: “selected by numbering every patient delivered in the hospital and choosing the patients who were to be in the control group by a series of previously randomised numbers” |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement of 'low risk' or 'high risk' |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Loss to follow‐up not reported. |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Kruse 2021.
| Study characteristics | ||
| Methods | 2‐arm, parallel assignment RCT No blinding Antenatal recruitment Setting: Department of Obstetrics and Gynecology, Herning Hospital, Denmark |
|
| Participants | Number of women eligible: 328 Number of participants randomised to treatment groups: 143 (A)72 (B)71) Number of post‐randomisation exclusions (per group if available): A) 0 B) 0 Number of women included in ITT analysis: A) 72, B) 71 Number of women responding to questionnaire (Parents’ Postnatal Sense of Security): A) 53/72 B) 52/71 Maternal age (years) (mean (SD)) (per group if available): A) 33.4 (4.5) B) 32.6 (4.6) Gestational age at birth (per group if available):38.7 (SD 0.54) 38.9 (SD 0.48) Inclusion criteria: planned caesarean section Exclusion criteria: nulliparity, multiple pregnancy, gestational age < 37 + 0, planned prolonged postoperative observation, pre‐pregnancy BMI > 35 kg/m2, maternal age,18 yrs, living alone, or inability to read and write Danish. Discharge criteria: no symptoms of postpartum complications, sufficient mobilisation and analgesia, normal voiding function and successfully initiated breastfeeding if anticipated. Inclusion Criteria:
Exclusion Criteria:
|
|
| Interventions | A: (n = 72) [discharge at 28 hours] B: (n = 71) [discharge > 48 hours] Duration of follow‐up: 1 month | |
| Outcomes | Primary outcome:
Secondary outcomes:
|
|
| Notes | Co‐interventions: home visit by a midwife 48‐72 hours after delivery
Dates of study: September 2016 ‐ September 2019
Funding sources: Brodene Hartmanns Foundation
Declarations of interest: the authors have ‘no conflicts of interest to declare’ Data and additional information provided by author (June 2020) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Randomization was conducted using a computerized random number generator (www.randomization.com). The randomisation was generated in a 1:1 ratio in blocks of two and four and stratified according to site and BMI < 30 or 30 kg/m2” |
| Allocation concealment (selection bias) | Low risk | “Envelopes were sealed individually and opened by the woman when written consent was obtained.”Correspondence from study author: “sequentially numbered, opaque sealed envelopes” |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Correspondence from study author: “the outcome assessors were not blinded to the allocations” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Very low attrition: 7/72 and 5/71 excluded from per‐protocol analysis due to emergency caesarean, vaginal delivery or decision not to adhere to allocated group but these women were included in ITT analysis). All women included in the ITT analysis. |
| Selective reporting (reporting bias) | Low risk | No published protocol. Trial was registered prospectively and not all pre‐specified outcomes are reported in full but correspondence with trial author confirms that the outcomes were measured and the data analysis is in process. |
| Other bias | Low risk | No indication of other sources of bias |
McKeever 2002.
| Study characteristics | ||
| Methods | Design: RCT Setting: Toronto, Canada PN recruitment | |
| Participants | Number of women eligible: 214
Number of participants randomised to treatment groups: 148 (A: 72; B: 66)
Number of post‐randomisation exclusions (per group if available): A: 1/72; B: 0/66.
Number of withdrawals: A: 7 withdrew/lost to follow‐up, 5 excluded from analysis; B: 11 withdrew/lost to follow‐up, 7 excluded from analysis
Number of women analysed: A: 56; B: 36. Maternal age (years) (mean, SD): A: 32.0 (4.2); B: 33.1 (4.4) Gestational age at delivery (weeks): A: 38–40 wk 92%, 41 wk 8%; B: 38–40 wk 81%, 41 wk 19% Inclusion criteria: Mothers were eligible if they had delivered a live, singleton infant within the preceding 12 hours, were at least 21 years of age, resided in the defined metropolitan area, had a telephone, intended to breastfeed, were breastfeeding at discharge, and would receive satisfactory support at home. Satisfactory support was determined by postpartum nurses who assessed mothers’ circumstances to ensure the safety and well‐being of infants and mothers. The main criterion was that mothers were not isolated, and had accessible family and friends to provide assistance when necessary. Their newborns were eligible to participate if they were 35 weeks’ gestational age or greater, were breastfed at discharge, and did not have congenital anomalies or morbidities, including hyperbilirubinaemia, blood group incompatibility, or sepsis. Exclusion criteria: Women were excluded if they did not speak English and had experienced caesarean deliveries, postpartum complications, and morbidities such as fever and abnormal bleeding, chronic illnesses, or disabilities. |
|
| Interventions | A: (n = 53) discharged at 24 to 36 hours postpartum and scheduled to receive up to 3 home visits from community nurses qualified as lactation consultants. B: (n = 48) “standard length of hospitalisation” Duration of follow‐up: 12 days postpartum | |
| Outcomes | Proportion of baby’s feeds in past 24 hr that were exclusively breastfeeding % of mothers who used no supplementation in past 24 hr Length of hospitalisation Adverse infant outcomes between the term standard care and experimental groups, such as hyperbilirubinaemia, dehydration, or weight loss |
|
| Notes | Co‐interventions: “As a matter of standard hospital care, mothers of near‐term infants in both groups were made aware of the outpatient hospital breastfeeding clinic, and were encouraged to use a pre existing 24‐hour telephone help line. Mothers of term infants in both groups were also provided with information on these services.” Dates of study: July 1999 to December 2000 Funding sources: “This project was supported by a grant from the Health Transition Fund, Canada,Ottawa,and by a financial contribution from The Hospital for Sick Children Foundation,Toronto,Ontario, Canada.” Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Using central randomisation procedures, eligible mother‐newborn pairs were stratified as term or near term (35–37 weeks’ gestational age), and allocated to either the standard or experimental groups by research staff who had no contact with patient” |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Not possible to blind women. Lack of blinding not like to have an effect on the outcomes measured in the trial. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | “Interviewers were originally blinded to group status. However, in the course of answering questions about postpartum care and satisfaction, mothers inadvertently revealed their group status.” |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Slightly higher attrition in early discharge group. In the full paper, analysis is carried out only in women who completed follow‐up but abstract seems to report outcomes for the full number of women randomised. |
| Selective reporting (reporting bias) | High risk | Outcomes not reported in full per randomised group. No protocol (study published before common practice of publishing protocol) |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Sainz Bueno 2005.
