

Abstract
This study identified subgroups of adolescents with distinct patterns of involvement with overt and relational in-person and cyber aggression and victimization. We also assessed subgroup similarities and differences in exposure to adverse childhood experiences (ACEs), exposure to community violence, and trauma symptoms. Using latent class analysis, we identified three subgroups among 265 adolescents (Mage = 14.3 years; 57% female; 96% African American) residing in three urban high-burden communities that included youth who reported: (a) combined (cyber and in-person) aggression and victimization (17%), (b) in-person aggression and victimization (51%), and (c) adolescents with limited involvement (32%). Youth in the combined aggressive-victims subgroup had the highest probability of endorsing exposure to community violence, trauma symptoms, and a higher number of ACEs overall as well as higher rates of both verbal and physical abuse compared to the other subgroups. Our results indicated that the adolescents who reported the highest frequencies of aggressive behavior were also the most victimized and traumatized. These findings provide context to aggressive behavior among adolescents living in high-burden, urban communities and underscore the need for trauma-informed prevention interventions.
Keywords: adolescence, adverse childhood experiences, aggression, cyber aggression, latent class analysis
1 |. INTRODUCTION
Many adolescents experience aggression via in-person and electronic communications (e.g., texting, social media), both of which are associated with negative mental health outcomes for perpetrators and victims (e.g., Kowalski et al., 2014; Reijntjes et al., 2011). In-person and cyber aggression include acts that are overt (i.e., threats of physical harm and teasing) or relational (e.g., social exclusion and spreading rumors) (Mehari & Farrell, 2018). Cyber aggression may be used to reach wider audiences more anonymously and cyber victimization can be more pervasive, as content can remain on social media indefinitely (Kowalski et al., 2014). In a U.S. national survey of adolescents ages 13–17, approximately 1 in 3 African American adolescents identified social media as their primary method of communication, and adolescents whose families fell in the lowest income bracket (<$30,000 annually) were most likely to use social media to contact friends (Lenhart et al., 2015). Yet, few studies have identified patterns of in-person and cyber aggression and victimization among adolescents, and none to our knowledge focused on minority youth living in U.S. high-burden urban communities.
Adolescents living in under-resourced areas are more likely to experience stressful experiences that can negatively impact their development (García Coll et al., 1996), such as youth violence, exposure to community violence, child maltreatment, and other adverse experiences (e.g., Zimmerman & Messner, 2013). African American youth are overrepresented in communities with structural risk factors for youth violence and child maltreatment, such as concentrated poverty, high residential density, and elevated levels of neighborhood disorganization (Molnar et al., 2016; Nation, 2018; Sampson et al., 1997). Living in areas of concentrated poverty has been identified as a key risk factor for higher rates of violence exposure among African American versus European American youth (Zimmerman & Messner, 2013). Although empirical evidence consistently supports relations between peer aggression and exposure to community violence, trauma symptoms, and adverse experiences (Duke et al., 2010; Thompson & Farrell, 2019), most studies to date have overlooked empirical research and theory highlighting distinct patterns of aggression and/or victimization among adolescents. The current study identified patterns of peer aggression and victimization (including both in-person and cyber forms) among a predominantly African American sample of adolescents living in urban communities that are experiencing a high-burden from violence and determined whether the identified groups differed in their exposure to community violence, trauma symptoms, and adverse childhood experiences (ACEs).
1.1 |. Patterns of in-person, cyber aggression, and victimization
Prior research has highlighted the value of subgroup analysis for understanding the covariation of aggression and victimization and informing interventions. Studies have consistently identified four subgroups of youth based on their pattern of involvement in aggression and victimization: (a) youth who are mostly victimized, (b) youth who are mostly aggressive, (c) youth with limited involvement in aggression and victimization, and (d) youth who are both aggressive and victimized (i.e., aggressive-victims; O’Connor, 2021). Much of what we know about risk factors for aggression and victimization is based on studies using variable-centered approaches, which precludes understanding of the potentially unique risk factors for aggressive-victims and thus may impact the efficacy of interventions targeting risk factors for aggression or victimization (O’Connor, 2021). Aggressive-victims are theorized to be at a higher risk for long-term mental health challenges and future involvement in violence relative to youth with other patterns of involvement in aggression and victimization (Schwartz et al., 2001), in part because they are more likely to experience risk factors for and consequences of both aggression and victimization (O’Connor et al., 2019). This hypothesis has been partially corroborated through studies focused on in-person aggression and victimization; however, findings are inconsistent overall, and most prior studies have relied on arbitrary cutoffs rather than person-centered methods to define subgroups (for a systematic review, see O’Connor, 2021). Furthermore, most studies using a person-centered approach to examine patterns of aggression and victimization have focused solely on in-person forms of aggression and victimization. However, some of these studies did include African American adolescents living in urban, under-resourced areas (e.g., Bettencourt et al., 2013; O’Connor et al., 2019).
We identified only two studies that used a person-centered approach to identify subgroups with distinct patterns of in-person and cyber forms of aggression and victimization (i.e., Antoniadou et al., 2019; Liu et al., 2021). Both studies focused on bullying, a severe form of aggression that involves repeated and intentional acts of aggression and a power imbalance between the perpetrator and victim (Olweus, 1993). Antoniadou et al. (2019) found support for four subgroups in a sample of 1097 Greek early adolescents: (a) “uninvolved” (75%); (b) “bully/victims” (11%); (c) “bullies” (6%); and (d) “victims” (8%). Notably, both bullies and bully/victims exhibited elevated (i.e., above the sample mean) levels of cyber-bullying perpetration and victimization, but in-person victimization was only elevated among bullies and victims. Liu et al. (2021) similarly found support for four subgroups among a representative sample of 12,642 adolescents in the United States: (a) “severe bully-victims” (7%), (b) “moderate bullies” (7%), (c) “moderate victims” (27%), and (d) “not involved” (59%). Severe bully-victims had the highest probability of endorsing cyber-bullying and cyber-victimization, whereas all other subgroups had a relatively low probability of endorsing these indicators. The response patterns for in-person aggression and victimization were similar to those seen in prior studies focused solely on in-person forms (e.g., O’Connor et al., 2019). Taken together, the findings of these studies suggest that cyber forms of aggression and victimization play a distinct role in distinguishing aggressor/victim subgroups rather than simply mirroring the patterns of in-person aggression and victimization. This is consistent with evidence that cyber and in-person aggression and victimization are two distinct (yet correlated) forms of aggression (e.g., Farrell et al., 2020; Mehari & Farrell, 2018). Nevertheless, it remains unclear whether these findings can be generalized to racial and ethnic minority adolescents residing in high-burden urban communities, which may be particularly important given Liu et al. (2021) finding that severe bully-victims had lower family SES levels and included a higher proportion of African American youth than in the non-involved subgroup.
