

Abstract
Purpose of review:
The purpose of this review was to synthesize the empirical literature regarding key risk and protective factors for child maltreatment at each level of the socioecological model and to identify directions for future research and practice.
Recent findings:
Prior research has largely focused on risk and protective factors at the individual and interpersonal levels of the socioecological model. More recently, research has begun to examine risk and protective factors at the community and societal levels, with results suggesting that programmatic and policy interventions that reduce risk and enhance protection at these levels are promising primary prevention strategies for child maltreatment.
Summary:
Future research should continue to focus on risk and protective factors at the community and societal levels with the aim of building the evidence base for population-wide prevention strategies. Such strategies have the potential to create contexts in which families and children thrive.
Keywords: child maltreatment, child abuse and neglect, risk factors, protective factors, socioecological model
Introduction
Child maltreatment: prevalence and consequences
Child maltreatment is a clear and pressing public health issue in the United States. At the Federal level, the Child Abuse Prevention and Treatment Act (CAPTA) defines child maltreatment as “any recent act or failure to act on the part of a parent or caregiver that results in death, serious physical or emotional harm, sexual abuse, or exploitation, or an act or failure to act that presents an imminent risk of serious harm” to a child under the age of 18 years. As such, child maltreatment includes experiences of physical, sexual, and emotional abuse and multiple forms of neglect (e.g., physical, emotional, supervisory, medical, educational).1 In 2018, child protective services (CPS) agencies in the U.S. received more than 4 million reports of suspected maltreatment involving approximately 7.8 million children.2 Recent research indicates that by age 18 years, more than 1 in 3 U.S. children will have had a CPS investigation for suspected maltreatment3 and 1 in 8 will have experienced confirmed (i.e., substantiated) maltreatment based on the findings of a CPS investigation.4 However, it is widely accepted that official CPS reports underestimate the true prevalence of maltreatment as not all cases come to the attention of the child welfare system.5,6 Estimates based on adult and adolescent self-report suggest that more than 40% of individuals experience maltreatment during childhood,7,8 underscoring the magnitude of this issue.
A large body of research demonstrates the potential impact of childhood experiences of maltreatment on health and development across the life course. Among young children, several studies show an association between child maltreatment and lower cognitive skills,9,10 anxious, depressed, withdrawn, and aggressive behaviors,10,11 and poor emotional, social, and school functioning.12,13 In adolescence and adulthood, research indicates that child maltreatment is associated with poor mental health,14,15 problematic substance use behaviors,16,17 violent victimization and perpetration,18,19 and chronic conditions such as asthma, diabetes, pain, and obesity.20,21 While there is individual variation in the short and long term outcomes associated with experiences of child maltreatment, results from this body of research emphasize the potential impact of maltreatment on muptile domains of functioning.
The magnitude and potential adverse consequences of child maltreatment indicate that evidence based, interdisciplinary approaches to primary prevention are critically needed. Crucial to informing effective prevention is a comprehensive understanding of risk and protective factors for child maltreatment. Here, we define risk factors as experiences, behaviors, characteristics, and contexts that increase the likelihood that a child will experience maltreatment. We define protective factors as experiences, behaviors, characteristics, and contexts that decrease the likelihood that a child will experience maltreatment. Importantly, we define protective factors not merely as the absence of risk, but as something additional in the child’s environment that functions to reduce the likelihood of maltreatment. Knowledge of salient risk and protective factors can advance the child maltreatment research and practice agenda by elucidating directions for future research and key targets for prevention.
Socioecological model
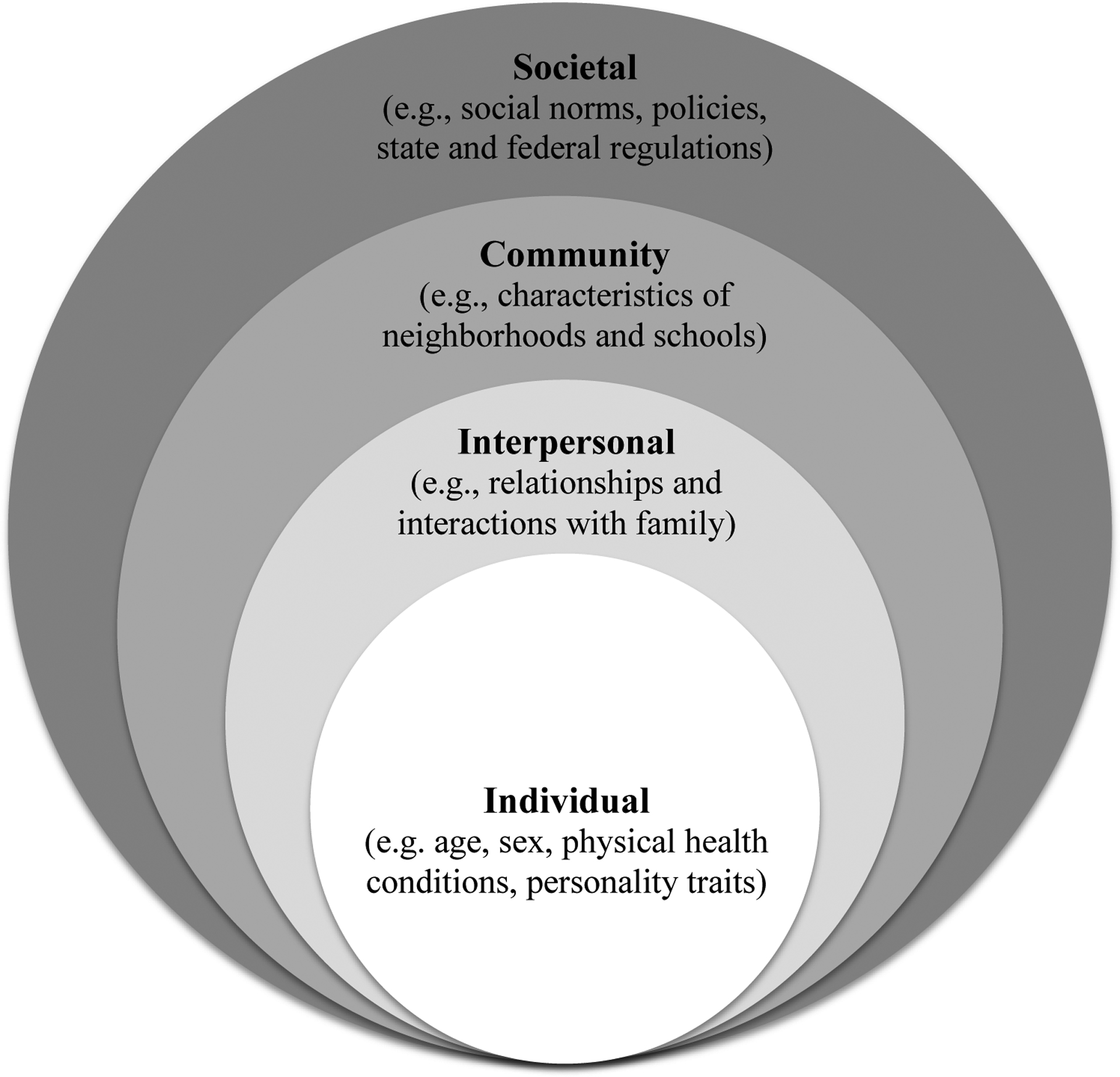
