

Abstract
BACKGROUND:
In recent times, mental health problems have been on the increase worldwide. Among these are eating disorders. The current study aim was to assess the prevalence of the symptoms of eating disorders in patrons of sport centers in the Eastern Province of Saudi Arabia, and its association with patrons' sociodemographic, and exercise characteristics, as well as social media use.
MATERIALS AND METHODS:
This cross-sectional study was conducted among 560 sport center clients. The Eating Attitude Test (EAT-26), as well as questions on sociodemographic, exercise, and the use of the social media was collected through self-administered questionnaires. Descriptive statistics, Chi-squared test, and Fischer's exact tests were performed.
RESULTS:
The prevalence of the symptoms of eating disorders was found to be 36.6% according to the results of the EAT-26. There were no significant differences in the rates of eating disorders between genders. Frequencies of eating disorder symptoms increased with an increase in the body mass index of the participants. In addition, more than half of the participants who were pressured by social media to be slim and perceived that social media influencers motivated them to go to the gym had eating disorders' symptoms.
CONCLUSION:
The prevalence of eating disorders symptoms was high among the sport center patrons examined. The findings from this study might help family physicians, mental health professionals, and sport medicine specialists wishing to understand this issue in Arab populations. Developing strategies regarding mental health in sport center patrons are suggested. In addition, a screening program is recommended for this population to identify those who need further evaluation and management.
Keywords: Eating disorders, exercise, social media, sport centers
Introduction
Mental health problems have been increasing globally in recent decades and among these problems are eating disorders, which are rapidly rising, particularly in young women.[1]
Eating disorders are characterized by a persistent disruption of eating or behaviors related to eating, which is linked to the intake or absorption of nutrition and which consequently affects physical or psychological health. These disorders include avoidant/restrictive food intake disorder, rumination disorder, pica, bulimia nervosa, anorexia nervosa, and binge-eating disorder.[2]
Studies have revealed the paucity of data on the prevalence of eating disorders in the general population and many reported epidemiological studies have used case registers in psychiatry departments and patient records in hospitals. Moreover, patients usually deny or suppress their illness to avoid seeking professional advice.[3,4]
In the past, eating disorders have been reported specifically in industrialized and Western cultures. However, of late, eating disorders and behavioral eating problems have been reported in non-Western populations, including Arab countries. An increasing rate of eating disorders in non-Western cultures has been associated with globalization, transition in the cultures, urbanization, modernization, and the impact of media that promote Western ideals of beauty.[3,4]
Literature shows that the media plays an important role in articulating what society perceives as an attractive appearance. Increasing slimness and muscular beauty ideals which sometimes are unattainable, significantly lead to disturbed body image, body dissatisfaction, and eating disorders.[1]
The attention to eating disorders and exercise has been on the increase. A review reported that eating disorders were more prevalent in both genders of adult athletes compared to nonathletes, and the prevalence was higher in females (6%–45%) as compared to males (0%–19%).[5] The pressure to lose weight, regular weight monitoring, dieting, coaching behaviors, and personality traits of the subject such as perfectionism have all increased the burden on athletes who then become vulnerable to eating disorders.[5]
Limited studies conducted on eating disorders in Saudi Arabia have been focused on female students.[6,7,8] Moreover, to the best of our knowledge, no prior study has been carried out to assess eating disorders in sport center patrons. One of the main objectives of “The quality of life program,” a major program in Vision 2030 in Saudi Arabia, is to increase public participation in sports and athletic activities. Therefore, the demand to explore this issue is increasing.[9]
The objective of this study was to assess the prevalence of eating disorders' symptoms in sport center patrons in the Eastern Province of Saudi Arabia and to assess its association with patrons' sociodemographic characteristics and exercising pattern, as well as their use of the social media.
Materials and Methods
This cross-sectional study was conducted on sport center patrons in three major cities in the Eastern Province of Saudi Arabia (Qatif, Dammam, and Khobar cities) between December 2019 and January 2020.
Sport center clients aged 18–60 years old of both genders were included in the study. The exclusion criteria included those with any medical conditions that could affect weight and appetite, such as pregnancy, malignancy or the use of chemo or radiotherapy, thyroid diseases, use of systemic corticosteroids, and diabetes mellitus.
The calculated minimum required sample size was 498 participants. This was calculated using Epi Info™ (a database and statistics program for public health professionals. CDC, Atlanta, GA, USA), a 29.4% prevalence of eating disorder as reported in a previous Saudi study that used Eating Attitude Test-26 (EAT-26) tool, at a 95% confidence level and margin of error of 4%.[6] The sample size was increased to 600 to overcome any potential missing values.
A list of sport centers in each city was obtained from the Ministry of Commerce. This list included 14, 21, and 27 centers from Qatif, Dammam, and Khobar cities, respectively. These sport centers are private, and the members pay for registration. The sample included 16 sport centers (8 for males and 8 for females) as the following: 4 from Qatif, 8 from Dammam, and 4 from Khobar cities. The sample was divided proportionately between the three cities according to their populations, and equally between male and female sport centers. In each city, the sample was further divided equally between sport centers with high and low monthly membership costs. The sport centers from each category (low and high monthly membership cost) in each city were selected through a simple random sampling technique, and the selection of patrons from each center was by a convenient sample.
