

Abstract
Objectives:
To evaluate the association between maxillary arch dimensions and fundamental frequency and formants of voice in prepubertal subjects.
Materials and Methods:
Thirty-five consecutive prepubertal patients seeking orthodontic treatment were recruited (mean age = 11.41 ± 1.46 years; range, 8 to 13.7 years). Participants with a history of respiratory infection, laryngeal manipulation, dysphonia, congenital facial malformations, or history of orthodontic treatment were excluded. Dental measurements included maxillary arch length, perimeter, depth, and width. Voice parameters comprising fundamental frequency (f0_sustained), Habitual pitch (f0_count), Jitter, Shimmer, and different formant frequencies (F1, F2, F3, and F4) were measured using acoustic analysis prior to initiation of any orthodontic treatment. Pearson's correlation coefficients were used to measure the strength of associations between different dental and voice parameters. Multiple linear regressions were computed for the predictions of different dental measurements.
Results:
Arch width and arch depth had moderate significant negative correlations with f0 (r = −0.52; P = .001 and r = −0.39; P = .022, respectively) and with habitual frequency (r = −0.51; P = .0014 and r = −0.34; P = .04, respectively). Arch depth and arch length were significantly correlated with formant F3 and formant F4, respectively. Predictors of arch depth included frequencies of F3 vowels, with a significant regression equation (P-value < .001; R2 = 0.49). Similarly, fundamental frequency f0 and frequencies of formant F3 vowels were predictors of arch width, with a significant regression equation (P-value < .001; R2 = 0.37).
Conclusions:
There is a significant association between arch dimensions, particularly arch length and depth, and voice parameters. The formant most predictive of arch depth and width is the third formant, along with fundamental frequency of voice.
Keywords: Maxilla, Arch, Voice, Acoustic, Association, Prepubertal
INTRODUCTION
Voice is a reflection of who we are. It is a sign of health and sickness and a reference to our social norm, culture, and gender identity. Vocal characteristics such as pitch and timbre are often an acoustic cue to our personality and morphology. As air is slowly exhaled, the muscles of the larynx pulsate the vocal folds, leading to vibrations in the air that was supplied. The number of cycles of vibration (opening-closing) of vocal folds per second is the fundamental frequency (f0_sustained) or the pitch. The average f0 for a person is calculated uttering a long steady vowel, whereas the average f0 calculated while the subject is counting to 10 is referred to as the habitual frequency or f0_count. The sound waves produced by the vocal folds in the larynx must be amplified and modified by the vocal tract resonators: oral and nasal cavities as well as sinuses. The shape, size, and muscle tension of the resonators will produce the human voice as we know it and give it its individual quality and character. These important speech characteristics that are intimately related to the vocal apparatus are the formants.
The concept of voice timbre has been closely related to both organic and functional components of the vocal tract. Variability in these structural components explains the disparities in acoustic features among speakers. Strong correlation has been shown to exist between vocal tract morphology and vocal characteristics in both dysphonic1 and nondysphonic subjects.1,2 Jesus et al.3 reported higher values for the second formant (second preferred harmonic) in patients with unilateral vocal fold paralysis, in comparison to controls. Similarly, Titze2 described clustering of the first two formants in patients with unilateral vocal fold paralysis, alluding to the narrowing of the vocal tract in compensation for inefficient phonation. An intuitive example in nondysphonic subjects is voice sexual dimorphism in relation to the vocal tract morphologic differences between men and women.4 On a larger scale, voice has also been considered an acoustic cue to body size and shape.5,6 There is invariably an inverse relationship among body weight, height, and vocal pitch.7 More so, there is a correlation among vocal pitch, shoulder and waist-to-hip ratio, and skull and chest circumference.8 However, several other authors9–11 failed to demonstrate any correlation between body characteristics and voice. Franco et al.12 examined somatotype and body composition differences among dysphonic and nondysphonic patients in 72 adults and found no significant difference between the dysphonic group (n = 32) and controls (n = 40).