The socioecological model is a framework for understanding complex associations between multiple factors that affect health and development. As shown in Figure 1, the socioecological model consists of a set of nested environments that represent the proximal and distal contexts surrounding health and development.22 These nested environments include the individual, interpersonal, community, and societal levels. Each level is embedded within the next to illustrate that an individual’s immediate environment (i.e., the individual and interpersonal levels) is influenced by the broader conditions surrounding these environments (i.e., the community and societal levels). In the socioecological model, the individual level includes biological and personal history factors such as age, sex, physical health conditions, and personality traits.23 The interpersonal level includes relationships and interactions with partners, peers, and family.23 The community level includes various settings in which people live and interact with others such as schools, neighborhoods, and workplaces.23 The societal level includes factors such as social and cultural norms, economic and educational policies, and state and federal regulations that shape the larger social context within which the child develops.23 As a key public health framework, the socioecological model provides insight into factors at multiple levels of influence that affect the likelihood of a specific experience or outcome and that can be targeted in scientific research and prevention efforts. Leading child maltreatment researchers have proposed use of the socioecological model as a broad, integrative framework for conceptualizing the multiple factors contributing to the etiology of maltreatment.24,25 In the following sections, we use the socioecological model as an organizing framework to review the empirical literature regarding key risk and protective factors for child maltreatment and to identify potential directions for future research and prevention.
Figure 1.
Socioecological model
Risk factors for child maltreatment
Individual level risk factors
While no child is responsible for their experiences of abuse or neglect, some child level characteristics may increase a child’s risk of maltreatment, including child age and special healthcare needs or disabilities.
According to the National Child Abuse and Neglect Data System (NCANDS), a repository of investigated maltreatment reports from all state CPS agencies, the highest rate of child maltreatment is among children less than one year.2,4 In 2017, the rate of confirmed maltreatment was 25.3 per 1,000 children less than one year, and more than a quarter of cases of confirmed maltreatment involved child less than three years.2 In general, the rate of confirmed maltreatment steadily decreases or remains constant as children age.2,4 Young children may have an increased risk for maltreatment given greater dependency on and time spent with caregivers compared to older children. In addition, the same physical force may cause more harm among younger children, requiring medical attention and prompting CPS involvement.
Research also indicates that children with special health care needs or disabilities are at greater risk for maltreatment.26–28 Recent research demonstrated a higher risk of CPS confirmed maltreatment among children with cleft lip, spina bifida, and Down Syndrome compared to unaffected children.26,27 A longitudinal study of Medicaid-enrolled children found that children with a chronic physical illness or a behavioral/mental health condition (e.g., attention deficit hyper-activity disorder) were more likely to experience CPS confirmed maltreatment compared to children without these conditions.28 Notably, children with special health care needs or disabilities often require multiple caregivers and frequent interactions with healthcare providers. Frequent interactions with healthcare providers may increase the likelihood that a professional observes risk for harm and notifies CPS, contributing to a greater likelihood of confirmed maltraetment.26,27 In addition, greater dependency on and contact with numerous adult caregivers may increase opportunities for children with special health care needs or disabilities to experience maltreatment.
Of note, child race/ethnicity is often conceptualized as an individual level risk factor for child maltreatment. Indeed, official statistics indicate that Black and American Indian/Alaska Native children have higher rates of CPS reports, CPS confirmed maltreatment, and out-of-home placements compared to white children and that children of color are disproportionately represented in the child welfare system relative to their presence in the population.2–4,29 However, it is likely not the child’s race/ethnicity that places them at an increased risk for maltreatment, but rather structural and systemic racism, discrimination, and implicit and explicit biases that increase the likelihood that Black and American Indian/Alaska Native children will be reported to CPS. Moreover, these structural and systemic factors may also contribute to an increased likelihood of interpersonal and community level risk factors for maltreatment among families and communities of color, such as parental substance use and concentrated disadvantage (discussed in detail in Interpersonal and Community level risk factors sections),30 further affecting child risk for maltreatment.
Interpersonal level risk factors
With respect to child maltreatment, the focus of the interpersonal level is often on the child’s primary caregivers and family context. A large body of research has examined family level risk factors for child maltreatment as researchers previously considered maltreatment to be an issue occurring largely within families and thus the family context to be the most influential in determining risk for maltreatment.25,31 Well-established family level risk factors for maltreatment include poverty, parental mental health and substance use disorders, and intimate partner violence (IPV).
