

Abstract
Background:
There is a paucity of current data describing injuries in professional basketball players. Utilizing publicly available injury data will allow for greater transparency for stakeholders to use the data as a shared resource to create future basketball injury prevention programs.
Purpose:
To describe injury and illness incidence, severity, and temporal trends in National Basketball Association (NBA) players. Among those who develop time-loss injury or illness, we estimated severity based on games missed because of injury or illness.
Study Design:
Descriptive epidemiology study.
Methods:
Publicly available NBA data were extracted through a reproducible computer-programmed process from the 2008 to 2019 seasons. Data were externally validated by 2 independent reviewers through other publicly available data sources. Injury and illness were calculated per 1000 athlete game-exposures (AGEs). Injury severity was calculated as games missed because of injury or illness. Injury and illness data were stratified by body part, position, severity (slight, minor, moderate, or severe), month, and year.
Results:
A total of 1369 players played a total of 302,018 player-games, with a total of 5375 injuries and illnesses. The overall injury and illness incidence was 17.80 per 1000 AGEs. The median injury severity was 3 games (interquartile range, 0-6 games) missed per injury. Overall, 33% of injuries were classified as slight; 26%, as minor; 26%, as moderate; and 15%, as severe. The ankle (2.57 injuries/1000 AGEs), knee (2.44 injuries/1000 AGEs), groin/hip/thigh (1.99 injuries/1000 AGEs), and illness (1.85 illnesses/1000 AGEs) had the greatest incidence of injury and illness. Neither injury or illness incidence nor severity was different among basketball playing positions. Injury incidence demonstrated increasing incremental trends with season progression. Injuries were similar throughout the 11-year reporting period, except for a substantial increase in the lockout-shortened 2012 season.
Conclusion:
The ankle and knee had the greatest injury incidence. Injury incidence was similar among basketball positions. Injury incidence increased throughout the season, demonstrating the potential relationship between player load and injury incidence.
Keywords: knee, ankle, hip, overtraining syndrome, injury prevention, player loading
Professional basketball is a contact sport involving repeated landing and pivoting at high speeds. 11,37 Professional basketball athletes play as long as 48 minutes per game and can run 4.8 to 8.1 km per game, over an 82-game regular season. 37 Because of its physical nature and the number of games played, professional basketball has high injury rates compared with its collegiate and amateur counterparts. 6,10 It is estimated that the National Basketball Association (NBA), a men’s professional basketball league in North America composed of 30 teams, loses $300 million each season because of time-loss injuries. 35 Because of the high burden associated with NBA injuries, basketball stakeholders have sought to prevent injuries. 30
Basketball injuries can be prevented through a stepwise process consisting of incidence and severity description and injury risk factor characterization, which is dependent on high-quality data. 12 Professional basketball injury and severity have been previously described 9,11,37 ; however, the most current NBA injury reporting is 15 years old, potentially decreasing the current validity and usefulness. For example, over a 10-year period between the 1988 and 1998 seasons, NBA injuries increased by 12.4%. This 10-year increase in injuries may have been due to rule changes, player characteristics, or the style of play. 37 In addition, it is unknown whether risk associated with player position has been changing over time. Since the previous NBA injury reporting, ending in 2005, 11 many NBA rule changes have occurred, including expanding NBA rosters from 10 to 15 players 29 and integrating concussion protocols, 27 which may have affected overall injury risk and severity. Because of the length of time since the previous injury reporting and the potential for altered injury risk and severity over this period, an update of injury epidemiologic reporting is necessary.
One way to investigate and report injuries in professional sports is through publicly available data. 16,27 Using publicly available data can allow for greater research transparency, frequent updating, and use of that data as part of an iterative process involving multiple stakeholders to enhance and distribute results. 24,25 Publicly available injury reporting has been previously performed within the NBA. 16,27 For the 1999-2000 NBA seasons, it was found that the publicly reported injury data had a high reporting reliability. 16 Since this data reporting, many technological and public reporting advancements have been made, potentially further increasing the data precision and detail. 20 NBA concussion incidence was reported using publicly available data for the 1999-2018 seasons. However, these data did not report other injuries or illnesses and utilized hand-search methods instead of a systematic and automated computerized repeatable process. 27 As a result, these data did not inform general injury prevention strategies and mitigate the potential for these publicly available data to become a shared transparent resource.
