

Abstract
Background
Mental health-related positive and negative aspects of telework are understudied. This study aimed to evaluate anxiety, depression and sleep quality in full-time teleworkers during lockdown imposed by the coronavirus disease 2019 (COVID-19) pandemic and explore potential relationships between these variables, sociodemographic characteristics, quality of life and perceived productivity.
Methods
A cross-sectional study was conducted on 143 full-time teleworkers. Participants were assessed for anxiety, depression and sleep quality using validated clinical instruments.
Results
This study found a high prevalence of poor sleep quality (74%, N = 106). Participants reported anxiety/depressive symptoms with the predominance of anxiety and very high levels of sleep impairment. Better sleep quality was associated with longer sleep duration and better job satisfaction, whereas the use of hypnotic medication and higher depression/anxiety scores seem to point a correlation with sleep impairment. Anxiety/depression positively correlated with worse sleep quality and negatively associated with quality of life. Male sex was negatively associated with perceived productivity.
Conclusions
A higher prevalence of poor sleep quality was found in comparison with other studies performed during the COVID-19 pandemic as well as high levels of anxiety and depression. These results highlight the relevance of considering the potential negative impact of telework on mental health.
Keywords: COVID-19, mental health, occupational health, psychiatry, sleep
Introduction
The global public health crisis due to the novel coronavirus disease 2019 (COVID-19) pandemics led to an abrupt worldwide revolution in the way millions of individuals work. Lockdown was imposed by governments, and social distancing encouraged as a means of decreasing transmission risk. Widespread usage of new technologies was the solution implemented by many companies in order to maintain activity in this context.
Alternate ways of working besides the traditional in-office work are not new and have been studied in smaller scale in the past. Although the concept of remote work is not new, its conceptual framework is ill-defined with different partially overlapping terms used in the literature (remote work, telecommuting, telework, distributed work, virtual teams) such that there is no universally accepted definition of telework.1 Telework implies work and/or provision of services done outside employer’s locations—typically from home—using information and communications technologies.2
Telework presents potential benefits for individual workers, companies and society. On the individual level, it allows increased flexibility and autonomy in the management of professional tasks, including the ability to adjust and manage a schedule according to specific needs and demands.3 Benefits associated with the time saved in commuting between home and office are also noteworthy. Indeed, reduced transportation costs and commute-induced stress are the most frequently cited reasons by workers to prefer telework.4
Companies are able to reduce operational costs and absenteeism while benefiting from increased flexibility in the recruitment and retention/employment of qualified employees based in distant locations.1 Societal benefits include reduction in the environmental impact through reduction of office-home commute with less traffic, air pollution levels and improved quality of life in cities.5 Rural areas may also benefit when the distance to a physical office is no longer an issue with telework potentially creating new job opportunities for these communities.6
Literature on the impact of telework on productivity is contradictory. Some studies report increased productivity due to the reduced breaks and distractions that often present in the workplace environment. This increase may also be explained by the subjective sense of authority and autonomy that a home–office allows to the worker, amplifying the level of self-confidence in their own skills and abilities.4 Teleworkers consistently report overall increased job satisfaction and better quality of life.7 On the other hand, companies may lose grip of the ability to monitor their employees’ performance and some workers may lack the necessary self-discipline to manage their own schedule without external monitoring, thereby negatively impacting overall productivity.8
Informal social contact with coworkers is essential to establish meaningful interpersonal relationships and cooperation within the structure of organizations. This lack of direct social interaction may hinder the implementation of remote work in some companies. For this reason, some companies deciding to fully implement telework still made the decision to require the physical presence of their workers at least once a week in the office. This aspect was considered essential to avoid isolation from their peers and keep part of the social aspect of a traditional workplace environment.9
Telework implies a lack of development of social working relationship with coworkers, especially those working in the office. Human beings are eminently social living beings who not only happen to live among other individuals but have an imperative need to live with other human beings. COVID-19 pandemics deprived most people of close contact with coworkers, friends and family. Despite the increasing number and availability of digital tools that promote virtual social interactions (e.g. Zoom®, WhatsApp®, Facebook®), the recommended physical distancing resulted in social distancing and isolation with adverse consequences on mental health outcomes.10,11
Published studies show that the lack of real human interactions is the main disadvantage reported by individuals in telework mode.12 Social deprivation and solitude have well-established negative health consequences: worse sleep quality, increased anxiety and depression and increased risk of suicide.13–18 However, there is a lack of data on the specific impact of telework on mental health, in particular the association with depression and stress.19
The current COVID-19 pandemic has led to an exponential increase in full-time telework worldwide with the highest number of individuals working remotely. The balance between the positive and negative aspects of different modalities of telework and its impact on mental health, productivity and job satisfaction is still understudied and presents inconsistent results although data seem to suggest that the further extent to which workers work from home the more likely they may present negative consequences.20–22 The massification of this new way of working—and its consequences on the isolation of workers—justifies the relevance of further studying the impact of this work mode on mental health.