Family poverty has long been considered an important risk factor for child maltreatment. In the child maltreatment research literature, poverty is often measured as annual household income (e.g., income below the Federal Poverty Level), primary health insurance type (e.g., public vs. private), or participation in public benefits programs (e.g., Temporary Assistance to Needy Families (TANF)).32 More recently, child maltreatment researchers have explored measures of material hardship, including difficulties affording basic needs like housing, food, utilities, and medical care, as a more direct measures of the tangible ways in which poverty affects daily life.33,34 In a sample of families receiving TANF, families reporting housing instability (e.g., difficulty paying rent, eviction), utility shut-offs, food insecurity, and a greater number of total hardships were more likely to experience a CPS investigation compared to families without these hardships.33 In another study, housing instability was associated with an increase in the number of maternal self-reported maltreatment behaviors, and food insecurity was associated with increased use of mother-to-child physical and psychological aggression.35
Multiple studies consistently demonstrate associations of parental mental health and substance use disorders and IPV with child maltreatment. For example, recent research found maternal post-traumatic stress and depressive symptoms to be associated with self-reported abuse and neglect36 and paternal depressive symptoms to be associated with self-reported neglect.37 Similarly, heavy drinking and illicit substance use were associated with an increased frequency of maltreatment behaviors among parents of young children,38 and mothers who reported IPV by a current partner were more likely to endorse physical and psychological aggression, spanking, and neglect.39 Conceptually, issues related to family poverty, material hardship, mental health, substance use, and IPV may negatively affect parental functioning and stress, increasing the risk for maltreatment.
Community level risk factors
At the community level, most child maltreatment research has examined aspects of the child and family’s neighborhood, broadly defined, that may contribute to experiences of maltreatment. Two community level risk factors that have been investigated in the empirical literature are neighborhood crime and violence and concentrated disadvantage. Researchers hypothesize that such factors increase risk for child maltreatment by elevating levels of parent and family stress and eroding social networks and community organization.40–42
With respect to neighborhood crime and violence, longitudinal data from Davidson County, Tennessee revealed that higher rates of crime were associated with an increased risk of CPS confirmed physical and sexual abuse at the zip code level.40 Similarly, data from Fort Worth, Texas found that indicators of community violence (i.e., IPV, aggravated assaults, murders, drug crimes) predicted increases in CPS confirmed maltreatment.41
Concentrated disadvantage has been measured in the child maltreatment literature in multiple ways, including area level poverty, unemployment, and housing foreclosure and vacancy. For example, in a large, urban county, increases in the percent of the population living in poverty and the percent of vacant houses were associated with increased rates of child maltreatment hospitalizations and death at the census tract level.42 Across the U.S., increases in the percent of children living in poverty and in the unemployment rate were associated with higher rates of CPS investigations at the county level.43 In Pennsylvania, higher unemployment and housing foreclosure rates demonstrated associations with increases in both investigated and confirmed maltreatment.44
Notably, many studies examining neighborhood crime and violence and concentrated disadvantage as risk factors for maltreatment adjust for individual and family level risk factors, indicating that adverse neighborhood conditions contribute to maltreatment risk above and beyond the effect of individual and family level factors.
Societal level risk factors
Policies, trends, and norms at the societal level have received increasing attention in the research literature as potential risk factors for child maltreatment. In the existing literature, specific economic policies and trends, such as the Great Recession and regressive taxes, and social norms regarding gender equity have received empirical support as risk factors for maltreatment. Researchers hypothesize that such societal level factors help to create contexts within which maltreatment is more likely to occur.
Results from several studies show that economic policies and trends with the potential to reduce household income and create widespread financial uncertainty are associated with increases in maltreatment. The Great Recession (December 2007-June 2009) provided a unique opportunity to examine the impact of larger economic trends on maltreatment.45,46 In two studies, macro-economic indicators of the Great Recession, such as decreases in consumer confidence, were associated with an increase in self-reported mother-to-child physical and psychological aggression46 and high frequency spanking (i.e., spanking more than 11 times in the past year).45
Regressive taxes, or taxes that take a larger proportion of income from low income compared to high income households, and changes in prices of common consumer goods also provide a unique opportunity to examine the impact of broad economic policies and trends on child maltreatment. National data regarding cigarette and sales taxes indicate that increases in these regressive taxes at the state level are associated with increases in state rates of CPS investigations.47 Recent research also found that higher gas prices at the state level, an economic trend likely to affect families’ disposable income, are associated with higher rates of CPS investigations.48
The existing research literature also indicates that gender inequality, a well-established risk factor for multiple forms of violence including sexual assault and IPV,49 may be a societal level risk factor for maltreatment.4,5 Across multiple low, middle, and high income countries, results from recent studies found that higher levels of discrimination against women, gender inequity (e.g., gender differences in workforce participation), and gender gaps (e.g., gaps in educational and political engagement) were associated with higher proportions of adults endorsing severe physical discipline (e.g., hitting the child with an object) and supervisory neglect in the past month.50,51 While the mechanisms explaining this association are not clear, these results align with a large body of research suggesting that gains in women’s rights and empowerment are associated with positive outcomes across multiple domains of child health and development.52,53
Protective factors for child maltreatment
Individual level protective factors
Just as no child is responsible for contributing to their risk of maltreatment, no child is responsible for preventing their experiences of maltreatment. At the individual level, there is a lack of research focused on primary prevention. Most research has examined individual level factors that are associated with resilience (i.e., positive adaptation54) following experiences of maltreatment55–57 rather than individual level factors that prevent maltreatment from occurring. Results from this body of research suggest that certain characteristics, such as self-regulation skills, social competence, adaptive functioning, and self-esteem, help promote positive outcomes among children and adolescents who have experienced abuse or neglect.55–57 For example, in a longitudinal sample of children investigated for maltreatment, children with consistently high or increasing levels of social skills over time (i.e., cooperation, assertion, responsibility, self-control) were more likely to perform well in school and have positive expectations about the future and less likely to engage in delinquent behaviors and substance use in adolescence compared to children with lower levels of social skills.58 Similarly, early self-regulation skills (i.e., the ability to control emotional and behavioral responses following stressful situations) were associated with positive social and emotional development in a sample of young children investigated for maltreatment.59 These and other individual level protective factors are posited to increase the likelihood that a child will receive support following maltreatment or that the child will be able to effectively navigate stressful and traumatic experiences such as maltreatment,60,61 increasing the likelihood of positive outcomes.
