

Abstract
The disease burden of AF is greater in Asia-Pacific than other areas of the world. Direct oral anticoagulants (DOACs) have emerged as effective alternatives to vitamin K antagonists (VKA) for preventing thromboembolic events in patients with AF. The Asian Pacific Society of Cardiology developed this consensus statement to guide physicians in the management of AF in Asian populations. Statements were developed by an expert consensus panel who reviewed the available data from patients in Asia-Pacific. Consensus statements were developed then put to an online vote. The resulting 17 statements provide guidance on the assessment of stroke risk of AF patients in the region, the appropriate use of DOACs in these patients, as well as the concomitant use of DOACs and antiplatelets, and the transition to DOACs from VKAs and vice versa. The periprocedural management of patients on DOAC therapy and the management of patients with bleeding while on DOACs are also discussed.
Keywords: AF, Asia, bleeding, consensus, non-vitamin K antagonist oral anticoagulants, vitamin K antagonist, haemostasis
With a proportionally larger older population, the disease burden of AF is greater in the Asia-Pacific region than other areas of the world. By 2050, approximately 72 million people in the area will have AF.[1]
Despite the potential risks of major bleeding, oral anticoagulation (OAC) has a clear net benefit as it is highly effective in preventing ischaemic strokes in AF patients.[2] Direct oral anticoagulants (DOACs) have emerged as alternatives to vitamin K antagonists (VKA) for the prevention of thromboembolic events (TEE) in AF patients.
DOACs interfere with thrombus formation by direct inhibition of thrombin or through inhibition of factor Xa (FXa), which converts prothrombin to thrombin.[3] Dabigatran etexilate mesylate is a competitive direct thrombin inhibitor, while rivaroxaban, apixaban and edoxaban are FXa inhibitors.
This consensus aims to guide clinicians to manage AF with reference to issues pertinent to Asia, such as the underuse of OAC and inappropriate dose reduction of DOAC. The authors were part of the guideline working committee and the guidelines were based on available evidence that were appraised based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) as:
High (authors have high confidence that the true effect is similar to the estimated effect).
Moderate (authors believe that the true effect is probably close to the estimated effect).
Low (true effect might be markedly different from the estimated effect).
Very low (true effect is probably markedly different from the estimated effect).[4]
Each author then indicated their agreement to each statement (agree, neutral or disagree) via an online poll. Consensus was considered to have been reached when 80% of votes were agree or neutral.
Indication for Direct Oral Anticoagulants in Patients with AF
Statement 1. DOAC use is recommended over warfarin in DOAC-eligible AF patients.
Level of evidence: High.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Consistent evidence from the RE-LY, ROCKET-AF, ARISTOTLE and the ENGAGE AF-TIMI 48 randomised controlled trials (RCTs), comparing DOACs with warfarin in AF patients demonstrated at least non-inferiority of DOACs for reducing stroke or systemic embolism (S/SE) risk, and a superior safety profiles with reduced intracranial haemorrhage (ICH) rates.[5–8]
Meta-analysis of these RCTs showed that DOACs significantly reduced S/SE risk compared with warfarin driven, at least in part, by reducing haemorrhagic strokes.[9] DOACs significantly reduced all-cause mortality and ICH but with increased risk of gastrointestinal bleeding. These results show that, compared with warfarin, DOACs have a favourable risk-benefit profile. The relative efficacy and safety of DOACs were consistent across a wide range of patients. Concurring real-world evidence showed that DOACs were associated with reduced ICH risk and similar rates of S/SE compared with warfarin.[10]
Consistent with other AF management guidelines and consensuses, this panel recommends DOAC use over warfarin in Asian DOAC-eligible AF patients.[11–14] This is supported by multiple Asian studies and systematic reviews documenting the efficacy and added safety of DOACs in preventing S/SE among AF patients.[15–21]
Statement 2. DOACs can be used in patients with valvular disease in the absence of moderate-to-severe mitral stenosis or mechanical heart valves.
Level of evidence: High.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
The inclusion and exclusion criteria of pivotal trials have been summarised elsewhere.[22] Patients with concomitant moderate-to-severe mitral stenosis or prosthetic/mechanical heart valves were excluded from pivotal RCTs.[5–8] It was demonstrated that compared to warfarin, dabigatran use increased TEE rates and bleeding complications in AF patients with mechanical heart valves; hence there is a lack of benefit and excess risk.[23] Conversely, patients with valvular heart disease who did not meet the exclusion criteria were included in pivotal trials.[5–8,22] An ongoing trial, INVICTUS-VKA (NCT02832544), aims to evaluate DOAC efficacy and safety compared with warfarin in patients with rheumatic heart disease.
Patients with non-AF indications for anticoagulation were excluded and few AF patients with hypertrophic cardiomyopathy (HCM) were included in these DOAC trials.[5–8] Large retrospective studies have demonstrated that DOAC-treated AF patients with HCM have comparable rates of S/SE and major bleeding and lower mortality than warfarin-treated patients.[24] Despite limited prospective data, AF patients with HCM may be eligible for DOACs.
DOACs have not been evaluated for use in pregnant women and children and should not be used for these patients. Table 1 summarises the recommended indications and contraindications for DOACs in AF patients.[25]
Table 1: Recommended Indications and Contraindications for Direct Oral Anticoagulant Use in AF Patients.
| Conditions | Eligibility for DOAC Therapy |
|---|---|
| Recommended for use | |
| AF in the absence of moderate-to-severe mitral stenosis or mechanical heart valves | Included in DOAC trials |
| Mild-to-moderate other native valvular disease (e.g. mild to moderate aortic stenosis or regurgitation, degenerative mitral regurgitation etc) | Included in DOAC trials |
| Bioprosthetic valve (>3 months postoperatively) | Acceptable for degenerative mitral regurgitation or in the aortic position Not advised if rheumatic mitral stenosis |
| Consider for use, although limited data | |
| Mitral valve repair (>3 months postoperatively) | Some patients included in some DOAC trials |
| Severe aortic stenosis | Limited data (excluded in RE-LY trial)[59] |
| Percutaneous transluminal aortic valvuloplasty; transcatheter aortic valve implantation | No published prospective data yet May require combination with single or dual antiplatelet therapy |
| Hypertrophic cardiomyopathy | Limited data but patients may be eligible for DOAC |
| Contraindicated | |
| Mechanical prosthetic valve | Contraindicated |
| Moderate-to-severe mitral stenosis (usually rheumatic origin) | Contraindicated |
| Pregnant women and children | No data available, not recommended |
DOAC = Direct oral anticoagulants. Source Steffel et al. 2018.[25] Adapted with permission from Oxford University Press.
Statement 3. The CHA2DS2-VASc score is well-validated; the CHA2DS2-VA score can be considered for use in practice.
Level of evidence: Low.