This work aims to evaluate anxiety, depression and sleep quality in a population of full-time teleworkers. Furthermore, it explores the potential association of these mental health variables with perceived productivity and quality of life.
Methods
Study design, setting and participants
The study was designed as a cross-sectional descriptive study. It was conducted remotely with a convenience sample of alumni from the Portuguese AESE Business School. According to the aim of our study we defined as inclusion criteria for participants being a full-time teleworker in the previous 3 months. All participants in our study were full-time teleworkers in the 3 months preceding data collection. Individuals working full-time in the office or partial teleworkers were excluded. Data were collected between 6 and 22 August 2020. Telework was imposed by lockdown due to the COVID-19 pandemic, and before this restriction, all participants in our study were working in the office. An e-mail invitation to participate in this study was sent to 4987 alumni with a unique hyperlink to access an online survey. Participation in the study was voluntary and the questionnaire was confidential and anonymous. The study received ethical approval from the institutional review board (Department of Human Behaviour of AESE Business School, Ref. ASA CHO, 1/2020) and principles outlined in the Declaration of Helsinki have been followed. A total of 458 questionnaires were completed (9.2% total response rate) and validated, and a total of 143 individuals were selected according to inclusion criteria.
Data sources and measurement
Data were collected through a general questionnaire designed by the authors and regarding the main variables of interest with standardized validated instruments (Hospital Anxiety and Depression Scale [HADS] and Pittsburgh Sleep Quality Index [PSQI]).
Sociodemographic, clinical, work and quality of life questionnaire
A self-completion questionnaire was designed to ensure study eligibility and to collect relevant socio-demographic, clinical and work-related data (age, gender, marital status, number of children, education level, regular physical activity, quality of life, antidepressant/anxiolytic medication use, weekly working hours and days, job satisfaction, perceived productivity). Quality of life and job satisfaction was assessed with a self-report 11-point Likert scale ranging from 0 (‘worst’) to 10 (‘best’). Perceived productivity in comparison to the participants’ previous experience in presential work was assessed qualitatively on a 7-point ordinal scale ranging from the same level of productivity to increased or decreased productivity (‘slightly’, ‘moderately’ and ‘extremely’).
Hospital anxiety and depression scale
HADS is a self-reported 14-item used to examine depressive and anxiety symptoms.23 HADS includes two 7-item subscales, one measuring anxiety and one measuring depression, which may be scored separately. Each item is scored on a 4-point Likert scale (0–3) with scores ranging from 0 to 21 for both subscales. Higher scores indicate a higher level of depression or anxiety (total score of 15 or higher suggestive of pathological anxiety/depression).
Pittsburgh sleep quality index
PSQI is a self-reported 19-item questionnaire used to assess sleep quality and sleep patterns.24 These items allow an evaluation of seven components: subjective sleep quality, sleep latency, total sleep duration, habitual sleep efficiency, sleep disturbances, medication use and daytime dysfunction. Each component is scored on a 4-point Likert scale (0–3). A total score of 5 or higher is suggestive of a sleep disorder.