The data were collected by a paper-based, self-administered questionnaire comprising questions on sociodemographic characteristics, self-reported anthropometric data, EAT-26, exercising patterns, and social media usage.
EAT-26 questionnaire, a tool established by Garner and Garfinkel in 1979, is composed of 26 items and participants were asked to rate their answers on a 6-point Likert scale (always = 3, usually = 2, often = 1, sometimes, rarely and never = 0 for items 1–25, and the reverse direction of scoring for item 26). At the end of the questionnaire were five eating behavior questions and selecting one of these 5 questions indicated that the participant had a problematic eating behavior. A total score of 20 or more on the EAT-26 indicated that the participant was at risk of developing an eating disorder. Participants who scored 20 or more in EAT-26 or who selected any of the 5 additional eating behavior questions were considered for referral to a qualified mental health professional for further evaluation.[6,7,10]
EAT-26 is a highly sensitive, reliable screening tool used in previous studies to assess eating disorder risks in students at high school or college, and athletes.[6,7,10,11] However, the EAT-26 alone does not provide a definite diagnosis of eating disorders and further clinical evaluation is crucial.[1,10]
Body mass index (BMI) was calculated according to the self-reported weight and height based on the following equation: Body weight (in kg) divided by height (in m2) and then the BMI (in kg/m2) was categorized as: Underweight (BMI <18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25.0–29.9), and obese (BMI ≥30.0).[11]
Questions on exercising patterns included perceived importance of exercise and level of fitness, exercise frequency, preference, time, and the usual duration spent in the gym.
The part in the questionnaire concerning the social media use included questions on the perceived effects of the social media on fitness, diet, weight, and eating disorders.
Two versions of the questionnaire (Arabic and English) were developed, and four experts reviewed the two versions to enhance content validity. The EAT-26 tool had been previously used and validated in Saudi studies.[6,7,8] However, it was novel to the population in the current study, and so was tested in a pilot study on 50 sport center patrons, who were excluded from the sample, to ensure clarity of terms and questions used. After the pilot study, no major modifications were made to the questions. The internal consistency for the EAT-26 scale was found to be good (Cronbach's coefficient = 0.82).
Ethical approval was obtained from the Institutional Review Board of Imam Abdulrahman Bin Faisal University vide letter No. IRB-PGS-2019-01-398 dated 19/12/2019, and informed written consent was taken from all participants in the study.
Descriptive analysis was performed by counts and percentages for the categorical variables and means ± standard deviations for the continuous variables. The study had three main outcomes; risk of eating disorders (≥20 as high risks), problematic eating behavior (choosing any of the five behavioral questions), and the need for a referral to a mental health professional (≥20 on EAT-26 or choosing any of the five behavioral questions). Bivariate analysis was done through the Chi-squared and Fischer's exact test where applicable. All statistical analyses were performed using the IBM SPSS for Windows, Version 24.0. (IBM Corp., Armonk, NY, USA).[12] P < 0.05 was considered statistically significant.
Results
A total of 560 participants, aged between 18 and 60 years old, with a mean age of 31 ± 9 years completed the questionnaires (93.3% response rate). All sociodemographic characteristics are presented in Table 1. Of the participants, 36.6% were categorized as at a high level of concern for eating disorders based on the EAT-26 scores, 76.6% were categorized with problematic eating behavior, and 80.9% were categorized as needing a referral to a mental health professional [Figure 1].
Table 1.
