

Abstract
Acne is associated with depression and anxiety; however, the relationship between acne and suicide is still unclear. This study is aimed to evaluate the association between acne and suicide by conducting a meta-analysis. Studies were identified by electronic searches of the PubMed and EMBASE databases from their inception through Jan 10, 2020. Two authors separately assessed the quality and extracted data from the selected studies. When the heterogeneity was significant, we used a random-effects model to calculate overall pooled risk estimates.
Five studies involving a total of 2,276,798 participants were finally included in the meta-analysis; 52,075 participants had acne. Suicide was positively associated with acne in the overall analysis (odds ratio (OR) 1.50, 95% confidence interval (95% CI): 1.09–2.06, P = .004, I2 = 74.1%). Subgroup analyses were performed for suicidal behavior groups (P = .002, I2 = 80.4%), suicidal ideation or thoughts groups (P = .849, I2 = 0.0%), International Classification of Diseases version 9 (ICD-9) groups (P = .137, I2 = 49.6%), non-ICD-9 groups (P = .950, I2 = 0.0%), American groups (P = .311, I2 = 2.4%), and non-American groups (P = .943, I2 = 0.0%). Sensitivity analyses indicated flawed results. No publication bias was detected.
Acne may significantly increase suicide risk. Clinicians should actively treat acne and consider suicide screening. Further international studies with high-quality analyses are needed as more data are published.
Ethical approval and patient consent are not required because this study is a literature-based study.
Keywords: acne, suicide, meta-analysis
1. Introduction
Acne, one of the most common skin diseases, is a multifactorial disease of the pilosebaceous glands. The pathogenesis of acne involves four main processes: oversecretion of androgens, excess sebum production, inflammation, and proliferation of Propionibacterium acnes. Clinically, open and closed comedones, inflammatory papules, pustules, cysts, nodules, and even scarring may be seen in patients with various forms of acne. Although all age groups may be affected by its many variants, acne most often occurs in adolescence. Women have higher rates of acne than men in all age groups 20 years or older.[1] Both active acne and scars from previous acne have an undeniable psychosocial impact, and affected individuals have an increased likelihood of self-consciousness, social isolation, depression and even suicidal ideation.[2] Isotretinoin is considered to be a remarkably efficacious treatment for severe acne.[3] However, its use is still controversial. Since its approval by the US Food and Drug Administration (FDA) in the 1980s, isotretinoin has been related to psychiatric disorders such as depression, anxiety and suicidality (including suicidal ideation, suicide attempts, and suicide), leading to widespread media coverage. A review of the psychiatric literature indicated strong evidence of an association between isotretinoin and psychiatric side effects.[4] However, some studies have shown that there is no evidence to support a connection between isotretinoin and depression, suicide, or other psychiatric disorders.[5,6] Therefore, to avoid the results being affected by the side effects of isotretinoin, we did not include articles with a clear history of isotretinoin use.
Suicide is a major public health problem worldwide. Suicidal behaviors can be classified as suicidal ideation (thoughts, fantasies and wanting to end one's own life),[7] suicidal plan creation (formulation of a specific means to end one's own life),[8] suicide attempt (self- destructive act where the individual has at least some intention to end their own life),[9] and completed suicide.[10,11] The World Health Organization (WHO) reports that approximately one million people die from suicide each year worldwide and that the suicide rate is increasing in the young age group (WHO); suicide is the second leading cause of death in 15- to 29-year-olds.[12]
Suicide is not rare among patients with dermatologic conditions. In the 1990s, a study reported that 7 of 16 cases of completed suicide among dermatology patients were due to acne.[13] The average age of the 7 acne patients who completed suicide was 20.4 years. Dermatologists need to be aware of the mental health of adolescent acne patients. A growing number of studies have specifically investigated suicide in skin disease (such as acne, alopecia areata, psoriasis, atopic dermatitis, etc.) patients. [14–17] Concerns have been raised about the potential for suicide among patients with acne, but no specific meta-analysis of the association between suicide risk and acne has been conducted to date. The aim of this meta-analysis was to examine the relationship between acne and suicide.
2. Methods
2.1. Search strategy
A literature search for articles published from database inception to 10 February 2020 was conducted in the PubMed, EMBASE, and Web of Science databases. The search terms used were:
-
1.
