

Abstract
Aim
The aim of this study was to assess the effectiveness of listening to music or Quran in reducing cancer patients’ anxiety before chemotherapy administration. Reducing anxiety in people with cancer, prior to chemotherapy administration, is a crucial goal in nursing care.
Design
An experimental comparative study was conducted.
Methods
A simple randomization sampling method was applied. Two hundred thirty‐eight people with cancer who underwent chemotherapy were participated. They are assigned as Quran, music and control groups.
Results
The overall score of Arabic State Anxiety Inventory in all groups revealed that there was a significant difference between pre‐test and post‐test among participants. Listening to Quran or music reduced the chemotherapy‐induced anxiety. There was no difference between these two ways to reduce anxiety in people with cancer. Listening to Quran or music can be added in nursing care plans prior chemotherapy administrations to reduce cancer patients’ anxiety.
Keywords: anxiety, cancer, chemotherapy, music, quran
1. INTRODUCTION
Cancer is still the main health problem worldwide and one of the highest leading cause of death around the world (National Cancer Institute, 2018; Siegel et al., 2019). Over the past 10 years, the prevalence of cancer has been increased in the Middle East, especially in Iraq (Behadili et al., 2019; Iraqi Cancer Board, 2018). Although many studies have been done regarding cancer, it remains a public health problem that needs to be considered by researchers (Siegel et al., 2019). One of the main treatments for cancer is chemotherapy (American Cancer Society, 2019; National Cancer Institute, 2015). This treatment makes a lot of side effects, which can increase anxiety (Lin et al., 2011; Williams & Hopper, 2015). Anxiety is defined as “an emotion characterized by feelings of tension, worried thoughts and physical changes” (American Psychological Association, n.d. a, para,1). Cancer itself and its treatment both have negative effects on emotional status and make anxiety (Chien et al., 2014; Hosseini et al., 2016; Karagozoglu et al., 2013; Vanbockstael et al., 2016; Williams & Hopper, 2015). The prevalence of chemotherapy‐induced anxiety is 15.38% in patients who receive chemotherapy (Pandey et al., 2006).
In addition, anxiety is one of the complications that people with cancer may face before chemotherapy (Charalambous et al., 2015). A high level of anxiety can put the people with cancer under the risk of some immunological problems, impairment in quality of life and functional loss (Bilgiç & Acaroğlu, 2017; Ghiasi & Keramat, 2018; Moons & Shields, 2015; Spilioti et al., 2017). On the other hand, immunity disturbance is one of the main side effects of chemotherapy (Heydarzadeh et al., 2020). Anxiety during chemotherapy increases patients’ heart rate, respiratory rate and blood pressure as a result of releasing noradrenaline and adrenaline hormones (Cameron et al., 2016; Lin et al., 2011). Moreover, chemotherapy‐induced anxiety can increase the side effects of chemotherapy after administration (Lin et al., 2011; Vichaya et al., 2015). Indeed, anxiety not only affects the patients’ emotional status, but also the effectiveness of chemotherapy (Garcia, 2014) and the duration of hospitalization (Mirbagher Ajorpaz & Aghajani, 2011). Furthermore, some studies declared that anxiety increases patients’ nausea and vomiting before and after chemotherapy (Dadkhah et al., 2019). Therefore, reducing cancer patients’ anxiety before chemotherapy administration minimizes the possible side effects of chemotherapy and increases the efficiency of treatment. In fact, nursing care is a holistic approach that aims to guarantee the comfort of patients (Kim and Kwon, 2007). Reducing anxiety in people with cancer can enhance patients’ comfort and minimize patients’ problems.
There are many techniques such as spiritual care, music therapy, verbal relaxation, progressive muscle relaxation or guided imagery that have been studied to reduce chemotherapy‐induced anxiety (Charalambous et al., 2015; Lin et al., 2011; Moeini et al., 2014). American Music Therapy Association (n.d.) has defined music therapy as “the clinical and evidence‐based use of music interventions to accomplish individualized goals within a therapeutic relationship by a credentialed professional who has completed an approved music therapy program” (“What is Music Therapy?” section). Listening to music can help raise the patients’ relaxation by positive impacts on neurophysiological and emotional responses (Novotney, 2013). On the other hand, “spirituality is distinguished from all other things—humanism, values, morals, and mental health—by its connection to that which is sacred” (Koenig et al., 2012, p.3). Quran recitation, as a religious faith, can be used in a way of the spiritual therapy (Dein et al., 2010; Koenig, 2012).
2. BACKGROUND
Music has been demonstrated to be an effective technique to reduce anxiety in patients undergoing chemotherapy (Bilgiç & Acaroğlu, 2017; Jasemi et al., 2016; Karagozoglu et al., 2013; Lin et al., 2011; Nightingale et al., 2013; Spilioti et al., 2017). Spiritual care is another effective technique that can be used to reduce chemotherapy‐induced anxiety, and some studies assessed the effect of listening to the Quran as a spiritual technique to reduce anxiety in people with different types of cancer (Ghiasi & Keramat, 2018; Moeini et al., 2014; Sulistyawati & Probosuseno, 2019). Although these mentioned studies have demonstrated that the music and spiritual techniques to decrease chemotherapy‐induced anxiety, there is no study that has assessed which technique is more effective. In this study, these two techniques were compared to assess their effectiveness in reducing cancer patients’ anxiety before chemotherapy administration.