| Study characteristics | ||
| Methods | Recruitment and randomisation in postnatal ward. Blinding: caregivers and women unblinded to intervention; blinding outcome assessment unclear. Follow‐up to 6 months pp. Analysis by intention to treat. Loss to follow‐up: 36/430 (8.4%), including 22 women who did not attend 7 to10 days pp follow‐up; 14 women withdrew consent, see note regarding missing data for maternal satisfaction. Duration: April 1999 to April 2001. Setting: urban maternity hospital, Spain. |
|
| Participants | 430 women recruited and randomised; 213 to early discharge and 217 to standard care Number of withdrawals: A: 19; B: 18. Number of women analysed (per group if available): A: 213; B: 217 Inclusion criteria: primiparous and multiparous women deemed eligible for early discharge, => 37 weeks' gestation with baby of appropriate weight for gestational age; vaginal birth; residence within 20 km of the hospital. Characteristics: age > 30 years A: 41.8%; B: 41.1%; primiparous A: 36.6%; B: 37.8%; married A: 97.2%; B: 97.2%; completed secondary education A: 22.5%; B: 14.7%; infant birthweight A: 3348 g (SD 396); B: 3335 g (SD 372); gestation A: 39.5 weeks (SD 1.13); B: 39.5 weeks (SD 1.12); spontaneous vaginal birth A: 87.8%; B: 88.5%. |
|
| Interventions | A: (n = 213): discharge planned for < 24 hours. B: (n = 217): minimum stay of 48 hours. Co‐intervention: A monitored at home for first 24 to 48 hours post discharge by qualified nurse; A and B attended visit in clinic at 7 to 10 days pp. |
|
| Outcomes | Infant readmissions in first 28 days. Maternal readmissions in first 28 days. Proportion depressed at 4 weeks pp. Proportion breastfeeding at 4 weeks, 12 weeks and 6 months pp. Proportion reporting maternal exhaustion at 7 to 10 days and 4 weeks pp. Proportion reporting physical health problems in first 6 months. Maternal satisfaction with postnatal care. Proportion of women saying length of stay too long. Costs of hospital care post birth; costs of maternal and infant readmissions; cost of maternal and neonatal consultations (post discharge). |
|
| Notes | Significant missing data for maternal satisfaction, with differential loss to follow‐up I 17.8% missing, C 42% missing data. Dates of study: April 1999 to April 2001 Funding sources: not reported Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “randomisation by blocks” Insufficient information in the report to assess whether sequence generation was adequate. |
| Allocation concealment (selection bias) | Low risk | "opaque sealed envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details about how missing data was accounted for |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Smith‐Hanrahan 1995.
| Study characteristics | ||
| Methods | Method of randomisation: unclear.
Recruitment and randomisation: on admission to postnatal unit post birth. Blinding: caregivers and women unblinded; outcome assessment ‐ blinding unclear. Follow‐up to 6 weeks pp. Loss to follow‐up: 44/125 (35.2%); all post‐randomisation exclusions. Analysis: not intention to treat. Duration: not reported. Setting: tertiary teaching hospital, eastern Canada. |
|
| Participants | 139 women approached; 125 agreed and randomised Number of participants randomised to treatment groups: A: 58; B: 67 Number of post‐randomisation exclusions: A: 20; B: 29 Total number of withdrawals: A: 23/58 (3 did not complete the study, 20 excluded ‐ 18 due to jaundice, 1 due to Down’s syndrome, 1 due to mother’s request) B: 21/67 (6 did not complete the study, 7 did not stay long enough, 6 received postnatal home follow‐up, 2 had to stay longer in hospital, 29 transferred to early discharge group due to bed shortages) Number of women analysed (per group if available): A: 35 B: 17 Inclusion criteria: English or French speaking; another adult present at home at least 12 hours/day for 1st 2 days post discharge; no major obstetrical complications at any stage; no prolonged mother‐infant separation in hospital (24 hrs+); medical follow‐up plan before discharge; no complications in infant: 2500‐4500 g; good colour/activity level; vital signs normal; voided and stooled; feeding established. Characteristics of participants: Maternal age: early mean 29.5 (SD 4.5), standard mean 29.3 (SD 4.63). Parity: early 37.1% primiparous, standard 58.7% primiparous. Marital status: early 97.1% married, standard 95.7% married. All vaginal births. Income ‐ % > 40,000+: early 74.1%, standard 55%. Completed college/university education: early 73.5%, standard 54.6%. % not of Canadian/US nationality: early 39.5%, standard 23.5%. |
|
| Interventions | A: (n = 58): early discharge: before 60 hrs.
C (n = 57): discharge: after stay of 60 hrs or more. Co‐inteventions: No antenatal preparation for discharge in either group. Early group received telephone call from nurse within 24 hours of discharge leading to a decision to visit or continue to consult by phone; also received phone number for postnatal follow‐up service which could be called at any time; followed by usual paediatric and obstetric office visits. Standard discharge group received traditional follow‐up post discharge ‐ visit to paediatric office at 2 weeks and obstetric office visit at 6 weeks. |
|
| Outcomes | Infant and maternal re‐admissions to 6 weeks pp. Proportion of women breastfeeding at 6 weeks. Maternal fatigue intensity score at 2 to 3 days pp, 1 week pp and 6 weeks pp. | |
| Notes | 29 women allocated to standard care were sent home early due to bed shortages. The authors ana lyze outcomes for this group separately from the early and standard care groups. For the purposes of this review analyses have been done re‐combining these 29 women with the standard care group, to approximate more closely an intention‐to‐treat analysis. Dates of study: Not reported Funding sources: "This research was supported by a grant from the Fraser Fund of the Royal Vistoria Hospital and a computer equipment grant form the Faculties of Graduate Studies and Research and Meidcine of McGill University" Declarations of interest: Not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information in the report to assess whether sequence generation was adequate. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | High number of withdrawals (due to participants no longer meeting trial criteria) but not differential. A: 23/58 (3 did not complete the study, 20 excluded ‐ 18 due to jaundice, 1 due to Down’s syndrome, 1 due to mother’s request); B: 21/67 (6 did not complete the study, 7 did not stay long enough, 6 received postnatal home follow‐up, 2 had to stay longer in hospital, 29 transferred to early discharge group due to bed shortages) |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Taiba 2012.