Level of agreement: 95% agree, 0% neutral, 5% disagree.
Stroke risk assessment forms a critical part of AF management.[11–14] The identification of AF patients at elevated stroke risk would allow targeted prescription of oral anticoagulation to the appropriate subgroup of AF patients with a favourable benefit-risk ratio.[26] Multiple clinical, anatomical and biochemical risk factors for stroke have been identified in AF patients.[27] However, a simple, reliable and widely accepted risk score such as the CHA2DS2-VASc would be more practical for front-line clinicians than a more complex risk score involving multiple other non-clinical factors, even if the latter is more accurate (with a marginally higher C statistic).[28,29]
Clinicians also need to be aware of the dynamic nature of individual components of the CHA2DS2-VASc risk score.[30,31] Almost half of AF patients initially at low stroke risk (CHA2DS2-VASc 0 or 1) are no longer low risk after a mean follow-up of 4 years.[32] The CHA2DS2-VASc score increases in about 12% of initially low-risk AF patients each year – hence it would be reasonable to reassess this risk score more frequently.[33]
Recent studies have attempted to improve the accuracy of the CHA2DS2-VASc score in several east Asian populations. Lower ages have been proposed for the scoring and hence initiation of anticoagulation.[34,35] If the tipping point for DOAC use was a stroke risk of 0.9% per year, there would be different age thresholds for Asian AF patients with different other single risk factors beyond gender.[26,36] However, having multiple age thresholds would increase the complexity of the CHA2DS2-VASc score. Until further data is available and a more widespread consensus develops among Asian AF physicians, it is reasonable to continue to use the traditional CHA2DS2-VASc score (as published in the 2020 European Society of Cardiology guidelines for the diagnosis and management of AF) for Asian patients.[37]
Sex category (Sc) in the CHA2DS2-VASc score is a stroke risk modifier rather than a risk factor per se.[38,39] If a more accurate stroke risk prediction is desired, the CHA2DS2-VASc score should be used.[40,41] However, if the intent of the physician in using the risk score is to determine when anticoagulation is indicated, as will be discussed in statement 4, and the threshold is determined to be CHA2DS2-VASc ≥1 for men and ≥2 for women, then Sc becomes unnecessary and CHA2DS2-VA can be reasonably used with a recommendation to start DOAC anticoagulation when CHA2DS2-VA ≥1.[42] This would provide a simplified and consistent threshold recommendation for both sexes as per the Australian AF guidelines.[43]
Statement 4. DOAC use is recommended in Asian AF patients with CHA2DS2-VA ≥1 or CHA2DS2-VASc ≥1 (for men) and ≥2 (for women).
Level of evidence: Moderate.
Level of agreement: 90% agree, 5% neutral, 5% disagree.
The annual incidence of stroke in Asians is generally higher than in white people, particularly for patients with CHA2DS2-VASc scores of 0–1 (Supplementary Table 1). Thus, while American and European guidelines recommend that OAC be considered in patients with >1 risk factor for stroke (besides being a woman), this panel recommends that DOACs be used in Asian patients with CHA2DS2-VA score ≥1.[11,14,37] If clinicians use the CHA2DS2-VASc score, then we recommend OAC be considered when CHA2DS2-VASc ≥1 (for men) and ≥2 (for women) as per current major AF guidelines.
It should be noted that HCM patients with a CHA2DS2-VASc / CHA2DS2-VA score of 0 should still be anticoagulated.[14]
Statement 5. Elderly patients should not be excluded from anticoagulation for stroke prevention and DOAC use is recommended over warfarin.
Level of evidence: High.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Post-hoc analyses of pivotal DOAC trials have been reviewed in another position paper; stroke risk-reduction benefits of DOACs, compared with warfarin, were maintained in both older and younger patients with no significant difference in overall major bleeding and ICH rates across all age groups.[44] These studies demonstrated that major bleeding risk markedly increased with age, underscoring the need for anticoagulation strategies with improved safety profiles to mitigate bleeding risk.[44] A meta-analysis of the four RCTs also showed that, compared with warfarin, DOACs decreased S/SE risk in people aged ≥75 years, without significant differences in the overall risk of major bleeding.[9] A retrospective observational study in elderly Taiwanese AF patients (aged ≥90 years) showed that, compared with warfarin, DOACs (dabigatran, rivaroxaban and apixaban) were associated with lower ICH risk and no difference in ischaemic stroke risk.[45]
These results, as well as those from other Asian studies, show that efficacy and safety of DOACs are preserved in elderly populations.[45,46] Since stroke and major bleeding risks increase with age, DOAC use is likely to yield greater absolute risk reduction and greater net clinical benefit in elderly populations when compared with warfarin.
In very old patients who may otherwise be considered ineligible for oral anticoagulation therapy due to frailty, some countries may consider lowering the dose if well-designed clinical trials have demonstrated the effectiveness of this strategy. A Phase III, multicentre, randomised, double-blind, placebo-controlled trial that included Japanese patients aged ≥80 years found low-dose edoxaban (15 mg once daily) reduced the risk of S/SE compared with placebo (p<0.001) although gastrointestinal bleeding was also increased in the edoxaban group.[47] However, in the absence of such compelling clinical data, the approved recommended doses should be used.
Statement 6. Aspirin or other antiplatelet agents should not be used for stroke risk management in AF patients.
Level of evidence: Moderate.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Current evidence does not support the use of aspirin and other antiplatelet agents for the management of the risk of stroke in AF patients.[48,49] A meta-analysis (n=13,000) showed that dose-adjusted warfarin was substantially more efficacious than antiplatelet therapy for stroke risk reduction in AF patients.[48] Warfarin was also superior to aspirin in preventing S/SE in AF patients ≥75 years without increasing major bleeding rates.[44,50]
With alternative therapeutic options available, such as warfarin, and DOACs having greater efficacy in stroke risk reduction and comparable overall safety profiles with aspirin, antiplatelet therapy should not be used for stroke-risk management in AF patients. This recommendation is consistent with other guidelines and consensus.[12–14]
Dose Regimens of Direct Oral Anticoagulants
Statement 7. Trial-approved doses of DOACs and/or doses recommended in respective country guidelines/regulations should be used, i.e. DOAC dose should not be reduced inappropriately.
Level of evidence: Low.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Only doses of DOACs evaluated in pivotal trials have been demonstrated to be at least non-inferior to warfarin in thromboembolic risk-reduction efficacy, with superior safety profiles in terms of reduced ICH risk.[5–8] A meta-analysis of landmark DOAC trials also demonstrated the safety profile of DOACs over warfarin in Asians and non-Asians with significant reductions in major bleeding and ICH.[51] Nonetheless, patients are frequently underdosed. A retrospective cohort study of about 15,000 AF patients treated with DOAC showed that 13.3% of patients with no renal indication for dose reduction were potentially underdosed.[52] The study also found that apixaban underdosing was associated with a fourfold increase in stroke risk with no statistically significant difference in major bleeding risk.[52] Several real-world studies in Asia also reported much higher rates of underdosing, ranging from 27% to 36% of patients with suboptimal outcomes.[53–56] Underdosed patients were generally found to have a higher ischaemic stroke risk compared to those receiving appropriate doses.