“Acne Vulgaris”, “Acne”, “ Acne Conglobata”;
-
2.
“Suicide”, “Suicidal thoughts”, “Suicidal ideation”, “Suicide attempts”, “Assisted Suicide”, and “Suicidal behavior”
2.2. Selection criteria
We read reference abstracts to determine eligibility on the basis of the inclusion criteria, which were as follows:
-
1.
noninterventional studies (e.g., case-control, cross-sectional, and cohort studies);
-
2.
studies with no clear history of administration of or treatment with isotretinoin;
-
3.
studies including patients with no definite history of mental illness;
-
4.
studies that evaluated the association between acne and suicide incidence; and
-
5.
studies with sufficient data to calculate the numbers of patients affected, odds ratios (ORs) or risk ratios (RRs) and the corresponding 95% confidence intervals (CIs).
No language restriction was imposed. Studies were excluded if they included nonhuman study subjects. Reviews, conference abstracts, letters to editors, case reports and commentary articles were excluded. We evaluated the included literature and searched for citations to identify any additional studies that might have been missed in the initial search.
2.3. Data extraction
All articles identified by the search were imported to EndNote X8. After excluding duplicate studies, two researchers independently evaluated the eligible studies based on the aforementioned selection criteria. The following information was extracted from each included article by two other trained investigators: author, year, country, data sources, sample size, gender, number of patients with acne, age, type of study, outcome measures, ORs and 95% CIs, and adjustment variables. If we encountered multiple studies with the same population, we chose the most recent or complete study. The Newcastle–Ottawa Scale (NOS)[18,19] was used for methodological quality assessment in this meta-analysis. The NOS has three parameters: selection, comparability, and exposure (case-control studies) or outcome (cohort studies). A NOS score of seven or more was deemed high quality. Any disagreements were resolved by discussion with other reviewers.
2.4. Statistical analyses
We computed a pooled OR and 95% CI from the RRs or ORs and 95% CIs reported in the studies. RRs were generally replaced by ORs when incidence was very low. Q-tests and I2 tests were used to assess statistical heterogeneity. We used I2 tests to assess between-study heterogeneity, and the thresholds of ≥25%, ≥50% and ≥75% represented low, moderate and high heterogeneity, respectively.[20] When the heterogeneity of the included studies was significant (the P value was <.1 and the I2 value was >50%), we employed the DerSimonian and Laird (D-L) random-effects model as the pooling method;[21] otherwise, the M-H fixed effect model[22] was used to estimate the overall summary. Subgroup analyses based on study variables (suicidal behaviors, suicidal ideation or thoughts, and gender) were performed to further explore the source of heterogeneity. We used Begg's rank correlation tests and Egger's linear regression tests to assess potential publication bias.[23] A sensitivity analysis was performed by excluding one study per cycle to evaluate the stability of the results.[24] All analyses were performed using STATA statistical software version 14.0.
3. Results
3.1. Literature search and study characteristics
A total of 272 articles (91 from PubMed, 73 from EMBASE, 106 from Web of Science, and 2 from other sources) were initially identified. After removing the duplicate articles, 105 records were included for further assessment. Of these records, 93 records were excluded after screening the titles and abstracts and reviewing the full texts. Finally, 5 studies[2,5,25–27] involving 2,276,798 participants, of whom 52,075 had acne, were included in our analysis (Fig. 1).
Figure 1.
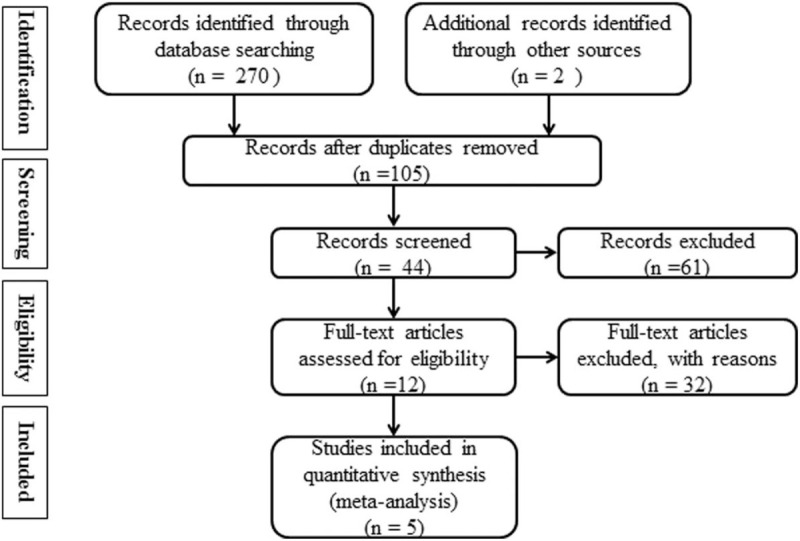
Flow chart of the meta-analysis.