Statistical methods
Standard descriptive summary statistics were used to characterize the sample. Associations between variables were evaluated using the χ2 test (categorical variables) and the one-way analysis of variance F test (continuous variables). Regression analysis was performed on PQSI, HADS, socio-demographic variables and working habits. The stepwise selection method using the Akaike Information Criterion was used for model selection. In all regression analysis, symmetry of residuals and large sample size guaranteed estimates quality. A P-value < 0.05 was considered significant. Data statistical analysis was performed using R v4.0.2, a free open source project that is distributed under the GNU General Public License.
Results
A sociodemographic profile and overall characteristics of the study population of full-time teleworkers is presented in Tables 1 and 2. Study population (N = 143) was a homogeneous sample in regard to most sociodemographic variables, including gender (males 56%, N = 80; females 44%, N = 63), average age 49.2 (standard deviation [SD] 8.89), marital status (married 72%, N = 103) and presence of children (88%, N = 126). Most individuals completed bachelor, master or doctoral degrees (94%, N = 135) and worked on average 39 hours per week and 5 days per week. Most individuals reported subjective impression of being more productive in full-time telework (65%, N = 91), with 26% (N = 36) reporting being extremely more productive. Productivity in telework was reportedly the same as in traditional office work in 16% (N = 22) of individuals and only 19% (N = 27) reported feeling less productive. No relevant statistically significant associations between sociodemographic variables were found.
Table 1.
Demographic, lifestyle and health characteristics
| N = 143 | |
|---|---|
| Age, mean (SD) | 49.2 (8.89) |
| Gender, N (%) | |
| Female | 63 (44.1) |
| Male | 80 (55.9) |
| Marital status, N (%) | |
| Married | 103 (72.0) |
| Common law | 18 (12.6) |
| Single | 11 (7.7) |
| Divorced | 10 (7.0) |
| Widower | 1 (0.7) |
| Children, N (%) | |
| No | 17 (11.9) |
| Yes | 126 (88.1) |
| Number of children, mean (SD) | 1.7 (1) |
| Education level, N (%) | |
| Doctoral degree | 6 (4.2) |
| Master degree | 67 (46.9) |
| Bachelor degree | 62 (43.4) |
| Secondary education | 8 (5.6) |
| Practice of regular physical activity, N (%) | 76 (53.1) |
| Antidepressant/anxiolytic medication, N (%) | 20 (14) |
| Quality of life (scale 0–10), mean (SD) | 7.1 (1.6) |
Table 2.
Work-related characteristics of study participants
| Professional area, N (%) | |
|---|---|
| Public service and ONGs | 3 (2.1) |
| Logistics and commerce | 6 (4.2) |
| Education and culture | 6 (4.2) |
| Finance | 13 (9.1) |
| Management | 67 (46.9) |
| Medicine and health industry | 10 (6.9) |
| Tourism | 3 (2.1) |
| Journalism and marketing | 2 (1.4) |
| Other | 33 (23.1) |
| Corporate position, N (%) | |
| President/CEO | 17 (11.9) |
| Department head | 62 (43.4) |
| Section head | 27 (18.9) |
| Supervisor | 24 (16.8) |
| Staff | 1 (0.7) |
| Other | 12 (8.4) |
| Weekly working hours, mean (SD) | 38.7 (14.9) |
| Weekly working days, mean (SD) | 4.9 (0.9) |
| Job satisfaction (scale 0–10), mean (SD) | 7.4 (1.9) |
Sleep quality was significantly disturbed in the study participants with PSQI total score averaging 6.21 (SD 2.99). Individual components with the highest scores suggest the presence of sleep disorders (component 5, average score 1.17, SD 0.49) and daytime dysfunction (component 7, average score 1.29, SD 0.81). Indeed, using a cut-off of PSQI ≥5 there was a remarkably high prevalence of sleep disturbances in the study population of teleworkers (74.1%, N = 106) (Fig. 1).
Fig. 1.