As almost 99% of Iraqis are Muslims (Iraqi Minorities and Council, 2015), recitation of Quran was chosen in this study to be a spiritual care to reduce chemotherapy‐induced anxiety in people with cancer. Music is the other technique that has been chosen in this study to reduce anxiety in people with cancer who are under chemotherapy. Music was chosen as not all Muslims are religious. In this study, the researchers aimed to determine the effect of listening to Quran or music in order to reduce chemotherapy‐induced anxiety in people with cancer. Also, the researchers hypothesized that:
. Listening to Quran or music will reduce the anxiety level prior to chemotherapy sessions in people with cancer.
. Listening to Quran will be more effective in reducing chemotherapy‐induced anxiety in people with cancer than listening to music.
. Demographics such as age, gender, educational level and marital status will play significant roles in the levels of chemotherapy‐induced anxiety in all groups (control, Quran and music).
3. METHODOLOGY
3.1. Design
An experimental comparative design was done to assess the effectiveness of Quran and music in reducing chemotherapy‐induced anxiety in people with cancer. Spiritual care (recitation of Quran) and music are the independent variables in this study, and the dependent variable is anxiety.
3.2. Method
In order to maintain a transparent and scientific‐based randomization process, simple randomization was used in assigning participants (individuals: people with cancer) to Quran, music and control groups assuming that each participant has an equal chance of being assigned to any group. The randomization procedure involved choosing a number from a sealed envelope that contained two numbers: one and two (1 was in the control group and 2 was in the intervention group). Then, in order to allocate the patients in Quran and music groups, another sealed envelope that contains two numbers (1 was in spiritual therapy [recitation of Quran] and 2 was in music) was given to the patients who were allocated in the intervention group in the previous step. Indeed, three groups were allocated randomly. The blind method was assured as patients were not aware that listening to music or Quran may reduce their chemotherapy‐induced anxiety. This was important as patients may indoctrinate themselves to reduce the anxiety level, which may affect the results in this study. Thus, a single‐blind method was applied in order to prevent possible biases. On the other hand, all the steps of data collection were done by two of the researchers who were trained to collect the data.
Lin et al. (2011) determined that the effect size of anxiety reduction in a group of people with cancer was 0.55. In this study, the minimum sample size for each group would be 28 as calculated based on the confidence level of 80% and a 5% margin of error (Cohen et al., 2013). Regarding the inclusion criteria, all adult Muslim patients who have been diagnosed with cancer and admitted to hospitals for inpatient chemotherapy were included in the study. Adult patients above 18 (male and female) who were scheduled to receive their chemotherapy were included in this study. Concerning the exclusion criteria, patients with lower than sixth‐grade educational level were excluded as American Psychological Association (n.d. b) suggested that the State Anxiety Inventory (STAI) is not suitable for those who have not passed the sixth grade. Non‐Muslim patients were excluded. Also, patients who do not know their medical diagnosis, have mental illnesses, are blind or deaf, or undergoing radiotherapy were excluded from the study sample. Furthermore, participants were excluded if they could not complete the session of spiritual or music before the administration of chemotherapy. The total sample of 238 patients were eligible, and they agreed to participate in the study. However, 79 were excluded from the study based on the mentioned reasons of exclusion criteria. The final number of 159 patients with the inclusion criteria was randomly assigned to the intervention and control groups. Study flow diagram is shown in Figure 1 explaining the recruitment and allocation to study groups.
FIGURE 1.
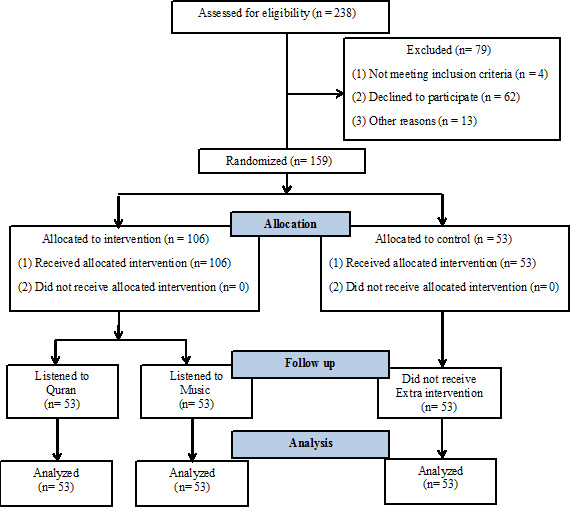
Clinical trial flow diagram
3.2.1. Instrumentation
Many studies have been used State Anxiety Inventory (STAI) for Adults to assess the level of anxiety before diagnostic or treatment procedures (Babamohamadi et al., 2015; Ganjou & Akbari, 2013; Lin et al., 2011; Massimiliani et al., 2017; Mirbagher Ajorpaz and Aghajani, 2011; Mirsane et al., 2016). STAI is a valid and reliable tool that was developed by Spielberger et al. (1983) with a range from 0.86–0.95 of internal consistency coefficients. This scale consists of 40 questions in two parts: Form Y‐1 (to assess state anxiety) and Form Y‐2 (to assess trait anxiety). The items are rated on a 4‐point scale (Not at all, Somewhat, Moderately so and Very much so). The total point ranges from 40–160. A high score indicates a high level of anxiety.