Except in countries where population-specific evidence demonstrated that reduced doses of DOACs are effective for thromboembolic risk reduction, trial-approved doses of DOACs should be used, even in Asian populations. Recommendations for DOAC dosing regimens with respect to approved dose-reduction criteria and renal function are summarised in Figure 1.
Figure 1: Direct Oral Anticoagulant Dosing with Respect to Renal Function.

*150 mg twice daily may be considered in suitable patients with low bleeding risk.†In appropriate countries where 10 mg dose is approved, 10 mg may be considered in suitable patients with high bleeding risk.‡In patients with CrCl 15–29 ml/min, recommended dose is 2.5 mg twice daily independent of age or body weight.§ Creatinine clearance estimated by the Cockcroft-Gault equation. CrCl = creatinine clearance.
Clinicians should also be mindful of the potential interaction of DOACs with other drugs, including herbal medicines and traditional Chinese medicine, especially those that modulate CYP3A4 and P-glycoprotein activity although data on these potential interactions are limited.[57] The clinical impact of these potential interactions is still not established, however, a literature review found 194 verified reports of interactions with anticoagulants or antiplatelets with 79.9% attributable to pharmacodynamic interactions.[58] Some of these interactions (mostly associated with danshen, dong quai, ginger, ginkgo, licorice, and turmeric) resulted in increased bleeding risks.
Statement 8. Rivaroxaban, apixaban and edoxaban can be used in patients with severe renal impairment – creatine clearance (CrCl) 15–29 ml/min – with appropriate dose adjustment.
Level of evidence: Low.
Level of agreement: 90% agree, 5% neutral, 5% disagree.
Safety and efficacy of DOACs relative to warfarin in patients with creatinine clearance (CrCl) 30–59 ml/min were consistent with that of patients with normal renal function.[59,60] All DOACs can be used in Asian patients with CrCl ≥30 ml/min (Figure 1).
The RE-LY trial showed that the 110 mg twice daily dose of dabigatran had similar thromboembolic risk reduction efficacy and lower major bleeding rates than warfarin.[5] The European Medicines Agency recommended that dabigatran be used at 110 mg twice daily in patients with CrCl 30–50 ml/min with high bleeding risk. Since Asians have higher risks of major bleeding and ICH compared with non-Asians, this panel recommends that dabigatran be used at 110 mg twice daily in AF patients with CrCl 30–50 ml/min.[44] Since dabigatran is predominantly (80%) eliminated via renal excretion, dabigatran use in patients with CrCl <30 ml/min is not recommended in agreement with European guidelines.[3,14]
DOAC RCTs mostly excluded patients with CrCl <30 ml/min and limited randomised data are available regarding DOAC use in patients with CrCl 15–29 ml/min. However, based on pharmacokinetic studies and renal excretion characteristics, FXa inhibitors have been approved in Europe for AF patients with CrCl 15–29 ml/min. Evidence from small retrospective studies also showed that reduced doses of FXa inhibitors in patients with CrCl 15–29 ml/min did not lead to increases in major bleeding or thrombotic events.[61,62]
Similar to other guidelines, this panel recommends that reduced doses of rivaroxaban, apixaban and edoxaban, but not dabigatran, can be considered for patients with CrCl 15–29 ml/min.[13,25] Various formulae to estimate CrCl result in slightly different values: the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) formulae generally result in higher values among patients with advanced age or low body weight compared with the Cockcroft-Gault (CG) formula.[63,64] These variability may lead to inappropriate dosing with the use of CKD-EPI or MDRD among these subgroups. Hence, guidelines recommend the use of the CG formula in CrCl estimation.[37,43,63]
Statement 9. Rivaroxaban and apixaban may be used in patients with end-stage renal disease on haemodialysis.
Level of evidence: Very low.
Level of agreement: 64% agree, 27% neutral, 9% disagree.
Pharmacokinetic studies showed no significant change in systemic exposure to FXa inhibitors pre- or post-haemodialysis, indicating that haemodialysis did not significantly impact FXa inhibitor clearence.[65]
Apixaban undergoes approximately 27% renal clearance.[65] Compared with subjects with normal renal function, systemic exposure of apixaban increased 36% with no increase in maximum plasma concentration in patients with end-stage renal disease (ESRD) (CrCl <15 ml/min) on haemodialysis. Rivaroxaban undergoes approximately 33% renal clearance and, compared with subjects with normal renal function, systemic exposure to rivaroxaban increased 56% in ESRD subjects on haemodialysis, an extent similar to patients with severe renal impairment (CrCl 15–29 ml/min) not undergoing dialysis.[65]
Recent registry-based studies also showed that compared with warfarin, rivaroxaban and apixaban use in AF patients with severe renal impairment or undergoing haemodialysis is associated with significantly less major bleeding events but no significant reduction in thromboembolic risk.[66,67] However, these studies did not specify the duration of OAC treatment and whether warfarin-treated patients were within therapeutic range. The RENAL-AF trial, which compared apixaban with warfarin in ESRD patients on haemodialysis, was terminated early with inconclusive findings relative to bleeding and stroke rates.[68]
Despite the current lack of prospective data, pharmacokinetic studies and real-world evidence suggest that rivaroxaban and apixaban may be used in ESRD patients on haemodialysis. Conversely, clinical and observational data to support edoxaban use in these patients are relatively lacking. Although the pharmacokinetic profile of edoxaban in ESRD patients on haemodialysis is similar to that of other FXa inhibitors, FDA labelling states that edoxaban is not recommended in patients with CrCl <15 ml/min.[65,69] This position may change should further evidence emerge, perhaps from the ongoing AXADIA study (NCT02933697).
Concomitant DOAC and Antiplatelet Use in AF Patients with Acute Coronary Syndrome or Who Have Undergone Percutaneous Coronary Intervention
Statement 10. Following percutaneous coronary intervention, triple therapy (DOAC + aspirin + P2Y12 inhibitor) is recommended for up to 1 month (keeping it as short as possible), and dual therapy (DOAC + P2Y12 inhibitor) is recommended for up to 12 months, after which the patient may be maintained on DOAC monotherapy.
Level of evidence: High.
Level of agreement: 95% agree, 5% neutral, 0% disagree.
Statement 11. The duration of triple therapy may be lengthened or shortened depending on the patient’s thrombotic and bleeding risks.