| Study characteristics | ||
| Methods | Design: RCT Setting: Dhaka, Bangladesh AN/PN recruitment: not reported | |
| Participants | Number of women eligible: 300
Number of participants randomised to treatment groups: A: 150; B: 150.
Number of post‐randomisation exclusions: 0
Number of women who remained in trial (per group if available): A) B)
Number of withdrawals (per group if available): A: 100/150; B: 0/150.
Number of women analysed (per group if available): A: 50; B: 150.
Gestational age at delivery (weeks): not reported
Inclusion criteria: term pregnant women undergoing elective or emergency caesarean section Exclusion criteria: not reported |
|
| Interventions | A: (n = 150) discharge at 72 hours after caesarean B: (n = 150) discharge at 7 days after caesarean Duration of follow‐up: 7 days after caesarean. | |
| Outcomes | Maternal: Urinary and respiratory tract infections wound infection puerperal sepsis Infant: Umbilical cord sepsis Septicemia respiratory distress syndrome |
|
| Notes | Co‐interventions: not reported Dates of study: July 2006 to December 2006 Funding sources: Not reported Declarations of interest: Not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Randomized” used in title but no description of randomisation.“300 consecutive cases fulfilling the enrolment criteria were included in the study” |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible but lack of blinding not likely to have an effect on the outcomes measured in the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 100/150 withdrawals in early discharge group, no withdrawals in 7 day group. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. No indication of what the pre‐specified outcomes were. |
| Other bias | Low risk | No indication of any other source of bias |
Thompson 1999.
| Study characteristics | ||
| Methods | Design: RCT Setting: Canberra Hospital, Australia AN recruitment | |
| Participants | Number of women eligible: 118
Number of participants randomised to treatment groups: 50 (A: 24; B: 26)
Number of post‐randomisation exclusions: A: 13; B: 5 excluded postpartum and 3 antenatal withdrawals but no explanation for these 3 withdrawals.
Number of women who remained in trial (per group if available): A: 11 (remained eligible for early discharge); B: 18 (remained eligible for early discharge)
Number of withdrawals (described in trial as “did not comply”): A: 8/11; B: 9/18
Number of women analysed (per group if available): A: 11; B: 18.
Inclusion criteria: “women eligible for early discharge (i.e. not classified as high risk and not having a planned caesarean delivery)” Exclusion criteria: “Intrapartum exclusion criteria included caesarean delivery or postpartum haemorrhage. Postpartum exclusion criteria for the mother included inability to care for herself or her infant or any medical conditions requiring close medical supervision. Postpartum exclusion criteria for the baby included jaundice requiring phototherapy, admission to the special care or neonatal intensive care unit, or both. |
|
| Interventions | A: (n = 24) length of stay 36 hours or less B: (n = 26) length of stay 37‐72 hours Duration of follow‐up: 72 hours after giving birth | |
| Outcomes | Women’s satisfaction with group allocation | |
| Notes | Co‐interventions: not reported Dates of study: “a six week period in 1996” Funding sources: “This project was supported from donations by the Salaried Special” Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Women were randomly allocated to groups 1 or 2 at the time of recruitment. The allocation sequence was generated from random number table” |
| Allocation concealment (selection bias) | Low risk | Allocation was “concealed in sequentially numbered, opaque sealed envelopes” |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding not possible. lack of blinding is likely to have an effect on the outcomes measured in the trial. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | No clinical outcomes were measured |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 13/24 and 5/26 postpartum exclusions (i.e. no longer eligible for early discharge) 3/11 and 9/18 complied. No clinical outcomes were measured so unlikely to be any risk of attrition bias |
| Selective reporting (reporting bias) | High risk | The trial was designed to test a null hypothesis of no significant difference between the frequency of postnatal depression in mothers discharged from hospital within 6 hours (A) compared with those discharged 37‐72 hours after delivery (B)’. This outcome was not reported. |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Waldenström 1987.
| Study characteristics | ||
| Methods | Method of randomisation: unclear.
AN recruitment Blinding: women and caregivers not blinded; blinding of outcome assessment ‐ unclear. Follow‐up: women to 6 weeks; infants to 6 months. Loss to follow‐up: 60/164 (36.6%); 47 post‐randomisation exclusions; 13 withdrawals in early discharge group; 100% response to 6‐week questionnaires. Analysis: not intention to treat. Duration: March 1984 to June 1985. Setting: teaching hospital, Uppsala, Sweden. |
|
| Participants | Number of women eligible: 1604
Number of participants randomised to treatment groups: 164 (A: 85; B: 79)
Number of post‐randomisation exclusions: A: 26% (22?); B: 32% (25?)
Number of women who remained in trial: A: 63; B: 54.
Number of withdrawals: A: 13 (various reasons for choosing to stay in hospital longer) B: 0 (5 left hospital early but were included in analysis as per allocated group) Number of women analysed: A: 50; B: 54. Inclusion criteria: pregnancy and birth free from significant complications; vaginal delivery; singleton; gestational age > 37 weeks, birthweight >= 3000 g, Apgar >= 7 at 5 min; and no significant infant or maternal morbidity in first 24 hours. Characteristics of participants: mean maternal age: early 28, standard 27. Proportion primiparous: early 20%, standard 30%. Maternal university education: early 28%, standard 19%. Mean birthweight: early 3658 g, standard 3481 g. In comparison with non‐participants, trial participants had less education, were more 'family‐oriented' and confident about parenthood, and more negative about care in hospital. |
|
| Interventions | A: (n = 85) discharge 24 to 48 hours.