As the study sample in this study speaks Arabic, the questionnaire was in Arabic language. The questionnaire consists of demographics and the Arabic version of STAI. The Arabic version of STAI has the same number of items and the same rating scale as the original one has. Bahammam (2016) evaluated the validity and reliability of the Arabic version of STAI to be used in Arabic‐speaking population. Bahammam (2016) found that the Arabic version of STAI has adequate convergent and criterion validity, and it is reliable with Cronbach's alpha value of 0.989. In the current study, the Arabic version of STAI was used to assess the state anxiety and trait anxiety in people with cancer before chemotherapy administration. The permission to use the tool was sought and received via email. The demographics include patients’ age, gender, marital status, level of education, number of chemotherapy prior the survey and days interval for hospital entries to take chemotherapy.
3.2.2. Setting and data collection
Five hospitals in Baghdad that are the main hospitals to treat people with cancer were included as the settings in this study. Indeed, people with cancer from different cities in Iraq are admitted to these hospitals in order to receive chemotherapy. In fact, not all the five hospitals agreed to conduct the study. The administrators in three hospitals refused to sign the approval letter to collect the data. However, in two hospitals (Al‐Kadhumain Teaching Hospital and Oncology Teaching Hospital), the approval letters were officially signed by the administrators to collect the data. The researchers collected the data in those two hospitals. A total of 238 patients were agreed to participate in the study. The data collection started from 2 June 2020 till 30 July 2020. A pre‐test and post‐test method was used to collect the data. Before the chemotherapy administration, participants were given the questionnaire to fill in order to assess their anxiety. Filling the survey took about 8–15 min by each participant. Then, each participant in the intervention groups was given an MP3 device and a headphone to listen to Quran (Surah Yaseen in verse 22 with the voice of Mishary Rashid Al‐Efasy) or music (Monamour by Heron Borelli) for 20 min. After 10 min, the questionnaire was given again to the participants to be filled in order to assess their anxiety again. For the control group, no interventions were done, and the duration between the pre‐test and post‐test was 30 min. All the data collection process was done before the administration of chemotherapy. Participants were excluded if they receive chemotherapy during the process of data collection.
3.2.3. Analysis of data
The data were analysed using Statistical Package for the Social Sciences (SPSS) MAC version 23.0.0.2. Pre‐test characteristics of the groups were examined using one‐way analysis of variance ANOVA and chi‐square. The paired t test was used to compare the mean differences in levels of anxiety (STAI).
Two‐way repeated‐measures analysis of variance (ANOVA) was used to compare differences between the groups and characteristics of participants for changes in level of anxiety. The effects were tested by examining the interaction effect, using partial eta‐squared (η2) values as a measure of group‐by‐time effect size. For this analysis, the data were normalized using the log transformation (Feng et al., 2014). The strength of eta‐squared values was interpreted as 0.01 being a small effect, 0.06 a moderate effect and 0.14 a large effect (Cohen, 1988). A t test with Tukey's honestly significant difference was employed to examine the mean difference between groups and level of anxiety. The level of significance was set at p <.05.
3.3. Ethics
The study protocol was approved by the Institutional Review Board (IRB) in the College of Nursing at University of Baghdad. Also, approvals were obtained from two hospitals (Al‐Kadhumain Teaching Hospital and Oncology Teaching Hospital) to collect the data. Signing the approval letters by the administrators was not an easy process. Three hospitals did not agree to be settings for this study. Indeed, patients’ privacy and safety were the main aspects that the hospital administrators concern about. However, ensuring patients’ privacy and safety are mentioned in the informed consent. The written informed consent was given to the participants to be signed in order to get their agreements to voluntarily participate in this study. The oral consent was taken from those patients who wished to participate in this study but did not want to sign the informed consent. Adequate information about using the MP3 player, headphone and filling the questionnaire and duration of therapy were explained to the participants in the study groups. Also, the participants had the right to refuse participation or withdraw from the study at any time they wish without any consequences. Moreover, patients’ privacy was maintained throughout the research process by assuring anonymity and not getting personal information.
This study was done in compliance with the Declaration of Helsinki, and the protocol was approved by the Iranian Registry of Clinical Trials (IRCT20200429047244N1).
4. RESULTS
Two hundred thirty‐eight patients agreed to participate in this study. Seventy‐nine patients withdrew during the process of data collection because of going to do diagnostic procedures (e.g., X‐ray) or personal needs (e.g., toileting). Some were excluded as the chemotherapy administration started during the data collection process. The total of 159 patients was included in the data analysis. Based on the randomization technique that has been mentioned in the methodology, the study sample was divided into three groups: 53 patients in the control group, 53 in spiritual therapy and 53 in music. Regarding demographic information, 52.8% of the study sample were male. Nearly, half of the study sample (49.1%) were high school graduates, and most of the patients (64.2%) were married. The mean of participants’ age was 45.9 (SD: 14.06) years. Regarding patients’ diagnoses, 19.5%, 18.9%, 13.2%, 10.7%, 10.1%, 10.1%, 8.8% and 8.8% were breast cancer, leukaemia, cancer of prostate, non‐Hodgkin lymphoma, multiple myeloma, cancer of the pancreas, Hodgkin's lymphoma and cancer of the liver, respectively. The mean number of chemotherapy sessions, received by patients, was 9.46 (SD: 6.2) times since patients’ diagnosis with a mean of 33.49 (SD: 25.5) days’ interval for hospital entries. The demographics based on each group are shown in Table 1. This table also shows that there were no significant differences between the three groups in the assessed characteristics (age, chemotherapy sessions, hospital entry days’ interval, diagnosis, gender, marital status and educational levels).