There is a paucity of current data describing injury incidence, severity, and temporal trends in professional basketball players. Utilizing robust publicly available injury data will allow for greater transparency for sports medicine clinicians and organizations to use the data as a shared resource and create future basketball injury prevention programs. Therefore, the aim of this study was to describe injury and illness incidence, severity, and temporal trends in NBA players. In addition, among those who develop time-loss injury or illness, we estimated severity based on games missed because of injury or illness.
Methods
Participants
Eligible participants were NBA players aged 18 years and older with at least 1 season played between 2008 and 2019, both with and without time-loss injury or illness reported during the study period.
Study Design
Publicly available data from the NBA were investigated for the purpose of this study. Data were extracted through a reproducible programmed process known as “data scraping,” in which a programming language retrieves data from online publicly available depositories (eg, websites) and puts it in a readable output. 19 Three large online resources were utilized to create a combined data set for this study: https://www.prosportstransactions.com, https://www.basketball-reference.com, and https://stats.nba.com. The Pro Sport Transactions website documents every professional North American sport transaction, including trades, the draft, free agent signings, injuries, and disciplinary and legal actions. The Basketball-Reference website provides current and historical basketball statistics for the NBA, American Basketball Association (predecessor to the NBA), Women’s NBA, and Euroleague. The NBA website is the official website for NBA statistics.
External Validation
The retrieved and harmonized data set was collected using a systematic, repeatable approach including automated checks of operations involving data where possible. However, the assumptions that these data are of high quality cannot be made without external validation. As a result, 2 independent examiners (J.V. and D.G.), with the assistance of a number generator (R Core Team), randomly sampled 180 data points from the data set (Appendix 1A, available as supplemental material). The 2 external examiners then proceeded to assess the validity of injury occurrence and body part from publicly sourced internet websites (NBA.net, ESPN.com, or respective individual team websites) and compared these findings with the data set using the data retrieved. The randomly selected records had a relatively low positive predictive value (PPV) of 44.7% for the exact date of the injury but very high PPVs of 84.1% for the missed games and of 95.6% for the injury site (Appendix 1B, available as supplemental material). The low PPV for date of injury was a result of the data set displaying the first game the athlete missed as a result of injury, where oftentimes the validation found the actual date of injury. For example, if an athlete incurred an injury during training, the external validation would define the injury date as the date of the training session, whereas the data set would define the date of injury as the first game after the training session. Furthermore, the majority of discrepancies concerning the number of missed games were due to athletes being activated on the roster but not playing in the NBA game. This potentially demonstrates that while NBA athletes may have been physically cleared to play, the injury may have continued to prevent the athlete from playing at his full potential, inhibiting his game participation.
Definitions and Injury/Illness Classifications
An injury was defined as tissue damage or other derangement of normal physical function reported by a player and his team that occurred during any NBA team–sponsored activity or event and was followed by at least 1 game missed. 3,11 An illness was defined as a complaint or disorder reported by a player and his team that was not related to injury and resulted in at least 1 game missed. 3,11 Examples of illness included physical or mental. 3 The season time frame was classified as the first regular season game to the last regular season. Preseason, training camp, playoffs, and off-season injuries were not investigated. Injuries were categorized by body part. 13,26 If a player was fully healthy but did not play in the game, the player was not counted as having a game exposure. Body parts were categorized as head/neck, shoulder/arm/elbow, forearm/wrist/hand, trunk/back/buttock, groin/hip/thigh, knee, lower leg/Achilles tendon, ankle, and foot/toe. 13,26 Concussions were coded as a separate medical condition, as per the International Olympic Committee Injury and Illness Epidemiology Consensus Group. 3 Injury severity was calculated as games missed because of injury or illness. Injury and illness severity was stratified into slight (1 game), minor (2-3 games), moderate (4-13 games), or severe (≥14 games). 15
Data Extraction
The online data repository https://www.prosportstransactions.com was accessed on December 1, 2019, and data were retrieved between inception and December 1, 2019. Because of the 2020 COVID-19 season shutdown, the 2019-2020 season data were excluded from the analyses. Injury data extraction (scraping) was conducted via R Version 3.5.1 using the rvest, tm, and xml2 packages. For each season and player in the study period, Basketball-Reference.com and stats.nba.com data were retrieved for individual games played, games missed, playing position, and season summary statistics. The custom R package “NBAinjuries” was used to extract these data. For the complete code and raw data obtained for this study, refer to the freely available online code and data repository GitHub R Package “tylerferguson/NBAinjuries.”
