

Key Points
Question
How is disease burden associated with female representation in US-based clinical trials, and how are disease category and other clinical trial features associated with female representation in clinical trials?
Findings
In this cross-sectional study of 20 020 clinical trials enrolling more than 5 million participants between 2000 and 2020, clinical trials in the fields of oncology, neurology, immunology, and nephrology had the lowest female participant representation relative to corresponding disability-adjusted life-years. Clinical trials in cardiology and pediatrics had the greatest negative associations with female enrollment, and clinical trials of preventive interventions had a positive association.
Meaning
This study’s findings suggest that sex bias persists within clinical trials, with male and female participants underrepresented in different areas of research.
Abstract
Importance
Although female representation has increased in clinical trials, little is known about how clinical trial representation compares with burden of disease or is associated with clinical trial features, including disease category.
Objective
To describe the rate of sex reporting (ie, the presence of clinical trial data according to sex), compare the female burden of disease with the female proportion of clinical trial enrollees, and investigate the associations of disease category and clinical trial features with the female proportion of clinical trial enrollees.
Design, Setting, and Participants
This cross-sectional study included descriptive analyses and logistic and generalized linear regression analyses with a logit link. Data were downloaded from the Aggregate Analysis of ClinicalTrials.gov database for all studies registered between March 1, 2000, and March 9, 2020. Enrollment was compared with data from the 2016 Global Burden of Disease database. Of 328 452 clinical trials, 70 095 were excluded because they had noninterventional designs, 167 936 because they had recruitment sites outside the US, 69 084 because they had no reported results, 1003 because they received primary funding from the US military, and 314 because they had unclear sex categories. A total of 20 020 interventional studies enrolling approximately 5.11 million participants met inclusion criteria and were divided into those with and without data on participant sex.
Exposures
The primary exposure variable was clinical trial disease category. Secondary exposure variables included funding, study design, and study phase.
Main Outcomes and Measures
Sex reporting and female proportion of participants in clinical trials.
Results
Among 20 020 clinical trials from 2000 to 2020, 19 866 studies (99.2%) reported sex, and 154 studies (0.8%) did not. Clinical trials in the fields of oncology (46% of disability-adjusted life-years [DALYs]; 43% of participants), neurology (56% of DALYs; 53% of participants), immunology (49% of DALYs; 46% of participants), and nephrology (45% of DALYs; 42% of participants) had the lowest female representation relative to corresponding DALYs. Male participants were underrepresented in 8 disease categories, with the greatest disparity in clinical trials of musculoskeletal disease and trauma (11.3% difference between representation and proportion of DALYs). Clinical trials of preventive interventions were associated with greater female enrollment (adjusted relative difference, 8.48%; 95% CI, 3.77%-13.00%). Clinical trials in cardiology (adjusted relative difference, −18.68%; 95% CI, −22.87% to −14.47%) and pediatrics (adjusted relative difference, −20.47%; 95% CI, −25.77% to −15.16%) had the greatest negative association with female enrollment.
Conclusions and Relevance
In this study, sex differences in clinical trials varied by clinical trial disease category, with male and female participants underrepresented in different medical fields. Although sex equity has progressed, these findings suggest that sex bias in clinical trials persists within medical fields, with negative consequences for the health of all individuals.
This cross-sectional study uses data from clinical trials registered in ClinicalTrials.gov between 2000 and 2020 to assess the presence of clinical trial data according to sex, female burden of disease relative to female proportion of enrollees, and associations of disease category and study features with female proportion of enrollees.
Introduction
Medical research has historically focused on male health.1,2,3,4,5 Female individuals were often excluded from clinical trials, supposedly to ensure homogeneity of treatment effect and reduce potential maternal-fetal liability.6 Sex bias persisted, even after research reported sex differences in diagnostic test results, disease progression, treatment response, drug metabolism, and surgical outcomes.7 Studies have associated this lack of female inclusion with suboptimal health care and adverse medical outcomes.4,8 In response to the recognition of sex bias in clinical trials and corresponding health disparities, national and international organizations have mobilized legislative efforts to increase female inclusion.9 Research documented the ensuing increase in female representation in clinical trials and dismantled inaccurate notions that female participants complicated results by introducing confounding social and biological variables.9 By 2013, female enrollees comprised more than one-half of all participants in National Institutes of Health research.9
Most studies on sex bias in research have focused on equality and sex matching, pairing female representation with male representation.5,10 Sex matching and power for sex-specific analysis permit study stratification and the detection of effect differences between male and female participants. However, these parameters may not adequately capture heterogeneity or adverse events in subpopulations because they rarely account for the varied distributions and manifestations of disease within sexes.11 Greater emphasis on parity and representation, not simply statistical power, has emerged with the increasing interest in pragmatic clinical trials and clinical trials that evaluate effectiveness rather than efficacy.11,12 Despite the inherent association between representation and burden of disease, little is known about how the sex of clinical trial participants compares with disease prevalence.13
We aimed to address this gap by characterizing sex reporting (ie, the presence of clinical trial data on the number of male and female participants) in US-based clinical trials that were registered in the ClinicalTrials.gov database between 2000 and 2020 and by comparing sex representation in clinical trials with the burden of disease by sex. We also investigated the associations of clinical trial funding, clinical trial phase, and other clinical trial features with female representation across medical disciplines.