The characteristics of the included studies are shown in Table 1. The data from the different cities/countries (Boston, London, Norway, Taiwan, and Detroit) were obtained from the following datasets: Canadian Saskatchewan Health Database; Youth 2000 Survey (New Zealand National Survey of Youth Health); Oslo section of the Youth 2004 Study; the National Health Insurance (NHI) Database; and 8 other health systems. A total of 4 studies investigated suicidal behaviors including combined attempted and completed suicides, and 2 studies investigated suicidal ideation/thoughts.
Table 1.
Characteristics of the 5 studies.
| Gender | ||||||||||
| Author, year | Country, data sources | Sample size | Male | Female | No. of patients | Age: mean of range or range | Type of study | Outcome measures | OR and 95% CI | Adjustments |
| Susan S. Jick, 2000 | Boston; The Canadian Saskatchewan Health Database | Approximately 1,000,000 | NR | NR | 13,700 | 10–29 y | Cohort | Suicide and suicide attempts: ICD-9 | 0.5 (0.1-1.6) | NR |
| Diana Purvis, 2006 | London; Youth 2000 (New Zealand National Survey of Youth Health) | 9398 | NR | NR | 1329 | 12–18 y | Cross-sectional | Suicidal thoughts and suicide attempts: self-reported suicide attempts | 1.82 (1.64-2.01)) | NR |
| Jon A. Halvorsen, 2011 | Norway; the Oslo section of the Youth 2004 Study | 3620 | 1,596 | 2,024 | 489 | 18–19 y | Cross-sectional | Suicidal ideation: HSCL-90 | 1.80 (1.30-2.50)) | Ethnicity, family income, and gender |
| Yi-Chien Yang, 2014 | Taiwan; the NHI Database | 1,000,000 | 495,838 | 506,362 | 30,543 | 7–12 y (14.39%) | Cross-sectional | Suicide: ICD-9-CM: E950-E959 | 2.08 (0.96-4.53)) | Age categories |
| Deepak Prabhakar, 2018 | Detroit; 8 health systems∗ (2000-2013) | 267,400 | NR | NR | 6014 | NR | Case-control | Suicide death: ICD-9:706,706.1 | 1.04 (0.77-1.40) | Age, sex and mental health of substance use conditions |
3.2. Main analysis
Suicide was positively associated with acne in the overall analysis (OR 1.50, 95% CI: 1.09–2.06) (Fig. 2). However, evidence of significant heterogeneity was observed across studies (I2 = 74.1%; P = .004).
Figure 2.
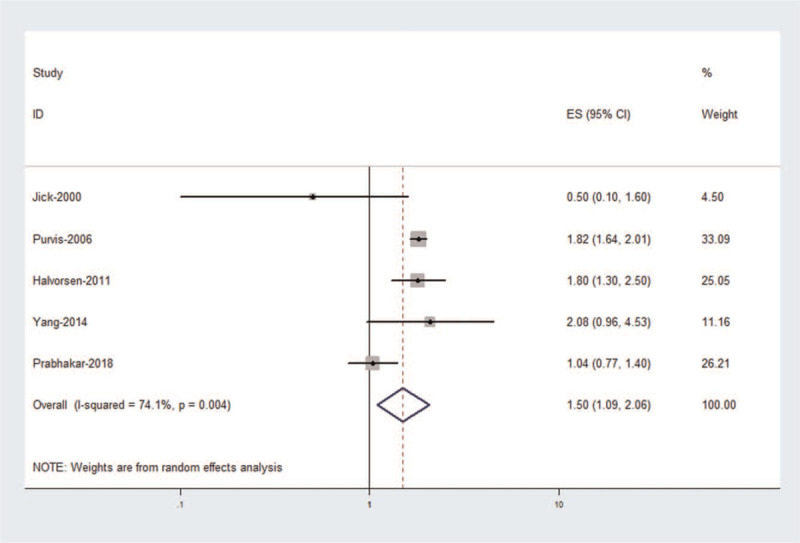
Forest plot of suicide associated with acne.
