

Abstract
Popliteus tendon injuries most often occur in a traumatic setting with damage to multiple other knee structures. Isolated popliteal injuries, however, are rare. To our knowledge, there are no cases of a female pediatric patient with an intrasubstance popliteal tendon rupture in the current literature. This case report aims to illustrate symptoms, imaging, and treatment of an isolated popliteal tendon rupture in an adolescent female. An athletic 14-year-old female presented with right knee pain 4 weeks after a basketball injury in which she dove for the ball and fell, twisting and striking her knee. She had diffuse pain on both sides of the right knee for 3 weeks and pain with running, jumping or twisting. The knee exam was otherwise unremarkable. A right knee MRI demonstrated a complete rupture of the popliteal tendon. No other knee injuries were visualized. The patient was treated non-operatively and gradually returned to normal activities and sports at 6 weeks post injury. On 6-year follow up, the patient had no residual pain or instability and was able to play basketball without difficulty. Isolated popliteal tendon ruptures are extremely rare and difficult to diagnose given non-specific clinical exam findings. While these ruptures can be difficult to visualize on MRI, imaging can help to clarify the diagnosis by ruling out other injuries with similar clinical presentations. In the case of this young and active patient, diagnosis and full recovery without limitations were achieved with 6 weeks of conservative management.
Keywords: popliteus, isolated, rupture, orthopedic, knee, posterolateral corner
Case Presentation
An athletic 14-year-old Asian-American female with no significant past medical history presented 4 weeks after a basketball injury with right knee pain. She was playing in a high school competition when she dove for the ball and fell to the ground. She struck her right knee with the contralateral knee and twisted her right knee as she fell. The right knee was swollen for several days. There was an audible “pop” at the time of the injury. She continued to have pain on the medial and lateral aspects of the right knee which gradually improved. She was able to bear full weight, and she wore a compression knee sleeve.
On examination the patient did not have an antalgic gait. The right knee had no bruising and there was no residual effusion. Bilateral knee range of motion was 0° to 145° and painless. There was no tenderness to palpation along the right medial or lateral joint lines and McMurray’s test (evaluates for meniscal injury) was normal. The right knee demonstrated normal stability with anterior and posterior drawer tests and with varus and valgus stress (respective tests for anterior, posterior, lateral, and medial ligamentous injuries). The patella was stable without apprehension and painless with the patellar grind test (evaluates for patellar chondral injury). The Dial test was symmetric and normal at 30° and 90° bilaterally without pain (evaluates for posterolateral corner injuries). The neurovascular exam was normal. The patient had no other significant physical exam findings but she was unable to run, jump or twist. Due to her history and her inability to return to sports an MRI was ordered.
Imaging Studies
A six-sequence, closed, 3.0T MRI was completed. A high grade-to-complete rupture of the popliteus tendon was seen at the level of the popliteal hiatus, with retracted tendon distal and medial to the tibiofibular articulation. This tear can be visualized in Figure 1 (axial MRI) as an enlarged cross section of the popliteus resulting from retraction and scarring of the muscle. The posterior compartment of the knee is visualized in Figure 2 (Sagittal MRI), however, the popliteus is not seen in the popliteal hiatus due to the tear (green arrow). It would normally be seen at the posterior horn of the lateral meniscus. There is edema adjacent to the soleus muscle posterior to the popliteal hiatus, deep to the lateral head of the gastrocnemius (blue arrow). This resulted from the popliteus injury. The distal popliteus is visualized (blue arrows) in Figure 3 (Coronal MRI) however a gap is seen where the tendon should attach proximally at the fibular head and lateral femoral condyle (yellow circle). A few proximal tendinous fibers remain.
Figure 1.