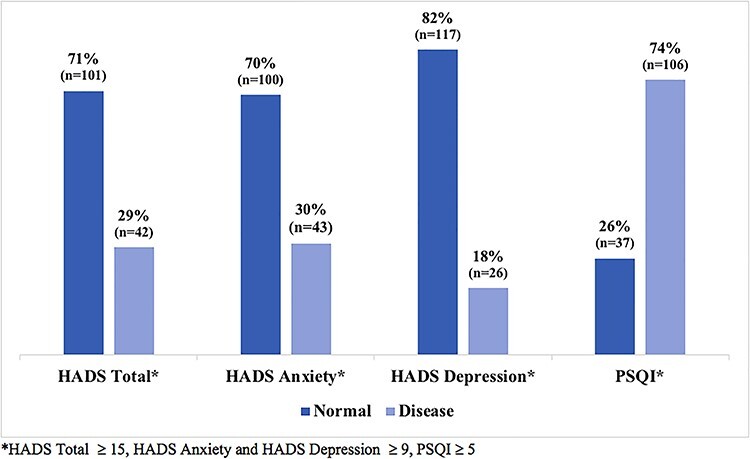
Anxiety, depression and sleep quality in full-time teleworkers.
HADS total score averaged 11.2 (SD 7.1) revealing a considerably high prevalence of depressive and anxiety symptoms. Evaluation of HADS-Anxiety and HADS-Depression subscales suggests that anxiety symptoms are more prevalent (mean 6.7, SD 4.2) than depression symptoms (mean 4.5, SD 3.5). Fig. 1 presents the prevalence of pathological levels of overall depression/anxiety (29.4%, N = 42), anxiety (30.1%, N = 43) and depression (18.2%, N = 26) in this population. Despite the fact that HADS scores are not synonymous with a formal diagnosis of specific anxiety or mood disorders according to current diagnostic classification systems, these results show that teleworkers report symptoms that are highly suggestive of these disorders.
Results of the regression analysis for PSQI, HADS and perceived productivity are shown in Table 3.
Table 3.
Stepwise variable selection algorithm regression results for PSQI, HADS and perceived productivity
| Dependent variables | Independent variables | (Constant) | Estimate |
|---|---|---|---|
| PSQI | 12.48 | ||
| Male sex | −0.54 | ||
| Job satisfaction | −0.17 | ||
| Hypnotic medication
use Never < 1/week 1–2/week ≥3/week |
0.00 2.18 3.12 4.50 |
||
| Sleep hours | −1.13 | ||
| HADS | 0.15 | ||
| HADS | 11.82 | ||
| Civil status Married Common law Single Divorced Widower |
0.00 −2.28 −4.94 1.02 −1.36 |
||
| Weekly working days | 1.03 | ||
| Quality of life | −1.70 | ||
| Antidepressant or anxiolytic medication use | 2.51 | ||
| Hypnotic medication
use Never < 1/week 1–2/week ≥3/week |
0.00 −0.18 −5.28 −6.44 |
||
| PSQI | 1.17 | ||
| Perceived productivity | 1.73 | ||
| Male sex | −0.92 | ||
| Job satisfaction | 0.36 | ||
| Antidepressants and anxiolytic medication use | 0.53 | ||
| Practice of regular physical activity | 0.43 |
Table 3 shows a negative relationship between sleep quality (PSQI total score) and male sex, the level of job satisfaction and the number of sleep hours. This means that higher number of sleep hours and higher levels of job satisfaction were associated with lower PSQI scores and hence, better overall sleep quality. On the other hand, the use of hypnotic medication in the previous month and HADS score were positively correlated with PSQI scores. This suggests that the need for the increased use of hypnotic medication and the presence of anxious and/or depressive symptoms are associated with worse sleep quality.
Anxiety and depression symptoms (HADS total score) have a positive correlation with the number of working days per week, antidepressant and anxiolytic medication use, PSQI total score and divorced status. Additionally, there were negative correlations with quality of life, hypnotic medication use and unmarried status (common law, single and widower).
Regression analysis for perceived productivity suggests a positive correlation with job satisfaction, antidepressant and anxiolytic medication use and the practice of regular physical activity. Male sex seems to have a negative relationship with the subjective perception of productivity in telework.