Data Reduction
Injury data were checked for consistency through visual inspection and grouping data by year. Data were observed to be inconsistent before 2008, with inconsistencies consisting of missed injuries, missed days, or missed teams. As a result, data before 2008 were omitted from the data set. The data source https://www.prosportstransactions.com contains reliable dates of injury occurrence but frequently omits the date of injury resolution. These injury data were combined with the individual game data to find the first game played by each player after an injury was reported. The date of a player’s first game after injury was used as a proxy for the date of injury resolution. Injuries that were sustained at the end of the season but continued into the next season were considered the same original injury. If a player sustained an injury and proceeded to play basketball at a lower level for rehabilitation reasons, these games were not counted toward return to play. Two counts were also added as a measure of injury severity: the number of days an injury lasted and the number of games missed during the injury. As part of this data pre-preprocessing sample, automated internal validation checks were performed to ensure that implausible (eg, missing or negative) values did not occur.
Statistical Analysis
Continuous variables were reported as means (standard deviations [SDs]) or medians (interquartile ranges [IQRs]). Count data were reported as percentages. Injury and illness incidence was calculated as the sum of injuries and divided by the sum of person-games, multiplied by 1000 athlete game-exposures (AGEs). Injury incidence was stratified by position, body part, and injury severity. Monthly (number of injuries and illnesses by person-games per month) and yearly (number of injuries by person-games per year) injury and illness incidence trends were also calculated for overall injuries, body part, and injury severity. All analyses were performed in R Version 3.5.1 (R Core Team [2013]; R Foundation for Statistical Computing; www.R-project.org).
Results
A total of 1369 players (mean ± SD: age, 26.4 ± 4.2 years; height, 2.00 ± 0.09 m; mass, 100.6 ± 11.9 kg; number of seasons played, 9.3 ± 4.6 seasons) were recorded for the 2008-2009 through the 2018-2019 NBA seasons. A total of 41% were guards (age, 26.3 ± 4.2 years; height, 1.92 ± 0.06 m; mass, 90.3 ± 6.6 kg), 38% were forwards (age, 26.4 ± 4.2 years; height, 2.04 ± 0.04 m; mass, 105.0 ± 7.1 kg), and 21% were centers (age, 26.7 ± 4.4 years; height, 2.11 ± 0.03 m; mass, 114.0 ± 8.7 kg). NBA players played a total of 302,018 player-games, and a total of 5375 injuries and illnesses were recorded between the 2008-2009 and 2018-2019 seasons.
Incidence and Severity
Overall, 66% of players sustained an injury during the reporting period. The overall injury and illness incidence was 17.80 injuries per 1000 AGEs. The injury incidence was 15.60 injuries per 1000 AGEs. The median injury and illness severity was 3 games (IQR, 0-6 games) missed per injury. Overall, 33% of injuries and illnesses were classified as slight; 26%, as minor; 26%, as moderate; and 15%, as severe. Refer to Table 1 for full injury descriptions by body part or illness.
Table 1.
Overall Injury Incidence by Body Part or Illness
| Injury Severity Incidence c | |||||||
|---|---|---|---|---|---|---|---|
| Body Part or Illness | Injury Count | Injury Severity (No. of Games Missed) a | Injury Incidence b | Slight Injury | Minor Injury | Moderate Injury | Severe Injury |
| Ankle | 776 | 3 (0.5-5.5) | 2.57 | 0.90 | 0.83 | 0.87 | 0.33 |
| Knee | 736 | 3 (0-8.5) | 2.44 | 0.74 | 0.73 | 0.69 | 0.72 |
| Groin/hip/thigh | 601 | 3 (0-6) | 1.99 | 0.64 | 0.68 | 0.73 | 0.29 |
| Illness | 559 | 1.0 (0-3) | 1.85 | 1.01 | 0.50 | 0.33 | 0.08 |
| Trunk/back/buttock | 469 | 2 (0-4) | 1.55 | 0.67 | 0.51 | 0.37 | 0.18 |
| Foot/toe | 321 | 3 (0-7.5) | 1.06 | 0.32 | 0.30 | 0.34 | 0.25 |
| Forearm/wrist/hand | 285 | 5 (0-11.5) | 0.94 | 0.24 | 0.20 | 0.32 | 0.32 |
| Shoulder/arm/elbow | 274 | 3 (0-7) | 0.91 | 0.32 | 0.22 | 0.28 | 0.20 |
| Lower leg/Achilles tendon | 227 | 4 (0-8) | 0.75 | 0.19 | 0.18 | 0.29 | 0.17 |
| Head/neck | 104 | 2 (0-4) | 0.34 | 0.17 | 0.07 | 0.09 | 0.04 |
| Concussion | 93 | 3 (1-5) | 0.31 | 0.08 | 0.11 | 0.09 | 0.05 |
a Reported as median (interquartile range).
b Reported per 1000 athlete game-exposures.
c Slight injury, 1 game missed; minor injury, 2-3 games missed; moderate injury, 4-13 games missed; severe injury, ≥14 games missed.