B: (n = 79) discharge 6 days after giving birth Co‐interventions: Early group ‐ nurse home visit 4 weeks before term; visit to hospital on day 5 for paediatric examination; daily nurse home visits for 3 to 4 days post discharge. Standard group: traditional hospital care and no home visits post‐discharge. Duration of follow‐up: infants followed up for 6 months, women followed up for 6 weeks. |
|
| Outcomes | Infant and maternal re‐admissions within 6 and 8 weeks pp respectively. Maternal depressed mood in first 6 weeks. Breastfeeding at 2 and 6 months. Maternal fatigue in first 14 days. Maternal satisfaction with care. | |
| Notes | Mean length of stay at time of study was 6 days; but shorter in standard discharge group where mean stay was 4.1 nights. Women who 'crossed over' were treated differently in early and standard groups: 13 women excluded because they went home later than allocation, whereas 5 women allocated to standard discharge who went home early (but without home visits), were retained in analysis. Dates of study: March 1984 to June 1985 Funding sources: "This study was supported by grants from The Swedish Ministry of Health and Social Affairs, Commission for Social Research (Project no. F 83/18)" Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information in the report to assess whether sequence generation was adequate. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmission |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | More missing data from early discharge group than control group. 13/63 women in the early discharge group chose to stay longer in hospital) and were not included in analysis, except for data obtained from Child Health Center records pertaining to infant morbidity and breastfeeding). 5/54 in the control group chose to leave hospital early and were included in analysis. |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Winterburn 2000.
| Study characteristics | ||
| Methods | Method of randomisation: via "selecting sealed envelopes"; process unclear.
Antenatal recruitment Blinding: women and caregivers not blinded; unclear for outcome assessment. Analysis: by intention to treat and on basis of actual length of stay. Loss to follow‐up: 7/255 (2.7%). Follow‐up: to 1 month pp. Duration: February 1996 to June 1998. Setting: large teaching hospital, north of England. |
|
| Participants | Number of women eligible: not reported
Number of participants randomised to treatment groups: 248 (A: 121; B: 127)
Number of post‐randomisation exclusions: 0
Number of women who remained in trial: A: 121; B: 127.
Number of withdrawals: 7 withdrew for reasons not related to the intervention (study does not report which groups they were in)
Number of women analysed: A: 121; B: 127. Inclusion criteria: first time mothers wanting to breastfeed and with no preference about length of hospital stay; no specified early discharge criteria. Characteristics of participants: no information about socio‐demographic characteristics. |
|
| Interventions | A: (n = 121) hospital stay of 6 to 48 hours.
B: (n = 127) hospital stay of > 48 hours. Co‐interventions: community midwife home visits to support breastfeeding (number of visits and over what time period not specified). |
|
| Outcomes | Proportion of women breastfeeding. | |
| Notes | Major limitation due to cross‐over of study participants ‐ in both directions, resulting in only 51 women experiencing early discharge and 197 experiencing standard discharge.
Unclear whether home visits offered to all women who went home < 48 hours, regardless of allocated group status. Dates of study: February 1996 to June 1998 Funding sources: "The study was supported by a grant from the Northern General Hospital Trust Research Committee." Declarations of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information in the report to assess whether sequence generation was adequate. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcomes measured. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 7/155 women withdrew for reasons not related to duration of hospital stay.All other women analysed according to allocated group. |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
Yanover 1976.
| Study characteristics | ||
| Methods | RCT Antenatal recruitment Setting: Departments of Obstetrics, Pediatrics and Nursing, Kaiser‐Permanente Medical Center, San Francisco, USA. |
|
| Participants | Number of women eligible: not reported
Number of participants randomised to treatment groups: 128 randomised
Number of post‐randomisation exclusions (not reported per group): 15 (4 stillbirth, 4 pre‐eclampsia, 2 premature labour, 2 caesarean sections, 3 ‘other’)
Number of women who remained in trial: A: 44 B: 44
Number of withdrawals (not reported per group): 25
Number of women analysed: A: 44; B: 44. Inclusion criteria: parity 0 or 1; maternal age 19 to 35; low medical risk; at least 12th grade education; father willing to attend prenatal classes; prospective parents living together; adequate English; living within 32 km of hospital; and assessment of mother and infant as eligible for early discharge (range of pre‐specified criteria). Characteristics of participants: no differences between groups on maternal age, race, father's occupation, planned pregnancy duration of marriage, time to conceive, maternal and paternal education, presence of another child at home, maternal preferences for infant feeding, prenatal education or natural childbirth; BUT no data given. |
|
| Interventions | A: (n = 44) discharge from 12 to 48 hours pp (12 were discharged later than 48 hours); median stay 26 hours, range = 12‐86 hours.
B: (n = 44) discharge at > 48 hours pp (5 discharged at < 48 hours); median stay = 68 hours, range = 31 to 167 hours. Co‐interventions: A: nursing staff intensively trained for early discharge; prospective parents in early group attended prenatal early discharge preparation classes; daily home visits through 4th day pp. B: received prenatal education; paediatric visit at 2 weeks pp; and an obstetric visit at 6 weeks. Duration of follow‐up: 6 weeks |
|
| Outcomes | Infant and maternal re‐admissions to 6 weeks pp. Maternal views about length of hospital stay. | |
| Notes | Highly selected study participants; cross‐over a problem. Dates of study: Not reported Funding sources: "Supported by Kaiser Foundation Research Institute, General Research Support, under a grant (5 501 RR05521‐10) from the US Public Health Service Declarations of interest: Not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information in the report to assess whether sequence generation was adequate. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible for mothers but unlikely to influence the outcome of hospital readmissions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear for outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 15/128 excluded for no longer meeting early discharge criteria, and 25/128 withdrew due to reasons unrelated to duration of hospital stay but the study authors do not report the numbers of exclusions and withdrawals per group. |
| Selective reporting (reporting bias) | Unclear risk | Not common practice to publish protocol at that time |
| Other bias | Low risk | Nothing to indicate any other source of bias |
C: control CHF: Swiss francs CS: caesarean section hrs: hours I: intervention min: minutes pp: postpartum RCT: randomised controlled trial SD: standard deviation
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Escobar 2001 | Women participating in this trial were randomised to home visits or hospital‐based group follow‐up visits after early obstetric discharge, i.e. randomisation was not used to compare early with longer length of stay. |
| Lieu 2000 | Women participating in this trial were randomised to home visits or hospital‐based group follow‐up visits after early obstetric discharge, i.e. randomisation was not used to compare early with longer length of stay. |
| Steel O'Connor 2003 | Women participating in this trial were randomised to public health nurse follow‐up or a screening telephone call after early obstetric discharge, i.e. randomisation was not used to compare early with longer length of stay. |
Characteristics of studies awaiting classification [ordered by study ID]
NCT04422041 2020.