Sociodemographic characteristics of sport center patrons in Saudi Arabia according to the level of concern due to eating disorders, problematic eating behavior and need for referral to a mental health professional
| Characteristics | Total (n=560) N (%) | EAT-26 (level of eating disorder concern) | Problematic eating behavior | Referral need to mental health professional | |||
|---|---|---|---|---|---|---|---|
| LowN (%) | HighN (%) | LowN (%) | High N (%) | NoN (%) | YesN (%) | ||
| Gender | |||||||
| Males | 286 (51.1) | 190 (66.4) | 96 (33.6) | 76 (26.6) | 210 (73.4) | 62 (21.7) | 224 (78.3) |
| Females | 274 (48.9) | 165 (60.2) | 109 (39.8) | 55 (20.1) | 219 (79.9) | 45 (16.4) | 229 (83.6) |
| P-value | 0.12 | 0.06 | 0.13 | ||||
| Age group (years) | |||||||
| 18 - <30 | 279 (49.8) | 174 (62.4) | 105 (37.6) | 69 (24.7) | 210 (75.3) | 57 (20.4) | 222 (79.6) |
| 30 - <40 | 181 (32.3) | 116 (64.1) | 65 (35.9) | 28 (15.5) | 153 (84.5) | 24 (13.3) | 157 (86.7) |
| 40 - <50 | 59 (10.5) | 34 (57.6) | 25 (42.4) | 21 (35.6) | 38 (64.4) | 16 (27.1) | 43 (72.9) |
| 50 - 60 | 41 (07.3) | 31 (75.6) | 10 (24.4) | 13 (31.7) | 28 (68.3) | 10 (24.4) | 31 (75.6) |
| P-value | 0.30 | 0.004 | 0.05 | ||||
| City | |||||||
| Dammam | 285 (50.9) | 169 (47.6) | 116 (56.6) | 68 (51.9) | 217 (50.6) | 55 (51.4) | 230 (50.8) |
| Khobar | 131 (23.4) | 86 (24.2) | 45 (22.0) | 37 (28.2) | 94 (21.9) | 30 (28.0) | 101 (22.3) |
| Qatif | 144 (25.7) | 100 (28.2) | 44 (21.5) | 26 (19.8) | 118 (27.5) | 22 (20.6) | 122 (26.9) |
| P-value | 0.09 | 0.13 | 0.27 | ||||
| Marital status | |||||||
| Single | 266 (47.5) | 170 (63.9) | 96 (36.1) | 68 (25.6) | 198 (74.4) | 59 (22.2) | 207 (77.8) |
| Married | 278 (49.6) | 175 (62.9) | 103 (37.1) | 59 (21.2) | 219 (78.8) | 45 (16.2) | 233 (83.8) |
| Divorced | 16 (02.9) | 10 (62.5) | 6 (37.5) | 4 (25.0) | 12 (75.0) | 3 (18.8) | 13 (81.2) |
| P-value | 0.97 | 0.48 | 0.20 | ||||
| Educational level | |||||||
| High school | 247 (44.1) | 149 (60.3) | 98 (39.7) | 57 (23.1) | 190 (76.9) | 47 (19.0) | 200 (81.0) |
| Bachelors | 288 (51.4) | 190 (66.0) | 98 (34.0) | 70 (24.3) | 218 (75.7) | 58 (20.1) | 230 (79.9) |
| Higher education (masters/PhD) | 25 (04.5) | 16 (64.0) | 9 (36.0) | 4 (16.0) | 21 (84.0) | 2 (08.0) | 23 (92.0) |
| P-value | 0.40 | 0.63 | 0.33 | ||||
| Living with | |||||||
| Family | 254 (45.4) | 163 (64.2) | 91 (35.8) | 65 (25.6) | 189 (74.4) | 56 (22.0) | 198 (78.0) |
| Alone | 89 (15.9) | 56 (62.9) | 33 (37.1) | 24 (27.0) | 65 (73.0) | 19 (21.3) | 70 (78.7) |
| Spouse | 217 (38.7) | 136 (62.7) | 81 (37.3) | 42 (19.4) | 175 (80.6) | 32 (14.7) | 185 (85.3) |
| P-value | 0.94 | 0.19 | 0.11 | ||||
| Occupation | |||||||
| Student | 95 (17.0) | 65 (68.4) | 30 (31.6) | 27 (28.4) | 68 (71.6) | 26 (27.4) | 69 (72.6) |
| Administrative | 118 (58.0) | 75 (63.6) | 43 (36.4) | 26 (22.0) | 92 (78.0) | 24 (20.3) | 94 (79.7) |
| Engineering | 58 (10.4) | 40 (69.0) | 18 (31.0) | 11 (19.0) | 47 (81.0) | 8 (13.8) | 50 (86.2) |
| Healthcare | 77 (13.8) | 51 (66.2) | 26 (33.8) | 17 (22.1) | 60 (77.9) | 15 (19.5) | 62 (80.5) |
| Military | 13 (02.3) | 4 (30.8) | 9 (69.2) | 5 (38.5) | 8 (61.5) | 2 (15.4) | 11 (84.6) |
| Teaching | 47 (08.4) | 28 (59.6) | 19 (40.4) | 10 (21.3) | 37 (78.7) | 7 (14.9) | 40 (85.1) |
| Business | 21 (03.8) | 13 (61.9) | 8 (38.1) | 6 (28.6) | 15 (71.4) | 4 (19.0) | 17 (81.0) |
| Unemployed/retired | 131 (23.4) | 79 (60.3) | 52 (39.7) | 29 (22.1) | 102 (77.9) | 21 (16.0) | 110 (84.0) |
| P-value | 0.26 | 0.73 | 0.73 | ||||
| Monthly income (SR) | |||||||
| < 5,000 | 90 (16.1) | 58 (64.4) | 32 (35.6) | 23 (25.6) | 67 (74.4) | 21 (23.3) | 69 (76.7) |
| 5,000 - <10,000 | 219 (39.1) | 139 (63.5) | 80 (36.5) | 56 (25.6) | 163 (74.4) | 45 (20.5) | 174 (79.5) |
| ≥10,000 | 251 (44.8) | 158 (62.9) | 93 (37.1) | 52 (20.7) | 199 (79.3) | 41 (16.3) | 210 (83.7) |
| P-value | 0.96 | 0.40 | 0.27 | ||||
EAT=Eating attitude test, SR=Saudi riyals
Figure 1.