Level of evidence: Very low.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Early Triple Antithrombotic Therapy with DOAC + Aspirin + P2Y12 Inhibitor
Although optimal combination and duration of antithrombotic therapy in AF patients who have undergone percutaneous coronary intervention (PCI) are not well-established, expert consensus have recommended a short period of triple antithrombotic therapy in suitable patients.[11–14]
Four RCTs of AF patients who underwent PCI and/or presented concomitant acute coronary syndrome (ACS) showed that, compared with standard triple therapy (STT) of dose-adjusted warfarin plus dual antiplatelet therapy (DAPT), DOACs + P2Y12 inhibitor led to lower rates of major or clinically relevant bleeding.[70–74] Clinically significant bleeding occurred in 16.1% of aspirin-treated patients compared with 9% of patients receiving aspirin-matched placebo (p<0.001) in the AUGUSTUS trial.[71] Although not statistically significant, the rates of stent thrombosis in placebo-treated patients was almost twice that of patients treated with aspirin.[71] Stent thrombosis rates in the ENTRUST-AF PCI trial were also higher in the dual therapy group (edoxaban + P2Y12 inhibitor) than the STT group. However, these studies were not powered to detect statistically significant differences in stent thrombosis rates between treatment groups.[74]
Recent meta-analyses showed significantly increased stent thrombosis rates with early-dual versus triple antithrombotic therapy, which do not support the use of dual therapy immediately after PCI in Asian AF patients.[73] This panel recommends a short duration of triple therapy, of up to 1 month (keeping it as short as possible), following PCI in AF patients; duration of triple therapy may be tailored based on the relative thrombotic and bleeding risks before transitioning to dual therapy. For AF patients with ACS not undergoing PCI, early dual antithrombotic therapy (DOAC + P2Y12 inhibitor) is reasonable (Figure 2).
Figure 2: Antithrombotic Therapy in AF patients with Acute Coronary Syndrome or Post-percutaneous Coronary Intervention.
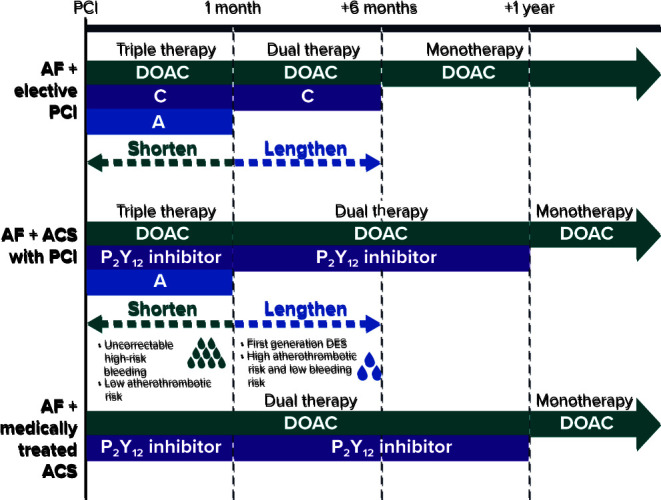
A = aspirin; ACS = acute coronary syndrome; DES = drug eluting stent; C = clopidogrel; PCI = percutaneous coronary intervention.
Mid-term Dual Antithrombotic Therapy with DOAC + P2Y12 Inhibitor
Several trials have demonstrated that dual therapy with DOAC + P2Y12 inhibitor reduced bleeding risk compared with STT.[70–72,74] Consistent with other guidelines, dual therapy is recommended for up to 12 months, corresponding to the duration evaluated in most trials (Figure 2).[13,14]
Long-term Monotherapy with Direct Oral Anticoagulants
The AFIRE trial in AF patients with chronic coronary artery disease showed that, compared with the combination group (rivaroxaban + single antiplatelet), rivaroxaban alone resulted in no significant difference in TEE but reduced bleeding events and mortality.[75] Global guidelines also recommend OAC monotherapy 12 months after PCI or ACS in AF patients.[12–14,25] DOAC monotherapy is recommended for most patients after 12 months post-PCI in line with statement 1, (Figure 2).
Transitioning to Direct Oral Anticoagulants from VKA and Vice Versa
Statement 12. When switching from VKA to DOAC, DOAC can be started the same day if the international normalised ratio (INR) <2 or the next day if INR is 2–3. If INR >3, INR should be reassessed after an appropriate interval as determined by the clinician, before deciding on when to switch from VKA to DOAC.
Level of evidence: Very low.
Level of agreement: 90% agree, 10% neutral, 0% disagree.
Major bleeding risk in patients with INR >3 is twice that of when INR = 2–3 while TEE risk increases by at least two-fold with INR <2.[14] Given the quick onset of action and short half-life of DOACs, these agents can be started on the same day if INR <2, or the following day if the patient is in the therapeutic INR range (2–3).[3] If INR >3, DOACs should be withheld until the INR is at the indicated threshold (Supplementary Figure 1).
Statement 13. When switching from DOAC to VKA, VKA should be started while the patient is on DOAC. DOAC can then be stopped once the INR >2 (if target INR is 2–3). INR should be reassessed 1–2 days after stopping DOAC.
Level of evidence: Very low.
Level of agreement: 95% agree, 5% neutral, 0% disagree.
VKAs have a slow onset of action and it may take days before the INR is in therapeutic range. Thus, DOAC and VKA should be administered concomitantly until the INR is in the appropriate therapeutic range. DOACs present in the body may also affect the accuracy of INR measurements.[25] Depending on the patient’s renal function, INR should be reassessed 1–2 days after DOAC discontinuation to ascertain INR levels while solely on VKA and ensure adequate anticoagulation.
Periprocedural Management
Statement 14. Avoid unnecessary or prolonged interruption of DOAC therapy for surgical procedures in AF patients.
Level of evidence: Moderate.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Statement 15. Parenteral anticoagulation overlap with DOAC therapy is not advised.
Level of evidence: Very low.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Unnecessary prolonged interruption of DOACs should be avoided given that periprocedural interruption/cessation of DOACs increased TEE risk by around 20-fold.[76] Patient characteristics, including age, renal function, history of bleeding complications and concomitant medications, should also be considered when deciding to discontinue or restart DOACs.
Recent evidence from the PAUSE cohort study, evaluating the safety of a standardised perioperative DOAC management strategy, showed that omitting FXa inhibitors one day before a procedure with a low-risk of bleeding and two days before a procedure with a high risk of bleeding was associated with a 30-day postoperative major bleeding rate of <2% and a stroke rate of <1%.[77]
Figure 3 summarises the bleeding risks associated with common elective procedures and the recommended intervals for DOAC interruption prior to these procedures. Less invasive procedures have a relatively low risk of severe bleeding and may not necessitate discontinuation; omitting one dose of DOAC before low-risk procedures may be considered to avoid nuisance bleeding episodes, which can contribute to DOAC therapy non-adherence. Consistent with other guidelines, complex left-sided ablation procedures may proceed with uninterrupted anticoagulation or after omitting one dose of DOAC.[78]
Figure 3: Periprocedural Management of Patients on Direct Oral Anticoagulants.