Discussion
Main finding of this study
In this study, mental health variables and sleep quality were assessed in a population of teleworkers suggesting a marked impairment of sleep quality and a significant prevalence of depression and anxiety. Indeed, results suggest high levels of anxiety/depression (29%, N = 42) but in particular a very high prevalence of poor sleep quality (74%, N = 106) among full-time teleworkers in comparison with other studies performed during the pandemic.
What is already known on this topic
COVID-19 pandemic led to a fast-worldwide implementation of telework with scarce data on the potential negative impact on mental health this work mode might entail. In searchable databases (PubMed/Medline) no previous studies were found using specific validated scales to assess mental health outcomes. Indirect assessments were usually provided in this regard.
What this study adds
Anxiety and depression symptoms were prevalent in the population studied (29%, N = 42) with a predominance of anxiety over depressive symptoms. Notwithstanding the fact that it is unquestionable the association of the pandemic situation with higher levels of these symptoms when compared to baseline levels in each studied population, recent data on the prevalence of anxiety and depression during COVID-19 pandemics are still inconsistent.25
In the present study, there was also a negative association between HADS scores and quality of life which is in line with literature on this subject. Previous studies clearly establish the association between higher levels of anxiety and depressive symptoms and lower quality of life.26
Multiple potential explanatory factors behind the significant levels of anxiety and depressive symptoms found in the study population merit further discussion. Social isolation in particular is an established risk factor that negatively impacts mental health, namely increased anxiety and depressive symptoms.11 The negative emotional impact of telework is a contributing factor due to the increased levels of reported isolation and loneliness in comparison with office workers.12 As discussed below high prevalence of poor sleep quality in our sample and its bidirectional relationship with anxiety and depression may also partially explain these findings.
This study identified a very high prevalence of poor sleep quality in teleworkers (74%, N = 106). Recent studies have shown that sleep quality worsened during SARS-CoV-2 disease pandemics usually in correlation with negative mood, stress and anxiety.27 However, in this work, the prevalence of sleep disorders is significatively higher than reported in literature regarding overall sleep disorders during the current COVID-19 pandemic.28
The hypothesis of a bidirectional causal relationship between psychiatric symptoms and sleep disorders reported in numerous studies is replicated in our work as evidenced by the positive correlations in the regression analysis results for both PSQI and HADS scores.29 Although the association of poor sleep quality with anxiety and depression symptoms can be one of the main contributing factors explaining the high prevalence of sleep disorder in our population, there are further explanatory hypotheses to consider.
Teleworkers usually work from home with reduced physical activity, in a sitting position, without recommended regular breaks resulting in increased sedentarism, obesity and osteoarticular disease.30 The relationship between physical activity and sleep is complex but there seems to be an association between physical inactivity and increased risk of sleep disorders.31 On the other hand, in studies during the COVID-19 lockdown, physically active adults seemed to score lower levels of anxiety and depression, although further research would be necessary to assess the impact on sleep quality.32
Natural daytime natural light exposure and nighttime artificial light and screen exposure in individuals impact sleep due to its complex effect on melatonin production and regulation of circadian rhythms. Exposure to light at night and the use of devices with screens are associated with depressive symptoms and insomnia, respectively.33 There also strong evidence that exposure to bright light during the day improves sleep quality.34 Since individuals working from home tend to be less exposed to natural light during the day and work with electronic devices this is a likely contributory factor to the high index of poor sleepers in our study. The lack of a clear separation from the worker’s personal and family space results in an increase in working hours into the night, stress, loss of regular social and professional schedules finally resulting in sleep cycle dysregulation and impairment of sleep quality.35
Evidence that successful psychological detachment in virtual teams enables the setting of work-personal life boundaries, and positive correlation to sleep quality is an example of how research on this topic is essential to improve working conditions of remote workers.35
The negative association between male sex and productivity suggests that men report lower productivity levels in relation to female teleworkers. Several disadvantages reported in remote work may help explain these findings, including work–family conflict, career stagnation and social isolation.36 The impact of working remotely in work-family balance is unclear. Although some authors report that telework allows for a more positive balance between work and family life, other studies highlight the negative impact that working from home may have on the dissolution of the natural boundaries that the traditional office allows.37 We hypothesize that one of the factors that may help justify the lower perceived productivity in male teleworkers is a more favorable work-family balance in females with stricter boundaries set between their different roles and consequent reduced impact on productivity when working remotely from home. However, data on this subject are controversial with contradictory results emerging from previous studies.38,39
Regarding productivity it is noteworthy that poor sleep quality is often associated with lower levels of productivity in workers across different professional fields.40 This relationship is explained chiefly by the impact of poor sleep on subjective cognitive impairment which in turn impacts performance as reflected by work productivity.41 Although this study did not find such an association between poor sleep quality and productivity, this may be explained due to the potential bias that our sample included a very high prevalence of poor sleep quality among participants (74%, N = 106).