Interpersonal level protective factors
At the interpersonal level, the existing research literature has focused on various aspects of caregiver social support, including support from a romantic partner, family, and friends, as protective factors for child maltreatment. Researchers hypothesize that positive support from various social networks can provide a buffer to reduce caregiver stress and promote caregiver wellbeing, reducing overall maltreatment risk.62
A specific body of research has examined support from a romantic partner as a protective factor in preventing the intergenerational transmission of maltreatment.63–66 Prior studies indicate that harsh, hostile, and abusive parenting can continue across generations, such that individuals who experienced child maltreatment may be more likely to abuse or neglect their own children.63,64 However, recent studies suggest that among parents who experienced maltreatment in childhood, a nurturing and supportive relationship with a romantic partner can prevent the continuation of abusive and neglectful behaviors toward their own children.63–65 For example, in a three-generation cohort study, among parents with a history of maltreatment, warmth, positive communication, and support from a romantic partner were associated with a decreased likelihood of harsh, abusive behaviors toward their child.63,64 Similarly, in a longitudinal study, satisfaction with their relationship with a romantic partner was associated with a decreased likelihood of confirmed CPS reports among parents with a history of maltreatment.65
Support outside of a romantic relationship has also been found to protect against maltreatment.62,67,68 For example, in a population-based sample of caregivers in California, emotional support (e.g., having a friend to share private worries and fears with) was associated with a lower frequency of parent self-reported physical abuse.67 In addition, in a longitudinal study of child development, family support (e.g., “I know my family will stand by me no matter what”) was associated with a lower frequency of caregiver self-reported maltreatment.68
Community level protective factors
Community level factors that have received empirical support as protective factors for child maltreatment include neighborhood availability of services for parents and families and neighborhood processes such as social cohesion (i.e., mutual trust among neighbors) and control (i.e., willingness to intervene). Such modifiable social processes and structural characteristics have the potential to provide a supportive environment that promotes positive parenting.
Existing evidence indicates that greater community availability of health, social, and educational services may be a protective factor for child maltreatment. Among parents in California, greater proximity to mental health and substance abuse services was associated with fewer self-reported neglectful behaviors.69 Similarly, at the census tract level in Bergen County, New Jersey, greater proximity to substance abuse services was associated with low rates of CPS reports.70 In Los Angeles, California, neighborhoods with a higher percent of children attending preschool had lower rates of CPS reports and CPS confirmed maltreatment, and neighborhoods with more license child care spaces relative to child care need had lower rate of CPS reports.71 At the zip code level, a higher density of services for multiple needs (substance abuse, adoption, mental health, domestic violence, independent living, pregnant and parenting teens, housing, and children with special needs) was associated with lower rates of CPS reports and out-of-home placements.72 These results suggest that greater availability of supportive services for parents, including services that address family level risk factors (e.g., substance use), may protect against maltreatment.
With respect to neighborhood social processes, in Franklin County, Ohio, greater neighborhood social cohesion was associated with a lower likelihood of parent self-reported neglect.73 Neighborhoods higher in social cohesion, social control, and intergenerational closure (i.e., families know each other’s children) in Illinois had lower rates of CPS confirmed neglect, physical abuse, and sexual abuse.74 Similarly, greater neighborhood social control and reciprocated exchange (e.g., neighbors visit each other and do favors for each other) were associated with less frequent self-reported physical abuse among parents in California.75
Societal level protective factors
More recently, studies have examined the impact of social and economic policies on child maltreatment. A small but growing evidence base suggests that policies aimed at reducing the burden of common child-related expenses and increasing household income among families with young children, such as paid parental leave, earned income tax credits (EITC), increases in minimum wage, and more generous welfare benefits, may prevent maltreatment.
Results from two studies show that California’s paid family leave policy and EITC across multiple states resulted in decreases in hospitalizations for abusive head trauma among infants.76,77 Similarly, among a sample of families eligible for EITC, an increase in the amount of EITC benefit was associated with reductions in behaviorally approximated neglect among caregivers and self-reported CPS involvement.78 Using national data, researchers found that increases in state-level minimum wage were associated with decreases in CPS investigations for suspected maltreatment, particularly neglect.79 A study of the impact of restrictions to TANF benefits (i.e., caregiver work requirements, time limits for benefits) at the state level demonstrated that TANF restrictions were associated with an increase in CPS investigations for abuse and neglect and an increase in out-of-home placements,80 suggesting that more generous TANF benefits may protect against maltreatment. Importantly, results from many of these studies indicate that modest increases in family income due to policy changes are associated with population level declines in maltreatment, suggesting that policy and safety net shifts do not need to be drastic to prevent maltreatment.
Conclusions
Child maltreatment is a complex public health issue, with risk and protective factors at all levels of the socioecological model impacting the likelihood that a child will experience maltreatment (Table 1). Importantly, risk and protection can accumulate and interact across levels of the socioecological model to increase or decrease the likelihood of maltreatment,81 contributing to the complexity in designing and implementing effective prevention strategies. In this review, we sought to provide a comprehensive overview of key risk and protective factors for child maltreatment at each level of the sociological model in order to illuminate potential directions for research and practice.
Table 1.