1.2 |. Correlates of patterns of in-person, cyber aggression, and victimization
Little is known about relations between patterns of in-person and cyber aggression and victimization and trauma symptoms, exposure to community violence, and ACEs given that prior research has focused on primarily on examining psychosocial correlates of aggressor/victim subgroups (e.g., Antoniadou et al., 2019). The lack of literature examining exposure to violence and trauma symptoms across subgroups of aggressive and victimized youth is surprising considering the salient influence of both factors on the psychosocial and behavioral adjustment of youth (e.g., McDonald & Richmond, 2008). For instance, a study of a large sample of primarily White adolescents found that the risk of violence perpetration increased by 35%–144% for each adverse event an adolescent endorsed (Duke et al., 2010). There is a burgeoning criminological literature linking greater exposure to ACEs with an increased likelihood of gang involvement (Wolff et al., 2020), serious, violent, and chronic offending (e.g., Baglivio et al., 2015), and, for boys in particular, offending throughout the life course (e.g., Craig et al., 2017). Along with historically identified ACEs, exposure to community violence, in particular incidents involving guns, is an ACE related to higher levels of externalizing behavior (Rajan et al., 2019). Developmental traumatology underscores that trauma induced by ACEs can create stress-induced neurological changes (e.g., emotional and behavioral dysregulation) that increase the chance of further victimization or aggressive responses to perceived threats (De Bellis et al., 1999). Thus, the correlates we examined may provide insight into differences in emotion dysregulation and social-cognitive risk factors across patterns of aggression and victimization that were found in previous studies and described in theory (e.g., Bettencourt et al., 2013; O’Connor et al., 2019; Schwartz et al., 2001).
1.3 |. The current study
Using latent class analysis (LCA), we identified patterns of in-person and cyber aggression and victimization in a sample of primarily African American adolescents living in three under-resourced urban communities. The only prior studies to our knowledge that examined patterns of in-person and cyber aggression perpetration and victimization focused on European adolescents (Antoniadou et al., 2019) or a nationally representative sample of adolescents in the United States (Liu et al., 2021) and the extent to which the patterns that were identified can be generalized to other socio-demographic groups remains unclear. Based on existing research and theory (e.g., Antoniadou et al., 2019; Schwartz et al., 2001), we hypothesized four subgroups of adolescents characterized by (a) predominant aggressors, (b) predominant victims, (c) aggressive-victims, and (d) limited involvement. It was difficult to make specific hypotheses about the function of cyber and in-person aggression perpetration and victimization due to limited prior studies and, more specifically, the lack of prior studies among ethnic minority youth in urban contexts. However, we did expect engagement in cyber and in-person forms to function as distinct constructs such that they may vary within and across subgroups (Antoniadou et al., 2019; Liu et al., 2021).
Our second aim was to examine whether identified subgroups differed based on adolescents’ age, sex, or community. These analyses were exploratory, given mixed evidence regarding the effects of demographic characteristics on adolescents’ pattern of involvement in aggression and victimization, particularly in urban, high-burden areas (e.g., Bettencourt et al., 2013). Finally, we explored the extent to which the identified subgroups differed based on youths’ levels of exposure to community violence, ACEs, and trauma symptoms. Although psychosocial correlates have been assessed (e.g., Antoniadou et al., 2019; Liu et al., 2021) no studies examined correlates including exposure to community violence, ACEs, and trauma symptoms. Relative to youth with other patterns of involvement, we expected that youth who reported engagement in aggression and victimization would endorse higher levels of these correlates, particularly if they also endorsed both in-person and cyber forms.
2 |. METHODS
2.1 |. Setting and participants
Data were collected from June 2018 to April 2019 from adolescents residing in three high-burden urban communities in the Southeastern United States as a part of a project evaluating a community-level approach to youth violence prevention. The communities consisted primarily of subsidized housing and were selected due to having high rates of violence and crime. The effects of community-level interventions were tested using a multiple baseline design that included three participating communities (1, 2, and 3). Data in the present study were collected at baseline before beginning any intervention activities. Participants were 265 adolescents ages 12–17 (M = 14.3 years old, SD = 1.7) and median family income of $10,000 or less. There were slightly more female participants (56%). The majority of participants who disclosed their race endorsed African American as either their sole racial identity (88%) or as one of multiple racial identities (8%).
2.2 |. Procedure
The University’s Institutional Review Board approved all study procedures. A neighborhood canvasing approach was used to recruit eligible families and written parental permission and adolescents’ assent was obtained before data collection. A total of 67% of eligible families identified participated in the study, which is consistent with other community-based studies (e.g., Kliewer et al., 2018). Computerized surveys (using REDcap) were administered to adolescents in their home or another convenient place (e.g., local community center) based on each family’s preference, with most surveys (96%) being administered in the home. Adolescents completed the surveys using headphones and could opt to skip any question. Study staff were present to address any questions. Adolescents took approximately one hour to complete the survey (M = 59.6 min) and received $25 for their participation.
2.3 |. Measures
2.3.1 |. Physical, relational, cyber aggression, and victimization
Aggression and peer victimization were measured using subscales from the problem behavior frequency scale–adolescent report version 2 (PBFS-AR) (Farrell et al., 2016, 2020). Items assessing aggression began with, “In the last 3 months, how many times have you…” and those assessing victimization began with, “In the last 3 months, how many times has this happened to you…” All subscales were scored on a Likert-type scale with responses ranging from 1 (Never) to 6 (20 or more times). We used a subset of 18 items drawn from the following PBFS-AR subscales: physical aggression (3 items), physical victimization (3 items), relational aggression (3 items), relational victimization (3 items), cyber aggression (3 items), and cyber victimization (3 items). All items included from this measure are listed in Table 1. The PBFS-AR has shown measurement invariance across gender, grade, and settings as well as concurrent validity with measures of beliefs, peer associations, and problem behaviors (Farrell et al., 2020). Subscales demonstrated acceptable internal consistency in the current study ranging from 0.81 to 0.89.