Limitations of this study
We acknowledge that the present study presents several limitations. First, the descriptive nature of any cross-sectional study design and the relatively low response rate may limit conclusions drawn because results may change over time. Data were collected regarding the first 3 months of stricter lockdown in Portugal, and the initial widespread implementation of remote work in many companies with participants who had switched from traditional office work to full-time telework imposed by lockdown measures. The adaptation of individuals to home isolation and more restrictive measures, the natural progression of the epidemiological situation, and adjustment of employers to create virtual teams are all dynamic factors to be taken into consideration. Assessment of the long-term impact of telework would benefit from further studies with a longitudinal design. Secondly, the current global public health crisis is unprecedented in modern history, and its direct impact on mental health may interfere with the mental health outcomes assessed in this work. Furthermore, the consequences of prolonged lockdown periods invariably resulted in social and economic crisis in most countries that have a well-established negative impact on mental health, including depression, anxiety and suicide.42 Additionally, the generalizability of our findings may be impaired due to potential biases since participants were alumni from a business school, mostly office workers with an average higher educational level in comparison with the general population. Although the assessment of quality of life, perceived productivity and job satisfaction was not the main aim of the study, the fact that self-report questionnaires scored in Likert scales were used may limit the interpretation of these results. Finally, when assessing sleep quality and sleep patterns, no objective method was used, such as polysomnography.
Conclusion
This study aimed at the evaluation of mental health in full-time teleworkers revealing high prevalence of poor sleep quality and high levels of anxiety and depression. Current massification of remote work driven by COVID-19 pandemic changed overnight the way millions of individuals and their families live, work, study and experience their daily routines. Employers, companies and governments alike must cooperate on their way to find a new balance that enables us to move forward in this new reality in a healthy and productive way. The remarkably high prevalence of poor sleep quality and high levels of anxiety and depression in the present study highlights the potential negative impact of telework on mental health outcomes. Although data are still lacking, it is clear that these changes ultimately have a profound impact in society, including on public mental health. Further studies should be performed to further inform a rational evidence-based planning of businesses, policy review and legislation updates hopefully avoiding adverse health outcomes.
Acknowledgments
The authors would like to acknowledge AESE Business School for enabling the conduction of this study.
Pedro Afonso, Professor
Miguel Fonseca, Professor
Tomás Teodoro, Researcher and Psychiatry Specialist Registrar
Contributor Information
Pedro Afonso, Faculty of Medicine, University Clinics of Psychiatry and Medical Psychology, Universidade de Lisboa, Lisbon 1649-028, Portugal.
Miguel Fonseca, Department of Mathematics and Center for Mathematics and Applications, NOVA School of Science and Technology, Universidade NOVA de Lisboa, Caparica, Lisbon 2829-516, Portugal.
Tomás Teodoro, Department of Psychiatry, Centro Hospitalar Psiquiátrico de Lisboa, Lisbon 1749-002, Portugal; CHRC - Comprehensive Health Research Centre, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon 1169-056, Portugal.
Funding
This work was supported by national funds through the FCT—Fundação para a Ciência e a Tecnologia, I.P. [UIDB/00297/2020] (Center for Mathematics and Applications).
Conflicts of interest
MF received research funds through the Center for Mathematics and Applications. PA and TT report no financial or other relationships relevant to the subject of this article.