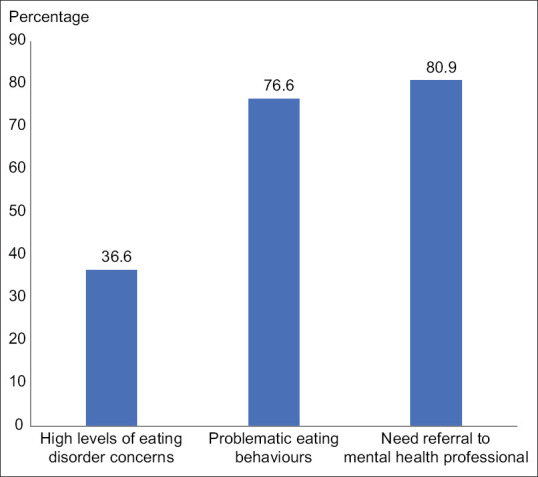
Distribution of high level of concern about eating disorders, risk of problematic eating behavior, and need for referral to mental health professional among sport center participants in Saudi Arabia
No statistically significant difference was found between eating disorders, problematic eating behavior and the need for referral to a mental health professional, and gender, marital status, city of the sport center, educational level, living alone or with family, occupation, or monthly income. However, in the 30 < 40 year age group, 84.5% were classified as high risk for problematic eating behavior (P = 0.004) [Table 1].
Table 2 shows the distribution of the health status characteristics of our sample. Average sleeping hours was associated significantly with a need for referral to a mental health professional (P = 0.02). 83.3% of participants who slept <5 h required referral to mental health professional. On the other hand, 68.2% of participants who slept for more than 8 h required referral. BMI was statistically significant with all three outcomes, and the frequencies of eating disorder symptoms increased with an increase in BMI of the respondents according to EAT-26 scores. Participants who were classified as being within the high-risk eating behaviors comprised 84.6% of the obese, 80.3% of the overweight, and 73.7% of those who were underweight. The need for referral to a mental health professional was indicated for 90.6% of the obese, 84.2% of the overweight participants, and 78.9% of participants who were underweight [Figure 2].
Table 2.
Health status characteristics of sport center patrons in Saudi Arabia according to the level of concern about eating disorders, problematic eating behavior and need for referral to a mental health professional
| Characteristics | Total (n=560) N (%) | EAT-26 (level of eating disorder concern) | Problematic eating behavior | Referral need to mental health professional | |||
|---|---|---|---|---|---|---|---|
| LowN (%) | HighN (%) | LowN (%) | High N (%) | NoN (%) | YesN (%) | ||
| Chronic diseases | |||||||
| Yes | 62 (11.1) | 39 (62.9) | 23 (37.1) | 16 (25.8) | 46 (74.2) | 12 (19.4) | 50 (80.6) |
| No | 498 (88.9) | 316 (63.5) | 182 (36.5) | 115 (23.1) | 3883 (76.9) | 95 (19.1) | 403 (80.9) |
| P-value | 0.93 | 0.63 | 0.95 | ||||
| Average sleeping h/day | |||||||
| <5 | 42 (07.5) | 21 (50.0) | 21 (50.0) | 11 (26.2) | 31 (73.8) | 7 (16.7) | 35 (83.3) |
| 5-8 | 452 (80.7) | 289 (63.9) | 163 (36.1) | 98 (21.7) | 354 (78.3) | 79 (17.5) | 373 (82.5) |
| >8 | 66 (11.8) | 45 (68.2) | 21 (31.8) | 22 (33.3) | 44 (66.7) | 21 (31.8) | 45 (68.2) |
| P-value | 0.13 | 0.10 | 0.02 | ||||
| Regularity of menses among females | |||||||
| Regular | 213 (79.8) | 130 (61.0) | 83 (39.0) | 44 (20.7) | 169 (79.3) | 36 (16.9) | 177 (83.1) |
| Irregular | 54 (20.2) | 31 (57.4) | 23 (42.6) | 10 (18.5) | 44 (81.5) | 8 (14.8) | 46 (85.2) |
| P-value | 0.62 | 0.72 | 0.71 | ||||
EAT=Eating attitude test
Figure 2.
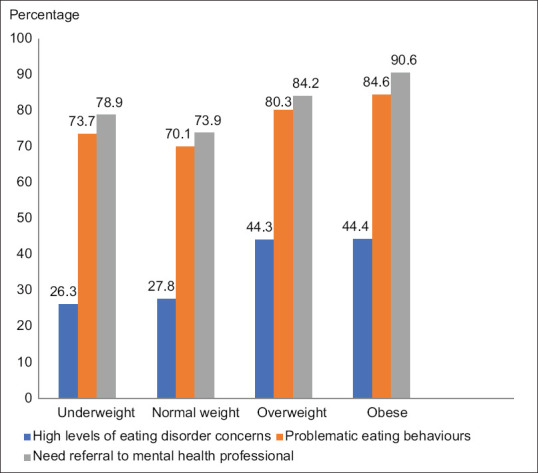
Distribution of high level of concern about eating disorders, risk of problematic eating behavior, and need for referral to mental health professional among sport center participants in Saudi Arabia according to their body mass index categories
Participants who said that their families thought they exercised too much or too frequently gave a higher level of concern for eating disorders (54.1%), problematic eating behavior (91.9%), and a need for referral to mental health professionals (92.8%) than their counterparts (P < 0.001) [Table 3]. Similar associations were seen with participants who perceived that exercise was very important. Increasing the self-perceived level of fitness from beginners to advanced among the participants was associated with an increase in the frequencies of a high level of concern of eating disorder (from 34% to 51.1%, P = 0.009) and problematic eating behavior (from 65.1% to 83%, P = 0.005). Exercise frequency was significantly associated with the three outcomes in Table 3 and higher rates reported in participants who exercised more frequently per week (P < 0.001). Frequencies of problematic eating behavior and the need for referral to mental health professionals were found more in participants who reported that they spent more time in the gym (P < 0.001).