CrCl = creatinine clearance; ICD = implantable cardioverter defibrillator; VT = ventricular tachycardia.
In patients with renal impairment, a longer duration of DOAC interruption is recommended before procedures with moderate and high bleeding risk. As dabigatran undergoes extensive renal clearance, dabigatran should be stopped earlier than FXa inhibitors in patients with impaired renal function for these procedures.[3]
The quick onset of action of DOACs makes it feasible to time the interruption of DOACs before a procedure with a predictable decline of its anticoagulation effects.[3] Perioperative overlap of DOAC therapy with parenteral anticoagulation (‘bridging’) is not necessary and has been shown to increase major bleeding complications rates without reduction in cardiovascular events.[79] DOACs can be resumed after the procedure when the bleeding risk is deemed acceptable.
As with thrombotic risk, bleeding risk is also dynamic, as demonstrated by a Taiwanese study that included 19,566 AF patients treated with warfarin. After a follow-up of 93,783 person years, 61.8% of patients had a change in HAS-BLED score, and an increased score was associated with major bleeding.[80] This underscores the need to reassess bleeding risk before deciding to alter anticoagulant therapy.
Management of Bleeding That Occurs While on Direct Oral Anticoagulants
Statement 16. An institution-specific policy should be developed for managing bleeding events, placing focus on the (pro)haemostatic agents available as direct reversal agents which are not widely available for use.
Level of evidence: Very low.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
DOAC-related bleeding events will inevitably increase as the number of patients using DOACs rises. This panel recommends that hospitals implement institution-specific protocols for managing bleeding events as reversal agents are not uniformly available in Asia-Pacific hospitals and a wide diversity of (pro)haemostatic agents are available. Physicians may refer to the HAS-BLED score for identification and modification of bleeding risk factors such as adequate hypertension control, labile INR (on warfarin), excessive alcohol intake and concomitant antiplatelet therapy or non-steroidal anti-inflammatory drugs.[25] Managing these modifiable risk factors further minimises bleeding risk.
Bleeding management strategies for DOAC-treated patients depend on bleeding severity and on individual patient factors such as time of last DOAC intake. Figure 4 summarises the recommended management strategies for bleeding complications.
Figure 4: Strategies for Bleeding Management While on Direct Oral Anticoagulants.

aPCC = activated prothrombin complex concentrates; PCC = prothrombin complex concentrates.
Fresh frozen plasma (FFP) may be considered for volume expansion in major bleeding complications but FFP does not reverse DOAC anticoagulation. Use of direct reversal agents may be considered. Idarucizumab, a monoclonal antibody that binds dabigatran with a higher affinity than thrombin, reverses the anticoagulant effect of dabigatran within minutes when administered intravenously.[25] IV administration of andexanet alfa, a recombinant modified FXa decoy protein, neutralises the effects of direct and indirect FXa inhibitors immediately.[25]
Where direct reversal agents are unavailable, data from observational studies suggest that coagulation factors such as activated prothrombin complex concentrates may be used to achieve haemostasis in patients who experience life-threatening bleeding while on DOACs.[25]
Post-bleed Management of AF Patients
Statement 17. Following a major bleeding episode, DOAC should be restarted after the cause of bleed has been corrected. If the cause of bleed is not found, an interdisciplinary consensus should be reached for an individualised anticoagulation strategy.
Level of evidence: Low.
Level of agreement: 100% agree, 0% neutral, 0% disagree.
Whether to restart DOAC therapy after major bleeding episodes, such as ICH, gastrointestinal bleeding or a fall/trauma, is a common dilemma. OAC resumption in AF patients after ICH was associated with reduced TEE risk and overall mortality without increased risk of recurrent ICH compared with patients who did not resume OAC.[81] Although anticoagulation is contraindicated in those with a history of spontaneous ICH, the panel recommends that DOAC therapy be restarted if the cause of bleed, such as uncontrolled hypertension, has been reversed (Figure 5). Evidence is lacking about when to restart DOACs and timing and dose of DOACs when restarted after a major bleeding episode should be determined after a multidisciplinary discussion.
Figure 5: Management Strategy After Major Bleeding Episode.

LAA = left atrial appendage.
If the cause of the bleed has not been reversed, an individualised strategy for thrombotic risk management should be reached after a multidisciplinary discussion, weighing the patient’s thrombotic and recurrent bleeding risks. Left atrial appendage occlusion may be considered as an alternative in AF patients unsuitable for long-term anticoagulation (Figure 5).
Conclusion
The 17 statements in this paper provide guidance to front-line physicians on select contemporary issues in Asia, such as the underuse of OAC and inappropriate dose reduction of DOACs.
Supplementary Material
Acknowledgments
Medical writing support was provided by Tan Ee Min and Ivan Olegario of MIMS Pte Ltd.