Methods
Data Sources
We downloaded all clinical trials registered between March 1, 2000, and March 9, 2020, to ClinicalTrials.gov using the Aggregate Analysis of ClinicalTrials.gov (AACT) database.14 Observational studies were excluded. Although the ClinicalTrials.gov registry captures most US-based clinical trials, many international clinical trials are registered in other international or country-specific databases. Thus, we limited our study to US-based clinical trials to ensure accurate comparisons between the clinical trial sample and the represented population. The analysis included all studies that (1) were registered in ClinicalTrials.gov; (2) were conducted between March 1, 2000, and March 9, 2020; (3) reported sex results; and (4) were interventional in design. We referenced 2016 Global Burden of Disease (GBD) data to assess the US burden of disease for each sex.15 This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.16 The study was reviewed and approved by the institutional review board of Stanford University and granted exemption from informed consent because the study did not involve human participants and included only publicly available data sets.
Exposure Variables
Primary exposure variables included clinical trial disease category and clinical trial funding. Secondary analyses investigated clinical trial phase and other clinical trial features.
We defined burden of disease as disability-adjusted life-years (DALYs; ie, years of healthy life lost) based on GBD data.15 We selected DALYs rather than prevalence because DALYs capture the varied sequelae and burden of disease by sex. We combined medical subject heading (MeSH) terms and GBD information by manually assigning diseases in the GBD database (eMethods 1 in the Supplement) to 1 or more of the 17 most prevalent MeSH disease categories in the US population: (1) musculoskeletal and trauma, (2) psychiatry, (3) cardiology, (4) neurology (including ocular disease), (5) oncology, (6) pulmonology, (7) pediatrics, (8) endocrinology, (9) gastroenterology, (10) nutritional and metabolic, (11) infectious disease, (12) immunology, (13) otorhinolaryngology (including stomatognathic disease), (14) dermatology, (15) nephrology and genitourinary (subdivided into male-specific, female-specific, and sex-nonspecific), (16) hematology (hemic and lymphatic disease), and (17) congenital. Categories were not exclusive because given diseases may have implications for multiple organ systems, and they were modeled as binary variables in the analysis.17
We classified funding in accordance with previous studies on the AACT database,17,18 using both the lead sponsor and collaborating agencies. Industry-funded clinical trials included all studies with an industry source as a sponsor or collaborator. Remaining clinical trials with a US government funder were labeled US government. Given that the US military is predominantly male, we excluded clinical trials with military funding. Remaining clinical trials (listed as other in the AACT database) were labeled academic, as 90% of the funders in the other category have been reported in previous studies to be academic institutions.18,19
Clinical trial features included (1) primary purpose, (2) intervention, (3) phase, (4) number of arms, (5) estimated enrollment, (6) registration year, (7) blinding, (8) randomization, (9) placebo control, (10) control with active comparator, (9) data safety monitoring committee oversight, (11) number of sites, and (12) study status.
Outcomes
The primary outcomes were sex reporting and the proportion of female participants in clinical trials. Sex was defined according to the biological definitions of male and female. Although there are inherent associations between sex and gender (a cultural and psychosocial term that captures the complex manifestations associated with sex in a societal context20), we exclusively focused on sex as reported in the AACT and GBD databases. In the AACT database, sex and gender can be entered as sex, male, female and/or gender, customized. More than 45 terms characterize gender in the database. Using both manual and programmatic searches, we identified and extracted clinical trials that reported sex or customized gender enrollment data. Two authors (B.E.T. and B.O.W.) manually reviewed all gender-customized labels and sorted them into 2 categories, male or female, in accordance with the enrollees’ biological sex. Clinical trials with unintelligible sex reporting that could not be characterized as male or female (ie, incorrectly completed fields) were excluded. Although the ClinicalTrials.gov registry only developed a reporting repository for enrollee demographic data in 2007,21 we included clinical trials registered before 2007 if they had reported results in the AACT database.
Statistical Analysis
We aimed to (1) describe the rate of sex reporting, (2) compare the female burden of disease with the proportion of female clinical trial enrollees, (3) characterize the proportion of female enrollees by clinical trial features, (4) investigate the associations between primary exposure variables (disease category and funding) and the proportion of female enrollees, and (5) examine the associations of other clinical trial features with the proportion of female enrollees. Descriptive statistics were reported using medians and interquartile ranges (IQRs).
We examined the associations with the proportion of female enrollees using multivariable fractional regression analysis with a logit link.22 Regression analyses only included clinical trials with associated MeSH terms; therefore, 2495 clinical trials (12.5%) without MeSH terms were excluded from those analyses. To examine the association of disease category with the proportion of female enrollees, we used 2 regression models; model 1 included disease category, and model 2 included clinical trial features (without disease category). All analyses were 2-sided with a significance threshold of α = .05. Data were analyzed using R software, version 3.5.0 (R Foundation for Statistical Computing).
Missing Data in Multivariable Regression Analysis
Each clinical trial feature had 0% to 7.9% missing data, which we addressed using multiple imputation by chained equations with 30 imputed data, with the assumption that missingness was random.23 Our analysis included pooled bayesian logistic regression models for binary data and pooled bayesian multinomial logistic regression models for categorical data (our sample did not have missing continuous data).
Results
Clinical Trial Population and Sex Reporting
Of the 328 452 clinical trials registered between March 1, 2000, and March 9, 2020, in the ClinicalTrials.gov database, 21 337 clinical trials enrolling more than 5.11 million participants reported results. After excluding those with military funding or unclear sex categories, 20 020 clinical trials met inclusion criteria (Figure 1). Of those, 19 866 clinical trials (99.2%) reported sex.
Figure 1. Flow Diagram of Clinical Trials Included in the Analysis.

Sex Representation and Burden of Disease
Female representation across all clinical trials was approximately 50% between 2000 and 2020, with the lowest female representation occurring in 2002 (median, 41.1%; IQR, 29.2%-56.2%) and the highest occurring in 2018 (median, 60.0%; IQR, 40.6%-77.8%) (Figure 2).