A correlation between facial measurements and various acoustic parameters has been previously reported. A significant moderate negative correlation was found between facial width, maxillary and mandibular width, and f0_sustained and f0_count. Facial length also correlated moderately with f0_count.13 The association between formant frequencies and their dispersion with the length and projection of the upper and lower jaws was found14 to be significant between F3, F4, and the length of the mandible and maxilla for the vowels [a, i, o, u]. The impact of rapid maxillary expansion on voice has also been reported,14 and results indicated that treatment can lower the first and second formants for the vowel [a] for most subjects. While the maxillary and mandibular arches provided bony support for the lips in the production of the sound of the bilabial phonemes,15 orthodontic treatment with labial appliances was found to affect speech production.16,17
The findings of all the aforementioned investigations corroborated the strong interplay between vocal tract measurements and fundamental frequency and its harmonics. Thus, the purpose of this investigation was to further analyze the correlation between maxillary arch measurements and various acoustic parameters, namely the fundamental frequency, perturbation parameters, and the first four formants.
MATERIALS AND METHODS
A total of 35 consecutive growing patients seeking orthodontic treatment at the Division of Orthodontics and Dentofacial Orthopedics at the American University of Beirut-Lebanon were recruited for this study. Institutional review board (IRB) approval was obtained prior to the initiation of this study (IRB ID: OTO.AH.30), and all participants' guardians signed the consent form. A speech language expert pathologist performed the acoustic analysis and excluded participants with any history of respiratory infection, laryngeal manipulation, or dysphonia. Other exclusion criteria were congenital facial malformations and history of orthodontic treatment. Hand wrist radiographs were evaluated to determine bone age of the patients. Female and male subjects were excluded when their bone age exceeded 11.5 and 13.5 years, respectively.
Dental Measurements
Maxillary dental measurements were performed on pretreatment dental models (Figure 1). The cast measurements included arch length, perimeter, depth, and width. Arch length was equal to the distance along the midline perpendicular to the intermolar plane, which passed through the mesio-buccal cusps of the first molar (Figure 1). Arch perimeter was measured from the mesio-buccal cusp of the first permanent molar on one side to the mesio-buccal cusp of the molar on the other side (Figure 1). Arch width was measured as the horizontal distance between the mesio-buccal cusps of the right and left first molars (Figure 1). Arch depth was equal to the distance from the intermolar plane (between the mesio-buccal cusps of the first molars) to the palate (Figure 2).
Figure 1.
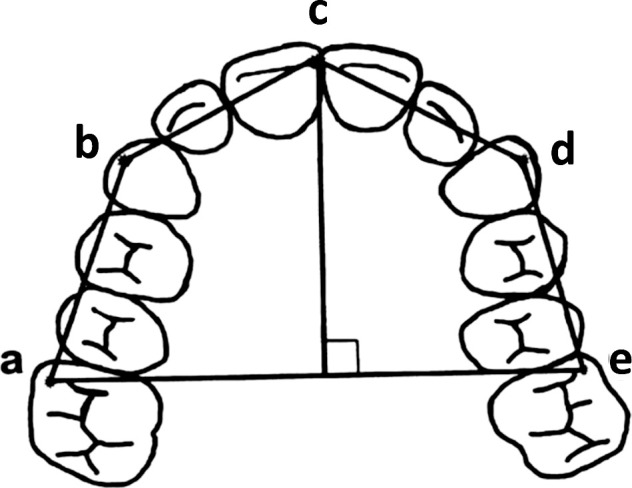
Maxillary arch dimensions. Arch width: distance between the mesio-buccal cusps of the maxillary first molars (a–e); Arch length: distance from point c to line a–e; Arch perimeter: the sum of distances a–b, b–c, c–d, and d–e.
Figure 2.
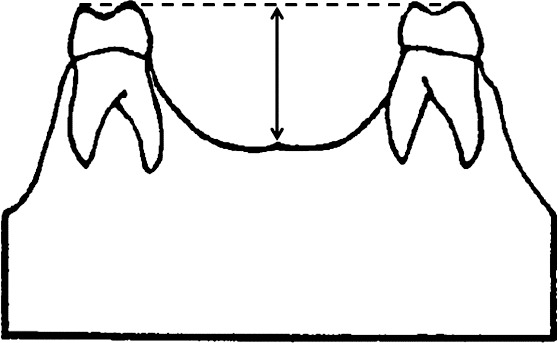
Arch depth: distance from the intermolar plane (between the mesio-buccal cusps of the first molars) to the palate.