TABLE 1.
Descriptive statistics for latent class indicators and correlates among primarily African American adolescents living in urban, high-burden communities
| M | SD | 1 | 2 | 3 | |
|---|---|---|---|---|---|
| 1.Violent victimization | 0.4 | 0.5 | – | ||
| 2.Witnessing community violence | 1.1 | 0.8 | 0.697* | – | |
| 3.Trauma symptoms | 21.3 | 9.5 | 0.409* | 0.412* | – |
| 4.Number of ACEs endorsed | 2.1 | 1.8 | 0.244* | 0.348* | 0.364* |
| % | n | |
|---|---|---|
| ACEs | ||
| Verbal abuse | 13.8 | 34 |
| Physical abuse | 11.9 | 29 |
| Sexual abuse | 7.5 | 19 |
| Emotional neglect | 28 | 70 |
| Physical neglect | 4.7 | 12 |
| Parental separation/divorce | 64.6 | 157 |
| Exposure to IPV | 10.2 | 25 |
| Substance abuse by a household member | 12.8 | 32 |
| Mentally ill household member | 13.1 | 33 |
| Incarcerated household member | 50.2 | 123 |
| Latent class indicators | ||
| Hit or slapped someone | 41.8 | 107 |
| Shoved or pushed someone | 44.7 | 115 |
| Thrown something at someone to hurt them | 26.1 | 67 |
| Made fun of someone to make others laugh | 48.2 | 124 |
| Not let someone be in your group anymore because you were mad at them | 32.3 | 83 |
| Spread a false rumor about someone | 14.8 | 38 |
| Used text-messaging to make fun of someone | 16.8 | 43 |
| Posted rude comments about someone you know online | 12.9 | 33 |
| Spread rumors about someone you know online or through texting | 12.1 | 31 |
| Someone hit you hard enough to hurt | 25.7 | 65 |
| Someone pushed or shoved you | 38.2 | 97 |
| Someone threw something at you to hurt you | 21.3 | 54 |
| Someone made fun of you to make others laugh | 45.3 | 115 |
| Someone left you out on purpose when it was time to do an activity | 26.3 | 67 |
| Someone spread a false rumor about you | 30.6 | 77 |
| Someone used text-messaging to make fun of you | 22.0 | 56 |
| Someone posted rude comments about you online | 18.0 | 46 |
| Someone spread rumors about you online or by texting | 17.1 | 43 |
Note: N = 261; n for each variable ranged from 246 to 257 due to missing data.
Abbreviations: ACE, adverse childhood experience; IPV, intimate partner violence.
p < .001.
2.3.2 |. Exposure to community violence
A modified version of the Survey of Children’s Exposure to Community Violence Long Form (Richters & Saltzman, 1990) was used to measure exposure to community violence. The scale included 33 items and assessed both witnessing violence (19 items) and violent victimization (11 items) in the past 3 months. Three items that assessed lifetime exposure to three forms of severe violence were excluded from the measure. Thirty items began with the question, “In the last 3 months, how many times have you…” For example, “…been chased by someone who wanted to hit, jump, or attack you?” Response options were on a five-point Likert scale and ranged from 0 (never) to 4 (more than six times). Scale scores for victimization and witnessing were calculated by averaging across items within a scale. The subscales demonstrated good reliability (witnessing violence, α = .93; victimization, α = .84).
2.3.3 |. Adverse childhood experiences
Childhood stressors, trauma, abuse, and neglect were assessed using the ACEs questionnaire (Murphy et al., 2007). The scale includes 10 items to determine emotional, physical, and sexual abuse; emotional and physical neglect; witnessing intimate partner violence (IPV), parental marital discord, substance abuse, mental illness, and incarceration of a household member. The stem of the original measure was changed from, “During your first 18 years of life…” to read, “During your whole life…” because respondents were between the ages of 12 and 17. Response options included “yes” or “no.” For example, “Did a parent or other adult in the household often… swear at you, insult you, put you down, or humiliate you? or Act in a way that made you afraid that you might be physically hurt?” This scale had acceptable reliability (α = .66).
2.3.4 |. Trauma symptoms
The child report of posttraumatic symptoms (Greenwald & Rubin, 1999) was used to measure trauma symptoms including avoidance, intrusive thoughts and memories, and psychological arousal. The 26-item scale includes instructions to, “Mark how true each statement feels for you in the past week.” For example, “I try to forget about bad things that have happened.” Respondents rated each item from 0 (None) to 2 (Lots). One item (i.e., “my future looks bad”) was not included in scoring the measure per Greenwald and Rubin (1999). The total score was calculated by taking the sum across items, with scores ranging from 0 to 50 and scores of 19 or higher indicating clinical concern. The scale’s alpha coefficient was .90.
2.4 |. Data analysis
All analyses were conducted with Mplus version 8.4 (Muthén & Muthén, 1998–2017). Four participants were excluded due to missing data on the latent class indicators. We estimated a series of unconstrained latent class models using items assessing in-person (both physical and relational) and cyber forms of aggression and victimization as latent class indicators. We used model fit statistics, previous research and theory, and subgroup size considerations to inform our decision regarding the optimal number of subgroups (Masyn, 2013). We compared several fit indices across models specifying one through six classes, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and sample-size adjusted BIC (aBIC), with lower values indicating better fitting models (Masyn, 2013). We also examined the significance of the Lo-Mendell-Rubin likelihood ratio test (LMR-LRT) to determine whether the addition of another class significantly improved the fit of the model. We examined entropy and condition number as indications of classification quality and model identification, respectively. We employed the manual three-step Bolck, Croon, and Hagenaars method (Asparouhov & Muthén, 2021) to test relations between subgroups and hypothesized correlates. Missing data for correlates was addressed using Full Information Maximum Likelihood. The effect of age, sex, and community on subgroup membership was evaluated with a Wald test. Female adolescents and Community 2 served as the reference group. Community 2 was selected as the reference group given that community was the most geographically isolated area from resources. We examined differences in ACEs across subgroups using the same approach (i.e., latent class regression with covariates). Finally, differences in community violence exposure (i.e., witnessing and violent victimization), trauma symptoms, and the total number of ACEs endorsed across subgroups were examined.