Figure 2. Median Enrollment of Female Participants in US Clinical Trials by Year.

Global proportion of female enrollment over time. Black lines represent the median proportion of female enrollees. Gray bars show interquartile ranges (IQRs). The IQR for 2020 could not be calculated because of the small number of clinical trials submitted to the ClinicalTrials.gov registry before March 2020.
Sex representation varied by disease category (Figure 3). Female participants comprised the smallest proportions of enrollees in cardiology (41.4%), sex-nonspecific nephrology and genitourinary (41.7%), and hematology (41.7%) clinical trials. Clinical trials in oncology had the greatest female underrepresentation relative to the female proportion of corresponding DALYs (42.9% vs 46.5%, respectively), followed by clinical trials in neurology (52.7% vs 56.1%), immunology (45.9% vs 48.8%), and sex-nonspecific nephrology and genitourinary disease (41.7% vs 45.2%).
Figure 3. Burden of Disease, Female Proportion of Disability-Adjusted Life-Years (DALYs), and Female Proportion of Clinical Trial Enrollees by Disease Focus.
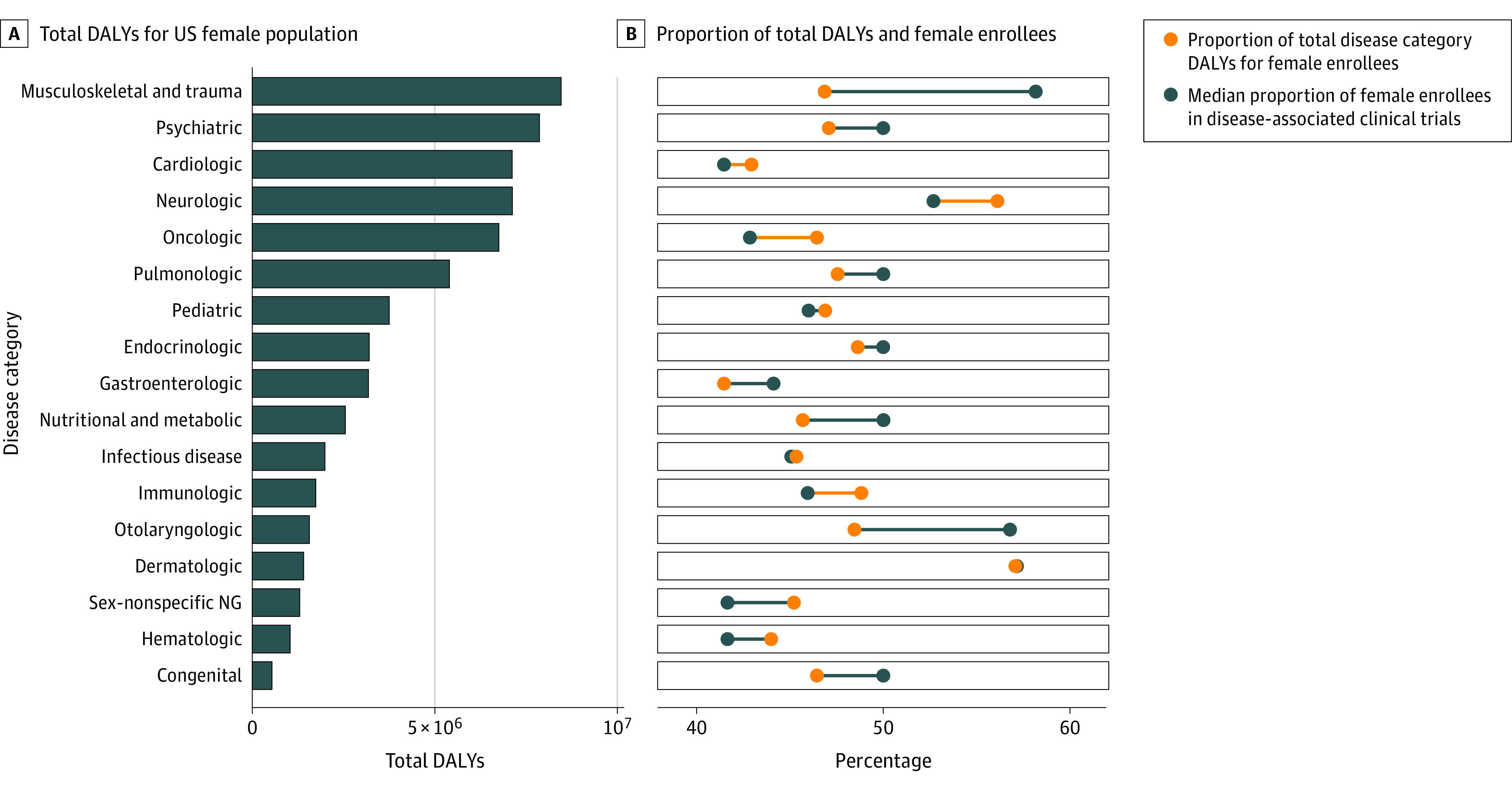
Lines connecting yellow and blue dots show the difference between the proportion of female participants and female DALYs. Blue lines indicate that the proportion of female participants is greater than the proportion of female DALYs. Yellow lines indicate that the proportion of female participants is less than the proportion of female DALYs. NG indicates nephrological and genitourinary.