References
- 1.Wong CX,, Brown A,, Tse HF et al. Epidemiology of atrial fibrillation: The Australian and Asia-Pacific perspective. Heart Lung Circ. 2017;26:870–9. doi: 10.1016/j.hlc.2017.05.120. [DOI] [PubMed] [Google Scholar]
- 2.Singer DE,, Chang Y,, Fang MC et al. The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med. 2009;151:297–305. doi: 10.7326/0003-4819-151-5-200909010-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Raval AN,, Cigarroa JE,, Chung MK et al. Management of patients on non-vitamin K antagonist oral anticoagulants in the acute care and periprocedural setting: a scientific statement from the American Heart Association. Circulation. 2017;135:e604–33. doi: 10.1161/CIR.0000000000000513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Balshem H,, Helfand M,, Schünemann HJ et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–6. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 5.Connolly SJ,, Ezekowitz MD,, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–51. doi: 10.1056/NEJMoa0905561. [DOI] [PubMed] [Google Scholar]
- 6.Patel MR,, Mahaffey KW,, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–91. doi: 10.1056/NEJMoa1009638. [DOI] [PubMed] [Google Scholar]
- 7.Granger CB,, Alexander JH,, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–92. doi: 10.1056/NEJMoa1107039. [DOI] [PubMed] [Google Scholar]
- 8.Giugliano RP,, Ruff CT,, Braunwald E et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–104. doi: 10.1056/NEJMoa1310907. [DOI] [PubMed] [Google Scholar]
- 9.Ruff CT,, Giugliano RP,, Braunwald E et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383:955–62. doi: 10.1016/S0140-6736(13)62343-0. [DOI] [PubMed] [Google Scholar]
- 10.Ntaios G,, Papavasileiou V,, Makaritsis K et al. Real-world setting comparison of nonvitamin-K antagonist oral anticoagulants versus vitamin-K antagonists for stroke prevention in atrial fibrillation: a systematic review and meta-analysis. Stroke. 2017;48:2494–503. doi: 10.1161/STROKEAHA.117.017549. [DOI] [PubMed] [Google Scholar]
- 11.January CT,, Wann LS,, Calkins H et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. 2019;140:e125–51. doi: 10.1161/CIR.0000000000000719. [DOI] [PubMed] [Google Scholar]
- 12.Joung B,, Lee JM,, Lee KH et al. 2018 Korean guideline of atrial fibrillation management. Korean Circ J. 2018;48:1033–80. doi: 10.4070/kcj.2018.0339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chiang CE,, Okumura K,, Zhang S et al. 2017 consensus of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation. J Arrhythm. 2017;33:345–67. doi: 10.1016/j.joa.2017.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kirchhof P,, Benussi S,, Kotecha D et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–962. doi: 10.1093/eurheartj/ehw210. [DOI] [PubMed] [Google Scholar]
- 15.Kohsaka S,, Katada J,, Saito K et al. Safety and effectiveness of non-vitamin K oral anticoagulants versus warfarin in real-world patients with non-valvular atrial fibrillation: a retrospective analysis of contemporary Japanese administrative claims data. Open Heart. 2020;7:e001232. doi: 10.1136/openhrt-2019-001232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ohshima A,, Koyama T,, Ogawa A et al. Oral anticoagulants usage in Japanese patients aged 18–74 years with non-valvular atrial fibrillation: a retrospective analysis based on insurance claims data. Fam Pract. 2019;36:685–92. doi: 10.1093/fampra/cmz016. [DOI] [PubMed] [Google Scholar]
- 17.Koretsune Y,, Yamashita T,, Yasaka M et al. Comparative effectiveness and safety of warfarin and dabigatran in patients with non-valvular atrial fibrillation in Japan: A claims database analysis. J Cardiol. 2019;73:204–9. doi: 10.1016/j.jjcc.2018.09.004. [DOI] [PubMed] [Google Scholar]
- 18.Kohsaka S,, Katada J,, Saito K,, Terayama Y. Safety and effectiveness of apixaban in comparison to warfarin in patients with nonvalvular atrial fibrillation: a propensity-matched analysis from Japanese administrative claims data. Curr Med Res Opin. 2018;34:1627–34. doi: 10.1080/03007995.2018.1478282. [DOI] [PubMed] [Google Scholar]
- 19.Cha MJ,, Choi EK,, Han KD et al. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants in Asian patients with atrial fibrillation. Stroke. 2017;48:3040–8. doi: 10.1161/STROKEAHA.117.018773. [DOI] [PubMed] [Google Scholar]
- 20.Chan YH,, Lee HF,, Chao TF et al. Real-world comparisons of direct oral anticoagulants for stroke prevention in Asian patients with non-valvular atrial fibrillation: a systematic review and meta-analysis. Cardiovasc Drugs Ther. 2019;33:701–10. doi: 10.1007/s10557-019-06910-z. [DOI] [PubMed] [Google Scholar]
- 21.Wang KL,, Chiu CC,, Giugliano RP et al. Drug class, renal elimination, and outcomes of direct oral anticoagulants in Asian patients: a meta-analysis. J Stroke Cerebrovasc Dis. 2018;27:857–64. doi: 10.1016/j.jstrokecerebrovasdis.2017.10.027. [DOI] [PubMed] [Google Scholar]
- 22.Di Biase L. Use of direct oral anticoagulants in patients with atrial fibrillation and valvular heart lesions. J Am Heart Assoc. 2016;5:e002776. doi: 10.1161/JAHA.115.002776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Eikelboom JW,, Connolly SJ,, Brueckmann M et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med. 2013;369:1206–14. doi: 10.1056/NEJMoa1300615. [DOI] [PubMed] [Google Scholar]
- 24.Jung H,, Yang PS,, Jang E et al. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation with hypertrophic cardiomyopathy: a nationwide cohort study. Chest. 2019;155:354–63. doi: 10.1016/j.chest.2018.11.009. [DOI] [PubMed] [Google Scholar]
- 25.Steffel J,, Verhamme P,, Potpara TS et al. The 2018 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39:1330–93. doi: 10.1093/eurheartj/ehy136. [DOI] [PubMed] [Google Scholar]
- 26.Eckman MH,, Singer DE,, Rosand J,, Greenberg SM. Moving the tipping point: the decision to anticoagulate patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2011;4:14–21. doi: 10.1161/CIRCOUTCOMES.110.958108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Alkhouli M,, Friedman PA. Ischemic stroke risk in patients with nonvalvular atrial fibrillation: JACC review topic of the week. J Am Coll Cardiol. 2019;74:3050–65. doi: 10.1016/j.jacc.2019.10.040. [DOI] [PubMed] [Google Scholar]