References
- 1. Allen TD, Golden TD, Shockley KM. How effective is telecommuting? Assessing the status of our scientific findings. Psychol Sci Public Interest 2015;16(2):40–68. [DOI] [PubMed] [Google Scholar]
- 2. European Foundation for the Improvement of Living and Working Conditions ., International Labour Office. Working anytime, anywhere: the effects on the world of work. LU: Publications Office; 2017. 10.2806/425484 (30 October 2020, date last accessed) [DOI] [Google Scholar]
- 3. Gajendran RS, Harrison DA. The good, the bad, and the unknown about telecommuting: meta-analysis of psychological mediators and individual consequences. J Appl Psychol 2007;92(6):1524–41. [DOI] [PubMed] [Google Scholar]
- 4. Bailey DE, Kurland NB. A review of telework research: findings, new directions, and lessons for the study of modern work. J Organ Behav 2002;23(4):383–400. [Google Scholar]
- 5. Nilles JM. Traffic reduction by telecommuting: a status review and selected bibliography. Transportation Research Part A: General 1988;22(4):301–17. [Google Scholar]
- 6. Simpson L, Daws L, Pini B et al. Rural telework: case studies from the Australian outback. New Tech Work Empl 2003;18(2):115–26. [Google Scholar]
- 7. Wheatley D. Good to be home? Time-use and satisfaction levels among home-based teleworkers: home-based teleworkers. New Technology, Work and Employment 2012;27(3):224–41. [Google Scholar]
- 8. Day F, Burbach ME. Does organization sector matter in leading teleworker teams? A comparative case study. Int J Bus Res Devel 2014;3(4):8–21. [Google Scholar]
- 9. Pérez MP, Sánchez AM, de Luis Carnicer MP. Benefits and barriers of telework: perception differences of human resources managers according to company’s operations strategy. Technovation 2002;22(12):775–83. [Google Scholar]
- 10. Banerjee D, Rai M. Social isolation in Covid-19: the impact of loneliness. Int J Soc Psychiatry 2020;66(6):525–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Luo M, Guo L, Yu M et al. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – a systematic review and meta-analysis. Psychiatry Res 2020;291:113190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Mann S, Holdsworth L. The psychological impact of teleworking: stress, emotions and health. N Technol Work Empl 2003;18(3):196–211. [Google Scholar]
- 13. Aanes MM, Hetland J, Pallesen S et al. Does loneliness mediate the stress-sleep quality relation? The Hordaland health study. Int Psychogeriatr 2011;23(6):994–1002. [DOI] [PubMed] [Google Scholar]
- 14. Beutel ME, Klein EM, Brähler E et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatry 2017;17(1):97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Santini ZI, Koyanagi A, Tyrovolas S et al. The association between social relationships and depression: a systematic review. J Affect Disord 2015;175:53–65. [DOI] [PubMed] [Google Scholar]
- 16. Hoffman YSG, Grossman ES, Bergman YS et al. The link between social anxiety and intimate loneliness is stronger for older adults than for younger adults. Aging Ment Health 2020;1–8. doi: 10.1080/13607863.2020.1774741. [DOI] [PubMed] [Google Scholar]
- 17. Calati R, Ferrari C, Brittner M et al. Suicidal thoughts and behaviors and social isolation: a narrative review of the literature. J Affect Disord 2019;245:653–67. [DOI] [PubMed] [Google Scholar]
- 18. Stickley A, Koyanagi A. Loneliness, common mental disorders and suicidal behavior: findings from a general population survey. J Affect Disord 2016;197:81–7. [DOI] [PubMed] [Google Scholar]
- 19. Tavares AI. Telework and health effects review. IJH 2017;3(2):30. [Google Scholar]
- 20. Golden TD, Veiga JF. The impact of extent of telecommuting on job satisfaction: resolving inconsistent findings. J Manag 2005;31(2):301–18. [Google Scholar]
- 21. Golden TD. The role of relationships in understanding telecommuter satisfaction. J Organ Behav 2006;27(3):319–40. [Google Scholar]
- 22. Schall MA. The Relationship Between Remote Work and Job Satisfaction: The Mediating Roles of Perceived Autonomy, Work-Family Conflict, and Telecommuting Intensity Master of Science. San Jose, CA, USA: San Jose State University; 2019. https://scholarworks.sjsu.edu/etd_theses/5017 (31 December 2020, date last accessed). [Google Scholar]