| Methods | Randomised controlled trial Setting: Universidad Autonoma de Nuevo Leon, School of Medicine, Mexico |
| Participants | Recruitment target: 354 Inclusion criteria: healthy newborns that were born from vaginal delivery in primiparous or multiparous women where both the mother and the newborn were deemed as eligible for early discharge according to the American Association of Pediatrics criteria and by a clinical obstetric mother evaluation. Exclusion criteria: placenta praevia, abnormal bleeding during vaginal delivery (considered as greater than 500mL), inability to deambulate, medical complications from previous a previous pregnancy, 3rd or 4th degree perineal laceration as well as medical conditions that required any monitorization for more than 24 hours after delivery. |
| Interventions | Early discharge: Time to discharge less than 24 hours after birth Comparator: Discharge time between 24 and 48 hours after birth |
| Outcomes | Readmission to hospital: proportion of infants readmitted within 28 days Proportion of newborns who attended the emergency services within 28 days |
| Notes | Registered June 2020. Trial reported as having taken place from July 2016 to June 2018. No published results available. |
Characteristics of ongoing studies [ordered by study ID]
Namagembe 2014.
| Study name | Maternal outcome following discharge on 2nd versus 3rd day post caesarean section at Mulago Hospital |
| Methods | Parallel, 2 arm RCT. Setting: Kampala, Uganda Mothers who had uncomplicated Caesarean section, will be randomised after 24 hours after the operation and those who fall on the control group will be discharged after 72 hours |
| Participants | Recruitment target: 338 Inclusion criteria:
Exclusion criteria:
|
| Interventions | Group 1: day 2 discharge Group 2: day 3 discharge |
| Outcomes | Primary outcome: wound infection Secondary outcomes: postpartum haemorrhage, wound dehiscence, acceptability with the hospital discharge |
| Starting date | January 2014 |
| Contact information | Cecilia Thomas cecyliamasili@yahoo.com Imelda Namagembe namagime@gmail.com |
| Notes | Funding source: St Augustine University of Tanzania Study authors were contacted by email but the study authors did not reply |
Differences between protocol and review
We added in a search of ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform (ICTRP).
We made several changes to the outcomes for the review: maternal and infant mortality at 28 days and one year were added as secondary outcomes; we changed the secondary outcome 'women dissatisfied with their postnatal care' to 'women satisfied with their postnatal care' and the time points for 'Women scoring above the cut‐off score indicating probable depression on a well‐validated standardized instrument for measuring depression' was changed from six to eight weeks, three months and six months to within six months after the birth.
We also prespecified subgroup analyses for very early discharge (24 hours and under) and early discharge (48 hours and greater) and mode of birth (vaginal birth or caesarean section).
The certainty of evidence has been assessed using the GRADE approach and 'Summary of findings' tables have been added.
Contributions of authors
For the original review (2002): Stephanie Brown and Rhonda Small undertook the background review of the literature. Stephanie Brown wrote the protocol with input from all review authors. Brenda Argus and Ann Krastev conducted the original literature search to identify trials. Each review author independently evaluated trials for quality and extracted data. Rhonda Small, Brenda Argus and Ann Krastev independently entered the data. Stephanie Brown wrote the text of the review with input from the other review authors.
For the first update (2009): Stephanie Brown and Rhonda Small updated the literature search, independently reviewed new trials, extracted and entered data and updated the text of the review. Brenda Argus, Ann Krastev and Peter Davis reviewed the manuscript.
For this update (2021): Lynn Hampson (Cochrane Pregnancy and Childbirth Information Specialist) updated the literature search, all review authors updated the protocol and agreed the GRADE outcomes for the review update. Ellie Jones and Fiona Stewart independently assessed new trials and previously excluded studies, evaluated trials for risk of bas, extracted and entered data and performed data analyses. Beck Taylor assisted with resolving any disagreement with the data extraction and analysis process. Fiona Stewart and Ellie Jones wrote the text of the review with input from the other review authors Beck Taylor, Stephanie Brown and Peter Davis.
Sources of support
Internal sources
La Trobe University, Australia
Royal Women's Hospital, Melbourne, Australia
Murdoch Childrens Research Institute, Australia
External sources
No sources of support provided
Declarations of interest
Stephanie Brown: salary and project support from the Australian National Health and Medical Research Council.
Peter G Davis: salary and project support from the Australian National Health and Medical Research Council.