The greatest injury and illness incidence was to the ankle (2.57 injuries/1000 AGEs), followed by the knee (2.44 injuries/1000 AGEs), groin/hip/thigh (1.99 injuries/1000 AGEs), and illness (1.85 illnesses/1000 AGEs). Slight illnesses (1.01 illnesses/1000 AGEs), followed by slight ankle injuries (0.90 injuries/1000 AGEs), had the greatest slight injury severity (1 game). Minor ankle injuries (0.83 injuries/1000 AGEs), followed by minor knee injuries (0.73 injuries/1000 AGEs), had the greatest minor injury severity. Moderate ankle injuries (0.87 injuries/1000 AGEs), followed by moderate groin/hip/thigh injuries (0.73 injuries/1000 AGEs), had the greatest moderate injury severity. Severe knee injuries (0.72 injuries/1000 AGEs), followed by severe ankle injuries (0.33 injuries/1000 AGEs), had the greatest severe injury severity.
Injury and Illness per Position Played
Neither injury and illness incidence nor severity was different among basketball playing positions. The injury and illness incidence was 18.17 per 1000 AGEs for guards, 17.23 injuries or illnesses per 1000 AGEs for forwards, and 18.16 injuries or illnesses per 1000 AGEs for centers. The median injury severity was 3 (IQR, 0-6) for guards, 2 (IQR, 0-5) for forwards, and 3 (IQR, 0-7) for centers. Guard injury and illness severity was 33% for slight, 25% for minor, 28% for moderate, and 14% for severe. Forward injury and illness severity was 33% for slight, 28% for minor, 24% for moderate, and 15% for severe. Center injury and illness severity was 31% for slight, 23% for minor, 28% for moderate, and 18% for severe. Injury incidence was similar per body part compared by position (Appendix 2, available as supplemental material).
Injury and Illness Trends During the Season
Injury and illness incidence demonstrated increasing incremental trends with season progression, apart from February when a substantial drop in injury incidence was observed. Similar relationships were observed separately for injury and illness. The overall injury and illness incidence rates for each month between October and April were 5.40, 14.68, 17.44, 20.32, 14.64, 21.97, and 27.61 injuries per 1000 AGEs, respectively. Similar injury and illness incidence trends were observed by injury severity stratification (Figure 1 and Appendix 3, available as supplemental material). Slight injuries were reported to have the greatest injury incidence, and severe injuries were reported to have the lowest injury incidence throughout the season. The injury and illness incidence increased between October and November for all 4 injury severity categories. The slight, minor, moderate, and severe injury severity categories were observed to have similar injury incidence rates between November and January. Slight injuries continued to increase through January. All 4 injury and illness severity categories were observed to decrease in injury incidence between January and February, followed by a subsequent increase in injury incidence between February and the end of the season in April. All injuries stratified by body part and illnesses had similar seasonal trends (Figure 2 and Appendix 4, available as supplemental material).
Figure 1.

Injury and illness trends throughout the season, stratified by injury severity.
Figure 2.

Injury and illness trends throughout the season, stratified by body part injured.
Temporal Trends Over Past 12 Seasons
The overall injury and illness incidence ranged from 13.54 injuries or illnesses per 1000 AGEs (2008-2009 season) to 21.68 injuries or illnesses per 1000 AGEs (lockout-shortened 2012 season). Injury severity was similar among seasons except for the lockout-shortened 2012 season (slight, 6.65 injuries/1000 AGEs; severe, 5.01 injuries/1000 AGEs) (Figure 3 and Appendix 5, available as supplemental material). The body part or illness or injury incidence was similar among seasons except for the lockout-shortened 2012 season (slight ankle injury, 1.01 injuries/1000 AGEs; severe ankle injury, 0.82 injuries/1000 AGEs) (Appendix 6, available as supplemental material).
Figure 3.