Key risk and protective factors for child maltreatment at each level of the socioecological model
| Key risk factors | Key protective factors | |
|---|---|---|
| Individual levela | ||
| Interpersonal level | ||
| Community level | ||
| Societal level |
Individual level protective factors are those that promote resilience among children who have experienced maltreatment
Existing child maltreatment prevention strategies have largely focused on mitigating risk and enhancing protection at the interpersonal level. Home visiting programs targeting high-risk populations, such as the Nurse Family Partnership,82 Parents as Teachers,83 and Healthy Families America,84 are a common child maltreatment prevention strategy. These programs often focus on improving parents’ knowledge of child development, enhancing parenting skills, and reducing parental stress and depression. While these programs have positive impacts on some child and family outcomes, evidence to support home visiting programs as a primary prevention strategy for child maltreatment is mixed,85,86 with a recent meta-analysis finding, on average, no significant impact of home visiting on child maltreatment.87 Moreover, such highly targeted, resource intensive programs are only available to small segments of the population, and scalability and sustainability are challenging. This reduces the potential of home visiting and other programs focused interpersonal level factors, even if effective, to prevent maltreatment at the larger population level.
A key assumption in focusing child maltreatment prevention efforts at the interpersonal level is that the child’s family has control over all of the factors contributing to maltreatment risk. Our review indicates that there are multiple factors at the community and societal levels that increase or decrease the likelihood of maltreatment, many of which are beyond the parent or family’s control. This further reinforces that addressing interpersonal level risk and protective factors for maltreatment may not be sufficient and suggests that strategies focused at the societal and community levels are needed. The existing research literature indicates that social, economic, and educational policies at the societal level, such as paid parental leave, more generous welfare benefits, and improved child care availability, as well as increased investments in community resources and services, have the potential to create a larger context within which parents and families receive they support they need to care for their children. Prevention strategies at the societal and community levels can also reach larger segments of the population and thus may have a greater overall impact in reducing maltreatment. Moreover, because the individual and interpersonal levels are embedded within the community and societal levels, prevention strategies implemented at these outer levels have the potential to impact risk and protective factors at the inner levels as well, further enhancing protective effects.
To prevent child maltreatment, programs and policies that address risk and protective factors at multiple levels of the socioecological model are likely needed. Focusing on implementation and evaluation of societal and community level prevention strategies in tandem with existing interpersonal level strategies has the potential to strengthen and support contexts in which families and children thrive. Future research should continue to focus on the impacts of risk and protective factors that are malleable and amenable to programmatic and policy intervention and building the evidence base for societal and community level prevention strategies.
Funding:
This work was supported in part by an award to the UNC Injury Prevention Research Center from the National Center for Injury Control and Prevention, Centers for Disease Control and Prevention (R49CE003092) and by the UNC Center of Excellence in Maternal and Child Health Science, Education, and Practice, funded by an award to the Department of Maternal and Child Health from the Maternal and Child Health Bureau of the Health Resources and Services Administration (T76MC00004).
Footnotes
Conflicts of interests/competing interests: The authors have no conflicts of interest or competing interests to disclose.
References
●Denotes important reference published within the last 3 years.
- 1.DePanfilis D. Child neglect: A guide for prevention, assessment, and intervention. 2006. Retrieved from https://www.childwelfare.gov/pubPDFs/neglect.pdf.
- 2. ●.United States Department of Health and Human Services. Child Maltreatment 2018. 2018. Retireved from https://www.acf.hhs.gov/cb/research-data-technology/statistics-research/child-maltreatment.; Annual report providing national data on child maltreamtnet known to child protective service agencies in the United States.
- 3. ●.Kim H, Wildeman C, Jonson-Reid M, Drake B. Lifetime prevalence of investigating child maltreatment among U.S. children. American Journal of Public Health. 2017;107(2):274–280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wildeman C, Emanuel N, Leventhal JM, Putnam-Hornstein E, Waldfogel J, Lee H. The prevalence of confirmed maltreatment among U.S. children, 2004 to 2011. JAMA Pediatrics. 2014;168(8):706–713. [DOI] [PMC free article] [PubMed] [Google Scholar]; Estimates the lifetime (proir to age 18 years) prevalence of investigated child protective services reports among U.S. children.