TABLE 1.
Pre‐test characteristics of the groups of participants (total, control, Quran and music)
| Total (n = 159) | Control (n = 53) | Quran (n = 53) | Music (n = 53) | p‐value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | ANOVA |
| Age | 45.91 | 14.1 | 47.17 | 15.1 | 47.13 | 13.1 | 43.42 | 13.9 | .289 |
| Hospital entry days’ interval | 33.49 | 25.5 | 31.62 | 25.4 | 32.62 | 25.2 | 36.23 | 26.2 | .624 |
| Chemotherapy sessions | 9.46 | 6.2 | 10.15 | 7.05 | 8.38 | 6.16 | 9.89 | 5.57 | .296 |
| Diagnosis | n | (%) | n | (%) | n | (%) | n | (%) | Chi‐square |
|---|---|---|---|---|---|---|---|---|---|
| Hodgkin lymphoma | 14 | 8.8 | 4 | 7.5 | 3 | 5.7 | 7 | 13.2 | 0.918 |
| Non‐Hodgkin lymphoma | 17 | 10.7 | 7 | 13.2 | 6 | 11.3 | 4 | 7.5 | |
| Multiple myeloma | 16 | 10.1 | 6 | 11.3 | 8 | 15.1 | 2 | 3.8 | |
| Ca liver | 14 | 8.8 | 4 | 7.5 | 5 | 9.4 | 5 | 9.4 | |
| Ca breast | 31 | 19.5 | 10 | 18.9 | 11 | 20.8 | 10 | 18.9 | |
| Ca prostate | 21 | 13.2 | 7 | 13.2 | 6 | 11.3 | 8 | 15.1 | |
| Ca pancreas | 16 | 10.1 | 6 | 11.3 | 5 | 9.4 | 5 | 9.4 | |
| Leukaemia | 30 | 18.9 | 9 | 17 | 9 | 17 | 12 | 22.6 | |
| Gender | |||||||||
| Male | 84 | 52.8 | 27 | 50.9 | 26 | 49.1 | 31 | 58.5 | 0.589 |
| Female | 75 | 47.2 | 26 | 49.1 | 27 | 50.9 | 22 | 41.5 | |
| Marital status | |||||||||
| Single | 26 | 16.4 | 6 | 11.3 | 7 | 13.2 | 13 | 24.5 | 0.518 |
| Married | 102 | 64.2 | 38 | 71.7 | 33 | 62.3 | 31 | 58.5 | |
| Divorced | 9 | 5.7 | 2 | 3.8 | 5 | 9.4 | 2 | 3.8 | |
| Separated | 2 | 1.3 | 1 | 1.9 | 1 | 1.9 | 0 | 0 | |
| Widow | 20 | 12.6 | 6 | 11.3 | 7 | 13.2 | 7 | 13.2 | |
| Educational status | |||||||||
| Primary school graduate | 25 | 15.7 | 13 | 24.5 | 6 | 11.3 | 6 | 11.3 | 0.184 |
| Middle school graduate | 20 | 12.6 | 3 | 5.7 | 10 | 18.9 | 7 | 13.2 | |
| High school graduate | 78 | 49.1 | 26 | 49.1 | 23 | 43.4 | 29 | 54.7 | |
| Bachelor degree | 36 | 22.6 | 11 | 20.8 | 14 | 26.4 | 11 | 20.8 | |
The result of the study, as shown in Table 2, revealed that, in the pre‐test assessment, the mean Arabic‐STAI score for all groups was 111.13 (SD: 11.12). In the post‐test assessment, the mean Arabic‐STAI score for all groups was 92.84 (SD: 14.13). Regarding the overall score of Arabic‐STAI in all groups, the results indicated that there was a significant difference (t = 14.93, p = .000) between pre‐test and post‐test among participants. In all groups, the level of anxiety has been reduced (control, t = 3.500, p =.001; Quran, t = 13.125, p = .000; music, t = 14.714, p = .000).
TABLE 2.
Level of anxiety by groups over time
| Measure | Paired t test | Two‐way analysis of variance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | t | p‐value | F | p‐value | η2 | ||||
| Level of Anxiety (STAI) | Control | Pre‐test | 106.17 | 13.177 | 3.500 | .001 | Time | 357.25 | .000 | 0.708 |
| Post‐test | 101.81 | 15.466 | Time × Group | 50.597 | .000 | 0.408 | ||||
| Group | 12.957 | .000 | 0.150 | |||||||
| Quran | Pre‐test | 113.38 | 9.083 | 13.125 | .000 | |||||
| Post‐test | 88.23 | 12.485 | ||||||||
| Music | Pre‐test | 113.85 | 9.075 | 14.714 | .000 | |||||
| Post‐test | 88.51 | 9.462 | ||||||||
At pre‐test, there was a significant difference in mean scores between groups (F = 6.363, p = .002). Significant differences in mean scores were found in pairs control and Quran (p =.002) besides control and music (p =.001). No significant differences were found in the mean score of Quran and music (p =.972) as shown in Table 3. In the post‐test, the mean level of anxiety had significantly decreased in the all groups: control (p =.001), Quran (p =.000) and music (p =.000) as shown in Table 2.
TABLE 3.