3 |. RESULTS
3.1 |. Descriptive statistics
Descriptive statistics for trauma symptoms, exposure to violence, and ACEs are shown in Table 1. These constructs correlated in the expected direction. Notably, the mean level of trauma symptoms among participants is 21.3 (SD = 9.5), which suggests that youth in the sample are, on average, exhibiting trauma symptoms at a level of clinical concern (i.e., ≥19; Greenwald & Rubin, 1999). The indicators were highly skewed, with low endorsement rates (0% to 8%) in the highest response categories (i.e., 3–5 times, 6–9 times, 10–19 times, 20 or more times). Thus, to reduce the number of parameters in the model, to avoid any cells with values of zero, and to facilitate interpretation of the response patterns, all indicators were dichotomized to reflect 0 (never) and 1 (1 or more times) within the past three months. Prevalence rates for PBFS-AR items in the current study are presented in Table 1.
3.2 |. Latent class enumeration
We selected 18 items from the PBFS-AR that represented nine parallel forms of in-person (i.e., relational and physical) and cyber forms of aggression and victimization (see Figure 1). We intentionally selected an equal number of items within each PBFS-AR subscale (i.e., physical, relational, cyber) to avoid placing more weight on any one type of aggression during the enumeration process. In doing so, we considered endorsement rates and the conceptual importance of the items. We excluded items that were endorsed by less than 10% of participants because of evidence that aggressive-victims tend to make up about 10% of adolescent samples (e.g., O’Connor et al., 2019).
FIGURE 1.
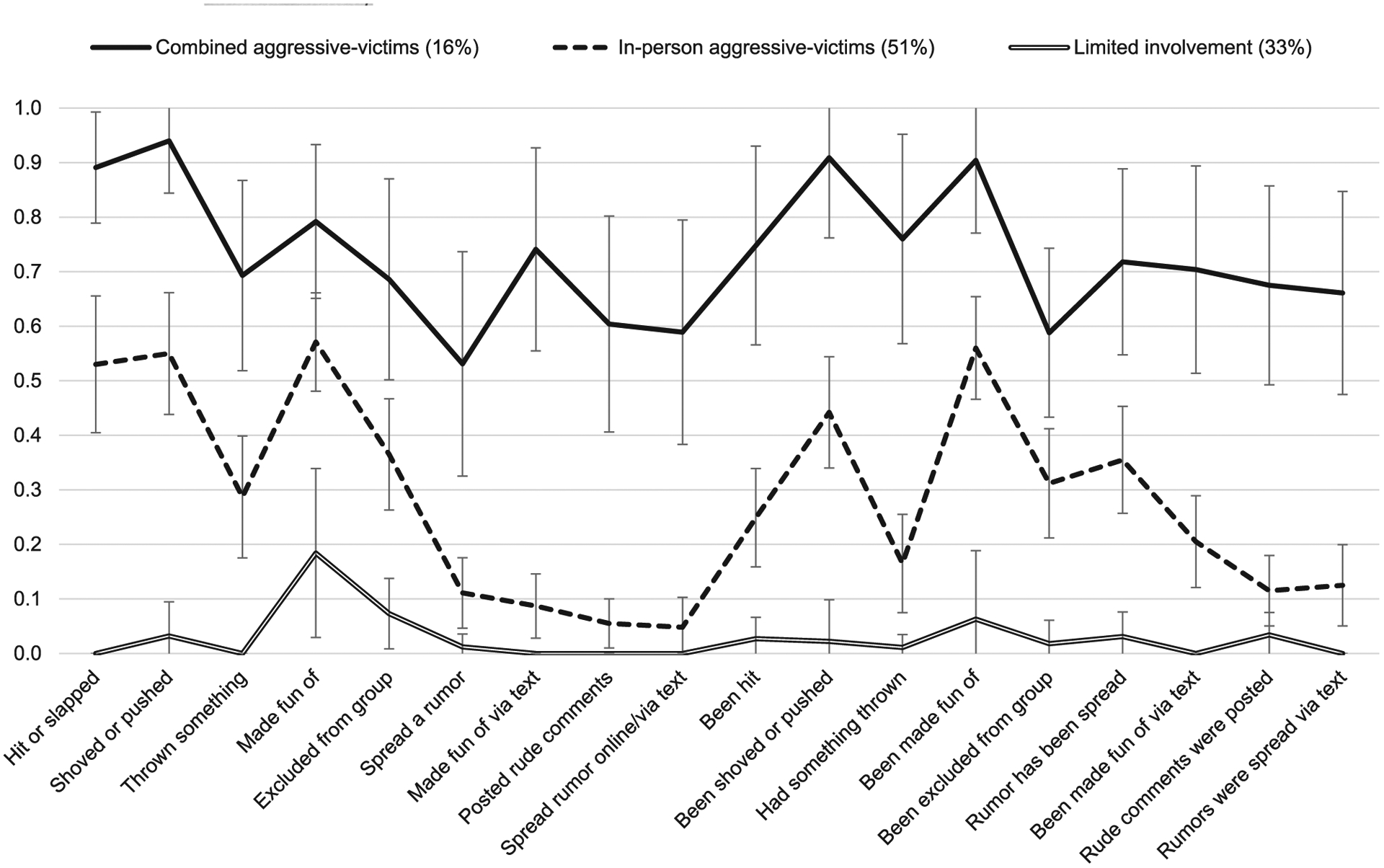
Item probability plot for the three-class model among primarily African American adolescents living in urban, high-burden communities. Error bars represent 95% confidence intervals
We compared fit statistics across models specifying one to six latent classes with 18 latent class indicators that represent in-person and cyber forms of aggression and victimization (see Table 2). In contrast to our hypotheses and previous studies using LCA (e.g., Antoniadou et al., 2019; Bettencourt et al., 2013), we found clear support for a three-class solution. The four-class model had a slightly lower BIC than the three-class model and the AIC and aBIC continued to decline as the number of classes increased across models. Per the recommendations of Masyn (2013), we examined a scree plot of these information criteria across k-class models to identify the point at which the decrease in each criterion’s value plateaued (e.g., the “elbow” on the scree plot). This approach identified a two- or three-class model as potential solutions. We then examined the results of the LMR-LRT and VLMR-LRT, which indicate that the three-class model significantly improves upon the fit of the two-class model, yet the four-class model does not significantly improve upon the fit of the three-class model. The three-class model demonstrated good separation between subgroups and homogeneity within subgroups (i.e., average posterior class probabilities were above 0.8 for each class). The entropy, condition number, and bivariate residuals of the three-class model were also satisfactory. Examination of item response probabilities within each subgroup (Figure 1) were consistent with the following patterns: (a) combined aggressive-victims (16%), represented by participants who had a moderate to high probability of endorsing indicators of physical, relational, and cyber aggression and victimization; (b) in-person aggressive-victims (51%), represented by participants who had a moderate to high probability of endorsing of physical and relational (but not cyber) aggression and victimization; and (c) limited involvement (33%), represented by participants who had a low probability of endorsement across nearly all latent class indicators.