Table 3.
Exercising patterns of sport center patrons in Saudi Arabia according to the level of concern about eating disorders, problematic eating behavior and need for referral to a mental health professional
| Characteristics | Total (n=560) N (%) | EAT-26 (level of eating disorder concern) | Problematic eating behavior | Referral need to mental health professional | |||
|---|---|---|---|---|---|---|---|
| LowN (%) | HighN (%) | LowN (%) | High N (%) | NoN (%) | YesN (%) | ||
| Family think you exercise too much | |||||||
| Yes | 111 (19.8) | 51 (45.9) | 60 (54.1) | 9 (08.1) | 102 (91.9) | 8 (07.2) | 103 (92.8) |
| No | 449 (80.2) | 304 (67.7) | 145 (32.3) | 122 (27.2) | 327 (72.8) | 99 (22.0) | 350 (78.0) |
| P-value | <0.001 | <0.001 | <0.001 | ||||
| Perceived importance of exercise | |||||||
| Very important | 446 (79.6) | 268 (60.1) | 178 (39.9) | 86 (19.3) | 360 (80.7) | 69 (15.5) | 377 (84.5) |
| Moderately important | 90 (16.1) | 68 (75.6) | 22 (24.2) | 35 (38.9) | 55 (61.1) | 30 (33.3) | 60 (66.7) |
| Slightly important | 274 (04.3) | 19 (79.2) | 5 (20.8) | 10 (41.7) | 14 (58.3) | 8 (33.3) | 16 (66.7) |
| P-value | 0.005 | <0.001 | <0.001 | ||||
| Perceived level of fitness | |||||||
| Beginner | 106 (18.9) | 70 (66.0) | 36 (34.0) | 37 (34.9) | 69 (65.1) | 27 (25.5) | 79 (74.5) |
| Intermediate | 366 (65.4) | 242 (66.1) | 124 (33.9) | 79 (21.6) | 287 (78.4) | 67 (18.3) | 299 (81.7) |
| Advanced | 88 (15.7) | 43 (48.9) | 45 (51.1) | 15 (17.0) | 73 (83.0) | 13 (14.8) | 75 (85.2) |
| P-value | 0.009 | 0.005 | 0.13 | ||||
| Exercise frequency | |||||||
| 1-2 times a week | 136 (24.3) | 104 (76.5) | 32 (23.5) | 55 (40.4) | 81 (59.6) | 46 (33.8) | 90 (66.2) |
| 3-4 times a week | 193 (34.5) | 131 (67.9) | 62 (32.1) | 46 (23.8) | 147 (76.2) | 38 (19.7) | 155 (80.3) |
| >4 times a week | 231 (41.2) | 120 (51.9) | 111 (48.1) | 30 (13.0) | 201 (87.0) | 23 (10.0) | 208 (90.0) |
| P-value | <0.001 | <0.001 | <0.001 | ||||
| Exercise preference | |||||||
| Alone | 196 (35.0) | 113 (57.7) | 83 (42.3) | 40 (20.4) | 156 (79.6) | 33 (16.8) | 163 (83.2) |
| With a friend | 156 (27.9) | 103 (66.0) | 53 (34.0) | 46 (29.5) | 110 (70.5) | 36 (23.1) | 120 (76.9) |
| In a group or class | 208 (37.1) | 139 (66.8) | 69 (33.2) | 45 (21.6) | 163 (78.4) | 38 (18.3) | 170 (81.7) |
| P-value | 0.11 | 0.10 | 0.31 | ||||
| Exercise time | |||||||
| Morning | 176 (31.4) | 109 (61.9) | 67 (38.1) | 42 (23.9) | 134 (76.1) | 35 (19.9) | 141 (80.1) |
| Afternoon | 282 (50.4) | 174 (61.7) | 108 (38.3) | 65 (23.0) | 217 (77.0) | 51 (18.1) | 231 (81.9) |
| Evening | 102 (18.2) | 72 (70.6) | 30 (29.4) | 24 (23.5) | 78 (76.5) | 21 (20.6) | 81 (79.4) |
| P-value | 0.24 | 0.98 | 0.81 | ||||
| Time spent in the gym per day (min) | |||||||
| <30 | 118 (21.1) | 86 (72.9) | 32 (27.1) | 50 (42.4) | 68 (57.6) | 41 (34.7) | 77 (65.3) |
| 30 - <60 | 215 (38.4) | 136 (63.3) | 79 (36.7) | 44 (20.5) | 171 (79.5) | 33 (15.3) | 182 (84.7) |
| 60 - <90 | 134 (23.9) | 82 (61.2) | 52 (38.8) | 27 (20.1) | 107 (79.9) | 26 (19.4) | 108 (80.6) |
| ≥90 | 93 (16.6) | 51 (54.8) | 42 (45.2) | 10 (10.8) | 83 (89.2) | 7 (07.5) | 86 (92.5) |
| P-value | 0.05 | <0.001 | <0.001 | ||||
EAT=Eating attitude test
Patterns of social media usage relating to eating disorders and problematic eating behavior are presented in Table 4. Of the total sample, 42.7% reported that the social media encouraged them to stay fit and 41.4% of them reported high scores in EAT-26 (P = 0.03). More than half of participants (52.2%) who reported to be motivated by influencers in the social media to go to the gym had higher scores of EAT-26 (P < 0.001). Participants who used the social media to improve their diet and for weight loss had a problematic eating behavior (85.7%, P = 0.008, and 85.3%, P = 0.01, respectively) and need for referral to a mental health professional l (89.1%, P = 0.01, and 88.8%, P = 0.02, respectively).