Level of anxiety by mean differences in groups
| Measure | (I) Group | (J) Group | Mean differences (I‐J) | Standard error | p‐value |
|---|---|---|---|---|---|
| Level of Anxiety (STAI) | Control | Quran | 6.78 a | 1.480 | .000 |
| Music | 6.33 a | 1.467 | .000 | ||
| Quran | Control | −6.78 a | 1.480 | .000 | |
| Music | −0.44 | 1.428 | .948 | ||
| Music | Control | −6.33 a | 1.467 | .000 | |
| Quran | 0.44 | 1.428 | .948 |
The mean difference is significant at the level.
The results of the two‐way ANOVA on the level of anxiety showed a significant interaction between groups and time. Analysis of simple main effect test results showed a significant difference between the groups in the post‐test (p =.000) and a significant difference over time in the Quran (p = 0,000) and music (p =.000) groups (Table 3). The estimated effect size was large (η2 = 0.408).
Concerning the third hypothesis, the result of two‐way ANOVA showed that there were no significant differences in anxiety levels in terms of age (p =.906), chemotherapy sessions (p = 0,949), days interval for hospital entries (p =.906), diagnosis (p =.381), gender (p = 0,296), marital status (p =.713) and educational level (p = 0,065). The level of anxiety has been decreased (p =.000) regardless of the mentioned demographics (Table 4).
TABLE 4.
Two‐ way Analysis of variance and pre‐test/post‐test means differences by groups of participants characteristics (n = 159)
| Two‐way analysis of variance | ||||
|---|---|---|---|---|
| Characteristics | F | p‐value | η2 | |
| Age | Time | 28.284 | .000 | 0.153 |
| Time × Group | 1.003 | .318 | 0.006 | |
| Group | 0.014 | .906 | 0.000 | |
| Chemotherapy sessions | Time | 102.01 | .000 | 0.394 |
| Time × Group | 1.717 | .192 | 0.011 | |
| Group | 0.004 | .949 | 0.000 | |
| Hospital entry days’ interval | Time | 28.284 | .000 | 0.153 |
| Time × Group | 1.003 | .318 | 0.006 | |
| Group | 0.014 | .906 | 0.000 | |
| Diagnosis | ||||
| Hodgkin lymphoma | Time | 204.11 | .000 | 0.575 |
| Non‐Hodgkin lymphoma | Time × Group | 0.849 | .549 | 0.038 |
| Multiple myeloma | Group | 1.077 | .381 | 0.048 |
| Ca liver | ||||
| Ca breast | ||||
| Ca prostate | ||||
| Ca pancreas | ||||
| Leukaemia | ||||
| Gender | ||||
| Male | Time | 220.59 | .000 | 0.584 |
| Female | Time × Group | 0.018 | .892 | 0.000 |
| Group | 1.099 | .296 | 0.007 | |
| Marital status | ||||
| Single | Time | 44.364 | .000 | 0.224 |
| Married | Time × Group | 2.211 | .070 | 0.054 |
| Divorced | Group | 0.531 | .713 | 0.014 |
| Separated | ||||
| Widow | ||||
| Educational level | ||||
| Primary school graduate | Time | 179.65 | .000 | 0.537 |
| Middle school graduate | Time × Group | 3.267 | .023 | 0.059 |
| High school graduate | Group | 2.452 | .065 | 0.045 |
| Bachelor degree | ||||
5. DISCUSSION
The results showed that the effect size was high in the interventions groups (Quran and music). Based on Cohen (1988), the effect size indicates the practical significant difference. Although there was a significant difference in the anxiety level in pre‐ and post‐test in the control group, it does not indicate that this difference is practically significant. In this study, the explanation of the effect is retrieved from Cohen (1988). The results indicated that the effect size of the control group was 0.33, which means there was a small effect in the post‐test as the difference between the pre‐test and post‐test means was 4.35. With Cohen's d of 0.3, there was a change in the anxiety level in almost 63% of the participants in the control group after the post‐test. In the Quran and music groups, the difference between the pre‐test and post‐test means was 25.15 and 25.34, and the effect size was 2.76 and 2.67, respectively. Indeed, two and more are in the higher level of Cohen's d. According to the results, the probability of alteration in anxiety levels was more than 92% in participants who listened to Quran or music. Comparing the effect size between the control group and the two intervention groups, listening to Quran or music can reduce the anxiety level significantly. Based on these results, the first hypothesis is supported. The effect sizes are very close between the Quran and music groups. This indicates that listening to Quran or music has a large effect to reduce the anxiety level in people with cancer. In fact, this result was expected by the researchers as many studies suggested Quran (Ghiasi & Keramat, 2018; Moeini et al., 2014; Sulistyawati & Probosuseno, 2019) and other studies suggested music (Bilgiç & Acaroğlu, 2017; Burns et al., 2008; Jasemi et al., 2016; Karagozoglu et al., 2013; Lin et al., 2011; Nightingale et al., 2013; Spilioti et al., 2017) as strategies to reduce anxiety in people with cancer and some studies in non‐cancer patients, too (Babaii et al., 2015; Frih et al., 2017; Mirbagher Ajorpaz & Aghajani, 2011). The researchers assumed that spiritual therapy (listening to Quran) has more effects to reduce chemotherapy‐induced anxiety than music. However, the results of this study revealed that there is no significant difference in anxiety levels among patients who listened to Quran and who listened to music. This means that listening to Quran and music has the same effects in reducing the level of anxiety in people with cancer before chemotherapy administration. Although some studies approved the role of Quran and music to reduce anxiety in people with cancer, the current study was the first one to compare the effect of the two strategies on chemotherapy‐induced anxiety in people with cancer. Using music or spiritual therapy can be added in nursing care plans for people with cancer prior chemotherapy administrations in order to reduce chemotherapy‐induced anxiety. Listening to Quran is an effective way that can be used as spiritual therapy.