TABLE 2.
Fit indices for LCA models with 1–6 latent classes among primarily African American adolescents living in urban, high-burden communities
| No. of classes | No. of parameters | LL | AIC | BIC | aBIC | VLMR-LRT (p Value) | LMR-LRT (p Value) | Entropy | Condition number | Smallest class size (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 18 | −2545.1 | 5126.2 | 5190.4 | 5133.3 | – | – | – | 0.03290 | 100.0% |
| 2 | 37 | −2117.7 | 4309.4 | 4441.3 | 4324.0 | 0.002 | 0.002 | 0.879 | 0.00879 | 35.6% |
| 3 | 56 | −2004.4 | 4120.8 | 4320.4 | 4142.8 | 0.003 | 0.003 | 0.894 | 0.00389 | 16.1% |
| 4 | 75 | −1949.7 | 4049.4 | 4316.7 | 4079.0 | 0.085 | 0.087 | 0.866 | 0.00100 | 13.8% |
| 5 | 94 | −1909.2 | 4006.5 | 4341.5 | 4043.5 | 0.306 | 0.309 | 0.888 | 0.00333 | 12.3% |
| 6 | 113 | −1873.2 | 3972.5 | 4375.3 | 4017.0 | 0.029 | 0.030 | 0.894 | 0.10345 | 10.3% |
Note: VLMR-LRT, LMR-LRT, and Entropy not applicable for 1-class model. N = 261.
Abbreviations: aBIC, sample-adjusted BIC; AIC, Akaike’s Information Criterion; BIC, Bayesian Information Criterion; LCA, latent class analysis; LL, Loglikelihood; LMR-LRT, Lo-Mendell-Rubin adjusted likelihood ratio test; VLMR-LRT, Vuong-Lo-Mendell-Rubin likelihood ratio test.
3.3 |. Correlates of subgroup membership
Subgroup membership did not differ by sex (χ2 (2) = 1.21, p = .546), age (χ2 (2) = 1.45, p = .485), or community (χ2 (4) = 2.44, p = .655).Nevertheless, these variables remained in the model as covariates. We found significant differences across subgroups in their reported levels of exposure to community violence, including both witnessing (χ2 (2) = 66.81, p < .001) and violent victimization (χ2 (2) = 45.97, p < .001), and posttraumatic stress symptoms (χ2 (2) = 71.67, p < .001). Relative to the limited involvement subgroup, combined aggressive-victims and in-person aggressive-victims reported higher levels of witnessing community violence (ds = 1.47 and 0.65, respectively, ps < .001), violent victimization (d = 1.44 and 0.35, respectively, ps < .001), and posttraumatic stress symptoms (d = 1.40 and 0.63, respectively, ps < .001). Compared with in-person aggressive victims, combined aggressive-victims reported significantly higher levels of witnessing community violence (d = 0.82, p < .001), violent victimization (d = 1.10, p < .001), and posttraumatic stress symptoms (d = 0.77, p < .001).
Subgroups differed in their total number of ACEs experienced (χ2 (2) = 20.03, p < .001), with combined aggressive-victims reporting a greater number of ACEs on average compared with in-person aggressive-victims (d = 0.56, p < .001) and the limited involvement subgroup (d = 0.93, p < .001). Additionally, subgroups differed significantly in their endorsement of specific ACEs, including verbal abuse (χ2 (2) = 9.00, p = .011), physical abuse (χ2 (2) = 9.28, p = .010), and emotional neglect (χ2 (2) = 14.90, p = .001) (see Figure 2). Specifically, adolescents reporting a history of verbal abuse (odds ratio [OR] = 4.41, p = .045), physical abuse (OR = 2.63, p = .048), or emotional neglect (OR = 2.54, p = .018) had higher odds than those who did not endorse each item of being classified in the combined aggressive-victims subgroup. We also found that the proportion of youth who had been exposed to IPV in their home differed across subgroups (χ2 (2) = 10.40, p = .006). However, odds ratios were not statistically significant for any of the subgroups. This may be due to the small sample size (and thus large standard errors) for the combined aggressive-victims subgroup, as the odds of endorsing versus not endorsing exposure to IPV were quite high in this subgroup (OR = 4.39, p = .074). There were no significant differences across subgroups in rates of sexual abuse (χ2 (2) = 5.52, p = .063), physical neglect (χ2 (2) = 1.39, p = .499), parental divorce/separation (χ2 (2) = 4.64, p = .098), and having a household member who was an alcoholic or used street drugs (χ2 (2) = 2.85, p = .241), was incarcerated (χ2 (2) = 5.94, p = .051), or was mentally ill (χ2 (2) = 5.68, p = .058).
FIGURE 2.

Probability of endorsing ACEs by subgroup among primarily African American adolescents living in urban, high-burden communities. Error bars represent 95% confidence intervals
4 |. DISCUSSION
Positive relations between peer aggression and victimization and exposure to community violence, ACEs, and trauma symptoms have been found among adolescents (Duke et al., 2010; Thompson & Farrell, 2019). However, most studies have used a variable-centered approach, which does not account for the distinct patterns of peer aggression and victimization supported in the adolescent literature. Studies using a person-centered approach to identify patterns of peer aggression and victimization have mainly examined psychosocial correlates and not examined the role of adverse experiences or trauma symptoms in distinguishing subgroup membership (e.g., Antoniadou et al., 2019). Finally, few studies have identified patterns of peer aggression and victimization using items that assessed both in-person and cyber aggression and victimization. The current study addressed these limitations by identifying patterns of cyber and in-person aggression and victimization and examining relations between these patterns and exposure to community violence, ACEs, and trauma symptoms in a sample of primarily African American adolescents living in under-resourced, urban communities.