Acoustic Measurements
Voice parameters (Fundamental frequency f0_sustained, Habitual pitch f0_count, Jitter, and Shimmer) were measured using acoustic analysis prior to the initiation of any orthodontic treatment. Acoustic analysis was performed using Visi-Pitch IV (model 3300; KayPENTAX, Montvale, NJ), along with a condenser microphone (SHURE SM 48, coupled to the PENTAX Visi-Pitch IV 3950B) used at a distance of 15 cm from the mouth. The participant's vocal signal was recorded into the system between 2:00 and 5:00 PM to rule out the daily variations and time influence on the voice parameters. The fundamental frequency was computed as an average of the fundamental frequencies for vocalization in a time window of 2 seconds selected by a cursor while the patient was sustaining the vowel [a]. Jitter, reported as a percent, represented a valuation or estimate of the pitch period variability within the sample analyzed in percent, thus representing the very short-term variability referred to as cycle-to-cycle variation in pitch. Shimmer percent was also reported as a percentage and refers to very short-term peak-to-peak amplitude variability.18
The habitual frequency was recorded by asking the patient to count from 1 to 10 in a normal voice. Each participant was asked to pronounce the vowels [a, i, o, u] for 5–7 seconds at a comfortable pitch and intensity in order to record the different formant frequencies (F1, F2, F3, and F4), which were determined by placing the cursor in the middle of the vowel formant band for consistency.
Statistical Method
Descriptive statistics, including mean, standard deviation (SD), and range, were derived for the participants' characteristics as well as dental and acoustic measurements of the total sample. Pearson's correlation coefficients were used to measure the strength of associations between the different dental and voice parameters. Multiple linear regressions were computed for the predictions of different dental measurements, and R2 was used as a measure of the regression model performance between the dependent variables (dental measures) and the independent variables (voice parameters). Statistical significance was set at a P-value <.05, and the analyses were performed using Stata/SE™ (College Station, TX: StataCorp LP.) data analysis and statistical software (version 11.1).
RESULTS
Demographic Data
A total of 35 subjects (12 males and 23 females) were enrolled in the study. The mean age was 11.41 ± 1.46 years, with age ranging from 8 to 13.7 years. All subjects were in the prepubertal stage of growth. The mean age of the female group was 11.45 ± 1.28 years, and that of the male group 11.32 ± 1.81 years (Table 1).
Table 1.
Means and Standard Deviations (SDs) of Age, Arch Dimensions, and Voice Parameters
| Females |
Males |
Total |
||||
| Mean |
(SD) |
Mean |
(SD) |
Mean |
(SD) |
|
| N | 23 | 12 | 35 | |||
| Age, y | 11.45 | 1.28 | 11.32 | 1.81 | 11.41 | 1.46 |
| Intermolar width, mm | 48.74 | 2.91 | 51.42 | 3.37 | 49.66 | 3.29 |
| Arch depth, mm | 17.99 | 1.79 | 18.40 | 2.55 | 18.14 | 2.06 |
| Arch length, mm | 28.62 | 2.84 | 28.68 | 2.75 | 28.65 | 2.77 |
| Arch perimeter, mm | 80.31 | 4.30 | 82.85 | 5.01 | 81.19 | 4.65 |
| Fundamental frequency–F0, Hz | 236.8434 | 23.46488 | 206.6743 | 46.64744 | 226.4997 | 35.65621 |
| Habitual frequency, Hz | 236.3422 | 22.80691 | 202.3717 | 52.9096 | 224.6951 | 38.85765 |
| Jitter, % | 1.107217 | 0.479491 | 1.184667 | 0.550324 | 1.133771 | 0.498137 |
| Shimmer, % | 4.280391 | 1.432317 | 5.238667 | 2.432314 | 4.608943 | 1.858626 |
Means of Maxillary Arch Dimensions
The mean intermolar width was 49.66 ± 3.29 mm, arch depth was 18.14 ± 2.06 mm, arch length was 28.65 ± 2.77 mm, and arch perimeter was 81.19 ± 4.65 mm (Table 1).