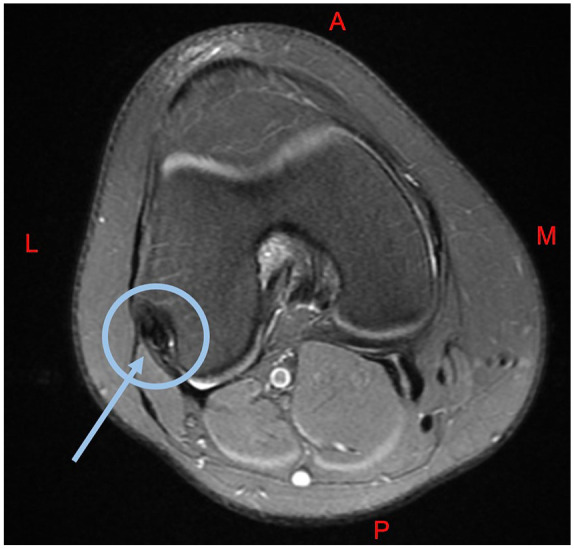
Axial MRI of the right knee. The popliteus is visualized in the blue circle with an enlarged cross section resulting from retraction and scarring of the muscle.
Abbreviations: M, Medial; L, Lateral; A, Anterior; P, Posterior.
Figure 2.
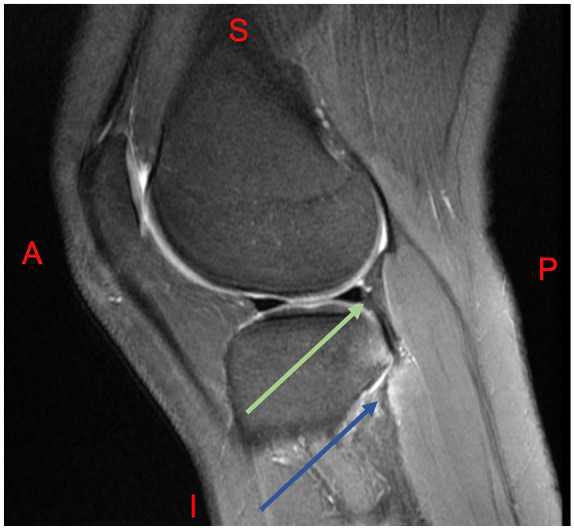
Sagittal MRI of the right knee. The posterior compartment of the knee is visualized; however, the popliteus is not seen in the popliteal hiatus (green arrow). It would normally be seen at the posterior horn of the lateral meniscus. There is edema around the soleus muscle posterior to the popliteal hiatus, deep to the lateral head of the gastrocnemius (blue arrow).
Abbreviations: S, Superior; I, Inferior; A, Anterior; P, Posterior.
Figure 3.
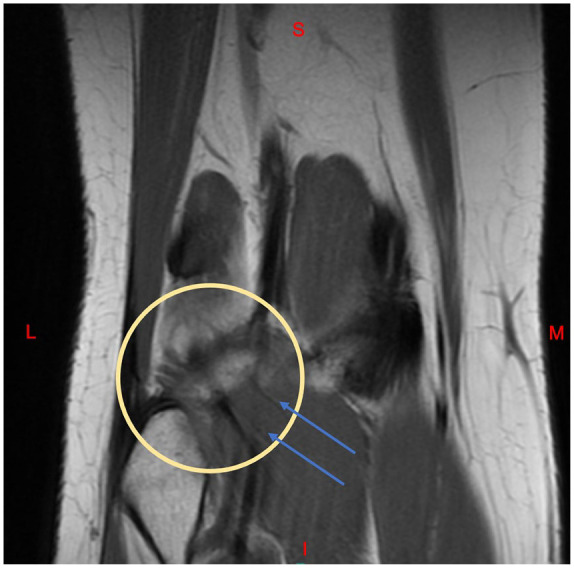
Coronal MRI of the right knee. The distal popliteal muscle is visualized (blue arrows), however a gap is seen where the tendon should attach proximally at the fibular head and lateral femoral condyle (yellow circle). A few proximal tendinous fibers remain.