In contrast to our hypothesis that we would find support for four patterns of aggression and victimization, we identified three subgroups including combined (i.e., in-person and cyber) aggressive-victims (16%), in-person aggressive-victims (51%), and limited involvement (33%). These results differ from prior LCAs of in-person (e.g., Bettencourt et al., 2013; O’Connor et al., 2019) and of in-person and cyber aggression and victimization (Antoniadou et al., 2019; Liu et al., 2021) as we did not identify separate subgroups of youth who were mostly victimized or mostly aggressive. Nevertheless, our findings align with prior research suggesting that cyber forms of aggression are distinct from in-person forms (e.g., Liu et al., 2021; Mehari & Farrell, 2018), as we found two subgroups of aggressive-victims that were distinguished by their involvement (or lack thereof) in cyber aggression and/or victimization. Our sample was homogeneous based on race/ethnicity and community context, and future studies should determine whether our findings can be replicated across more diverse samples.
We did not find differences in subgroup membership by age, sex, or community. Previous research on gender differences in subgroup membership is mixed. Prior studies examining patterns of cyber and in-person aggression and victimization have found that girls are more likely than boys to be classified as victims (Liu et al., 2021) or have limited involvement (Antoniadou et al., 2019), and boys are more likely to be classified into aggressive subgroups (i.e., bullies, bully-victims; Antoniadou et al., 2019). The findings of studies examining only in-person forms of aggression are mixed, with some studies finding no evidence of gender differences (e.g., Bettencourt & Farrell, 2013) and others finding that boys are overrepresented in aggressive subgroups (e.g., O’Connor et al., 2019). Perhaps gender differences were not detected in the current study because physical and relational subtypes of aggression and victimization were co-occurring across both aggressive-victim subgroups. Our null results regarding age differences across subgroups is supported by previous findings that aggressive-victims are relatively stable in their subgroup membership over time (e.g., Bettencourt et al., 2013). Finally, our finding that subgroups did not differ by community was not surprising given that all three communities had similar socioeconomic, demographic, and geographical characteristics.
In considering correlates of subgroup membership, the key findings of our study were: (a) both subgroups of aggressive-victims were at elevated risk for exposure to violence, emotional neglect, and elevated trauma symptoms relative to the limited involvement subgroup; and (b) combined aggressive-victims report the highest levels of exposure to community violence and some ACEs, and exhibited clinically elevated levels of traumatic symptoms. These findings suggest an additive effect of cyber forms of peer victimization and aggression when combined with in-person forms. Not surprisingly, our findings are broadly consistent with prior LCAs of aggression and victimization in that the limited involvement subgroup experienced the lowest rates of psychosocial and behavioral difficulties (e.g., Liu et al., 2021; O’Connor et al., 2019). However, our findings are novel as they highlight correlates of subgroup membership that, to our knowledge, have not been examined in prior work (e.g., ACEs, exposure to community violence). Similar to Antoniadou et al. (2019) and Liu et al. (2021), the co-occurrence of in-person and cyber aggression and victimization was associated with the highest level of difficulties in psychosocial and behavioral health. Previous research has found that, relative to those with limited involvement, those with high levels of cyber and in-person aggression and victimization have greater difficulty communicating with peers, fewer friends, higher levels of callous-unemotional traits, less self-control, increased mental health problems, lower levels of parental monitoring and school belongingness, and are more likely to engage in substance use (Antoniadou et al., 2019; Liu et al., 2021). We added to this literature by demonstrating that higher levels of exposure to community violence (i.e., witnessing violence, violence victimization), trauma symptoms, and ACEs were found in a combined aggressor-victim subgroup as compared to in-person aggressor-victim and limited involvement subgroups.
4.1 |. Limitations
Several limitations of this study should be considered. First, the specificity of our sample limits the generalizability of our findings. However, we believe this focus was a relative strength of this study given most prior studies have recruited school-based samples and/or primarily White samples with a higher median income (Antoniadou et al., 2019; Liu et al., 2021). Second, given the cross-sectional design of this study, we are not able to determine the direction of effects among the observed relations. Prior studies have found evidence of bidirectional associations among constructs examined in this study (e.g., trauma and physical aggression; Thompson & Farrell, 2019). More research is needed to determine whether adolescents’ pattern of involvement in cyber and in-person aggression and victimization changes over time as a function of their exposure to adversity and trauma. Another limitation is our reliance on self-report data. Future studies should gather data from multiple informants (e.g., teachers, peers) to further understand relations among problem behaviors and trauma. Furthermore, future research should consider measures of propensity (e.g., self-control), as prior studies have documented a link between such factors and adolescent problem behaviors (e.g., Antoniadou et al., 2019). Additionally, the number of participants classified as physical, relational, and cyber aggressive-victims led to larger standard errors for this subgroup, which likely resulted in increased p values for some variables examined. Finally, although LCA provides many advantages over more commonly used cutoff methods, LCA is an exploratory method and subgroups can be identified in the sample regardless of whether they truly exist in the population.
4.2 |. Implications and conclusion
There are clear public health implications for understanding patterns of peer aggression and victimization and adverse experiences among adolescents from urban, high-burden communities; especially as adolescents who experience a confluence of adverse experiences are at risk for juvenile justice involvement (Craig et al., 2017). Our study findings and related research highlight a number of areas for further study. There are potential benefits from implementing trauma-informed interventions within youth-serving agencies. For example, schools can provide teachers and staff with training on identifying trauma symptoms among youth and the application of trauma-informed care in the classroom setting. Youth who require additional support may benefit from Trauma-Focused Cognitive Behavioral Therapy®, an evidence-based treatment for posttraumatic stress among children and adolescents (Cary & McMillen, 2012; de Arellano et al., 2014). Primary prevention strategies targeting ACEs and youth violence among those living in urban, high-burden communities are also warranted. These may include skill-based programs for youth (e.g., promoting alternative thinking strategies; Conduct Problems Prevention Research Group, 2010) and their parents (e.g., strong African American families; Brody et al., 2008), modifying the environmental characteristics of a community (e.g., vacant lot remediation, green space), and by providing high-quality childcare and education early in life (CDC, 2019; David-Ferdon et al., 2016).