Voice Parameters
Fundamental frequency f0 average was 226.49 ± 35.85 Hz, and habitual frequency average was 224.69 ± 38.85 Hz. The stratification by gender is shown in Table 2. The means and SDs of the first four formants, F1–F4 for the vowels [a, i, o, u], for the total sample, are displayed in Table 3.
Table 2.
Means and Standard Deviations (SDs) of Formant Frequencies for Vowels /a/, /i/, /o/, and /u/
| /a/ |
/i/ |
/o/ |
/u/ |
|||||
| Mean, Hz |
SD |
Mean, Hz |
SD |
Mean, Hz |
SD |
Mean, Hz |
SD |
|
| F1 | 830.8286 | 122.7114 | 481.0571 | 91.60046 | 572.7429 | 98.67276 | 472.2941 | 122.1962 |
| F2 | 1488.771 | 124.1723 | 2688.543 | 408.6057 | 1193.229 | 242.5064 | 1069 | 307.7506 |
| F3 | 3134.343 | 297.3406 | 3451.371 | 334.7757 | 3079.086 | 314.4737 | 3126.879 | 399.2855 |
| F4 | 4031.029 | 238.7724 | 4141.323 | 198.0812 | 3970.8 | 228.3087 | 4036.645 | 201.1148 |
Table 3.
Associations between Arch Dimensions and Voice Parameters
| Fundamental Frequency–F0 |
Habitual Frequency |
Jitter |
Shimmer |
|||||
|
r |
P-Value |
r |
P-Value |
r |
P-Value |
r |
P-Value |
|
| Arch width | −0.52* | .0014 | −0.51* | .0014 | 0.075 | .6692 | −0.20 | .2576 |
| Arch depth | −0.2158 | .2132 | −0.28 | .1074 | −0.48* | .0038 | −0.21 | .2272 |
| Arch length | −0.09 | .5963 | −0.16 | .3663 | −0.15 | .3871 | 0.11 | .5429 |
| Arch perimeter | −0.39* | .0222 | −0.34* | .0475 | −0.12 | .506 | 0.17 | .317 |
* statistically significant
Associations between Arch Dimensions and f0_Sustained, f0_Count, Jitter, and Shimmer
There was a moderate significant negative correlation between arch width and f0 (r = −0.52; P = .0014) and Habitual frequency (r = −0.51; P = .0014) (Table 3). Similarly, the arch perimeter correlated moderately and at a significant level with f0 (r = −0.39; P = .022) and Habitual frequency (r = −0.34; P = .04). Neither the arch width nor the arch depth had any significant correlation with the Jitter and Shimmer, unlike arch depth, which correlated significantly with Jitter (r = −0.48; P = .0038) (Table 4).
Table 4.
Correlations Between Formant Frequencies and Arch Dimensions
| Arch Width |
Arch Depth |
Arch Length |
Perimeter |
|||||
|
r |
P- Value |
r |
P- Value |
r |
P- Value |
r |
P- Value |
|
| F1 | ||||||||
| /a/ | −0.21 | .23 | −0.02 | .92 | 0.02 | .89 | −0.11 | .54 |
| /i/ | −0.25 | .14 | 0.06 | .74 | −0.28 | .10 | −0.31 | .07 |
| /o/ | 0.16 | .36 | 0.16 | .36 | −0.06 | .72 | −0.08 | .63 |
| /u/ | 0.24 | .16 | 0.07 | .68 | 0.06 | .76 | 0.35 | .04* |
| F2 | ||||||||
| /a/ | −0.28 | .10 | −0.11 | .55 | −0.06 | .74 | −0.02 | .89 |
| /i/ | −0.06 | .74 | −0.20 | .24 | −0.05 | .79 | 0.01 | .97 |
| /o/ | 0.09 | .61 | 0.39 | .02* | 0.10 | .58 | 0.11 | .55 |
| /u/ | 0.27 | .13 | 0.32 | .06 | 0.06 | .72 | 0.24 | .18 |
| F3 | ||||||||
| /a/ | −0.33 | .05 | −0.43 | .01* | −0.42 | .01* | −0.44 | .01* |
| /i/ | −0.13 | .45 | −0.65 | .00* | −0.12 | .50 | −0.23 | .18 |
| /o/ | −0.37 | .03* | 0.00 | .99 | −0.29 | .09 | −0.37 | .03* |
| /u/ | −0.26 | .15 | −0.35 | .05* | −0.19 | .28 | −0.26 | .15 |
| F4 | ||||||||
| /a/ | −0.12 | .48 | −0.11 | .55 | −0.38 | .02* | −0.29 | .09 |
| /i/ | −0.22 | .24 | −0.10 | .60 | 0.10 | .58 | −0.25 | .17 |
| /o/ | −0.20 | .25 | 0.03 | .85 | −0.48 | .00* | −0.28 | .10 |
| /u/ | 0.07 | .69 | −0.28 | .13 | −0.42 | .02* | 0.07 | .71 |
Statistically significant.