The greatest disparities existed in disease categories in which male participants were underrepresented compared with their burden of disease (Figure 3; eTable 1 in the Supplement). Male participants were underrepresented in 8 disease categories, with the greatest disparity in clinical trials of musculoskeletal disease and trauma (11.3% difference between representation and proportion of DALYs). Only 46.9% of musculoskeletal disease and trauma DALYs were attributable to the female population, but 58.2% (IQR 40.0%-77.7%) of clinical trial participants were female. In otorhinolaryngology clinical trials, female enrollees comprised 56.8% (IQR, 42.2%-66.7%) of participants despite representing only 48.5% of DALYs. Although female enrollees represented 50% of clinical trial participants overall, they were overrepresented relative to their burden of disease in congenital (difference, −3.6%), nutritional and metabolic (difference, −4.3%), gastroenterology (difference, −2.7%), and psychiatry (difference, −2.9%) clinical trials. Dermatology and infectious disease clinical trials had relative parity (difference, −0.1% and 0.3%, respectively). Other disease foci indicated minor discrepancies (≤2% difference between proportion of DALYs and of female representation in clinical trials).
Sex Representation and Clinical Trial Features
Several clinical trial features differed in female representation (Table 1). Although industry- and academic-funded clinical trials enrolled approximately equal proportions of male and female participants, US government–funded clinical trials had a median female enrollment of 46.7% (IQR, 30.8%-65.0%). Behavioral clinical trials enrolled a greater proportion of female participants (median, 56.7%; IQR, 40.7%-76.0%) than medical device clinical trials (median, 51.6%; IQR, 36.4%-70.6%). Female enrollees represented fewer than one-half of participants in clinical trials of biologic drugs and supplements (48.0%; IQR, 32.3%-65.6%), procedures (46.1%; IQR, 31.7%-64.6%), and other interventions (48.0%; IQR, 32.1%-66.7%). Clinical trial phase had the greatest variation in female enrollment; in phase 2/3 to phase 3 clinical trials, 51.7% (IQR, 38.9%-67.9%) of enrollees were female, and in phase 4 clinical trials, 51.1% (IQR, 36.4%-70.0%) were female. Phase 1 clinical trials had a median female enrollment of 42.9% (IQR, 27.8%-57.1%), and phase 1/2 to phase 2 clinical trials had a median female enrollment of 44.8% (IQR, 29.4%-62.5%).
Table 1. Proportion of Female Participants in Clinical Trials by Clinical Trial Feature.
| Feature | No. | Female proportion of participants, median (IQR), % | |
|---|---|---|---|
| Total studies | Total female participants | ||
| Fundinga | |||
| Industry | 9249 | 995 262 | 49.6 (33.3-65.6) |
| Academic | 6647 | 470 397 | 50.0 (34.8-72.0) |
| US government | 4124 | 886 371 | 46.7 (30.8-65.0) |
| Primary purpose | |||
| Treatment | 14 844 | 897 859 | 48.4 (33.0-66.7) |
| Basic scientific research | 782 | 17 496 | 48.1 (29.3-64.8) |
| Otherb | 2364 | 834 096 | 51.7 (38.5-70.0) |
| Prevention | 1514 | 476 769 | 53.6 (41.7-76.2) |
| Missing | 516 | 105 810 | 45.9 (30.1-64.4) |
| Intervention | |||
| Behavioral | 1346 | 285 894 | 56.7 (40.7-76.0) |
| Medical device | 3170 | 455 370 | 51.6 (36.4-70.6) |
| Biologic drugs or supplements | 15 262 | 1 266 289 | 48.0 (32.3-65.6) |
| Procedure | 1321 | 360 902 | 46.1 (31.7-64.6) |
| Other | 3158 | 523 205 | 48.0 (32.1-66.7) |
| Phase | |||
| Not applicablec | 5800 | 1 294 097 | 52.5 (37.5-73.4) |
| 1 | 1401 | 25 958 | 42.9 (27.8-57.1) |
| 1/2-2 | 7582 | 235 049 | 44.8 (29.4-62.5) |
| 2/3-3 | 2440 | 579 472 | 51.7 (38.9-67.9) |
| 4 | 2797 | 197 454 | 51.1 (36.4-70.0) |
| Blinding | |||
| None | 11 606 | 1 129 049 | 46.9 (32.0-64.9) |
| Double | 5944 | 601 746 | 50.7 (35.2-69.0) |
| Single | 2452 | 541 042 | 54.2 (40.0-72.3) |
| Missing | 18 | 60 193 | 50.5 (40.1-63.8) |
| Randomization | |||
| Nonrandomized | 8062 | 462 842 | 46.2 (30.8-64.7) |
| Randomized | 11 854 | 1 865 245 | 50.0 (35.6-68.9) |
| Missing | 104 | 3943 | 50.0 (33.3-65.2) |
| Overseen by a data safety monitoring committee | |||
| No | 10 135 | 1 221 154 | 50.0 (34.8-68.4) |
| Yes | 8265 | 688 597 | 46.9 (31.6-66.0) |
| Missing | 1620 | 422 279 | 50.0 (35.8-67.2) |
Abbreviation: IQR, interquartile range.
Funding categories were determined through data on the sponsor and collaborators. Industry funding includes clinical trials with an industry sponsor or collaborating agency. US government funding includes remaining clinical trials with a US government sponsor or collaborating agency.
Other primary purposes include diagnostic, screening, supportive care, health services research, and other interventions.
In the ClinicalTrials.gov registry, not applicable is used to describe clinical trials without US Food and Drug Administration–defined phases, including clinical trials of medical devices or behavioral interventions.