More studies are encouraged to be accomplished in different Muslim populations and different countries to assess whether listening to Quran has more effect than music to reduce chemotherapy‐induced anxiety. It is recommended that patients choose the musical theme or the verse of the Quran and the reciter voice, that they want to listen, by their own preferences.
5.1. Limitation
The participants had different types of cancer with different stages of the disease. Also, the type of chemotherapy differs from a patient to another. These factors may affect the level of anxiety prior chemotherapy. On the other hand, the musical theme or the verse of the Quran and the voice of the reciter that provided to patients may do not meet their preferences. Furthermore, there was no follow‐up after the 20‐min intervention, which limits realizing the long of the intervention's effect.
6. CONCLUSION
The results of this study highlighted that listening to Quran or music can reduce the level of chemotherapy‐induced anxiety in people with cancer. However, listening to Quran does not affect more than listening to music to reduce chemotherapy‐induced anxiety in people with cancer. On the other hand, age, gender, educational level and marital status did not play significant roles at the level of chemotherapy‐induced anxiety.
It is recommended that nurses use Quran as a spiritual care for Muslim patients in order to reduce their anxiety before chemotherapy administration. Music can be used also for Muslim and non‐Muslim patients for the same reason. Listening to both Quran and music can be used in nursing care plans to reduce chemotherapy‐induced anxiety in people with cancer. In fact, listening to Quran or music is harmless, easy to implement and does not cost. By reducing the level of anxiety prior chemotherapy administration, holistic care can be approached in primary and secondary health care.
CLINICAL TRIAL REGISTRATION NUMBER
This study was done in compliance with the Declaration of Helsinki, and the protocol was approved by the Iranian Registry of Clinical Trials (IRCT20200429047244N1).
CONFLICT OF INTEREST
No conflict interest has been declared by the authors.
AUTHOR CONTRIBUTION
Mohammed Baqer Al‐Jubouri: Conceptualization, methodology, writing—original draft, writing—review and editing, supervision. Safad Riyadh Isam: Investigation, resources, writing—review and editing. Shaymaa Mohammed Hussein: Investigation, resources, writing—review and editing. Felipe Machuca‐Contreras: Validation, formal analysis, writing—review and editing.
ACKNOWLEDGEMENTS
The authors thank Maha A. Bahammam for her support and giving the permission to use the Arabic version of STAI scale. Also, the College of Nursing at University of Baghdad is acknowledged for its support and providing the IRB approval. Furthermore, the authors thank the administrators in Al‐Kadhumain Teaching Hospital and Oncology Teaching Hospital for giving the approval letters to collect the data.
Al‐Jubouri MBA, Isam SR, Hussein SM, Machuca‐Contreras F. Recitation of quran and music to reduce chemotherapy‐induced anxiety among adult patients with cancer: A clinical trial. Nurs Open. 2021;8:1606–1614. 10.1002/nop2.781
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- American Music Therapy Association . (n.d.). Definition and quotes about music therapy: What is music therapy? https://www.musictherapy.org/about/quotes/.
- Iraqi Minorities Council (2015). Iraq. https://www.justice.gov/eoir/page/file/1027311/download.
- American Cancer Society (2019). How is chemotherapy used to treat cancer? https://www.cancer.org/treatment/treatments‐and‐side‐effects/treatment‐types/chemotherapy/how‐is‐chemotherapy‐used‐to‐treat‐cancer.html .
- American Psychological Association . (n.d. b). The State‐Trait Anxiety Inventory (STAI). https://www.apa.org/pi/about/publications/caregivers/practice‐settings/assessment/tools/trait‐state.aspx.
- American Psychological Association (n.d. a). Anxiety. https://www.apa.org/topics/anxiety/index.