3.3. Subgroup meta-analysis
The results of the subgroup analyses are shown in Table 2. According to suicide type, we observed a positive association between acne and suicidal behaviors in the studies (P = .002, I2 = 80.4%). No statistical heterogeneity was observed in the suicidal ideation/thoughts group (P = .849, I2 = 0.0%). Subgroup analyses were performed according to region and outcome measure (American groups (P = .311, I2 = 2.4%), non-American groups (P = .943, I2 = 0.0%), ICD-9 groups (P = .137, I2 = 49.6%), and non-ICD-9 groups (P = .950, I2 = 0.0%)).
Table 2.
Subgroup analyses of the association between acne and suicide risk.
| Factor | No. of studies | OR (95% CI) | Heterogeneity P (I2%) |
| Region | |||
| America | 2 | 1.00 (0.72, 1.39) | .311 (2.4%) |
| Non Americans | 3 | 1.82 (1.65, 2.01) | .943 (0.0%) |
| Suicide types | |||
| Suicidal behaviors | 4 | 1.38 (0.88, 2.18) | .002 (80.4%) |
| Suicidal ideation/thoughts | 2 | 1.75 (1.56, 1.96) | .849 (0.0%) |
| Outcome measures | |||
| ICD-9 | 3 | 1.16 (0.65, 2.08) | .137 (49.6%) |
| Others | 2 | 1.82 (1.65, 2.00) | .950 (0.0%) |
3.4. Sensitivity analysis
For the meta-analysis, individual studies were deleted one at a time to conduct a sensitivity analysis by recalculating the pooled results from the primary analyses. Our results showed that the pooled OR was slightly changed (Fig. 3), and sensitivity was not perfect.
Figure 3.
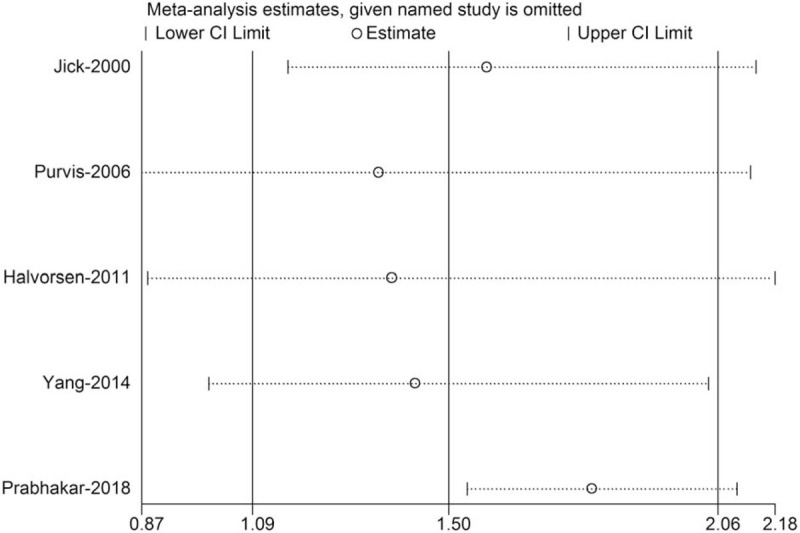
Sensitivity analysis of suicide associated with acne.
3.5. Publication bias
Begg's rank correlation test (P > |z| = .806) and Egger's linear regression test (P > |z| = .016) indicated no evidence of publication bias among the studies (Figs. 4 and 5).
Figure 4.