Clinical Trial Features Associated With Sex Representation
In model 1, which accounted for disease category, several disease categories were associated with lower female enrollment in the multivariable regression analysis (Table 2). Pediatric clinical trials had the most significant association with lower female enrollment (adjusted relative difference, −20.47%; 95% CI, −25.77% to −15.16%), followed by cardiology (adjusted relative difference, −18.68%; 95% CI, −22.87% to −14.47%) and infectious disease (adjusted relative difference, −18.51%; 95% CI, −24.25% to −12.76%) clinical trials. Less substantial associations were observed in clinical trials associated with gastroenterology (adjusted relative difference, −12.81%; 95% CI, −17.84% to −7.83%), sex-nonspecific nephrology and genitourinary disease (adjusted relative difference, −12.72%; 95% CI, −19.17% to −6.34%), psychiatry (adjusted relative difference, −11.29%; 95% CI, −15.80% to −6.81%), hematology (adjusted relative difference, −11.89%; 95% CI, −17.94% to −5.91%), and endocrinology (adjusted relative difference, −7.93%; 95% CI, −14.04% to −1.92%), which had negative associations with the proportion of female participants compared with all other clinical trials. No disease foci had a positive association with the proportion of female participants.
Table 2. Factors Associated With the Proportion of Female Participants Enrolled in Clinical Trialsa.
| Factor | Relative difference (95% CI), % |
|---|---|
| Fundingb | |
| Industry | 1 [Reference] |
| Academic | 2.38 (−0.73 to 5.44) |
| US government | 0.14 (−3.45 to 3.66) |
| Primary purpose | |
| Treatment | 1 [Reference] |
| Basic scientific research | 0.58 (−6.89 to 7.75) |
| Otherc | 4.29 (0.11 to 8.35) |
| Prevention | 8.48 (3.77 to 13.00) |
| Intervention | |
| All other clinical trials | 1 [Reference] |
| Behavioral | 4.17 (−1.84 to 9.94) |
| Medical device | −5.31 (−10.82 to 0.09) |
| Biologic drugs or supplements | −3.97 (−9.46 to 1.38) |
| Procedure | −1.54 (−6.61 to 3.40) |
| Other | −1.26 (−4.90 to 2.32) |
| Phase | |
| 2/3-3 | 1 [Reference] |
| Not applicabled | 1.44 (−3.56 to 6.29) |
| 1 | −5.43 (−12.18 to 1.15) |
| 1/2-2 | −3.07 (−7.48 to 1.26) |
| 4 | 2.44 (−2.40 to 7.13) |
| Blinding | |
| None | 1 [Reference] |
| Double | 2.12 (−1.79 to 5.94) |
| Single | 2.86 (−1.76 to 7.34) |
| Randomization | |
| Nonrandomized | 1 [Reference] |
| Randomized | −1.33 (−6.76 to 3.96) |
| Oversight by data safety monitoring committee | |
| No | 1 [Reference] |
| Yes | −1.30 (−3.92 to 1.28) |
| Disease focuse | |
| Musculoskeletal and trauma | 2.76 (−2.82 to 8.14) |
| Psychiatry | −11.29 (−15.80 to −6.81) |
| Cardiology | −18.68 (−22.87 to −14.47) |
| Neurology | 0.20 (−3.49 to 3.81) |
| Oncology | −1.29 (−5.40 to 2.74) |
| Pulmonology | −4.41 (−9.01 to 0.11) |
| Pediatrics | −20.47 (−25.77 to −15.16) |
| Endocrinology | −7.93 (−14.04 to −1.92) |
| Gastroenterology | −12.81 (−17.84 to −7.83) |
| Nutrition and metabolic | −2.14 (−7.70 to 3.28) |
| Infectious disease | −18.51 (−24.25 to −12.76) |
| Immunology | 0.92 (−3.70 to 5.41) |
| Otorhinolaryngology | −2.90 (−10.46 to 4.40) |
| Dermatology | 4.79 (−0.79 to 10.14) |
| Sex-nonspecific nephrology and genitourinary | −12.72 (−19.17 to −6.34) |
| Hematology | −11.89 (−17.94 to −5.91) |
| Congenital | −0.75 (−7.77 to 6.01) |
Model 1 includes disease category.
Funding categories were determined through data on the sponsor and collaborators. Industry funding includes clinical trials with an industry sponsor or collaborating agency. US government funding includes remaining clinical trials with a US government sponsor or collaborating agency.
Other primary purposes include diagnostic, screening, supportive care, health services research, and other interventions.
In the ClinicalTrials.gov registry, not applicable is used to describe clinical trials without US Food and Drug Administration–defined phases, including clinical trials of medical devices or behavioral interventions.
Clinical trials could have more than 1 disease category. For analysis, each disease category was treated as a binary variable.
In the same model, the primary purpose of the clinical trial had the most significant association with the proportion of female enrollees. Clinical trials of preventive interventions and other primary purposes (including diagnostic, screening, supportive care, health services research, and other interventions) had adjusted relative differences of 8.48% (95% CI, 3.77%-13.00%) and 4.29% (95% CI, 0.11%-8.35%) in female enrollment, respectively, compared with clinical trials of treatment (Table 2). These associations were more substantial in model 1 relative to model 2, which did not account for disease category (eTable 2 in the Supplement). In contrast, although blinding and oversight by a data monitoring committee had significant associations with the proportion of female enrollees in model 2, these associations were not observed when disease category was included in model 1. Funding indicated no significant association with the proportion of female enrollees in either model.
Discussion
This cross-sectional study of 20 020 US-based clinical trials found that, although male and female individuals had similar representation in all clinical trials conducted over the past 20 years, sex bias in clinical trial enrollment persists within medical specialties. Few previous studies have compared sex representation in clinical trials with burden of disease or have analyzed the association of clinical trial features with female representation across medical specialties. Compared with their respective burdens of disease, female participants are most underrepresented in oncology clinical trials, and male participants are most underrepresented in clinical trials of musculoskeletal disorders and trauma. Even after accounting for other clinical trial factors, disease category had the most significant association with lower female enrollment compared with other clinical trial features, particularly in the fields of cardiology, pediatrics, and infectious disease.