Abbreviations: S, Superior; I, Inferior; M, Medial; L, Lateral.
Bone contusions were seen in the posterolateral corner on the tibial plateau and adjacent fibular head. There was no further injury to the posterolateral corner including the lateral collateral ligament (LCL) and biceps femoris. There was no tear of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), or menisci. The medial collateral ligament (MCL) and iliotibial (IT) band and were intact. There was no damage to the articular cartilage.
Final Diagnosis
Isolated Popliteus Tendon Rupture.
Treatment Course
The patient was instructed to progressively return to normal level of activity. She started with stationary cycling, then advanced to elliptical, to light jogging, and then to walking alternating with jogging. She was instructed to avoid jumping and impact activities for 6 weeks. When she was able to do these activities without pain or instability, she was released to return to all activities. She continued to play competitive high school basketball for the next 2 years without incident or limitations. At the 6-year follow up, she was still without limitations to her movement, stability, and strength. She plays sports including basketball and soccer without limitations.
Discussion
The popliteus is a thin triangular muscle with a wide attachment on the posteromedial tibial surface. The popliteus tendon courses superior and laterally, entering the knee joint through the popliteal space before inserting at the lateral femoral condyle inferior to the LCL. The tendon forms an additional strong attachment to the fibular head with other variable attachments to the posterior horn of the lateral meniscus. Functionally, the popliteus muscle internally rotates of the tibia and forms part of the posterolateral corner. The muscle helps initiate knee flexion by lateral rotation of the femur on the tibia and plays a part in preventing excessive posterior tibial translation and rotation. There is some debate in literature as to whether or not the popliteus tendon plays a role in controlling lateral meniscus displacement.1,2
Injuries to the popliteus in general are not particularly uncommon as they can occur in association with more extensive injury of the posterolateral corner or ACL.1,3 Isolated injury of the popliteus tendon, however, is an extremely rare injury. When seen in the case of skeletally immature patients, there is typically avulsion of the tendon rather than intrasubstance tear. 5 While this young athlete was skeletally immature, her tendon instead underwent intrasubstance rupture.
Mechanism of injury is typically traumatic, with lesions of the popliteus tendon attributed to acute external rotation of the tibia in a partially flexed knee, without contact or through varus force with a fixed femur. 4 In the case of our patient, the mechanism was likely the twist of the right knee as she fell in combination with the force of the contralateral knee striking her right knee.
Diagnosis of isolated popliteal injuries based on physical examination can be difficult as symptoms are often non-specific. In our case, the patient presented with acute swelling at the time of injury and improving joint line tenderness, ligamentous stability under clinical examination, and normal gait. These symptoms can be associated with various knee injuries. Though non-specific, hallmarks that should raise suspicion for isolated popliteus injury include acute hemarthrosis, joint effusions, posterolateral joint-line tenderness, and discomfort on range of motion in an otherwise stable knee. Patients can present with an accentuated external rotation of the tibia with flexion. The stability of the knee despite swelling and tenderness may be indicative of isolated popliteus rupture.1,3-6
As clinical examination can raise suspicion of but is insufficient to diagnose isolated popliteus tendon rupture, MRI is utilized to further evaluate the knee joint in order to exclude ACL, lateral meniscus, or other posterolateral corner injury and to confirm the tendon rupture itself.
In the case of popliteal tendon injuries associated with ligament rupture, meniscal tear, avulsion, or further PLC injury, surgical reconstruction is almost always indicated.5,7 However, as isolated intrasubstance popliteus injuries do not typically result in instability and have not been shown to increase the long-term risk of knee arthritis. This injury can be treated conservatively without further consequence to the knee’s stability. Literature also reports the use of diagnostic arthroscopy in confirming popliteus injury. 5 However, as isolated popliteus injuries are best treated conservatively, our recommendation is for non-surgical treatment. Concurrent injuries necessitating surgery can be visualized by MRI. 1
A course of conservative treatment with early weight bearing and functional rehabilitation has been shown to be a viable option in the context of isolated popliteus injury. Guha et al 3 reported return to activity at 6 weeks and no instability at 12 months with non-operative management of a semi-professional athlete with complete intra-substance rupture. Koong et al 4 similarly described return to full contact activities at 4 weeks in a 22-year-old professional ruby player who had sustained a complete popliteus tendon rupture at the musculotendinous junction. This player returned to regular season matches soon after.