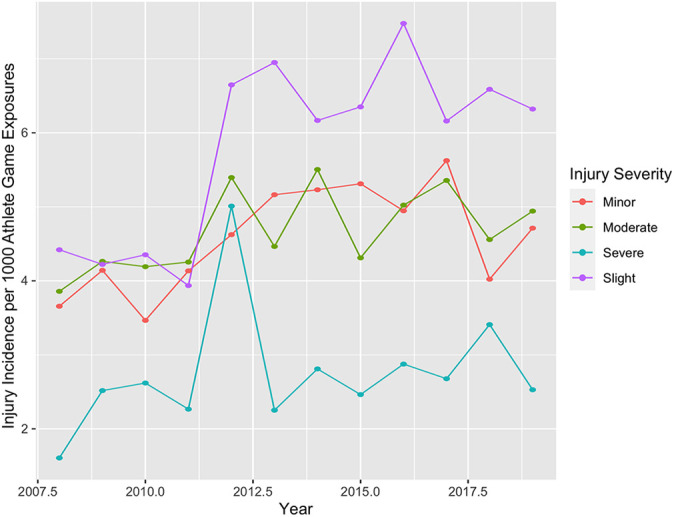
Injury and illness severity trends from 2008 to 2019.
Discussion
The most common professional basketball injuries were to the ankle and knee, and these results were similar when stratified by severity and throughout the season, as well as throughout the 11-year period. The overall injury and illness incidence was similar among basketball playing positions (guard, forward, and center) for injury severity, body part, and monthly and yearly temporal trends. Injury incidence increased throughout the season, with similar injury trends for injury severity and body part; however, there was a significant decrease in February, suggesting a potential effect of the All Star break on recovery. Moderate and severe injuries were similar throughout the 11-year reporting period except for a substantial increase in the lockout-shortened 2012 season. Slight and minor injuries demonstrated an increase in injury incidence beginning in the 2012 season, with similar injury incidence rates between the 2012 and 2019 seasons. For the first time, we describe illness incidence as the third most common reason for missing professional games. As illnesses can be potentially targeted using medical and preventive management of risk factors, this can provide a significant avenue for performance gains.
Ankle and knee injuries were observed to have the greatest injury incidence, which supports previous literature. 9,11,37 Ankle injury incidence was slightly lower than that reported in previous literature (2.6 vs 3.4 injuries/1000 AGEs), while knee injury incidence was slightly higher (2.4 vs 1.5 injuries/1000 AGEs). 11 Ankle injuries demonstrated greater slight, minor, and moderate injury incidence rates, while knee injuries demonstrated greater severe injury incidence. These injury severity observations for the ankle are similar to those reported in the previous literature. 8,22 For example, 1 previous study found that >50% of basketball ankle injuries result in <1 week of time loss and 55% of basketball players who sustain an ankle injury do not seek medical treatment at all, 22 suggesting the general slight to minor nature of basketball ankle injuries. While ankle injuries are predominantly slight or minor, physical detriments still occur. 16 Ankle injuries can incur decreased proprioception and balance, 17 potentially predisposing affected athletes to future recurrent ankle injuries. 17,28 On the other hand, severe basketball knee injuries can have a detrimental effect on joint integrity and physical performance. 7,8,32 Professional basketball players who have sustained a substantial knee injury have demonstrated decreased quadriceps strength and repeated jumping ability compared with matched controls. 32 Busfield et al 8 reported that only 78% of professional basketball players who sustain an anterior cruciate ligament injury return to sport. Furthermore, of the professional basketball players who did return to sport, the majority of these athletes (57%) demonstrated decreased performance after their return, as quantified through the player efficiency rating. 8 These results indicated that ankle and knee joint injuries should be a focus when designing injury prevention programs for basketball players. Because of the greater severity and long-term implications on joint health and performance decrements associated with knee injuries, a greater emphasis may need to be placed on the knee joint in basketball prevention programs.