Beck Taylor: is supported by the UK National Institute for Health Research (NIHR) Applied Research Centre (ARC) West Midlands. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Fiona Stewart: none known
Eleanor Jones: is supported by the National Institute for Health Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Bayoumi 2016 {published data only}
- Bayoumi YA, Bassiouny YA, Hassan AA, Gouda HM, Zaki SS, Abdelrazek AA. Is there a difference in the maternal and neonatal outcomes between patients discharged after 24 h versus 72 h following cesarean section? A prospective randomized observational study on 2998 patients. Journal of Maternal-Fetal & Neonatal Medicine 2016;29(8):1339-43. [DOI] [PubMed] [Google Scholar]
Boulvain 2004 {published data only}
- Boulvain M, Perneger TV, Othenin-Girard V, Petrou S, Berner M, Irion O. Home-based versus hospital-based postnatal care: a randomised trial. BJOG: An International Journal of Obstetrics and Gynaecology 2004;111:807-13. [DOI] [PubMed] [Google Scholar]
- Petrou S, Boulvain M, Simon J, Maricot P, Borst F, Perneger T, et al. Home-based care after a shortened hospital stay versus hospital-based care postpartum: an economic evaluation. BJOG: An International Journal of Obstetrics and Gynaecology 2004;111:800-6. [DOI] [PubMed] [Google Scholar]
Brooten 1994 {published data only}
- Brooten D, Knapp H, Borucki L, Jacobsen B, Finkler S, Arnold L, et al. Early discharge and home care after unplanned cesarean birth: nursing care time. Journal of Obstetric, Gynecologic and Neonatal Nursing 1996;25(7):595-600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooten D, Roncoli M, Finkler S, Arnold L, Cohen A, Mennuti M. A randomized trial of early hospital discharge and home follow-up of women having caesarean birth. Obstetrics & Gynecology 1994;84(5):832-8. [PMC free article] [PubMed] [Google Scholar]
Burnell 1982 {published data only}
- Burnell I, McCarthy M, Chamberlain GVP, Hawkins DF, Elbourne DR. Patient preference and postnatal hospital stay. Journal of Obstetrics and Gynaecology 1982;3:43-7. [Google Scholar]
Carty 1990 {published data only}
- Carty E, Bradley C. A randomized, controlled evaluation of early postpartum hospital discharge. Birth 1990;17(4):199-204. [DOI] [PubMed] [Google Scholar]
- Carty EM, Bradley CF. A randomized, controlled evaluation of early postpartum hospital discharge. Breastfeeding Review 1991;2(4):168-72. [DOI] [PubMed] [Google Scholar]
Chiong 2012 {published data only}
- Chiong Tan P, ISRCTN27523895. Hospital discharge on the first versus second day after planned cesarean delivery: a randomized trial. isrctn.com/ISRCTN27523895 (first received 6 June 2012).
- Chiong Tan P, Jin M, Zawiah S. Hospital discharge on the first compared with the second day after a planned cesarean delivery: A randomized controlled trial. Obstetrics and Gynecology 2012;120(6):1273-82. [DOI] [PubMed] [Google Scholar]
Gagnon 1997 {published data only}
- Gagnon A, Edgar L, Kramer M, Papageorgiou A, Waghorn K, Klein M. A randomized trial of a program of early postpartum discharge with nurse visitation. American Journal of Obstetrics and Gynecology 1997;176(1):205-11. [DOI] [PubMed] [Google Scholar]
Hellman 1962 {published data only}
- Hellman LM, Kohl SG. Early hospital discharge in obstetrics. Lancet 1962;1:227-33. [DOI] [PubMed] [Google Scholar]
Kruse 2021 {unpublished data only}
- Kruse A, NCT02911727. Fast-track discharge after elective cesarean section. clinicaltrials.gov/ct2/show/NCT02911727 (first received 22 September 2016).
- Kruse AR, Lauszus FF, Forman A, Kesmodel US, Rugaard MB, Knudsen RK, et al. Effect of early discharge after planned cesarean section on recovery and parental sense of security. A randomized clinical trial. Acta Obstetricia et Gynecologica Scandinavica 2021 May;100(5):955-63. [CENTRAL: CN-02201592] [EMBASE: 633406706] [PMID: ] [DOI] [PubMed] [Google Scholar]
McKeever 2002 {published data only}
- McKeever P, Stevens B, Miller K-L, MacDonell KW, Gibbins S, Guerriere D, et al. Home versus hospital breastfeeding support for newborns: a randomized controlled trial. Birth 2002;29(4):258-65. [DOI] [PubMed] [Google Scholar]
- Stevens B, McKeever P, Coyte P, Daub S, Dunn M, Gibbins S, et al. The impact of home versus hospital support of breastfeeding on neonatal outcomes [abstract]. Pediatric Research 2001;49 Suppl(4):261A. [Google Scholar]
Sainz Bueno 2005 {published data only}
- Sainz Bueno JA, Romano MR, Teruel RG, Benjumea AG, Palacin AF, Gonzalez CA, et al. Early discharge from obstetrics-pediatrics at the Hospital de Valme, with domiciliary follow-up. American Journal of Obstetrics and Gynecology 2005;193(3 Pt 1):714-26. [DOI] [PubMed] [Google Scholar]
Smith‐Hanrahan 1995 {published data only}
- Smith-Hanrahan C, Deblois D. Postpartum early discharge: impact of maternal fatigue and functional ability. Clinical Nursing Research 1995;4(1):50-66. [DOI] [PubMed] [Google Scholar]
Taiba 2012 {published data only}
- Taiba JMM, Begum K. Outcome of early discharge of lower uterine caesarean section patients from hospital-a randomized clinical trial. International Journal of Gynecology and Obstetrics 2012;119(Suppl 3):S607. [Google Scholar]
Thompson 1999 {published data only}
- Thompson JF, Roberts CL, Ellwood DA. Early discharge after childbirth: too late for a randomised controlled trial. Birth 1999;26(3):192-5. [DOI] [PubMed] [Google Scholar]
Waldenström 1987 {published data only}
- Waldenström U, Lindmark G. Early and late discharge after hospital birth. A comparative study of parental background characteristics. Scandinavian Journal of Social Medicine 1987;15:159-67. [DOI] [PubMed] [Google Scholar]
- Waldenström U, Sundelin C, Lindmark G. Early and late discharge after hospital birth. Health of mother and infant in the postpartum period. Uppsala Journal of Medical Sciences 1987;92:301-14. [DOI] [PubMed] [Google Scholar]
- Waldenström U, Sundelin C, Lindmark G. Early and late discharge after hospital birth: breastfeeding. Acta Paediatrica Scandinavica 1987;76:727-32. [DOI] [PubMed] [Google Scholar]