Table 4.
Social media use relating to exercise among sport center patrons in Saudi Arabia according to the level of concern about eating disorders, problematic eating behavior and need for referral to a mental health professional
| Characteristics | Total (n=560) N (%) | EAT-26 (level of eating disorder concern) | Problematic eating behavior | Referral need to mental health professional | |||
|---|---|---|---|---|---|---|---|
| LowN (%) | HighN (%) | Low N (%) | High N (%) | NoN (%) | YesN (%) | ||
| Social media encourages me to stay fit | |||||||
| Yes | 239 (42.7) | 140 (58.6) | 99 (41.4) | 51 (21.3) | 188 (78.7) | 42 (17.6) | 197 (82.4) |
| No | 114 (20.4) | 83 (72.8) | 31 (27.2) | 36 (31.6) | 78 (68.4) | 29 (25.4) | 85 (74.6) |
| Sometimes | 207 (37.0) | 132 (63.8) | 75 (36.2) | 44 (21.3) | 163 (78.7) | 36 (17.4) | 171 (82.6) |
| P-value | 0.03 | 0.06 | 0.15 | ||||
| A social media influencer motivated me to go to the gym | |||||||
| Yes | 115 (20.5) | 55 (47.8) | 60 (52.2) | 23 (20.0) | 92 (80.0) | 16 (13.9) | 99 (86.1) |
| No | 360 (64.3) | 251 (69.7) | 109 (30.3) | 83 (23.1) | 277 (76.9) | 71 (19.7) | 289 (80.3) |
| Sometimes | 85 (15.2) | 49 (57.6) | 36 (42.4) | 25 (29.4) | 60 (70.6) | 20 (23.5) | 65 (76.5) |
| P-value | <0.001 | 0.28 | 0.20 | ||||
| Using social media to improve diet | |||||||
| Yes | 147 (26.2) | 84 (57.1) | 63 (42.9) | 21 (14.3) | 126 (85.7) | 16 (10.9) | 131 (89.1) |
| No | 357 (63.8) | 236 (66.1) | 121 (33.9) | 93 (26.1) | 264 (73.9) | 79 (22.1) | 278 (77.9) |
| Sometimes | 56 (10.0) | 35 (62.5) | 21 (37.5) | 17 (30.4) | 39 (69.6) | 12 (21.4) | 44 (78.6) |
| P-value | 0.16 | 0.008 | 0.01 | ||||
| Using social media groups for weight loss | |||||||
| Yes | 143 (25.5) | 81 (56.6) | 62 (43.4) | 21 (14.7) | 122 (85.3) | 16 (11.2) | 127 (88.8) |
| No | 340 (60.7) | 226 (66.5) | 114 (33.5) | 89 (26.2) | 251 (73.8) | 74 (21.8) | 266 (78.2) |
| Sometimes | 77 (13.8) | 48 (62.3) | 29 (37.7) | 21 (27.30) | 56 (72.7) | 17 (22.1) | 60 (77.9) |
| P-value | 0.12 | 0.01 | 0.02 | ||||
| Social media pressures me to be slim | |||||||
| Yes | 77 (13.8) | 30 (39.0) | 47 (61.0) | 7 (09.1) | 70 (90.9) | 6 (07.8) | 71 (92.2) |
| No | 295 (52.7) | 206 (69.8) | 89 (30.2) | 75 (25.4) | 220 (74.6) | 62 (21.0) | 233 (79.0) |
| Sometimes | 188 (33.6) | 119 (63.3) | 69 (36.7) | 49 (26.1) | 139 (73.9) | 39 (20.7) | 149 (79.3) |
| P-value | <0.001 | 0.006 | 0.02 | ||||
| Social media is a contributing factor in eating disorders | |||||||
| Yes | 185 (33.0) | 109 (58.9) | 76 (41.1) | 36 (19.5) | 149 (80.5) | 29 (15.7) | 156 (84.3) |
| No | 179 (32.0) | 119 (66.5) | 60 (33.5) | 53 (29.6) | 126 (70.4) | 41 (22.9) | 138 (77.1) |
| Sometimes | 196 (35.0) | 127 (64.8) | 69 (35.2) | 42 (21.4) | 154 (78.6) | 37 (18.9) | 159 (81.1) |
| P-value | 0.28 | 0.05 | 0.21 | ||||
EAT=Eating attitude test
Participants who reported that the social media put pressure on them to be a slim had a higher EAT-26 scores (P < 0.001), more problematic eating behavior (P = 0.006), and the need for referral (P = 0.02).