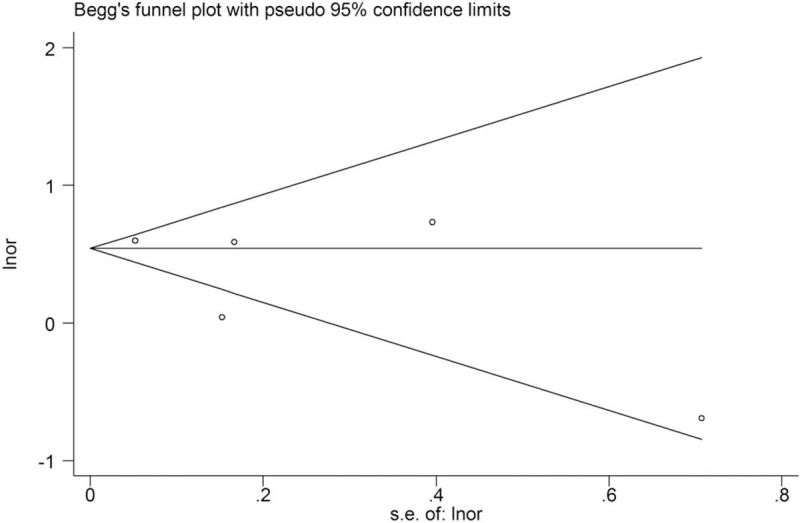
Begg's funnel plot.
Figure 5.
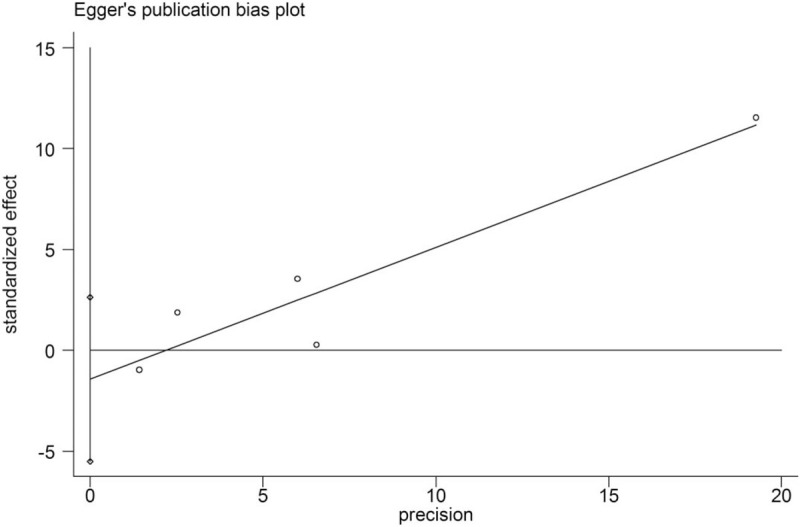
Egger's publication bias plot.
4. Discussion
Suicide is a multifactorial behavior associated with cultural differences, socioeconomic status, unemployment, alcoholism and mental illness.[28] Acne can affect facial appearance and lead to mental problems, such as depression, anxiety and suicide.[29] To our knowledge, this study is the first meta-analysis to examine associations between acne and suicide.
Our study results showed that acne was positively associated with suicide. Some previous literature has also indicated that acne is associated with major depression and suicide.[25,26] In addition, the study by Halvorsen and colleagues revealed that acne is associated with social and psychological problems.[2] Adverse events, including suicidal ideation and depression, which have been associated with therapies for acne, may reflect the burden of substantial acne rather than the effects of medication. Nevertheless, the case-control study provides no evidence of an increased risk of death by suicide in individuals with acne in the US general population.[27] In addition, heterogeneity was observed among the included studies. By performing subgroup analyses based on study variables, we found that studies conducted in certain regions and outcome measures contribute to heterogeneity. Moreover, no publication bias was observed in our study. In America, the suicide rate is 10.8 per 100,000 persons, and suicide is the 11th leading cause of death, accounting for 1.4% of all US deaths. In total, 9%–15% of US dermatology patients with psoriasis, atopic dermatitis, and acne are at risk of suicide.[17] In the future, more research is needed to provide evidence.