The present analysis allowed for the novel assessment of associations between different disease areas and female enrollment. The analyses found that female participants were underrepresented in oncology, neurology, immunology, urology, cardiology, and hematology relative to their disease burden. The finding that lower proportions of female participants were enrolled in clinical trials in cardiology and oncology is consistent with historical patterns in both fields.7,24,25,26,27 This finding is concerning because cardiologic and oncologic diseases are the leading causes of death among female individuals in the US.25,26 Furthermore, clinical trials provide an important mechanism for patients to access the best innovative therapies, particularly in the field of oncology. Underrepresentation of female participants in these clinical trials widens the previously documented sex gap in outcomes such as mortality.25 Parity in clinical trial enrollment can be considered a minimum standard, and efforts are needed to actively focus research on the female population. The historical underrepresentation of female participants in clinical trials is likely associated with the relative deficiency in knowledge of preventive strategies, disease manifestations, prognosis, and treatment of cardiovascular and neoplastic disease in the female population.4,8 This paradigm is also evident for obstetric conditions. Most pregnant women are excluded from clinical trials of diseases that may have consequences for their health,28 and clinical trials specifically focused on obstetric conditions comprise fewer than 2% of all clinical trials.18 A greater allocation of resources for female-focused clinical trials may be important to improving care and discerning the heterogenous manifestations of disease within the female population.
The present study highlights lesser-known disparities in immunology, sex-nonspecific nephrology and genitourinary disease, and hematology clinical trials. Despite the enrollment disparity observed in the descriptive analysis, these inequities were not associated with lower female enrollment in the multivariable analyses, suggesting that perhaps lower female enrollment is associated with other clinical trial factors. These disease areas warrant further investigation to identify the reasons that female enrollees represent a minority of clinical trial participants. Sex differences across these fields are well documented and important to developing beneficial preventive, diagnostic, and treatment strategies. Increased parity, in combination with sex-specific analysis, could elucidate these differences and provide the best approach to reducing corresponding DALYs for each sex.
This study also presents novel findings on male underrepresentation in clinical trials. Male enrollees comprised a minority of participants in 3 disease categories and were underrepresented compared with their disease burden in 8 disease categories. This imbalance is consistent with the observations of a previous study, which indicated that sex bias may have negative implications for both sexes.29 The finding that clinical trials of preventive interventions were independently associated with greater female enrollment is consistent with the established paradigm regarding sex-specific use of preventive services and access to health care.29 Identifying areas of research in which sex bias disadvantages male individuals is important to improving population health. The present study’s finding of male underrepresentation in mental health and trauma research assumes greater importance in American society, in which suicide, violence, and substance use are increasingly associated with higher morbidity and premature mortality in the male population.30
This study included an innovative multivariable analysis of the clinical trial features associated with female enrollment across medical specialties. Previous univariable, often single-specialty, analyses suggested that there were associations between funding, randomization, study phase, number of sites, intervention type, and enrollment.10,13,25 One previous study compared sex bias with the prevalence of disease among global studies registered in the ClinicalTrials.gov database; however, the study used a limited analysis that controlled only for registry submission year and disease category.24 The novel findings of the present study may reflect the larger sample, longer study period, or different dynamics within medical fields. For example, within cardiology clinical trials, several studies indicated that female enrollment varied with individual diseases and funding for those diseases.10,13,25,31 Studies from other fields have similarly reported that clinical trial features may vary within disease foci.31,32 Medical fields with more balanced sex representation may serve as a model for decreasing sex bias in clinical trials.
The consistently high rates of sex reporting in clinical trials are encouraging. The current study found higher rates of sex reporting compared with a previous study of clinical trial publications from the same period.31 Discrepancies between reporting in the ClinicalTrials.gov registry and published results represent an important gap; given that registry reporting indicates that sex data exist, these data can be included in clinical trial publications and used for sex-specific analysis. Some medical journals do not require sex reporting or sex-specific analysis for publication.33 We propose that sex reporting represents an important step toward equitable enrollment and examination of sex-specific pathophysiologic disease factors and treatment.
Despite the high rates of sex reporting in the ClinicalTrials.gov registry, a meaningful analysis of the representation of gender was not possible because of the small number of clinical trials that included and reported on nonbinary genders or transgender health, highlighting a need for greater inclusion of gender diversity in medical research. A standardized system that includes all sexes and genders, including transgender and nonbinary genders, in reporting is necessary to improve health for all. The relative absence of the gender nonbinary and transgender community from clinical trials limits medical progress for these communities.
Strengths and Limitations
This study has several strengths. A 2018 study has called for the comparison of disease burden with sex representation as the next step in understanding sex bias in clinical research.13 Our study assesses 2 databases that accurately capture the entire US landscape of clinical trials and burden of disease, avoiding the sampling biases found in previous studies by comparing US data from the ClinicalTrials.gov registry with global disease burden. Although previous investigations narrowed their focus to specific diseases,7,31,32,34,35 the present study provides novel data, assessing and comparing 17 disease categories. This study’s distinct multivariable analysis examines potential factors, including disease category, that may be associated with sex bias among all US-based clinical trials. The study also elucidates important factors that may be negatively associated with male health, an underexamined area of sex bias.