Basketball playing positions (guard, forward, and center) demonstrated similar injury incidence, injured body parts, and injury temporal patterns. While no previous studies have investigated injuries stratified by basketball playing position, previous studies have investigated the relationship among player height, mass, and basketball injuries, and no relationship between height or mass and NBA injuries was observed. 11,37 While not a direct analysis among anthropomorphic measurements, within our study, there were descriptive differences among positions by height and mass. These data suggested that positional differences were not related to injury incidence. However, these results may have been affected by a portion of players playing multiple positions, such as shooting guard and small forward. Nevertheless, no matter the overall player size, position-specific force production, change of direction, and conditioning should be taken into account when assessing and designing injury prevention and rehabilitation programs. 2,21,34
There was an overall increase in injury and illness incidence throughout the season, and these results were similar when stratified by injury severity and body part. Increased cumulative training load has been associated with increased injury and illness. 33,36 Our data demonstrated similar trends with injury and illness, potentially suggesting that these basketball athletes are susceptible to overtraining syndrome resulting from cumulative season load. 33,36 Overtraining syndrome ramifications include increased risk of illness and greater risk for overuse musculoskeletal injuries, 31,33,36 which can only be attenuated through rest and recovery strategies. 18 However, because rest is not a long-term viable option in professional sport, monitoring and prescribing loading strategies can potentially mitigate overtraining syndrome. 14,23 It should be noted that there was a decrease in injury incidence between January and February, with a subsequent increase in injury incidence through March and April. This trend may have occurred because of the All Star break that occurs in mid-February or because of the increased competition playoff spots at the end of the season. The 3-day play hiatus has been anecdotally used in the NBA as a period to rest or attenuate playing load before the final third of the season. The decreased injury incidence during February may demonstrate this anecdotal trend. Nevertheless, the overall average injury increase throughout the season suggests a proportional relationship between basketball competition load and injury risk, which can be further accentuated by cumulative seasonal loads, resulting in overtraining.
Injury incidence was similar throughout the 11-year reporting period except for a substantial increase in the lockout-shortened 2012 season. Acute rapid increases in overall training load can increase injury risk. 14,31 Players during the lockout-shortened 2012 season were only allowed 16 days of training camp compared with the conventional average of 33 days. 38 Furthermore, because of the compressed time schedule, players competed in more games per week and more back-to-back games (games on consecutive days, with teams playing 3 games in 3 days in some cases during 2012), further increasing acute workloads. 38 While all 4 injury severity classes increased in the 2012 season, severe injuries had the greatest increase, from 2.2 injuries per 1000 athlete-exposures in the 2010-2011 season to 5.0 injuries per 1000 AGEs in the 2012 season. This suggests that greater increases in acute workload may have a more substantive effect on severe injury risk compared with lesser injury severity classes. As a result, the potential greater risk of severe injuries needs to be considered when acute increases in workload are undertaken. After the 2012 season, slight and minor injury incidence remained elevated. Possible explanations include internal changes in leaguewide injury reporting or using slight injury reporting as an actual opportunity to rest players. Within the past 5 years, resting players to help mitigate overall player load has become conventional practice. However, because of the potential league penalties involved with resting players, NBA teams may be using slight injury reporting as a cover for rest, potentially explaining the continued elevated slight injury incidence after the 2012 seasons. However, these explanations are only speculation without further internal league data.
Strengths and Limitations
With this data set, research code, and a custom R software package, freely available with this paper, we hope this article will transform the use of big data in sports injury surveillance and prevention programs. This is aligned with current recommendations for open-access data and code sharing 5 based on concerns regarding ethical aspects of the scientific process 1 and science reproducibility in clinical research. 4 Injury incidence, severity, and monthly and yearly temporal trends were investigated over 11 years, increasing the generalizability of these results. Injury data were also stratified by position and body part, increasing the clinical interpretability of these findings. Publicly available data and open-source code were utilized in this study, increasing the transparency and access of these methods and results. Only NBA injuries were assessed, decreasing the generalizability of these findings to the other professional basketball leagues or amateur basketball. The public nature of these data does not allow for missing data to be quantified, decreasing the precision of these results; however, external data validation was performed using other publicly available data to increase the interpretability of these results. Misclassification bias is also a possibility especially because injuries that did not result in time loss were not recorded, decreasing the precision of these data. Furthermore, injury temporal trends were calculated from the first missed game. Injuries that were sustained in a previous game, practice, or training session could not be accurately determined, decreasing the precision of the temporal and severity analyses. Previous literature 9,11,37 has used number of days missed to classify injury severity; however, because of the use of publicly available data, it was determined that using games missed would decrease bias. Nevertheless, this decreases the interpretability of the results. Subclinical injuries that did not result in games missed were not captured in these data. Basketball exposure could only be quantified by games played and not by minutes played, decreasing the precision of these findings. Some injuries were reported to the nearest body part, with further injury body part classification (eg, ankle injury vs lateral ankle sprain) not possible, decreasing the clinical interpretability of these findings. Basketball performance data were not included in this study, decreasing the basketball interpretability of these data.