- 5.Negriff S, Schneiderman JU, Trickett PK. Concordance between self-reported childhood maltreatment versus case record reviews for child welfare–affiliated adolescents: Prevalence rates and associations with outcomes. Child Maltreatment. 2017;22(1):34–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sedlak AJ, Mettenburg J, Basena M, Peta I, McPherson K, Greene A. Fourth national incidence study of child abuse and neglect (NIS-4). Washington, DC: US Department of Health and Human Services. 2010. [Google Scholar]
- 7.Finkelhor D, Turner HA, Shattuck A, Hamby SL. Violence, crime, and abuse exposure in a national sample of children and youth: an update. JAMA Pediatrics. 2013;167(7):614–621. [DOI] [PubMed] [Google Scholar]
- 8.Hussey JM, Chang JJ, Kotch JB. Child maltreatment in the United States: prevalence, risk factors, and adolescent health consequences. Pediatrics. 2006;118(3):933–942. [DOI] [PubMed] [Google Scholar]
- 9.Font SA, Berger LM. Child maltreatment and children’s developmental trajectories in early to middle childhood. Child Development. 2015;86(2):536–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jaffee SR, Maikovich-Fong AK. Effects of chronic maltreatment and maltreatment timing on children’s behavior and cognitive abilities. Journal of Child Psychology and Psychiatry. 2011;52(2):184–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Font SA, Berger LM. Child maltreatment and children’s developmental trajectories in early to middle childhood. Child Development. 2015;86(2):536–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lanier P, Kohl PL, Raghavan R, Auslander W. A preliminary examination of child well-being of physically abused and neglected children compared to a normative pediatric population. Child Maltreatment. 2015;20(1):72–79. [DOI] [PubMed] [Google Scholar]
- 13.Jonson-Reid M, Drake B, Kim J, Porterfield S, Han L. A prospective analysis of the relationship between reported child maltreatment and special education eligibility among poor children. Child Maltreatment. 2004;9(4):382–394. [DOI] [PubMed] [Google Scholar]
- 14.Kaplow JB, Widom CS. Age of onset of child maltreatment predicts long-term mental health outcomes. Journal of Abnormal Psychology. 2007;116(1):176. [DOI] [PubMed] [Google Scholar]
- 15.Mills R, Scott J, Alati R, O’Callaghan M, Najman JM, Strathearn L. Child maltreatment and adolescent mental health problems in a large birth cohort. Child Abuse & Neglect. 2013;37(5):292–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mills R, Alati R, Strathearn L, Najman JM. Alcohol and tobacco use among maltreated and non-maltreated adolescents in a birth cohort. Addiction. 2014;109(4):672–680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Herrenkohl TI, Hong S, Klika JB, Herrenkohl RC, Russo MJ. Developmental impacts of child abuse and neglect related to adult mental health, substance use, and physical health. Journal of Family Violence. 2013;28(2):191–199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Manchikanti Gómez A. Testing the cycle of violence hypothesis: Child abuse and adolescent dating violence as predictors of intimate partner violence in young adulthood. Youth & Society. 2011;43(1):171–192. [Google Scholar]
- 19.Roberts AL, McLaughlin KA, Conron KJ, Koenen KC. Adulthood stressors, history of childhood adversity, and risk of perpetration of intimate partner violence. American Journal of Preventive Medicine. 2011;40(2):128–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Scott KM, Von Korff M, Angermeyer MC, et al. Association of childhood adversities and early-onset mental disorders with adult-onset chronic physical conditions. Archives of General Psychiatry. 2011;68(8):838–844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shin SH, Miller DP. A longitudinal examination of childhood maltreatment and adolescent obesity: Results from the National Longitudinal Study of Adolescent Health (Add Health) Study. Child Abuse & Neglect. 2012;36(2):84–94. [DOI] [PubMed] [Google Scholar]
- 22.Bronfenbrenner U. Toward an experimental ecology of human development. American Psychologist. 1977;32(7):513. [Google Scholar]
- 23.Centers for Disease Control and Prevention. The social-ecological model: A framework for violence prevention. 2002. https://www.cdc.gov/violenceprevention/pdf/sem_framewrk-a.pdf.
- 24.Belsky J. Child maltreatment: An ecological integration. American Psychologist. 1980;35(4):320. [DOI] [PubMed] [Google Scholar]
- 25.Cicchetti D, Lynch M. Toward an ecological/transactional model of community violence and child maltreatment: Consequences for children’s development. Psychiatry. 1993;56(1):96–118. [DOI] [PubMed] [Google Scholar]
- 26.Van Horne BS, Moffitt KB, Canfield MA, et al. Maltreatment of children under age 2 with specific birth defects: a population-based study. Pediatrics. 2015;136(6):1504–e1512. [DOI] [PubMed] [Google Scholar]
- 27.Van Horne BS, Caughy MO, Canfield M, et al. First-time maltreatment in children ages 2–10 with and without specific birth defects: A population–based study. Child Abuse & Neglect. 2018;84:53–63. [DOI] [PubMed] [Google Scholar]
- 28.Jaudes PK, Mackey-Bilaver L. Do chronic conditions increase young children’s risk of being maltreated? Child Abuse & Neglect. 2008;32(7):671–681. [DOI] [PubMed] [Google Scholar]
- 29.Austin AE, Parrish JW, Shanahan ME. Using time-to-event analysis to identify preconception and prenatal predictors of child protective services contact. Child Abuse & Neglect. 2018;82:83–91. [DOI] [PubMed] [Google Scholar]
- 30.Williams DR, Lawrence JA, Davis BA. Racism and health: evidence and needed research. Annual Review of Public Health. 2019;40:105–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mulder TM, Kuiper KC, van der Put CE, Stams G-JJM, Assink M. Risk factors for child neglect: A meta-analytic review. Child Abuse & Neglect. 2018;77:198–210. [DOI] [PubMed] [Google Scholar]
- 32. ●.Conrad-Hiebner A, Byram E. The temporal impact of economic insecurity on child maltreatment: a systematic review. Trauma, Violence, & Abuse. 2020;21(1):157–178. [DOI] [PubMed] [Google Scholar]; Synthezies and critically evaluates the existing literature regarding the impact of economic insecurity, including mutliple measures of material hardship, on child matlreatment.
- 33.Yang M-Y. The effect of material hardship on child protective service involvement. Child Abuse & Neglect. 2015;41:113–125. [DOI] [PubMed] [Google Scholar]
- 34.Pelton LH. The continuing role of material factors in child maltreatment and placement. Child Abuse & Neglect. 2015;41:30–39. [DOI] [PubMed] [Google Scholar]
- 35.Marcal KE. The impact of housing instability on child maltreatment: a causal investigation. Journal of Family Social Work. 2018;21(4–5):331–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Chemtob CM, Gudiño OG, Laraque D. Maternal posttraumatic stress disorder and depression in pediatric primary care: Association with child maltreatment and frequency of child exposure to traumatic events. JAMA Pediatrics. 2013;167(11):1011–1018. [DOI] [PubMed] [Google Scholar]
- 37. ●.Lee SJ, Taylor CA, Bellamy JL. Paternal depression and risk for child neglect in father-involved families of young children. Child Abuse & Neglect. 2012;36(5):461–469. [DOI] [PubMed] [Google Scholar]; Demonstrates an association of paternal depression with an increased likelihood of child neglect. Paternal risk factors for maltreatment have received little attention in the peer-reveiwed literature.