This study also has limitations. The study does not address whether potential participants (male or female) were approached for study participation. In addition, the point in the clinical trial process at which barriers to enrollment occur is not clear. Database limitations within the ClinicalTrials.gov registry also exist. Most clinical trials do not report results, presenting a possible selection bias and preventing extrapolation to the entirety of clinical research. The National Library of Medicine does not require or enforce valid data entry in the ClinicalTrials.gov registry, and quality reviews may only identify a small proportion of data errors.36 Other established limitations include changes to the database over time and heterogeneity in data entry. In addition, disease prevalence may have changed over the study period, and the GBD data account for only a portion of the years examined.
Conclusions
Professional and governmental organizations have mobilized numerous efforts to increase female representation in clinical trials over the past 30 years.9 Although sex equity has progressed, sex bias persists within medical fields, with potentially negative consequences for all individuals. Sex reporting and sex-specific analysis are warranted for all research bodies. Furthermore, efforts are needed to ensure that sex representation better reflects the health burdens of the population. Without sex-specific analysis and increased parity, the interpretation of data for both male and female populations remains unreliable,8 and the benefits of research may not reach both groups.27,37 Analysis of the most important factors associated with sex bias within medical fields may reveal areas for improvement and mechanisms to increase inclusivity so that the research represents and serves both sexes.
eMethods 1. Clinical Trial Disease Category and Medical Subject Heading (MeSH) Categories
eMethods 2. Global Burden of Disease Data and Medical Subject Heading (MeSH) Categories
eTable 1. Comparison of Female Burden of Disease and Female Enrollment by Disease Category
eTable 2. Factors Associated With the Proportion of Female Participants Enrolled in Clinical Trials
References
- 1.Murciano-Goroff YR. Differences in the percentage of illustrations showing males versus females in general medicine and general surgery textbooks. Med Sci Educ. 2015;25(2):123-126. doi: 10.1007/s40670-015-0116-8 [DOI] [Google Scholar]
- 2.Hawkes S, Haseen F, Aounallah-Skhiri H. Measurement and meaning: reporting sex in health research. Lancet. 2019;393(10171):497-499. doi: 10.1016/S0140-6736(19)30283-1 [DOI] [PubMed] [Google Scholar]
- 3.Mazure CM, Jones DP. Twenty years and still counting: including women as participants and studying sex and gender in biomedical research. BMC Womens Health. 2015;15:94. doi: 10.1186/s12905-015-0251-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Holdcroft A. Gender bias in research: how does it affect evidence based medicine? J R Soc Med. 2007;100(1):2-3. doi: 10.1177/014107680710000102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sugimoto CR, Ahn YY, Smith E, Macaluso B, Lariviere V. Factors affecting sex-related reporting in medical research: a cross-disciplinary bibliometric analysis. Lancet. 2019;393(10171):550-559. doi: 10.1016/S0140-6736(18)32995-7 [DOI] [PubMed] [Google Scholar]
- 6.van der Graaf R, van der Zande ISE, den Ruijter HM, et al. Fair inclusion of pregnant women in clinical trials: an integrated scientific and ethical approach. Trials. 2018;19(1):78. doi: 10.1186/s13063-017-2402-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Holroyd-Leduc JM, Kapral MK, Austin PC, Tu JV. Sex differences and similarities in the management and outcome of stroke patients. Stroke. 2000;31(8):1833-1837. doi: 10.1161/01.STR.31.8.1833 [DOI] [PubMed] [Google Scholar]
- 8.Bartlett C, Doyal L, Ebrahim S, et al. The causes and effects of socio-demographic exclusions from clinical trials. Health Technol Assess. 2005;9(38):iii-iv, ix-x, 1-152. doi: 10.3310/hta9380 [DOI] [PubMed] [Google Scholar]
- 9.Clayton JA, Collins FS. Policy: NIH to balance sex in cell and animal studies. Nature. 2014;509(7500):282-283. doi: 10.1038/509282a [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mansukhani NA, Yoon DY, Teter KA, et al. Determining if sex bias exists in human surgical clinical research. JAMA Surg. 2016;151(11):1022-1030. doi: 10.1001/jamasurg.2016.2032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tunis SR, Stryer DB, Clancy CM. Practical clinical trials: increasing the value of clinical research for decision making in clinical and health policy. JAMA. 2003;290(12):1624-1632. doi: 10.1001/jama.290.12.1624 [DOI] [PubMed] [Google Scholar]
- 12.Glasgow RE, Lichtenstein E, Marcus AC. Why don’t we see more translation of health promotion research to practice? rethinking the efficacy-to-effectiveness transition. Am J Public Health. 2003;93(8):1261-1267. doi: 10.2105/ajph.93.8.1261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Prakash VS, Mansukhani NA, Helenowski IB, Woodruff TK, Kibbe MR. Sex bias in interventional clinical trials. J Womens Health (Larchmt). 2018;27(11):1342-1348. doi: 10.1089/jwh.2017.6873 [DOI] [PubMed] [Google Scholar]
- 14.Tasneem A, Aberle L, Ananth H, et al. The database for aggregate analysis of ClinicalTrials.gov (AACT) and subsequent regrouping by clinical specialty. PLoS One. 2012;7(3):e33677. doi: 10.1371/journal.pone.0033677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Global Data Health Exchange. Global Burden of Disease Study 2016 (GBD 2016) data resources. Institute for Health Metrics and Evaluation, University of Washington; 2016. Accessed June 5, 2020. http://ghdx.healthdata.org/gbd-2016