- 23. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67(6):361–70. [DOI] [PubMed] [Google Scholar]
- 24. Buysse DJ, Reynolds CF, Monk TH et al. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28(2):193–213. [DOI] [PubMed] [Google Scholar]
- 25. Pandey D, Bansal S, Goyal S et al. Psychological impact of mass quarantine on population during pandemics—the COVID-19 lock-down (COLD) study. Santana GL, editor. PLoS One 2020;15(10):e0240501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Cerne A, Rifel J, Rotar-Pavlic D et al. Quality of life in patients with depression, panic syndrome, other anxiety syndrome, alcoholism and chronic somatic diseases: a longitudinal study in Slovenian primary care patients. Wien Klin Wochenschr 2013;125(1–2):1–7. [DOI] [PubMed] [Google Scholar]
- 27. Targa ADS, Benítez ID, Moncusí-Moix A et al. Decrease in sleep quality during COVID-19 outbreak. Sleep Breath 2020. doi: 10.1007/s11325-020-02202-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Bigalke JA, Greenlund IM, Carter JR. Sex differences in self-report anxiety and sleep quality during COVID-19 stay-at-home orders. Biol Sex Differ 2020;11(1):56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Fang H, Tu S, Sheng J et al. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med 2019;23(4):2324–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Crawford JO, MacCalman L, Jackson CA. The health and well-being of remote and mobile workers. Occup Med 2011;61(6):385–94. [DOI] [PubMed] [Google Scholar]
- 31. Yang Y, Shin JC, Li D et al. Sedentary behavior and sleep problems: a systematic review and meta-analysis. Int J Behav Med 2017;24(4):481–92. [DOI] [PubMed] [Google Scholar]
- 32. Ernstsen L, Havnen A. Mental health and sleep disturbances in physically active adults during the COVID-19 lockdown in Norway: does change in physical activity level matter? Sleep Med 2020;77:309–12. [DOI] [PubMed] [Google Scholar]
- 33. Fossum IN, Nordnes LT, Storemark SS et al. The association between use of electronic media in bed before going to sleep and insomnia symptoms, daytime sleepiness, morningness, and chronotype. Behav Sleep Med 2014;12(5):343–57. [DOI] [PubMed] [Google Scholar]
- 34. Münch M, Wirz-Justice A, Brown SA et al. The role of daylight for humans: gaps in current knowledge. Clocks Sleep 2020;2(1):61–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Rohwer E, Kordsmeyer A-C, Harth V et al. Boundarylessness and sleep quality among virtual team members – a pilot study from Germany. J Occup Med Toxicol 2020;15(1):30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Baruch Y, Nicholson N. Home, sweet work: requirements for effective home working. J Gen Manag 1997;23(2):15–30. [Google Scholar]
- 37. Hill EJ, Ferris M, Märtinson V. Does it matter where you work? A comparison of how three work venues (traditional office, virtual office, and home office) influence aspects of work and personal/family life. J Vocat Behav 2003;63(2):220–41. [Google Scholar]
- 38. Bilodeau J, Marchand A, Demers A. Psychological distress inequality between employed men and women: a gendered exposure model. SSM - Population Health 2020;11:100626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Jacukowicz A, Merecz-Kot D. Work-related internet use as a threat to work-life balance - a comparison between the emerging on-line professions and traditional office work. Int J Occup Med Environ Health 2020;33(1):21–33. [DOI] [PubMed] [Google Scholar]
- 40. Doi Y, Minowa M, Tango T. Impact and correlates of poor sleep quality in Japanese white-collar employees. Sleep 2003;26(4):467–71. [DOI] [PubMed] [Google Scholar]
- 41. Lee S, Buxton OM, Andel R et al. Bidirectional associations of sleep with cognitive interference in employees’ work days. Sleep Health 2019;5(3):298–308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. World Health Organization . Impact of Economic Crises on Mental Health. WHO Regional Office for Europe, 2011. [Google Scholar]