Our study had some limitations. First, the studies were limited to those published in English; and whether the risk of suicide differs in patients with acne elsewhere and in non-English studies is unclear. Another limitation was that studies with nonsignificant results, especially those that show an absence of effects, may not be published because they are rejected by journals or because the investigators are unwilling to submit them for publication. Third, none of the included studies examined the effects of anti-acne drugs on suicide. For example, Isotretinoin has been described in acne cases treatment with depression and suicide-related psychiatric adverse drug reactions, however, its evidence is still limited, therefore the reader is suggested to use this information carefully and apply it according to each case. [30] Last, the number of included studies for some comparisons was small, which might have affected our results. The addition of more studies in the future may increase the quality of evidence.
This study should remind clinicians that attention should be paid to acne patients’ mental health and the outcome of suicide by acne patients should be prevented as much as possible.
5. Conclusions
In summary, this meta-analysis demonstrates that acne may significantly increase suicide risk. Clinicians should actively treat acne and consider suicide screening. Further international studies with high-quality analyses are needed as more data are published.
Author contributions
Data curation: Shuangyan Xu, Yun Zhu, Hu Hu, Xiuhong Liu, Li Li, Binbin Yang, Wei Wu.
Funding acquisition: Shuangyan Xu, Zuohui Liang.
Supervision: Shuangyan Xu, Yun Zhu.
Writing – original draft: Shuangyan Xu, Yun Zhu.
Methodology: Hu Hu, Xiuhong Liu, Li Li, Binbin Yang, Wei Wu.
Software: Hu Hu, Xiuhong Liu, Li Li, Binbin Yang, Wei Wu.
Conceptualization: Zuohui Liang, Danqi Deng.
Writing – review & editing: Zuohui Liang, Danqi Deng.
Footnotes
Abbreviations: CI = confidence interval, HSCL-90 = the 90-question version of the Hopkins Symptom Checklist, ICD = International Classification of Diseases, NR = not reported, OR = odds ratio.
How to cite this article: Xu S, Zhu Y, Hu H, Liu X, Li L, Yang B, Wu W, Liang Z, Deng D. The analysis of acne increasing suicide risk. Medicine. 2021;100:24(e26035).
SX and YZ contributed equally to this study.
This work is supported by grants from the Scientific Research Foundation of Education Department of Yunnan Province (No. 2021J0304), Joint special fund of Applied Fundamental Research of Kunming Medical University granted by Science and Technology Office of Yunnan (No. 2018FE001(-175)), and Yunnan health training project of high level talents.
The authors have no conflicts of interest to disclose.
All data generated or analyzed during this study are included in this published article.
∗8 health systems include HealthPartners (Minnesota), Harvard Pilgrim Health Care (Massachusetts), Henry Ford Health System (Michigan), and the Kaiser Permanente health systems in Colorado, Georgia, Hawaii, Washington and the Northwest. y, years; NR, not reported; ICD, International Classification of Diseases; HSCL-90, the 90-question version of the Hopkins Symptom Checklist; OR, odds ratio; and 95% CI, 95% confidence interval.
References
- [1].Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol 2008;58:56–9. [DOI] [PubMed] [Google Scholar]
- [2].Halvorsen JA, Stern RS, Dalgard F, Thoresen M, Bjertness E, Lien L. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol 2011;131:363–70. [DOI] [PubMed] [Google Scholar]
- [3].Peck GL, Olsen TG, Butkus D, et al. Isotretinoin versus placebo in the treatment of cystic acne. A randomized double-blind study. J Am Acad Dermatol 1982;6:735–45. [DOI] [PubMed] [Google Scholar]
- [4].Bremner JD, Shearer KD, McCaffery PJ. Retinoic acid and affective disorders: the evidence for an association. J Clin Psychiatry 2012;73:37–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Jick SS, Kremers HM, Vasilakis-Scaramozza C. Isotretinoin use and risk of depression, psychotic symptoms, suicide, and attempted suicide. Arch Dermatol 2000;136:1231–6. [DOI] [PubMed] [Google Scholar]