Conclusion
The ankle and knee were observed to have the greatest injury incidence, with knee injuries having the greatest severity of injury incidence. Injury incidence was similar based on basketball position, and these relationships were similar for injury severity and monthly and yearly temporal trends. Injury incidence increased throughout the season, demonstrating the potential relationship between season player load and injury incidence. Yearly injury temporal trends demonstrated similar injury incidence rates throughout the 11-year study span except for the 2012 lockout-shortened season, which showed almost double the incidence of severe injuries.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211004094 for Temporal Trends and Severity in Injury and Illness Incidence in the National Basketball Association Over 11 Seasons by Garrett S. Bullock, Tyler Ferguson, Jake Vaughan, Desiree Gillespie, Gary Collins and Stefan Kluzek in Orthopaedic Journal of Sports Medicine
Supplemental Material, sj-xlsx-1-ojs-10.1177_23259671211004094 for Temporal Trends and Severity in Injury and Illness Incidence in the National Basketball Association Over 11 Seasons by Garrett S. Bullock, Tyler Ferguson, Jake Vaughan, Desiree Gillespie, Gary Collins and Stefan Kluzek in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 12, 2020; accepted November 22, 2020
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211004094.
References
- 1. Alfonso F, Adamyan K, Artigou JY, et al. Data sharing: a new editorial initiative of the International Committee of Medical Journal Editors. Implications for the Editors’ Network. Cardiologia Croatica. 2017;12(5-6):264–272. [Google Scholar]
- 2. Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701. [DOI] [PubMed] [Google Scholar]
- 3. Bahr R, Clarsen B, Derman W, et al. International Olympic Committee Consensus Statement: methods for recording and reporting of epidemiological data on injury and illness in sports 2020 (including the STROBE Extension for Sports Injury and Illness Surveillance (STROBE-SIIS)). Orthop J Sports Med. 2020;8(2):232596712090290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Baker M. 1,500 scientists lift the lid on reproducibility. Nature. 2016;533(7604):452–454. [DOI] [PubMed] [Google Scholar]
- 5. Bertagnolli MM, Sartor O, Chabner BA, et al. Advantages of a truly open-access data-sharing model. New Engl J Med. 2017;376(12):1178. [DOI] [PubMed] [Google Scholar]
- 6. Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005–2007. Am J Sports Med. 2008;36(12):2328–2335. [DOI] [PubMed] [Google Scholar]
- 7. Brunner MC, Flower SP, Evancho AM, Allman FL, Apple DF, Fajman WA. MRI of the athletic knee: findings in asymptomatic professional basketball and collegiate football players. Investigative Radiol. 1989;24(1):72–75. [DOI] [PubMed] [Google Scholar]
- 8. Busfield BT, Kharrazi FD, Starkey C, Lombardo SJ, Seegmiller J. Performance outcomes of anterior cruciate ligament reconstruction in the National Basketball Association. Arthroscopy. 2009;25(8):825–830. [DOI] [PubMed] [Google Scholar]
- 9. Deitch JR, Starkey C, Walters SL, Moseley JB. Injury risk in professional basketball players: a comparison of Women’s National Basketball Association and National Basketball Association athletes. Am J Sports Med. 2006;34(7):1077–1083. [DOI] [PubMed] [Google Scholar]
- 10. Dick R, Hertel J, Agel J, Grossman J, Marshall SW. Descriptive epidemiology of collegiate men’s basketball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):194. [PMC free article] [PubMed] [Google Scholar]
- 11. Drakos MC, Domb B, Starkey C, Callahan L, Allen AA. Injury in the National Basketball Association: a 17-year overview. Sports Health. 2010;2(4):284–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9(1-2):3–10. [DOI] [PubMed] [Google Scholar]
- 13. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand J Med Sci Sports. 2006;16(2):83–92. [DOI] [PubMed] [Google Scholar]
- 14. Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273–280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hägglund M, Waldén M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med. 2005;39(6):340–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hayes J, Orchard J. Using the World Wide Web to conduct epidemiological research: an example using the National Basketball Association. Int J Sports Med. 2001;2(2):1–15. [Google Scholar]
- 17. Hertel J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J Athl Train. 2002;37(4):364. [PMC free article] [PubMed] [Google Scholar]
- 18. Kellmann M. Preventing overtraining in athletes in high-intensity sports and stress/recovery monitoring. Scand J Med Sci Sports. 2010;20:95–102. [DOI] [PubMed] [Google Scholar]