- Waldenström U. Early and late discharge after hospital birth: fatigue and emotional reactions in the postpartum period. Journal of Psychosomatic Obstetrics and Gynaecology 1988a;8:127-35. [Google Scholar]
- Waldenström U. Early and late discharge: fathers' involvement in infant care. Early Human Development 1988;17:19-28. [DOI] [PubMed] [Google Scholar]
- Waldenström U. Early discharge with domiciliary visits and hospital care. Scandinavian Journal of Caring Sciences 1987;1:51-8. [DOI] [PubMed] [Google Scholar]
Winterburn 2000 {published data only}
- Winterburn S, Fraser R. Does the duration of postnatal stay influence breast-feeding rates at one month in women giving birth for the first time? A randomized control trial. Journal of Advanced Nursing 2000;32(5):1152-7. [DOI] [PubMed] [Google Scholar]
Yanover 1976 {published data only}
- Yanover MJ, Jones D, Miller MD. Perinatal care of low-risk mothers and infants. Early discharge with home care. New England Journal of Medicine 1976;294(13):702-5. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Escobar 2001 {published data only}
- Escobar G, Braveman P, Ackerson L, Odouli R, Coleman-Phox K, Lieu T. Home visits vs. hospital-based group follow-up visits after early postpartum discharge [abstract no: 1111]. In: Pediatric Academic Societies Annual Meeting; 2001 April 28-May 1; Baltimore, USA. 2001. [DOI] [PubMed]
- Escobar GJ, Braveman PA, Ackerson L, Odouli R, Coleman-Phox K, Capra AM, et al. A randomized comparison of home visits and hospital-based group follow-up visits after early postpartum discharge. Pediatrics 2001;108:719-27. [DOI] [PubMed] [Google Scholar]
Lieu 2000 {published data only}
- Lieu TA, Braveman PA, Escobar GJ, Fischer AF, Jensvold NG, Capra AM. A randomized comparison of home and clinic follow-up visits after early postpartum hospital discharge. Pediatrics 2000;105:1058-65. [DOI] [PubMed] [Google Scholar]
Steel O'Connor 2003 {published data only}
- Steel O'Connor KO, Mowat DL, Scott HM, Carr PA, Dorland JL, Young Tai KF. A randomized trial of two public health nurse follow-up programs after early obstetrical discharge: an examination of breastfeeding rates, maternal confidence and utilization and costs of health services. Canadian Journal of Public Health. Revue Canadienne de Sante Publique 2003;94(2):98-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
NCT04422041 2020 {published data only}
- NCT04422041. Comparison of early versus very early postnatal discharge on hospital readmissions in newborns [Comparison of early versus very early postnatal discharge on hospital readmissions in newborns: a prospective study]. Https://clinicaltrials.gov/show/NCT04422041 (first received 2020 Jun 9). [CENTRAL: CN-02118712]
References to ongoing studies
Namagembe 2014 {published data only}
- Namagembe I, PACTR201404000786372. Maternal outcome following discharge on 2nd versus 3rd day post caesarean section at Mulago hospital. https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=786 (first received 8 March 2014).
Additional references
Beck 1991
- Beck C. Early postpartum discharge programs in the United States: a literature review and critique. Women and Health 1991;17(1):125-38. [DOI] [PubMed] [Google Scholar]
Benahmed 2017
- Benahmed N, San Miguel L, Devos C, Fairon N, Christiaens W. Vaginal delivery: How does early discharge affect mother and child outcomes? A systematic literature review. BMC Pregnancy and Childbirth 2017;17(1):289. [DOI] [PMC free article] [PubMed] [Google Scholar]
Braveman 1995
- Braveman P, Egeter S, Pearly M, Marchi K, Miller C. Early discharge of newborns and mothers: a critical review of the literature. Pediatrics 1995;96:716-26. [PubMed] [Google Scholar]
Britton 1994
- Britton J, Britton H, Beebe S. Early discharge of the term newborn: a continuing dilemma. Pediatrics 1994;94:291-5. [PubMed] [Google Scholar]
Brown 2004
- Brown S, Bruinsma F, Darcy M-A, Small R, Lumley J. Early discharge: no evidence of adverse outcomes in three consecutive population-based Australian surveys of recent mothers conducted in 1989, 1994 and 2000. Paediatric and Perinatal Epidemiology 2004;18:202-13. [DOI] [PubMed] [Google Scholar]
Campbell 2016
- Campbell O, Cegolon L, MacLeod D, Benova L. Length of stay after childbirth: compilation of reported data and a cross-sectional analysis from nationally representative surveys. PLoS Medicine 2016;13(3):e1001972. [DOI] [PMC free article] [PubMed] [Google Scholar]
Care Quality Commisson 2017
- Care Quality Commission. Survey of women's experiences of maternity care (2017). Available from www.cqc.org.uk/sites/default/files/20180130_mat17_statisticalrelease.pdf.
Catz 1995
- Catz C, Hanson JW, Simpson L, Yaffe SJ. Summary of a workshop: early discharge and neonatal hyperbilirubinemia. Pediatrics 1995;96:743-5. [PubMed] [Google Scholar]
CETS 1997
- Conseil d'évaluation des technologies de la santé du Québec. Evaluation of the risks and benefits of early postpartum discharge. Report submitted to the Minister of Health and Social Services of Québec, Canada. Québec: CETS, 1997. [Google Scholar]
Danielson 2000
- Danielson B, Castles AG, Damberg CL, Gould JB. Newborn discharge timing and readmissions: California, 1992-1995. Journal of Pediatrics 2000;106:31-9. [DOI] [PubMed] [Google Scholar]
Day 1997
- Day P, Lancaster P, Huang J. Australia's Mothers and Babies 1995. Sydney: Australian Institute of Health and Welfare National Perinatal Statistics Unit, 1997. [Google Scholar]
Declerq 1997
- Declerq E, Simmes D. The politics of 'drive-through deliveries': putting early postpartum discharge on the legislative agenda. Milbank Quarterly 1997;75:172-202. [DOI] [PMC free article] [PubMed] [Google Scholar]
Edmonson 1997
- Edmonson MB, Stoddard JJ, Owens LM. Hospital readmission with feeding-related problems after early postpartum discharge of normal newborns. JAMA 1997;278:299-303. [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Hamilton, Ontario, Canada: McMaster University (developed by Evidence Prime), 2016. Available from gradepro.org.