- Babaii, A. , Abbasinia, M. , Hejazi, S. F. , Seyyed Tabaei, S. R. , & Dehghani, F. (2015). The effect of listening to the voice of Quran on anxiety before cardiac catheterization: A randomized controlled trial. Health, Spirituality and Medical Ethics, 2(2), 2–7. [Google Scholar]
- Babamohamadi, H. , Sotodehasl, N. , Koenig, H. G. , Jahani, C. , & Ghorbani, R. (2015). The effect of Holy Qur’an recitation on anxiety in hemodialysis patients: A randomized clinical trial. Journal of Religion and Health, 54(5), 1921–1930. 10.1007/s10943-014-9997-x [DOI] [PubMed] [Google Scholar]
- Bahammam, M. A. (2016). Validity and reliability of an Arabic version of the state‐trait anxiety inventory in a Saudi dental setting. Saudi Medical Journal, 37(6), 668. 10.15537/smj.2016.6.13935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behadili, S. F. , Abd, M. S. , Mohammed, I. K. , & Al‐Sayyid, M. M. (2019). Breast cancer decisive parameters for Iraqi women via data mining techniques. Journal of Contemporary Medical Sciences, 5(2). [Google Scholar]
- Bilgiç, Ş. , & Acaroğlu, R. (2017). Effects of listening to music on the comfort of chemotherapy patients. Western Journal of Nursing Research, 39(6), 745–762. 10.1177/0193945916660527 [DOI] [PubMed] [Google Scholar]
- Burns, D. S. , Azzouz, F. , Sledge, R. , Rutledge, C. , Hincher, K. , Monahan, P. O. , & Cripe, L. D. (2008). Music imagery for adults with acute leukemia in protective environments: A feasibility study. Supportive Care in Cancer, 16(5), 507–513. [DOI] [PubMed] [Google Scholar]
- Cameron, A. C. , Touyz, R. M. , & Lang, N. N. (2016). Vascular complications of cancer chemotherapy. Canadian Journal of Cardiology, 32(7), 852–862. 10.1016/j.cjca.2015.12.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charalambous, A. , Giannakopoulou, M. , Bozas, E. , & Paikousis, L. (2015). A randomized controlled trial for the effectiveness of progressive muscle relaxation and guided imagery as anxiety reducing interventions in breast and prostate cancer patients undergoing chemotherapy. Evidence‐Based Complementary and Alternative Medicine, 2015, 1–10. 10.1155/2015/270876 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chien, C. H. , Liu, K. L. , Chien, H. T. , & Liu, H. E. (2014). The effects of psychosocial strategies on anxiety and depression of patients diagnosed with prostate cancer: A systematic review. International Journal of Nursing Studies, 51(1), 28–38. 10.1016/j.ijnurstu.2012.12.019. [DOI] [PubMed] [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates, Lawrence Erlbaum. [Google Scholar]
- Cohen, J. , Cohen, P. , West, S. G. , & Aiken, L. S. (2013). Applied multiple regression/correlation analysis for the behavioral sciences. Routledge. [Google Scholar]
- Dadkhah, B. , Anisi, E. , Mozaffari, N. , Amani, F. , & Pourghasemian, M. (2019). Effect of music therapy with periorbital massage on chemotherapy‐induced nausea and vomiting in gastrointestinal cancer: A randomized controlled trial. Journal of Caring Sciences, 8(3), 165. 10.15171/jcs.2019.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dein, S. , Cook, C. C. , Powell, A. , & Eagger, S. (2010). Religion, spirituality and mental health. The Psychiatrist, 34(2), 63–64. 10.1192/pb.bp.109.025924. [DOI] [Google Scholar]
- Feng, C. , Wang, H. , Lu, N. , Chen, T. , He, H. , Lu, Y. , & Tu, X. (2014). Log‐transformation and its implications for data analysis. Shanghai Archives of Psychiatry, 26(2), 105–109. 10.3969/j.issn.1002-0829.2014.02.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frih, B. , Mkacher, W. , Bouzguenda, A. , Jaafar, H. , ALkandari, S. A. , Ben Salah, Z. , Sas, B. , Hammami, M. , & Frih, A. (2017). Effects of listening to Holy Qur’an recitation and physical training on dialysis efficacy, functional capacity, and psychosocial outcomes in elderly patients undergoing haemodialysis. Libyan Journal of Medicine, 12(1), 10.1080/19932820.2017.1372032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ganjou, M. , & Akbari, Z. (2013). A comparative study on the effects of holly Quran and music sound on student’s text anxiety. Complementary Medicine Journal of Faculty of Nursing & Midwifery, 3(2), 471–480. [Google Scholar]
- Garcia, S. (2014). The effects of education on anxiety levels in patients receiving chemotherapy for the first time: An integrative review. Clinical Journal of Oncology Nursing, 18(5), 516–521. 10.1188/14.CJON.18-05AP. [DOI] [PubMed] [Google Scholar]
- Ghiasi, A. , & Keramat, A. (2018). The effect of listening to holy Quran recitation on anxiety: A systematic review. Iranian Journal of Nursing and Midwifery Research, 23(6), 411. 10.4103/ijnmr.IJNMR_173_17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heydarzadeh, L. , Alilu, L. , Habibzadeh, H. , & RasouIi, J. (2020). The effect of peer education on knowledge, comprehension, and knowledge application of patients regarding chemotherapy complications. Iranian Journal of Nursing and Midwifery Research, 25(1), 40. 10.4103/ijnmr.IJNMR_69_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hosseini, M. , Tirgari, B. , Forouzi, M. A. , & Jahani, Y. (2016). Guided imagery effects on chemotherapy induced nausea and vomiting in Iranian breast cancer patients. Complementary Therapies in Clinical Practice, 25, 8–12. 10.1016/j.ctcp.2016.07.002 [DOI] [PubMed] [Google Scholar]
- Iraqi Cancer Board (2018). Annual Report Iraqi Cancer Registry. https://moh.gov.iq/upload/upfile/ar/1090.pdf .