- 38.Kepple NJ. The complex nature of parental substance use: Examining past year and prior use behaviors as correlates of child maltreatment frequency. Substance Use & Misuse. 2017;52(6):811–821. [DOI] [PubMed] [Google Scholar]
- 39.Taylor CA, Guterman NB, Lee SJ, Rathouz PJ. Intimate partner violence, maternal stress, nativity, and risk for maternal maltreatment of young children. American Journal of Public Health. 2009;99(1):175–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. ●.Morris MC, Marco M, Maguire-Jack K, et al. Connecting child maltreatment risk with crime and neighborhood disadvantage across time and place: A Bayesian spatiotemporal analysis. Child Maltreatment. 2019;24(2):181–192. [DOI] [PMC free article] [PubMed] [Google Scholar]; Provides evidence of the association of community level factors including crime and concentrated disadvantage with substantiaed maltreatment while accounting for changes in rates over time.
- 41.Daley D, Bachmann M, Bachmann BA, Pedigo C, Bui M-T, Coffman J. Risk terrain modeling predicts child maltreatment. Child Abuse & Neglect. 2016;62:29–38. [DOI] [PubMed] [Google Scholar]
- 42. ●.Thurston H, Freisthler B, Bell J, et al. Environmental and individual attributes associated with child maltreatment resulting in hospitalization or death. Child Abuse & Neglect. 2017;67:119–136. [DOI] [PubMed] [Google Scholar]; Provides evidnece of the association of community level factors including child care burdnen, conentrated disadvantage, and service provider avaliablity with child maltreatment hospitalizations and death while accounting for family level factors.
- 43. ●.Smith BD, Kay ES, Womack BG. How can county-level maltreatment report rates better inform child welfare practice? Children and Youth Services Review. 2017;79:341–347. [Google Scholar]; Employs multi-level modeling to examine the associaton of county level factors with child maltreatment reports and identifies ways national child matlreatment data can be use to inform child welfare practice.
- 44.Frioux S, Wood JN, Fakeye O, Luan X, Localio R, Rubin DM. Longitudinal association of county-level economic indicators and child maltreatment incidents. Maternal and Child Health Journal. 2014;18(9):2202–2208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Brooks-Gunn J, Schneider W, Waldfogel J. The Great Recession and the risk for child maltreatment. Child Abuse & Neglect. 2013;37(10):721–729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. ●.Schneider W, Waldfogel J, Brooks-Gunn J. The Great Recession and risk for child abuse and neglect. Children and Youth Services Review. 2017;72:71–81. [DOI] [PMC free article] [PubMed] [Google Scholar]; Demonstrates the impact of a recent social and economic event, the Great Recession, on maternal self-reported maltreatment to further an understanding of the impact of broader economic trends on maltreatment risk.
- 47. ●.McLaughlin M. The relationship between cigarette taxes and child maltreatment. Child Abuse & Neglect. 2018;79:339–349. [DOI] [PubMed] [Google Scholar]; Examines the impact of a regressive tax not typically considered to be relevant to child maltratment, cigarette taxes, on child maltreatment investigations.
- 48. ●.McLaughlin M. Less money, more problems: How changes in disposable income affect child maltreatment. Child Abuse & Neglect. 2017;67:315–321. [DOI] [PubMed] [Google Scholar]; Examines the impact of changes in disposable income using a novel measures (changes in gasoline prices, a common expense for U.S. families) on child maltreatment investigations.
- 49.Krug EG, Mercy JA, Dahlberg LL, Zwi AB. The world report on violence and health. The Lancet. 2002;360(9339):1083–1088. [DOI] [PubMed] [Google Scholar]
- 50.Klevens J, Ports KA. Gender inequity associated with increased child physical abuse and neglect: A cross-country analysis of population-based surveys and country-level statistics. Journal of Family Violence. 2017;32(8):799–806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. ●.Klevens J, Ports KA, Austin C, Ludlow IJ, Hurd J. A cross-national exploration of societal-level factors associated with child physical abuse and neglect. Global Public Health. 2018;13(10):1495–1506. [DOI] [PMC free article] [PubMed] [Google Scholar]; Across 42 countries, identifies modifiable country level factors including gender inequity, literacy, and development associated with caregiver report of physical abuse and negect.