Grullon 1997
- Grullon KE, Grimes D. The safety of early postpartum discharge: a review and critique. Obstetrics & Gynecology 1997;90:860-5. [DOI] [PubMed] [Google Scholar]
Gupta 2006
- Gupta P, Malhotra S, Singh DK, Dua T. Length of postnatal stay in healthy newborns and re-hospitalisation following their early discharge. Indian Journal of Pediatrics 2006;73:897-900. [DOI] [PubMed] [Google Scholar]
Harron 2017
- Harron K, Gilbert R, Crowell D, Oddie S, Meulen J. Newborn length of stay and risk of readmission. Paediatric and Perinatal Epidemiology 2017;31(3):221-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Heck 2003
- Heck K, Schoendorf KC, Chavez GF, Braveman P. Does postpartum length of stay affect breastfeeding duration? A population-based study. Birth 2003;30:153-9. [DOI] [PubMed] [Google Scholar]
Higgins 2019
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Available from www.cochrane-handbook.org.
Jones 2020
- Jones, E, Taylor B, MacArthur C, Bradshaw S, Hope L, Cummins, C. Early Postnatal Discharge for Infants: A Meta-analysis. . Pediatrics September 2020;146 (3):e20193365. [DOI] [PubMed] [Google Scholar]
Kotagol 1999
- Kotagol UR, Atherton HD, Eshett R, Schoettker PJ, Perstein PH. Safety of early discharge for Medicaid newborns. JAMA 1999;282(12):1150-6. [DOI] [PubMed] [Google Scholar]
Lain 2014
- Lain S, Roberts C, Bowen J, Naggar N. Trends in New South Wales infant hospital readmission rates in the first year of life: a population‐based study. Medical Journal of Australia 2014;201(1):40-3. [DOI] [PubMed] [Google Scholar]
Lain 2015
- Lain SJ, Robets CL, Bowen JR, Nassar N. Early discharge of infants and risk of readmissions for jaundice. Journal of Pediatrics 2015;135(2):314-21. [DOI] [PubMed] [Google Scholar]
Lansky 2006
- Lansky A, Barfield WD, Marchi KS, Egerter SA, Galbraith AA, Braveman PA. Early postnatal care among healthy newborns in 19 states: pregnancy risk assessment monitoring system, 2000. Maternal and Child Health Journal 2006;10:277-84. [DOI] [PubMed] [Google Scholar]
Liu 1997
- Liu LL, Clemens CJ, Shay DK, Davis RL, Novack AH. The safety of newborn early discharge. The Washington State experience. JAMA 1997;278:293-8. [PubMed] [Google Scholar]
Liu 2000
- Liu S, Wen SW, McMillan D, Trouton K, Fowler D, McCourt C. Increased neonatal readmission rate associated with decreased length of hospital stay at birth in Canada. Canadian Journal of Public Health 2000;91:46-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
MacArthur 2002
- MacArthur C, Winter HR, Bick DE, Knowles H, Lilford R, Henderson C, et al. Effects of redesigned community postnatal care on women's health 4 months after birth: a cluster randomised controlled trial. Lancet 2002;359:378-85. [DOI] [PubMed] [Google Scholar]
MacGregor 2020
- MacGregor R, Hillman S, Bick D. Falling through the cracks: the impact of COVID-19 on postnatal care in primary care.. British Journal of General Practice 26 November 2020;70:578-579. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maisels 1995
- Maisels MJ, Newman TB. Kernicterus in otherwise healthy, breast-fed newborns. Pediatrics 1995;96:730-3. [PubMed] [Google Scholar]
Malkin 2000
- Malkin JD, Garber S, Broder MS, Keeler E. Infant mortality and early postpartum discharge. Obstetrics & Gynecology 2000;96:183-8. [DOI] [PubMed] [Google Scholar]
Mandl 1997
- Mandl KD, Brennan TA, Wise PH, Tronick EZ, Homer CJ. Maternal and infant health - Effects of moderate reductions in postpartum length of stay. Archives of Pediatrics & Adolescent Medicine 1997;151(9):915-21. [DOI] [PubMed] [Google Scholar]
Margolis 1995
- Margolis LH. A critical review of studies of newborn discharge timing. Clinical Pediatrics 1995;34:626-34. [DOI] [PubMed] [Google Scholar]
NHS Digital 2019
- UK National Health Service (NHS) Digital. NHS Maternity Statistics (31 October 2019). Available from digital.nhs.uk/data-and-information/publications/statistical/nhs-maternity-statistics/2018-19.
Norr 1987
- Norr KF, Nacion K. Outcomes of postpartum early discharge 1960-1986. A comparative review. Birth 1987;14:135-41. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rush 1989
- Rush J, Chalmers I, Enkin M. Care of the new mother and baby. In: Chalmers I, Enkin M, Keirse MJNC, editors(s). Effective Care in Pregnancy and Childbirth. Oxford: Oxford University Press, 1989:1341-4. [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.gradepro.org/app/handbook/handbook.html.
Waldenström 2004
- Waldenström U, Aarts C. Duration of breastfeeding and breastfeeding problems in relation to postpartum stay: a longitudinal cohort study of a national Swedish sample. Acta Paediatrica 2004;93:669-76. [PubMed] [Google Scholar]
World Health Organization 2013
- United Nations Children’s Fund. Accountability for maternal, newborn and child survival. Geneva: World Health Organization, 2013. [Google Scholar]
References to other published versions of this review
Brown 2002
- Brown S, Small R, Argus B, Davis PG, Krastev A. Early postnatal discharge from hospital for healthy mothers and term infants. Cochrane Database of Systematic Reviews 2002, Issue 3. Art. No: CD002958. [DOI: 10.1002/14651858.CD002958] [DOI] [PubMed] [Google Scholar]