Despite successes of conservative treatment reported in the literature, there is little specificity regarding rehabilitation protocol. Typically, however, there is some period of rest or immobilization followed by strengthening exercises, graduated range of motion, and gradual return to activity. In this case, with the absence of any injuries requiring surgery, as indicated by both physical examination and the MRI, confirmatory arthroscopy was unnecessary. The patient did well with conservative management.
In this case of a complete traumatic tendon rupture, conservative treatment proved successful. At the 6-year follow up, the patient was pain-free, active, and without limitations from the ruptured tendon.
Conclusion
Isolated popliteal tendon ruptures are rare, and difficult to diagnose on clinical examination as the presenting symptoms are non-specific. Isolated popliteal tendon rupture can be visualized on MRI. MRI can rule out more serious injuries with similar presentations that might require early surgical intervention. In the case of this young active patient, full recovery and return to sports without ongoing limitations was achieved by conservative management. Conservative treatment is indicated in the case of isolated popliteal tendon rupture and prognosis is excellent.
Footnotes
Author Contributions: NLN: Participated in data collection; drafted the manuscript; revised the manuscript critically and incorporated intellectual input; approved the final version of the manuscript.
CMK: Participated in data collection; drafted the manuscript; revised the manuscript critically and incorporated intellectual input; approved the final version of the manuscript.
HNY: Participated in data collection; revised the manuscript critically and incorporated intellectual input; approved the final version of the manuscript.
PAB: Participated in data collection; revised the manuscript critically and incorporated intellectual input; approved the final version of the manuscript.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent: Institutional review board approval is not required for a deidentified single case report. Informed consent was obtained from the patient and guardian for the publication of this case report.
ORCID iD: Nicholas L. Newcomb  https://orcid.org/0000-0003-0936-9966
https://orcid.org/0000-0003-0936-9966
References
- 1. Jadhav SP, More SR, Riascos RF, Lemos DF, Swischuk LE. Comprehensive review of the anatomy, function, and imaging of the popliteus and associated pathologic conditions. Radiographics. 2014;34:496-513. [DOI] [PubMed] [Google Scholar]
- 2. Wheeler LD, Lee EYP, Lloyd DCF. Isolated popliteus tendon avulsion in skeletally immature patients. Clin Radiol. 2008;63:824-828. [DOI] [PubMed] [Google Scholar]
- 3. Guha AR, Gorgees KA, Walker DI. Popliteus tendon rupture: a case report and review of the literature. Br J Sports Med. 2003;37:358-360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Koong DPH, An VVG, Lorentzos P, Moussa P, Sivakumar BS. Non-operative rehabilitation of isolated popliteus tendon rupture in a rugby player. Knee Surg Relat Res. 2018;30:269-272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Burstein DB, Fischer DA. Isolated rupture of the popliteus tendon in a professional athlete. Arthroscopy. 1990;6:238-241. [DOI] [PubMed] [Google Scholar]
- 6. Westrich GH, Hannafin JA, Potter HG. Isolated rupture and repair of the popliteus tendon. Arthroscopy. 1995;11: 628-632. [DOI] [PubMed] [Google Scholar]
- 7. Rue CJP, Kilcoyne CK, Dickens CJ, Kluk CM. Diagnosis and treatment of injuries to the posterolateral ligament complex. J Knee Surg. 2011;24:143-150. [DOI] [PubMed] [Google Scholar]