- 52.Heaton TB. Are improvements in child health due to increasing status of women in developing nations? Biodemography and Social Biology. 2015;61(3):252–265. [DOI] [PubMed] [Google Scholar]
- 53.Homan P. Political gender inequality and infant mortality in the United States, 1990–2012. Social Science & Medicine. 2017;182:127–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology. 2014;5(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Yoon S, Howell K, Dillard R, McCarthy KS, Napier TR, Pei F. Resilience following child maltreatment: Definitional considerations and developmental variations. Trauma, Violence, & Abuse. 2019:1–19. [DOI] [PubMed] [Google Scholar]
- 56.Meng X, Fleury M-J, Xiang Y-T, Li M, D’arcy C. Resilience and protective factors among people with a history of child maltreatment: A systematic review. Social Psychiatry and Psychiatric Epidemiology. 2018;53(5):453–475. [DOI] [PubMed] [Google Scholar]
- 57.Domhardt M, Münzer A, Fegert JM, Goldbeck L. Resilience in survivors of child sexual abuse: A systematic review of the literature. Trauma, Violence, & Abuse. 2015;16(4):476–493. [DOI] [PubMed] [Google Scholar]
- 58.Oshri A, Topple TA, Carlson MW. Positive youth development and resilience: Growth patterns of social skills among youth investigated for maltreatment. Child Development. 2017;88(4):1087–1099. [DOI] [PubMed] [Google Scholar]
- 59.Sattler KMP, Font SA. Resilience in young children involved with child protective services. Child Abuse & Neglect. 2018;75:104–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Werner EE. The children of Kauai: Resiliency and recovery in adolescence and adulthood. Journal of Adolescent Health. 1992;13(4):262–268. [DOI] [PubMed] [Google Scholar]
- 61.Eisenberg N, Valiente C, Eggum ND. Self-regulation and school readiness. Early Education and Development. 2010;21(5):681–698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Thompson RA. Social support and child protection: Lessons learned and learning. Child Abuse & Neglect. 2015;41:19–29. [DOI] [PubMed] [Google Scholar]
- 63.Schofield TJ, Conger RD, Conger KJ. Disrupting intergenerational continuity in harsh parenting: Self-control and a supportive partner. Development and Psychopathology. 2017;29(4):1279–1287. [DOI] [PubMed] [Google Scholar]
- 64.Conger RD, Schofield TJ, Neppl TK, Merrick MT. Disrupting intergenerational continuity in harsh and abusive parenting: The importance of a nurturing relationship with a romantic partner. Journal of Adolescent Health. 2013;53(4):11–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Thornberry TP, Henry KL, Smith CA, Ireland TO, Greenman SJ, Lee RD. Breaking the cycle of maltreatment: The role of safe, stable, and nurturing relationships. Journal of Adolescent Health. 2013;53(4):25–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Schofield TJ, Lee RD, Merrick MT. Safe, stable, nurturing relationships as a moderator of intergenerational continuity of child maltreatment: A meta-analysis. Journal of Adolescent Health. 2013;53(4):32–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Price-Wolf J. Social support, collective efficacy, and child physical abuse: Does parent gender matter? Child Maltreatment. 2015;20(2):125–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Martin A, Gardner M, Brooks-Gunn J. The mediated and moderated effects of family support on child maltreatment. Journal of Family Issues. 2012;33(7):920–941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Maguire-Jack K, Klein S. Parenting and proximity to social services: Lessons from Los Angeles County in the community context of child neglect. Child Abuse & Neglect. 2015;45:35–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Morton CM. The moderating effect of substance abuse service accessibility on the relationship between child maltreatment and neighborhood alcohol availability. Children and Youth Services Review. 2013;35(12):1933–1940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Klein S. The availability of neighborhood early care and education resources and the maltreatment of young children. Child Maltreatment. 2011;16(4):300–311. [DOI] [PubMed] [Google Scholar]
- 72.Freisthler B. Need for and access to supportive services in the child welfare system. GeoJournal. 2013;78(3):429–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Maguire-Jack K, Showalter K. The protective effect of neighborhood social cohesion in child abuse and neglect. Child Abuse & Neglect. 2016;52:29–37. [DOI] [PubMed] [Google Scholar]
- 74.Molnar BE, Goerge RM, Gilsanz P, et al. Neighborhood-level social processes and substantiated cases of child maltreatment. Child Abuse & Neglect. 2016;51:41–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Freisthler B, Maguire-Jack K. Understanding the interplay between neighborhood structural factors, social processes, and alcohol outlets on child physical abuse. Child Maltreatment. 2015;20(4):268–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Klevens J, Luo F, Xu L, Peterson C, Latzman NE. Paid family leave’s effect on hospital admissions for pediatric abusive head trauma. Injury Prevention. 2016;22(6):442–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. ●.Klevens J, Schmidt B, Luo F, Xu L, Ports KA, Lee. Effect of the earned income tax credit on hospital admissions for pediatric abusive head trauma, 1995–2013. Public Health Reports. 2017;132(4):505–511. [DOI] [PMC free article] [PubMed] [Google Scholar]; Demonstrates the protective effect of a state policy designed to increase household income on abusive head trauma hospitlaizaitons.
- 78.Berger L, Font SA, Slcak KS, Waldfogel JW. Income and child maltreatment: Evidence from the Earned Income Tax Credit. 2013. Retrieved from http://www.appam.org/assets/1/7/Income_and_Child_Maltreatment_Evidence_from_the_Earned_Income_Tax_Credit.pdf. [DOI] [PMC free article] [PubMed]
- 79. ●.Raissian KM, Bullinger LR. Money matters: Does the minimum wage affect child maltreatment rates? Children and Youth Services Review. 2017;72:60–70. [Google Scholar]; Provides evidence that increases in state minimum wage are assocaited with reduced child maltreatment reports.
- 80.Ginther DK, Johnson-Motoyama M. Do State TANF policies affect child abuse and neglect? 2017. Retrieved from https://www.econ.iastate.edu/files/events/files/gintherjohnsonmotoyama_appam.pdf.
- 81.Masten AS, Wright MOD. Cumulative risk and protection models of child maltreatment. Journal of Aggression, Maltreatment & Trauma. 1998;2(1):7–30. [Google Scholar]
- 82.Olds DL. The nurse-family partnership: An evidence-based preventive intervention. Infant Ment Health Journal. 2006;27(1):5–25. [DOI] [PubMed] [Google Scholar]
- 83.Wagner MM, Clayton SL. The Parents as Teachers program: Results from two demonstrations. The Future of Children. 1999:91–115. [PubMed] [Google Scholar]
- 84.Daro DA, Harding KA. Healthy Families America: Using research to enhance practice. The Future of Children. 1999:152–176. [PubMed] [Google Scholar]
- 85.Duggan A, Caldera D, Rodriguez K, Burrell L, Rohde C, Crowne SS. Impact of a statewide home visiting program to prevent child abuse. Child Abuse & Neglect. 2007;31(8):801–827. [DOI] [PubMed] [Google Scholar]
- 86.Olds DL. Preventing child maltreatment and crime with prenatal and infancy support of parents: The nurse‐family partnership. Journal of Scandinavian Studies in Criminology and Crime Prevention. 2008;9(1):2–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Filene JH, Kaminski JW, Valle LA, Cachat P. Components associated with home visiting program outcomes: A meta-analysis. Pediatrics. 2013;132(2):100–109. [DOI] [PMC free article] [PubMed] [Google Scholar]