- 16.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573-577. doi: 10.7326/0003-4819-147-8-200710160-00010 [DOI] [PubMed] [Google Scholar]
- 17.Turner B, Rajeshuni N, Tran EM, et al. Characteristic of ophthalmology trials registered in ClinicalTrials.gov, 2007-2018. Am J Ophthalmol. 2020;211:132-141. doi: 10.1016/j.ajo.2019.11.004 [DOI] [PubMed] [Google Scholar]
- 18.Steinberg JR, Weeks BT, Reyes GA, et al. The obstetrical research landscape: a cross-sectional analysis of clinical trials from 2007-2020. Am J Obstet Gynecol MFM. 2021;3(1):100253. doi: 10.1016/j.ajogmf.2020.100253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Magnani CJ, Steinberg JR, Harmange CI, et al. Clinical trial outcomes in urology: assessing early discontinuation, results reporting, and publication in ClinicalTrials.gov registrations 2007-2019. J Urol. 2021;205(4):1159-1168. doi: 10.1097/JU.0000000000001432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Connell R. Gender, health and theory: conceptualizing the issue, in local and world perspective. Soc Sci Med. 2012;74(11):1675-1683. doi: 10.1016/j.socscimed.2011.06.006 [DOI] [PubMed] [Google Scholar]
- 21.Tse T, Fain KM, Zarin DA. How to avoid common problems when using ClinicalTrials.gov in research: 10 issues to consider. BMJ. 2018;361:k1452. doi: 10.1136/bmj.k1452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Papke LE, Wooldridge JM. Econometric methods for fractional response variables with an application to 401(k) plan participation rates. J Appl Econ (Chichester Engl). 1996;11(6):619-632. doi: 10.1002/(SICI)1099-1255(199611)11:6<619::AID-JAE418>3.0.CO;2-1 [DOI] [Google Scholar]
- 23.Buuren SV, Groothuis-Oudshoorn K. mice: multivariate imputation by chained equations in R. J Stat Softw. 2011:45:1-68. doi: 10.18637/jss.v045.i03 [DOI] [Google Scholar]
- 24.Feldman S, Ammar W, Lo K, Trepman E, van Zuylen M, Etzioni O. Quantifying sex bias in clinical studies at scale with automated data extraction. JAMA Netw Open. 2019;2(7):e196700. doi: 10.1001/jamanetworkopen.2019.6700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kwiatkowski K, Coe K, Bailar JC, Swanson GM. Inclusion of minorities and women in cancer clinical trials, a decade later: have we improved? Cancer. 2013;119(16):2956-2963. doi: 10.1002/cncr.28168 [DOI] [PubMed] [Google Scholar]
- 26.Carcel C, Woodward M, Balicki G, et al. Trends in recruitment of women and reporting of sex differences in large-scale published randomized controlled trials in stroke. Int J Stroke. 2019;14(9):931-938. doi: 10.1177/1747493019851292 [DOI] [PubMed] [Google Scholar]
- 27.Harris DJ, Douglas PS. Enrollment of women in cardiovascular clinical trials funded by the National Heart, Lung, and Blood Institute. N Engl J Med. 2000;343(7):475-480. doi: 10.1056/NEJM200008173430706 [DOI] [PubMed] [Google Scholar]
- 28.Shields KE, Lyerly AD. Exclusion of pregnant women from industry-sponsored clinical trials. Obstet Gynecol. 2013;122(5):1077-1081. doi: 10.1097/AOG.0b013e3182a9ca67 [DOI] [PubMed] [Google Scholar]
- 29.The Lancet. Raising the profile of men’s health. Lancet. 2019;394(10211):1779. doi: 10.1016/S0140-6736(19)32759-X [DOI] [PubMed] [Google Scholar]
- 30.Stein EM, Gennuso KP, Ugboaja DC, Remington PL. The epidemic of despair among white Americans: trends in the leading causes of premature death, 1999-2015. Am J Public Health. 2017;107(10):1541-1547. doi: 10.2105/AJPH.2017.303941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Weinberger AH, McKee SA, Mazure CM. Inclusion of women and gender-specific analyses in randomized clinical trials of treatments for depression. J Womens Health (Larchmt). 2010;19(9):1727-1732. doi: 10.1089/jwh.2009.1784 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kalliainen LK, Wisecarver I, Cummings A, Stone J. Sex bias in hand surgery research. J Hand Surg Am. 2018;43(11):1026-1029. doi: 10.1016/j.jhsa.2018.03.026 [DOI] [PubMed] [Google Scholar]
- 33.Johnston RE, Heitzeg MM. Sex, age, race and intervention type in clinical studies of HIV cure: a systematic review. AIDS Res Hum Retroviruses. 2015;31(1):85-97. doi: 10.1089/aid.2014.0205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zagni E, Simoni L, Colombo D. Sex and gender differences in central nervous system–related disorders. Neurosci J. 2016;2016:1-13. doi: 10.1155/2016/2827090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Farzal Z, Stephenson ED, Kilpatrick LA, Senior BA, Zanation AM. Sex bias: is it pervasive in otolaryngology clinical research? Laryngoscope. 2019;129(4):858-864. doi: 10.1002/lary.27497 [DOI] [PubMed] [Google Scholar]
- 36.Viergever RF, Ghersi D. The quality of registration of clinical trials. PLoS One. 2011;6(2):e14701. doi: 10.1371/journal.pone.0014701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sen G, Ostlin P, George A; Women and Gender Equity Knowledge Network. Unequal, unfair, ineffective and inefficient. gender inequity in health: why it exists and how we can change it. final report to the WHO Commission on Social Determinants of Health. 2007. Accessed April 13, 2020. https://www.who.int/social_determinants/resources/csdh_media/wgekn_final_report_07.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods 1. Clinical Trial Disease Category and Medical Subject Heading (MeSH) Categories
eMethods 2. Global Burden of Disease Data and Medical Subject Heading (MeSH) Categories
eTable 1. Comparison of Female Burden of Disease and Female Enrollment by Disease Category
eTable 2. Factors Associated With the Proportion of Female Participants Enrolled in Clinical Trials