Associations between Arch Dimensions and Formant Frequencies
Arch depth and arch length had the highest significant negative correlations with formant frequencies of the voice. On one hand, arch depth significantly correlated with formant F3, with r = −0.44, −0.65, and −0.35 for vowels /a/, /i/, and /u/, respectively (Table 4). On the other hand, arch length associated with formant F4 for the vowels /a/, /o/, and /u/, with r = −0.38, −0.48, and −0.42, respectively. In addition, arch depth had a statistically significant positive correlation with F2 for the vowel /o/, with r = 0.39. F3 was the only formant that had statistically significant correlations with all maxillary arch dimensions (Table 4).
Prediction Models
Multiple linear regression models were performed to predict arch depth based on voice parameters. A significant regression equation was found (P < .001; R2 = 0.49). All of the predictors were from the frequencies of the third formant F3 vowels. Arch depth decreased 0.3 mm for every 100 Hz of F3/i/, while adjusting for F3/a/ and F3/u/. Although F3a and F3u were included in the final model, they were not significant predictors of arch depth (Table 5).
Table 5.
Multiple Linear Regression Model for the Prediction of Arch Deptha
| Predictors |
β |
SE |
P-Value |
95% CI |
R2 |
| F3a | −0.0020 | 0.0010 | .057 | −0.0041: 0.0001 | 0.4929 |
| F3i | −0.0033 | 0.0009 | .001 | −0.0051: −0.0014 | |
| F3u | 0.0003 | 0.0008 | .703 | 0.0013: 0.0019 |
SE indicates standard error; CI, confidence interval. P-value for the model: P = .0002.
Similarly, multiple linear regressions were calculated to predict arch width based on voice parameters. A significant regression equation was found (P < .001; R2 = 0.37). Arch width decreased 4.5 mm for each 100-Hz increase of the fundamental frequency F0 and 0.33 mm for each 100-Hz increase of F3/o/. Both F0 and F3o were significant predictors for arch width (Table 6).
Table 6.
Multiple Linear Regression Model for the Prediction of Arch Widtha
| Predictors |
β |
SE |
P-Value |
95% CI |
R2 |
| F0 | −0.0451 | 0.0130 | .002 | −0.0716: −0.0186 | 0.3704 |
| F3o | −0.0033 | 0.0015 | .031 | −0.0063: −0.0003 |
SE indicates standard error; CI, confidence interval. P-value for the model: P = .0006.
DISCUSSION
The vocal tract shapes acoustically the vocal signal emitted at the level of the vocal folds. As a resonator, its configuration is extremely important for propelling and amplification of the various sound frequencies.19 Indeed, measurements such as oropharyngeal width and vocal tract length have been intimately correlated with the position and dispersion of the formants, which represent individual vocal characteristics and attributes. For instance, F1 and F2 are primarily responsible for the vowel color, whereas F3, F4, and F5 relate more to the personal voice timbre.20
Given the intricate relationship between the shape of the vocal tract and sound, it may be that there is an association between arch dimensions, the speaking fundamental frequency, and its formants. The results of this investigation indicated a mild to moderate negative correlation between arch width and perimeter and f0_sustained and f0_count. More so, arch depth significantly correlated with formant F3 for vowels /a/, /i/, and /u/, and arch length was associated with formant F4 for the vowels /a/, /o/, and /u/. The formant that correlated the most with arch dimensions was F3. What was more noticeable was the predictive value of F3/i/ for arch depth and of F3/o/ for arch width.