- 19. Landers RN, Brusso RC, Cavanaugh KJ, Collmus AB. A primer on theory-driven web scraping: automatic extraction of big data from the Internet for use in psychological research. Psych Method. 2016;21(4):475. [DOI] [PubMed] [Google Scholar]
- 20. McAfee A, Brynjolfsson E, Davenport TH, Patil D, Barton D. Big data: the management revolution. Harvard Business Rev. 2012;90(10):60–68. [PubMed] [Google Scholar]
- 21. McClay IS, Robinson JR, Andriacchi TP, et al. A profile of ground reaction forces in professional basketball. J Appl Biomech. 1994;10(3):222–236. [Google Scholar]
- 22. McKay GD, Goldie P, Payne WR, Oakes B. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med. 2001;35(2):103–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Meeusen R, Duclos M, Foster C, et al. Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc. 2013;45(1):186. [DOI] [PubMed] [Google Scholar]
- 24. Newman K. Go public! Using publicly available data to understand the foreclosure crisis. J Am Planning Assoc. 2010;76(2):160–171. [Google Scholar]
- 25. Oki NO, Nelms MD, Bell SM, Mortensen HM, Edwards SW. Accelerating adverse outcome pathway development using publicly available data sources. Curr Environ Health Rep. 2016;3(1):53–63. [DOI] [PubMed] [Google Scholar]
- 26. Orchard J, Rae K, Brooks J, et al. Revision, uptake and coding issues related to the open access Orchard Sports Injury Classification System (OSICS) versions 8, 9 and 10.1. Open Access J Sports Med. 2010;1:207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Patel BH, Okoroha KR, Jildeh TR, et al. Concussions in the National Basketball Association: analysis of incidence, return to play, and performance from 1999 to 2018. Orthop J Sports Med. 2019;7(6):2325967119854199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Payne KA, Berg K, Latin RW. Ankle injuries and ankle strength, flexibility, and proprioception in college basketball players. J Athl Train. 1997;32(3):221. [PMC free article] [PubMed] [Google Scholar]
- 29. Podlog L, Buhler CF, Pollack H, Hopkins PN, Burgess PR. Time trends for injuries and illness, and their relation to performance in the National Basketball Association. J Sci Med Sport. 2015;18(3):278–282. [DOI] [PubMed] [Google Scholar]
- 30. Riva D, Bianchi R, Rocca F, Mamo C. Proprioceptive training and injury prevention in a professional men’s basketball team: a six-year prospective study. J Strength Cond Res. 2016;30(2):461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Rogalski B, Dawson B, Heasman J, Gabbett TJ. Training and game loads and injury risk in elite Australian footballers. J Sci Med Sport. 2013;16(6):499–503. [DOI] [PubMed] [Google Scholar]
- 32. Schiltz M, Lehance C, Maquet D, Bury T, Crielaard JM, Croisier JL. Explosive strength imbalances in professional basketball players. J Athl Train. 2009;44(1):39–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Schwellnus M, Soligard T, Alonso JM, et al. How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br J Sports Med. 2016;50(17):1043–1052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Shalfawi SA, Sabbah A, Kailani G, Tønnessen E, Enoksen E. The relationship between running speed and measures of vertical jump in professional basketball players: a field-test approach. J Strength Cond Res. 2011;25(11):3088–3092. [DOI] [PubMed] [Google Scholar]
- 35. Smith S. What is the real cost of injuries in professional sport? Medium. Accessed June 4, 2020. https://medium.com/@stephensmith_ie/what-is-the-real-cost-of-injuries-in-professional-sport-fee1d66a7502
- 36. Soligard T, Schwellnus M, Alonso JM, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016;50(17):1030–1041. [DOI] [PubMed] [Google Scholar]
- 37. Starkey C. Injuries and illnesses in the National Basketball Association: a 10-year perspective. J Athl Train 2000;35(2):161. [PMC free article] [PubMed] [Google Scholar]
- 38. Wikipedia. 2012. NBA lockout. Accessed June 4, 2020. https://en.wikipedia.org/wiki/2011_NBA_lockout
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211004094 for Temporal Trends and Severity in Injury and Illness Incidence in the National Basketball Association Over 11 Seasons by Garrett S. Bullock, Tyler Ferguson, Jake Vaughan, Desiree Gillespie, Gary Collins and Stefan Kluzek in Orthopaedic Journal of Sports Medicine
Supplemental Material, sj-xlsx-1-ojs-10.1177_23259671211004094 for Temporal Trends and Severity in Injury and Illness Incidence in the National Basketball Association Over 11 Seasons by Garrett S. Bullock, Tyler Ferguson, Jake Vaughan, Desiree Gillespie, Gary Collins and Stefan Kluzek in Orthopaedic Journal of Sports Medicine