- [6].Jacobs DG, Deutsch NL, Brewer M. Suicide, depression, and isotretinoin: is there a causal link? J Am Acad Dermatol 2001;45:S168–75. [DOI] [PubMed] [Google Scholar]
- [7].Zhu Y, Zhang H, Shi S, et al. Suicidal risk factors of recurrent major depression in Han Chinese women. PLoS one 2013;8:e80030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Lee S, Fung SC, Tsang A, et al. Lifetime prevalence of suicide ideation, plan, and attempt in metropolitan China. Acta Psychiatr Scand 2007;116:429–37. [DOI] [PubMed] [Google Scholar]
- [9].Kao YC, Liu YP, Cheng TH, Chou M-K. Subjective quality of life and suicidal behavior among Taiwanese schizophrenia patients. Soc Psychiatry Psychiatr Epidemiol 2012;47:523–32. [DOI] [PubMed] [Google Scholar]
- [10].Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 2008;192:98–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Dong M, Wang SB, Li Y, et al. Prevalence of suicidal behaviors in patients with major depressive disorder in China: A comprehensive meta-analysis. J Affect Disord 2018;225:32–9. [DOI] [PubMed] [Google Scholar]
- [12].World Health Organization;, Organization WH. Preventing suicide: a global imperative. 2014. [Google Scholar]
- [13].Cotterill JA, Cunliffe WJ. Suicide in dermatological patients. Br J Dermatol 1997;137:246–50. [DOI] [PubMed] [Google Scholar]
- [14].Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Br J Dermatol 1998;139:846–50. [DOI] [PubMed] [Google Scholar]
- [15].Picardi A, Mazzotti E, Pasquini P. Prevalence and correlates of suicidal ideation among patients with skin disease. J Am Acad Dermatol 2006;54:420–6. [DOI] [PubMed] [Google Scholar]
- [16].Picardi A, Lega I, Tarolla E. Suicide risk in skin disorders. Clin Dermatol 2013;31:47–56. [DOI] [PubMed] [Google Scholar]
- [17].Gupta MA, Pur DR, Vujcic B, Gupta AK. Suicidal behaviors in the dermatology patient. Clin Dermatol 2017;35:302–11. [DOI] [PubMed] [Google Scholar]
- [18].Wells G, Shea B, O’connell D, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2014. [Google Scholar]
- [19].Wells G. The Newcastle–Ottawa Scale (NOS) for assessing the quality of non randomised studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp [access date 2001, English version]. [Google Scholar]
- [20].Higgins JP, Thompson SG, Deeks JJ, Altmann DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [22].Leonard T, Duffy JC. A Bayesian fixed effects analysis of the Mantel–Haenszel model applied to meta-analysis. Stat Med 2002;21:2295–312. [DOI] [PubMed] [Google Scholar]
- [23].Harbord RM, Egger M, Sterne JA. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med 2006;25:3443–57. [DOI] [PubMed] [Google Scholar]
- [24].Chootrakool H, Shi JQ, Yue R. Meta-analysis and sensitivity analysis for multi-arm trials with selection bias. Stat Med 2011;30:1183–98. [DOI] [PubMed] [Google Scholar]
- [25].Purvis D, Robinson E, Merry S, et al. Acne, anxiety, depression and suicide in teenagers: a cross-sectional survey of New Zealand secondary school students. J Paediatr Child Health 2006;42:793–6. [DOI] [PubMed] [Google Scholar]
- [26].Yang YC, Tu HP, Hong CH, et al. Female gender and acne disease are jointly and independently associated with the risk of major depression and suicide: a national population-based study. BioMed Res Int 2014;2014:504279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Prabhakar D, Peterson EL, Hu Y, et al. Dermatologic conditions and risk of suicide: a case-control study. Psychosomatics 2018;59:58–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Al-Sharifi A, Krynicki CR, Upthegrove R. Self-harm and ethnicity: a systematic review. Int J Soc Psychiatry 2015;61:600–12. [DOI] [PubMed] [Google Scholar]
- [29].Saitta P, Keehan P, Yousif J, Way BV, Grekin S, Brancaccio R. An update on the presence of psychiatric comorbidities in acne patients. Part 2: depression, anxiety, and suicide. Cutis 2011;88:92–7. [PubMed] [Google Scholar]
- [30].Thomas KH, Martin RM, Potokar J, Pirmohamed M, Gunnell D. Reporting of drug induced depression and fatal and non-fatal suicidal behaviour in the UK from 1998 to 2011. BMC Pharmacol Toxicol 2014;15:54. [DOI] [PMC free article] [PubMed] [Google Scholar]