Based on numerous reports, the findings of this study are not surprising. The results of Marunick and Menaldi21 on palatal dimensions helped in stratifying singers into different vocal groups. In that pilot study on nine professional female singers, the depth and volumes of the maxillary dental arch were predictive of the vocal classification as soprano, mezzo, or alto. The palatal measurements were taken from an impression of the palatal arch, and the voice samples were based on several acoustic analyses conducted before voice classification was made.21 In another radiologic study by Roers et al.22 using 132 images taken from students who were classified as soprano, mezzosoprano, alto, tenor, baritone, and bass, the results indicated that the total vocal tract length varied with voice classification and that sopranos had the shortest vocal tract compared to others.
These findings are commensurate with the fact that one can also tune his or her voice by narrowing, widening, lengthening, or shortening the vocal tract. This is done using the articulators, such as the tongue, mandible, and lips, to modulate the vocal tract and thus manipulate the position of the vocal formants. For instance, protruding the lips or lowering the larynx can lower all the formants, and constrictions of the vocal tract, on the other hand, can raise these formants.20
Each formant is modulated preferentially by a given articulator. For instance, F1 is affected mainly by movement of the mandible, whereas F2 is mostly sensitive to the shape and position of the tongue. The third formant is determined primarily by the size of the oral cavity, and the fourth and fifth formants are very much dependent on the configuration of the lower pharynx and larynx. Indeed, the results of this investigation, which indicated the presence of a significant negative correlation between F3 and arch depth, did corroborate the strong association between F3 and size of the oral cavity. More importantly, F3/i/ and F3/o/ were significant predictors of arch depth and width, respectively. Similarly, the negative correlation reported in this investigation between arch length and F4 for the vowels /a/, /o/, and /u/ is in alignment with the association between vocal tract length and all formants. An increase in the length of the vocal tract, part of which is the palatal arch, results in a decrease in F1 to F4 with alteration in their dispersion. The results of Roers et al.22 confirmed the strong interplay between vocal tract dimensions and formant frequencies. The length of the vocal tract, in particular the length of the pharyngeal cavity, varies significantly with the different vocal classifications.22
This study provided further information on the strong association between vocal parameters and morphology of the vocal tract. It confirmed previous reports on the relationship between oral and pharyngeal cavity dimensions and the formant frequencies. It also represents a step forward toward the establishment of palatal and oropharyngeal models that can predict the vocal characteristics of a speaker and assist vocal teachers in classifying voices into the right vocal categories and matching the right tessitura to singing students. Nevertheless, this study also had two main limitations: the relatively small number of subjects and the fact that all subjects were prepubertal. A future investigation that takes into account the age of participants may be more widely applicable to adults.
CONCLUSIONS
There is a significant association between arch dimensions, particularly arch length and depth and voice.
The formant most predictive of arch depth and width is the third formant.
There is a pronounced negative correlation between F3 and arch depth and between F4 and arch length.
REFERENCES
- 1.Lee JW, Kang HG, Choi JY, Son YI. An investigation of vocal tract characteristics for acoustic discrimination of pathological voices. Biomed Res Int. 2013;Vol. No. 1:2013:758731. doi: 10.1155/2013/758731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Titze I. Principles of Voice Production 2nd ed. Iowa City, Iowa: National Center for Voice and Speech;; 2000. [Google Scholar]