At present, several gaps in our knowledge of the relation between cyber and in-person aggression exist, including (a) the direction of the relation between these forms of aggression, (b) factors that increase the risk of one form of aggression turning into another, (c) the risk factors for engaging in both in-person and cyber aggression, and (d) the protective factors that may weaken the relationship between these risk factors and in-person and cyber aggression outcomes. Although this study addressed the risk processes, longitudinal research is needed to explore how the co-occurrence of in-person and cyber aggression and victimization is related to exposure to violence, ACEs, and trauma over time. Also, more research is needed to understand the role of social media as a potential conduit for youth violence and the ways that threats of violence and acts of overt and relational aggression online may escalate the risk of these types of aggression in face-to-face interactions (Patton et al., 2014). More qualitative efforts would be useful to provide more information about the motivations for using or not using social media to aggress against peers, given our finding that not all aggressive-victims were involved in cyber forms of aggression and victimization. Finally, prospective studies are needed to understand the stability of subgroup membership across adolescence and whether more adolescents transition into the combined aggressive-victim subgroup during middle and/or high school.
ACKNOWLEDGMENTS
Research reported in this publication was supported by the Centers for Disease Control and Prevention (CDC), CDC Cooperative Agreement U01CE002766, and the Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD) (Grant number: F31HD100073). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC or NICHD.
Funding information
National Center for Injury Prevention and Control, Grant/Award Number: U01CE002766; Eunice Kennedy Shriver National Institute of Child Health and Human Development, Grant/Award Number: 5F31HD100073-02
Footnotes
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
REFERENCES
- Antoniadou N, Kokkinos C, & Fanti KA (2019). Traditional and cyber bullying/victimization among adolescents: Examining their psychosocial profile through latent profile analysis. International Journal of Bullying Prevention, 1, 85–98. 10.1007/s42380-019-00010-0 [DOI] [Google Scholar]
- de Arellano MAR, Lyman DR, Jobe-Shields L, George P, Dougherty RH, Daniels AS, & Delphin-Rittmon ME (2014). Trauma-focused cognitive-behavioral therapy for children and adolescents: Assessing the evidence. Psychiatric Services, 65(5), 591–602. 10.1176/appi.ps.201300255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asparouhov T, & Muthén B (2021). Auxiliary variables in mixture modeling, (Mplus Web Notes: No. 21, Version 11). Retrieved from http://www.statmodel.com/examples/webnotes/webnote21.pdf
- Baglivio MT, Wolff KT, Piquero AR, & Epps N (2015). The relationship between childhood adverse experiences (ACE) and juvenile offending trajectories in a juvenile offender sample. Journal of Criminal Justice, 43, 229–241. [Google Scholar]
- De Bellis MD, Baum AS, Birmaher B, Keshavan MS, Eccard CH, Boring AM, Jenkins FJ, & Ryan ND (1999). Developmental traumatology part I: Biological stress systems. Biological Psychiatry, 45(10), 1259–1270. 10.1016/S0006-3223(99)00044-X [DOI] [PubMed] [Google Scholar]
- Bettencourt A, Farrell A, Liu W, & Sullivan T (2013). Stability and change in patterns of peer victimization and aggression during adolescence. Journal of Clinical Child and Adolescent Psychology, 42(4), 429–441. 10.1080/15374416.2012.738455 [DOI] [PubMed] [Google Scholar]
- Bettencourt A, & Farrell AD (2013). Individual and contextual factors associated with patterns of aggression and peer victimization during middle school. Journal of Youth and Adolescence, 42(2), 285–302. 10.1007/s10964-012-9854-8 [DOI] [PubMed] [Google Scholar]
- Brody GH, Kogan SM, Chen Y, & McBride Murry V (2008). Long-term effects of the Strong African American Families Program on youths’ conduct problems. Journal of Adolescent Health, 43(5), 474–481. 10.1016/j.jadohealth.2008.04.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cary CE, & McMillen JC (2012). The data behind the dissemination: A systematic review of trauma-focused cognitive behavioral therapy for use with children and youth. Children and Youth Services Review, 34(4), 748–757. [Google Scholar]
- Centers for Disease Control and Prevention [CDC]. (2019). Preventing adverse childhood experiences: Leveraging the best available evidence. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/violenceprevention/pdf/preventingACES.pdf [Google Scholar]
- Conduct Problems Prevention Research Group. (2010). The effects of a multiyear universal social–emotional learning program: The role of student and school characteristics. Journal of Consulting and Clinical Psychology, 78(2), 156–168. 10.1037/a0018607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craig JM, Piquero AR, Farrington DP, & Ttofi M (2017). A little early risk goes a long bad way: Adverse childhood experiences and life-course offending in the Cambridge study. Journal of Criminal Justice, 53, 34–45. 10.1016/j.jcrimjus.2017.09.005 [DOI] [Google Scholar]
- David-Ferdon C, Vivolo-Kantor AM, Dahlberg LL, Marshall KJ, Rainford N, & Hall JE (2016). A comprehensive technical package for the prevention of youth violence and associated risk behaviors. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/violenceprevention/pdf/yv-technicalpackage.pdf [Google Scholar]
- Duke NN, Pettingell SL, McMorris BJ, & Borowsky IW (2010). Adolescent violence perpetration: associations with multiple types of adverse childhood experiences. Pediatrics, 125(4), e778–e786. 10.1542/peds.2009-0597 [DOI] [PubMed] [Google Scholar]