- 28.Borre ED,, Goode A,, Raitz G et al. Predicting thromboembolic and bleeding event risk in patients with non-valvular atrial fibrillation: a systematic review. Thromb Haemost. 2018;118:2171–87. doi: 10.1055/s-0038-1675400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Graves KG,, May HT,, Knowlton KU et al. Improving CHA(2)DS(2)-VASc stratification of non-fatal stroke and mortality risk using the Intermountain Mortality Risk Score among patients with atrial fibrillation. Open Heart. 2018;5:e000907-e. doi: 10.1136/openhrt-2018-000907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chao TF,, Lip GYH,, Liu CJ et al. Relationship of aging and incident comorbidities to stroke risk in patients with atrial fibrillation. J Am Coll Cardiol. 2018;71:122–32. doi: 10.1016/j.jacc.2017.10.085. [DOI] [PubMed] [Google Scholar]
- 31.Yoon M,, Yang PS,, Jang E et al. Dynamic changes of CHA2DS2-VASc Score and the risk of ischaemic stroke in Asian patients with atrial fibrillation: a nationwide cohort study. Thromb Haemost. 2018;118:1296–304. doi: 10.1055/s-0038-1651482. [DOI] [PubMed] [Google Scholar]
- 32.Chao TF,, Liao JN,, Tuan TC et al. Incident co-morbidities in patients with atrial fibrillation initially with a CHA2DS2-VASc score of 0 (males) or 1 (females): implications for reassessment of stroke risk in initially ‘low-risk’ patients. Thromb Haemost. 2019;119:1162–70. doi: 10.1055/s-0039-1683933. [DOI] [PubMed] [Google Scholar]
- 33.Domek M,, Gumprecht J,, Mazurek M et al. Should we judge stroke risk by static or dynamic risk scores? A focus on the dynamic nature of stroke and bleeding risks in patients with atrial fibrillation. J Cardiovasc Pharmacol. 2019;74:491–8. doi: 10.1097/FJC.0000000000000750. [DOI] [PubMed] [Google Scholar]
- 34.Turc G,, Maïer B,, Naggara O et al. Clinical scales do not reliably identify acute ischemic stroke patients with large-artery occlusion. Stroke. 2016;47:1466–72. doi: 10.1161/STROKEAHA.116.013144. [DOI] [PubMed] [Google Scholar]
- 35.Choi SY,, Kim MHH,, Lee KM Age-dependent anticoagulant therapy for atrial fibrillation patients with intermediate risk of ischemic stroke: A nationwide population-based study. Thromb Haemost. 2020. epub ahead of press. [DOI] [PubMed]
- 36.Chao TF,, Lip GYH,, Lin YJ et al. Age threshold for the use of non-vitamin K antagonist oral anticoagulants for stroke prevention in patients with atrial fibrillation: insights into the optimal assessment of age and incident comorbidities. Eur Heart J. 2019;40:1504–14. doi: 10.1093/eurheartj/ehy837. [DOI] [PubMed] [Google Scholar]
- 37.Hindricks G,, Potpara T,, Dagres N 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2020. epub ahead of press. [DOI] [PubMed]
- 38.Nielsen PB,, Skjoth F,, Overvad TF et al. Female sex is a risk modifier rather than a risk factor for stroke in atrial fibrillation: should we use a CHA2DS2-VA score rather than CHA2DS2-VASc? Circulation. 2018;137:832–40. doi: 10.1161/CIRCULATIONAHA.117.029081. [DOI] [PubMed] [Google Scholar]
- 39.Wu VCC,, Wu M,, Aboyans V et al. Female sex as a risk factor for ischaemic stroke varies with age in patients with atrial fibrillation. Heart. 2019;106:534–40. doi: 10.1136/heartjnl-2019-315065. [DOI] [PubMed] [Google Scholar]
- 40.Nielsen PB,, Overvad TF. Female sex as a risk modifier for stroke risk in atrial fibrillation: using CHA2DS2-VASc versus CHA2DS2-VA for stroke risk stratification in atrial fibrillation: a note of caution. Thromb Haemost. 2020;120:894–8. doi: 10.1055/s-0040-1710014. [DOI] [PubMed] [Google Scholar]
- 41.Overvad TF,, Potpara TS,, Nielsen PB. Stroke risk stratification: CHA2DS2-VA or CHA2DS2-VASc? Heart Lung Circ. 2019;28:e14–e5. doi: 10.1016/j.hlc.2018.08.012. [DOI] [PubMed] [Google Scholar]
- 42.Chao TF,, Liu CJ,, Wang KL et al. Should atrial fibrillation patients with 1 additional risk factor of the CHA2DS2-VASc score (beyond sex) receive oral anticoagulation? J Am Coll Cardiol. 2015;65:635–42. doi: 10.1016/j.jacc.2014.11.046. [DOI] [PubMed] [Google Scholar]
- 43.National Heart Foundation of Australia (NHFA), Cardiac Society of Australia and New Zealand (CSANZ). NHFA and CSANZ: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Heart Lung Circ. 2018;27:1209–66. doi: 10.1016/j.hlc.2018.06.1043. [DOI] [PubMed] [Google Scholar]
- 44.Andreotti F,, Rocca B,, Husted S et al. Antithrombotic therapy in the elderly: expert position paper of the European Society of Cardiology Working Group on Thrombosis. Eur Heart J. 2015;36:3238–49. doi: 10.1093/eurheartj/ehv304. [DOI] [PubMed] [Google Scholar]
- 45.Chao TF,, Liu CJ,, Lin YJ et al. Oral anticoagulation in very elderly patients with atrial fibrillation: a nationwide cohort study. Circulation. 2018;138:37–47. doi: 10.1161/CIRCULATIONAHA.117.031658. [DOI] [PubMed] [Google Scholar]
- 46.Kitazono T,, Ikeda T,, Ogawa S et al. Real-world outcomes of rivaroxaban treatment in elderly Japanese patients with nonvalvular atrial fibrillation. Heart Vessels. 2020;35:399–408. doi: 10.1007/s00380-019-01487-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Okumura K,, Akao M,, Yoshida T et al. Low-dose edoxaban in very elderly patients with atrial fibrillation. N Engl J Med. 2020;383:1735–45. doi: 10.1056/NEJMoa2012883. [DOI] [PubMed] [Google Scholar]
- 48.Hart RG,, Pearce LA,, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–67. doi: 10.7326/0003-4819-146-12-200706190-00007. [DOI] [PubMed] [Google Scholar]
- 49.Sato H,, Ishikawa K,, Kitabatake A et al. Low-dose aspirin for prevention of stroke in low-risk patients with atrial fibrillation: Japan Atrial Fibrillation Stroke Trial. Stroke. 2006;37:447–51. doi: 10.1161/01.STR.0000198839.61112.ee. [DOI] [PubMed] [Google Scholar]
- 50.Mant J,, Hobbs FD,, Fletcher K et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet. 2007;11:493–503. doi: 10.1016/S0140-6736(07)61233-1. [DOI] [PubMed] [Google Scholar]
- 51.Lip GY,, Wang KL,, Chiang CE. Non-vitamin K antagonist oral anticoagulants for stroke prevention in Asian patients with atrial fibrillation: time for a reappraisal. Int J Cardiol. 2015;180:246–54. doi: 10.1016/j.ijcard.2014.11.182. [DOI] [PubMed] [Google Scholar]
- 52.Yao X,, Shah ND,, Sangaralingham LR et al. Non-vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. J Am Coll Cardiol. 2017;69:2779–90. doi: 10.1016/j.jacc.2017.03.600. [DOI] [PubMed] [Google Scholar]
- 53.Yu HT,, Yang PS,, Jang E et al. Label adherence of direct oral anticoagulants dosing and clinical outcomes in patients with atrial fibrillation. J Am Heart Assoc. 2020;9:e014177-e. doi: 10.1161/JAHA.119.014177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lee SR,, Lee YS,, Park JS et al. Label adherence for non-vitamin K antagonist oral anticoagulants in a prospective cohort of Asian patients with atrial fibrillation. Yonsei Med J. 2019;60:277–84. doi: 10.3349/ymj.2019.60.3.277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Chan YH,, Chao TF,, Chen SW Off-label dosing of non-vitamin K antagonist oral anticoagulants and clinical outcomes in Asian patients with atrial fibrillation. Heart Rhythm. 2020. epub ahead of press. [DOI] [PubMed]