- Jasemi, M. , Aazami, S. , & Zabihi, R. E. (2016). The effects of music therapy on anxiety and depression of cancer patients. Indian Journal of Palliative Care, 22(4), 455. 10.4103/0973-1075.191823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karagozoglu, S. , Tekyasar, F. , & Yilmaz, F. A. (2013). Effects of music therapy and guided visual imagery on chemotherapy‐induced anxiety and nausea–vomiting. Journal of Clinical Nursing, 22(1–2), 39–50. 10.1111/jocn.12030. [DOI] [PubMed] [Google Scholar]
- Kim, K. S. , & Kwon, S. H. (2007). Comfort and quality of life of cancer patients. Asian Nursing Research, 1(2), 125–135. 10.1016/S1976-1317(08)60015-8. [DOI] [PubMed] [Google Scholar]
- Koenig, H. G. (2012). Religion, spirituality, and health: The research and clinical implications. International Scholarly Research Network. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenig, H. , Koenig, H. G. , King, D. , & Carson, V. B. (2012). Handbook of religion and health, psychiatry, 2012. : OUP. 10.5402/2012/278730. [DOI] [Google Scholar]
- Lin, M. F. , Hsieh, Y. J. , Hsu, Y. Y. , Fetzer, S. , & Hsu, M. C. (2011). A randomised controlled trial of the effect of music therapy and verbal relaxation on chemotherapy‐induced anxiety. Journal of Clinical Nursing, 20(7–8), 988–999. 10.1111/j.1365-2702.2010.03525.x. [DOI] [PubMed] [Google Scholar]
- Massimiliani, V. , Pellegrino, R. , Donnarumma, L. , Perrone, L. , Riondino, S. , & Roselli, M. (2017). Music intervention during chemotherapy infusion reduces anxiety in oncological patients. Annals of Oncology, 28, vi82.– 10.1093/annonc/mdx434.002. [DOI] [Google Scholar]
- Mirbagher Ajorpaz, N. , & Aghajani, M. (2011). The effects of music and Holy Quran on patients' anxiety and vital signs before abdominal surgery. Evidence Based Care, 1(1), 63–76. [Google Scholar]
- Mirsane, S. A. , Kheirkhah, D. , Shafagh, S. , Mirbagher Ajorpaz, N. , & Aminpour, J. (2016). The effect of listening to Vaghe'a Surah and its translation on the state and trait anxiety before general surgeries: A randomized controlled clinical trial. Health, Spirituality and Medical Ethics, 3(3), 12–17. [Google Scholar]
- Moeini, M. , Taleghani, F. , Mehrabi, T. , & Musarezaie, A. (2014). Effect of a spiritual care program on levels of anxiety in patients with leukemia. Iranian Journal of Nursing and Midwifery Research, 19(1), 88. [PMC free article] [PubMed] [Google Scholar]
- Moons, W. G. , & Shields, G. S. (2015). Anxiety, not anger, induces inflammatory activity: An avoidance/approach model of immune system activation. Emotion, 15(4), 463. 10.1037/emo0000055. [DOI] [PubMed] [Google Scholar]
- National Cancer Institute (2015). Chemotherapy to treat cancer. https://www.cancer.gov/about‐cancer/treatment/types/chemotherapy .
- National Cancer Institute (2018). Cancer statistics. https://www.cancer.gov/about‐cancer/understanding/statistics.
- Nightingale, C. L. , Rodriguez, C. , & Carnaby, G. (2013). The impact of music interventions on anxiety for adult cancer patients: A meta‐analysis and systematic review. Integrative Cancer Therapies, 12(5), 393–403. 10.1177/1534735413485817. [DOI] [PubMed] [Google Scholar]
- Novotney, A. (2013). Music as medicine. American Psychological Association., https://www.apa.org/monitor/2013/11/music.
- Pandey, M. , Sarita, G. P. , Devi, N. , Thomas, B. C. , Hussain, B. M. , & Krishnan, R. (2006). Distress, anxiety, and depression in cancer patients undergoing chemotherapy. World Journal of Surgical Oncology, 4, 68. 10.1186/1477-7819-4-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siegel, R. L. , Miller, K. D. , & Jemal, A. (2019). Cancer statistics, 2019. CA: A Cancer Journal for Clinicians, 69(1), 7–34. 10.3322/caac.21551. [DOI] [PubMed] [Google Scholar]
- Spielberger, C. D. , Gorsuch, R. L. , Lushene, R. , Vagg, P. R. , & Jacobs, G. A. (1983). Manual for the State‐Trait Anxiety Inventory. Consulting Psychologists Press. [Google Scholar]
- Spilioti, E. D. , Galanis, P. A. , & Kalokairinou, A. G. (2017). The Effects of music on cancer patients submitted to chemotherapy treatment. International Journal of Caring Sciences, 10(3), 1465–1477. [Google Scholar]
- Sulistyawati, R. A. , Probosuseno, S. & Setiyarini, S. (2019). Dhikr therapy for reducing anxiety in cancer patients. Asia‐Pacific Journal of Oncology Nursing, 6(4), 411. 10.4103/apjon.apjon_33_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanbockstael, J. , Coquan, E. , Gouerant, S. , Allouache, D. , Faveyrial, A. , Noal, S. , Delcambre, C. , Galais, M.‐P. , Héron, J.‐F. , Lefebvre, A.‐C. , Sevin, E. , Hrab, I. , Polycarpe, F. , André, M. , Kaluzinski, L. , Gervais, R. , Gunzer, K. , Vié, B. , Saucier, G. , … Joly, F. (2016). How to improve the prevention of chemotherapy‐induced nausea and vomiting? The French NAVI study. Supportive Care in Cancer, 24(3), 1131–1138. 10.1007/s00520-015-2882-7 [DOI] [PubMed] [Google Scholar]
- Vichaya, E. G. , Chiu, G. S. , Krukowski, K. , Lacourt, T. E. , Kavelaars, A. , Dantzer, R. , Heijnen, C. , & Walker, A. K. (2015). Mechanisms of chemotherapy‐induced behavioral toxicities. Frontiers in Neuroscience, 9, 131. 10.3389/fnins.2015.00131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, L. S. , & Hopper, P. D. (2015). Understanding medical surgical nursing. FA Davis. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.