- Farrell AD, Sullivan TN, Goncy EA, & Le AT (2016). Assessment of adolescents’ victimization, aggression, and problem behaviors: Evaluation of the problem behavior frequency scale. Psychological Assessment, 28(6), 702–714. 10.1037/pas0000225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrell AD, Thompson EL, Mehari KR, Sullivan TN, & Goncy EA (2020). Assessment of in-person and cyber aggression and victimization, substance use, and delinquent behavior during early adolescence. Assessment, 27(6), 1213–1229. 10.1177/1073191118792089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- García Coll C, Crnic K, Lamberty G, Wasik BH, Jenkins R, Vasquez García H, & Pipes McAdoo H (1996). An integrative model for the study of developmental competencies in minority children. Child Development, 67, 1891–1914. 10.1111/j.1467-8624.1996.tb01834.x [DOI] [PubMed] [Google Scholar]
- Greenwald R, & Rubin A (1999). Assessment of posttraumatic symptoms in children: Development and preliminary validation of parent and child scales. Research on Social Work Practice, 9, 61–75. 10.1177/10497315990090010 [DOI] [Google Scholar]
- Kliewer W, Sosnowski DW, Wilkins S, Garr K, Booth C, McGuire K, & Wright A (2018). Do parent-adolescent discrepancies predict deviant peer affiliation and subsequence substance use? Journal of Youth and Adolescence, 47, 2596–2607. 10.1007/s10964-018-0875-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kowalski RM, Giumetti GW, Schroeder AN, & Lattanner MR (2014). Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychological Bulletin, 140, 1073–1137. 10.1037/a0035618 [DOI] [PubMed] [Google Scholar]
- Lenhart A, Smith A, Anderson M, Duggan M, & Perrin A (2015). Teens, technology, and friendships. Retrieved from the Pew Research Center website: https://www.pewresearch.org/internet/wp-content/uploads/sites/9/2015/08/Teens-and-Friendships-FINAL2.pdf
- Liu J, Gui S, Weissman R, & Liu H (2021). Investigating factors associated with bullying utilizing latent class analysis among adolescents. School Psychology International, 42, 11–32. 10.1177/0143034320967061 [DOI] [Google Scholar]
- Masyn K (2013). Latent class analysis and finite mixture modeling. In Little TD, & Nathan PE (Eds.), The Oxford handbook of quantitative methods in psychology, Vol. 2: Statistical analysis (pp. 551–611). Oxford University Press. [Google Scholar]
- McDonald C, & Richmond TR (2008). The relationship between community violence exposure and mental health symptoms in urban adolescents. Journal of Psychiatric and Mental Health Nursing, 15(10), 833–849. 10.1111/j.1365-2850.2008.01321.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehari K, & Farrell AD (2018). Where does cyberbullying fit? A comparison of competing models of adolescent aggression. Psychology of Violence, 8, 31–42. 10.1037/vio0000081 [DOI] [Google Scholar]
- Molnar BE, Goerge RM, Gilsanz P, Hill A, Subramanian SV, Holton JK, Duncan DT, Beatriz ED, & Beardslee WR (2016). Neighborhood-level social processes and substantiated cases of child maltreatment. Child Abuse & Neglect, 51, 41–53. 10.1016/j.chiabu.2015.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy A, Dube S, Steele M, & Steele H (2007) Clinical ACE and child clinical ACE questionnaires (Unpublished Manuscript).
- Muthén LK, & Muthén BO (1998–2017). Mplus user’s guide (8th ed.). Muthén & Muthén. [Google Scholar]
- Nation M (2018). Concentrated disadvantage in urban neighborhoods: Psychopolitical validity as a framework for developing psychology-related solutions. Journal of Community Psychology, 36, 187–198. 10.1002/jcop.20230 [DOI] [Google Scholar]
- O’Connor KE (2021). Psychosocial adjustment across aggressor/victim subgroups: A systematic review and critical evaluation of theory. Clinical Child and Family Psychology Review. Advance online publication. 10.1007/s10567-021-00347-3 [DOI] [PubMed] [Google Scholar]
- O’Connor KE, Farrell AD, Kliewer W, & Lepore S (2019). Social and emotional adjustment across aggressor/victim subgroups: Are aggressive-victims distinct? Journal of Youth and Adolescence, 48, 2222–2240. 10.1007/s10964-019-01104-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olweus D (1993). Victimization by peers: Antecedents and long-term outcomes. In Rubin KH, & Asendorpf JB (Eds.), Social withdrawal, inhibition, and shyness in childhood (pp. 315–341). Lawrence Erlbaum Associates. [Google Scholar]
- Patton DU, Hong JS, Ranney M, Patel S, Kelley C, Eschmann R, & Washington T (2014). Social media as a vector for youth violence: A review of the literature. Computers in Human Behavior, 35, 548–553. 10.1016/j.chb.2014.02.043 [DOI] [Google Scholar]
- Rajan S, Branas C, Myers D, & Agrawal N (2019). Youth exposure to violence involving a gun: Evidence for adverse childhood experience classification. Journal of Behavioral Medicine, 43(4), 646–657. 10.1007/s10865-019-00053-0 [DOI] [PubMed] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, Boelen PA, van der Schoot M, & Telch MJ (2011). Prospective linkages between peer victimization and externalizing problems in children: A meta-analysis. Aggressive Behavior, 37, 215–222. 10.1002/ab.20374 [DOI] [PubMed] [Google Scholar]
- Richters J, & Saltzman W (1990). Survey of exposure to community violence: Self report version. National Institute of Mental Health. [Google Scholar]
- Sampson R, Raudenbush S, & Earls F (1997). Neighborhoods and violent crime: A multilevel study of collective efficacy. Science, 277, 918–924. 10.1126/science.277.5328.918 [DOI] [PubMed] [Google Scholar]
- Schwartz D, Proctor LJ, & Chien DH (2001). The aggressive victim of bullying: Emotional and behavioral dysregulation as a pathway to victimization by peers. In Juvonen J, & Graham S (Eds.), Peer harassment in school: The plight of the vulnerable and victimized (pp. 147–174). Guilford. [Google Scholar]
- Thompson EL, & Farrell AD (2019). Longitudinal relations between trauma-related psychological distress and physical aggression among urban early adolescents. Journal of Clinical Psychology, 75, 1626–1642. 10.1002/jclp.22781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolff KT, Baglivio M, Klein H, Piquero AR, DeLisi M, & Howell J (2020). Adverse childhood experiences (ACEs) and gang involvement among juvenile offenders: Assessing the mediation effects of substance use and temperament deficits. Youth Violence and Juvenile Justice, 18(1), 24–53. 10.1177/1541204019854799 [DOI] [Google Scholar]
- Zimmerman GM, & Messner SF (2013). Individual, family background, and contextual explanations of racial and ethnic disparities in youths’ exposure to violence. American Journal of Public Health, 103(3), 435–442. 10.2105/AJPH.2012.300931 [DOI] [PMC free article] [PubMed] [Google Scholar]