- 56.Lee KN,, Choi JI,, Boo KY et al. Effectiveness and safety of off-label dosing of non-vitamin K antagonist anticoagulant for atrial fibrillation in Asian patients. Sci Rep. 2020;10:1801. doi: 10.1038/s41598-020-58665-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Di Minno A,, Frigerio B,, Spadarella G et al. Old and new oral anticoagulants: food, herbal medicines and drug interactions. Blood Rev. 2017;31:193–203. doi: 10.1016/j.blre.2017.02.001. [DOI] [PubMed] [Google Scholar]
- 58.Tsai HH,, Lin HW,, Lu YH et al. A review of potential harmful interactions between anticoagulant/antiplatelet agents and Chinese herbal medicines. PLoS One. 2013;8:e64255. doi: 10.1371/journal.pone.0064255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hijazi Z,, Hohnloser SH,, Oldgren J et al. Efficacy and safety of dabigatran compared with warfarin in relation to baseline renal function in patients with atrial fibrillation: a RE-LY trial analysis. Circulation. 2014;129:961–70. doi: 10.1161/CIRCULATIONAHA.113.003628. [DOI] [PubMed] [Google Scholar]
- 60.Bohula EA,, Giugliano RP,, Ruff CT et al. Impact of renal function on outcomes with edoxaban in the ENGAGE AF-TIMI 48 trial. Circulation. 2016;134:24–36. doi: 10.1161/CIRCULATIONAHA.116.022361. [DOI] [PubMed] [Google Scholar]
- 61.Stanton BE,, Barasch NS,, Tellor KB. Comparison of the safety and effectiveness of apixaban versus warfarin in patients with severe renal impairment. Pharmacotherapy. 2017;37:412–9. doi: 10.1002/phar.1905. [DOI] [PubMed] [Google Scholar]
- 62.Fazio G,, Dentamaro I,, Gambacurta R et al. Safety of edoxaban 30 mg in elderly patients with severe renal impairment. Clin Drug Investig. 2018;38:1023–30. doi: 10.1007/s40261-018-0693-6. [DOI] [PubMed] [Google Scholar]
- 63.Lee KN,, Choi JI,, Kim YG et al. Comparison of renal function estimation formulae for dosing direct oral anticoagulants in patients with atrial fibrillation. J Clin Med. 2019;8:2034. doi: 10.3390/jcm8122034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chan YH,, Chao TF,, Lee HF et al. Impacts of different renal function estimation formulas on dosing of DOACs and clinical outcomes. J Am Coll Cardiol. 2020;76:1808–10. doi: 10.1016/j.jacc.2020.08.025. [DOI] [PubMed] [Google Scholar]
- 65.Turpie AGG,, Purdham D,, Ciaccia A. Nonvitamin K antagonist oral anticoagulant use in patients with renal impairment. Ther Adv Cardiovasc Dis. 2017;11:243–56. doi: 10.1177/1753944717714921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Coleman CI,, Kreutz R,, Sood NA et al. Rivaroxaban versus warfarin in patients with nonvalvular atrial fibrillation and severe kidney disease or undergoing hemodialysis. Am J Med. 2019;132:1078–83. doi: 10.1016/j.amjmed.2019.04.013. [DOI] [PubMed] [Google Scholar]
- 67.Siontis KC,, Zhang X,, Eckard A et al. Outcomes associated with apixaban use in patients with end-stage kidney disease and atrial fibrillation in the United States. Circulation. 2018;138:1519–29. doi: 10.1161/CIRCULATIONAHA.118.035418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Pokorney S,, Kumbhani DJ. RENAL-AF trial interim results. Presented at American Heart Association Annual Scientific Sessions, Philadelphia, PA, US. 16 November 2019
- 69.Daiichi Sankyo. Savaysa™ (edoxaban) prescribing information. Daiichi Sankyo, Tokyo, Japan, 2019
- 70.Gibson CM,, Mehran R,, Bode C et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N Engl J Med. 2016;375:2423–34. doi: 10.1056/NEJMoa1611594. [DOI] [PubMed] [Google Scholar]
- 71.Lopes RD,, Heizer G,, Aronson R et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med. 2019;380:1509–24. doi: 10.1056/NEJMoa1817083. [DOI] [PubMed] [Google Scholar]
- 72.Cannon CP,, Bhatt DL,, Oldgren J et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017;377:1513–24. doi: 10.1056/NEJMoa1708454. [DOI] [PubMed] [Google Scholar]
- 73.Galli M,, Andreotti F,, Porto I, Crea F. Intracranial haemorrhages vs. stent thromboses with direct oral anticoagulant plus single antiplatelet agent or triple antithrombotic therapy: a meta-analysis of randomized trials in atrial fibrillation and percutaneous coronary intervention/acute coronary syndrome patients. EP Europace. 2020;22:538–46. doi: 10.1093/europace/euz345. [DOI] [PubMed] [Google Scholar]
- 74.Vranckx P,, Valgimigli M,, Eckardt L et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): a randomised, open-label, phase 3b trial. Lancet. 2019;394:1335–43. doi: 10.1016/S0140-6736(19)31872-0. [DOI] [PubMed] [Google Scholar]
- 75.Yasuda S,, Kaikita K,, Akao M et al. Antithrombotic therapy for atrial fibrillation with stable coronary disease. N Engl J Med. 2019;381:1103–13. doi: 10.1056/NEJMoa1904143. [DOI] [PubMed] [Google Scholar]
- 76.Vene N,, Mavri A,, Gubenšek M et al. Risk of thromboembolic events in patients with non-valvular atrial fibrillation after dabigatran or rivaroxaban discontinuation – data from the Ljubljana registry. PloS One. 2016;11:e0156943-e. doi: 10.1371/journal.pone.0156943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Douketis JD,, Spyropoulos AC,, Duncan J et al. Perioperative management of patients with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019;179:1469–78. doi: 10.1001/jamainternmed.2019.2431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Calkins H,, Hindricks G,, Cappato R et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. J Arrhythm. 2017;33:369–409. doi: 10.1016/j.joa.2017.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Beyer-Westendorf J,, Gelbricht V,, Forster K et al. Peri-interventional management of novel oral anticoagulants in daily care: results from the prospective Dresden NOAC registry. Eur Heart J. 2014;35:1888–96. doi: 10.1093/eurheartj/eht557. [DOI] [PubMed] [Google Scholar]
- 80.Chao TF,, Lin YJ,, Chang SL et al. Incident risk factors and major bleeding in patients with atrial fibrillation treated with oral anticoagulants: a comparison of baseline, follow-up and delta HAS-BLED scores with an approach focused on modifiable bleeding risk factors. Thromb Haemost. 2018;47:768–77. doi: 10.1055/s-0038-1636534. [DOI] [PubMed] [Google Scholar]
- 81.Nielsen PB,, Larsen TB,, Skjøth F,, Lip GYH. Outcomes associated with resuming warfarin treatment after hemorrhagic stroke or traumatic intracranial hemorrhage in patients with atrial fibrillation. JAMA Intern Med. 2017;177:563–70. doi: 10.1001/jamainternmed.2016.9369. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.