Discussion
The current study contributes to the literature on the prevalence of eating disorders and its associated factors in sport center patrons in Saudi Arabia. Several studies from western countries have also investigated the prevalence of eating disorders in sport center clients. Differences in methodology, study tools, participants' characteristics, and sociocultural backgrounds make it difficult to compare the findings of the different studies. Moreover, data from Middle Eastern countries about this issue are sparse, and the majority are focused on adolescent females.[6,7,8] More than one-third of participants in our study were at a high level of concern for eating disorders according to the EAT-26 tool. This prevalence rate is slightly higher than the study of Alwosaifer et al., of 1st-year college female students in the Eastern Province of Saudi Arabia using the EAT-26 instrument which revealed that 29.4% had eating disorder symptoms.[6] Differences in the settings and age of the population involved could explain the variation between the prevalence reported in our study and the study referred to.
Studies from Western countries found that eating disorders were more common in athletes than nonathletes.[13] A large Norwegian study of 1620 athletes and 1696 controls revealed that 13.5% of the athletes and 4.6% of the controls had subclinical or clinical eating disorders based on the Diagnostic and Statistical Manual of Mental disorders criteria.[14] Studies have revealed that the prevalence of eating disorders in male athletes as 0%–19% and in female athletes as 6%–45%.[5]
A cross-sectional study of 755 athletes in Iceland using “Eating Disorder Examination Questionnaire” showed that 9.5% had symptoms of eating disorders.[15]
The higher rates reported in the current study may be attributed to many facts. Overweight and obesity, which are major driving forces of eating disorders, are both prevalent in the Middle Eastern countries, like Saudi Arabia. Therefore, high rates of eating disorders may be expected in these populations.[16] Consequently, the current study revealed that higher frequencies of eating disorder symptoms were found in participants with higher BMI. Similar results have been found in other studies in the Middle East.[6,8,16] Moreover, rapid advancement in life and the influence on beauty standards in the Middle East by the social media could eventually affect beliefs and perception of the ideal body weight and body image of both genders.[11,16] In line with this explanation is the fact that more than half of the participants in the current study who were said to have been encouraged by social media influencers to go to the gym had higher scores in EAT-26. Moreover, the majority of participants who used social media to improve the diet and weight had problematic eating behaviors and needed referral to a mental health provider. In addition, participants who reported that they were pressured by the social media to lose weight had higher EAT-26 scores, had more problematic eating behavior, and needed a referral to mental health providers. The family physicians have the important role of being a health advocate in the health-care system. In addition to their position in the frontline of patient care and their focus on maintaining doctor–patient relationship in the consultation, primary care providers should be vigilant when assessing their patients to detect any eating disorders early, provide the appropriate advice about diet and exercise, and correct any misconceptions.
In contrast to the studies which revealed that the prevalence of eating disorders is higher in female athletes than male athletes, there were no significant differences in frequencies of eating disorder symptoms between males and females in our study.[5,13] This finding suggests that eating disorders are common in sport center patrons in Saudi Arabia with comparable burden on both genders.
In the current study, 76.6% of participants had problematic eating behaviors and the reported prevalence was relatively higher in the 30 <40 year age group. There are many reasons for this: this age group is usually financially independent with a clear career path and so feel the need to focus on their appearance and beauty. Moreover, they probably have more free time to use social media, follow influencers, and engage in activities that focus on body image and beauty.
Studies have revealed that eating disorders have negative consequences on exercise performance through different mechanisms such as like self-induced vomiting or diet restriction, which sometimes lead to a negative caloric balance. Moreover, these actions are likely to cause dehydration through fluid reduction, leading to early fatigue and muscle spasms. In addition, hypokalemia and electrolyte imbalance could occur resulting in muscle cramps and fatigue.[17] In our study, exercise duration and frequency were significantly associated with eating disorders, and unfortunately, higher rates of symptoms were seen participants who exercised more frequently per week and spent more time spent in the gym. These are alarming findings and more attention to these participants is mandated.
To the best of our knowledge, this is the first Saudi study to examine the prevalence of eating disorder symptoms and its associated factors in sport center patrons of both genders of a wide age range. This is the strength of the study. However, there are some limitations. The cross-sectional design in this study limits the causality and temporality of the reported associations. EAT-26 tool used in the study is a screening, nondiagnostic tool and the positive cases need further assessment by mental health professionals. Therefore, the true prevalence of eating disorders in sport center patrons in Saudi Arabia needs further studies.