- 3.Jesus LM, Martinez J, Hall A, Ferreira A. Acoustic correlates of compensatory adjustments to the glottic and supraglottic structures in patients with unilateral vocal fold paralysis. Biomed Res Int. 2015;Vol. No.3:2015:704121. doi: 10.1155/2015/704121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fitch WT, Giedd J. Morphology and development of the human vocal tract: a study using magnetic resonance imaging. J Acoust Soc Am. 1999;106(3 Pt 1):1511–1522. doi: 10.1121/1.427148. [DOI] [PubMed] [Google Scholar]
- 5.Evans S, Neave N, Wakelin D. Relationships between vocal characteristics and body size and shape in human males: an evolutionary explanation for a deep male voice. Biol Psychol. 2006;72:160–163. doi: 10.1016/j.biopsycho.2005.09.003. [DOI] [PubMed] [Google Scholar]
- 6.Hamdan AL, Safadi B, Chamseddine G, Kasty M, Turfe ZA, Ziade G. Effect of weight loss on voice after bariatric surgery. J Voice. 2014;28:618–623. doi: 10.1016/j.jvoice.2014.03.004. [DOI] [PubMed] [Google Scholar]
- 7.Sataloff RT. Clinical anatomy and physiology of the voice. In: Sataloff RT, editor. Professional Voice: The Science and Art of Clinical Care, 4th ed. San Diego, Calif: Plural Publishing;; 2017. pp. 157–196. [Google Scholar]
- 8.Evans S, Neave N, Wakelin D, Hamilton C. The relationship between testosterone and vocal frequencies in human males. Physiol Behav. 2008;93:783–788. doi: 10.1016/j.physbeh.2007.11.033. 18; [DOI] [PubMed] [Google Scholar]
- 9.González J. Formant frequencies and body size of speaker: a weak relationship in adult humans. J Phon. 2004;32:277–287. [Google Scholar]
- 10.Hamdan AL, Al-Barazi R, Tabri D, et al. Relationships between acoustic parameters and body mass analysis in young males. J Voice. 2012;26:144–147. doi: 10.1016/j.jvoice.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 11.Hamdan AL, Al Barazi R, Khneizer G, et al. Formant frequency in relation to body mass composition. J Voice. 2013;27:567–571. doi: 10.1016/j.jvoice.2012.09.005. [DOI] [PubMed] [Google Scholar]
- 12.Franco D, Fragoso I, Andrea M, Teles J, Martins F. Somatotype and body composition of normal and dysphonic adult speakers. J Voice. 2017;31:132.e9–132.e21. doi: 10.1016/j.jvoice.2015.11.020. [DOI] [PubMed] [Google Scholar]
- 13.Macari AT, Karam IA, Ziade G, et al. Association between facial length and width and fundamental frequency. J Voice. 2017;31:410–415. doi: 10.1016/j.jvoice.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 14.Macari AT, Ziade G, Khandakji M, Tamim H, Hamdan AL. Effect of rapid maxillary expansion on voice. J Voice. 2016;30:760.e1–760.e6. doi: 10.1016/j.jvoice.2015.09.013. [DOI] [PubMed] [Google Scholar]
- 15.LeBlanc EM, Cisneros GJ. The dynamics of speech and orthodontic management in cleft lip and palate. In: Shprintzen RJ, Bardach J, editors. Cleft Palate Speech Management: A Multidisciplinary Approach. St Louis, Mo: Mosby;; 1995. pp. 305–326. [Google Scholar]
- 16.Paley JS, Cisneros GJ, Nicolay OF, LeBlanc EM. Effects of fixed labial orthodontic appliances on speech sound production. Angle Orthod. 2016;86:462–467. doi: 10.2319/052415-351.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kulak Kayikci ME, Akan S, Ciger S, Ozkan S. Effects of Hawley retainers on consonants and formant frequencies of vowels. Angle Orthod. 2012;82:14–21. doi: 10.2319/032911-226.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kay Elemetrics Corp. Disordered Voice Database, Version 1.03. Boston, Mass: MEEI, Voice and Speech Lab; 1994. (CD-ROM) [Google Scholar]
- 19.Petrovic-Lazic M, Jovanovic N, Kulic M, Babac S, Jurisic V. Acoustic and perceptual characteristics of the voice in patients with vocal polyps after surgery and voice therapy. J Voice. 2015;29:241–246. doi: 10.1016/j.jvoice.2014.07.009. [DOI] [PubMed] [Google Scholar]
- 20.Sundberg J, Rossing TD. The science of singing voice. J Acoust Soc Am. 1990;87:462–463. [Google Scholar]
- 21.Marunick MT, Menaldi CJ. Maxillary dental arch form related to voice classification: a pilot study. J Voice. 2000;14:82–91. doi: 10.1016/s0892-1997(00)80097-1. [DOI] [PubMed] [Google Scholar]
- 22.Roers F, Mürbe D, Sundberg J. Voice classification and vocal tract of singers: a study of x-ray images and morphology. J Acoust Soc Am. 2009;125:503–512. doi: 10.1121/1.3026326. [DOI] [PubMed] [Google Scholar]