Conclusion
This study has demonstrated a significant level of eating disorder symptoms in sport center clients, especially those in their thirties. Moreover, frequencies of eating disorder symptoms increased with an increase in the BMI of the participants. Besides, more than half of participants who perceived that social media influencers motivated them to go to the gym and those who were pressured by social media to be slim had eating disorder symptoms.
The findings from this study might help family physicians, mental health professionals, and sport medicine specialists who wish to understand this issue in Arab populations. The alarming findings from this study could help decision-makers to establish strategies on the mental health of sport center patrons. A screening system for this population is recommended to identify those who need further evaluation and management. Moreover, a qualitative in-depth study to assess the effects of social media is suggested.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Aparicio-Martinez P, Perea-Moreno AJ, Martinez-Jimenez MP, Redel-Macías MD, Pagliari C, Vaquero-Abellan M. Social media, thin-ideal, body dissatisfaction and disordered eating attitudes: An exploratory analysis. Int J Environ Res Public Health. 2019;16:4177. doi: 10.3390/ijerph16214177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.American Psychiatric Association. Washington DC, USA: American Psychiatric Pub; 2013. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®) [Google Scholar]
- 3.Smink FR, van Hoeken D, Hoek HW. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr Psychiatry Rep. 2012;14:406–14. doi: 10.1007/s11920-012-0282-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pike KM, Hoek HW, Dunne PE. Cultural trends and eating disorders. Curr Opin Psychiatry. 2014;27:436–42. doi: 10.1097/YCO.0000000000000100. [DOI] [PubMed] [Google Scholar]
- 5.Bratland-Sanda S, Sundgot-Borgen J. Eating disorders in athletes: Overview of prevalence, risk factors and recommendations for prevention and treatment. Eur J Sport Sci. 2013;13:499–508. doi: 10.1080/17461391.2012.740504. [DOI] [PubMed] [Google Scholar]
- 6.Alwosaifer AM, Alawadh SA, Abdel Wahab MM, Boubshait LA, Almutairi BA. Eating disorders and associated risk factors among Imam Abdulrahman bin Faisal University preparatory year female students in Kingdom of Saudi Arabia. Saudi Med J. 2018;39:910–21. doi: 10.15537/smj.2018.9.23314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Fatima W, Ahmad LM. Prevalence of disordered eating attitudes among adolescent girls in Arar City, Kingdom of Saudi Arabia. Health Psychol Res. 2018;6:7444. doi: 10.4081/hpr.2018.7444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abd El-Azeem Taha AA, Abu-Zaid HA, El-Sayed Desouky D. Eating disorders among female students of Taif University, Saudi Arabia. Arch Iran Med. 2018;21:111–7. [PubMed] [Google Scholar]
- 9.The Government of Saudi Arabia. Vision Realization Program. [[Last accessed on 2020 Aug 21]]. Available from: https://vision2030.gov.sa/ar/programs/QoL . Vision 2030.
- 10.Harris N, Gee D, d’Acquisto D, Ogan D, Pritchett K. Eating disorder risk, exercise dependence, and body weight dissatisfaction among female nutrition and exercise science university majors. J Behav Addict. 2015;4:206–9. doi: 10.1556/2006.4.2015.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ebrahim M, Alkazemi D, Zafar TA, Kubow S. Disordered eating attitudes correlate with body dissatisfaction among Kuwaiti Male College students. J Eat Disord. 2019;7:37. doi: 10.1186/s40337-019-0265-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.IBM Corp. Armonk, NY: IBM Corp; 2016. IBM SPSS Statistics for Windows, Version 24.0. [Google Scholar]
- 13.Joy E, Kussman A, Nattiv A. 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. Br J Sports Med. 2016;50:154–62. doi: 10.1136/bjsports-2015-095735. [DOI] [PubMed] [Google Scholar]
- 14.Sundgot-Borgen J, Torstveit MK. Prevalence of eating disorders in elite athletes is higher than in the general population. Clin J Sport Med. 2004;14:25–32. doi: 10.1097/00042752-200401000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Kristjánsdóttir H, Siguráardóttir P, Jónsdóttir S, Þorsteinsdóttir G, Saavedra J. Body image concern and eating disorder symptoms among elite Icelandic athletes. Int J Environ Res Public Health. 2019;16:2728. doi: 10.3390/ijerph16152728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saleh RN, Salameh RA, Yhya HH, Sweileh WM. Disordered eating attitudes in female students of An-Najah National University: A cross-sectional study. J Eat Disord. 2018;6:16. doi: 10.1186/s40337-018-0204-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.El Ghoch M, Soave F, Calugi S, Dalle Grave R. Eating disorders, physical fitness and sport performance: A systematic review. Nutrients. 2013;5:5140–60. doi: 10.3390/nu5125140. [DOI] [PMC free article] [PubMed] [Google Scholar]